Embed Size (px)
Citation preview
Stable Coronary Artery DiseaseOptimal Medical Therapy vs. Revascularization
Kreton Mavromatis MD FACCKreton Mavromatis MD FACCAtlanta VA Medical CenterAtlanta VA Medical Center
Emory University School of MedicineEmory University School of Medicine
RESCUE Investigators Meeting
OverviewOverviewOverviewWhat is the role of OMT +/-
revascularization in stable CAD?BackgroundStudies:
MASS II COURAGEBARI-2D
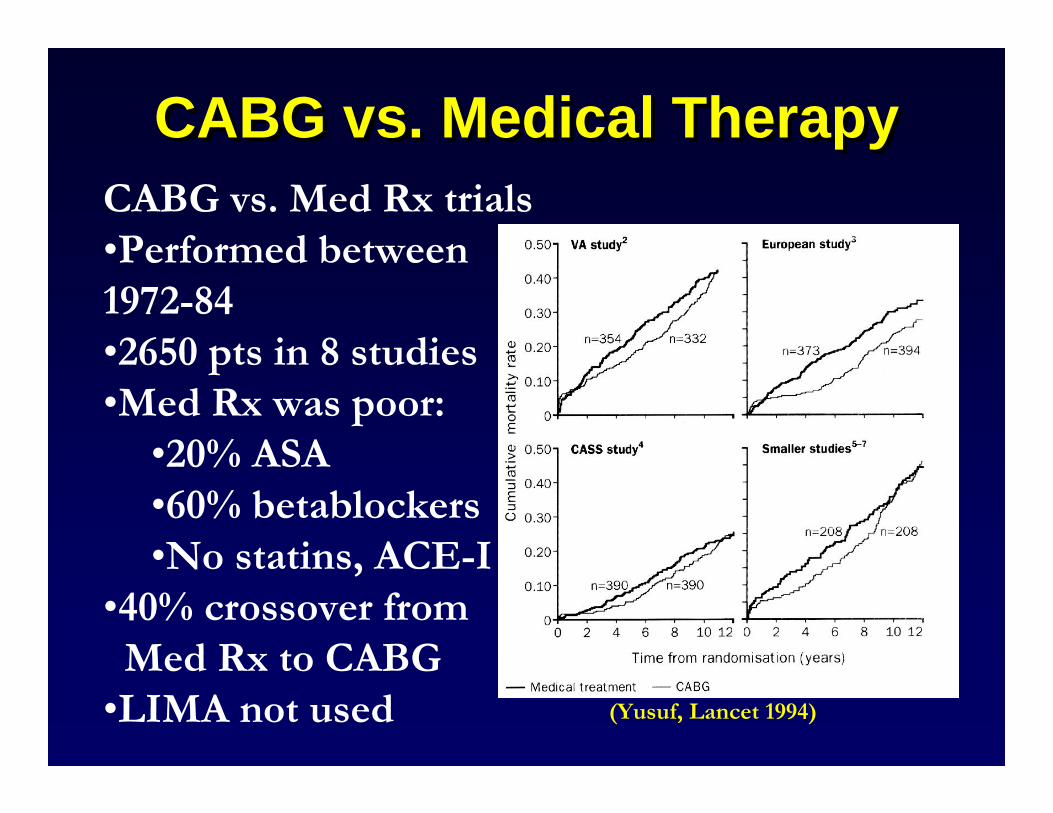
CABG vs. Med Rx trials•Performed between 1972-84•2650 pts in 8 studies•Med Rx was poor:•20% ASA•60% betablockers•No statins, ACE-I
