Embed Size (px)
Citation preview

[CANCERRESEARCH54,6137-6142,December1, 19941
ABSTRACT
Our purpose was to determine the maximum tolerated dose of, and themlnhnum interval between treatments with, multiple cycles of carboplatin(CBDCA)rescued with peripheral blood progenitors and fllgrastim. Eligible patients had advanced cancers without prior chemotherapy or radiotherapy. The study design involved a sequential cross-over in whichpatients initially received two or three courses of cyclophosphamide(CPA) at a dose of3.0 g/m2,supported by fllgrastim. Multiple leukapheresea were then performed during the rebound phase of hematologicalrecovery following each CPA-induced nadir to harvest peripheral bloodprogenitors, which were then reinfused as rescue foliowing each of fourcourses of CBDCA. We attempted to administer the CBDCA at 14-dayintervals. The CBDCA dose (mglm2/course) was escalated as follows insuccessive cohorts of patients: Level I, 500; Level II, 800; Level III, 1200;Level LIla, 1000. Following determination of the maximum tolerated dose
of CBDCA administered in this fashion, a subsequent cohort of patients(Level IV) were treated with two courses of high-dose CPA and four
courses of the combination of CBDCA (1000 mg/rn2) plus CPA (1500mglm2). Thirty-one patients were enrolled in the trial. Five patients wereremoved from study prior to completion of protocol therapy, three due totoxicity and two who developed progressive cancer while on study. Themaximum tolerated dose of CBDCA was 1000 mg/rn2, with dose-limitingototoxicity occurring at 1200 mg/m2. The median Inter-treatment intervalfor all cycles was 15 days (range, 12-30). The median intervals betweenCBDCA courses for each dose level were: Level I, 17 days; Level II, 17days; Level III, 14 days; Level ifs, 15 days; Level IV, 16 days. Themedian dose intensity of the CPA phase was 1493 mg/mi/week. Themedian (and range) CBDCA dose intensities (measured from the start ofCBDCA) for each dose level were: I, 185 (151—222);II, 328 (305—380);III,567 (512—646);ifia, 465 (363—481);Level IV, 468 (333—500).Neutropenicfever complicated 35 of 113 CBDCA or CBDCA/CPA courses. Platelettransfusion was required in 51 of 113 courses. One patient had severeepistaxis. There were no treatment-related deaths. Among 27 patients
with ovarian cancer who were evaluable for response, there were 5pathologically documented complete (including 3 of 10 at Level IV) and 16partial responses. We concluded that peripheral blood progenitors facilitate the simultaneous dose escalation and schedule intensification ofcarboplatin chemotherapy. The effect is sustained over four courses oftreatmenL The maximum tolerated dose of carboplatin administered inthis fashion, either as a singleagent or in combinationwith CPA, is 1000mg/m2, with an intertreatment interval of approximately 16 days.
INTRODUCTION
While cytotoxic chemotherapy can cure some types of disseminatedcancer, in most cases it fails to do so, due to mechanisms which arecollectively referred to as “drugresistance―(1). Some component of
Received 6/13/94; accepted 10/4/94.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
I Supported by a grant from Bristol-Myers, by the Avon Program, and by Grant
CA-05826.2 Supported by an American Cancer Society Qini@al Oncology Career Development
Award. To whom requests for reprints should be addressed, at St. Vincent's Hospital, ElmPark, Dublin 4, Ireland.
this drug resistance may be relative rather than absolute, however,inasmuch as it can be at least partially overcome by dose escalation ofthe drugs to which the tumor cells had become resistant. For example,patients with lymphoma (2) or germ cell cancer (3) which wasrefractory to prior, conventionally dosed therapy, can achieve complete remissions (some of which are durable), when treated withHDC3 in the range which requires autologous bone marrow infusionas rescue. HDC also produces frequent complete responses in patientswith breast (4) and ovarian neoplasia (5); however, most of theseremissions are temporary.
Those patients who do not respond or who have only a partialresponse to high-dose chemotherapy likely have tumors in whichhighly resistant cancer cells predominate. Conversely, the minority ofpatients who achieve durable complete remissions likely have tumorswhich consist predominantly of cells of unusual sensitivity. What,however, is the mechanism underlying the temporary complete responses which are so common after HDC? One explanation could bethe survival of highly resistant subpopulations of cells in tumorscomposed of clones with heterogeneous patterns of drug resistance,following the chemotherapy-induced eradication of the more sensitivecells (6).
An alternative explanation, however, derives both from the study ofmathematical models of tumor growth kinetics (7) and from theclinical experience with other, more curable cancers. The development of successful treatment programs for lymphoma and testicularcancer has necessitated the identification of highly active regimensand the application of a minimum number of courses of those regimens (8, 9). It is thus reasonable to hypothesize that the optimal useof these very active high-dose regimens might require the administration of multiple treatment courses. The Norton-Simon model,moreover, predicts that massive, but noneradicative cytoreductionmight be followed by a phase of such accelerated regrowth of theminimal volumes of residual cancer cells that much of the advantageof multiple treatment courses might be undermined in the event oflengthy delays between these courses. In practice, the toxicity ofhigh-dose chemotherapy has complicated attempts to administer multiple courses (10) and has necessitated substantial treatment delayswhere it has been attempted (1 1, 12).
Because myeloid recovery is a common rate-limiting step in chemotherapy treatment schedules and is a principal determinant of morbidity, a possible role for hematopoietic growth factors in dose escalation and schedule intensification has been studied. While thesefactors have facilitated intensification of chemotherapy with cyclophosphamide, etoposide, and some other agents (13—15),attempts toincrease the intensity of delivery of more profoundly myelosuppressive agents, e.g., carboplatin and thiotepa, have been limited bythrombocytopenia and cumulative myelosuppression (16, 17).
The colony-stimulating factors also mobilize hematopoietic progenitor cells into the peripheral blood, and it is possible to harvest
3 The abbreviations used are: HDC, very-high-dose chemotherapy; PBP, peripheral
blood progenitors; G-CSF, granulocyte-colony-stimulating factor.
