Embed Size (px)
Citation preview
Malnutrition in all its forms: a double burden & a double duty for food policyProf Corinna Hawkes, Director, Centre for Food PolicyCo-Chair, Global Nutrition Report
2.1 By2030endhungerandensureaccessbyallpeople,in
particularthepoorandpeopleinvulnerablesituationsincludinginfants,tosafe,nutritiousandsufficientfoodallyearround.
2.2 By2030endallformsofmalnutrition,includingachieving
by2025theinternationallyagreedtargetsonstuntingand
wastinginchildren.
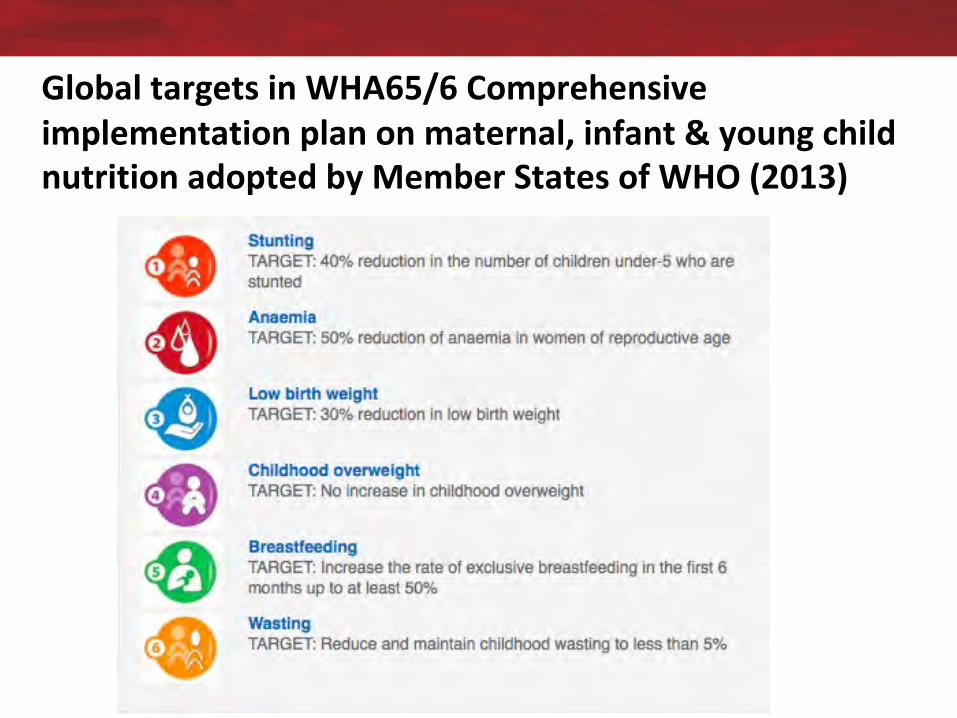
GlobaltargetsinWHA65/6Comprehensiveimplementationplanonmaternal,infant&youngchildnutritionadoptedbyMemberStatesofWHO(2013)

3.4By2030,reducebyonethirdprematuremortalityfromnon-communicable
diseasesthroughpreventionandtreatmentandpromotementalhealthandwell-being
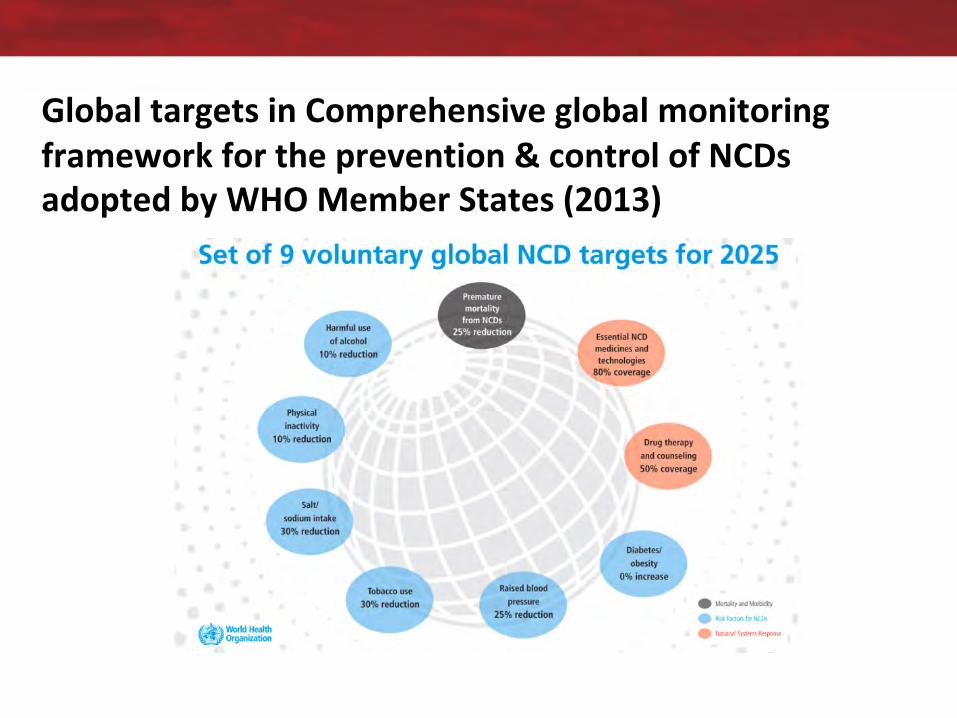
