Embed Size (px)
Citation preview

Management of Chronic ObstructivePulmonary Disease
Maher Khdour, Hussein Hallak, and Hani Abdeen
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Etiology, Pathogenesis, and Pathophysiology of the Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Prevalence and Disease Burden in Arab Countries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Morbidity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Pulmonary Function and Spirometry Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Lung Function Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Stages of COPD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Chest X-Rays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Arterial Blood Gas (ABG) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Sputum and Hematology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Clinical Presentation and Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Management of COPD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Pharmacological Management of COPD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Non-pharmacological Management of COPD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
AbstractThe World Health Organization (WHO) revealed that the fourth leading cause ofchronic morbidity and mortality worldwide is chronic obstructive pulmonarydisease (COPD). There is increased awareness of COPD by the medical
M. Khdour (*)Faculty of Pharmacy, Al-Quds University, Jerusalem, Palestinee-mail: [email protected]; [email protected]
H. Hallak · H. AbdeenFaculty of Medicine, Al-Quds University, Jerusalem, Palestine
© Springer Nature Switzerland AG 2019I. Laher (ed.), Handbook of Healthcare in the Arab World,https://doi.org/10.1007/978-3-319-74365-3_128-1
1

community. However, it remains a major public health problem because patientsand public health and government officials are unaware of it or ignore it.
The important fact to address is that this COPD epidemic is increasing in theArab world due to smoking. Despite persistent increases in the prevalence andincidence of COPD, health-care professionals worldwide underdiagnose andundertreat the disease, and for many patients the disease is mostly unrecognized.The purpose of this chapter is to describe factors that lead to increase in thedisease prevalence and to highlight the issues related to under management ofCOPD.
High-risk individuals, such as long-term smokers, often ignore the symptomsof chronic pulmonary disease until disability occurs. Signs and symptoms areoften insidious in nature and play an important role in preventing early diagnosisand treatment of chronic pulmonary diseases. Patients having difficulty breathingwith shortness of breath, cough, sputum production, and nose or throat irritationsthat do not subside within 2 weeks need medical attention. The importance ofincreasing public awareness of the consequences of smoking and the risk ofCOPD is imperative.
The definition, signs and symptoms, major risk factors associated with theonset of COPD, and the treatment plans for patients with stable COPD and forthose with an acute exacerbation are described in this chapter.
KeywordsCOPD · Middle East · Arab · Assessment · Management · Prevalence ofsmoking · Occupational dust
Introduction
Definition
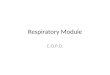
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines chronicobstructive pulmonary disease (COPD) as “COPD is a common, preventable andtreatable disease that is characterized by persistent respiratory symptoms and airflowlimitation that is due to airway and/or alveolar abnormalities usually caused bysignificant exposure to noxious particles or gases” (GOLD 2017). The disease isusually progressive and not fully reversible and is primarily caused by cigarettesmoking. The disease severity is related to other factors, including the systemiceffects (comorbidities) exhibited in patients with COPD (WHO 2004; ATS 1995)(Fig. 1).
COPD is characterized by chronic inflammation which destroys the lung paren-chyma. This process damages the small airways due to the loss of alveolar attach-ments and it decreases elastic recoil of the lung. These structural alterations and thenarrowing of the small airways diminish the capacity of the airways to stay openthroughout expiration. Spirometry is the most commonly used and reproduciblemethod to test lung function and airway limitation.
2 M. Khdour et al.

Emphysema is believed to be associated with an imbalance in the amounts ofproteases and antiproteases. Physiologic abnormalities characteristic of emphysema(lung parenchymal destruction) include:
• Increased lung compliance: destruction of elastin in lung parenchyma causes lossof elastic recoil, the lungs become permanently overdistended.
• Increased airway resistance: the small airways either collapse or narrow duringexpiration due to destruction of elastic lung tissue.
The breathing pattern of patients with emphysema includes an increased respira-tory rate, accessory muscle breathing, and a prolonged expiratory phase resultingfrom airway narrowing or collapse on expiration. These individuals spontaneouslyexhibit or practice pursed-lip breathing technique, which facilitates effective airexhalation.
The pathology of chronic bronchitis includes chronic inflammatory changes andhypertrophy of mucus-secreting glands in the small airways (Konzem and Stratton2002). Mucous gland hypertrophy and hyperplasia from chronic irritation causeexcessive mucus production. Clinically, patients are characterized by the presence ofa chronic productive cough for 3 months in each of 2 successive years where othercauses of chronic cough have been excluded.
Etiology, Pathogenesis, and Pathophysiology of the Disease
Smoking Habits in the Arab WorldMore than 90% of COPD patients are cigarette smokers, making it the primarycausative factor of COPD. However, only 15–20% of heavy smokers developCOPD. Patients with COPD experience a form of inflammation in their respiratorytract that is a variation of the natural inflammatory response that occurs in response
Fig. 1 Fundamental mechanisms of airflow limitation in COPD (Konzem and Stratton 2002)
Management of Chronic Obstructive Pulmonary Disease 3

