Embed Size (px)
Citation preview

.Parkinsonism and motor disorders
Supervised by Dr- hajaj.
Done by Ebrahim Al-Qunaibut.

.OBJECTIVES
Define parkinsonism and describe its etiology.
Explain the pathological finding of pakinson`s disease.
List the symptoms and signs of parkinsonism.
Outline the management of parkinsonism.

.INTODUCTION

.DEFINITION
It is a clinical syndrome characterized by diminished facial expression, stooped posture, slowness of voluntary movement, festinating gait, rigidity and tremor ( pill-rolling ).
This type of motor disturbance have in common damage to the nigro-striatal dopaminergic system.

.ETIOLOGY
there is selective degeneration of pigmented dopaminergic neurons of the substantia nigra
There are few real clues as to the cause of parkinsonism.
1. Nicotine :- PD is less prevalent in tobacco smokers than lifelong
abstainers.2. MPTP :- Minute doses of the pyridine compound cause sever
PD.

.ETIOLOGY
3. Environmental agent :-
Environmental MPTP – like herbicide are implicated.
4. Encephalitis lethargica :-
Some survivors of viral encephalitis lethargica developed sever PD.

.ETIOLOGY
5. Genetic factors :-There are 3 mutated proteins which have been found in
patients with PD.a ) alpha – synuclein gene on chromosome 2 and
account for autosomal dominant.B ) ubiquitin carboxyl-terminal hydrolase L1 on
chromosome 4 and also account for autosomal dominant
C ) parkin gene on chromosome 6 and found in families with autosomal recessive and some young. Account for most of cases below the age of 40.

.ETIOLOGY
Mutant parkin proteins are unable to interact and ubquinate form of alpha – synuclein accumulate.
6. Drugs :-
Side effects of several antipsychotic drugs (i.e., phenothiazides, butyrophenones, reserpine)


PATHOLOGICAL EXAMINATION.
Macroscopic examination :-The typical finding are pallor of the
substantia nigra and locus ceruleus. Microscopic examination :-there is loss of the pigmented
catecholaminergic neurons in these regions associated with gliosis and Lewy bodies

.LEWY BODY
Could be found in some of the remaining neurons.
Single or multiple. Cytoplasmic, eosinoplic, round to
elongated inclusion. Have dense core surrounded by a pale
hallo.

.LEWY BODY
Composed of fine filaments. These filaments are made of alpha –
synuclein, parkin and ubiquitin. May be found in other brainstem
nuclei.

.PATHOLOGICAL EXAMINATION

.SYMOPTOMS AND SIGNS
most symptoms do not appear until striata DA levels decline by at least 70-80%.
There are 3 main clinical features in PD :-
tremor, rigidity and bradykinesia or akinesia.

.( TREMOR ( resting tremor
It is asymptomatic at first. Characteristic 4-7Hz pill-rolling. PD present with resting tremor which is a rhythmical
movement. Resting tremors are present mostly during relaxation of the
muscles and decrease with action. Tremor consist of flextion and extension or pronation and
supination Usually affect distal joints. Nigrothalamic pathway is dopaminergic ( inhibtory ) and in PD
it is affected. So ,, excessive impulses pass from thalamus to motor cortex ( halamocortical projection is excitatory ). This produce oscillation which cause tremor.

.RIGIDITY
Define as an increase in resistance to passive movement.
Throughout the range of limb movement and is equal in opposing muscle groups.
Lead pipe or cogwheeling ??? Rigidity is more easily felt when a joint is moved
slowly and gently. The flow of impulses in the basal nuclei is from
cerebral cortex to neostriatum then to globus P. then again to cortex via thalamic nuclei. This feed back pathway is inhibited by dopaminergic nigrostriatal pathway which is already depleted.

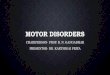
17
G pallidus
thalamus
S nigra
neostriatum
GABA
GABA
Dopamine
Dopamine
tremor
rigidity

.BRADYKINESIA
Difficulty in initiating movement. Not rigidity.
Rapid fine finger movement ( piano – playing ) become indistinct.
Facial immobility give a mask-like semblance of depression.
Spontaneous blinking is reduced producing a serpentine stare.

.OTHER SYMPTOMS AND SIGNS
Postural change :-
- stoop is characteristic.
- gait become hurrying (festinant) and shuffling with poor arm swinging.
- sometime called simian
- falls are common in later stage of PD.

.OTHER SYMPTOMS AND SIGNS
Speech :-
- pronunciation initially monotone.
- progresses to tremulous slurring dysarthria.
- combination of akinesia, tremor and rigidity, speech may be lost completely (anarthria).

.OTHER SYMPTOMS AND SIGNS
Heartburn. Dementia. Dribbling. Dysphagia. Constipation. Weight loss. Urinary difficulties (men).

.DIAGNOSIS
A diagnosis of PD can be made with some confidence in patients who present with at least two of the three cardinal signs
rest tremor , rigidity, and bradykinesia MR is normal

.TREATMENT

![Vascular parkinsonism · Vascular parkinsonism – REVIEW future science groupfuture science group 239 20%) suffered from parkinsonism with strong evidence of CVD [23]](https://img.pdfslide.us/doc/110x75/5c12e69c09d3f208438bb500/vascular-parkinsonism-vascular-parkinsonism-review-future-science-groupfuture.jpg)