Embed Size (px)
Citation preview

Alcoholic Liver Cirrhosis Alcoholic Liver Cirrhosis
and and
Hepatic EncephalopathyHepatic Encephalopathy
Major Clinical Case StudyMajor Clinical Case StudyFebruary 8, 2011February 8, 2011
Angela BoaduAngela Boadu
University of Maryland, College Park University of Maryland, College Park
Dietetic Intern Dietetic Intern
20102010--2011 2011

Discussion PointsDiscussion Points
�� Executive SummaryExecutive Summary
�� General InformationGeneral Information
�� Social HistorySocial History
�� Medical/Surgical DataMedical/Surgical Data�� Past Medical HistoryPast Medical History
�� Past Surgical HistoryPast Surgical History
�� Admitting Physical Exam Admitting Physical Exam
�� Diagnostic Tests Diagnostic Tests
�� Surgical Procedures Since Surgical Procedures Since AdmissionAdmission
�� Laboratory ValuesLaboratory Values
�� Nutritional History from Nutritional History from Initial EncounterInitial Encounter�� Diet HistoryDiet History
�� Weight HistoryWeight History
�� Physical Activity Level Physical Activity Level
�� Estimated Nutrient Needs Estimated Nutrient Needs
�� Nutrition Care ProcessNutrition Care Process
�� Hospital Course Hospital Course �� Medical and Nutritional Medical and Nutritional
Treatment Treatment
�� Medical ConsiderationsMedical Considerations
�� Medical Nutrition Therapy Medical Nutrition Therapy
�� ReferencesReferences

Executive SummaryExecutive Summary
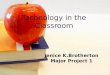
�� The liver is a 3The liver is a 3--pound organ, consisting of a right pound organ, consisting of a right
lobe and left lobe, which the body depends on to lobe and left lobe, which the body depends on to
provide metabolic and nutritional control. provide metabolic and nutritional control.
�� Alcoholic liver disease is a disease resulting from Alcoholic liver disease is a disease resulting from
excessive alcohol ingestion. The pathogenesis of excessive alcohol ingestion. The pathogenesis of
alcoholic liver disease progresses in three stages with alcoholic liver disease progresses in three stages with
the final stage being cirrhosis. the final stage being cirrhosis.
�� Treatment of cirrhosis focuses on stopping the Treatment of cirrhosis focuses on stopping the
development of the scar tissue if possible and development of the scar tissue if possible and
treating any complications. treating any complications.

Figure 1: A normal liver (left) showing no signs of scarring and a cirrhotic liver
(right).
(Source: Mayo Foundation for Medical Education and Research)

General InformationGeneral Information
�� 4747--yearyear--old Caucasian female with an extensive old Caucasian female with an extensive history of alcohol abusehistory of alcohol abuse
�� Admitted with abdominal pain, slurred speech, Admitted with abdominal pain, slurred speech, drowsiness, and yellowdrowsiness, and yellow--tinted whites of her eyes. tinted whites of her eyes.
�� Admission height: 5Admission height: 5’’ 77”” (170 cm) (170 cm)
�� Admission weight, following paracentesis of 6 liters Admission weight, following paracentesis of 6 liters of fluid: 142# (64.4kg); of fluid: 142# (64.4kg); BMI=22.2; IBW 135#BMI=22.2; IBW 135#
�� DxDx: H: Hepatic Encephalopathy with Significant Ascites, epatic Encephalopathy with Significant Ascites, and Alcoholic Liver Cirrhosis and Alcoholic Liver Cirrhosis
�� Date of admission: Date of admission: Wednesday, November 3, 2010 Wednesday, November 3, 2010
�� Date of discharge: Date of discharge: Thursday, November 13, 2010 Thursday, November 13, 2010

Social HistorySocial History
�� VM is a single mother of two sons, both VM is a single mother of two sons, both serving in the Navy. serving in the Navy.
�� She lives alone in a townhouse, with frequent She lives alone in a townhouse, with frequent
visitations from her supportive significant visitations from her supportive significant other. other.
�� Tobacco use is less than a half a pack a day. Tobacco use is less than a half a pack a day.
�� A distant history of spousal abuse was A distant history of spousal abuse was
thought to be the cause of her heavy drinking. thought to be the cause of her heavy drinking.
�� Current amounts were not clearly described Current amounts were not clearly described

