Embed Size (px)
Citation preview

J
O
Ldr
HKKKKH
a
b
RA
0d
ournal of Cardiology (2011) 58, 158—164
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / j j cc
riginal article
ong-term outcomes of women with coronary arteryisease following complete coronaryevascularization
itoshi Sato (MD)a, Takatoshi Kasai (MD, PhD)a,atsumi Miyauchi (MD, FJCC)a,∗, Naozumi Kubota (MD, PhD)a,an Kajimoto (MD, PhD)b, Tadashi Miyazaki (MD)a, Akihisa Nishino (MD)a,enji Yaginuma (MD)a, Hiroshi Tamura (MD)a, Takahiko Kojima (MD)a,en Yokoyama (MD)a, Takeshi Kurata (MD)a, Atsushi Amano (MD, FJCC)b,iroyuki Daida (MD, FJCC)a
Department of Cardiology, Juntendo University, School of Medicine, 2-1-1 Hongo, Bunkyo-ku, Tokyo, JapanDepartment of Cardiovascular Surgery, Juntendo University, School of Medicine, Tokyo, Japan
eceived 12 January 2011; received in revised form 28 February 2011; accepted 22 March 2011vailable online 18 July 2011
KEYWORDSCoronary arterydisease;Revascularization;Risk factors;Gender-related;Long-term outcomes
SummaryBackground: Although coronary artery disease (CAD) is less prevalent in women than in men,early mortality rate is higher in women with CAD than in men with CAD following coronaryrevascularization. In terms of the long-term outcomes after coronary revascularization, limiteddata are available. Especially, in the Japanese CAD population, no data about sex-related differ-ences in long-term outcomes after coronary revascularization exist. The aim of this study wasto compare long-term outcomes between men and women following complete revascularizationin Japanese patients with CAD.Methods: We collected data from 1836 consecutive patients who underwent complete revas-cularization by percutaneous coronary interventions and/or bypass surgeries. All-cause andcardiac mortality and the incidence of stroke were compared between men and women. Inaddition to the univariate analysis, a multivariate Cox regression was carried out in order toadjust for differences in baseline characteristics.
Results: There were 274 female patients (14.9%). They were older, had greater total cholesterollevels, and were more likely to have multivessel disease than men. During follow-up [mean (SD),11.4 (2.9) years], 412 patients died (including 131 patients who died of cardiac causes), and130 had a stroke. In the multivariate analysis, female patients did not have a significant risk forall-cause mortality (hazard ratio [HR], 1.01; p = 0.993), cardiac mortality (HR, 1.41; p = 0.256),or stroke (HR, 0.71; p = 0.309).∗ Corresponding author. Tel.: +81 3 5802 1056; fax: +81 3 5689 0627.E-mail addresses: [email protected], [email protected] (K. Miyauchi).
914-5087/$ — see front matter © 2011 Japanese College of Cardiology. Published by Elsevier Ltd. All rights reserved.oi:10.1016/j.jjcc.2011.03.003

Long-term outcomes of women with CAD after revascularization 159
Conclusions: In the present study involving CAD patients who underwent complete revascular-ization, we showed that, although women were older and had more unfavorable risk profiles,they did not have a greater risk of long-term all-cause mortality, cardiac mortality, or stroke
.ardi
at
ipfpir
awnws≥hd≥hsc1gsepPrgci
O
Scomwhdaoprafication of Diseases, Ninth Revision (ICD-9) codes 410—414,785.51, and 798. Stroke was defined, based on the WorldHealth Organization stroke definition [33], as a focal neu-
incidence, compared to men© 2011 Japanese College of C
Introduction
In individuals who are less than 60 years of age, the inci-dence of coronary artery disease (CAD) is markedly lower inwomen than in men [1]. Because there is a 20-year delayof CAD onset in women compared with men, it has beensuggested that women may have some mechanism that pro-tects them against CAD before menopause [2]. Therefore,the prevalence of CAD is generally lower in women than inmen, although the morbidity of women due to CAD has beenincreasing recently.
