Embed Size (px)
Citation preview

M. ValgimigliM. ValgimigliUniversity of University of
FerraraFerrara
ItalyItaly
Autologous bone marrow stem cell mobilization
Induced by G-CSF after MI
Autologous bone marrow stem cell mobilization
Induced by G-CSF after MI
FOURTH INTERNATIONAL SYMPOSIUM ON STEM CELL THERAPY AND APPLIED CARDIOVASCULAR BIOLOGY
FOURTH INTERNATIONAL SYMPOSIUM ON STEM CELL THERAPY AND APPLIED CARDIOVASCULAR BIOLOGY
Madrid, 26°April 2007Madrid, 26°April 2007Madrid, 26°April 2007Madrid, 26°April 2007
Direct InoculationDirect Inoculation
The New Paradigm?The New Paradigm?The “NO TOUCH” policy
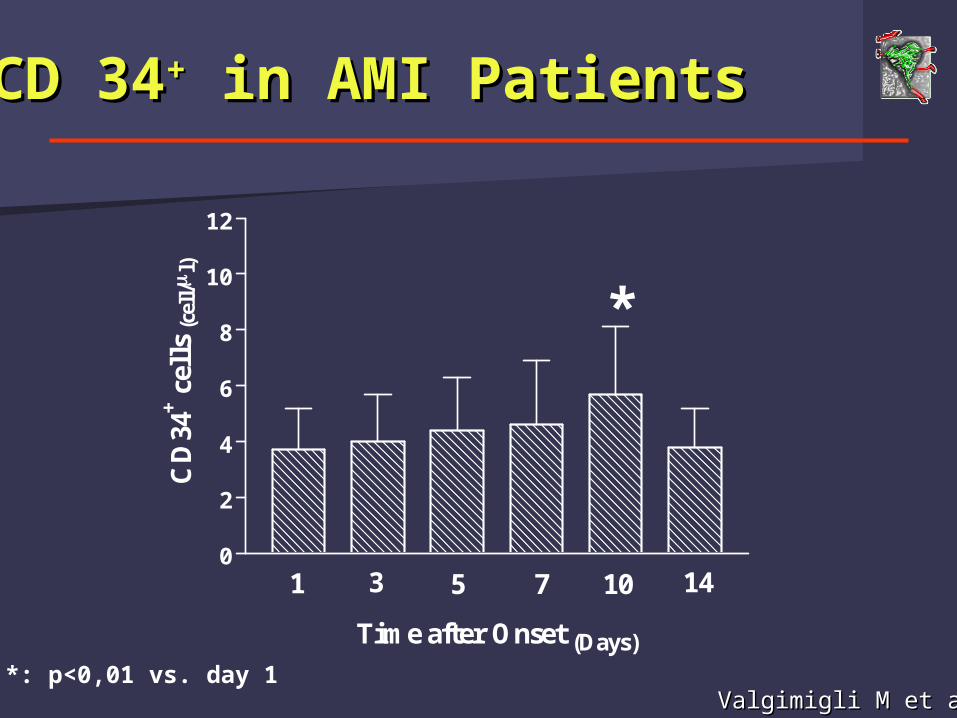
CD 34CD 34++ in AMI Patients in AMI Patients
0
2
4
6
8
10
12
1 3 5 7 10 14
*
Time after Onset (Days)
CD
34+ c
ells
(cel
l/
l)
*: p<0,01 vs. day 1Valgimigli M et al.Valgimigli M et al.
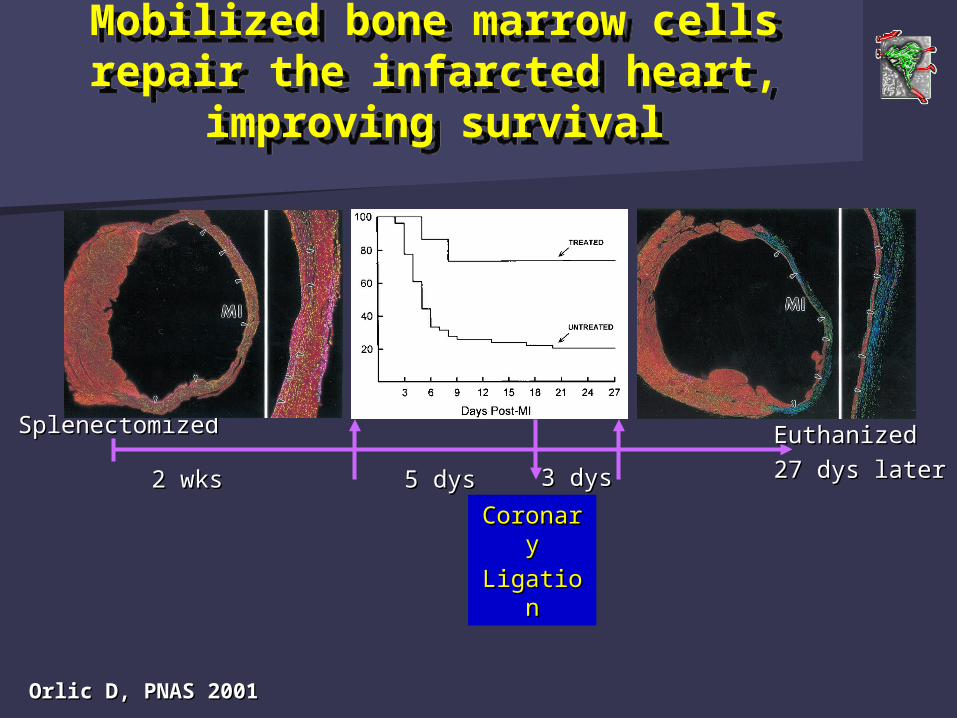
Mobilized bone marrow cells repair the infarcted heart,
improving survival
Mobilized bone marrow cells repair the infarcted heart,
improving survival
6 mice6 mice
SplenectomizedSplenectomized
2 wks2 wks
200 µg/kg/day SCF50 µg/kg/day G-CSF
5 dys5 dys 3 dys3 dys
CoronarCoronaryy
LigationLigation
EuthanizedEuthanized
27 dys later27 dys later
Orlic D, PNAS 2001Orlic D, PNAS 2001
G-CSF: the ideal G-CSF: the ideal candidatecandidate
G-CSF: the ideal G-CSF: the ideal candidatecandidate