Medical/Surgical Medical/Surgical
DataData

Past Medical HistoryPast Medical History
�� Thyroid cancer (no recurrence)Thyroid cancer (no recurrence)
�� HypothyroidismHypothyroidism
�� Liver diseaseLiver disease
�� CirrhosisCirrhosis
�� RosaceaRosacea
�� GERDGERD
�� Anxiety Disorder Anxiety Disorder
�� Prior Prior h/oh/o type 2 diabetes and hypertension no longer type 2 diabetes and hypertension no longer require medication, but are require medication, but are ““diet controlleddiet controlled””

Past Surgical HistoryPast Surgical History
�� Cervical excision and total Cervical excision and total thyroidectorythyroidectory
�� Tonsillectomy Tonsillectomy
�� AdenoidectomyAdenoidectomy
�� Breast reduction surgery as a young adult Breast reduction surgery as a young adult

Admitting Physical ExamAdmitting Physical Exam
�� SmallSmall--framed framed
�� Vital signs were stable. Vital signs were stable.
�� Facial rosaceaFacial rosacea
�� Abdomen was rounded and symmetric, positive Abdomen was rounded and symmetric, positive bowel sounds x4bowel sounds x4
�� The patient did note pain inside her ribs and under The patient did note pain inside her ribs and under her left breast, which is chronic but much improved her left breast, which is chronic but much improved after the paracentesis performed the morning of after the paracentesis performed the morning of admission. admission.
�� HemoccultHemoccult positive stool in the emergency positive stool in the emergency department department

Diagnostic Tests Diagnostic Tests
�� Abdominal xAbdominal x--ray suggestive of a small bowel ray suggestive of a small bowel
obstruction (11/4/10)obstruction (11/4/10)
�� Pelvic ultrasound demonstrating a large Pelvic ultrasound demonstrating a large
amount of ascites (11/4/10)amount of ascites (11/4/10)
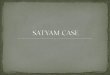
�� Computed tomography (CT) scan of the Computed tomography (CT) scan of the
patientpatient’’s abdomen and pelvis demonstrating s abdomen and pelvis demonstrating
massive abdominal and pelvic ascites massive abdominal and pelvic ascites
(11/6/10 )(11/6/10 )

Figure 3: CT (left) and Ultrasound (right) of Abdomen with Figure 3: CT (left) and Ultrasound (right) of Abdomen with loculatedloculated ascites ascites
(Source: Loyola University Health System (Source: Loyola University Health System StritchStritch School of MedicineSchool of Medicine))
Bowel loops float Bowel loops float anteriorlyanteriorly..

Surgical Procedures Since AdmissionSurgical Procedures Since Admission
�� UltrasoundUltrasound--guided paracentesis performed guided paracentesis performed
�� 11/3/10 (PTA) 11/3/10 (PTA) –– 6 Liters 6 Liters
�� 11/8/10 11/8/10 –– therapeutic therapeutic
�� 11/12/10 11/12/10 –– 4.5 Liters4.5 Liters

Laboratory Values Laboratory Values
�� ↓↓sodium = hyponatremiasodium = hyponatremia
�� ↓↓chloride = possible chloride = possible hypochloremiahypochloremia acidosisacidosis
�� ↓↓protein and albumin = protein and albumin = hypoalbuminemiahypoalbuminemia -- decreased decreased production of albumin contributing to ascitesproduction of albumin contributing to ascites
�� ↓↓amylase andamylase and↑↑ lipase = possible pancreatic damagelipase = possible pancreatic damage
�� ↑↑ammonia = contributing to hepatic encephalopathy ammonia = contributing to hepatic encephalopathy
�� ↑↑ glucose = glucose intoleranceglucose = glucose intolerance
�� ↑↑WBC = infectionWBC = infection
�� ↓↓hematologichematologic values, specifically RBC, values, specifically RBC, HgbHgb, , HctHct, MCV, MCH= , MCV, MCH= macrocytic anemia due to chronic disease and hypovolemia macrocytic anemia due to chronic disease and hypovolemia (most likely due to fluid losses or decreased fluid intake)(most likely due to fluid losses or decreased fluid intake)
�� ↑↑LFTS, specifically AST and LFTS, specifically AST and BilirubinBilirubin (= jaundice) = liver (= jaundice) = liver disease disease