GlobaltargetsinComprehensiveglobalmonitoringframeworkfortheprevention&controlofNCDsadoptedbyWHOMemberStates(2013)

Source:NCDAlliance
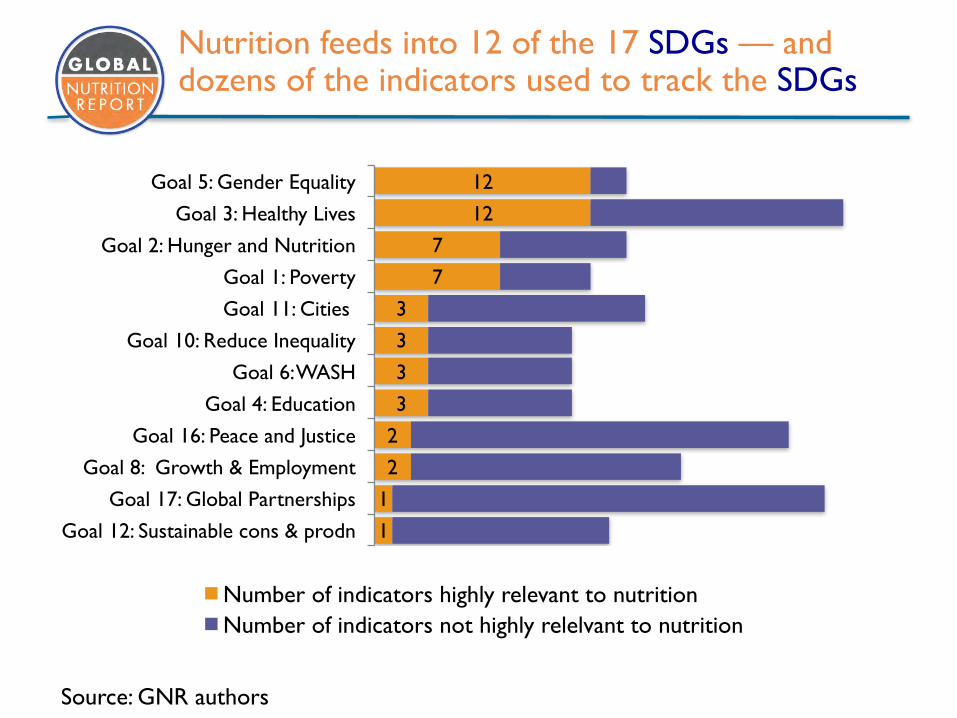
Nutrition feeds into 12 of the 17 SDGs — and dozens of the indicators used to track the SDGs
1
1
2
2
3
3
3
3
7
7
12
12
Goal 12: Sustainable cons & prodn
Goal 17: Global Partnerships
Goal 8: Growth & Employment
Goal 16: Peace and Justice
Goal 4: Education
Goal 6: WASH
Goal 10: Reduce Inequality
Goal 11: Cities
Goal 1: Poverty
Goal 2: Hunger and Nutrition
Goal 3: Healthy Lives
Goal 5: Gender Equality
Number of indicators highly relevant to nutritionNumber of indicators not highly relelvant to nutrition
Source: GNR authors

www.globalnutritionreport.org
www.globalnutritionreport.org#NutritionReport

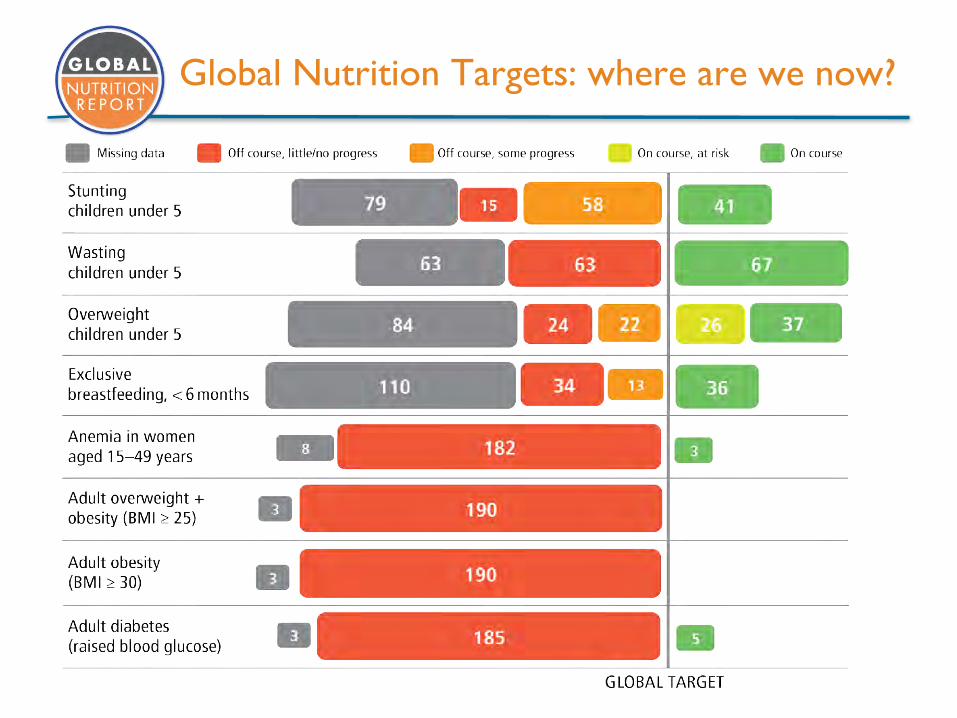
Global Nutrition Targets: where are we now?