Dose-dependent BM stem cells Dose-dependent BM stem cells mobilisizermobilisizer
Safety established on healthy donorsSafety established on healthy donors
Reassuring long-term data availableReassuring long-term data available
However:However:
Platelet activation with shortening of bleeding Platelet activation with shortening of bleeding time*time*
Fibrinogen and FVIII protein C and S*Fibrinogen and FVIII protein C and S*
Sporadical occurence of AMI in healthy donors Sporadical occurence of AMI in healthy donors *:Bone marrow transplantation 98; 22: 1087*:Bone marrow transplantation 98; 22: 1087
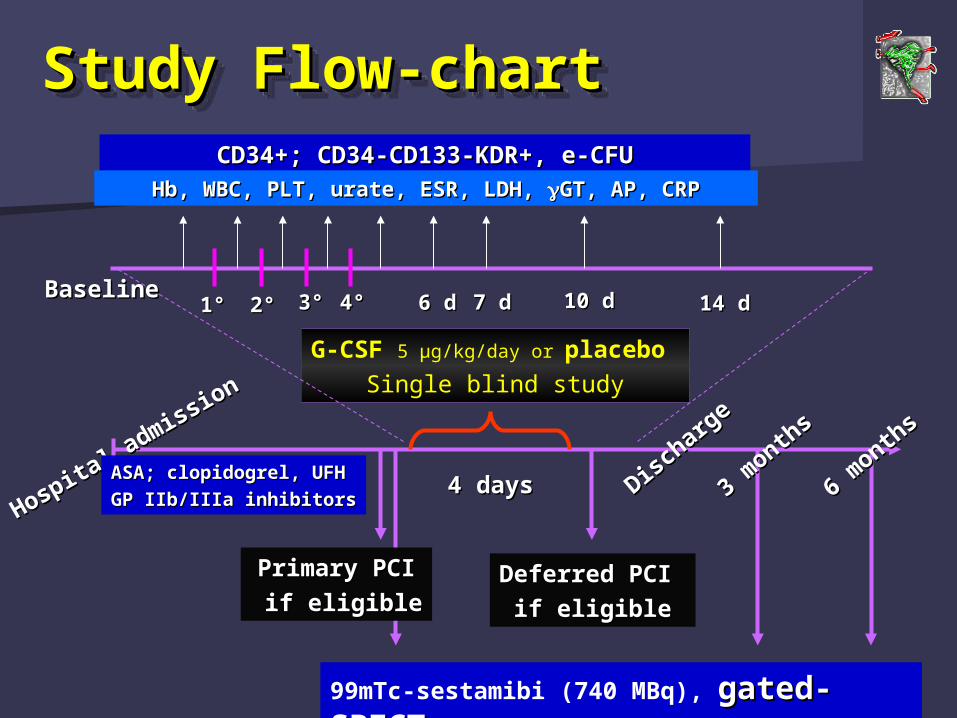
Study Flow-chartStudy Flow-chartStudy Flow-chartStudy Flow-chart
Primary PCIPrimary PCI
if eligibleif eligible
G-CSF 5 µg/kg/day or placebo Single blind study
Hospita
l admiss
ion
Hospita
l admiss
ion
ASA; clopidogrel, UFHASA; clopidogrel, UFH
GP IIb/IIIa inhibitorsGP IIb/IIIa inhibitors4 days4 days
Deferred PCI Deferred PCI
if eligibleif eligible
99mTc-sestamibi (740 MBq), gated-gated-SPECTSPECT
Disch
arge
Disch
arge
3 month
s
3 month
s
6 month
s
6 month
s
BaselineBaseline1°1° 2°2° 3°3° 4°4° 6 d6 d 7 d7 d 10 d10 d 14 d14 d
CD34+; CD34-CD133-KDR+, e-CFUCD34+; CD34-CD133-KDR+, e-CFUHb, WBC, PLT, urate, ESR, LDH, Hb, WBC, PLT, urate, ESR, LDH, GT, AP, CRPGT, AP, CRP
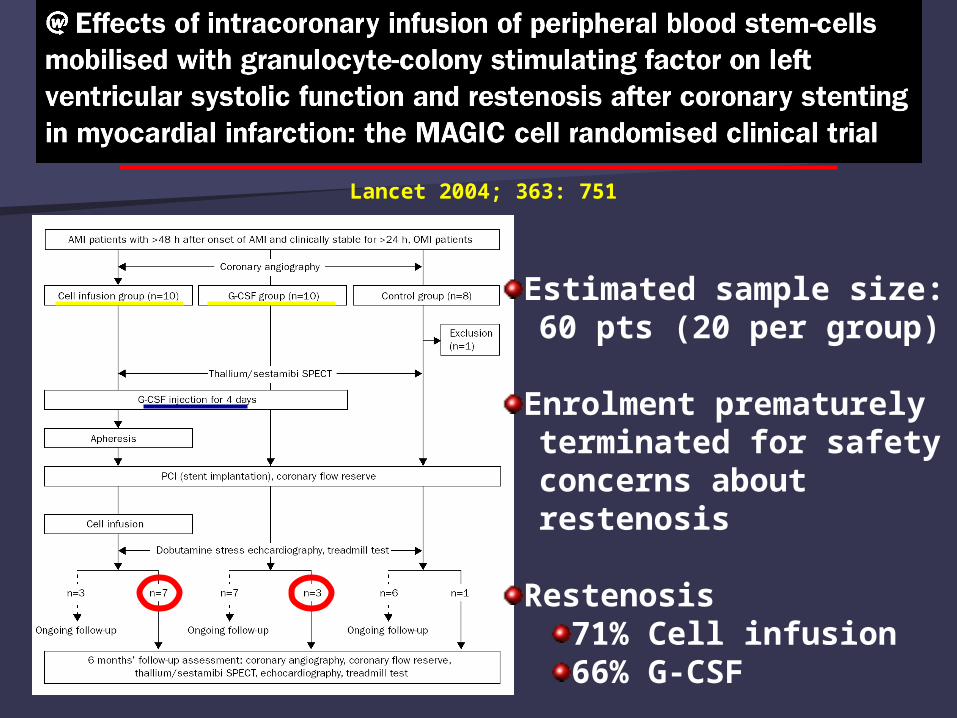