6137
Simultaneous Dose Escalation and Schedule Intensification of Carboplatin-based
Chemotherapy Using Peripheral Blood Progenitor Cells and Filgrastim:A Phase I Trial1
David Fennelly, Carolyn Wasserheit, Jeffrey Schneider, Thomas Hakes, Lillian Reich, John Curtin, T. J. Yao,Maurie Markman, Larry Norton, and John Crown2
Breast and Gynecologic Cancer Medicine Service, Department of Medicine, Gynecology Service, Department of Surgery. and Department of Biostatistics. Memorial SloanKettering Cancer Center, New York, New York 10021
on July 10, 2018. © 1994 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
DOSE ESCALATION/SCHEDULE INTENSIFICATION AND CARBOPLATIN
CARBOPLATINDOSE•l000mg/m2
PBP PBP PBP PBP
I @‘I@ hi7
LLLL LLLL
IJt12
v'@_―•o246810CTXCTXCBDCA
CTXCBDCACIXCBDCA CIXCBDCACTX3g/m23g/m21.5g/m1.SgIm1.6g/m1.5g/m
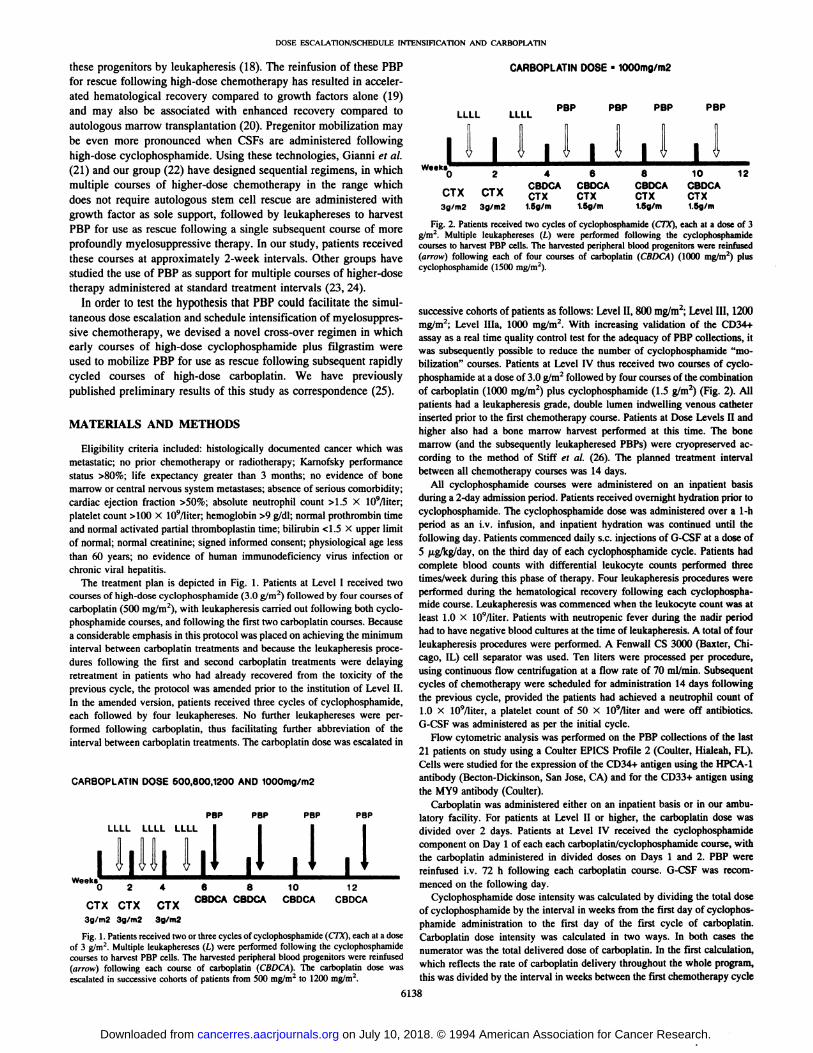
Fig. 2. Patients received two cycles of cyclophosphamide (CIX), each at a dose of 3g/m2. Multiple leukaphereses (L) were performed following the cyclophosphamidecourses to harvest PBP cells. The harvested peripheral blood progenitors were reinfused(arrow) following each of four courses of carboplatin (CBDCA) (1000 mg/rn2) pluscyclophosphamide (1500 mg/rn2).
successive cohorts of patients as follows: Level II, 800 mg/m2;Level III, 1200mg/m2; Level lila, 1000 mg/m2. With increasing validation of the CD34+assay as a real time quality control test for the adequacy of PBP collections, itwas subsequently possible to reduce the number of cyclophosphamide “mobilization―courses. Patients at Level IV thus received two courses of cyclophosphamide at a dose of 3.0 g/m2 followed by four courses of the combination
of carboplatin (1000 mg/m2) plus cyclophosphamide (1.5 g/m2) (Fig. 2). Allpatients had a leukapheresis grade, double lumen indwelling venous catheterinserted prior to the first chemotherapy course. Patients at Dose Levels II andhigher also had a bone marrow harvest performed at this time. The bonemarrow (and the subsequently leukapheresed PBPs) were cryopreserved according to the method of Stiff et a!. (26). The planned treatment intervalbetween all chemotherapy courses was 14 days.
All cyclophosphamide courses were administered on an inpatient basisduring a 2-day admission period. Patients received overnight hydration prior tocyclophosphamide. The cyclophosphamide dose was administered over a 1-hperiod as an iv. infusion, and inpatient hydration was continued until thefollowing day. Patients commenced daily s.c. injections of G-CSF at a dose of
5 @.tgfkg/day,on the third day of each cyclophosphamide cycle. Patients hadcomplete blood counts with differential leukocyte counts performed threetimes/week during this phase of therapy. Four leukapheresis procedures wereperformed during the hematological recovery following each cyclophospha
mide course. Leukapheresis was commenced when the leukocyte count was atleast 1.0 x 109/liter.Patients with neutropenic fever during the nadir periodhad to have negative blood cultures at the time of leukapheresis.A total of fourleukapheresis procedures were performed. A Fenwall CS 3000 (Baxter, Chicago, IL) cell separator was used. Ten liters were processed per procedure,using continuous flow centrifugation at a flow rate of 70 mI/mm. Subsequentcycles of chemotherapy were scheduled for administration 14 days followingthe previous cycle, provided the patients had achieved a neutrophil count of1.0 x lO9Iliter, a platelet count of 50 X l09lliter and were off antibiotics.G-GSF was administered as per the initial cycle.
Flow cytometric analysis was performed on the PBP collections of the last21 patients on study using a Coulter EPICS Profile 2 (Coulter, Hialeah, FL).Cells were studied for the expression of the CD34+ antigen using the HPCA-1antibody (Becton-Dickinson, San Jose, CA) and for the CD33+ antigen using
the MY9 antibody (Coulter).Carboplatin was administered either on an inpatient basis or in our ambu
latory facility. For patients at Level II or higher, the carboplatin dose wasdivided over 2 days. Patients at Level IV received the cyclophosphamidecomponent on Day 1 of each each carboplatin/cyclophosphamidecourse, withthe carboplatin administered in divided doses on Days 1 and 2. PBP werereinfused iv. 72 h following each carboplatin course. G-CSF was recom
10 1 2 menced on the following day.