•40% crossover fromMed Rx to CABG•LIMA not used (Yusuf, Lancet 1994)
CABG vs. Medical TherapyCABG vs. Medical TherapyCABG vs. Medical Therapy
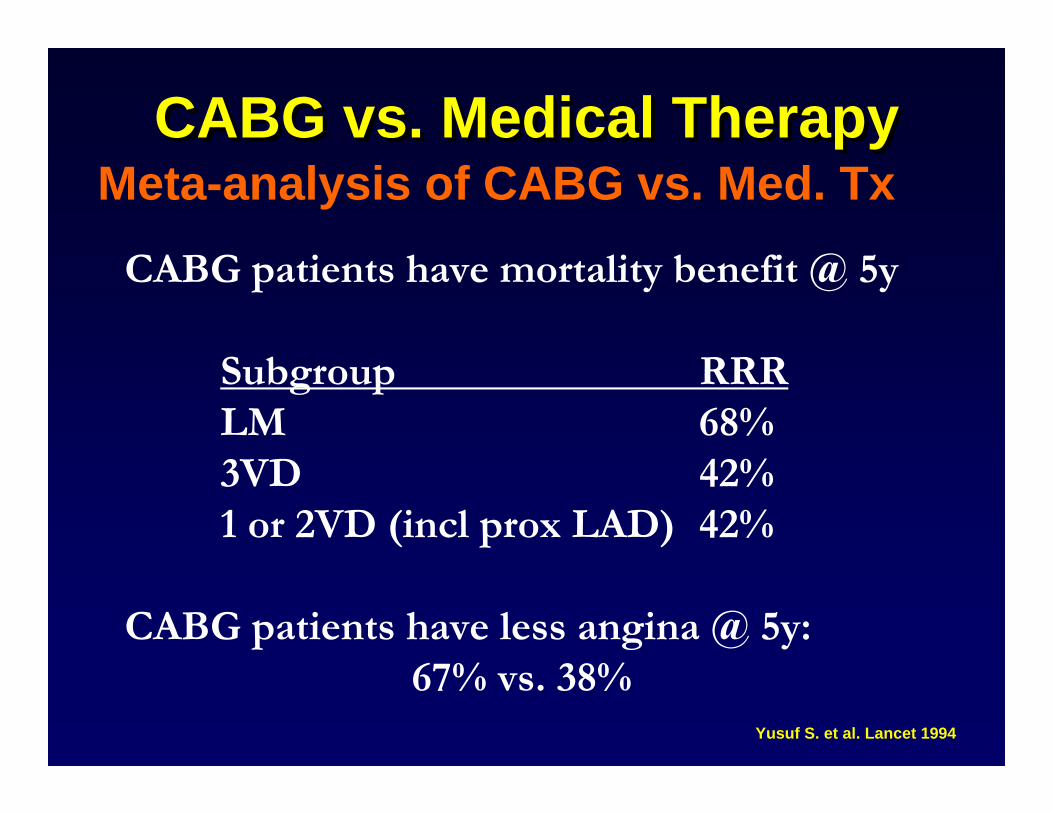
CABG patients have mortality benefit @ 5y
Subgroup RRRLM 68%3VD 42%1 or 2VD (incl prox LAD) 42%
CABG patients have less angina @ 5y: 67% vs. 38%
CABG vs. Medical TherapyCABG vs. Medical TherapyCABG vs. Medical Therapy
Yusuf S. et al. Lancet 1994
Meta-analysis of CABG vs. Med. Tx
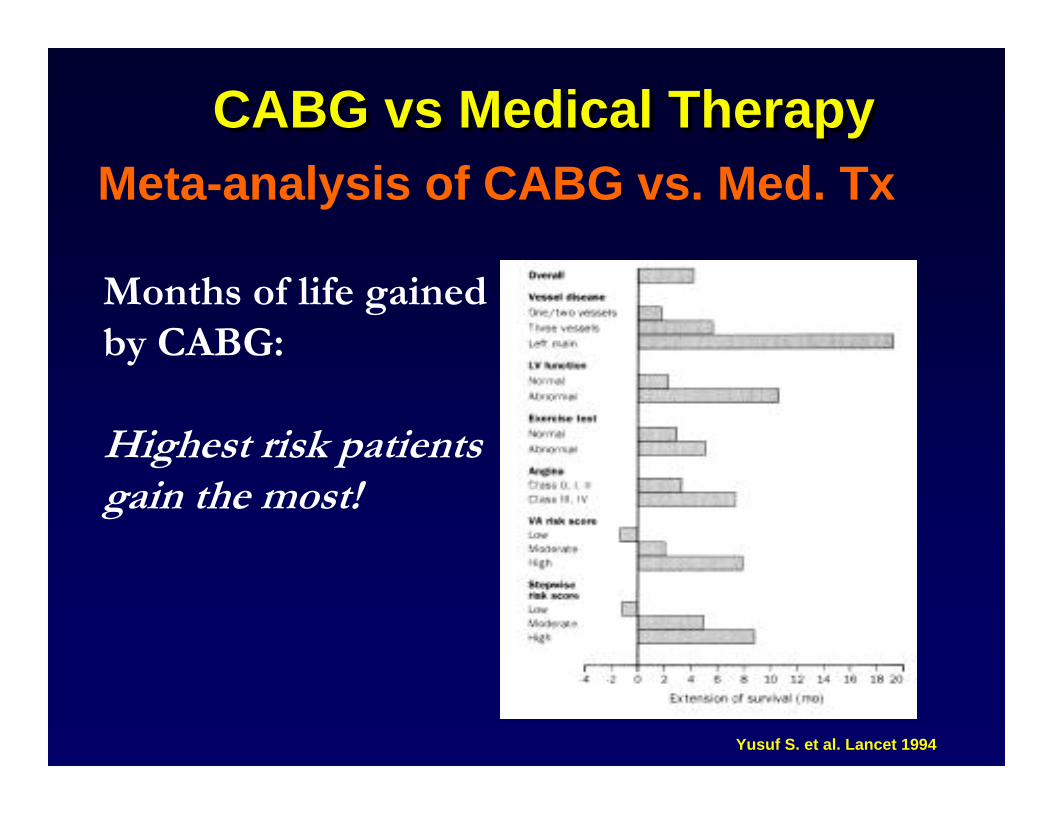
Months of life gained by CABG:
Highest risk patientsgain the most!
