Embed Size (px)
Citation preview

735
because a visit to the clinic is a period of inactivity anda break with normal routine.
The admission to hospital of patients with unstablecontrol for blood-glucose profiles is wasteful of beds andartificial since life in hospital is unlike normal life. Self-monitoring overcomes these problems and saves the pa-tient unnecessary hospital visits since changes in treat-ment can be made by telephone. Home blood-glucosemonitoring can also be used to assess long-term control.Its advantage over measurement of HbAlya-’6 is that itnot only detects poor control, but also shows how to cor-rect it.
We were impressed that blood-glucose could be main-tained at all times near or within the physiological rangewithout dangerous hypoglycaemia even in relativelylong-standing diabetics in whom endogenous insulin se-cretion is presumably lacking. 17 patients were includedin our study because they were thought to be well con-trolled on clinical criteria, and of these 14 had initialblood-glucose profiles where no value exceeded 10mmola. 18 more patients were brought within this levelof control by adjustment of their treatment with the aidof a Reflomat. Case 1 illustrates how a patient whosecontrol had always been poor achieved excellent blood-glucose values within a week and maintained them formany months. Control in the other 5 patients withsevere complications was also greatly improved,although it is too soon to say whether complications willregress.
Strict diabetic control in pregnancy may be difficult toachieve by standard methods of monitoring, especially ifthe renal threshold for glucose is low. Frequent andoften protracted clinic visits are necessary, and manycentres advocate admission during the last trimester. 5However, in one study, strict control in pregnant dia-betics could be maintained on an outpatient basis up tothe 39th week although patients had to be admitted for24-hour profiles." Self-monitoring, as reported by Westand Lowy,t8 is more convenient and we have confirmedits value for the outpatient management of pregnantdiabetics.
We did not encounter any serious difficulties with theReflomat. Diabetic patients are accustomed to needlesand the need for repeated finger pricks has not been amajor difficulty. In many patients a representativeprofile could have been obtained with fewer blood-sam-ples and hence less discomfort. The meter we used hasdrawbacks: it is mains operated and hence limits the pa-tient’s mobility (a smaller battery-operated model wouldbe an advantage); the range of blood-glucose measure-ment (3-20 mmol/1) is limited-the upper limit is of lit-tle practical significance, but the lower limit means thatasymptomatic hypoglycxmia cannot be detected norsymptomatic hypoglycaemia confirmed; the machine isexpensive to buy and to run-on the other hand, eachmachine can be used by many patients and its use ischeap when compared with hospital admission for stabi-lisation.
Sonksen et al.19 using a different reflectance meter,have reached similar conclusions about the value of self-monitoring of blood-glucose. Like them, we believe thatthis approach has advantages over and is a useful sup-plement to other methods used to assess and monitordiabetic control.
We thank the special trustees of Nottingham University Hospital fora grant to R. B. T.; and our secretaries, Mrs Jane Richards and MrsJudith Halford, for their help.
Requests for reprints should be sent to R. B. T.
REFERENCES1. Engerman, R., Bloodworth, J. M. B. Jr., Nelson, S. Diabetes, 1977, 26, 760.2. Mauer, S. M., Steffes, M. W., Sutherland, D. E. R., Najarian, J. S., Michael,
A. F., Brown, B. M. ibid. 1975, 24, 280.3. Fox, C. J., Darby, S. C., Ireland, J. T., Sönksen, P. H. Br. med. J. 1977,
ii, 605.4. Karson, K., Kjellmer, I. Am. J. Obstet. Gynec. 1972, 112, 213.5. Essex, N., Pyke, D. A., Watkins, P. J., Brudenell, J. M., Gamsu, H. R. Br.
med. J. 1973, iv, 89.6. Cahill, G. F., Etzwiler, D. D., Freinkel, N. New Engl. J. Med. 1976, 296,
1004.7. Drash, A. J. Pediat. 1976. 88, 1074.8. Siperstein, M. D., Foster, D. W., Knowles, H. C., Levine, R., Madison,
L. L., Roth, J. New Engl. J. Med. 1977, 196, 1060.9. Sommer, R., Herbinger, W. Dt. med. Wschr. 1975, 100, 1967.
10. Jarret, R. J., Keane, H., Hardwick, C. Diabetes, 1970, 19, 724.11. Brunton, W. A. T., Steel, J. M., Percy-Robb, I. W. Clin. chim. Acta. 1977,
75, 359.12. Knowles, H. C. Jr., in Diabetes Mellitus: Theory and Practice. (edited by M.