to chronic irritants such as cigarette smoke (Sze et al. 2015). Some COPD patientshave never smoked, and the course of the inflammatory response in such patients isunknown. Lung inflammation is also typically modified by oxidative stress and anexcess of proteinases. Jointly, these mechanisms contribute to the main pathologicalalterations in COPD.
Smoking cessation does not inhibit lung inflammation, and the reasons for this arenot clear. However, it might involve autoantigens and fluctuations in the lungmicrobiome (Lee et al. 2007).
COPD patients have increases in macrophages in their peripheral airways, lungparenchyma, and pulmonary vessels, and this occurs in conjunction with higherlevels of activated neutrophils and lymphocytes, including Tc1, Th1, Th17, andILC3 cells. In addition, in some patients, there are also increased levels of eosino-phils and Th2 or ILC2 cells, particularly in cases of a clinical overlap withasthma (Turato et al. 2001).
Smoking and subsequent development of COPD is an ever-increasing epidemicin Arab countries, with no signs of decline. The BREATHE study confirms that theprevalence of smoking and COPD has risen significantly in the Middle East–NorthAfrica (MENA) region, in large part due to the lack of knowledge of the risks ofsmoking and COPD (Khattab et al. 2012). Water pipe, cigar, and cigarette smoking isalso increasing across the Middle East and MENA region. The smoking rate in menranges from 29.7% in Morocco to 56% in Lebanon, whereas in women it rangesfrom 1.4% in Morocco to 47.3% in Lebanon. Overall, the highest rates of cigarettesmoking are in Jordan, Lebanon, and Syria (Khattab et al. 2012).
Cigarette smokers have an increased incidence of respiratory symptoms andaberrations in lung function. Thus, smokers experience larger decreases in annualrates of FEV1 and higher COPD mortality rates compared to nonsmokers (Jindal etal. 2006; Al-Fayez et al. 1988).
GenesCOPD is an illustration of a gene-environment interaction. Hereditary alpha-1antitrypsin (AAT) deficiency is the best documented genetic risk factor of COPD(Stoller and Aboussouan 2005; Blanco et al. 2006). Individuals of Northern Euro-pean decent commonly possess this uncommon recessive trait. Both nonsmokers andsmokers with AAT deficiency develop premature and accelerated panlobular emphy-sema and a reduction in lung function. However, smoking markedly increases thisrisk (Banasik 2001). Most patients with AAT deficiency are misdiagnosed orundiagnosed. Health-care professionals should suspect ATT deficiency whenemphysema occurs in patients under age 60, even those with a significant smokinghistory (Carson and Hieber 2001).
Inhalational ExposuresThere is a variable exposure to an assortment of inhaled particles over one’s lifetime,and one way to characterize this is to consider the sum of the burden of the inhaledparticles. Each of the different particles adds a unique risk to health risk dependingon their size and composition. Examples of inhaled particulate matter includeoutdoor air pollution, occupational exposure to dust and fumes, biomass-smoke
4 M. Khdour et al.

inhalation, etc. (Khattab et al. 2012). The cumulative effect of the exposure toinhaled materials (vapors, irritants, and fumes) known to cause COPD on theirown also adds to the total risk (Trupin et al. 2003; Matheson et al. 2005; Hnizdoet al. 2002).
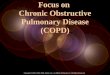
Occupational exposures, such as from organic and inorganic dust, chemicalagents, and fumes, are risk factors for COPD that are commonly underappreciated(Matheson et al. 2005). In addition, some forms of indoor pollution, such as heatingor cooking in inadequately ventilated places, are also important risk factors forCOPD (Warwick and Doig 2004). On the other hand, indoor air pollutants (tobacco,coal, wood, volatile organic compounds, and carbon monoxide) also contribute todevelopment of COPD (Hu et al. 2010) (Fig. 2).
Prevalence and Disease Burden in Arab Countries
Epidemiology
The ideal way for COPD diagnosis is through the use of spirometry that measureslung function along with symptoms and risk factors. Unfortunately, diagnosis ofCOPD in some countries can be made based on symptoms alone (Cerveri et al.2001). As such, one might speculate that the estimated prevalence is likely higherthan currently reported. This may also explain the conflicting epidemiological dataon COPD in different countries.
A systemic meta-analysis showed that overall prevalence of COPD in men was14.3% and women 7.6 across the world. Moreover, global prevalence of COPDincreased from 10.7% in 1990 to 11.7% in 2010 (WHO 2016). There has been a
Fig. 2 Risk factors for COPD (GOLD 2017)
Management of Chronic Obstructive Pulmonary Disease 5

surprising increase in the prevalence of smoking in the Eastern MediterraneanRegion (EMR) from 11.8% in 1990 to 13.4% in 2010 (Adeloye et al. 2015)
The Global Burden of Disease project identified COPD as the sixth leading causeof mortality. The disease accounts for 4.9% of total deaths in low- or middle-incomecountries (WHO 2004). According to WHO estimates, 64 million people currentlyhave COPD worldwide, and COPD is predicted to be the third leading cause of deathglobally by 2030 (WHO 2016). The BREATHE study, conducted in the Middle Eastand North Africa (Tageldin et al. 2012), reported the prevalence of COPD to be 3.6%(range: 1.9% in UAE to 6.1% in Syria). COPD was more frequent in men (5.2%)than in women (1.8%). As expected, the frequency of symptoms was significantlyhigher in cigarette smokers, as well as in water pipe users.
The Burden of Obstructive Lung Disease (BOLD) studies conducted in theMENA and Gulf region estimated the prevalence of COPD in Tunisia, Saudi Arabia,and Morocco to be 7.8%, 4.2%, and 12.6%, respectively (Al Ghobain et al. 2015).
Morbidity
Databases on COPD mortality are more readily available than morbidity as mea-sured by physician visits, hospitalization, or emergency department visits. Further-more, typical morbidity databases are not as dependable as mortality databases. Eventhough it is incomplete, the morbidity data indicates that COPD is greater in menthan in women and increases with age (Soriano et al. 2000). Other chronic diseaseconditions that may not be directly related to COPD can also affect morbidity fromCOPD (e.g., diabetes mellitus, musculoskeletal disease). Coexistence of chronicdisease negatively interferes with COPD management or negatively health status.
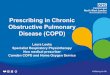
It is estimated that there are eight million COPD physician office/hospital outpa-tient visits in the United States and another 1.5 million emergency room visits and673,000 hospitalizations related to COPD (CDC 2002). The BREATHE study forthe Middle East and North Africa indicates that 62% of COPD patients had physi-cian office visits in the past year, of which 21% were hospitalized and 19% visitedthe emergency department (Uzaslan et al. 2012). Moreover, 28.4% reported that theirrespiratory condition prevented them from working, and this proportion rose to47.8% in subjects who perceived their respiratory condition as severe (Fig. 4).
Mortality
COPD resulted in more than three million deaths globally in 2012, and it is estimatedthat COPD will be the third leading cause of death worldwide in 2030 (WHO 2016).The WHO distributes the annual mortality statistics related to select medical condi-tions (http://www.who.int/evidence). Even with the variability observed with thedata per region, there is no doubt that COPD is an important risk factor for death allover the world. According to the Global Burden of Disease Study, COPD was thesixth leading cause of death in 1990, and by 2020, it is predicted to become the third
6 M. Khdour et al.