Nutritional HistoryNutritional History
from from
Initial Encounter Initial Encounter

Diet History Diet History
�� Balanced diet with minimal salty foods and sweets. Balanced diet with minimal salty foods and sweets. �� Canned and preCanned and pre--packaged foods were purchased for packaged foods were purchased for
convenience with patient not aware of high sodium convenience with patient not aware of high sodium content of some food items. content of some food items.
�� Prior to acute onset of symptoms, patientPrior to acute onset of symptoms, patient’’s appetite and s appetite and intake had been good. intake had been good.
�� ‘‘ReportedReported’’ physician directives in hospitalphysician directives in hospital
�� Allergies? NAllergies? N
�� Intake of vitamins, minerals, oral supplements, Intake of vitamins, minerals, oral supplements, and/or health food store alternative supplements? Nand/or health food store alternative supplements? N
�� Cultural attitudes that influence dietary intake? NCultural attitudes that influence dietary intake? N
�� Past/present dietary/nutritional therapy? NPast/present dietary/nutritional therapy? N

Weight History and Weight History and
Physical Activity LevelPhysical Activity Level
�� VM reported recent weight gain (secondary to fluid VM reported recent weight gain (secondary to fluid
retention) with loss of visible body muscle. retention) with loss of visible body muscle.
�� Limited physical activity, requiring a walker to get Limited physical activity, requiring a walker to get
around the housearound the house
�� New evening hours job limiting significant otherNew evening hours job limiting significant other’’s s
ability to provide physical and emotional support for ability to provide physical and emotional support for
VM VM
�� Mobility issues relate to reaching a bathroom on a Mobility issues relate to reaching a bathroom on a
different floor in the housedifferent floor in the house

Nutrition Care Process Nutrition Care Process
�� Initial Nutrition Initial Nutrition DiagnosisDiagnosis�� NBNB--1.11.1 FoodFood-- and nutritionand nutrition--knowledge deficit knowledge deficit related torelated to need for NAS diet (3need for NAS diet (3--
4 gm Na/low salt) of 1800 calories and nutritional supplement 4 gm Na/low salt) of 1800 calories and nutritional supplement as evidenced byas evidenced byhistory of liver disease and current diagnosis of alcoholic livehistory of liver disease and current diagnosis of alcoholic liver cirrhosis. r cirrhosis.
�� Initial Nutrition Initial Nutrition Intervention Intervention
�� EE--1.31.3 Education survival skills. Brief nutrition education to build Education survival skills. Brief nutrition education to build and reinforce and reinforce basic nutritionbasic nutrition--related knowledge and provide essential nutrition information related knowledge and provide essential nutrition information specific to management of liver cirrhosis. specific to management of liver cirrhosis.
�� Nutrition Nutrition Monitoring Monitoring �� FHFH--1.1.1.11.1.1.1 Total energy intakeTotal energy intake. Assessment of food recall given by patient . Assessment of food recall given by patient
verifying adequacy of intake in the promotion of healthy weight verifying adequacy of intake in the promotion of healthy weight gain gain
�� Laboratory values. Laboratory values. BDBD--1.2.51.2.5 Sodium. Sodium. Criteria: 135Criteria: 135--145 145 mmolmmol/L /L BD 1.11.1BD 1.11.1PrealbuminPrealbumin. . Criteria: 18Criteria: 18-- 45 mg/dl (to evaluate visceral protein stores and 45 mg/dl (to evaluate visceral protein stores and adequacy of intake) adequacy of intake)
�� May also want to monitor control of symptoms, such the reoccurreMay also want to monitor control of symptoms, such the reoccurrence of nce of ascitesascites

