Embed Size (px)
Citation preview

lopidogrel in lopidogrel in nstable Anginanstable Anginato Preventto Prevent ecurrentecurrent ventsvents

DisclaimerDisclaimer
This slide kit presents new data to support the rationale for This slide kit presents new data to support the rationale for the use of ADP receptor antagonists for approved and the use of ADP receptor antagonists for approved and unapproved indications. unapproved indications.
The slide kit has been prepared for medical and scientific The slide kit has been prepared for medical and scientific purposes. It contains information on a use that is not purposes. It contains information on a use that is not approved by the FDA and should not be construed as an approved by the FDA and should not be construed as an inducement to use clopidogrel for unapproved indications. inducement to use clopidogrel for unapproved indications. Neither Sanofi-Synthelabo Inc., Bristol-Myers Squibb nor Neither Sanofi-Synthelabo Inc., Bristol-Myers Squibb nor the partnership recommends the use of clopidogrel in any the partnership recommends the use of clopidogrel in any manner inconsistent with that described in the full manner inconsistent with that described in the full prescribing information.prescribing information.

CURE
CURE Study Investigators. Eur Heart J. 2000;21:2033-2041.PURSUIT Investigators. Am J Cardiol. 1999;83:1147-1151.
RationaleRationale
Despite treatment with aspirin and heparin, the incidence of Despite treatment with aspirin and heparin, the incidence of MI and CV death during hospitalization remains high, MI and CV death during hospitalization remains high, 6-8% 6-8%
Long term, the incidence of these events remain high at Long term, the incidence of these events remain high at 6-8% per year 6-8% per year
The majority of patients (80%) who enter the hospital with The majority of patients (80%) who enter the hospital with acute coronary syndrome (ACS) are already on aspirin acute coronary syndrome (ACS) are already on aspirin therapytherapy
The negative findings of the oral GP IIb/IIIa’s underscores The negative findings of the oral GP IIb/IIIa’s underscores the need for alternative strategies to treat ACS the need for alternative strategies to treat ACS

CURE
CURE Study Investigators. Eur Heart J. 2000; 21:2033-2041.
Study ObjectivesStudy Objectives
PrimaryPrimaryEvaluate the early and long-term efficacy of Evaluate the early and long-term efficacy of
clopidogrel vs placebo, both given in addition to aspirin clopidogrel vs placebo, both given in addition to aspirin and other standard therapy in preventing ischemic and other standard therapy in preventing ischemic complications in patients with ACS without ST-complications in patients with ACS without ST-segment elevation (unstable angina or non-ST-segment elevation (unstable angina or non-ST-segment elevation MI) segment elevation MI)
SecondarySecondaryEvaluate the safety of clopidogrel in combination with Evaluate the safety of clopidogrel in combination with
ASA therapy in patients with ACSASA therapy in patients with ACS

CURE
Clopidogrel 75mg q.d. + ASA 75-325 mg q.d.*
(6259 patients)
Placebo + ASA 75-325 mg q.d.*(6303 patients)
Day
1
6 m
. Vis
it
9 m
. Vis
it
12 m
.
or F
inal
Vis
it
3 m
. Vis
it
Dis
char
ge V
isit
1 m
. Vis
it
Patients withAcute Coronary
Syndrome
(unstable angina or non-ST-segment
elevation MI)
RR
Plac
ebo
load
ing
dose
R = Randomization* In combination with other standard therapy The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Study DesignStudy Design
3 months double-blind treatment 12 months3 months double-blind treatment 12 months
Clopidogrel 300 mg loading dose

CURE
1 CURE Study Protocol (Data on file, Sanofi-Synthelabo, Inc.)2 CURE Study Investigators. Eur Heart J. 2000; 21:2033-2041.
Key Inclusion Criteria Key Inclusion Criteria
Age Age 21 years 21 years11
Suspected UA or NSTEMI (no ST Suspected UA or NSTEMI (no ST 1.0 mm) 1.0 mm)22
Presentation Presentation 24 hours after onset of symptoms 24 hours after onset of symptoms22
ECG changes compatible with ischemia or elevated ECG changes compatible with ischemia or elevated cardiac enzymes or troponin I or T cardiac enzymes or troponin I or T 2 x ULN 2 x ULN22