leading cause of death globally. The increased death rate will likely be related to theexpanding smoking epidemic, the increased life expectancies, and the changingdemographics in many countries. It is likely that demographic changes are strongdrivers of the smoking epidemic (Lopez et al. 2006) (Fig. 3).
Pulmonary Function and Spirometry Tests
Lung Function Test
Spirometry tests are used in diagnosis of COPD and for following the progression ofdisease by measuring pulmonary function; however, it does not identify diseasecauses. Physiologic alterations that occur early in the disease can be detected byspirometry testing.
Spirometer measures airflow over time in fully inflated lungs and can identifyairflow obstruction. Forced vital capacity (FVC) measures the entire exhaled breath;forced expiratory volume in one second (FEV1) is the amount of air exhaled in thefirst second. Both of these measurements are reduced in COPD (Murphy 2004;GOLD 2017). Some values may sometimes be used for simplicity, such as thespirometer cut points (e.g., the post-bronchodilator FEV1/FVC ratio < 0.70 or theFEV1 < 80, 50, or 30% as predicted for mild, moderate, or severe disease,respectively). However, there is no clinical validation for these cut points. Currentdata supports the use of a fixed ratio. For example, the post-bronchodilator FEV1/FVC surpassed 0.70 in all age groups tested in a random population, where a valueof 70% after treatment with bronchodilators indicated COPD (Johannessen et al.2006).
Fig. 3 Impact on work activities according to the degree of perceived severity. Open bars, milddisease severity; gray bars, moderate disease severity; black bars, severe disease severity. Data arepresented for the 1264 subjects providing data on perceived disease severity and on impact on work.(Source: Uzaslan 2012)
Management of Chronic Obstructive Pulmonary Disease 7

Stages of COPD
The airflow limitation severity classification for COPD is shown in Table 1. Definedspirometric cut points were used for clarity. In addition, spirometry was completedfollowing the administration of a tolerable dose of at least one short-acting inhaledbronchodilator so that the variability was minimized (Mirza et al. 2018)
Symptoms that characterize COPD are sputum production, cough, and chronicprogressive dyspnea. Sputum production and chronic cough may precede airflowlimitation by many years. Hence, the diagnosis of COPD can be made at any stage ofthe illness (Fig. 4).
Chest X-Rays
Chest X-rays can also help in the diagnosis of COPD patients. Typical chest X-rayfilms demonstrate a flat, low diaphragm with overdistention of the lungs and an
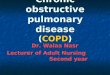
Fig. 4 A normal spirometry tracing and a spirometry tracing of typical patient with obstructivedisease (GOLD 2017)
Table 1 Airflow limitation severity classification for COPD patients
GOLD I Mild FEV1 � 80% predicted
GOLD II Moderate 50% � FEV1 <80% predicted
GOLD III Severe 30% � FEV1 < 50% predicted
GOLD IV Very Severe FEV1 < 30% predicted or
8 M. Khdour et al.

increased anteroposterior diameter of the chest. Increased bronchovascular markingscan occur in patients with chronic bronchitis.
Arterial Blood Gas (ABG)
ABG show mild or moderate hypoxemia without hypercapnia in the early stages ofCOPD. Alternatively, patients may develop severe hypoxemia and hypercapnia atlater stages of the disease. Symptoms may worsen during exercise, exacerbations,and sleep.
Sputum and Hematology
Sputum may be cultured for bacterial Gram stain and antibiotic sensitivity, with S.pneumoniae and H. influenzae being the most frequently observed pathogens.Chronic bronchitis is commonly associated with bronchial epithelial cells andneutrophils. Complete blood counts show erythrocytosis as measured by PaO2 levelsbelow 55 mm Hg. In addition, an AAT assay also may be requested.
Clinical Presentation and Assessment
COPD is a chronic, progressive disease, and the most distinctive symptom of COPDis difficulty in breathing (dyspnea). The first symptoms are intermittent, and this thenbecomes an everyday occurrence. “Chronic bronchitis” refers to regular sputumproduction for >3 months.
The modified Medical Research Council (mMRC) dyspnea scale is used to assessthe symptoms (Bestall et al. 1999; Nishimura et al. 2002), and a score�2 is used as acutoff point to separate “less breathlessness” and “more breathlessness” (Jones et al.2011, 2013).
Questionnaires such as the CAT (http://www.catestonline.org) and clinical COPDquestionnaire (CCQ; http://www.ccq.nl) are still used in assessment of COPD.
Management of COPD
Pharmacological Management of COPD
The GOLD 2017 and 2018 management strategies recommend a combined assess-ment of COPD based on symptoms and exacerbations to categorize patients intoclinical phenotypes (groups A–D). These groups have distinct pharmacologicaltreatment recommendations covering initial management and a stepwise approachto follow-up treatment (Fig. 5).
Management of Chronic Obstructive Pulmonary Disease 9

Pharmacologic therapy is used to diminish the incidence and gravity of exacer-bations. It also aids in preventing and controlling symptoms, improving exercisetolerance, and improving the overall health of the patient. COPD is a progressivedisease; none of the COPD medications modify the long-term decline in lungfunction (Vestbo et al. 1999; Burge et al. 2000)
Table 2 lists commonly used classes of medications used in treatment of COPD.Selection of individual therapies depends on a patient’s response and availability ofmedication.
BronchodilatorBronchodilators are the cornerstone in the management of COPD symptoms (Grosset al. 1989; Vathenen et al. 1988). They are commonly used by patients as needed forrelief of worsening and persistent symptoms or on a regular basis to reduce orprevent symptoms.
Beta2-AgonistsBeta2-agonists are available as short-acting (SABA) and long-acting (LABA) med-ications. An effect of 4–6 h can be expected from SABAs (Datta et al. 2003). Theduration of action of LABAs is at least 12 h and may even benefit from SABAtherapy as needed by patients.
LABAs significantly improve lung volumes, FEV1, exacerbation rate, dyspnea,number of hospitalizations, and overall health status (Kew et al. 2013). Unfortu-nately, beta2-agonists do not alter the course of lung function degeneration ormortality. The two most popular LABAs are formoterol and salmeterol commonlyprescribed for twice daily use. Indacaterol is a LABA that is prescribed for use once
Fig. 5 ABCD assessment tool by GOLD 2017. mMRC modified Medical Research Council(dyspnea scale), CAT COPD-assessment test
10 M. Khdour et al.