Hospital course Hospital course �� Day 1Day 1
�� Paracentesis Paracentesis
�� Hyponatremia and hyperkalemia Hyponatremia and hyperkalemia
�� Ammonia levelsAmmonia levels
�� Diet: 1800 calorie No Added Salt (NAS) diet (3Diet: 1800 calorie No Added Salt (NAS) diet (3--4 gm Na/low salt), and given the oral 4 gm Na/low salt), and given the oral nutritional supplement Ensure Plus B.I.D. Limited intake reportnutritional supplement Ensure Plus B.I.D. Limited intake reported.ed.
�� IV fluids: IV normal saline at 75 cc/hrIV fluids: IV normal saline at 75 cc/hr
�� Day 2Day 2�� Folic acid, thiamine, multivitaminsFolic acid, thiamine, multivitamins
�� IV normal saline was stopped due to concern on its impact on heaIV normal saline was stopped due to concern on its impact on heart rate. rt rate.
�� LactuloseLactulose was held was held
�� Day 3Day 3�� Possible spontaneous bacterial peritonitis Possible spontaneous bacterial peritonitis
�� Elevated finger sticksElevated finger sticks
�� Possible acute renal failure/acute kidney injury Possible acute renal failure/acute kidney injury
�� Possible short bowel obstruction, either an ileus or mechanical Possible short bowel obstruction, either an ileus or mechanical obstruction obstruction
�� Diet: NPODiet: NPO
�� Day 5Day 5�� Diet: NPO except meds and ice chips with eventual transition to Diet: NPO except meds and ice chips with eventual transition to a clear liquid diet for a clear liquid diet for
evening mealevening meal

Hospital Course ContinuedHospital Course Continued�� Day 6Day 6
�� Ascites reAscites re--accumulation, but minimal urinary output required some IV hydrataccumulation, but minimal urinary output required some IV hydration ion
�� Therapeutic paracentesis and IV albumin infusion Therapeutic paracentesis and IV albumin infusion
�� GI status improved, and NG tube was removed GI status improved, and NG tube was removed
�� Diet: NPO for procedure this morning, with orders for a soft diDiet: NPO for procedure this morning, with orders for a soft diet thereafter. et thereafter.
�� Day 7Day 7�� LactuloseLactulose was decreased, but pt still inconsistent in answers to questionwas decreased, but pt still inconsistent in answers to questions. s.
�� Diet: NPODiet: NPO
�� Day 8Day 8�� Diet: Soft, NAS diet w/ percent intake of meals intake reported Diet: Soft, NAS diet w/ percent intake of meals intake reported at 5%at 5%
�� Day 9Day 9�� Hepatic encephalopathy was resolved on Hepatic encephalopathy was resolved on RifaximinRifaximin and and LactuloseLactulose. .
�� Diet: Soft, NAS diet. PatientDiet: Soft, NAS diet. Patient’’s appetite fair w/ percent intake of meals noted at 25% s appetite fair w/ percent intake of meals noted at 25%
�� Day 10Day 10�� Paracentesis Paracentesis
�� Clostridium Clostridium difficiledifficile colitis colitis
�� Liver transplant list Liver transplant list
�� Diet: Sodium restriction continued on Soft, NAS diet w/ percentDiet: Sodium restriction continued on Soft, NAS diet w/ percent intake of meals noted intake of meals noted at 75%at 75%
�� Day 11Day 11�� Patient discharged home Patient discharged home
�� Diet: Soft, NAS diet with percent intake of meals 100%Diet: Soft, NAS diet with percent intake of meals 100%

Estimated Nutrient NeedsEstimated Nutrient Needs
�� BEE x 1.2BEE x 1.2--1.3 (hospitalized patient) 1.3 (hospitalized patient)
= = 16301630--1765 kcal/day1765 kcal/day
�� 0.8 0.8 –– 1.0 1.0 g/kg/dg/kg/d (hospitalized patient, non(hospitalized patient, non--stress) stress)
= = 5151--64 g protein/day64 g protein/day
�� 20 20 –– 25 ml/kg/d (hospitalized patient with 25 ml/kg/d (hospitalized patient with
ascites and sodium level below 128 ascites and sodium level below 128 mEqmEq/L) /L)
= = 12881288--1610 mL fluid/day1610 mL fluid/day