CURE
1 CURE Study Investigators. Eur Heart J. 2000; 21:2033-2041.2 CURE Study Protocol (Data on file, Sanofi-Synthelabo, Inc.)
Key Exclusion CriteriaKey Exclusion Criteria
NYHA Class IV heart failureNYHA Class IV heart failure11
Uncontrolled hypertensionUncontrolled hypertension22
Current use of anticoagulantsCurrent use of anticoagulants11, clopidogrel, ticlopidine, , clopidogrel, ticlopidine, or NSAIDS2, or GP IIb/IIIa inhibitor within 3 daysor NSAIDS2, or GP IIb/IIIa inhibitor within 3 days11
PCI or CABG within 3 monthsPCI or CABG within 3 months11
History of severe thrombocytopenia or neutropeniaHistory of severe thrombocytopenia or neutropenia22
At high risk for bleedingAt high risk for bleeding11
Contraindications to antithrombotic or antiplatelet therapyContraindications to antithrombotic or antiplatelet therapy11

CURE
Outcome Definitions Outcome Definitions MI:MI: At least two of the following criteria: chest pain, ECG changes, elevation At least two of the following criteria: chest pain, ECG changes, elevation of cardiac markers or enzymes (Troponin, CK, CK-MB) of cardiac markers or enzymes (Troponin, CK, CK-MB)Stroke:Stroke: Neurological deficit Neurological deficit 24 hrs (CT/MRI encouraged) 24 hrs (CT/MRI encouraged)CV Death:CV Death: Excludes any death for which there was no clearly documented non-CV causeExcludes any death for which there was no clearly documented non-CV causeRefractory Ischemia:Refractory Ischemia: In-hosp: recurrent ischemia on max med Rx + ECG changes + intervention In-hosp: recurrent ischemia on max med Rx + ECG changes + intervention
1 day 1 day After discharge: Rehosp for UA with ECG changesAfter discharge: Rehosp for UA with ECG changesSevere Ischemia:Severe Ischemia: Changes similar to in-hospital refractory ischemia, but no interventionChanges similar to in-hospital refractory ischemia, but no interventionRecurrent Angina:Recurrent Angina: All other ischemic chest pain in hospitalAll other ischemic chest pain in hospital
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.

CURE
Efficacy AnalysesEfficacy Analyses
First Primary End PointFirst Primary End PointFirst occurrence of any component of the cluster of:First occurrence of any component of the cluster of:
– Myocardial InfarctionMyocardial Infarction
– Stroke (ischemic, hemorrhagic, or of uncertain type)Stroke (ischemic, hemorrhagic, or of uncertain type)
– Cardiovascular deathCardiovascular death
Second Primary End PointSecond Primary End PointFirst occurrence of any component of the cluster of:First occurrence of any component of the cluster of:
– Myocardial InfarctionMyocardial Infarction
– Stroke (ischemic, hemorrhagic, or of uncertain type)Stroke (ischemic, hemorrhagic, or of uncertain type)
– Cardiovascular deathCardiovascular death
– Refractory ischemiaRefractory ischemia
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.

CURE
Age (mean) 64.2 64.2
Mean time from pain onset to randomization (hrs) 14.1 14.2
Mean heart rate (beats/min) 73.0 73.2
Mean systolic BP (mm Hg) 134.1 134.4
Female (%) 38.3 38.7
Diagnosis at Entry
Unstable Angina (%) 74.9 74.9
Non–ST-segment elevation MI (%) 25.1 25.1
ECG abnormalities (%) 93.9 93.7
PlaceboN = 6303
ClopidogrelN = 6259
Baseline CharacteristicsBaseline Characteristics
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.

CURE
History of MI 32.0 32.4
CABG Surgery/PTCA 18.1 17.7
Stroke 3.7 4.4
Heart Failure 7.8 7.4
Hypertension 57.8 59.9
Diabetes 22.8 22.4
Current or former smoker 60.9 60.6
PlaceboN = 6303
(%)
ClopidogrelN = 6259
(%)
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Patient HistoryPatient History

CURE
History Abnormal ECG 93.9 93.7
ST-segment Dep > 1 mm 42.0 42.2
ST-segment elevation < 1 mm 3.2 3.2
Major T-wave inversion 25.9 25.4
Other T-wave inversion 11.3 11.5
Other abnormalities 10.9 10.7
Placebo(%)
Clopidogrel(%)
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
ECG Abnormality Type ECG Abnormality Type