Women with CAD are more likely to have worse out-comes. In particular, women have a greater early mortalitycompared to men with CAD, following coronary revascu-larization with either percutaneous coronary interventions(PCI) or coronary artery bypass surgeries (CABG) [3—12]. Ithas been suggested that this is related to the less favor-able risk profiles of women. For example, women whoreceive coronary revascularization are generally older andhave more comorbidities and more extended CAD than men[7,8,13—15]. On the other hand, the sex differences inoutcomes following coronary revascularization are dimin-ished after adjustment for baseline confounders or if onlythe long-term outcomes are examined [16—21]. Thus, beinga woman in itself does not seem to pose an indepen-dent risk for poor outcome, and it has been suggestedthat safer or advanced treatment procedures, includingnewer PCI techniques, complete revascularization, the useof arterial grafts, and the off-pump technique, mightdecrease the disparity in mortality between women and men[17,22—25].
Limited data in regard to sex differences in the out-come in patients with CAD or those who undergo coronaryrevascularization are available for the Japanese popula-tion [26—28]. In addition, no data on whether there aresex differences in long-term outcomes in patients follow-ing complete revascularization exist. Therefore, the aimof this study was to compare long-term outcomes betweenmen and women following complete revascularization in theJapanese CAD patient population.
Methods
Subjects and baseline data collection
Data from consecutive patients who had undergone surgi-cal and/or percutaneous coronary revascularization at theJuntendo University Hospital between January 1984 andDecember 1992 were analyzed. Patients who had achievedcomplete coronary revascularization, which was defined
as no un-bypassed major vessels with a ≥50% stenosis,were enrolled [29,30]. Patients who had other known life-threatening diseases at baseline and who had associatedcomplex cardiac procedures, such as valve replacement orr2sr
ology. Published by Elsevier Ltd. All rights reserved.
neurysm repair, at the time of the surgical revasculariza-ion were excluded.
Demographic data, including age, sex, and body massndex (BMI), coronary risk factors (blood pressure, lipidrofile, fasting plasma glucose levels, smoking status, andamily history of CAD), medication use, revascularizationrocedure-related factors, comorbidities (prior myocardialnfarction or stroke, current dialysis treatment, or atrial fib-illation) were collected in the database at our institution.
For all analyses, patients were divided into 2 groupsccording to gender. During the study period, each patientas further categorized based on the presence of coro-ary risk factors using the following criteria. Patientsere considered hypertensive if their systolic blood pres-
ure was ≥140 mmHg, their diastolic blood pressure was90 mmHg, or they were currently being treated with anti-ypertensive medications. Patients were considered to haveiabetes mellitus if their fasting plasma glucose levels were126 mg/dL or they were currently being treated with oralypoglycemic drugs or insulin injections [31]. A currentmoker was defined as one who smoked at the time ofomplete revascularization or who had quit smoking withinyear before the complete revascularization. Estimated
lomerular filtration rate (eGFR) was obtained by using thepecific equation for Japanese [32]. Patients were consid-red to have atrial fibrillation if they had persistent orermanent atrial fibrillation at the time of the procedure.atients with isolated PCI were those in whom completeevascularization was achieved by PCI without any bypassrafting. This study was performed according to the ethi-al policies of Juntendo University and was approved by thenternal review board.
utcomes
urvival data and data about the incidence of stroke wereollected by serial contact (every 5 years) with the patientsr their families until September 30, 2000 and from theedical records of patients who had died and from thoseho continued to undergo follow-up examinations at ourospital. Information about the circumstances and date ofeath were obtained from the families of patients who diedt home, and details of the cardiac events or the causef death was supplied by other hospitals or clinics whereatients had been admitted. Mortality data were catego-ized according to the cause of death, such as death fromll causes or cardiac deaths using the International Classi-
ological disorder with rapid onset that persisted at least4 h or until death. This included ischemic and hemorrhagictroke (intracerebral hemorrhage or subarachnoid hemor-hage), but excluded transient ischemic attack (defined as

1 H. Sato et al.
fhcnfc
S
Ccpteamfrdwtimslrm(tetacaagdC
R
B
OppcwtwtatdiMbdApy
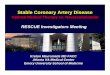
Figure 1 Survival curves (all-cause death) of men and women.There was no significant difference in the cumulative survivalfp
Ct
S
D1sToTable 2. In terms of all-cause mortality, the hazard ratio(HR) for women was not significant in the unadjusted anal-ysis (HR, 0.86; p = 0.305). However, in the age-adjustedmodel, women had a significantly lower risk for all-cause
60
ocal neurological symptoms lasting less than 24 h), subduralemorrhage, epidural hemorrhage, poisoning, or symptomsaused by trauma. The stroke diagnoses were verified byeurologists. In this analysis, the composite incidence ofatal and non-fatal stroke was recorded as the clinical out-ome.