Table 2 Commonly used drugs in COPD
Drug Inhaler (μg)
Solutionfornebulizer(mg/ml) Oral
Vials forinjection(mg)
Durationof action(hours)
β2-agonistsShort-acting
Fenoterol 100–200 (MDI) 1 0.50%(syrup) 4–6
Salbutamol(albuterol)
100,200(MDI &DPI)
5 5 mg (pill)Syrup0.024%
0.2,0.25 4–6
Terbutaline 400,500 (DPI) – 2.5,5 (pill) 0.2,0.25 4–6
Long-acting
Formoterol 4.5–12 (MDI & DPI) 12+
Salmeterol 25–50 (MDI & DPI) 12+
Anticholinergics
Short-acting
Ipratropiumbromide
20,40 (DMI) 0.25–0.5 6–8
Oxitropiumbromide
100 (MDI) 1.5 7–9
Long-acting
Tiotropium 18 (DPI) 24+
Combination short-acting β2-agonists plus anticholinergic in one inhaler
Fenoterol/ipratropium
200/80 (MDI) 1.25/0.5 6–8
Salbutamol/ipratropium
75/15 MDDI) 0.75/4.5 6–8
Methylxanthines
Aminophylline 200–600 mg(pill)
240 mg Variable,up to 24
Theophylline (SR) 100–600 mg(pill)
Variable,up to 24
Inhaled glucocorticosteroids
Beclomethasone 50–400 (MDI &DPI) 0.2–0.4
Budesonide 100,200,400 (DPI) 0.20,0.25,0.5
Fluticasone 50–500 (MDI &DPI)
Triamcinolone 100 (MDI) 40 40
Combination long-acting β2-agonists plus glucocorticosteroids in one inhaler
Formoterol/budesonide
4.5/160,9/320 (DPI)
Salmeterol/fluticasone
50/100,250,500(DPI)25/50, 125,250(MDI)
(continued)
Management of Chronic Obstructive Pulmonary Disease 11

daily. Olodaterol and vilanterol are newer LABAs prescribed for use once daily(Mirza et al. 2018).
Side effects of beta2-adrenergic agonist can include exaggerated somatic tremorsin older patients and at higher dose levels. In addition, some susceptible patients mayencounter resting sinus tachycardia that can precipitate cardiac rhythm disturbancesregardless of the route of administration.
Antimuscarinic DrugsAntimuscarinic drugs, which antagonize M3 muscarinic receptors which areexpressed in airway smooth muscle, inhibit acetylcholine-induced bronchocon-striction (Melani 2015). In addition, older treatments such as ipratropium andoxitropium, which are short-acting antimuscarinics (SAMAs), also disrupt the inhib-itory neuronal receptor M2 pathway. This action has the potential to stimulatevagally induced bronchoconstriction (Barnes 1995). On the other hand, tiotropium,aclidinium, glycopyrronium bromide, and umeclidinium are all long-acting anti-muscarinic antagonists (LAMAs) that have prolonged effects on M3 muscarinicreceptors, while M2 muscarinic receptor binding shows faster dissociation. Clinicaldata indicates that LAMA treatment with tiotropium can improve health status andsymptoms (Karner et al. 2014). LAMA also reduces exacerbations and improvespulmonary rehabilitation effectiveness and related hospitalization (Kesten et al.2008). The main side effect is dry mouth (Kesten et al. 2006) in addition tooccasional urinary symptoms. Ipratropium can cause a bitter, metallic taste insome patients.
MethylxanthinesThe most commonly used methylxanthine is theophylline, whose bronchodilatoryeffect is mediated by nonselective phosphodiesterase inhibition. The drug also has arange of non-bronchodilator actions (McKay et al. 1993). For example, patientstreated with methylxanthines can have enhanced inspiratory muscle function(McKay et al. 1993). It is important to note that a sustained release formulation oftheophylline has efficacy in all COPD studies.
Cytochrome P450-mixed function oxidases metabolize theophylline. The clear-ance of this drug is reduced with age and is increased in smokers. Comparison of
Table 2 (continued)
Drug Inhaler (μg)
Solutionfornebulizer(mg/ml) Oral
Vials forinjection(mg)
Durationof action(hours)
Systemic glucocorticosteroids
Prednisone 5–60 mg(pill)
Methylprednisolone 4,8,16 mg(pill)
Adapted from GOLD (2017)
12 M. Khdour et al.

salmeterol alone with the combination of theophylline and salmeterol shows that thecombination produces a greater improvement in FEV1 and breathlessness (Zacariaset al. 2007).
The occurrence of atrial and ventricular arrhythmias, which can be fatal, are sideeffects associated with theophylline. Patients often complain of palpitations andexperience grand mal convulsions, which appear regardless of a previous historyof epilepsy. Additional side effects, such as insomnia, headache, heartburn, andnausea, can also occur.
Combination Bronchodilator TherapySeveral combinations of bronchodilators are possible. For example, the combina-tions of SABA and SAMAs improve FEV1 better than either medication alone(Gross et al. 1998). Another possibility is the combination of LABA and LAMA.When formoterol and tiotropium are used in combination in separate inhalers, thereis a greater effect on FEV1 than when either constituent is used alone (Tashkin et al.2009).
The number of possible combinations with single inhaler use is increasing.Several of the combinations were evaluated in placebo-controlled studies. Thecombinations improve lung function relative to placebo. In addition, the efficacyof the combination is unfailingly better than the effects of a long-acting bronchodi-lator monotherapy. The degree of the enhancement is not entirely additive relative tothe response of each single component (Cazzola and Molimard 2010). Anotherapproach is to use the combination of a LABA/LAMA twice daily regimen atlower doses. The approach enhances the health status and symptoms for patientswith COPD.
Anti-inflammatory Agents
Inhaled Corticosteroids (ICS)Cumulative evidence indicates that when used alone, ICS does not decrease mortal-ity or the long-term regression of FEV1 for patients with COPD (Yang et al. 2012).The TORCH trial reported that using fluticasone propionate alone appeared to showhigher mortality rates compared to placebo or fluticasone propionate plus salmeterolcombination (Calverley et al. 2007). When ICS and LABA are combined for use inmoderate to severe COPD patients with exacerbations, it is more effective inimproving health status, lung function, and reducing exacerbations than eithercomponent alone (Nannini et al. 2013).
In general, ICS are well tolerated, and the possibility of major side effects isminimal. Long-term use of ICS has the potential to increase risk of cataract,pneumonia, mycobacterial infection, diabetes, and osteoporosis (Decramer et al.2013; Vogelmeier et al. 2011; Singh 2015). The risk of side effects appears to beincreased in patients with low body mass index, older patients, patients with historyof pneumonia, and patients with low FEV1 (Festic and Scanlon 2015). It is unclear ifICS benefits patients with COPD.
Management of Chronic Obstructive Pulmonary Disease 13