Medical Considerations Medical Considerations
�� Moderate to severe Moderate to severe malnutritionmalnutrition is a common finding in patients with liver is a common finding in patients with liver cirrhosis, and has a severe negative impact on a patientcirrhosis, and has a severe negative impact on a patient’’s prognosis. s prognosis.
�� Glucose intoleranceGlucose intolerance occurs in almost occurs in almost ⅔⅔ of patients with cirrhosis, and 10% to 37% of patients with cirrhosis, and 10% to 37% of patients will develop overt diabetes. of patients will develop overt diabetes.
�� HepatorenalHepatorenal syndromesyndrome is a renal failure associated with severe liver disease is a renal failure associated with severe liver disease without intrinsic kidney abnormalities without intrinsic kidney abnormalities
�� HyponatremiaHyponatremia often occurs because of decreased ability to excrete water often occurs because of decreased ability to excrete water resulting from the persistent release of antidiuretic hormone, sresulting from the persistent release of antidiuretic hormone, sodium losses via odium losses via paracentesis, or overly sodium restriction. paracentesis, or overly sodium restriction.
�� Portal hypertension, Portal hypertension, hypoalbuminemiahypoalbuminemia, and renal retention of sodium and fluid , and renal retention of sodium and fluid contribute to contribute to fluid retentionfluid retention�� LargeLarge--volume paracentesis volume paracentesis
�� Diuretic therapy: Diuretic therapy: SpironolactoneSpironolactone and and FurosemideFurosemide
�� AmmoniaAmmonia is a direct cerebral toxin. The main source of ammonia is its eis a direct cerebral toxin. The main source of ammonia is its endogenous ndogenous production by the gastrointestinal tract from the metabolism of production by the gastrointestinal tract from the metabolism of protein, and from protein, and from the degradation of bacteria and blood from gastrointestinal bleethe degradation of bacteria and blood from gastrointestinal bleeding. ding. �� LactuloseLactulose and and RifaximinRifaximin
�� Liver transplantLiver transplant

Medical Nutrition TherapyMedical Nutrition Therapy
�� Overall Overall meal plan that is well balancedmeal plan that is well balanced and includes fruits and includes fruits and vegetables, whole grains, lean meats, and lowand vegetables, whole grains, lean meats, and low--fat diary fat diary products. products.
�� SodiumSodium--restricted dietrestricted diet. .
�� Liquid supplementLiquid supplement taken by mouth or through a NG tube. taken by mouth or through a NG tube.
�� Consumption of Consumption of four to six mealsfour to six meals
�� Diets which include Diets which include ‘‘easy to digesteasy to digest’’ forms of proteinforms of protein, such as , such as legumes, poultry and fish legumes, poultry and fish
�� Supplementation of Supplementation of vitamins and mineralsvitamins and minerals is often necessary is often necessary because of inadequate intake and altered metabolism and because of inadequate intake and altered metabolism and absorption absorption
�� FluidFluid intake is usually restricted to 1 to 1.5 L/day, depending intake is usually restricted to 1 to 1.5 L/day, depending on the severity of the ascites. on the severity of the ascites.

Implications of findings to the Implications of findings to the
practice of dietetics practice of dietetics
Critical thinking on the part of the nutrition expert is Critical thinking on the part of the nutrition expert is
key to balance the therapy for different conditions. key to balance the therapy for different conditions.
So while there are evidenceSo while there are evidence--based guidelines based guidelines
provided in the Nutrition Care Manual and the provided in the Nutrition Care Manual and the
Evidenced Analysis Library that provide a strong Evidenced Analysis Library that provide a strong
foundation for nutritional recommendations it is foundation for nutritional recommendations it is
imperative to remember that the intuition and imperative to remember that the intuition and
problemproblem--solving skills of physicians and nutrition solving skills of physicians and nutrition
professionals are of utmost importance to provide professionals are of utmost importance to provide
patients with hepatic cirrhosis the most thought out, patients with hepatic cirrhosis the most thought out,
individualized individualized care.care.