CURE
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
Cu
mu
lati
ve H
azar
d R
ate
Clopidogrel Clopidogrel + ASA*+ ASA*
33 66 99
Placebo Placebo + ASA*+ ASA*
Months of Follow-UpMonths of Follow-Up
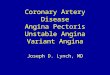
11.4%11.4%
9.3%9.3%
20% RRR20% RRRPP < 0.001 < 0.001
N = 12,562N = 12,562
00 1212
* In combination with standard therapy
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Primary End Point - MI/Stroke/CV DeathPrimary End Point - MI/Stroke/CV Death

CURE
0.00
0.01
0.02
0.03
0.04
0.05
0.06
Cu
mu
lati
ve H
azar
d R
ate
Clopidogrel Clopidogrel + ASA*+ ASA*
1010 2020 3030
Placebo Placebo + ASA*+ ASA*
Days of Follow-UpDays of Follow-Up
00
21% RRR21% RRRPP = 0.003 = 0.003
N = 12,562N = 12,562
* In combination with standard therapy
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
MI/Stroke/CV Death within 30 DaysMI/Stroke/CV Death within 30 Days

CURE
CV death, MI, stroke (Primary 11.4% 9.3% 20%
< 0.001end point)
MI 6.7% 5.2% 23%
Stroke 1.4% 1.2% 14%
CV death 5.5% 5.1% 7%
Relative Risk
Reduction P valueOutcome
Placebo + ASA*
N = 6303
Clopidogrel + ASA*
N = 6259
* In combination with standard therapy
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Main Efficacy Results - Primary EndpointMain Efficacy Results - Primary Endpoint

CURE
RRR P valueEnd PointPlacebo + ASA*
Clopidogrel + ASA*
Main Efficacy Results - Main Efficacy Results - Second Primary End PointSecond Primary End Point
* In combination with standard therapy** Not significant† Heart failure was a secondary end point
Second Primary End PointSecond Primary End Point 18.8%18.8% 16.5%16.5% 14%14% < 0.001< 0.001
Refractory IschemiaRefractory Ischemia 9.3%9.3% 8.7%8.7% 7%7% NS**NS**
– Refractory IschemiaRefractory Ischemiain hospitalin hospital 2.0%2.0% 1.4%1.4% 32%32% PP < 0.001 < 0.001
– Refractory Ischemia Refractory Ischemia after dischargeafter discharge 7.6%7.6% 7.6%7.6% 1%1% NS**NS**
Severe IschemiaSevere Ischemia 3.8%3.8% 2.8%2.8% 26%26% PP = 0.003 = 0.003
Recurrent IschemiaRecurrent Ischemia 22.9%22.9% 20.9%20.9% 9%9% PP = 0.01 = 0.01
Heart FailureHeart Failure†† 4.4%4.4% 3.7%3.7% 18%18% PP = 0.03 = 0.03
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.

CURE
Overall 12562 9.3 11.4
Associated MI 3283 11.3 13.7No associated MI 9279 8.6 10.6
Male sex 7726 9.1 11.9Female sex 4836 9.5 10.7
65 yr old 6354 5.4 7.665 yr old 6208 13.3 15.3
ST-segment deviation 6275 11.5 14.3No ST-segment deviation 6287 7.0 8.6
Enzymes elevated at entry 3176 10.7 13.0Enzymes not elevated at entry 9386 8.8 10.9
Diabetes 2840 14.2 16.7No diabetes 9722 7.9 9.9
Low risk 4187 5.1 6.7Intermediate risk 4185 6.5 9.4High risk 4184 16.3 18.0
History of revascularization 2246 8.4 14.4No history of revascularization 10316 9.5 10.7
Revascularization after randomization 4577 11.5 13.9No revascularization after randomization 7985 8.1 10.0
Placebo + ASA*Characteristic
No. ofPatients
Clopidogrel + ASA*
Percentage of Patients with Event
Placebo BetterClopidogrel Better
Relative Risk (95% CI)
1.21.00.80.60.4* In combination with standard therapy
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Beneficial Outcomes with Clopidogrel in Beneficial Outcomes with Clopidogrel in Various SubgroupsVarious Subgroups