Estimated sample size: 60 pts (20 per group)
Enrolment prematurely terminated for safety concerns about restenosis
Restenosis71% Cell infusion66% G-CSF
Lancet 2004; 363: 751
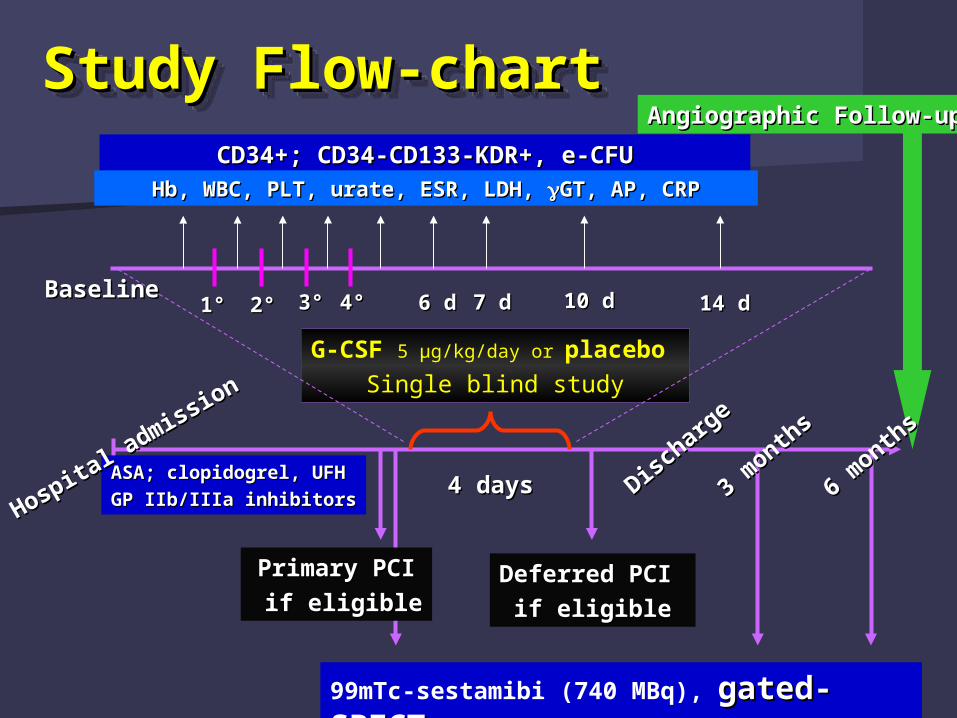
Study Flow-chartStudy Flow-chartStudy Flow-chartStudy Flow-chart
Primary PCIPrimary PCI
if eligibleif eligible
G-CSF 5 µg/kg/day or placebo Single blind study
ASA; clopidogrel, UFHASA; clopidogrel, UFH
GP IIb/IIIa inhibitorsGP IIb/IIIa inhibitors4 days4 days
Deferred PCI Deferred PCI
if eligibleif eligible
99mTc-sestamibi (740 MBq), gated-gated-SPECTSPECT
Disch
arge
Disch
arge
3 month
s
3 month
s
BaselineBaseline1°1° 2°2° 3°3° 4°4° 6 d6 d 7 d7 d 10 d10 d 14 d14 d
CD34+; CD34-CD133-KDR+, e-CFUCD34+; CD34-CD133-KDR+, e-CFUHb, WBC, PLT, urate, ESR, LDH, Hb, WBC, PLT, urate, ESR, LDH, GT, AP, CRPGT, AP, CRP
Angiographic Follow-upAngiographic Follow-up
6 month
s
6 month
s
Hospita
l admiss
ion
Hospita
l admiss
ion
Use of G-CSF during AMI to Use of G-CSF during AMI to Enhance BMSC in HumansEnhance BMSC in Humans
Clinical Safety ProfileClinical Safety Profile
20 pts out of 47 screened with AMI 20 pts out of 47 screened with AMI
3 pts per group not treated with 1° PCI due 3 pts per group not treated with 1° PCI due to late presentation, subsequently 1 pt per to late presentation, subsequently 1 pt per group underwent deferred PCI for evidence group underwent deferred PCI for evidence of myocardial viability in the infarcted areaof myocardial viability in the infarcted area