Ellenberg and H. Rifkin); p. 666. New York, 1970.13. Malone, J. I., Rosenbloom, A. L., Grgic, A., Weber, F. T. Am. J. Dis. Child.
1976, 130, 1324.14. Koenig, R. J., Peterson, C. M., Kilo, C., Cerami, A., Williamson, J. R. Dia-
betes, 1976, 25, 230.15. Koenig, R. J., Peterson, C. M., Jones, R. L., Saudek, C., Lehrman, M., Cer-
ami, A., New Engl. J. Med. 1976, 295, 417.16. Gonen, B., Rochman, H., Rubenstein, A. H., Tanega, S. P., Horwitz, D. L.
Lancet, 1977, ii, 734.17. Lewis, S. B., Murray, W. K., Wallin, J. D., Coustan, D. R., Daane, T. A.,
Tredway, D. R., Navins, J. P. Obstet. Gynec. 1976, 48, 260.18. West, T. E. T., Lowy, C. Br. med. J. 1977, i, 1252.19. Sönksen, P. H., Judd, S. L., Lowy, C. Lancet, 1978, i, 729.
LONG-TERM TREATMENT OFPARKINSONISM WITH BROMOCRIPTINE
DONALD B. CALNEADRIAN C. WILLIAMSANDREAS NEOPHYTIDES
CHARLES PLOTKINJOHN G. NUTT
PAUL F. TEYCHENNE*
*Present address: George Washington University Medical Center,Washington, D.C.
Experimental Therapeutics Branch, Intramural ResearchProgram, National Institute of Neurological and
Communicative Disorders and Stroke, National Institutes ofHealth, Bethesda, Maryland 20014, U.S.A.
Summary 92 patients with parkinsonism have beentreated with bromocriptine for up to 30
months. 48 continue to receive bromocriptine with bene-fit; of these, 35 take bromocriptine (mean dose 53 mgdaily) in combination with levodopa and 13 take bro-mocriptine (mean dose 45 mg daily) without levodopa.In those who were originally on levodopa, addition ofbromocriptine allowed a mean 41% reduction in thedose of levodopa; the largest group of patients to benefitfrom bromocriptine entered the study because of exces-sive dyskinesia or "on-off" phenomena induced by levo-dopa. In 40 patients bromocriptine was stopped becauseof adverse reactions, absence of therapeutic response, ornon-compliance with the protocol. The main problemswere psychiatric disturbance (8 patients) and erythrome-lalgia (7 patients); these effects tended to occur late(mean 6 months and 10 months, respectively) and withhigh dosage (mean 66 mg and 115 mg daily). Other fre-

736
quent adverse effects were dizziness and nausea; these
began considerably earlier (at 2 months and 1 month)and with much lower dosage (31 mg and 12 mg daily).4 patients died, for reasons apparently unrelated totherapy.
Introduction
BROMOCRIPTINE is an ergot derivative with dopa-minergic properties.’ Since 1972 it has been employedtherapeutically to reduce serum-prolactin, for which thedose does not usually exceed 10 mg daily.2.1’ In acro-megaly up to 60 mg daily has been given to suppressgrowth-hormone secretion. To alleviate motor deficits inparkinsonism doses as high as 150 mg daily have beenused but only in small groups of patients treated forshort periods;4-s we report here our experience with 92parkinsonian patients treated for up to 30 months withhigh doses of bromocriptine.
Patients and Methods
The patients had been referred to the National Institutes ofHealth for experimental therapy. Any with serious hepatic,renal, or psychiatric disease were excluded, but cardiovasculardisorders, if stable, were not regarded as an absolute contra-indication to bromocriptine therapy. As a group, our patientsdiffered from a random selection of the parkinsonian popula-tion in having a higher prevalence of problems with levodopatherapy. 90 patients had idiopathic parkinsonism, 1 had post-encephalitic parkinsonism, and 1 had calcification of the basalganglia.