CBDCA CBDCA Cyclophosphamidedoseintensitywas calculatedby dividing the total doseof cyclophosphamide by the interval in weeks from the first day of cyclophosphamide administration to the first day of the first cycle of carboplatin.Carboplatin dose intensity was calculated in two ways. In both cases thenumerator was the total delivered dose of carboplatin. In the first calculation,which reflects the rate of carboplatin delivery throughout the whole program,this was divided by the interval in weeks between the first chemotherapy cycle
these progenitors by leukapheresis (18). The reinfusion of these PBPfor rescue following high-dose chemotherapy has resulted in accelerated hematological recovery compared to growth factors alone (19)and may also be associated with enhanced recovery compared toautologous marrow transplantation (20). Pregenitor mobilization maybe even more pronounced when CSFs are administered followinghigh-dose cyclophosphamide. Using these technologies, Gianni et al.(21) and our group (22) have designed sequential regimens, in whichmultiple courses of higher-dose chemotherapy in the range whichdoes not require autologous stem cell rescue are administered withgrowth factor as sole support, followed by leukaphereses to harvestPBP for use as rescue following a single subsequent course of moreprofoundly myelosuppressive therapy. In our study, patients receivedthese courses at approximately 2-week intervals. Other groups havestudied the use of PBP as support for multiple courses of higher-dosetherapy administered at standard treatment intervals (23, 24).
In order to test the hypothesis that PBP could facilitate the simultaneous dose escalation and schedule intensification of myelosuppressive chemotherapy, we devised a novel cross-over regimen in whichearly courses of high-dose cyclophosphamide plus ifigrastim wereused to mobilize PBP for use as rescue following subsequent rapidlycycled courses of high-dose carboplatin. We have previouslypublished preliminary results of this study as correspondence (25).
MATERIALS AND METHODS
Eligibility criteria included: histologically documented cancer which was
metastatic; no prior chemotherapy or radiotherapy; Karnofsky performancestatus >80%; life expectancy greater than 3 months; no evidence of bonemarrow or central nervous system metastases; absence of serious comorbidity;
cardiac ejection fraction >50%; absolute neutrophil count >1.5 X l09lliter;platelet count >100 x 109/Iiter; hemoglobin >9 g/dl; normal prothrombin timeand normal activated partial thromboplastin time; bilirubin <1.5 X upper limitof normal; normal creatinine; signed informed consent; physiological age lessthan 60 years; no evidence of human immunodeficiency virus infection orchronic viral hepatitis.
The treatment plan is depicted in Fig. 1. Patients at Level I received twocourses of high-dose cyclophosphamide(3.0 g/m2)followed by four courses ofcarboplatin (500 mg/m2), with leukapheresis carried out following both cyclo
phosphamide courses, and following the first two carboplatin courses. Becausea considerable emphasis in this protocol was placed on achieving the minimuminterval between carboplatin treatments and because the leukapheresis procedures following the first and second carboplatin treatments were delaying
retreatment in patients who had already recovered from the toxicity of theprevious cycle, the protocol was amended prior to the institution of Level II.In the amended version, patients received three cycles of cyclophosphamide,each followed by four leukaphereses. No further leukaphereses were performed following carboplatin, thus facilitating further abbreviation of theinterval between carboplatin treatments. The carboplatin dose was escalated in
CARBOPLATIN DOSE 500,800,1200 AND l000mg/m2
PBP PBP PBP PBPLLLL LLLL LLLL
I 7il'IfllJilir ii II 11,vv@•o 2 4 6 8
CTX CTX CTX CBDCA CBDCA
3g/rn2 3g/m2 3g/m2
Fig. 1. Patients received two or three cycles of cyclophosphamide (CTh'), each at a doseof 3 g/m2. Multiple leukaphereses (L) were performed following the cyclophosphamidecourses to harvest PBP cells. The harvested peripheral blood progenitors were reinfused(arrow) following each course of carboplatin (CBDCA). The carboplatin dose wasescalated in successive cohorts of patients from 500 mg/m2 to 1200 mg/rn2.
6138
I@
on July 10, 2018. © 1994 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
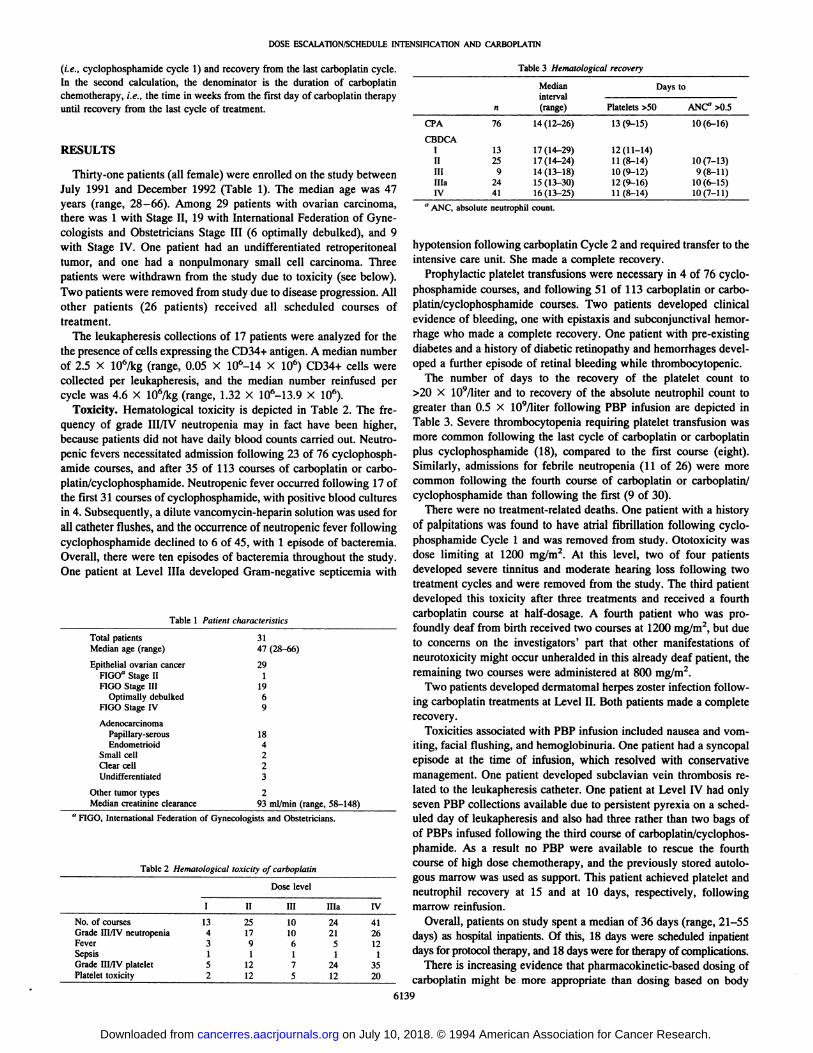
Table 3 HematologicalrecoverynMedian
interval(range)Days
toPlatelets
>50ANC―>0.5CPA7614(12—26)13(9—iS)10(6—16)CBDCA
IIIIIIlIlaIV
aANC,abso13
259
2441
lute neutr17(14—29)
17(14—24)14 (13—18)15 (13—30)16(13—25)
ophil count.12
(11—14)11(8—14)10 (9—12)12 (9—16)11(8—14)10(7—13)
9(8-11)10 (6—15)10(7—11)
Table 1 PatientcharacteristicsTotal
patients31Medianage (range) 47(28—66)Epithelial
ovarian cancer29FIGO―Stage II1FIGO
Stage III19Optimallydebulked6FIGO
Stage IV9AdenocarcinomaPapillary-serous
18Endometrioid4Small
cell2Clearcell2Undifferentiated
3Other
tumor types2Mediancreatinine clearance 93 mI/mm (range,58-148)a
HGO International Federation of Gynecologists andObstetricians.Table
2 Hematological toxicity ofcarboplatinDose
levelI
II IIIlIlaIVNo.