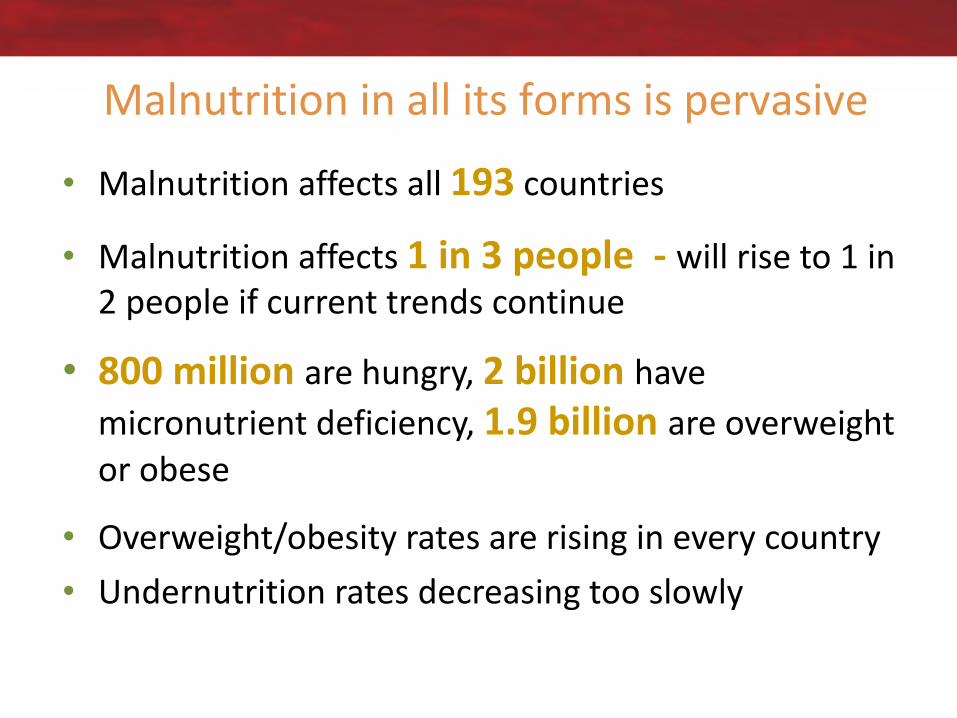
Malnutritioninallitsformsispervasive
• Malnutritionaffectsall193 countries
• Malnutritionaffects1in3people- willriseto1in2peopleifcurrenttrendscontinue
• 800millionarehungry,2billionhavemicronutrientdeficiency,1.9billionareoverweightorobese
• Overweight/obesityratesarerisingineverycountry• Undernutritionratesdecreasingtooslowly
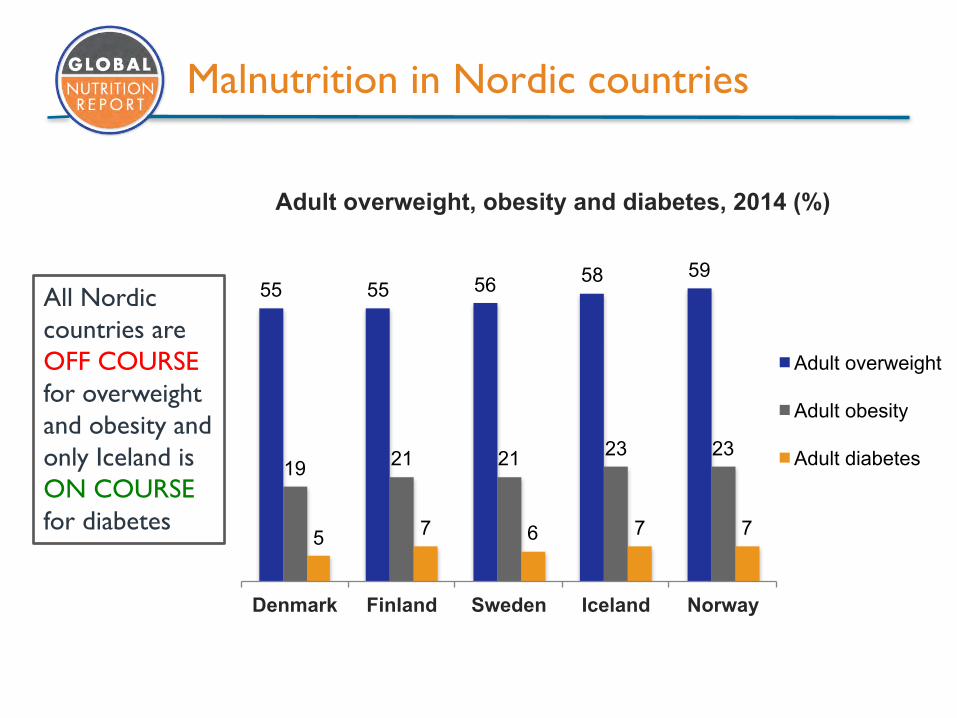
Malnutrition in Nordic countries
55 55 56 58 59
19 21 21 23 23
5 7 6 7 7
Denmark Finland Sweden Iceland Norway
Adult overweight, obesity and diabetes, 2014 (%)
Adult overweight
Adult obesity
Adult diabetes
All Nordic countries are OFF COURSE for overweight and obesity and only Iceland is ON COURSE for diabetes
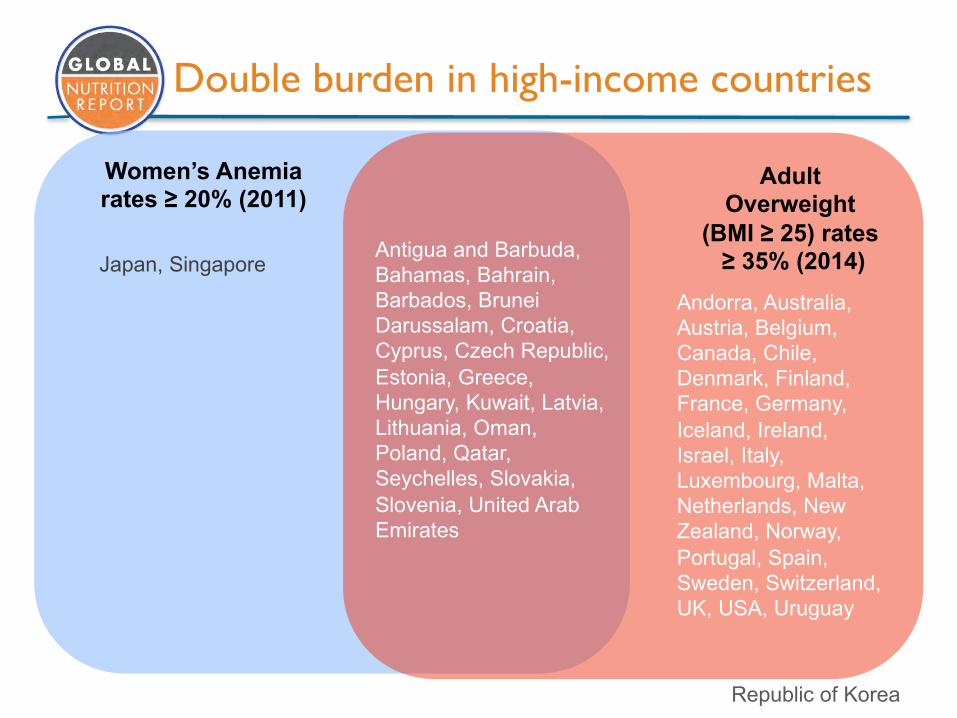
Women’s Anemia rates ≥ 20% (2011)
Adult Overweight
(BMI ≥ 25) rates≥ 35% (2014)Antigua and Barbuda,
Bahamas, Bahrain, Barbados, Brunei Darussalam, Croatia, Cyprus, Czech Republic, Estonia, Greece, Hungary, Kuwait, Latvia, Lithuania, Oman, Poland, Qatar, Seychelles, Slovakia, Slovenia, United Arab Emirates
Double burden in high-income countries
Andorra, Australia, Austria, Belgium, Canada, Chile, Denmark, Finland, France, Germany, Iceland, Ireland, Israel, Italy, Luxembourg, Malta, Netherlands, New Zealand, Norway, Portugal, Spain, Sweden, Switzerland, UK, USA, Uruguay
Japan, Singapore
Republic of Korea
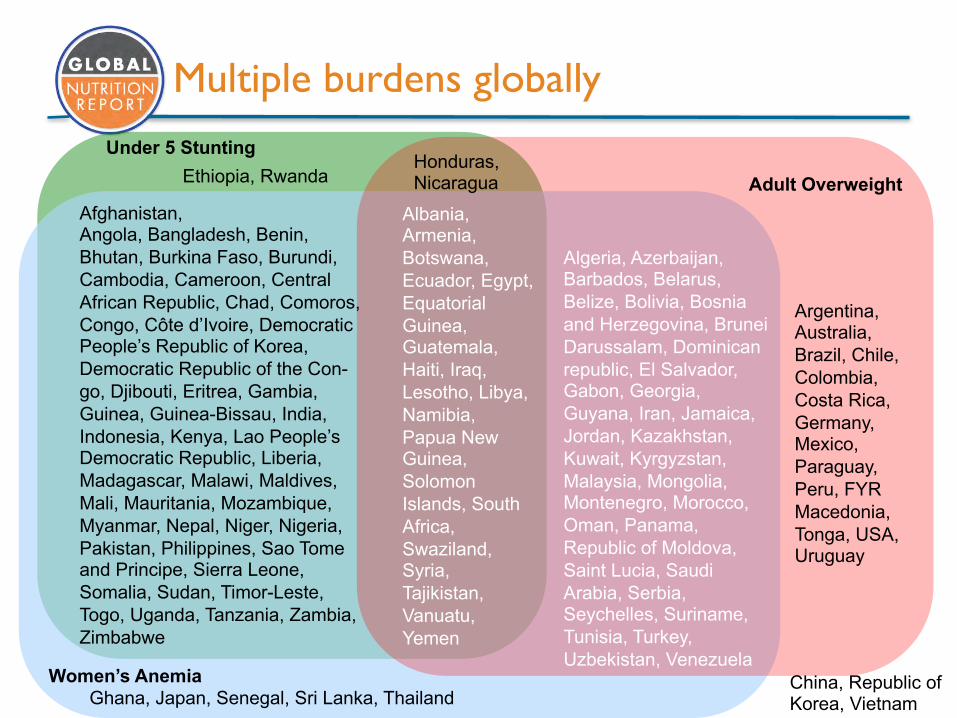
Under 5 Stunting
Women’s Anemia
Adult OverweightEthiopia, Rwanda
Ghana, Japan, Senegal, Sri Lanka, Thailand
Argentina, Australia, Brazil, Chile, Colombia, Costa Rica, Germany, Mexico, Paraguay, Peru, FYR Macedonia, Tonga, USA, Uruguay