Syntoms Onset to G-CSG: Syntoms Onset to G-CSG: 3737±265 hours (3-265) in the whole population±265 hours (3-265) in the whole population
16±66 hours (3-61) in those submitted to pPCI16±66 hours (3-61) in those submitted to pPCI
and and AngiographicAngiographic
Valgimigli et al. EHJ 2005;26: 1838–1845
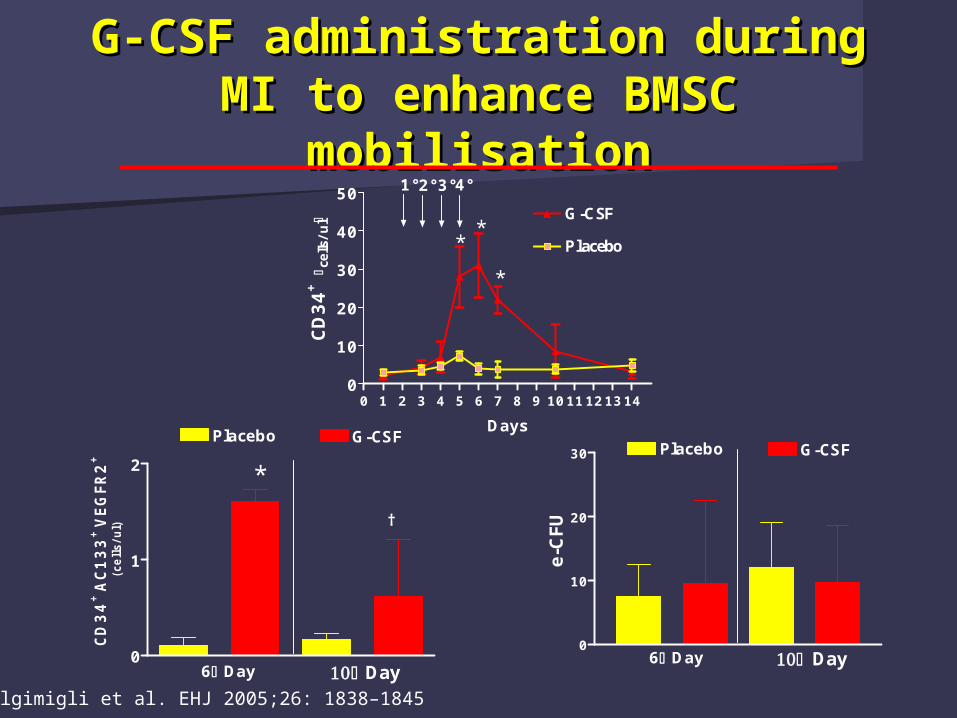
G-CSF administration during G-CSF administration during MI to enhance BMSC MI to enhance BMSC
mobilisationmobilisation
0 1 2 3 4 5 6 7 8 9 1011121314 0
10
20
30
40
50
Placebo
G-CSF
1°2°3°4°
*
*
*
Days
CD
34
+ c
ells
/ul
0
1
2
Placebo G-CSF
6 Day Day
*
†
CD
34
+A
C1
33
+V
EG
FR2
+
(ce
lls/
ul)
0
10
20
30 Placebo G-CSF
Day6 Day
e-CFU
Valgimigli et al. EHJ 2005;26: 1838–1845
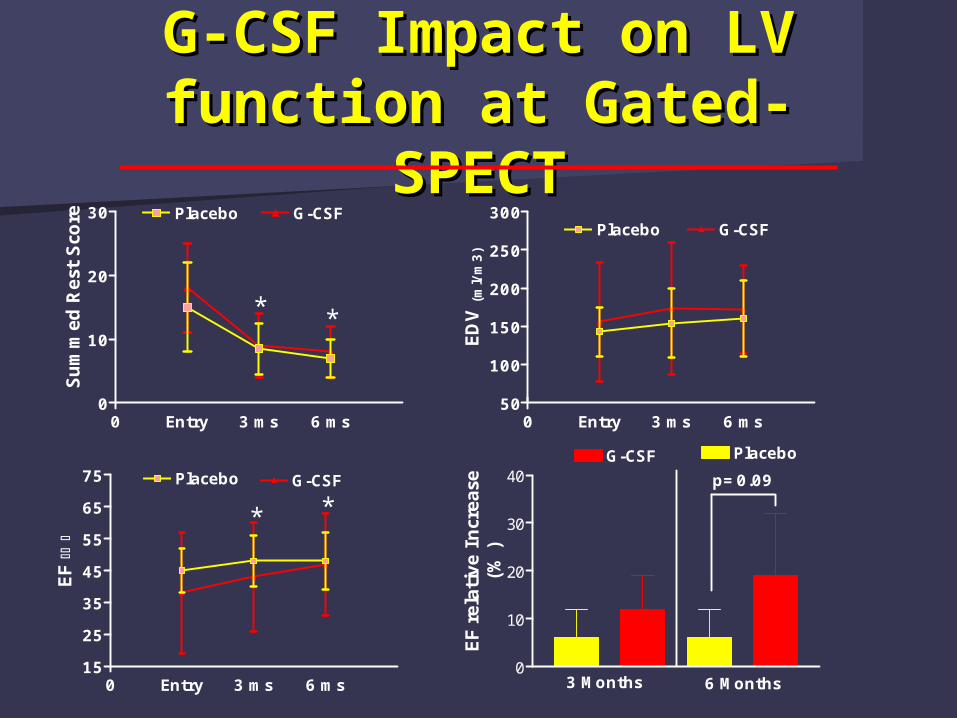
G-CSF Impact on LV G-CSF Impact on LV function at Gated-function at Gated-
SPECTSPECT
0 Entry 3 ms 6 ms 0
10
20
30 Placebo G-CSF
**
Sum
med
Res
t Sco
re
0 Entry 3 ms 6 ms 50
100
150
200
250
300Placebo G-CSF
ED
V(m
l/m
3)
0 Entry 3 ms 6 ms 15
25
35
45
55
65
75 Placebo G-CSF
* *
EF
0
10
20
30
40G-CSF Placebo
3 Months 6 Months
EF
rela
tive
Incr
ease
(%)
p=0.09
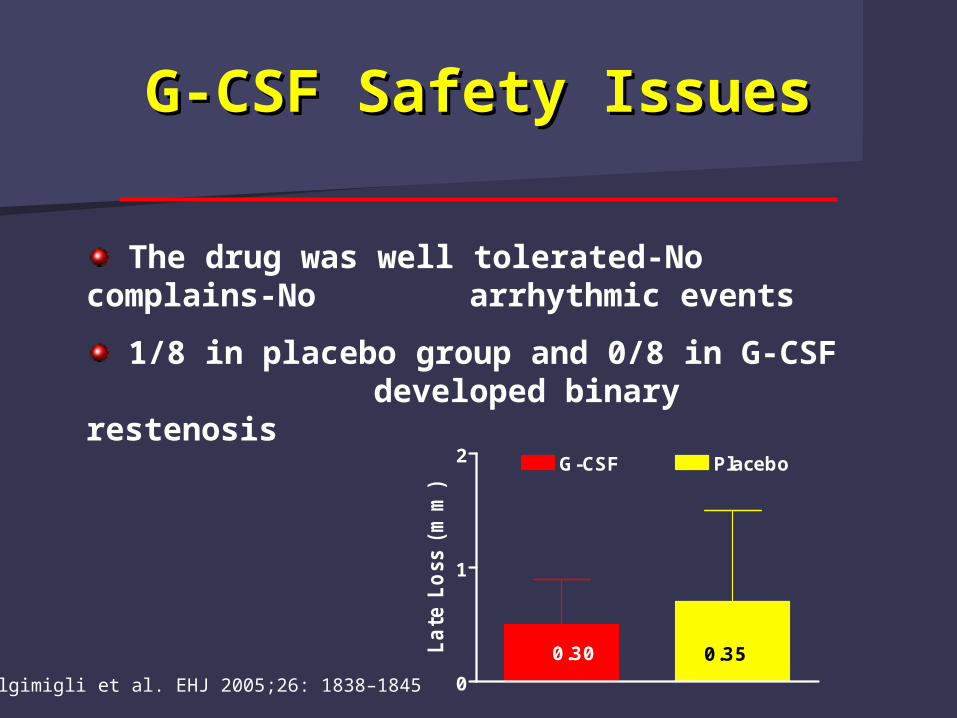
G-CSF Safety IssuesG-CSF Safety Issues
0
1
2 G-CSF Placebo