tatistical analysis
ontinuous variables are expressed as mean (SD) andompared using a Student’s t-test. Categorical data are dis-layed as frequencies and percentages and compared usinghe chi-square test or Fisher’s exact test. A Kaplan—Meierstimate with a log-rank test and Cox proportional haz-rds models were used for survival analyses. Univariate andultivariate Cox proportional hazard regressions were per-
ormed in order to examine the unadjusted and adjustedisks for all-cause and cardiac death and the composite inci-ence of fatal and non-fatal stroke in women comparedith that in men. In the multivariate analyses, we created
he following 2 adjusted models: (1) an age-adjusted modeln which only age was included; and (2) a full-adjustedodel in which age, BMI, diabetes mellitus, hyperten-
ion, total and high-density lipoprotein (HDL) cholesterolevels, triglyceride levels, smoking status, eGFR, atrial fib-illation, previous myocardial infarction, previous stroke,ultivessel disease, presence or absence of left main trunk
LMT) lesions, presence or absence of arterial bypass tohe left anterior descending (LAD) artery, left ventricularjection fraction (LVEF), whether complete revasculariza-ion was achieved using isolated PCI, and the use of aspirin,ngiotensin-converting enzyme (ACE) inhibitors, �-blockers,alcium channel blockers, and statins were included, inddition to gender. The assumption of proportional haz-rds was assessed and verified using a log-minus-log survivalraph. p-Values of <0.05 were considered significant. Allata were analyzed using Dr. SPSS II for Windows (SPSS Inc.,hicago, IL, USA).
esults
aseline characteristics
verall, complete revascularization was achieved in 1836atients during the study period. Among them, 274 (14.9%)atients were women. Baseline characteristics and clini-al events during follow-up [mean (SD), 11.4 (2.9) years]ere collected for all the patients. The baseline charac-
eristics of men and women are shown in Table 1. Womenere significantly older and had a lower BMI than men. In
erms of lipid profile, women had greater levels of totalnd HDL cholesterol but had lower triglyceride levels thanhose in men. Women were less likely to be hypertensive andiabetic, although these trends were not statistically signif-cant. Women had greater level of eGFR than that in men.oreover, they were less likely to be a current smoker and toe given ACE inhibitors than men. There were no significant
ifferences between the 2 groups in any other variables.ll patients underwent PCI with balloon angioplasty; noatients received stent implantation, since stents were notet available at the time of complete revascularization. AllFTfp
rom all-cause death between men and women (log-rank test,= 0.305).
ABG procedures were performed under on-pump conven-ional cardiopulmonary bypass.
urvival analyses
uring follow-up, 412 patients (22.4%) died from all causes,31 patients (7.2%) died from cardiac causes, and 130 (7.1%)troke events (95 ischemic and 35 hemorrhagic) occurred.he Kaplan—Meier curves are shown in Figs. 1—3. The resultsf the unadjusted and adjusted analyses are summarized in
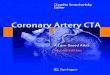
igure 2 Survival curves (cardiac death) of men and women.here was no significant difference in the cumulative survivalrom cardiac death between men and women (log-rank test,= 0.562).

Long-term outcomes of women with CAD after revascularization 161
Table 1 Baseline characteristics.