Patients were started on a 1 mg test dose of bromocriptinebecause higher initial doses occasionally cause serious hypoten-sive reactions; intake was increased to optimal levels (usually50-90 mg daily) over 4 weeks. The dose of levodopa wasreduced as necessary over this build-up period, to controladverse reactions. Patients who were receiving anticholinergicagents and amantadine continued on these drugs throughoutthe study, without any changes.
In the clinic each month, neurological status was reviewedand evidence of drug toxicity was sought. Blood-pressure andpulse rates were recorded with the patient lying and standing,and blood-samples were taken for estimation of haemoglobin,red-cell count, red-cell indices, total and differential white-cellcount, and serum protein, electrolytes, urea-nitrogen, creati-nine, uric acid, glutamic-oxaloacetic and glutamic-pyruvictransaminases (s.G.o.T., S.G.P.T.), alkaline phosphatase, andbilirubin. The urine was examined at each attendance.
Patients with angina, old myocardial infarcts, or hyperten-sion were admitted to hospital for careful cardiovascular moni-toring while starting bromocriptine.
Patients were kept on treatment as long as the benefits ofbromocriptine outweighed any ill-effects.
Results
Our experience with the 92 patients is summarised intables i - iv. 52% of the patients continue to take bromo-criptine and most of these are receiving levodopa con-
TABLE I-MEAN DOSES AND DURATIONS OF BROMOCRIPTINETREATMENT
comitantly. The patients receiving bromocriptine withoutlevodopa were made up of newly diagnosed cases andthose who had either experienced major adverse reac-tions to levodopa or had not responded to this drug.Because of the inclusion of newly diagnosed (mildlyaffected) subjects, the neurological deficits in the groupof patients receiving brpmocriptine alone were less thanthose in our total parkinsonian population. This prob-ably accounts for the lower mean dose of bromocriptinein this group. The 4 patients who died (see below) hadsevere parkinsonism and were receiving a high meandose of bromocriptine.The indications for experimental bromocriptine
therapy are shown in table ii together with a summary
TABLE II-RELATION BETWEEN MAIN REASON FOR ENTERING
STUDY AND CONTINUANCE ON BROMOCRIPTINE
*Patients who simply wanted to try any new treatment.
of how many patients benefited. The most useful resultswith bromocriptine were achieved in patients who weretroubled by prominent dyskinesia or "on-off" pheno-mena. A satisfactory response was also obtained in boththe patient with postencephalitic disease and the patientwith calcified basal ganglia. Of the patients who had apoor response to previous levodopa, a minority improvedsubstantially when bromocriptine was added, althoughmany remain on combined therapy.Of the 35 patients receiving bromocriptine with levo-
dopa, all had previously been taking higher doses oflevodopa. In these patients the dosage of levodopa wasreduced by an average of 41% when bromocriptine wasadded. This figure derives from the group of 35 patientswho continue on a combination of bromocriptine andlevodopa; when a patient was taking carbidopa this wasallowed for by multiplying the levodopa dose by four.