Triple TherapyThe combination of ICS, LABA, and LAMA is referred to as triple therapy. Thiscombination can be either in a single inhaler or in separate inhalers. Triple therapyreduces exacerbations and symptoms and improves lung function relative to ICS-LABA treatment and LAMA monotherapy (Welte et al. 2009; Singh et al. 2016).Comparison of LAMA-LABA treatment with triple therapy is not well studied andclinical data is sparse.
Oral GlucocorticoidsSystemic glucocorticoids are used in hospitalized patients or in emergency roomsettings for acute exacerbations. They reduce breathlessness and the rates of treat-ment failure and relapse and improve overall lung function (Walters et al. 2014). Oralcorticosteroids are used in the acute management of exacerbation and not in thechronic treatment of COPD due to the many side effects of steroids.
Phosphodiesterase-4 (PDE4) InhibitorsRoflumilast is a PDE4 inhibitor that inhibits intracellular cyclic AMP breakdownand reduces inflammation (Rabe 2011). The product has no direct bronchodilatoreffects (Calverley et al. 2009). Roflumilast administrated once daily (oral dosing)reduces severe exacerbations.
AntibioticsRecent evidence indicates clinical value in the prophylactic use of antibiotics (Ni etal. 2015). Treatment with azithromycin 250 or 500 three times weekly (for 1 year)reduces exacerbations risk relative to usual care (Albert et al. 2011). Such prophy-lactic use of antibiotics increases the risk of bacterial resistance (Francis et al. 1961),and the patient populations that may best respond to such prophylactic antibiotictreatment have not been sufficiently described (Han et al. 2014).
Non-pharmacological Management of COPD
Pulmonary RehabilitationPulmonary rehabilitation involves a thorough patient assessment and is undertakento provide a comprehensive patient-tailored intervention that includes education,behavior change, and exercise training, all of which are intended to enhance thepsychological and physical state of patients suffering from chronic respiratorydisease. Pulmonary rehabilitation attempts to stimulate health-enhancing long-termbehaviors (Spruit et al. 2013).
Pulmonary rehabilitation is part of a comprehensive patient management plan(Vogiatzis et al. 2016). The GOLD 2017 statement recommends pulmonary rehabil-itation for patients at risk of exacerbation or high symptoms burden. Other recom-mendations are that all symptomatic patients with COPD benefit from rehabilitation.The rehabilitation program is usually customized for each patient and takes intoconsideration patient comorbidities. The supervised program usually includes
14 M. Khdour et al.

smoking cessation, exercise training, self-management skills, and nutrition therapy.Full benefit from the program can be expected within 6–8 weeks (McCarthy et al.2015).
Self-Management EducationEducation is an important component of the non-pharmacological management ofCOPD. A COPD self-management intervention is a regulated but a personalizedprocess that frequently involves multiple components. The goals are to motivate,engage, and support patients in order to positively acclimate their health behavior(s)and to aid them in developing skills so that they can better manage their disease(Effing et al. 2016). The topics of the education programs cover smoking cessation,detailed knowledge about COPD, broad and specific approaches to the treatment andother parts of COPD, strategies to minimize symptoms, primarily dyspnea, andinitial management of exacerbations (Khdour et al. 2009, 2011).
Smoking CessationBased on the harmful effects of smoking on lung function and COPD diseaseprogression, it is not surprising that smoking cessation is high on the non-pharma-cological intervention list for management of COPD. An effective and dedicatedsmoking cessation program increases the chance of long-term cessation success rateto 25%. Smoking cessation improves lung function within a year of quittingsmoking (Pelkonen et al. 2000). Physicians should encourage patients to stop ratherthan reduce cigarette smoke intake (Scanlon et al. 2000).
The possible options for facilitating smoking cessation include nicotine replace-ment therapy (e.g., nicotine gum and transdermal patch), which enhances long-termsmoking abstinence frequencies (van der Meer et al. 2003). Nicotine replacementtherapy is contraindicated in patients with recent strokes or myocardial infarctions(Okuyemi et al. 2006).
The recent introduction of e-cigarettes as a type of nicotine replacement therapymay not be entirely accurate. Data on the use of e-cigarette for smoking cessation isstill controversial (McRobbie et al. 2014). There is insufficient data on the healtheffects of e-cigarettes, especially after long-term use.
Pharmacologic products such as bupropion (Tashkin et al. 2001), varenicline(Tashkin et al. 2011), and nortriptyline increase long-term cigarette quit rates (Cahillet al. 2013). Use of these pharmacologic agents should be part of a more compre-hensive supportive intervention program and not as the sole means in smokingcessation.
VaccinationDeath in COPD patients can be reduced by the administration of the influenzavaccine, which decreases the number patients who experience severe lower respira-tory tract infections that require hospitalization. Vaccination is recommended for allpatients over the age of 65. In addition, vaccination is also suggested for youngerpatients with COPD and other comorbidities such as heart disease (Wongsurakiat etal. 2004).
Management of Chronic Obstructive Pulmonary Disease 15

Nutritional SupportNutritional supplements are recommended for malnourished COPD patients. Nutri-tional supplementation positively effects fat mass, body weight, and fat-free mass. Inaddition, nutritional supplementation significantly improves health status when usedduring exercise training (Ferreira et al. 2012)
Oxygen TherapyLong-term oxygen therapy (>15 h per day) increases patient survival for thoseexperiencing severe resting hypoxemia and chronic respiratory failure. Continuedoxygen therapy requires reevaluation within 2–3 months in which arterial blood gasor SaO2 tests are conducted (Cranston et al. 2005).
Ventilatory SupportNoninvasive ventilation (NIV), used in the form of noninvasive positive pressureventilation (NPPV), is sometimes applied during COPD exacerbations. Such treat-ment is becoming part of the standard treatment for decreasing mortality andmorbidity in hospitalized COPD patients with exacerbation and acute respiratoryfailure (Lindenauer et al. 2014)
Surgical InterventionLung volume reduction surgery (LVRS) may be required in some patients withCOPD. Such a procedure involves reduction of hyperinflation parts of the lungs byresectioning (Martinez et al. 1997). This improves mechanical efficiency of respira-tory muscles, making them more effective pressure generators. Bullectomy relievesthe compressive effects of bullae in carefully selected COPD patients with largebulla with compressive effects or risk of spontaneous rupture (Marchetti and Criner2015).
Conclusion
The GOLD guidelines propose individual and comprehensive assessment strategiesfor accurate diagnosis of COPD that is based on a patient’s symptoms, risk ofexacerbation, and extent of airflow limitation. Early identification of COPD throughroutine screening for symptoms will lead to earlier diagnosis and treatment. Smokingcessation remains the cornerstone strategy and has a large impact on disease pro-gression. The pharmacological management of COPD relies on the availability ofLAMA, LABA, ICS, combination modalities, and affordable inhalers with goodefficacy, with the hope that future developments in pharmacological management ofCOPD will better aligned with the recently updated GOLD guidelines. Health-caresystems in Arab world should renew efforts to provide adequate professionaltraining and facilities for non-pharmacological interventions for the managementof COPD and develop centers for endoscopic lung volume reduction and lungtransplants in selected COPD patients.
16 M. Khdour et al.