Afghanistan, Angola, Bangladesh, Benin, Bhutan, Burkina Faso, Burundi, Cambodia, Cameroon, Central African Republic, Chad, Comoros, Congo, Côte d’Ivoire, Democratic People’s Republic of Korea, Democratic Republic of the Con-go, Djibouti, Eritrea, Gambia, Guinea, Guinea-Bissau, India, Indonesia, Kenya, Lao People’s Democratic Republic, Liberia, Madagascar, Malawi, Maldives, Mali, Mauritania, Mozambique, Myanmar, Nepal, Niger, Nigeria, Pakistan, Philippines, Sao Tome and Principe, Sierra Leone, Somalia, Sudan, Timor-Leste, Togo, Uganda, Tanzania, Zambia, Zimbabwe
Honduras, Nicaragua
Algeria, Azerbaijan, Barbados, Belarus, Belize, Bolivia, Bosnia and Herzegovina, Brunei Darussalam, Dominican republic, El Salvador, Gabon, Georgia, Guyana, Iran, Jamaica, Jordan, Kazakhstan, Kuwait, Kyrgyzstan, Malaysia, Mongolia, Montenegro, Morocco, Oman, Panama, Republic of Moldova, Saint Lucia, Saudi Arabia, Serbia, Seychelles, Suriname, Tunisia, Turkey, Uzbekistan, Venezuela
Albania, Armenia, Botswana, Ecuador, Egypt, Equatorial Guinea, Guatemala, Haiti, Iraq, Lesotho, Libya, Namibia, Papua New Guinea, Solomon Islands, South Africa, Swaziland, Syria, Tajikistan, Vanuatu, Yemen
China, Republic of Korea, Vietnam
Multiple burdens globally
Double burden: the new normal
2.Foodanddietasadriverofthedoubleburden
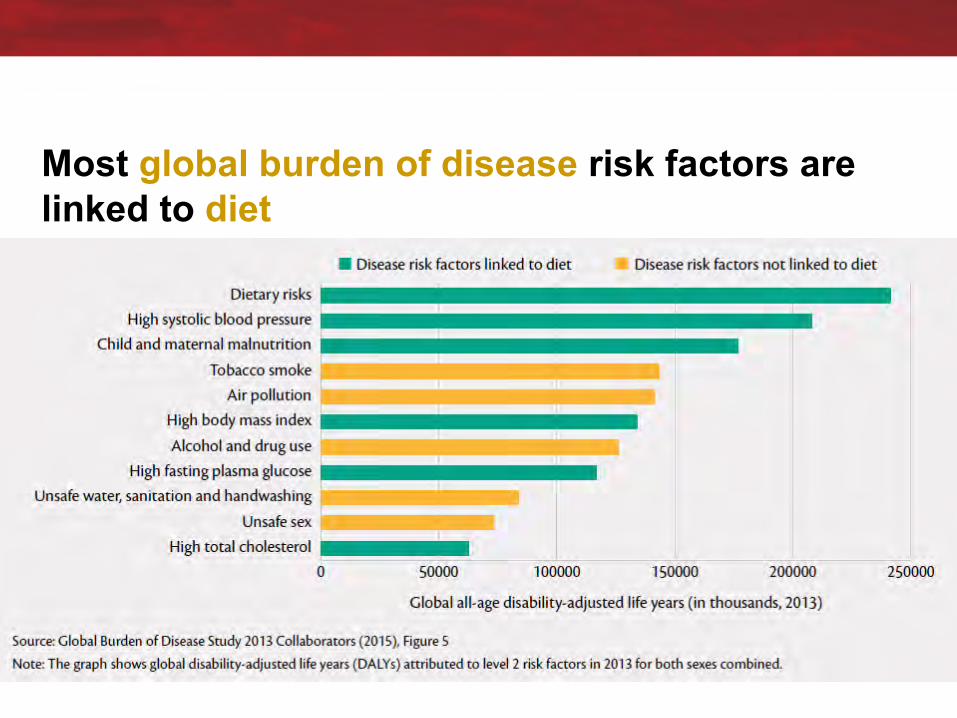
Most global burden of disease risk factors are linked to diet
Akeyfactorincommonbetweenpeopleatriskofundernutrition &obesity:poordietquality
Risingconsumptionofsugars,fats,ultra-processedfoodsinmostplacesandamongmostpeople,includinginfants
15% Anaverageofonly15%ofunder-2’sconsumeaminimallyacceptablediet.