About the same reduction in levodopa was achieved inthe 40 patients who stopped bromocriptine as in the pa-tients who continued on it. 29 patients were taken offbromocriptine because of adverse reactions. In another8 patients, bromocriptine was stopped because there wasno net benefit. A further 3 patients did not comply withthe protocol.The adverse reactions which most often led to with-
drawal of bromocriptine are summarised in table in.Table iv shows that unwanted effects tended to fall intotwo categories-those arising early in the treatment,before a high dose of bromocriptine could be built up(nausea and dizziness), and those arising after a longerperiod of treatment, at higher dosage (psychiatric reac-tions and erythomelalgia). Psychiatric reactions to
bromocriptine were similar to those induced by levo-dopa-namely, confusion, frequent vivid dreams, hallu-cinations, and delusions. The hallucinations were
usually visual (occasionally auditory or olfactory) andthe delusions generally paranoid. These psychotic fea-tures were usually more florid and persisted for longer
737
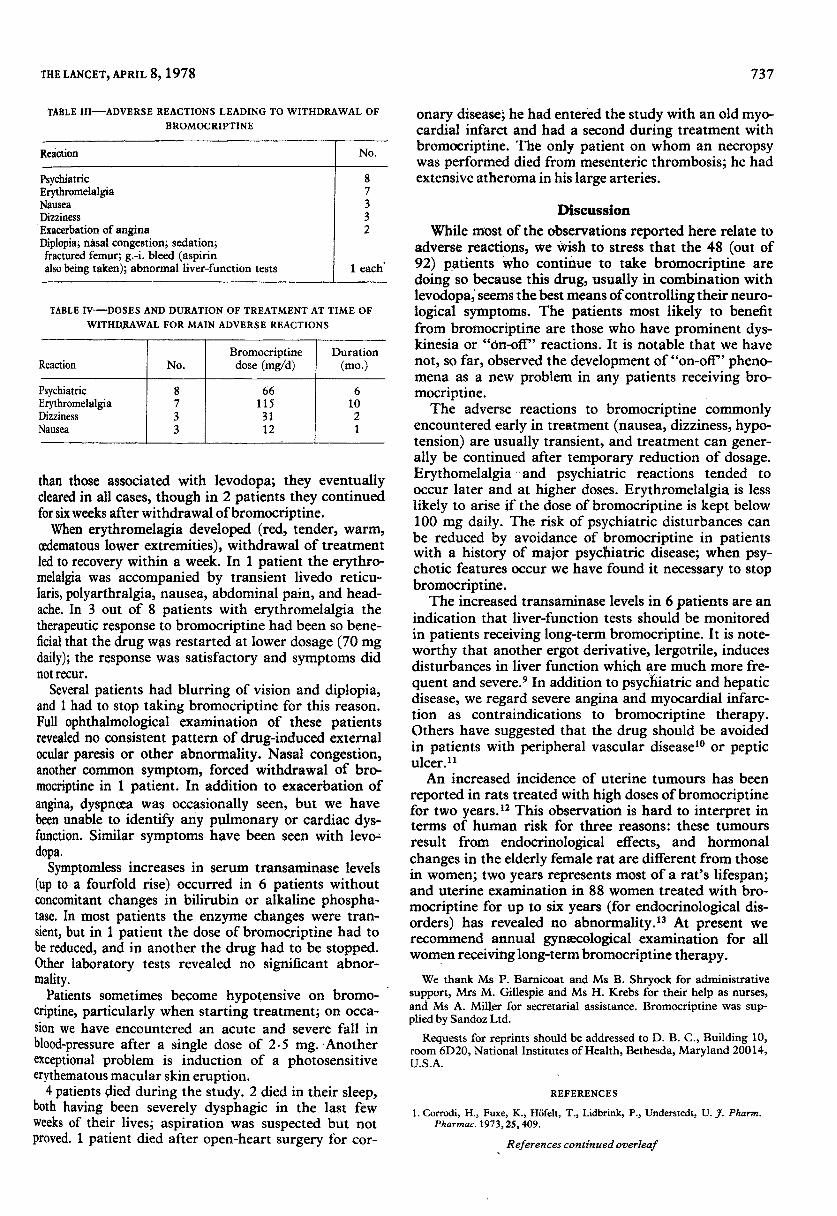
TABLE III-ADVERSE REACTIONS LEADING TO WITHDRAWAL OF
BROMOCRIPTINE
TABLE IV-DOSES AND DURATION OF TREATMENT AT TIME OF
WITHDRAWAL FOR MAIN ADVERSE REACTIONS
than those associated with levodopa; they eventuallycleared in all cases, though in 2 patients they continuedfor six weeks after withdrawal of bromocriptine.When erythromelagia developed (red, tender, warm,
oedematous lower extremities), withdrawal of treatmentled to recovery within a week. In 1 patient the erythro-melalgia was accompanied by transient livedo reticu-laris, polyarthralgia, nausea, abdominal pain, and head-ache. In 3 out of 8 patients with erythromelalgia thetherapeutic response to bromocriptine had been so bene-ficial that the drug was restarted at lower dosage (70 mgdaily); the response was satisfactory and symptoms didnot recur.
Several patients had blurring of vision and diplopia,and 1 had to stop taking bromocriptine for this reason.Full ophthalmological examination of these patientsrevealed no consistent pattern of drug-induced externalocular paresis or other abnormality. Nasal congestion,another common symptom, forced withdrawal of bro-mocriptine in 1 patient. In addition to exacerbation ofangina, dyspnoea was occasionally seen, but we havebeen unable to identify any pulmonary or cardiac dys-function. Similar symptoms have been seen with levo-dopa.Symptomless increases in serum transaminase levels
(up to a fourfold rise) occurred in 6 patients withoutconcomitant changes in bilirubin or alkaline phospha-tase. In most patients the enzyme changes were tran-sient, but in 1 patient the dose of bromocriptine had tobe reduced, and in another the drug had to be stopped.Other laboratory tests revealed no significant abnor-mality.