Men (N = 1562) Women (N = 274) p-Value
Age, years 58.6 (8.8) 62.5 (8.1) <0.001BMI, kg/m2 23.7 (2.6) 22.9 (2.7) <0.001Diabetes mellitus, n [%] 587 [37.6] 116 [42.3] 0.154Hypertension, n [%] 1046 [67.0] 192 [70.1] 0.346Total cholesterol, mg/dL 220.0 (49.0) 229.3 (49.1) 0.004HDL cholesterol, mg/dL 42.0 (12.6) 46.7 (13.3) <0.001Triglycerides, mg/dL 170.4 (104.3) 146.0 (69.5) <0.001Current smoker, n [%] 1260 [80.7] 99 [36.1] <0.001Family history of CAD, n [%] 484 [31.0] 91 [33.2] 0.508eGFR 79.5 (28.9) 109.1 (50.1) <0.001On dialysis, n [%] 25 [1.6] 2 [0.7] 0.405Previous MI, n [%] 756 [48.4] 125 [45.6] 0.433Previous stroke, n [%] 73 [4.7] 9 [3.3] 0.385Atrial fibrillation, n [%] 205 [13.1] 26 [9.5] 0.115Multivessel disease, n [%] 1163 [74.5] 222 [81.0] 0.024LMT lesion, n [%] 123 [7.9] 26 [9.5] 0.434Arterial bypass to LAD, n [%] 508 [32.5] 100 [36.5] 0.223LVEF, % 64.3 (12.9) 65.1 (12.9) 0.352Revascularization — isolated PCI, n [%] 1103 [70.6] 198 [72.3] 0.630Medications, n [%]
Aspirin 1112 [71.2] 201 [73.4] 0.509ACE inhibitors 85 [5.4] 5 [1.8] 0.016Beta blockers 444 [28.4] 75 [27.4] 0.776Calcium channel blockers 329 [21.1] 52 [19.0] 0.481Statins 274 [17.5] 54 [19.7] 0.157
Continuous variables are expressed as mean (SD). BMI, body mass index; HDL, high-density lipoprotein; CAD, coronary artery disease;tion;tion
b
eGFR, estimated glomerular filtration rate; MI, myocardial infarcventricular ejection fraction; PCI, percutaneous coronary interven
mortality than men (HR, 0.69; p = 0.015). When we fully
adjusted for differences in the baseline characteristics, riskfor all-cause mortality in women was not different fromthat in men (HR, 1.01; p = 0.176). There were no differencesin the risk of cardiac mortality between men and women(pn(
Table 2 Hazard ratios for women for all-cause mortality, cardiac
All-cause death Cardiac deat
HR 95%CI p HR 95
UnadjustedMen 1.00 Reference 1.00 RWomen 0.86 0.64—1.15 0.305 0.86 0.Age-adjustedMen 1.00 Reference 1.00 RWomen 0.69 0.52—0.93 0.015 0.73 0.Full-adjustedMen 1.00 Reference 1.00 RWomen 1.01 0.72—1.39 0.993 1.41 0.
The full-adjusted model included sex and age; BMI; diabetes mellitus; hsmoking, eGFR; atrial fibrillation; previous MI; previous stroke; multiabsence of arterial bypass to the LAD; LVEF; whether complete revascuACE inhibitors, �-blockers, calcium channel blockers, or statins. HR, hhigh density lipoprotein; eGFR, estimated glomerular filtration rate; Mdescending; LVEF, left ventricular ejection fraction; PCI, percutaneous
LMT, left main trunk; LAD, left anterior descending; LVEF, left; ACE, angiotensin-converting enzyme.
oth in the unadjusted (HR, 0.86; p = 0.562), age-adjusted
HR, 0.73; p = 0.234), and full-adjusted analyses (HR, 1.41;= 0.256). For the risk of stroke incidence, women had a sig-ificantly lower risk than men in the age-adjusted analysisHR, 0.50; p = 0.024), but this difference was not statisticallymortality, and the incidence of stroke.
h Stroke
%CI p HR 95%CI p
eference 1.00 Reference51—1.45 0.562 0.60 0.33—1.09 0.096
eference 1.00 Reference43—1.23 0.234 0.50 0.28—0.92 0.024
eference 1.00 Reference78—2.53 0.256 0.71 0.36—1.38 0.309
ypertension; total and HDL cholesterol levels; triglyceride levels;vessel disease; presence or absence of LMT lesion; presence orlarization was achieved using isolated PCI; and the use of aspirin,azard ratio; CI, confidence interval; BMI, body mass index; HDL,I, myocardial infarction; LMT, left main trunk; LAD, left anteriorcoronary intervention; ACE, angiotensin-converting enzyme.