References References
�� Calculations for nutrition assessment Calculations for nutrition assessment –– Diseases and Conditions of the Liver, Gallbladder, and PancreasDiseases and Conditions of the Liver, Gallbladder, and Pancreas
> Cirrhosis. American Dietetic Association Nutrition Care Manual> Cirrhosis. American Dietetic Association Nutrition Care Manual. Source: . Source: http://http://www.nutritioncaremanual.org/content.cfm?ncm_content_idwww.nutritioncaremanual.org/content.cfm?ncm_content_id=81465. Retrieved November 30, 2010.=81465. Retrieved November 30, 2010.
�� Cirrhosis. Medline Medical Encyclopedia. Source: Cirrhosis. Medline Medical Encyclopedia. Source:
http://http://www.nlm.nih.gov/medlineplus/cirrhosis.htmlwww.nlm.nih.gov/medlineplus/cirrhosis.html
Topic last reviewed: May 07, 2010. Retrieved: November 25, 2010.Topic last reviewed: May 07, 2010. Retrieved: November 25, 2010.
�� Cirrhosis Cirrhosis -- National Digestive Diseases Information Clearinghouse (NDDIC). National Digestive Diseases Information Clearinghouse (NDDIC). Source: Source:
http://digestive.niddk.nih.gov/ddiseases/pubs/cirrhosis/#treatmehttp://digestive.niddk.nih.gov/ddiseases/pubs/cirrhosis/#treatment.nt. Posted: December 2008. Accessed: December 14, Posted: December 2008. Accessed: December 14, 2010.2010.
�� Disease Process Disease Process –– Diseases and Conditions of the Liver, Gallbladder, and PancreasDiseases and Conditions of the Liver, Gallbladder, and Pancreas > Cirrhosis.> Cirrhosis.
American Dietetic Association Nutrition Care Manual. Source: American Dietetic Association Nutrition Care Manual. Source: http://http://www.nutritioncaremanual.org/content.cfm?ncm_content_idwww.nutritioncaremanual.org/content.cfm?ncm_content_id=81451. Retrieved November 30, 2010.=81451. Retrieved November 30, 2010.
�� Friedman, LS. (2010). Surgery in the Patient with Liver Disease.Friedman, LS. (2010). Surgery in the Patient with Liver Disease. Trans Am Trans Am ClinClin ClimatolClimatol Assoc. 2010; 121Assoc. 2010; 121, ,
192192––205. Source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2917124205. Source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2917124/. Retrieved December 14, 2010./. Retrieved December 14, 2010.
�� Lindsey, A. (2010). Profound hyponatremia in cirrhosis: a case rLindsey, A. (2010). Profound hyponatremia in cirrhosis: a case report. eport. Cases J. 2010; 3: 77Cases J. 2010; 3: 77. Source: . Source:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2851673/?tool=http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2851673/?tool=pubmedpubmed. Published online March 23, 2010. Retrieved . Published online March 23, 2010. Retrieved December 14, 2010.December 14, 2010.
�� Mahan, LK., Mahan, LK., EscottEscott--Stump, S. (2008). Stump, S. (2008). KrauseKrause’’s Food & Nutrition Therapy, 12th Editions Food & Nutrition Therapy, 12th Edition. St. Louis: . St. Louis:
Saunders Elsevier. pgs. 708Saunders Elsevier. pgs. 708--726.726.
�� SanyalSanyal, A. Mullen, K. Bass, N. (2010). The Treatment of Hepatic Enceph, A. Mullen, K. Bass, N. (2010). The Treatment of Hepatic Encephalopathy in the Cirrhotic Patient. alopathy in the Cirrhotic Patient.
GastroenterolGastroenterol HepatolHepatol (N Y). 2010 April; 6(4_Suppl): 1(N Y). 2010 April; 6(4_Suppl): 1––1212. Source: . Source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2886485/#__secid3913http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2886485/#__secid3913169. Retrieved: December 14, 2010.169. Retrieved: December 14, 2010.
�� TaberTaber’’s s CyclopedicCyclopedic Medical Dictionary, 20th Edition. (2001). Philadelphia: F.A. DaMedical Dictionary, 20th Edition. (2001). Philadelphia: F.A. Davis Company.vis Company.
�� Understanding Cirrhosis of the Liver Understanding Cirrhosis of the Liver –– Patient Center of the American Gastroenterological Association.Patient Center of the American Gastroenterological Association.
Source: Source: http://www.gastro.org/patienthttp://www.gastro.org/patient--center/digestivecenter/digestive--conditions/cirrhosisconditions/cirrhosis--ofof--thethe--liver.liver. Topic Last Reviewed: April 2008. Topic Last Reviewed: April 2008. Retrieved November 26, 2010. Retrieved November 26, 2010.

Questions ??Questions ??