of courses 13 25 102441GradeIII/IV neutropenia 4 17 102126Fever
3 9 6512Sepsis1 1 111Grade
III/IV platelet 5 12 72435Platelettoxicity 2 12 5 1220
DOSE ESCALA110N/SCHEDULE INTENSIFICATIONAND CARBOPLATIN
(i.e., cyclophosphamide cycle 1) and recovery from the last carboplatin cycle.In the second calculation, the denominator is the duration of carboplatinchemotherapy, i.e., the time in weeks from the first day of carboplatin therapyuntil recovery from the last cycle of treatment.
RESULTS
Thirty-one patients (all female) were enrolled on the study betweenJuly 1991 and December 1992 (Table 1). The median age was 47years (range, 28—66). Among 29 patients with ovarian carcinoma,there was 1 with Stage II, 19 with International Federation of Gynecologists and Obstetricians Stage III (6 optimally debulked), and 9with Stage IV. One patient had an undifferentiated retroperitonealtumor, and one had a nonpulmonary small cell carcinoma. Threepatients were withdrawn from the study due to toxicity (see below).Two patients were removed from study due to disease progression. Allother patients (26 patients) received all scheduled courses oftreatment.
The leukapheresis collections of 17 patients were analyzed for thethe presence of cells expressing the CD34+ antigen. A median numberof 2.5 x 106/kg (range, 0.05 x 106_14 X 106) CD34+ cells werecollected per leukapheresis, and the median number reinfused percycle was 4.6 X 106/kg (range, 1.32 X 106_13.9 X 106).
Toxicity. Hematological toxicity is depicted in Table 2. The frequency of grade hilly neutropenia may in fact have been higher,because patients did not have daily blood counts carried out. Neutropenic fevers necessitated admission following 23 of 76 cyclophosphamide courses, and after 35 of 113 courses of carboplatin or carboplatin/cyclophosphamide. Neutropenic fever occurred following 17 ofthe first 31 courses of cyclophosphamide, with positive blood culturesin 4. Subsequently, a dilute vancomycin-heparin solution was used forall catheter flushes, and the occurrence of neutropenic fever followingcyclophosphamide declined to 6 of 45, with 1 episode of bacteremia.Overall, there were ten episodes of bacteremia throughout the study.One patient at Level lila developed Gram-negative septicemia with
hypotension following carboplatin Cycle 2 and required transfer to theintensive care unit. She made a complete recovery.
Prophylactic platelet transfusions were necessary in 4 of 76 cyclophosphamide courses, and following 51 of 113 carboplatin or carboplatin/cyclophosphamide courses. Two patients developed clinicalevidence of bleeding, one with epistaxis and subconjunctival hemorrhage who made a complete recovery. One patient with pre-existingdiabetes and a history of diabetic retinopathy and hemorrhages developed a further episode of retinal bleeding while thrombocytopenic.
The number of days to the recovery of the platelet count to>20 X 109/liter and to recovery of the absolute neutrophil count togreater than 0.5 x 109/liter following PBP infusion are depicted inTable 3. Severe thrombocytopenia requiring platelet transfusion wasmore common following the last cycle of carboplatin or carboplatinplus cyclophosphamide (18), compared to the first course (eight).Similarly, admissions for febrile neutropenia (1 1 of 26) were morecommon following the fourth course of carboplatin or carboplatin/cyclophosphamide than following the first (9 of 30).
There were no treatment-related deaths. One patient with a historyof palpitations was found to have atrial fibrillation following cyclophosphamide Cycle 1 and was removed from study. Ototoxicity wasdose limiting at 1200 mg/m2. At this level, two of four patientsdeveloped severe tinnitus and moderate hearing loss following twotreatment cycles and were removed from the study. The third patientdeveloped this toxicity after three treatments and received a fourthcarboplatin course at half-dosage. A fourth patient who was profoundly deaf from birth received two courses at 1200 mg/m2, but dueto concerns on the investigators' part that other manifestations ofneurotoxicity might occur unheralded in this already deaf patient, theremaining two courses were administered at 800 mg/m2.
Two patients developed dermatomal herpes zoster infection following carboplatin treatments at Level II. Both patients made a completerecovery.
Toxicities associated with PBP infusion included nausea and vomiting, facial flushing, and hemoglobinuria. One patient had a syncopalepisode at the time of infusion, which resolved with conservativemanagement. One patient developed subclavian vein thrombosis related to the leukapheresis catheter. One patient at Level IV had onlyseven PBP collections available due to persistent pyrexia on a scheduled day of leukapheresis and also had three rather than two bags ofof PBPs infused following the third course of carboplatin/cyclophosphamide. As a result no PBP were available to rescue the fourthcourse of high dose chemotherapy, and the previously stored autologous marrow was used as support. This patient achieved platelet andneutrophil recovery at 15 and at 10 days, respectively, followingmarrow reinfusion.
Overall, patients on study spent a median of 36 days (range, 21—55days) as hospital inpatients. Of this, 18 days were scheduled inpatientdays for protocol therapy, and 18 days were for therapy of complications.