References
Adeloye D, Chua S, Lee CW et al (2015) Global and regional estimates of COPD prevalence:systemic review and meta-analysis. J Glob Health 5:020415
Al Ghobain M, Alhamad EH, Alorainy HS, Al Kassimi F, Lababidi H, Al-Hajjaj MS (2015) Theprevalence of chronic obstructive pulmonary disease in Riyadh, Saudi Arabia: a BOLD study.Int J Tuberc Lung Dis 9:1252–1257
Albert RK, Connett J, Bailey WC et al (2011) Azithromycin for prevention of exacerbations ofCOPD. N Engl J Med 365(8):689–698
Al-Fayez SF, Salleh M, Ardawi M, AZahran FM (1988) Effects of sheesha and cigarette smokingon pulmonary function of Saudi males and females. Trop Geogr Med 40(2):115–123
American Thoracic Society (1995) COPD: definitions, epidemiology, pathophysiology, diagnosisand staging. Am J Respir Crit Care Med 152(5, Pt 1):1713–1735
Banasik J (2001) Diagnosing alpha 1-antitrypsin deficiency. Nurse Pract 26(1):58–62Barnes P (1995) Bronchodilators: basic pharmacology. In: Calverley PMA, Pride NB (eds) Chronic
obstructive pulmonary disease. Chapman and Hall, London, pp 391–417Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA (1999) Usefulness of the
Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients withchronic obstructive pulmonary disease. Thorax 54:581–586
Blanco I, de Serres FJ, Fernandez-Bustillo E, Lara B, Miravitlles M (2006) Estimated numbers andprevalence of PI�S and PI�Z alleles of alpha1-antitrypsin deficiency in European countries. EurRespir J 27(1):77–84
Burge PS, Calverley PM, Jones PW, Spencer S, Anderson JA, Maslen TK (2000) Randomised,double blind, placebo controlled study of fluticasone propionate in patients with moderate tosevere chronic obstructive pulmonary disease: the ISOLDE trial. BMJ 320(7245):1297–1303
Cahill K, Stevens S, Perera R, Lancaster T (2013) Pharmacological interventions for smokingcessation: an overview and network meta-analysis. Cochrane Database Syst Rev (5):CD009329
Calverley PM, Anderson JA, Celli B et al (2007) Salmeterol and fluticasone propionate and survivalin chronic obstructive pulmonary disease. N Engl J Med 356(8):775–789
Calverley PM, Rabe KF, Goehring UM et al (2009) Roflumilast in symptomatic chronic obstructivepulmonary disease: two randomised clinical trials. Lancet 374(9691):685–694
Carson AR, Hieber KV (2001) Adult pediatric patients. Am J Nurse 101(3):46–55Cazzola M, Molimard M (2010) The scientific rationale for combining long-acting beta2-agonists
and muscarinic antagonists in COPD. Pulm Pharmacol Ther 23(4):257–267Centers for Disease Control and Prevention (2002) Surveillance summaries. MMWR 2002:51(No.
SS-6)Cerveri I, Accordini S, Verlato G, Corsico A, Zoia MC et al (2001) Variations in the prevalence
across countries of chronic bronchitis and smoking habits in young adults. Eur Respir J18(1):85–92
Cranston JM, Crockett AJ, Moss JR, Alpers JH (2005) Domiciliary oxygen for chronic obstructivepulmonary disease. Cochrane Database Syst Rev (4):CD001744
Datta D, Vitale A, Lahiri B, ZuWallack R (2003) An evaluation of nebulized levalbuterol in stableCOPD. Chest 124(3):844–849
Decramer ML, Chapman KR, Dahl R et al (2013) Once-daily indacaterol versus tiotropium forpatients with severe chronic obstructive pulmonary disease (INVIGORATE): a randomised,blinded, parallel-group study. Lancet Respir Med 1:524–533
Effing TW, Vercoulen JH, Bourbeau J et al (2016) Definition of a COPD self-managementintervention: International Expert Group consensus. Eur Respir J 48(1):46–54
Ferreira IM, Brooks D, White J, Goldstein R (2012) Nutritional supplementation for stable COPD.Cochrane Database Syst Rev (12):CD000998
Festic E, Scanlon PD (2015) Incident pneumonia and mortality in patients with chronic obstructivepulmonary disease: a double effect of inhaled corticosteroids? Am J Respir Crit Care Med191:141–148
Management of Chronic Obstructive Pulmonary Disease 17