50% Morethanhalfofallwomeninterviewedin6sub-Saharancountriesdonotconsumelegumes,nuts,vitaminA-richfruitsandvegetables,dairyoreggsinanygivenday
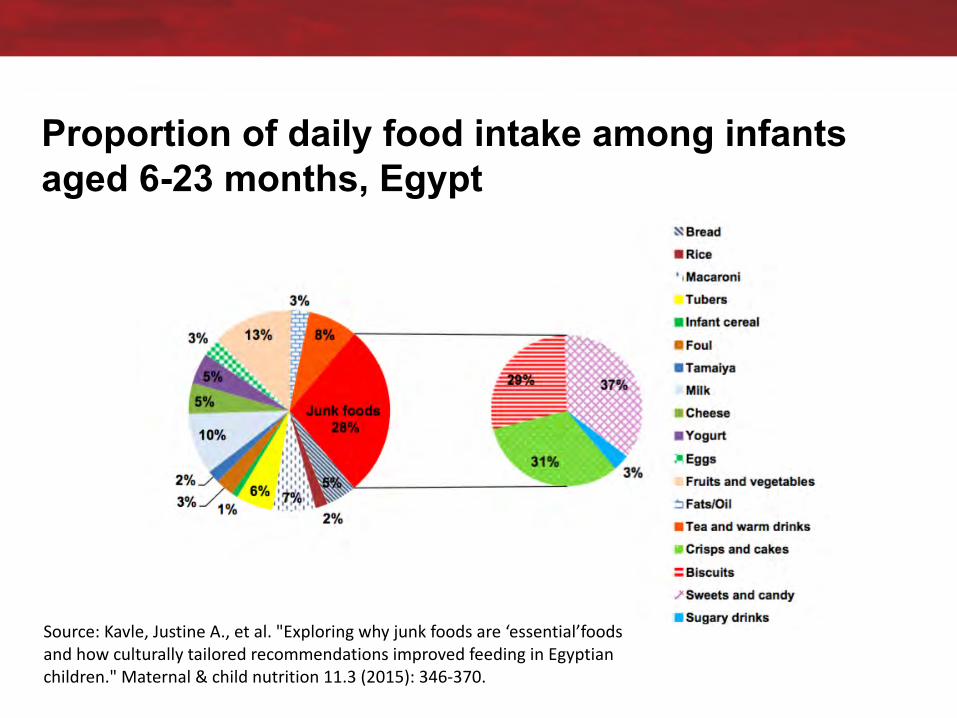
Proportion of daily food intake among infants aged 6-23 months, Egypt
Source:Kavle,JustineA.,etal."Exploringwhyjunkfoodsare‘essential’foodsandhowculturallytailoredrecommendationsimprovedfeedinginEgyptianchildren."Maternal&childnutrition11.3(2015):346-370.
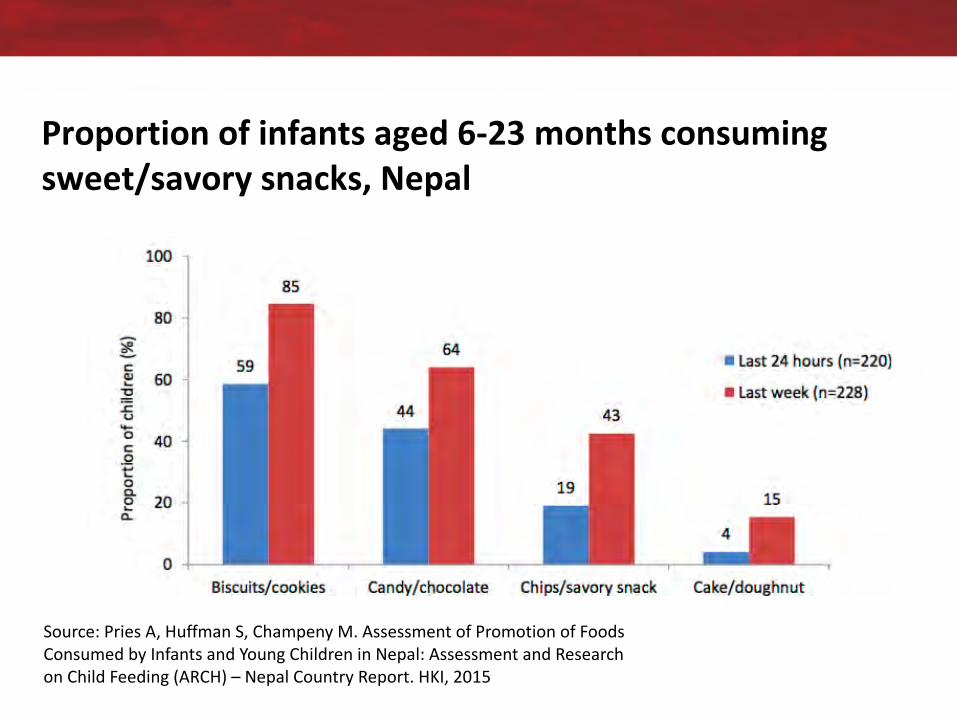
Proportionofinfantsaged6-23monthsconsumingsweet/savorysnacks,Nepal
Source:PriesA,HuffmanS,Champeny M.AssessmentofPromotionofFoodsConsumedbyInfantsandYoungChildreninNepal:AssessmentandResearchonChildFeeding(ARCH)– NepalCountryReport.HKI,2015

3.Whatapproacheshavebeentakentotodatetoaddressobesityandundernutrition?