There is increasing evidence that pharmacokinetic-based dosing ofcarboplatin might be more appropriate than dosing based on body
6139
on July 10, 2018. © 1994 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
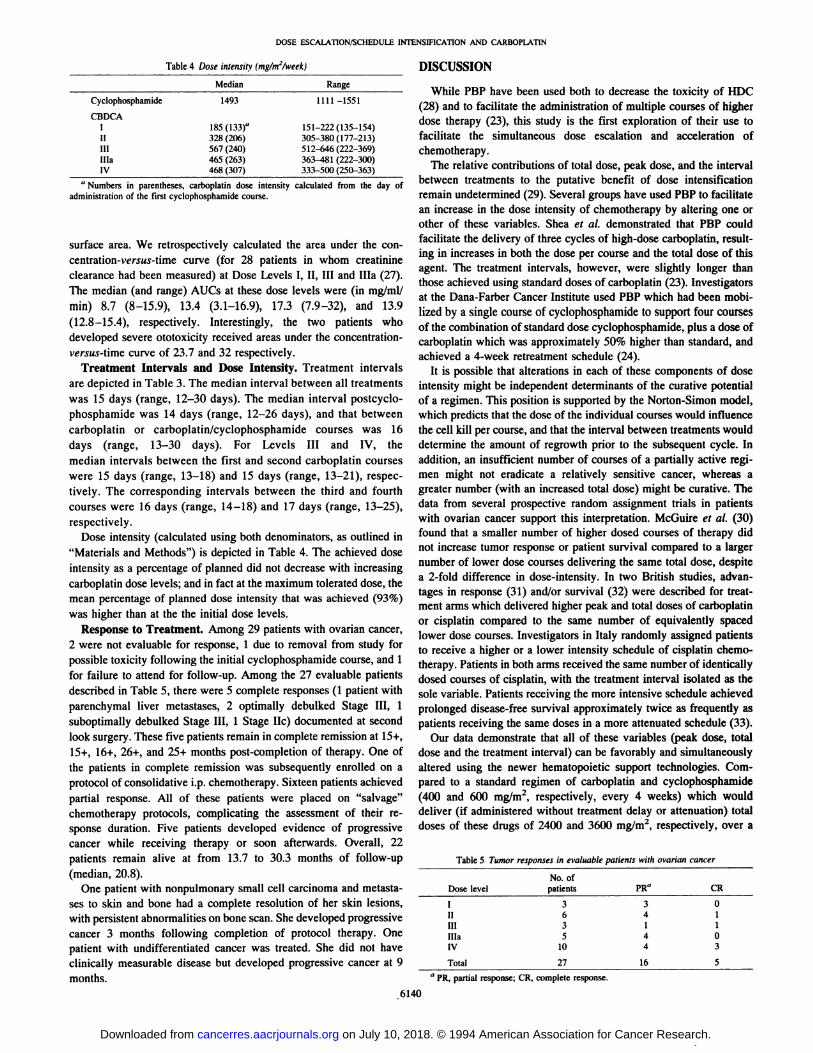
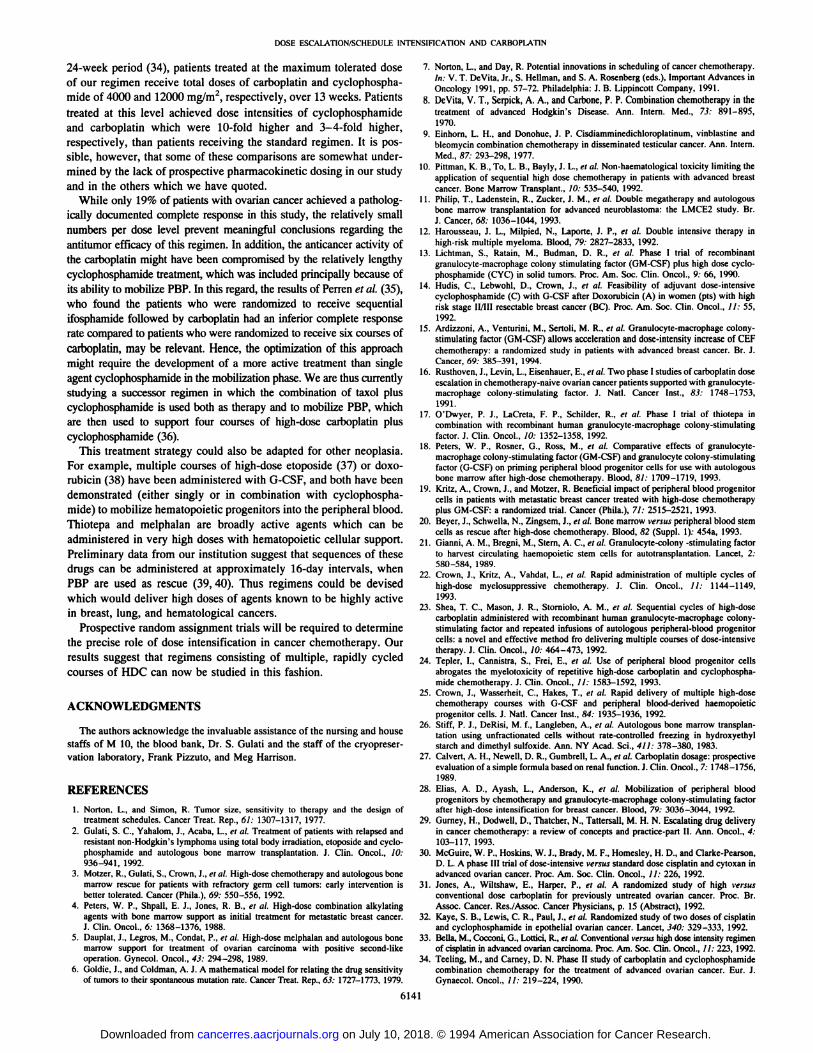
Table 4 Dose intensity(mg/m2/week)MedianRangeCyclophosphamide
14931111—1551CBDCA
I l85(133)aII 328 (206)III 567 (240)lIla 465 (263)IV 468 (307)151—222(135—154)
305-380 (177—213)512—646(222—369)363—481(222—300)
333—500(250—363)a
Numbersin parentheses,carboplatindoseintensityadministration of the first cyclophosphamide course.calculated
from the day of
Table 5Tumor responses in evaluable patients withovariancancerDose
levelNo.of
patientsPR―CRI
IIIIIlilaIv3
635103
41440
110
3Total27165a
PR,partialresponse;CR, complete response.