0.30 0.35Late
Lo
ss (
mm
)
The drug was well tolerated-No complains-No arrhythmic events
1/8 in placebo group and 0/8 in G-CSF developed binary restenosis
Valgimigli et al. EHJ 2005;26: 1838–1845
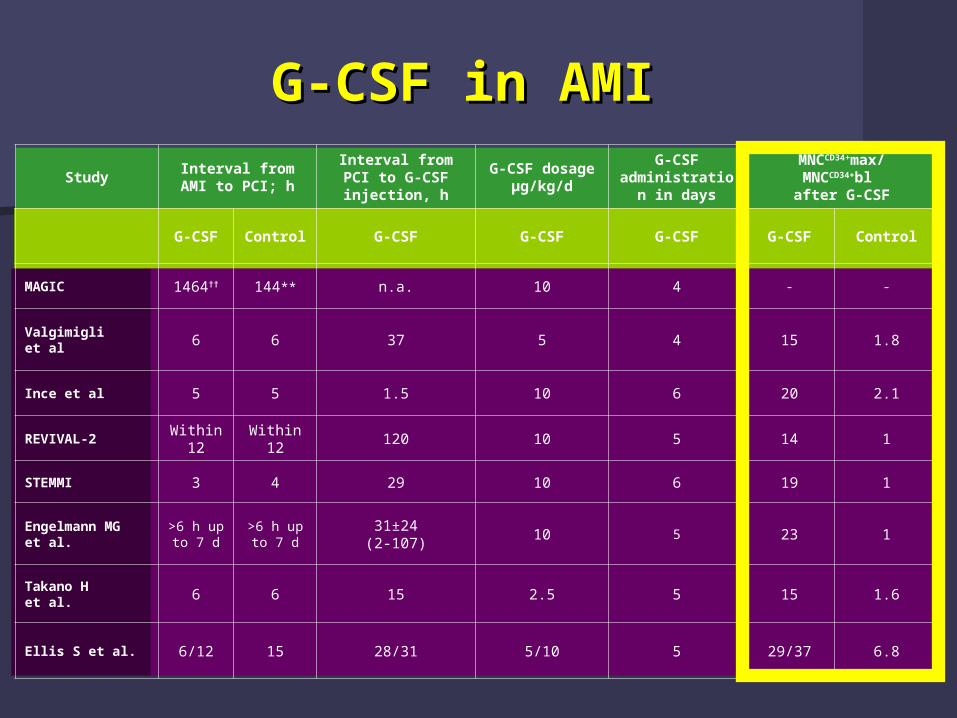
G-CSF in AMI G-CSF in AMI
StudyInterval from AMI to PCI; h
Interval from PCI to G-CSF injection, h
G-CSF dosageµg/kg/d
G-CSF administratio
n in days
MNCCD34+max/MNCCD34+bl after G-CSF
G-CSF Control G-CSF G-CSF G-CSF G-CSF Control
MAGIC 1464†† 144** n.a. 10 4 - -
Valgimigli et al 6 6 37 5 4 15 1.8
Ince et al 5 5 1.5 10 6 20 2.1
REVIVAL-2Within
12Within
12120 10 5 14 1
STEMMI 3 4 29 10 6 19 1
Engelmann MGet al.
>6 h up to 7 d
>6 h up to 7 d
31±24(2-107)
10 5 23 1
Takano Het al. 6 6 15 2.5 5 15 1.6
Ellis S et al. 6/12 15 28/31 5/10 5 29/37 6.8
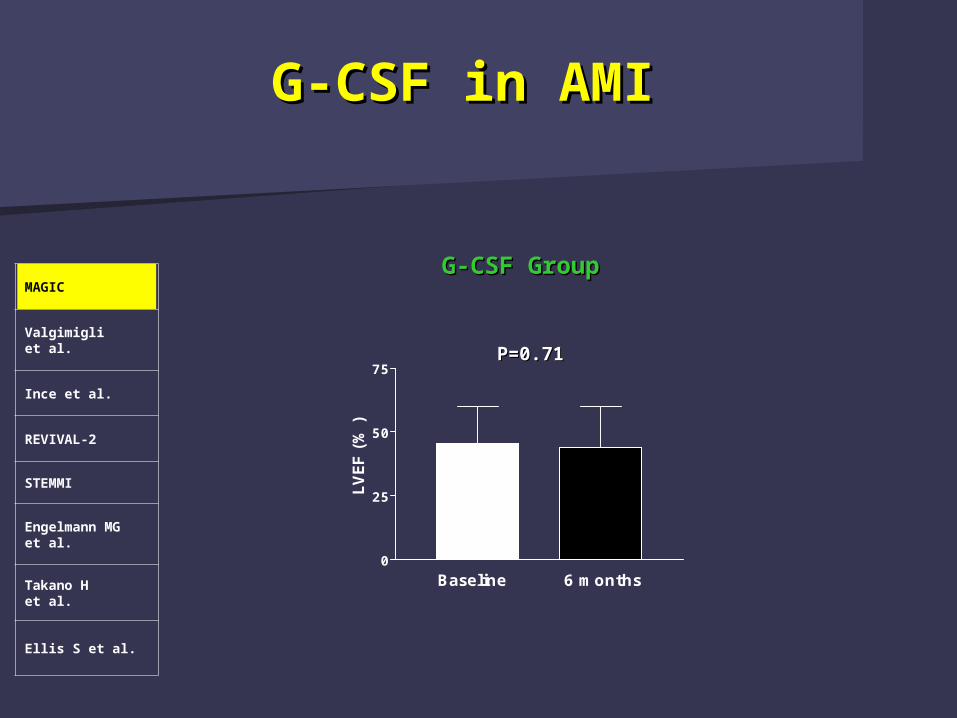
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
0
25
50
75
Baseline 6 months
LVEF (
%)
P=0.71P=0.71
G-CSF GroupG-CSF Group
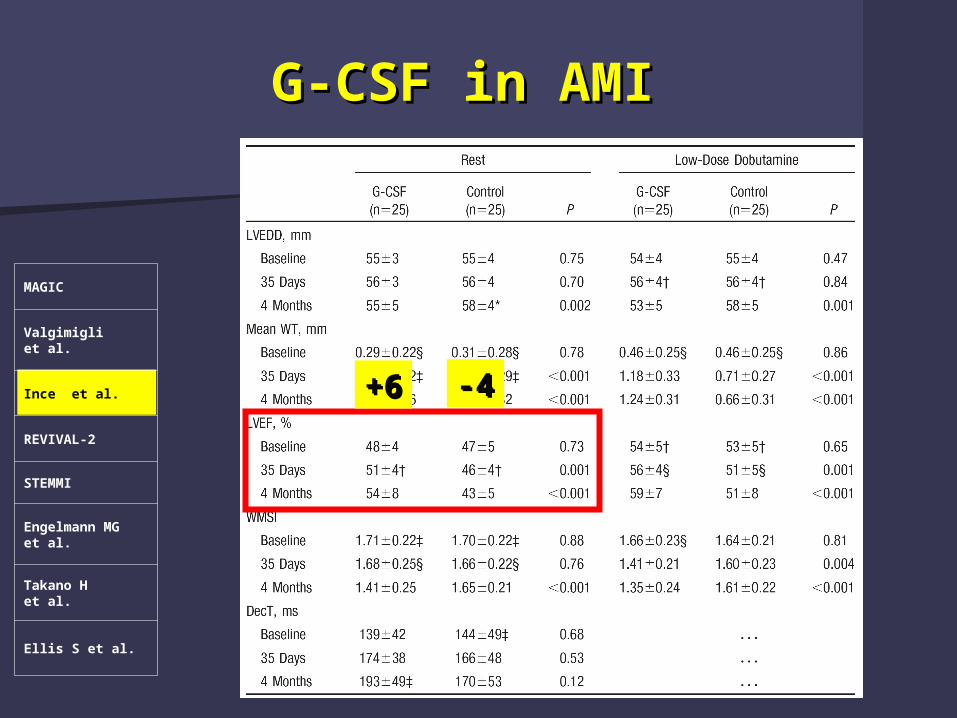
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
+6+6 -4-4
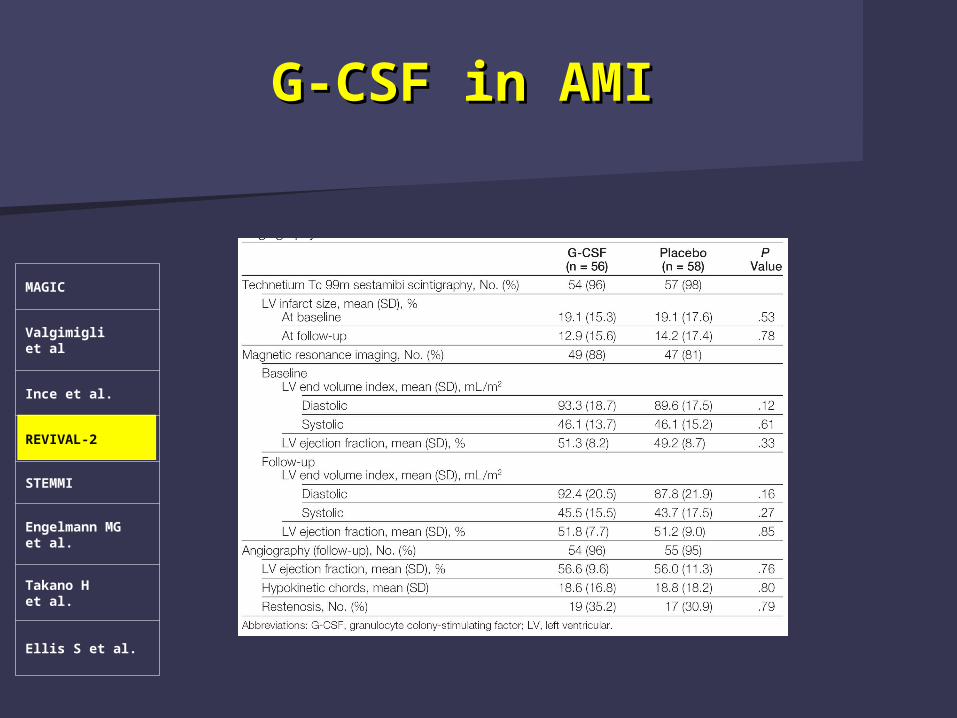
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
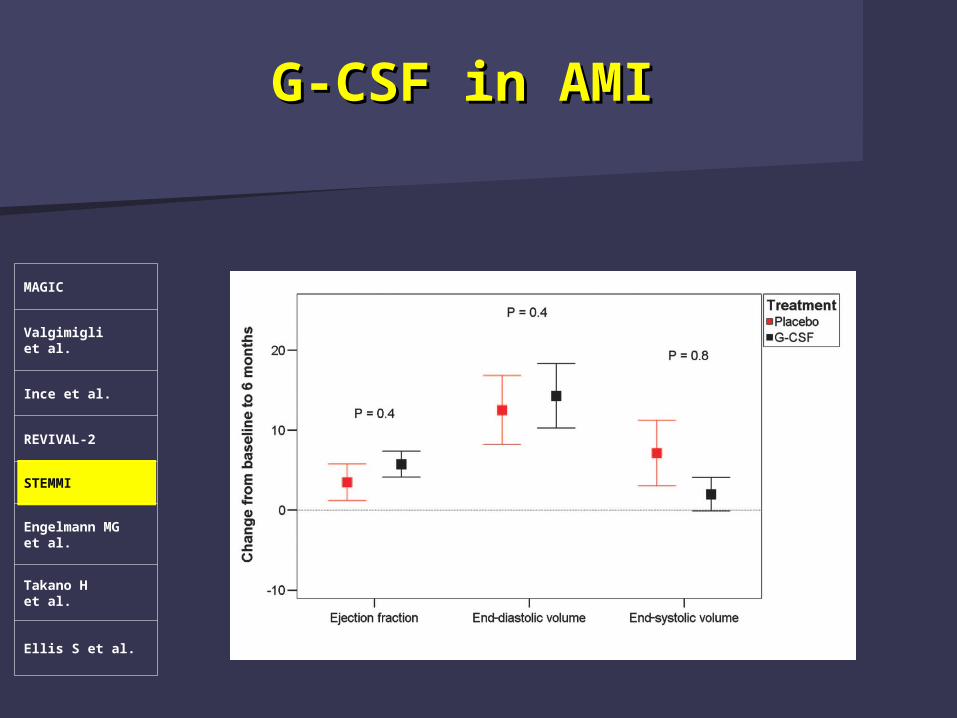
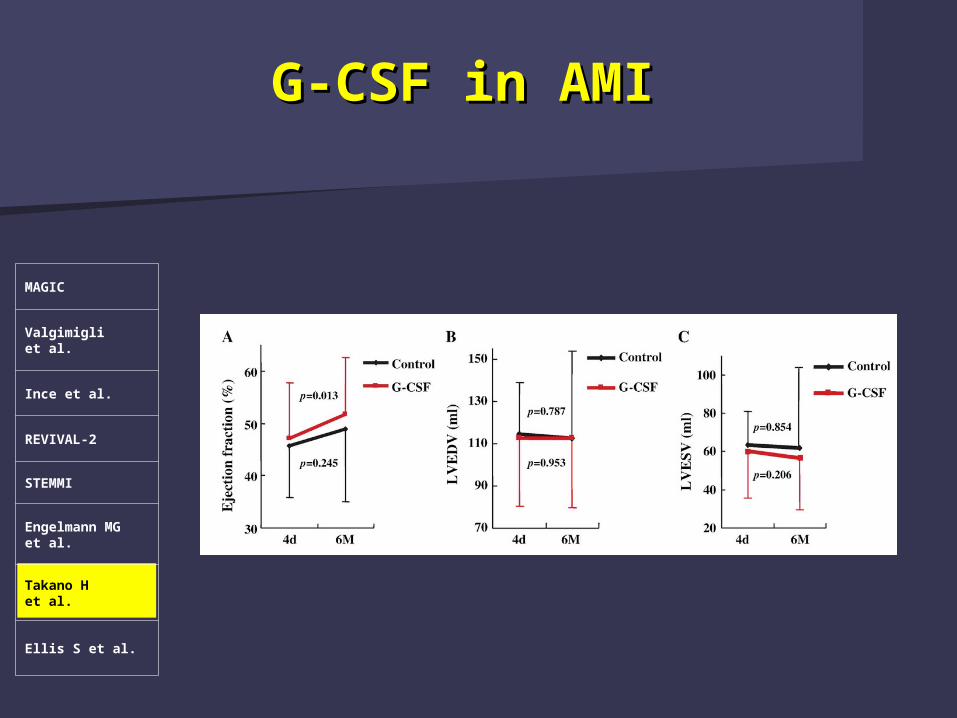
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
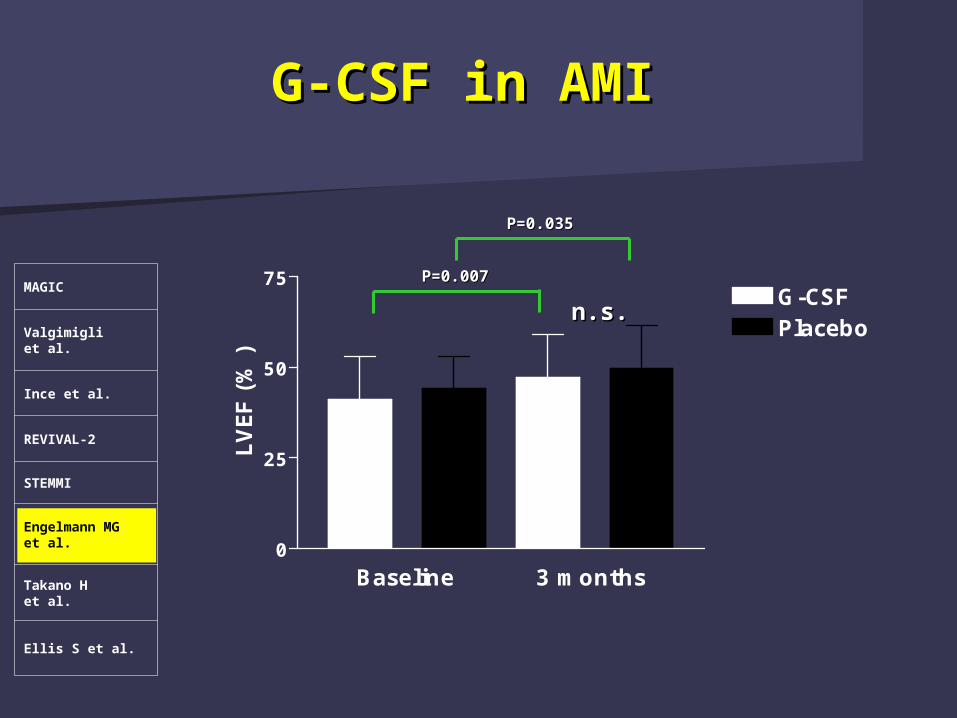