CURE
Relative Risk
Reduction P value
Placebo + ASA*
N = 6303
Clopidogrel + ASA*
N = 6259
ThrombolyticsThrombolytics 2.0%2.0% 1.1%1.1% 43%43% 0.43-0.76 0.43-0.76 < < 0.0010.001
IV GP IIb/IIIa InhibIV GP IIb/IIIa Inhib 7.2%7.2% 5.9%5.9% 18%18% 0.72-0.93 0.72-0.930.0030.003
CI
* As part of standard therapy
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Thrombolytic and IV GP IIb/IIIa Inhibitor Thrombolytic and IV GP IIb/IIIa Inhibitor Use After RandomizationUse After Randomization

CURE
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Definition of BleedingDefinition of Bleeding
Bleeding was defined as “Major” and “Minor”Bleeding was defined as “Major” and “Minor”
Major bleeding was defined as follows:Major bleeding was defined as follows: life threatening: fatal, symptomatic intracranial hemorrhage, life threatening: fatal, symptomatic intracranial hemorrhage,
leading to a drop in hemoglobin of at least 5 g/dL, significant leading to a drop in hemoglobin of at least 5 g/dL, significant hypotention requiring IV inotropes, requiring surgical hypotention requiring IV inotropes, requiring surgical intervention, or requiring transfusion of 4 or more units of bloodintervention, or requiring transfusion of 4 or more units of blood
non-life-threatening: substantially disabling, intraocular bleeding non-life-threatening: substantially disabling, intraocular bleeding leading to vision loss, or requiring at least 2 units of bloodleading to vision loss, or requiring at least 2 units of blood
Minor Minor any other bleeds that led to interruption of study medicationany other bleeds that led to interruption of study medication

CURE
Placebo + ASA*
N = 6303
Clopidogrel + ASA*
N = 6259
Major bleedingMajor bleeding 2.7%2.7% 3.7%**3.7%**
Life-threatening bleedingLife-threatening bleeding 1.8%1.8% 2.2% 2.2% ††
Non-life-threatening bleedingNon-life-threatening bleeding 0.9%0.9% 1.5% 1.5% ‡‡
Minor bleedingMinor bleeding 2.4%2.4% 5.1% 5.1% §§
End Point
* In combination with standard therapy
** P = 0.001; † P = NS; ‡ P = 0.002; § P < 0.001.
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Bleeding ResultsBleeding Results

CURE
Life-ThreateningLife-Threatening 1.81.8 2.22.2
FatalFatal 0.20.2 0.20.2
5 g/dL drop hemoglobin5 g/dL drop hemoglobin 0.90.9 0.90.9
Hypotension-inotropic therapyHypotension-inotropic therapy 0.50.5 0.50.5
Surgery requiredSurgery required 0.70.7 0.70.7
Hemorrhagic strokeHemorrhagic stroke 0.10.1 0.10.1
4 Blood units4 Blood units 1.01.0 1.21.2
Placebo + ASA*
N = 6303
(%)
Clopidogrel + ASA*
N = 6259
(%)
* In combination with standard therapy
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Life-Threatening BleedingLife-Threatening Bleeding

CURE
Active* DiffTrial N Placebo*
CURE:CURE: 1256212562 1.5%1.5% 2.0%2.0% +0.5%+0.5%
IV GP IIb/ IIIa Trials:IV GP IIb/ IIIa Trials:
PRISM-PLUSPRISM-PLUS 19151915 0.8%0.8% 1.4%1.4% +0.6%+0.6%
PURSUITPURSUIT 93759375 9.1%9.1% 10.6%10.6% +1.5%+1.5%
excluding CABGexcluding CABG 1.3%1.3% 3.0%3.0% +1.7%+1.7%
CAPTURECAPTURE 12651265 1.9%1.9% 3.8%3.8% +1.9%+1.9%
* In addition to standard therapy including aspirin and heparin
PRISM-PLUS Investigators. N Engl J Med. 1998;338:1488-97.PURSUIT Investigators. N Engl J Med. 1998;339:436-43.
CAPTURE Investigators. Lancet. 1997;349 (9063):1429-1435.
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Major Bleeding in IV GP IIb/IIIa Antagonists Major Bleeding in IV GP IIb/IIIa Antagonists ACS Trials vs CURE: within 30 DaysACS Trials vs CURE: within 30 Days