DOSE ESCALATION/SCHEDULEIN1ENSIFICATION AND CARBOPLATIN
surface area. We retrospectively calculated the area under the concentration-versus-time curve (for 28 patients in whom creatinineclearance had been measured) at Dose Levels I, II, III and lila (27).The median (and range) AUCS at these dose levels were (in mg/ml/mm) 8.7 (8—15.9),13.4 (3.1—16.9),17.3 (7.9—32),and 13.9(12.8—15.4), respectively. Interestingly, the two patients whodeveloped severe ototoxicity received areas under the concentrationversus-time curve of 23.7 and 32 respectively.
Treatment Intervals and Dose Intensity. Treatment intervalsare depicted in Table 3. The median interval between all treatmentswas 15 days (range, 12—30days). The median interval postcyclophosphamide was 14 days (range, 12—26days), and that betweencarboplatin or carboplatin/cyclophosphamide courses was 16days (range, 13—30 days). For Levels III and IV, themedian intervals between the first and second carboplatin courseswere 15 days (range, 13—18)and 15 days (range, 13—21),respectively. The corresponding intervals between the third and fourthcourses were 16 days (range, 14—18)and 17 days (range, 13—25),respectively.
Dose intensity (calculated using both denominators, as outlined in“Materialsand Methods―)is depicted in Table 4. The achieved doseintensity as a percentage of planned did not decrease with increasingcarboplatin dose levels; and in fact at the maximum tolerated dose, themean percentage of planned dose intensity that was achieved (93%)was higher than at the the initial dose levels.
Response to Treatment. Among 29 patients with ovarian cancer,2 were not evaluable for response, 1 due to removal from study forpossible toxicity following the initial cyclophosphamide course, and 1for failure to attend for follow-up. Among the 27 evaluable patientsdescribed in Table 5, there were 5 complete responses (1 patient withparenchymal liver metastases, 2 optimally debulked Stage III, 1suboptimally debulked Stage III, 1 Stage lic) documented at secondlook surgery. These five patients remain in complete remission at 15+,15+, 16+, 26+, and 25+ months post-completion of therapy. One ofthe patients in complete remission was subsequently enrolled on aprotocol of consolidative i.p. chemotherapy. Sixteen patients achievedpartial response. All of these patients were placed on “salvage―chemotherapy protocols, complicating the assessment of their response duration. Five patients developed evidence of progressivecancer while receiving therapy or soon afterwards. Overall, 22patients remain alive at from 13.7 to 30.3 months of follow-up(median, 20.8).
One patient with nonpulmonary small cell carcinoma and metastases to skin and bone had a complete resolution of her skin lesions,with persistent abnormalities on bone scan. She developed progressivecancer 3 months following completion of protocol therapy. Onepatient with undifferentiated cancer was treated. She did not haveclinically measurable disease but developed progressive cancer at 9months.
6140
DISCUSSION
While PBP have been used both to decrease the toxicity of HDC(28) and to facilitate the administration of multiple courses of higherdose therapy (23), this study is the first exploration of their use tofacilitate the simultaneous dose escalation and acceleration ofchemotherapy.
The relative contributions of total dose, peak dose, and the intervalbetween treatments to the putative benefit of dose intensificationremain undetermined (29). Several groups have used PBP to facilitatean increase in the dose intensity of chemotherapy by altering one orother of these variables. Shea et a!. demonstrated that PBP couldfacilitate the delivery of three cycles of high-dose carboplatin, resulting in increases in both the dose per course and the total dose of thisagent. The treatment intervals, however, were slightly longer thanthose achieved using standard doses of carboplatin (23). Investigatorsat the Dana-Farber Cancer Institute used PBP which had been mobilized by a single course of cyclophosphamide to support four coursesof the combination of standard dose cyclophosphamide, plus a dose ofcarboplatin which was approximately 50% higher than standard, andachieved a 4-week retreatment schedule (24).
It is possible that alterations in each of these components of doseintensity might be independent determinants of the curative potentialof a regimen. This position is supported by the Norton-Simon model,which predicts that the dose of the individual courses would influencethe cell kill per course, and that the interval between treatments woulddetermine the amount of regrowth prior to the subsequent cycle. Inaddition, an insufficient number of courses of a partially active regimen might not eradicate a relatively sensitive cancer, whereas agreater number (with an increased total dose) might be curative. Thedata from several prospective random assignment trials in patientswith ovarian cancer support this interpretation. McGuire et a!. (30)found that a smaller number of higher dosed courses of therapy didnot increase tumor response or patient survival compared to a largernumber of lower dose courses delivering the same total dose, despitea 2-fold difference in dose-intensity. In two British studies, advantages in response (31) and/or survival (32) were described for treatment arms which delivered higher peak and total doses of carboplatinor cisplatin compared to the same number of equivalently spacedlower dose courses. Investigators in Italy randomly assigned patientsto receive a higher or a lower intensity schedule of cisplatin chemotherapy. Patients in both arms received the same number of identicallydosed courses of cisplatin, with the treatment interval isolated as thesole variable. Patients receiving the more intensive schedule achievedprolonged disease-free survival approximately twice as frequently aspatients receiving the same doses in a more attenuated schedule (33).
Our data demonstrate that all of these variables (peak dose, totaldose and the treatment interval) can be favorably and simultaneouslyaltered using the newer hematopoietic support technologies. Compared to a standard regimen of carboplatin and cyclophosphamide(400 and 600 mg/m2, respectively, every 4 weeks) which woulddeliver (if administered without treatment delay or attenuation) totaldoses of these drugs of 2400 and 3600 mg/rn2, respectively, over a
on July 10, 2018. © 1994 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
DOSE ESCALATION/SCHEDULEINThNSIFICATION AND CARBOPLATIN
24-week period (34), patients treated at the maximum tolerated doseof our regimen receive total doses of carboplatin and cyclophosphamide of 4000 and 12000 mg/m2, respectively, over 13 weeks. Patients
treated at this level achieved dose intensities of cyclophosphamideand carboplatin which were 10-fold higher and 3—4-fold higher,respectively, than patients receiving the standard regimen. It is possible, however, that some of these comparisons are somewhat undermined by the lack of prospective pharmacokinetic dosing in our studyand in the others which we have quoted.