Francis RS, May JR, Spicer CC (1961) Chemotherapy of bronchitis. Influence of penicillin andtetracycline administered daily, or intermittently for exacerbations. A report to the ResearchCommittee of the British Tuberculosis Association by its Bronchitis Subcommittee. Br Med J2(5258):979–985
Global Initiative for Chronic Obstructive Lung Disease (2017) Global strategy for the diagnosis,management, and prevention of chronic obstructive lung disease. Available from: http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd. Accessed 10Sept 2017
Gross NJ, Petty TL, Friedman M, Skorodin MS, Silvers GW, Donohue JF (1989) Dose response toipratropium as a nebulized solution in patients with chronic obstructive pulmonary disease. Athree-center study. Am Rev Respir Dis 139(5):1188–1191
Gross N, Tashkin D, Miller R, Oren J, Coleman W, Linberg S (1998) Inhalation by nebulization ofalbuterol- ipratropium combination (Dey combination) is superior to either agent alone in thetreatment of chronic obstructive pulmonary disease. Dey Combination Solution Study Group.Respiration 65(5):354–362
Han MK, Tayob N, Murray S et al (2014) Predictors of chronic obstructive pulmonary diseaseexacerbation reduction in response to daily azithromycin therapy. Am J Respir Crit Care Med189:1503–1508
Hnizdo E, Sullivan PA, Bang KM, Wagner G (2002) Association between chronic obstructivepulmonary disease and employment by industry and occupation in the US population: a study ofdata from the Third National Health and Nutrition Examination Survey. Am J Epidemiol 156(8):738–746
Hu G, Zhou Y, Tian J et al (2010) Risk of COPD from exposure to biomass smoke: a meta-analysis.Chest 138:20–31
Jindal SK, Aggarwal AN, Chaudhry K, Chhabra SK, D’Souza GA, Gupta D et al (2006) Amulticentric study on epidemiology of chronic obstructive pulmonary disease and its relation-ship with tobacco smoking and environmental tobacco smoke exposure. Indian J Chest DisAllied Sci 48(1):23–29
Johannessen A, Lehmann S, Omenaas ER, Eide GE, Bakke PS, Gulsvik A (2006) Post-broncho-dilator spirometry reference values in adults and implications for disease management. Am JRespir Crit Care Med 173(12):1316–1325
Jones P, Tabberer M, Chen WH (2011) Creating scenarios of the impact of COPD and theirrelationship to COPD assessment test (CATTM) scores. BMC Pul Med 11:42
Jones PW, Adamek L, Nadeau G, Banik N (2013) Comparisons of health status scores with MRCgrades in COPD: implications for the GOLD 2011 classification. Eur Respir J 42:647–654
Karner C, Chong J, Poole P (2014) Tiotropium versus placebo for chronic obstructive pulmonarydisease. Cochrane Database Syst Rev (7):CD009285
Kesten S, Jara M, Wentworth C, Lanes S (2006) Pooled clinical trial analysis of tiotropium safety.Chest 130(6):1695–1703
Kesten S, Casaburi R, Kukafka D, Cooper CB (2008) Improvement in self-reported exerciseparticipation with the combination of tiotropium and rehabilitative exercise training in COPDpatients. Int J Chron Obstruct Pulmon Dis 3(1):127–136
Kew KM, Mavergames C, Walters JA (2013) Long-acting beta2-agonists for chronic obstructivepulmonary disease. Cochrane Database Syst Rev (10):CD010177
Khattab A, Javaid A, Iraqi G et al (2012) Smoking habits in the Middle East and North Africa:results of the BREATHE study. Respir Med 106(Suppl 2):S16–S24
Khdour MR, Kidney JC, Smyth BM, McElnay JC (2009) Clinical pharmacy-led disease andmedicine management programme for patients with COPD. Br J Clin Pharmacol 68(4):588–598
Khdour MR, Agus AM, Kidney JC, Smyth BM, Elnay JC, Crealey GE (2011) Cost-utility analysisof a pharmacy-led self-management programme for patients with COPD. Int J Clin Pharm33(4):665–673
18 M. Khdour et al.

Konzem SL, Stratton MA (2002) Chronic obstructive lung disease. In: DiPiro JT, Talbert RL, YeeGC et al (eds) Pharmacotherapy: a pathophysiologic approach, 5th edn. McGraw-Hill, NewYork, pp 511–529
Lee SH, Goswami S, Grudo A et al (2007) Anti-elastin autoimmunity in tobacco smoking-inducedemphysema. Nat Med 13(5):567–569
Lindenauer PK, Stefan MS, Shieh MS, Pekow PS, Rothberg MB, Hill NS (2014) Outcomesassociated with invasive and noninvasive ventilation among patients hospitalized with exacer-bations of chronic obstructive pulmonary disease. JAMA Intern Med 174(12):1982–1993
Lopez AD, Shibuya K, Rao C, Mathers CD, Hansell AL, Held LS et al (2006) Chronic obstructivepulmonary disease: current burden and future projections. Eur Respir J 27(2):397–412
Marchetti N, Criner GJ (2015) Surgical approaches to treating emphysema: lung volume reductionsurgery, bullectomy, and lung transplantation. Semin Respir Crit Care Med 36(4):592–608
Martinez FJ, de Oca MM, Whyte RI, Stetz J, Gay SE, Celli BR (1997) Lung-volume reductionimproves dyspnea, dynamic hyperinflation, and respiratory muscle function. Am J Respir CritCare Med 155(6):1984–1990
Matheson MC, Benke G, Raven J, SimMR, Kromhout H, Vermeulen R et al (2005) Biological dustexposure in the workplace is a risk factor for chronic obstructive pulmonary disease. Thorax60(8):645–651
McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y (2015) Pulmonary rehabili-tation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev (2):CD003793
McKay SE, Howie CA, Thomson AH, Whiting B, Addis GJ (1993) Value of theophylline treatmentin patients handicapped by chronic obstructive lung disease. Thorax 48(3):227–223
McRobbie H, Bullen C, Hartmann-Boyce J, Hajek P (2014) Electronic cigarettes for smokingcessation and reduction. Cochrane Database Syst Rev (12):CD010216
Melani AS (2015) Long-acting muscarinic antagonists. Expert Rev Clin Pharmacol 8(4):479–501Mirza S, Clay RD, Koslow MA, Scanlon PD (2018) COPD guidelines: a review of the 2018 GOLD
report. Mayo Clin Proc 93(10):1488–1502Murphy KR (2004) Asthma: helping patients breathe easier. Nurs Pract 29(10):38–55Nannini LJ, Poole P, Milan SJ, Kesterton A (2013) Combined corticosteroid and long-acting beta
(2)-agonist in one inhaler versus inhaled corticosteroids alone for chronic obstructive pulmonarydisease. Cochrane Database Syst Rev (8):CD006826
Ni W, Shao X, Cai X et al (2015) Prophylactic use of macrolide antibiotics for the prevention ofchronic obstructive pulmonary disease exacerbation: a meta-analysis. PLoS One 10(3):e0121257
Nishimura K, Izumi T, Tsukino M, Oga T (2002) Dyspnea is a better predictor of 5-year survivalthan airway obstruction in patients with COPD. Chest 121:1434–1440
Okuyemi KS, Nollen NL, Ahluwalia JS (2006) Interventions to facilitate smoking cessation. AmFam Physician 74(2):262–271
Pelkonen M, Tukiainen H, Tervahauta M et al (2000) Pulmonary function, smoking cessation and30-year mortality in middle aged Finnish men. Thorax 55:746–750
Rabe KF (2011) Update on roflumilast, a phosphodiesterase 4 inhibitor for the treatment of chronicobstructive pulmonary disease. Br J Pharmacol 163(1):53–67
Scanlon PD, Connett JE, Waller LA et al (2000) Smoking cessation and lung function in mild-to-moderate chronic obstructive pulmonary disease: the Lung Health Study. Am J Respir Crit CareMed 161:381–390
Singh D (2015) New combination bronchodilators for chronic obstructive pulmonary disease:current evidence and future perspectives. Br J Clin Pharmacol 79:695–708
Singh D, Papi A, Corradi M et al (2016) Single inhaler triple therapy versus inhaled corticosteroidplus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): adouble-blind, parallel group, randomised controlled trial. Lancet 388:963–973
Soriano JR, Maier WC, Egger P, Visick G, Thakrar B, Sykes J et al (2000) Recent trends inphysician diagnosed COPD in women and men in the UK. Thorax 55:789–794
Management of Chronic Obstructive Pulmonary Disease 19