162
Figure 3 Stroke-free survival curves of men and women.Tf
sfsosw
D
Tncpvurwtt
s[itibieaviIBemdfita
lslapesTnawwfspswutrdwsfbwb
crvwotoafsofmwf
wdsstmiatoisci
here was no significant difference in the cumulative stroke-ree survival between men and women (log-rank test, p = 0.092).
ignificant in both the unadjusted (HR, 0.60; p = 0.096) andull-adjusted analyses (HR, 0.71; p = 0.309). There were noex-related differences in the type of stroke events (hem-rrhagic or ischemic), with 32 hemorrhagic and 86 ischemictrokes in men and 3 hemorrhagic and 9 ischemic strokes inomen.
iscussion
his study showed two important findings. First, there wereo sex-related differences in the long-term outcome afteroronary revascularization among the Japanese CAD patientopulation, despite the fact that women have more unfa-orable baseline risk profiles. Second, in patients who hadndergone complete revascularization, which is generallyecommended to decrease the disparity between men andomen in early mortality following coronary revasculariza-
ion, long-term outcomes in women were not different fromhose in men.
Many studies have shown sex-related differences in thehort-term outcome following coronary revascularization3—12]. Most of these studies have been reported mainly bynstitutions in Western countries and suggest that, comparedo men, women have poorer short-term outcomes follow-ng either PCI or CABG in association with their unfavorableaseline risk profiles, which include older age and higherncidences of hypercholesterolemia, diabetes mellitus, andxtended CAD. Furthermore, since women generally havesmaller body habitus and, consequently, smaller coronary
essel size than men, these factors might also play a rolen the short-term mortality differences between the sexes.ndeed, in the present study, in addition to their smallerMI, women were older, had greater total cholesterol lev-ls, and were more likely to have multivessel disease thanen. Although some reports have shown that sex-related
ifferences remained after adjustment for baseline risk pro-les [5,6,10—12], most of the other studies have indicatedhat the disparities between men and women disappearedfter adjustment for baseline risk profiles [3,4,7—9]. Simi-o
l(
H. Sato et al.
arly, a recent report on Korean patients with acute coronaryyndrome (ACS) showed that women with ACS were moreikely to have vulnerable plaque components, which weressessed by virtual histology-intravascular ultrasound, com-ared to men with ACS. However, these findings may bexplained by a higher prevalence of diabetes and greaterystemic inflammation in women than in men with ACS [34].his finding is similar to Japanese patients undergoing coro-ary revascularization. Hirakawa et al. [35] showed that,mong patients who had undergone PCI, women were older,ere more likely to have unfavorable risk profiles, and hadorse in-hospital mortality than men, before adjustment
or the baseline profiles. However, after adjustment, theseex-related differences in the short-term outcomes disap-eared. Furthermore, Fukui and Takanashi [36] recentlyhowed that among patients who had undergone CABG, theomen were older and were more likely to non-electivelyndergo CABG, compared to men. After adjustment forhese baseline differences, women were not inferior withespect to their short-term mortality but still had a greaterisadvantage in the incidence of cerebrovascular eventshen compared with men. Taken together, these findings
uggest that being a woman may not be an independent riskactor for a short-term poor outcome, except for the cere-rovascular events, and the other unfavorable risk profiles inomen might play a more important role in the differencesetween sexes with respect to the short-term outcomes.