Patients sometimes become hypotensive on bromo-criptine, particularly when starting treatment; on occa-sion we have encountered an acute and severe fall inblood-pressure after a single dose of 2.5 mg. Anotherexceptional problem is induction of a photosensitiveerythematous macular skin eruption.
4 patients died during the study. 2 died in their sleep,both having been severely dysphagic in the last fewweeks of their lives; aspiration was suspected but notproved. 1 patient died after open-heart surgery for cor-
onary disease, he had entered the study with an old myo-cardial infarct and had a second during treatment withbromocriptine. The only patient on whom an necropsywas performed died from mesenteric thrombosis; he hadextensive atheroma in his large arteries.
Discussion
While most of the observations reported here relate toadverse reactions, we wish to stress that the 48 (out of92) patients who continue to take bromocriptine aredoing so because this drug, usually in combination withlevodopa, seems the best means of controlling their neuro-logical symptoms. The patients most likely to benefitfrom bromocriptine are those who have prominent dys-kinesia or "dn-off" reactions. It is notable that we havenot, so far, observed the development of "on-off" pheno-mena as a new problem in any patients receiving bro-mocriptine.The adverse reactions to bromocriptine commonly
encountered early in treatment (nausea, dizziness, hypo-tension) are usually transient, and treatment can gener-ally be continued after temporary reduction of dosage.Erythomelalgia and psychiatric reactions tended to
occur later and at higher doses. Erythromelalgia is lesslikely to arise if the dose of bromocriptine is kept below100 mg daily. The risk of psychiatric disturbances canbe reduced by avoidance of bromocriptine in patientswith a history of major psycbiatric disease; when psy-chotic features occur we have found it necessary to stopbromocriptine.The increased transaminase levels in 6 patients are an
indication that liver-function tests should be monitoredin patients receiving long-term bromocriptine. It is note-worthy that another ergot derivative, lergotrile, inducesdisturbances in liver function which are much more fre-quent and severe.9 In addition to psychiatric and hepaticdisease, we regard severe angina and myocardial infarc-tion as contraindications to bromocriptine therapy.Others have suggested that the drug should be avoidedin patients with peripheral vascular disease10 or pepticulcer.11An increased incidence of uterine tumours has been
reported in rats treated with high doses of bromocriptinefor two years.12 This observation is hard to interpret interms of human risk for three reasons: these tumoursresult from endocrinological effects, and hormonal
changes in the elderly female rat are different from thosein women; two years represents most of a rat’s lifespan;and uterine examination in 88 women treated with bro-mocriptine for up to six years (for endocrinological dis-orders) has revealed no abnormality. 13 At present werecommend annual gynaecological examination for allwomen receiving long-term bromocriptine therapy.We thank Ms P. Barnicoat and Ms B. Shryock for administrative
support, Mrs M. Gillespie and Ms H. Krebs for their help as nurses,and Ms A. Miller for secretarial assistance. Bromocriptine was sup-plied by Sandoz Ltd.
Requests for reprints should be addressed to D. B. C., Building 10,room 6D20, National Institutes of Health, Bethesda, Maryland 20014,U.S.A.
REFERENCES
1. Corrodi, H., Fuxe, K., Höfelt, T., Lidbrink, P., Understedt, U. J. Pharm.Pharmac. 1973, 25, 409.
738
2. Varga, L., Lutterbeck, P. M., Pryor, J. S., Wenner, R., Erb, H. Br. med. J.1972, ii, 743.
3. Besser, G. M., Parke, L., Edwards, C. R. W., Forsyth, I. A., McNeilly,A. S. Br. med. J. 1972, iii, 669.
4. Kartzinel, R., Perlow, M., Teychenne, P., Gielen, A. C., Gillespie, M. M.,Sadowsky, D. A., Calne, D. B. Lancet, 1976, ii, 272.