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
0
25
50
75G-CSFPlacebo
Baseline 3 months
LVEF (
%)
P=0.007P=0.007
P=0.035P=0.035
n.s.n.s.
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
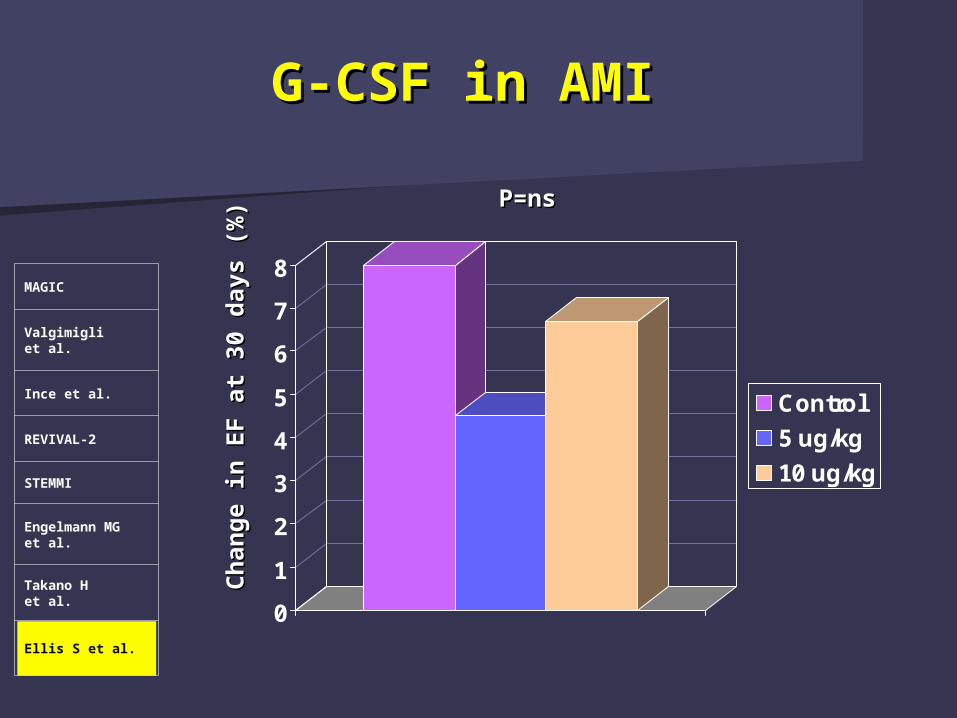
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
0
1
2
3
4
5
6
7
8
Control
5 ug/kg
10 ug/kg
Ch
an
ge in
EF a
t 30 d
ays (
%)
Ch
an
ge in
EF a
t 30 d
ays (
%)
P=nsP=ns
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
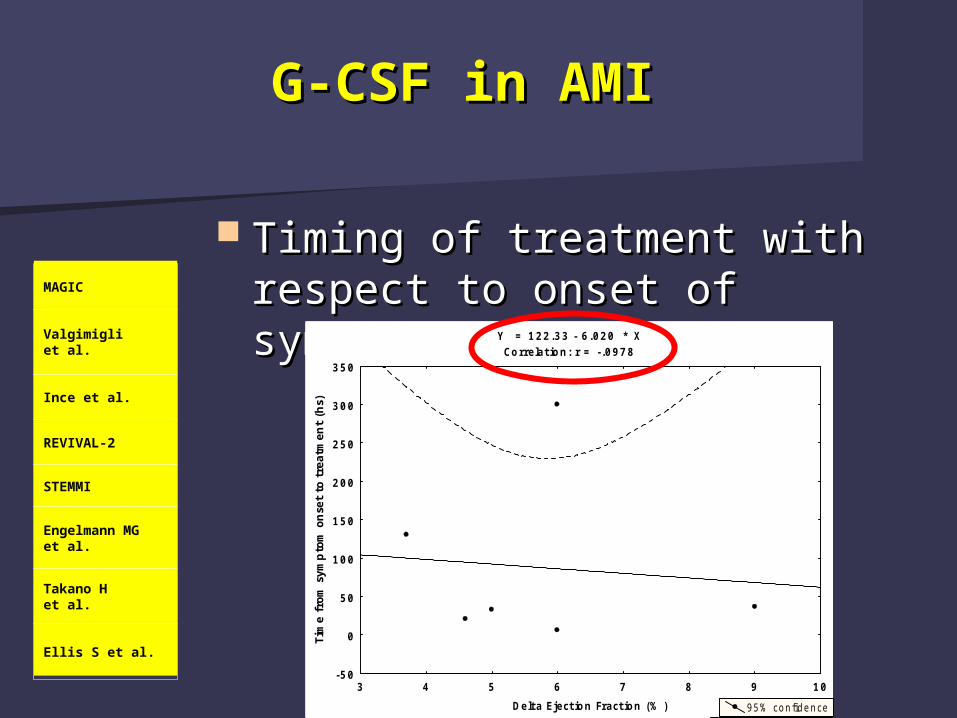
Timing of treatment with Timing of treatment with respect to onset of symptomsrespect to onset of symptoms
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
Y = 876 .87 - 129 .7 * XCo rrelat io n : r = - .8476
-4 -2 0 2 4 6 8 10
Delt a Eject io n Fract ion (% )
-200
0
200
400
600
800
1000
1200
1400
1600
Tim
e f
rom
sym
pto
m o
nse
t to
tre
atm
ent
(hs)
9 5% co nfidence
M A GIC
Y = 122 .33 - 6 .020 * XCo rrelat io n : r = - .0978
3 4 5 6 7 8 9 10
Delt a Eject io n Fract ion (% )
-50
0
50
100
150
200
250
300
350
Tim
e f
rom
sym
pto
m o
nse
t to
tre
atm
ent
(hs)
9 5 % con fid e n ce
Targeting the proper patient Targeting the proper patient populationpopulation
Severe LV function impairmentSevere LV function impairment
Anterior wall MIAnterior wall MI
Suboptimal mechanical reperfusionSuboptimal mechanical reperfusion
G-CSF in AMI G-CSF in AMI
MAGIC
Valgimigli et al.