When we focus on the long-term outcomes followingoronary revascularization, women showed comparable, or,ather, better outcomes than men despite women’s unfa-orable baseline risk profiles [16—21]. Most of the studies,hich have examined sex-related differences in long-termutcomes following PCI or CABG, were from Western coun-ries and showed no sex-related differences in the long-termutcomes following coronary revascularization, especiallyfter adjustment for baseline risk profiles. Considering theseacts, again, it is the unfavorable baseline risk profiles pere, and not being a woman, that may affect the long-termutcomes. Here, we showed that the long-term outcomesollowing coronary revascularization did not differ betweenen and women, even in a Japanese CAD patient population,hich is consistent with the findings from previous studies
rom Western countries.These findings also suggest that the modification of
omen’s unfavorable baseline risk profiles might affect theifference in long-term outcomes. For example, the use ofafer and more advanced or solid treatment procedures,uch as newer PCI techniques, complete revascularization,he use of arterial grafts and the off-pump technique,ight decrease the disparity in the short-term and, in turn,
n the subsequent long-term outcomes between womennd men. Indeed, there are supportive data suggestinghat those procedures altered women’s poor short-termutcomes [17,22—25]. However, there are no data show-ng that complete revascularization might affect suchex-related differences in long-term outcomes. Here, weompared long-term outcomes after complete revascular-zation between men and women and found that long-term
utcomes in women were not different from those in men.Achieving complete revascularization might prevent ateast one characteristic of women’s unfavorable risk profilesi.e. more extended CAD) and thereby diminish differences

tion
[
[
[
[
[
[
[
[
Long-term outcomes of women with CAD after revasculariza
in short-term outcomes [22]. Therefore, analyzing dataabout patients who achieved complete coronary revascu-larization may provide more of an estimation of the effectof being a woman, in itself, on the long-term outcomes.Actually, the present study showed that no differences inlong-term outcomes existed between the genders. Anotherpossible explanation why women with complete revascu-larization have comparable long-term outcomes to men,despite being older and more likely to have unfavorablerisk profiles, may be that women with CAD might be moremotivated to modify the CAD risk factors and to be morecompliant with medications or instructions by cardiologiststhan men with CAD. Nevertheless, this is the first studyinvestigating the presence or absence of sex-related dif-ferences in long-term outcomes among Japanese patientsfollowing complete coronary revascularization.
Study limitations
The present study has several limitations. First, this is aretrospective analysis of a cohort in a single institution.Therefore, the data from the present study should be inter-preted with caution. Second, balloon angioplasty was thesole PCI used in all patients, and all the CABG procedureswere performed under on-pump conventional cardiopul-monary bypass. It is difficult to determine whether the useof stents, including drug-eluting stents and off-pump CABG,which are common in the recent era of coronary revascular-ization, would have affected the results. Third, although weadjusted for the influence of baseline medical treatments inthe multivariable analyses and verified assumptions of theproportional hazard model for these treatments at baseline,the crossovers in drug usage or further interventions forrecurrent CAD during the follow-up period may affect theresults. It is also difficult to determine the relative impor-tance of improvements in both operator skills and adjunctivedrug therapies. Therefore, in the recent era of medicaltreatment and coronary revascularization, further investi-gation is needed to clarify whether sex differences existin the long-term outcomes after revascularization amongthe Japanese CAD population. Third, the number of casesexamined 15 years after revascularization was markedlyreduced. Therefore, the existence of gender-related dif-ferences in really long-term (>15 years) outcomes remainsunclear. Finally, the average life expectancy of women isgenerally longer than that of men in Japan. This should alsobe taken into account.
Conclusion
In the present study involving consecutive patients whounderwent complete revascularization, we showed thatalthough women were older and had more unfavorable riskprofiles, being a woman does not have greater risks for long-term all-cause or cardiac mortality or for stroke incidence,compared to men.
References
[1] Sytkowski PA, D’Agostino RB, Belanger A, Kannel WB. Sex andtime trends in cardiovascular disease incidence and mortal-
[
163
ity: the Framingham Heart Study, 1950—1989. Am J Epidemiol1996;143:338—50.
[2] Kannel WB, Wilson PW. Risk factors that attenuate thefemale coronary disease advantage. Arch Intern Med 1995;155:57—61.
[3] Bell MR, Holmes Jr DR, Berger PB, Garratt KN, Bailey KR,Gersh BJ. The changing in-hospital mortality of women under-going percutaneous transluminal coronary angioplasty. JAMA1993;269:2091—5.
[4] Azar RR, Waters DD, McKay RG, Giri S, Hirst JA, MitchellJF, Fram DB, Kiernan FJ. Short- and medium-term outcomedifferences in women and men after primary percutaneoustransluminal mechanical revascularization for acute myocar-dial infarction. Am J Cardiol 2000;85:675—9.
[5] Vakili BA, Kaplan RC, Brown DL. Sex-based differences in earlymortality of patients undergoing primary angioplasty for firstacute myocardial infarction. Circulation 2001;104:3034—8.
[6] Watanabe CT, Maynard C, Ritchie JL. Comparison of short-termoutcomes following coronary artery stenting in men versuswomen. Am J Cardiol 2001;88:848—52.