1.Obesity
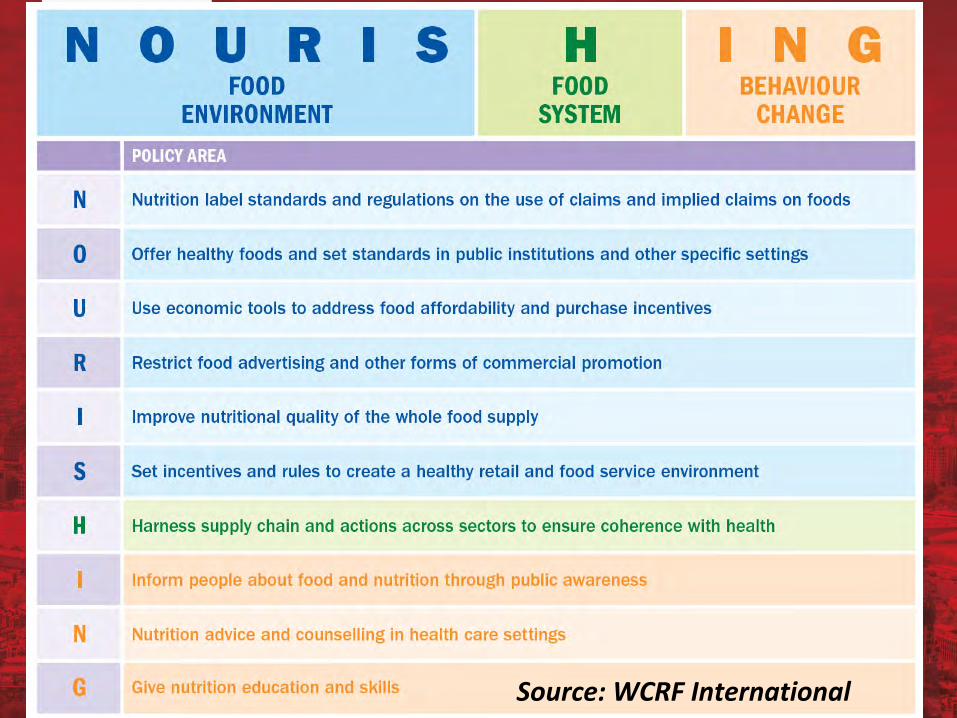
CROSS-SECTOR INITIATIVES OF THE UN AGENCIES
Source:WCRFInternational
2. Undernutrition
§ Folicacidsupplementationorfortification§Universalsaltiodization§Balancedenergy-proteinsupplementation§Calciumsupplementation§Multiplemicronutrientsupplementation§Promotionofbreastfeeding(counselling)§Promotionofcomplementaryfeeding(education)§ Feedingforchildrenwithmoderateacutemalnutrition§Therapeuticfeedingforseverelywastedchildren§VitaminAsupplementation§Zinctreatmentfordiarrhea§Preventivezincsupplementation
Directnutritioninterventions
Evidenceinpracticealsoshowscrucialroleofaddressingthe“causesofthecauses”
“In short, the causes of the impressive decline in childmalnutrition in Brazil appear to lie in the improvements incoverage of essential public services and increases infamily income, both particularly favoring the poor”(Monteiro, 2009)
2016 GNR success stories show key elements ofsuccess are: political commitment; economicgrowth/poverty reduction, education; female education;water, sanitation and health; health systems; socialprotection, supplementation as success factors in thereduction of undernutrition (food and diets not mentioned)
1960s/70s:assumptioninagriculturecommunitythatfoodavailabilitywastheanswerto“hunger”
“Itwasassumedthattheoverallincreaseintheaggregatefood