While only 19% of patients with ovarian cancer achieved a pathologically documented complete response in this study, the relatively smallnumbers per dose level prevent meaningful conclusions regarding theantitumor efficacy of this regimen. In addition, the anticancer activity ofthe carboplatin might have been compromised by the relatively lengthycyclophosphamide treatment, which was included principally because ofits ability to mobilize PBP. In this regard, the results of Perren et a!. (35),who found the patients who were randomized to receive sequentialifosphamide followed by carboplatin had an inferior complete response
rate compared to patients who were randomized to receive six courses ofcarboplatin, may be relevant. Hence, the optimization of this approachmight require the development of a more active treatment than singleagent cyclophosphamide in the mobilization phase. We are thus currentlystudying a successor regimen in which the combination of taxol pluscyclophosphamide is used both as therapy and to mobilize PBP, whichare then used to support four courses of high-dose carboplatin pluscyclophosphamide (36).
This treatment strategy could also be adapted for other neoplasia.For example, multiple courses of high-dose etoposide (37) or doxorubicin (38) have been administered with G-CSF, and both have beendemonstrated (either singly or in combination with cyclophosphamide) to mobilize hematopoietic progenitors into the peripheral blood.Thiotepa and melphalan are broadly active agents which can beadministered in very high doses with hematopoietic cellular support.Preliminary data from our institution suggest that sequences of thesedrugs can be administered at approximately 16-day intervals, whenPBP are used as rescue (39, 40). Thus regimens could be devisedwhich would deliver high doses of agents known to be highly activein breast, lung, and hematological cancers.
Prospective random assignment trials will be required to determinethe precise role of dose intensification in cancer chemotherapy. Ourresults suggest that regimens consisting of multiple, rapidly cycledcourses of HDC can now be studied in this fashion.
ACKNOWLEDGMENTS
The authors acknowledge the invaluable assistance of the nursing and housestaffs of M 10, the blood bank, Dr. S. Gulati and the staff of the cryopreservation laboratory, Frank Pizzuto, and Meg Harrison.
REFERENCES
1. Norton. L., and Simon, R. Tumor size, sensitivity to therapy and the design oftreatment schedules. Cancer Treat. Rep., 61: 1307—1317,1977.
2. Gulati,S. C.,Yahalom,J., Acaba,L.,et al. Treatmentof patientswithrelapsedandresistant non-Hodgkin's lymphoma using total body irradiation, etoposide and cyclophosphamide and autologous bone marrow transplantation. J. Gin. Oncol., 10:936—941, 1992.
3. Motzer, R., Gulati, S., Crown, J., et al. High-dose chemotherapy and autologous bonemarrow rescue for patients with refractory germ cell tumors: early intervention isbetter tolerated. Cancer (Phila.), 69: 550—556,1992.
4. Peters, W. P., Shpall, E. J., Jones, R. B., et al. High-dose combination alkylatingagents with bone marrow support as initial treatment for metastatic breast cancer.J. Clin. Oncol., 6: 1368—1376,1988.
5. Dauplat, J., Legros, M., Condat, P., et al. High-dose melphalan and autologous bonemarrow support for treatment of ovarian carcinoma with positive second-likeoperation. Gynecol. Oncol., 43: 294—298,1989.
6. Goldie, J., and Goldman, A. J. A mathematical model for relating the drug sensitivityof tumors to their spontaneousmutationrate. Cancer Treat. Rep., 63: 1727—1773,1979.
7. Norton, L., and Day, R. Potential innovations in scheduling of cancer chemotherapy.in: V. T. DeVita, Jr., S. Heilman, and S. A. Rosenberg (cdx.), Important Advances inOncology 1991, pp. 57—72.Philadelphia: J. B. Lippincott Company, 1991.
8. DeVita, V. T., Serpick, A. A., and Carbone, P. P. Combination chemotherapy in thetreatment of advanced Hodgkin's Disease. Ann. Intern. Med., 73: 891—895,1970.
9. Einhorn, L. H., and Donohue, J. P. Cisdiamminedichloroplatinum, vinblastine andbleomycin combination chemotherapy in disseminated testicular cancer. Ann. Intern.Med., 87: 293—298,1977.
10. Pittman, K. B., To, L. B., Bayly, J. L., et al. Non-haematological toxicity limiting theapplication of sequential high dose chemotherapy in patients with advanced breastcancer. Bone Marrow Transplant., 10: 535—540,1992.
11. Philip, T., Ladenstein, R., Zucker, J. M., et al. Double megatherapy and autotogousbone marrow transplantation for advanced neuroblastoma: the LMCE2 study. Br.J. Cancer, 68: 1036—1044,1993.
12. Harousseau, J. L., Milpied, N., Laporte, J. P., et al. Double intensive therapy inhigh-risk multiple myeloma. Blood, 79: 2827—2833,1992.
13. Lichtman, S., Ratain, M., Budman, D. R., et al. Phase I trial of recombinantgranulocyte-macrophage colony stimulating factor (GM-CSF) plus high dose cyclophosphamide (CYC) in solid tumors. Proc. Am. Soc. Clin. Oncol., 9: 66, 1990.
14. Hudis, C., Lebwohl, D., Crown, J., et aL Feasibility of adjuvant dose-intensivecyclophosphamide (C) with G-CSF after Doxorubicin (A) in women (pts) with highrisk stage Il/Ill resectable breast cancer (BC). Proc. Am. Soc. Clin. Oncol., I 1: 55,1992.
15. Ardizzoni, A., Venturini, M., Sertoli, M. R., et al. Granulocyte-macrophage colonystimulating factor (GM-CSF) allows acceleration and dose-intensity increase of CEFchemotherapy: a randomized study in patients with advanced breast cancer. Br. J.Cancer, 69: 385—391,1994.
16. Rusthoven, J., Levin, L., Eisenhauer, E., et al. Two phase I studies of carboplatin doseescalation in chemotherapy-nalve ovarian cancer patients supported with granulocytemacrophage colony-stimulating factor. J. NatI. Cancer Inst., 83: 1748—1753,1991.
17. O'Dwyer, P. J., LaCreta, F. P., Schilder, R., et a!. Phase I trial of thiotepa incombination with recombinant human granulocyte-macrophage colony-stimulatingfactor. J. Clin. Oncol., 10: 1352—1358,1992.
18. Peters, W. P., Rosner, G., Ross, M., et al. Comparative effects of granulocytemacrophage colony-stimulating factor (GM-CSF) and granulocyte colony-stimulatingfactor (G-CSF) on priming peripheral blood progenitor cells for use with autologousbone marrow after high-dose chemotherapy. Blood, 81: 1709—1719,1993.
19. Kritz, A., Crown, J., and Motzer, R. Beneficial impact ofperipheral blood progenitorcells in patients with metastatic breast cancer treated with high-dose chemotherapyplus GM-CSF: a randomized trial. Cancer (Phila.), 71: 2515—2521, 1993.