CURE
†† Up to 12 monthsUp to 12 months
ConclusionsConclusions
In the CURE study of 12,562 patients with ACS without ST-In the CURE study of 12,562 patients with ACS without ST-segment elevation:segment elevation:
clopidogrel demonstrated a 20% relative risk reduction in MI, clopidogrel demonstrated a 20% relative risk reduction in MI, stroke or cardiovascular death with long-term usestroke or cardiovascular death with long-term use†† ( (PP <0.001) <0.001)
the Kaplan-Meier curves began to diverge within hours and the Kaplan-Meier curves began to diverge within hours and continued to diverge over the course of 12 monthscontinued to diverge over the course of 12 months
clopidogrel also demonstrated a 14% relative risk reduction in MI, clopidogrel also demonstrated a 14% relative risk reduction in MI, stroke, cardiovascular death or refractory ischemia (stroke, cardiovascular death or refractory ischemia (P P <0.001)<0.001)
Clopidogrel in addition to aspirin and other standard therapy Clopidogrel in addition to aspirin and other standard therapy demonstrated an early effect (within hours) and sustained long-demonstrated an early effect (within hours) and sustained long-term benefit throughout the entire study period of 12 monthsterm benefit throughout the entire study period of 12 months
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.

CURE
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
ConclusionsConclusions
Minor bleeding was increased, but there was no increase Minor bleeding was increased, but there was no increase in life-threatening bleeds (including intracranial bleeds) in life-threatening bleeds (including intracranial bleeds)
18% Relative Risk Reduction in heart failure 18% Relative Risk Reduction in heart failure ((PP = 0.03) = 0.03)
Significant reductions in the reported use of:Significant reductions in the reported use of:
– IV GP IIb/IIIa inhibitor: 18% (IV GP IIb/IIIa inhibitor: 18% (PP = 0.003) = 0.003)
– thrombolytics: 43% (thrombolytics: 43% (PP < 0.001) < 0.001)

Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
DesignDesignProspectively designed study of patients undergoing PCI who were Prospectively designed study of patients undergoing PCI who were randomized to double-blind therapy with clopidogrel or placebo, randomized to double-blind therapy with clopidogrel or placebo, both in addition to aspirin and other standard therapy in the CURE both in addition to aspirin and other standard therapy in the CURE trialtrial
ObjectivesObjectives to test the hypothesis that pre-treatment with clopidogrel in addition to to test the hypothesis that pre-treatment with clopidogrel in addition to
aspirin and other standard therapy would be more effective than aspirin and other standard therapy would be more effective than aspirin and standard therapy alone in preventing major ischemic aspirin and standard therapy alone in preventing major ischemic events within the first 30 days events within the first 30 days after PCIafter PCI
to determine if long-term treatment (up to 1 year) with clopidogrel in to determine if long-term treatment (up to 1 year) with clopidogrel in addition to aspirin and other standard therapy after PCI would provide addition to aspirin and other standard therapy after PCI would provide additional clinical benefitadditional clinical benefit
PCI-CUREPCI-CURE

Study Design Study Design
Patients randomized to clopidogrel or placebo at CURE trial Patients randomized to clopidogrel or placebo at CURE trial entry, both in addition to aspirin and standard therapyentry, both in addition to aspirin and standard therapy
All patients undergoing PCI during the course of the CURE All patients undergoing PCI during the course of the CURE trial were included in PCI-CUREtrial were included in PCI-CURE
Timing of PCI was at the physician’s discretionTiming of PCI was at the physician’s discretion
At time of PCI, study drug was interrupted and open-label At time of PCI, study drug was interrupted and open-label therapy was initiated for 2-4 weekstherapy was initiated for 2-4 weeks
During open-label therapy, thienopyridines in combination with During open-label therapy, thienopyridines in combination with ASA was permittedASA was permitted
Follow-up ranged from 3-12 monthsFollow-up ranged from 3-12 months
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
PCI-CUREPCI-CURE

PCI
PLACEBO + ASA *
CLOPIDOGREL+ ASA *
30 days post PCIEnd of follow-upUp to 12 months
after randomization
Open-label thienopyridineOpen-label thienopyridine
Pretreatment
Open-label thienopyridineOpen-label thienopyridine
PretreatmentN = 2,658 patients undergoing PCI
* In combination with standard therapy
N = 1345
N = 1313
CURE PCI-CURE
Study DesignStudy Design
R
Mehta, SR. et al for the CURE Trial Investigators CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
PCI-CUREPCI-CURE