supplyandhigherincomethroughagriculture(thedominant
occupationofthepoor)werethemainroutestobetternutrition”
(WorldBank,2014)
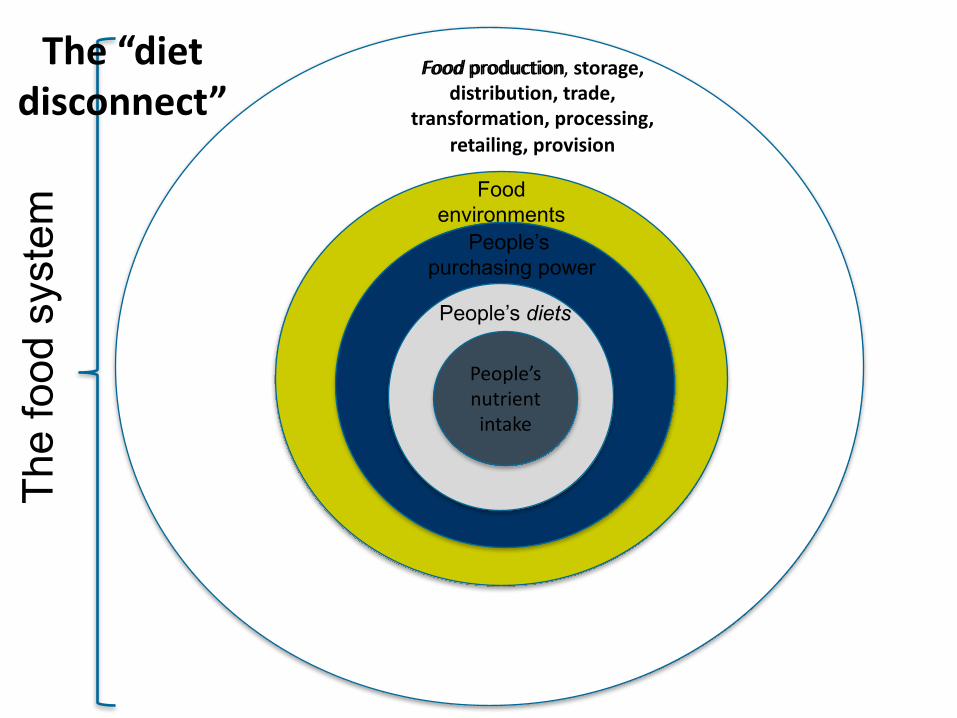
Food environments
Food production
People’s purchasing power
People’snutrientintake
People’s diets
Food production,storage,distribution,trade,
transformation,processing,retailing,provision
The
food
sys
tem
The“dietdisconnect”
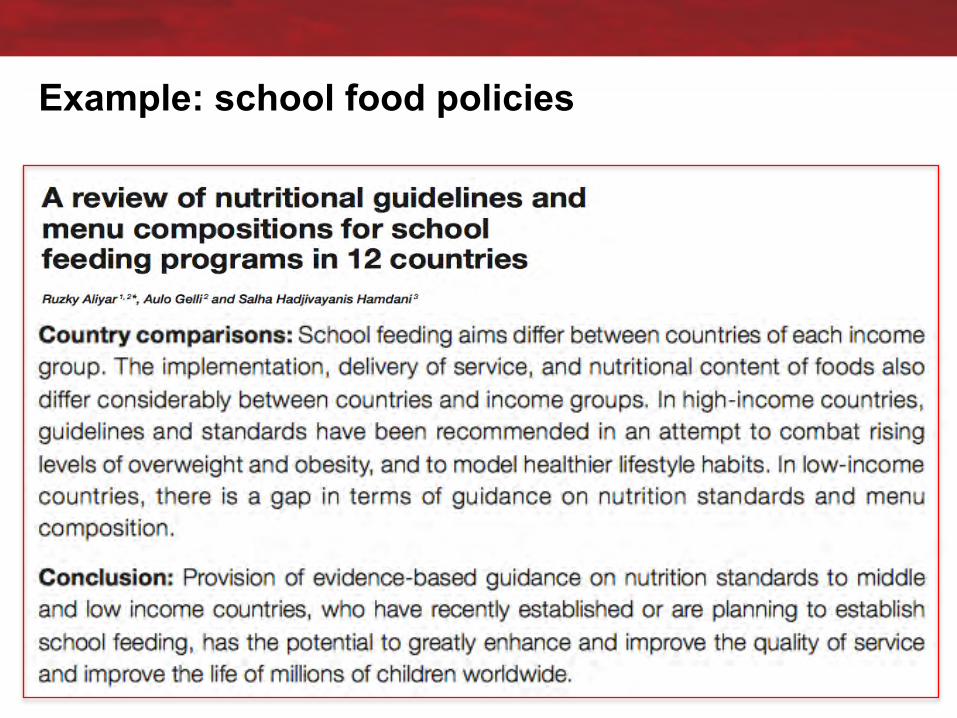
Example: school food policies

Healthyschoolmeals?
SchoolfoodprogrammeinSyria(Source:WorldFoodProgramme)

4.Whatcanfood policydo?
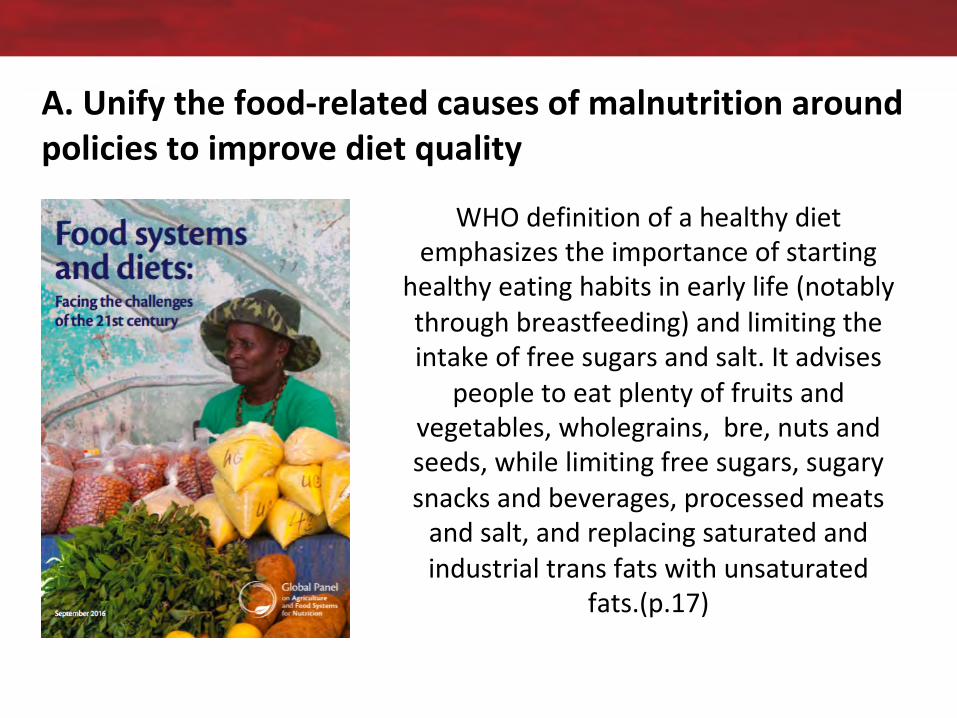
A.Unifythefood-relatedcausesofmalnutritionaroundpoliciestoimprovedietquality
WHOdefinitionofahealthydietemphasizestheimportanceofstarting
healthyeatinghabitsinearlylife(notablythroughbreastfeeding)andlimitingtheintakeoffreesugarsandsalt.Itadvises
peopletoeatplentyoffruitsandvegetables,wholegrains,bre,nutsandseeds,whilelimitingfreesugars,sugarysnacksandbeverages,processedmeatsandsalt,andreplacingsaturatedandindustrialtransfatswithunsaturated
fats.(p.17)
“Researchers who work on all forms of malnutrition should come together with the international agencies to identify
‘double-duty actions’ that can address undernutrition as well as overweight, obesity and nutrition-related non-communicable
diseases simultaneously.”