5. Lieberman, A., Kupersmith, M., Estey, E., Goldstein, M. New Engl. J. Med.1976, 295, 1400.
6. Parkes, J. D., Debono, A. G., Marsden, C. D. J. Neurol. Neurosurg. Psy-chiat. 1976, 39, 1101.
7. Godwin-Austen, R. B., Smith, N. H. ibid. 1977, 40, 479.8. Martinez-Lage, J. M., Delgado, G., Zubieta, J. L., Viteri, C. Excerpta med.
1977, 427, 23.9. Teychenne, P. F., Pfeiffer, R. F., Bern, S. M., McInturff, D., Calne, D. B.
Neurology (in the press).10. Wass, J. A. H., Thorner, M. O., Besser, G. M. Lancet, 1976, i, 1135.11. Wass, J. A. H., et al. Lancet, 1976, ii, 851.12. Griffith, R. W., Br. med. J. 1977, ii, 1605.13. Besser, G. M., et al. Br. med. J. 1977, ii, 868.
DOUBLE-BLIND CONTROLLED TRIAL OFELECTROCONVULSIVE THERAPY (E.C.T.)AND SIMULATED E.C.T. IN DEPRESSIVE
ILLNESS
C. P. L. FREEMAN J. V. BASSONA. CRIGHTON
Department of Psychiatry, Edinburgh University, and RoyalEdinburgh Hospital
Summary 40 patients prescribed electroconvulsivetherapy (E.C.T.) for treatment of a
depressive illness were randomly allocated to two
groups. One group had the first two E.C.T. treatments
replaced by simulated E.C.T. on a double-blind basis.The results show that E.C.T. is significantly superior tosimulated E.C.T. in the treatment of depressive illness.
Introduction
THE object of the trial was to compare the effective-ness, in the treatment of depressive illness, of bilateralelectroconvulsive therapy (E.C.T.) with a treatment
which simulated E.C.T. as closely as possible. E.C.T. is aneffective treatment for depressive illness 1-3 and hastended to become the standard against which noveltreatments for depression are assessed. But which partsof the treatment are therapeutically active is not clear.
Critics of E.C.T. say that it is a crude and unscientific
therapy which if it works does so through fear, punish-ment, or non-specific factors such as increased nursingand medical attention. The evidence at present availabledoes not support this view and points towards the seiz-ure as being the important therapeutic agent.4The ideal design for such a trial would have been to
have compared a full course of simulated E.C.T. with afull course of real E.C.T. We wanted to conduct the trialon severely and very severely depressed patients forwhom E.c.T. is primarily indicated, and we wanted toavoid the criticism that the trial showed E.C.T. to be inef-fective because the patients were not those who wouldusually receive it. We felt it ethically unjustified to with-hold for a complete course a treatment generallyregarded to be effective and to submit patients to per-haps unnecessary general anaesthesia. The method pre-sented here was therefore a compromise.
MethodPatients