[7] Antoniucci D, Valenti R, Moschi G, Migliorini A, Trapani M,Santoro GM, Bolognese L, Dovellini EV. Sex-based differencesin clinical and angiographic outcomes after primary angio-plasty or stenting for acute myocardial infarction. Am J Cardiol2001;87:289—93.
[8] Fisher LD, Kennedy JW, Davis KB, Maynard C, Fritz JK,Kaiser G, Myers WO. Association of sex, physical size, andoperative mortality after coronary artery bypass in the Coro-nary Artery Surgery Study (CASS). J Thorac Cardiovasc Surg1982;84:334—41.
[9] Cosgrove DM, Loop FD, Lytle BW, Baillot R, Gill CC, GoldingLA, Taylor PC, Goormastic M. Primary myocardial revascular-ization. Trends in surgical mortality. J Thorac Cardiovasc Surg1984;88:673—84.
10] Hannan EL, Bernard HR, Kilburn Jr HC, O’Donnell JF. Gen-der differences in mortality rates for coronary artery bypasssurgery. Am Heart J 1992;123:866—72.
11] Weintraub WS, Wenger NK, Jones EL, Craver JM, GuytonRA. Changing clinical characteristics of coronary surgerypatients. Differences between men and women. Circulation1993;88:II79—86.
12] Edwards FH, Carey JS, Grover FL, Bero JW, Hartz RS. Impactof gender on coronary bypass operative mortality. Ann ThoracSurg 1998;66:125—31.
13] Mehilli J, Kastrati A, Dirschinger J, Bollwein H, Neumann FJ,Schomig A. Differences in prognostic factors and outcomesbetween women and men undergoing coronary artery stenting.JAMA 2000;284:1799—805.
14] Mehilli J, Kastrati A, Bollwein H, Dibra A, Schuhlen H,Dirschinger J, Schömig A. Gender and restenosis after coronaryartery stenting. Eur Heart J 2003;24:1523—30.
15] Alfonso F, Hernandez R, Banuelos C, Fernandez-Ortiz A,Escaned J, Sabate M, Pérez-Vizcayno MJ, Fernández C,Macaya C. Initial results and long-term clinical and angio-graphic outcome of coronary stenting in women. Am J Cardiol2000;86:3—1380. A5.
16] Cowley MJ, Mullin SM, Kelsey SF, Kent KM, Gruentzig AR, DetreKM, Passamani ER. Sex differences in early and long-termresults of coronary angioplasty in the NHLBI PTCA Registry.Circulation 1985;71:90—7.
17] Jacobs AK, Johnston JM, Haviland A, Brooks MM, Kelsey SF,Holmes Jr DR, Faxon DP, Williams DO, Detre KM. Improvedoutcomes for women undergoing contemporary percutaneouscoronary intervention: a report from the National Heart
Lung, and Blood Institute Dynamic registry. J Am Coll Cardiol2002;39:1608—14.18] Lansky AJ, Hochman JS, Ward PA, Mintz GS, Fabunmi R, BergerPB, New G, Grines CL, Pietras CG, Kern MJ, Ferrell M, Leon

1
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
64
MB, Mehran R, White C, Mieres JH, et al. Percutaneous coro-nary intervention and adjunctive pharmacotherapy in women:a statement for healthcare professionals from the AmericanHeart Association. Circulation 2005;111:940—53.
19] Weintraub WS, Jones EL, Craver JM, Grosswald R, Guyton RA.In-hospital and long-term outcome after reoperative coronaryartery bypass graft surgery. Circulation 1995;92:II50—7.
20] Koch CG, Weng YS, Zhou SX, Savino JS, Mathew JP, HsuPH, Saidman LJ, Mangano DT, Ischemia Research and Educa-tion Foundation; Multicenter Study of Perioperative IschemiaResearch Group. Prevalence of risk factors, and not gen-der per se, determines short- and long-term survival aftercoronary artery bypass surgery. J Cardiothorac Vasc Anesth2003;17:585—93.
21] Rahimtoola SH, Bennett AJ, Grunkemeier GL, Block P, Starr A.Survival at 15 to 18 years after coronary bypass surgery forangina in women. Circulation 1993;88:II71—8.