B.Shiftpolicymakersmindsetsto“doingdoubledutyforthedoubleburden”
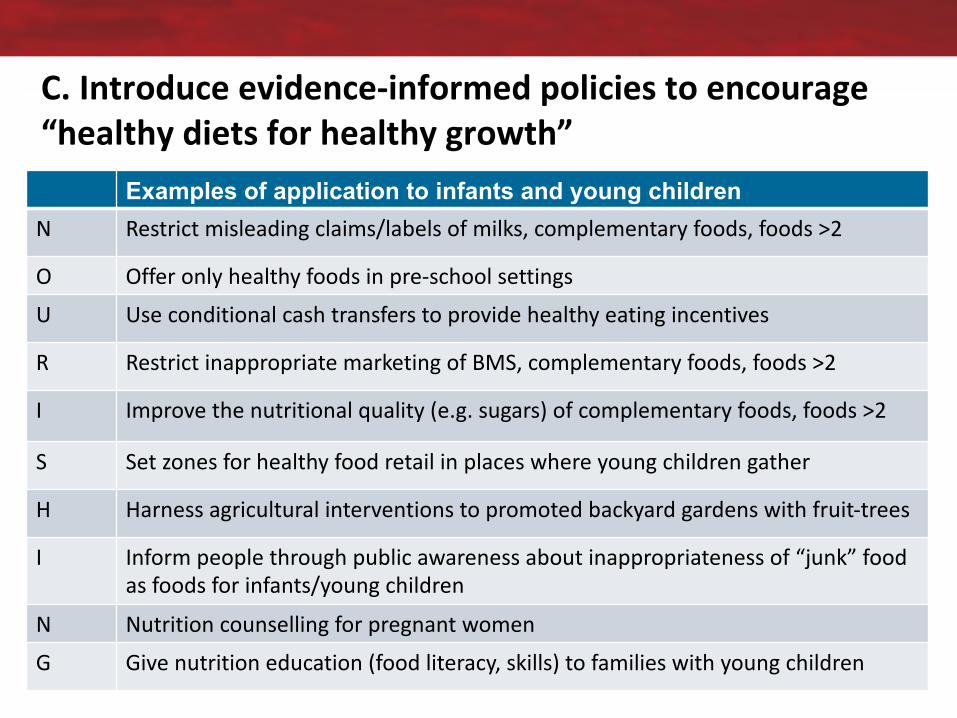
Examples of application to infants and young childrenN Restrict misleadingclaims/labelsofmilks,complementaryfoods,foods>2
O Offeronlyhealthyfoodsinpre-schoolsettingsU Useconditional cashtransferstoprovidehealthyeatingincentives
R Restrictinappropriate marketingofBMS,complementaryfoods,foods>2
I Improvethenutritionalquality(e.g. sugars)ofcomplementaryfoods,foods>2
S Setzones forhealthyfoodretailinplaceswhereyoungchildrengather
H Harnessagriculturalinterventionstopromotedbackyardgardenswithfruit-trees
I Informpeoplethroughpublicawarenessaboutinappropriatenessof“junk”foodasfoodsforinfants/youngchildren
N NutritioncounsellingforpregnantwomenG Give nutritioneducation(foodliteracy,skills)tofamilieswithyoungchildren
C.Introduceevidence-informedpoliciestoencourage“healthydietsforhealthygrowth”
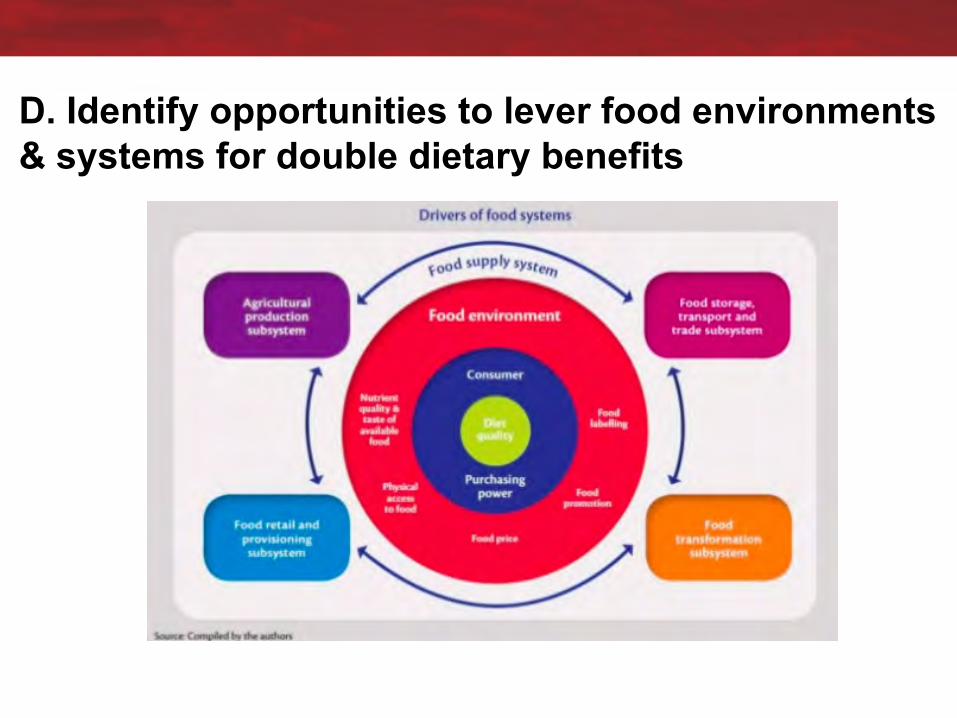
D. Identify opportunities to lever food environments & systems for double dietary benefits

City, University of LondonNorthampton SquareLondonEC1V 0HBUnited Kingdom
T: +44 (0)20 7040 5060E: [email protected]/department
Corinna HawkesProfessor of Food Policy
Director, Centre for Food PolicyCo-Chair, Global Nutrition Report
[email protected]@corinnahawkes@FoodPolicyCity
@GNReport







![SWAZILAND GOVERNMENT GAZETTE EXTRAORDINARY - Swaziland Competition … Commission Regulations... · SWAZILAND GOVERNMENT GAZETTE EXTRAORDINARY VOL. XLVIII] ... \ THE COMPETITION ACT,](https://img.pdfslide.us/doc/110x75/5ad0acb57f8b9a8b1e8e2be8/swaziland-government-gazette-extraordinary-swaziland-competition-commission.jpg)