Spruit MA, Singh SJ, Garvey C et al (2013) An official American Thoracic Society/EuropeanRespiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am JRespir Crit Care Med 188(8):e13–e64
Stoller JK, Aboussouan LS (2005) Alpha1-antitrypsin deficiency. Lancet 365(9478):2225–2236Sze MA, Dimitriu PA, Suzuki M et al (2015) Host response to the lung microbiome in chronic
obstructive pulmonary disease. Am J Respir Crit Care Med 192(4):438–445Tageldin MA, Nafti S, Khan JA, Nejjari C, Beji M, Mahboub B, Obeidat NM, Uzaslan E, Sayiner
A, Wali S, Rashid N (2012) Distribution of COPD-related symptoms in the Middle East andNorth Africa: results of the BREATHE study. Respir Med 106:S25–S32
Tashkin D, Kanner R, Bailey Wet al (2001) Smoking cessation in patients with chronic obstructivepulmonary disease: a double-blind, placebo-controlled, randomised trial. Lancet357(9268):1571–1575
Tashkin DP, Pearle J, Iezzoni D, Varghese ST (2009) Formoterol and tiotropium compared withtiotropium alone for treatment of COPD. COPD 6(1):17–25
Tashkin DP, Rennard S, Hays JT, Ma W, Lawrence D, Lee TC (2011) Effects of varenicline onsmoking cessation in patients with mild to moderate COPD: a randomized controlled trial. Chest139(3):591–599
Trupin L, Earnest G, San Pedro M, Balmes JR, Eisner MD, Yelin E et al (2003) The occupationalburden of chronic obstructive pulmonary disease. Eur Respir J 22(3):462–469
Turato G, Zuin R, Saetta M (2001) Pathogenesis and pathology of COPD. Respiration68(2):117–128
Uzaslan E, Mahboub B, Beji M, Nejjari C, Tageldin MA, Khan JA, Nafti S, Obeidat NM, SayinerA, Wali S, Rashid N (2012) The burden of chronic obstructive pulmonary disease in the MiddleEast and North Africa: results of the BREATHE study. Respir Med 106:S45–S59
van der Meer RM, Wagena EJ, Ostelo RW, Jacobs JE, van Schayck CP (2003) Smoking cessationfor chronic obstructive pulmonary disease. Cochrane Database Syst Rev (2):CD002999
Vathenen AS, Britton JR, Ebden P, Cookson JB, Wharrad HJ, Tattersfield AE (1988) High-doseinhaled albuterol in severe chronic airflow limitation. Am Rev Respir Dis 138(4):850–855
Vestbo J, Sorensen T, Lange P, Brix A, Torre P, Viskum K (1999) Long-term effect of inhaledbudesonide in mild and moderate chronic obstructive pulmonary disease: a randomized con-trolled trial. Lancet 353(9167):1819–1823
Vogelmeier C, Hederer B, Glaab T et al (2011) Tiotropium versus salmeterol for the prevention ofexacerbations of COPD. N Engl J Med 364:1093–1103
Vogiatzis I, Rochester CL, Spruit MA, Troosters T, Clini EM (2016) American Thoracic Society/European Respiratory Society Task Force on Policy in pulmonary rehabilitation. Increasingimplementation and delivery of pulmonary rehabilitation: key messages from the new ATS/ERSpolicy statement. Eur Respir J 47(5):1336–1341
Walters JA, Tan DJ, White CJ, Gibson PG, Wood-Baker R, Walters EH (2014) Systemic cortico-steroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane DatabaseSyst Rev (9):CD001288
Warwick H, Doig A (2004) Smoke the killer in the kitchen: indoor air pollution in developingcountries. ITDG Publishing, London. http://www.itdgpublishing.org.uk
Welte T, Miravitlles M, Hernandez P et al (2009) Efficacy and tolerability of budesonide/formoteroladded to tiotropium in patients with chronic obstructive pulmonary disease. Am J Respir CritCare Med 180(8):741–750
WHO (2004) http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. Accessed 10 Sept 2017
WHO (2016) http://www.who.int/healthinfo/paper36.pdf. Accessed 12 Oct 2017Wongsurakiat P, Maranetra KN, Wasi C, Kositanont U, Dejsomritrutai W, Charoenratanakul S
(2004) Acute respiratory illness in patients with COPD and the effectiveness of influenzavaccination: a randomized controlled study. Chest 125(6):2011–2020
20 M. Khdour et al.

World Health Organization (2016) Chronic obstructive pulmonary disease (COPD). Available from:www.who.int/mediacentre/factsheets/fs315/en. Accessed Dec 2017
Yang IA, Clarke MS, Sim EH, Fong KM (2012) Inhaled corticosteroids for stable chronicobstructive pulmonary disease. Cochrane Database Syst Rev (7):CD002991
Zacarias EC, Castro AA, Cendon S (2007) Effect of theophylline associated with short-acting orlong-acting inhaled beta2-agonists in patients with stable chronic obstructive pulmonary dis-ease: a systematic review. J Bras Pneumol 33(2):152–160
Management of Chronic Obstructive Pulmonary Disease 21