Ince et al.
REVIVAL-2
STEMMI
Engelmann MGet al.
Takano Het al.
Ellis S et al.
No data beyond 30 daysNo data beyond 30 days
12 pts G-CSF vs. 6 controls12 pts G-CSF vs. 6 controls
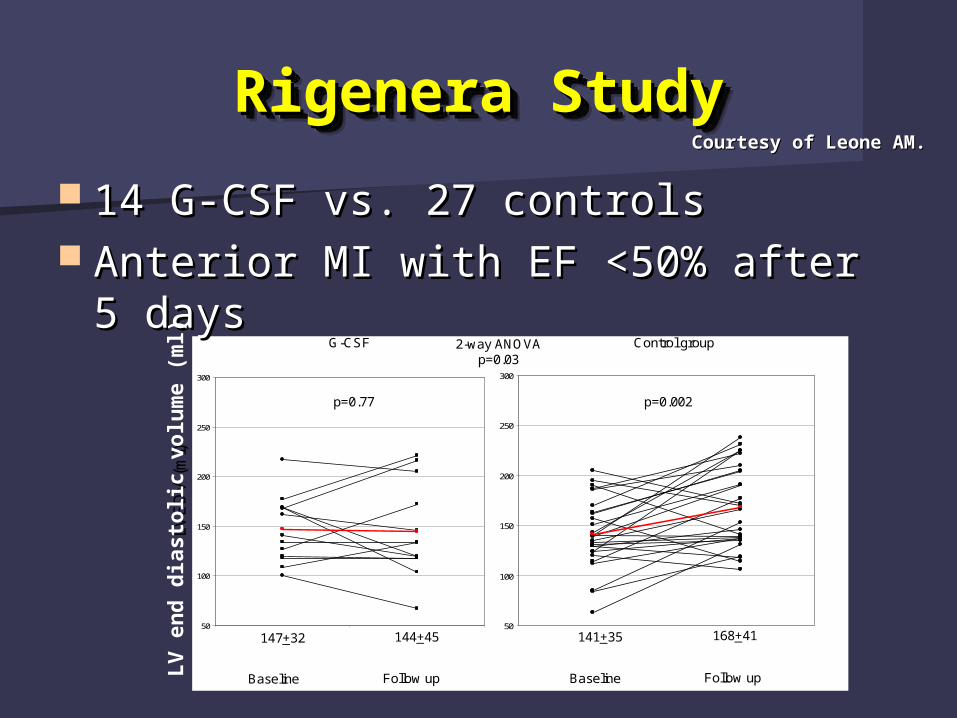
Rigenera StudyRigenera StudyRigenera StudyRigenera Study
14 G-CSF vs. 27 controls14 G-CSF vs. 27 controls Anterior MI with EF <50% after 5 Anterior MI with EF <50% after 5
daysdays
Courtesy of Leone AM.Courtesy of Leone AM.
50
100
150
200
250
300
50
100
150
200
250
300
LV
ED
V (
ml)
Baseline BaselineFollow up Follow up
147+32 144+45 141+35 168+41
G-CSF Control group
p=0.002p=0.77
2-way ANOVAp=0.03
LV
en
d d
iasto
lic v
olu
me (
ml)
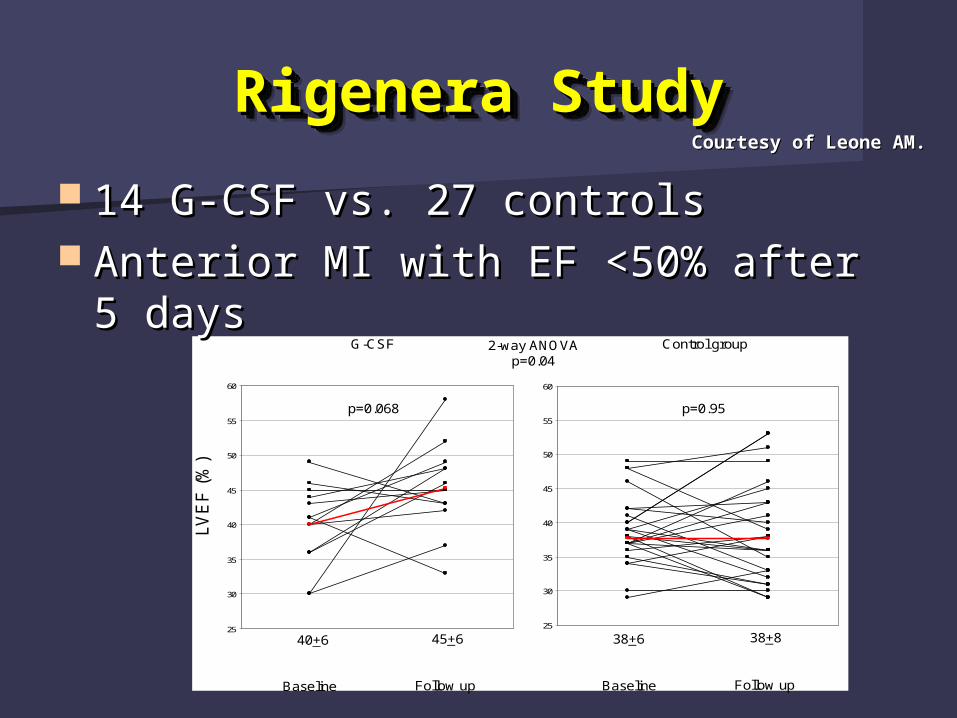
Rigenera StudyRigenera StudyRigenera StudyRigenera Study
14 G-CSF vs. 27 controls14 G-CSF vs. 27 controls Anterior MI with EF <50% after 5 Anterior MI with EF <50% after 5
daysdays
Courtesy of Leone AM.Courtesy of Leone AM.