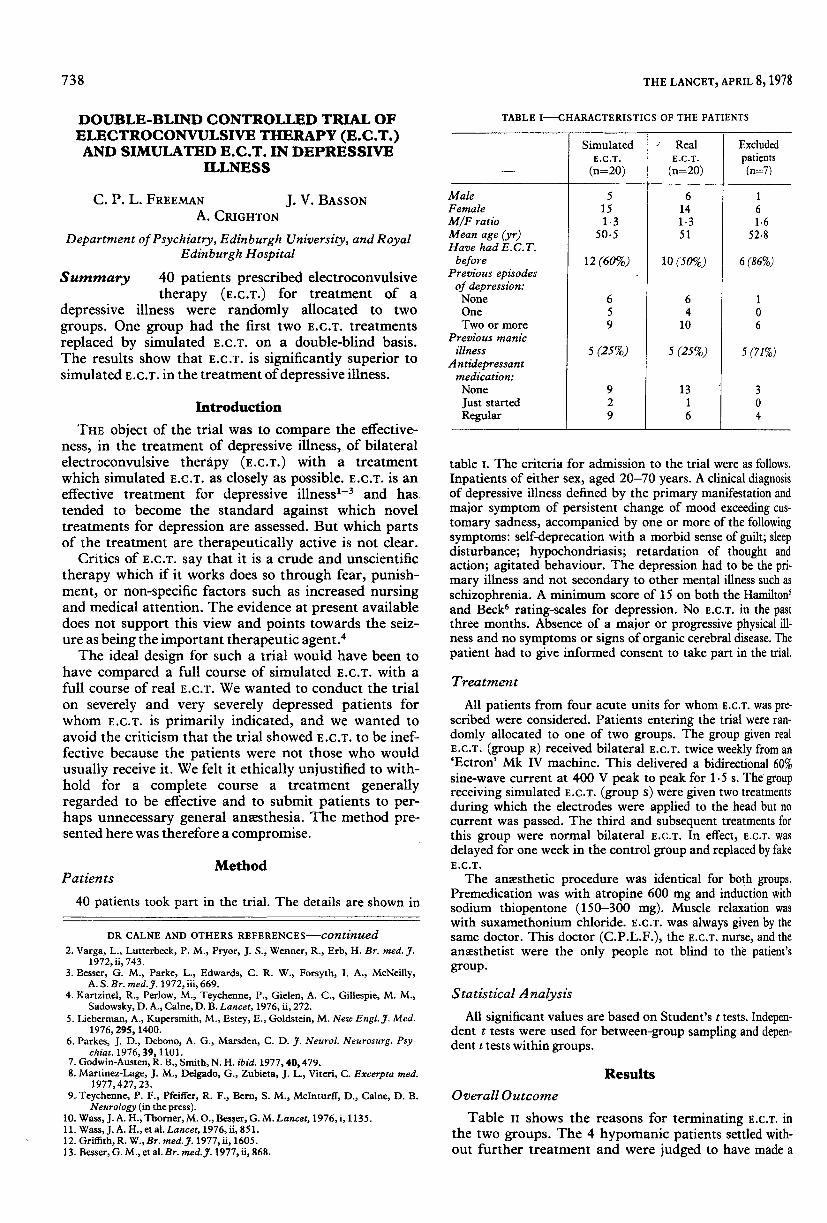
40 patients took part in the trial. The details are shown in
TABLE I—CHARACTERISTICS OF THE PATIENTS
table i. The criteria for admission to the trial were as follows.
Inpatients of either sex, aged 20-70 years. A clinical diagnosisof depressive illness defined by the primary manifestation andmajor symptom of persistent change of mood exceeding cus-tomary sadness, accompanied by one or more of the followingsymptoms: self-deprecation with a morbid sense of guilt; sleepdisturbance; hypochondriasis; retardation of thought andaction; agitated behaviour. The depression had to be the pri-mary illness and not secondary to other mental illness such asschizophrenia. A minimum score of 15 on both the Hamilton’and Beck rating-scales for depression. No E.C.T. in the pastthree months. Absence of a major or progressive physical ill-ness and no symptoms or signs of organic cerebral disease. Thepatient had to give informed consent to take part in the trial.
Treatment
All patients from four acute units for whom E.c.T. was pre-scribed were considered. Patients entering the trial were ran-domly allocated to one of two groups. The group given realE.c.T. (group R) received bilateral E.C.T. twice weekly from an’Ectron’ Mk IV machine. This delivered a bidirectional 60%sine-wave current at 400 V peak to peak for 1.5 s. The groupreceiving simulated E.C.T. (group s) were given two treatmentsduring which the electrodes were applied to the head but nocurrent was passed. The third and subsequent treatments forthis group were normal bilateral E.C.T. In effect, E.C.T. was
delayed for one week in the control group and replaced by fakeE.C.T.
The anaesthetic procedure was identical for both groups.Premedication was with atropine 600 mg and induction withsodium thiopentone (150-300 mg). Muscle relaxation waswith suxamethonium chloride. E.C.T. was always given by thesame doctor. This doctor (C.P.L.F.), the E.C.T. nurse, and theanaesthetist were the only people not blind to the patient’sgroup.
Statistical AnalysisAll significant values are based on Student’s t tests. Indepen-
dent t tests were used for between-group sampling and depen-dent t tests within groups.
Results
Overall Outcome
Table n shows the reasons for terminating E.C.T. inthe two groups. The 4 hypomanic patients settled with-out further treatment and were judged to have made a
![Vascular parkinsonism · Vascular parkinsonism – REVIEW future science groupfuture science group 239 20%) suffered from parkinsonism with strong evidence of CVD [23]](https://img.pdfslide.us/doc/110x75/5c12e69c09d3f208438bb500/vascular-parkinsonism-vascular-parkinsonism-review-future-science-groupfuture.jpg)