End PointsEnd Points
Composite of the following within 30 days of PCI:Composite of the following within 30 days of PCI:myocardial infarctionmyocardial infarctionurgent target-vessel revascularizationurgent target-vessel revascularizationcardiovascular deathcardiovascular death
Composite of the following from PCI to end Composite of the following from PCI to end of follow-up:of follow-up:myocardial infarctionmyocardial infarctioncardiovascular deathcardiovascular death
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
PCI-CUREPCI-CURE

Baseline CharacteristicsBaseline Characteristics
Age (mean, years)Age (mean, years) 61.4 61.4 61.661.6
Male (%)Male (%) 69.9 69.9 69.769.7
Diabetes (%)Diabetes (%) 19.0 19.0 19.019.0
Previous MI (%)Previous MI (%) 26.0 26.0 27.327.3
Prior PCI (%) Prior PCI (%) 13.8 13.8 13.413.4
Prior CABG (%)Prior CABG (%) 13.0 13.0 12.012.0
ST-segment depression (%)ST-segment depression (%) 42.4 42.4 43.243.2
ST-segment elevation (%)ST-segment elevation (%) 4.4 4.4 5.1 5.1
* In combination with standard therapy
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
PCI-CUREPCI-CURE
PlaceboPlacebo Clopidogrel Clopidogrel + ASA*+ ASA* + ASA* + ASA*
(N = 1345)(N = 1345) (N = 1313)(N = 1313)

Interventional CharacteristicsInterventional CharacteristicsPlaceboPlacebo Clopidogrel Clopidogrel + ASA*+ ASA* + ASA* + ASA*
(N = 1345)(N = 1345) (N = 1313)(N = 1313)
Overall median days afterOverall median days afterrandomization on which randomization on which PCI was donePCI was done 1010 1010
PCI during initial hospitalizationPCI during initial hospitalization 66 66
PCI after initial hospitalizationPCI after initial hospitalization 4949 4949
Stent use (%)Stent use (%) 81.381.3 82.482.4
Use of open-label thienopyridineUse of open-label thienopyridine
Before PCI (%)Before PCI (%) 24.724.7 26.426.4
Overall (%)Overall (%) 84.184.1 82.982.9
* In combination with standard therapy* In combination with standard therapy
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
PCI-CUREPCI-CURE

RRR P value
Placebo + ASA*
N = 1345
Clopidogrel + ASA*
N = 1313
From PCI to 30 daysFrom PCI to 30 days
MI, urgent revascularizationMI, urgent revascularizationor CV death or CV death 6.4%6.4% 4.5%4.5% 30%30% 0.030.03
From PCI to follow-upFrom PCI to follow-up
CV death or MI CV death or MI 8.0%8.0% 6.0%6.0% 25%25%0.0470.047
Efficacy OutcomesEfficacy Outcomes
* In combination with standard therapy* In combination with standard therapy
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
PCI-CUREPCI-CURE

0.150.15
0.100.10
0.050.05
0.00.0
0 100100 200200 300300 400400Days of follow-upDays of follow-up
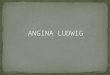
12.6%12.6%
8.8%8.8%
31% RRR31% RRRP P = 0.002= 0.002N = 2658N = 2658
ClopidogrelClopidogrel+ ASA*+ ASA*
PlaceboPlacebo+ ASA*+ ASA*
Cu
mu
lati
ve H
azar
d R
ate
* In combination with standard therapy
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001.
Composite of cardiovascular death or MI from randomization to end of follow-upComposite of cardiovascular death or MI from randomization to end of follow-up
Overall Long-Term ResultsOverall Long-Term Results
PCI-CUREPCI-CURE

30 Day Results30 Day Results
00 55 1010 1515 2020 2525 3030Days of follow-upDays of follow-up
0.00.0
0.020.02
0.040.04
0.060.06
0.080.08
30% RRR30% RRRPP = 0.03 = 0.03
N = 2658N = 2658
Cu
mu
lati
ve H
azar
d R
ate
* In combination with standard therapy
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
6.4%
4.5%
ClopidogrelClopidogrel+ ASA*+ ASA*
Placebo Placebo + ASA*+ ASA*
Composite of cardiovascular death, MI, or urgent revascularizationComposite of cardiovascular death, MI, or urgent revascularization
PCI-CUREPCI-CURE