20. Beyer, J., Schwella, N., Zingsem, J., et a!. Bone marrow versus peripheral blood stemcells as rescue after high-dose chemotherapy. Blood, 82 (Suppl. 1): 454a, 1993.
21. Gianni, A. M., Bregni, M., Stern, A. C., et al. Granulocyte-colony -stimulating factorto harvest circulating haemopoietic stem cells for autotransplantation. Lancet, 2:580—584,1989.
22. Crown, J., Kritz, A., Vahdat, L., et a!. Rapid administration of multiple cycles ofhigh-dose myelosuppressive chemotherapy. J. Clin. Oncol., I I: I 144—1149,1993.
23. Shea, T. C., Mason, J. R., Storniolo, A. M., et al. Sequential cycles of high-dosecarboplatin administered with recombinant human granulocyte-macrophage colonystimulating factor and repeated infusions of autologous peripheral-blood progenitorcells: a novel and effective method fro delivering multiple courses of dose-intensivetherapy. J. Chin. Oncol., 10: 464—473, 1992.
24. Tepler, I., Cannistra, S., Frei, E., ci aL Use of peripheral blood progenitor cellsabrogates the myelotoxicity of repetitive high-dose carboplatin and cyclophosphamide chemotherapy. J. Clin. Oncol., 11: 1583—1592,1993.
25. Crown, J., Wasserheit, C., Hakes, T., ci al. Rapid delivery of multiple high-dosechemotherapy courses with G-GSF and peripheral blood-derived haemopoieticprogenitor cells. J. Natl. Cancer Inst., 84: 1935—1936,1992.
26. Stiff, P. J., DeRisi, M. f., Langieben, A., ci aL Autologous bone marrow transplantation using unfractionated cells without rate-controlled freezing in hydroxyethylstarch and dimethyl sulfoxide. Ann. NY Acad. Sci., 411: 378—380, 1983.
27. Calvert, A. H., Newell, D. R., Gumbrell, L. A., et al. Carboplatin dosage: prospectiveevaluation of a simple formula based on renal function. J. Clin. Oncol., 7: 1748—1756,1989.
28. Elias, A. D., Ayash, L., Anderson, K., ci al. Mobilization of peripheral bloodprogenitors by chemotherapy and granulocyte-macrophage colony-stimulating factorafter high-dose intensification for breast cancer. Blood, 79: 3036-3044, 1992.
29. Gurney, H., Dodwell, D., Thatcher, N., Tattersall, M. H. N. Escalating drug deliveryin cancer chemotherapy: a review of concepts and practice-part II. Ann. Oncol., 4:103—117,1993.
30. McGuire, W. P., Hoskins, W. J., Brady, M. F., Homesley, H. D., and Clarke-Pearson,D. L. A phase III trial of dose-intensive versus standard dose cisplatin and cytoxan inadvanced ovarian cancer. Proc. Am. Soc. Clin. Oncol., 11: 226, 1992.
31. Jones, A., Wiltshaw, E., Harper, P., ci al. A randomized study of high versusconventional dose carboplatin for previously untreated ovarian cancer. Proc. Br.Assoc. Cancer. Res./Assoc. Cancer Physicians, p. 15 (Abstract), 1992.
32. Kaye, S. B., Lewis, C. R., Paul, J., ci aL Randomized study of two doses of cisplatinand cyclophosphamide in epothelial ovarian cancer. Lancet, 340: 329—333, 1992.
33. Bells, M., Cocconi, G., Lottici, It, ci aL Conventional versus high dose intensity regimenof cisplatinin advancedovariancarcinoma.Proc. Am. Soc. Chin.Oncol., 11: 223, 1992.
34. Teeling, M., and Carney, D. N. Phase II study of carboplatin and cyclophosphamidecombination chemotherapy for the treatment of advanced ovarian cancer. Eur. J.Gynaecol. Oncol., 11: 219—224,1990.
6141
on July 10, 2018. © 1994 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

DOSE ESCALATION/SCHEDULEINTENSIFICATIONAND CARBOPLATIN
35. Perren, 1. J., Wltshaw, E., Harper, P., ci a!. A randomized study of carboplatin versussequential ifospharnide/carboplatin for patients with FIGO stage III epithelial ovariancancer. Br. J. Cancer, 68: 1190—1194, 1993.
36. Crown, J., Fennelly, D., Schneider, J., et al. Escalating dose taxol + high-dosecyclophosphamide/G-CSF as induction and to mobilize peripheral blood progenitorsfor use as rescue following multiple courses of high-dose carboplatin: a phase I trialin ovarian cancer patients. Proc. Am. Soc. Clin. Oncol., /3: 262, 1994.
37. Gianni, A. M., Bregni, M., Siena, S., Magni, M., ci a!. Granulocyte-macrophagecolony-stimulating factor or granulocyte colony-stimulating factor infusion makeshigh-dose etoposide a safe outpatient regimen that is effective in lymphoma andmyeloma patients. J. Clin. Oncol., 10: 1955—1962,1992.
38. Dodwell, D., Ferguson, J., Howell, A., ci al. Intensification of Adriamycin andcyclophosphamide treatment for advanced breast cancer with subcutaneous G-f@SF:identification of optimal time to collect peripheral blood stem cells. Proc. Am. Soc.Clin. Oncol., 10: 56, 1991.
39. Crown, J., Vahdat, L., Raptis, 0., ci al. Rapidly cycled courses of high-dose chemotherapy supported by fllgrastim and peripheral blood progenitor cells in patients withmetastaticbreastcancer.Proc.Am.Soc.Clin.Oncol.,13: 110,1994.
40. Crown, J., Raptis, G., Vahdat, L., ci al. Rapid administration of sequential high-dosecyclophospharnide, meiphalan, thiotepa supported by fllgrastim and peripheral bloodprogenitorsinpatientswithmetastaticbreastcancer:a novelandveryactivetreatmentstrategy. Proc. Am. Soc. Clin. Oncol., 13: 110, 1994.
6142
on July 10, 2018. © 1994 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1994;54:6137-6142. Cancer Res David Fennelly, Carolyn Wasserheit, Jeffrey Schneider, et al. Progenitor Cells and Filgrastim: A Phase I TrialCarboplatin-based Chemotherapy Using Peripheral Blood Simultaneous Dose Escalation and Schedule Intensification of
Updated version
http://cancerres.aacrjournals.org/content/54/23/6137
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/54/23/6137To request permission to re-use all or part of this article, use this link
on July 10, 2018. © 1994 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from





