22] Parolari A, Dainese L, Naliato M, Polvani G, Loardi C, TrezziM, Fusari M, Beverini C, Tremoli E, Biglioli P, Alamanni F. Dowomen currently receive the same standard of care in coronaryartery bypass graft procedures as men? A propensity analysis.Ann Thorac Surg 2008;85:885—90.
23] Hammar N, Sandberg E, Larsen FF, Ivert T. Comparison of earlyand late mortality in men and women after isolated coro-nary artery bypass graft surgery in Stockholm, Sweden, 1980to 1989. J Am Coll Cardiol 1997;29:659—64.
24] Puskas JD, Edwards FH, Pappas PA, O’Brien S, Peterson ED,Kilgo P, Ferguson Jr TB. Off-pump techniques benefit men andwomen and narrow the disparity in mortality after coronarybypass grafting. Ann Thorac Surg 2007;84:1447—54 [discussion1454—6].
25] Singh M, Rihal CS, Gersh BJ, Roger VL, Bell MR, Lennon RJ, Ler-man A, Holmes Jr DR. Mortality differences between men andwomen after percutaneous coronary interventions. A 25-year,single-center experience. J Am Coll Cardiol 2008;51:2313—20.
26] Kambara H, Kinoshita M, Nakagawa M, Kawai C. Genderdifference in long-term prognosis after myocardial infarction—–clinical characteristics in 1000 patients. The Kyoto and
Shiga Myocardial Infarction (KYSMI) Study Group. Jpn Circ J1995;59:1—10.27] Matsui K, Fukui T, Hira K, Sobashima A, Okamatsu S, HayashidaN, Tanaka S, Nobuyoshi M. Impact of sex and its interaction
[
H. Sato et al.
with age on the management of and outcome for patients withacute myocardial infarction in 4 Japanese hospitals. Am HeartJ 2002;144:101—7.
28] Oe K, Shimizu M, Ino H, Yamaguchi M, Terai H, Hayashi K,Kiyama M, Sakata K, Hayashi T, Inoue M, Kaneda T, Mabuchi H.Effects of gender on the number of diseased vessels and clinicaloutcome in Japanese patients with acute coronary syndrome.Circ J 2002;66:435—40.
29] Jones EL, Weintraub WS. The importance of completenessof revascularization during long-term follow-up after coro-nary artery operations. J Thorac Cardiovasc Surg 1996;112:227—37.
30] McLellan CS, Ghali WA, Labinaz M, Davis RB, GalbraithPD, Southern DA, Shrive FM, Knudtson ML, Alberta Provin-cial Project for Outcomes Assessment in Coronary HeartDisease (APPROACH) Investigators. Association betweencompleteness of percutaneous coronary revasculariza-tion and postprocedure outcomes. Am Heart J 2005;150:800—6.
31] Diagnosis and classification of diabetes mellitus. Diabetes Care2007;30(Suppl. 1):S42—7.
32] Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, YamagataK, Tomino Y, Yokoyama H, Hishida A. Collaborators developingthe Japanese equation for estimated GFR Revised equations forestimated GFR from serum creatinine in Japan. Am J Kidney Dis2009;53:982—92.
33] WHO STEPS stroke manual: the WHO STEP-wise approach tostroke surveillance. Geneva: World Health Organization; 2006.
34] Hong YJ, Jeong MH, Choi YH, Ma EH, Cho SH, Ko JS, LeeMG, Park KH, Sim DS, Yoon NS, Youn HJ, Kim KH, Park HW,Kim JH, Ahn Y, et al. Gender differences in coronary plaquecomponents in patients with acute coronary syndrome: virtualhistology-intravascular ultrasound analysis. J Cardiol 2010;56:211—9.
35] Hirakawa Y, Masuda Y, Kuzuya M, Iguchi A, Kimata T, UemuraK. Impact of gender on in-hospital mortality of patients withacute myocardial infarction undergoing percutaneous coronaryintervention: an evaluation of the TAMIS-II data. Intern Med
2007;46:363—6.36] Fukui T, Takanashi S. Gender differences in clinical and angio-graphic outcomes after coronary artery bypass surgery. Circ J2010;74:2103—8.