Overall 12.6% 8.8% 0.69 0.54-0.87
Stent 11.7% 8.7% 0.73 0.56-0.95No stent 16.2% 9.4% 0.56 0.34-0.95
Age 65 9.8% 5.9% 0.59 0.41-0.84Age 65 16.9% 13.4% 0.79 0.57-1.08
Male 11.9% 7.9% 0.65 0.48-0.87Female 14.1% 11.0% 0.77 0.52-1.15
Diabetes 16.5% 12.9% 0.77 0.48-1.22No diabetes 11.7% 7.9% 0.66 0.50-0.87
During initial hosp 12.0% 8.3% 0.68 0.50-0.92After initial hosp 13.8% 9.8% 0.70 0.48-1.02
RRPlacebo+ ASA*
Clopidogrel+ ASA*
Placebo BetterClopidogrel BetterRelative Risk (95% CI)
95% CI
0.1 1.0 10.0* In combination with standard therapy
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
Subgroup AnalysisSubgroup Analysis
PCI-CUREPCI-CURE

RRR P value
Placebo + ASA*
N = 1345
Clopidogrel + ASA*
N = 1313
IV GP IIb/ IIIa useIV GP IIb/ IIIa use 26.6%26.6% 20.9%20.9% 21%21% 0.0010.001
SecondSecondrevascularizationrevascularization 17.1%17.1% 14.2%14.2% 18%18% 0.0490.049
* In combination with standard therapy
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
Other OutcomesOther Outcomes
PCI-CUREPCI-CURE

Placebo + ASA*
Clopidogrel + ASA*
From PCI to 30 daysFrom PCI to 30 days
MajorMajor 1.4%1.4% 1.6% 1.6% ††
Life threateningLife threatening 0.7%0.7% 0.7% 0.7% ††
MinorMinor 0.7%0.7% 1.0% 1.0% ††
From PCI to end of follow-upFrom PCI to end of follow-up
MajorMajor 2.5%2.5% 2.7% 2.7% ††
Life threateningLife threatening 1.3%1.3% 1.2% 1.2% ††
MinorMinor 2.1%2.1% 3.5% 3.5% ‡‡
* In combination with standard therapy
† P = NS, ‡ P = 0.03Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
Bleeding OutcomesBleeding Outcomes
PCI-CUREPCI-CURE

* In combination with standard therapy† Up to 12 months
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
ConclusionsConclusionsFor the composite of MI or cardiovascular death in the 2658 For the composite of MI or cardiovascular death in the 2658 patients who underwent PCI in the CURE trial:patients who underwent PCI in the CURE trial:
clopidogrel plus aspirin* demonstrated a 31% relative risk clopidogrel plus aspirin* demonstrated a 31% relative risk reduction from randomization to the end of follow-up reduction from randomization to the end of follow-up ((PP = 0.002) = 0.002)
clopidogrel plus aspirin* demonstrated a 25% relative risk clopidogrel plus aspirin* demonstrated a 25% relative risk reduction in the composite of MI or cardiovascular death with reduction in the composite of MI or cardiovascular death with long-term use† from PCI to end of follow-up (long-term use† from PCI to end of follow-up (PP = 0.04) = 0.04)
clopidogrel in addition to aspirin and other standard therapy clopidogrel in addition to aspirin and other standard therapy provides early beneficial effects and sustained long-termprovides early beneficial effects and sustained long-term†† benefit benefit in ACS patients requiring PCIin ACS patients requiring PCI
PCI-CUREPCI-CURE

† Up to 12 months
* In combination with standard therapy
Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
ConclusionsConclusions
Long-termLong-term†† administration of clopidogrel plus aspirin* administration of clopidogrel plus aspirin* resulted in an overall 25% relative risk reduction in MI and resulted in an overall 25% relative risk reduction in MI and CV death from PCI to end of follow-upCV death from PCI to end of follow-up
– Pretreatment with clopidogrel plus aspirin* resulted in a Pretreatment with clopidogrel plus aspirin* resulted in a 30% relative risk reduction in CV death, MI and target 30% relative risk reduction in CV death, MI and target vessel revascularization in 30 days post PCIvessel revascularization in 30 days post PCI
There was an increase in minor bleeding, but was There was an increase in minor bleeding, but was no significant difference in major or life-threatening no significant difference in major or life-threatening bleeding between the two treatment groupsbleeding between the two treatment groups
PCI-CUREPCI-CURE