25
30
35
40
45
50
55
60
25
30
35
40
45
50
55
60
LV
EF
(%
)
Baseline BaselineFollow up Follow up
40+6 45+6 38+6 38+8
G-CSF Control group
p=0.95p=0.068
2-way ANOVAp=0.04
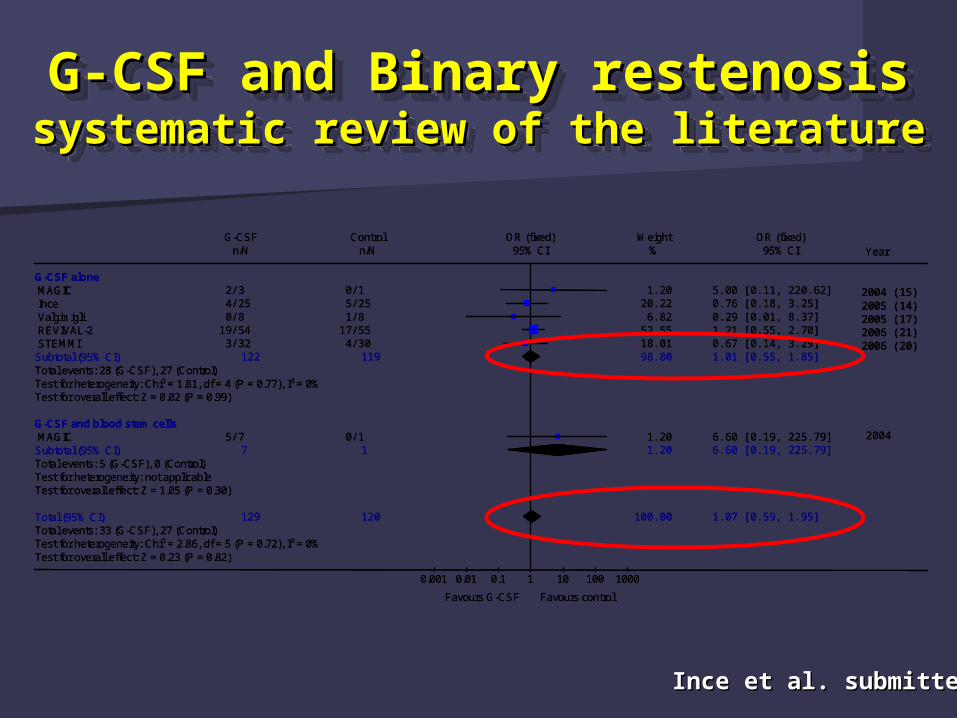
G-CSF and Binary restenosisG-CSF and Binary restenosissystematic review of the literaturesystematic review of the literatureG-CSF and Binary restenosisG-CSF and Binary restenosissystematic review of the literaturesystematic review of the literature
G-CSF Control OR (fixed) Weight OR (fixed)n/N n/N 95% CI % 95% CI Year
G-CSF aloneMAGIC 2/3 0/1 1.20 5.00 [0.11, 220.62] Ince 4/25 5/25 20.22 0.76 [0.18, 3.25] Valgimigli 0/8 1/8 6.82 0.29 [0.01, 8.37] REVIVAL-2 19/54 17/55 52.55 1.21 [0.55, 2.70] STEMMI 3/32 4/30 18.01 0.67 [0.14, 3.29]
Subtotal (95% CI) 122 119 98.80 1.01 [0.55, 1.85]Total events: 28 (G-CSF), 27 (Control)Test for heterogeneity: Chi² = 1.81, df = 4 (P = 0.77), I² = 0%Test for overall effect: Z = 0.02 (P = 0.99)
G-CSF and blood stem cellsMAGIC 5/7 0/1 1.20 6.60 [0.19, 225.79] 2004
Subtotal (95% CI) 7 1 1.20 6.60 [0.19, 225.79]Total events: 5 (G-CSF), 0 (Control)Test for heterogeneity: not applicableTest for overall effect: Z = 1.05 (P = 0.30)
Total (95% CI) 129 120 100.00 1.07 [0.59, 1.95]Total events: 33 (G-CSF), 27 (Control)Test for heterogeneity: Chi² = 2.86, df = 5 (P = 0.72), I² = 0%Test for overall effect: Z = 0.23 (P = 0.82)
0.001 0.01 0.1 1 10 100 1000
Favours G-CSF Favours control
2004 (15)2005 (14)2005 (17)2006 (21)2006 (20)
G-CSF Control OR (fixed) Weight OR (fixed)n/N n/N 95% CI % 95% CI Year
G-CSF aloneMAGIC 2/3 0/1 1.20 5.00 [0.11, 220.62] Ince 4/25 5/25 20.22 0.76 [0.18, 3.25] Valgimigli 0/8 1/8 6.82 0.29 [0.01, 8.37] REVIVAL-2 19/54 17/55 52.55 1.21 [0.55, 2.70] STEMMI 3/32 4/30 18.01 0.67 [0.14, 3.29]
Subtotal (95% CI) 122 119 98.80 1.01 [0.55, 1.85]Total events: 28 (G-CSF), 27 (Control)Test for heterogeneity: Chi² = 1.81, df = 4 (P = 0.77), I² = 0%Test for overall effect: Z = 0.02 (P = 0.99)
G-CSF and blood stem cellsMAGIC 5/7 0/1 1.20 6.60 [0.19, 225.79] 2004
Subtotal (95% CI) 7 1 1.20 6.60 [0.19, 225.79]Total events: 5 (G-CSF), 0 (Control)Test for heterogeneity: not applicableTest for overall effect: Z = 1.05 (P = 0.30)
Total (95% CI) 129 120 100.00 1.07 [0.59, 1.95]Total events: 33 (G-CSF), 27 (Control)Test for heterogeneity: Chi² = 2.86, df = 5 (P = 0.72), I² = 0%Test for overall effect: Z = 0.23 (P = 0.82)
0.001 0.01 0.1 1 10 100 1000
Favours G-CSF Favours control
2004 (15)2005 (14)2005 (17)2006 (21)2006 (20)
2004 (15)2005 (14)2005 (17)2006 (21)2006 (20)
Ince et al. submittedInce et al. submitted
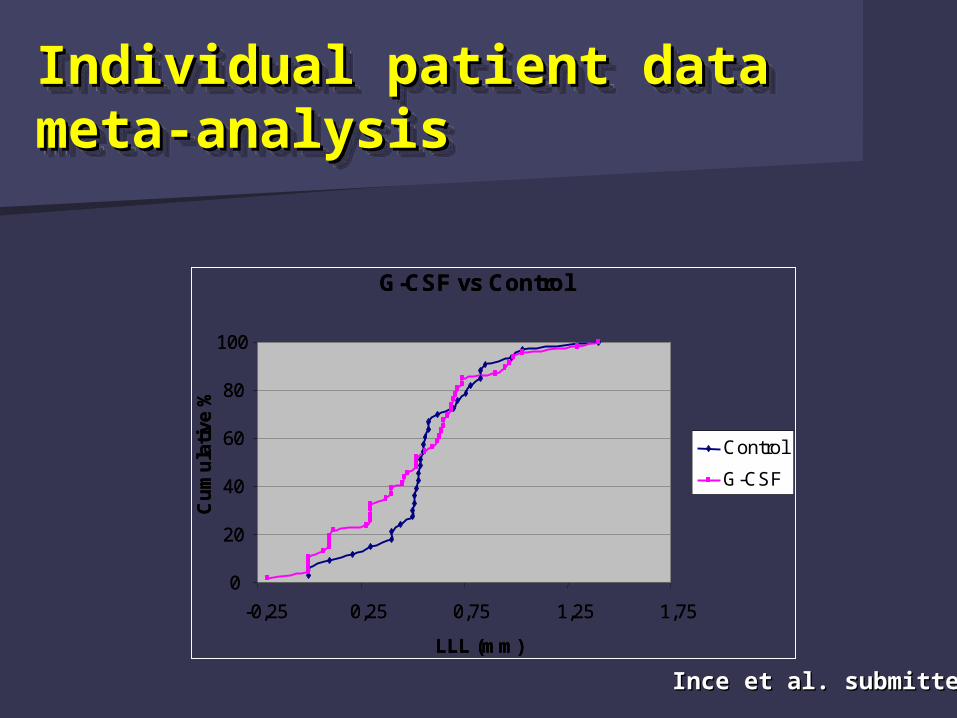
Individual patient data Individual patient data meta-analysismeta-analysisIndividual patient data Individual patient data meta-analysismeta-analysis
G-CSF vs Control
0
20
40
60
80
100
-0,25 0,25 0,75 1,25 1,75
LLL (mm)
Cu
mu
lati
ve %
Control
G-CSF
G-CSF vs Control
0
20
40
60
80
100
-0,25 0,25 0,75 1,25 1,75
LLL (mm)
Cu
mu
lati
ve %
Control
G-CSF
Ince et al. submittedInce et al. submitted
ConclusionsConclusionsConclusionsConclusions
G-CSF administration in acute MI is G-CSF administration in acute MI is feasiblefeasible
No No REALREAL concern regarding clinical concern regarding clinical and ANGIOGRAPHIC safety profileand ANGIOGRAPHIC safety profile
The effect of this treatment on LV The effect of this treatment on LV function improvement remains function improvement remains unclearunclear
The time has arrived for The time has arrived for
a multicenter RCT a multicenter RCT
The time has arrived for The time has arrived for
a multicenter RCT a multicenter RCT



















![Bone marrow transplants for cancer (other than …...An autologous or allogeneic (ablative and non-myeloablative [mini-transplant]) hematopoietic stem cell transplantation, single](https://img.pdfslide.us/doc/110x75/5f0ea6807e708231d440431f/bone-marrow-transplants-for-cancer-other-than-an-autologous-or-allogeneic-ablative.jpg)