CABG vs Medical TherapyCABG vs Medical TherapyCABG vs Medical TherapyMeta-analysis of CABG vs. Med. Tx
Yusuf S. et al. Lancet 1994
Limitations of Prior Randomized Trials
1999 AHA/ACC CABG Guidelines
CABG vs “Medical Therapy”CABG vs CABG vs ““Medical TherapyMedical Therapy””
Patient SelectionPatients <65 years of agePredominantly low-risk, stable patientsOnly 1 trial included women (CASS)
Surgical FactorsOnly 1 trial used arterial grafts (CASS) (in only 14% of patients)Newer modalities of cardioprotection not usedMinimally invasive, off-bypass techniques not used
MedicalTherapyAspirin not widely used or given postoperativelyb-Blockers used in only ~50%Lipid-lowering therapy, ACE-inhibitors, clopidogrel not used
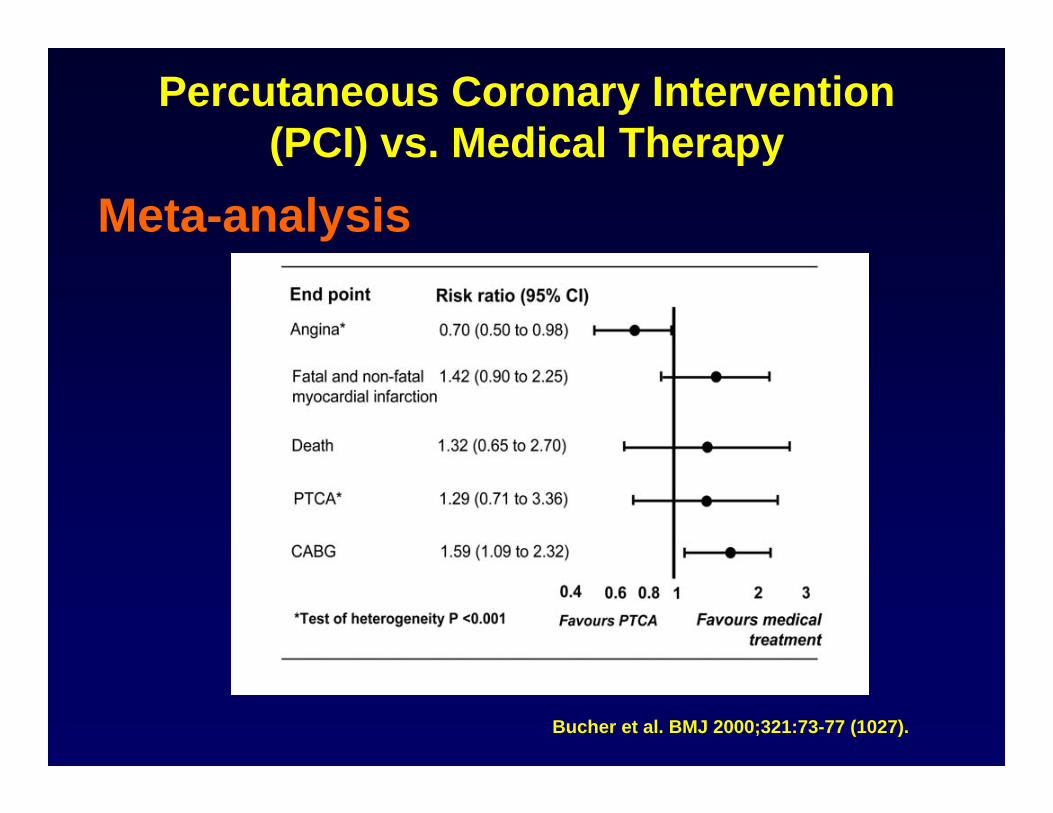
Percutaneous Coronary Intervention (PCI) vs. Medical Therapy
Bucher et al. BMJ 2000;321:73-77 (1027).
Meta-analysis
Limitations of Prior Randomized Trials
1999 AHA/ACC CABG Guidelines
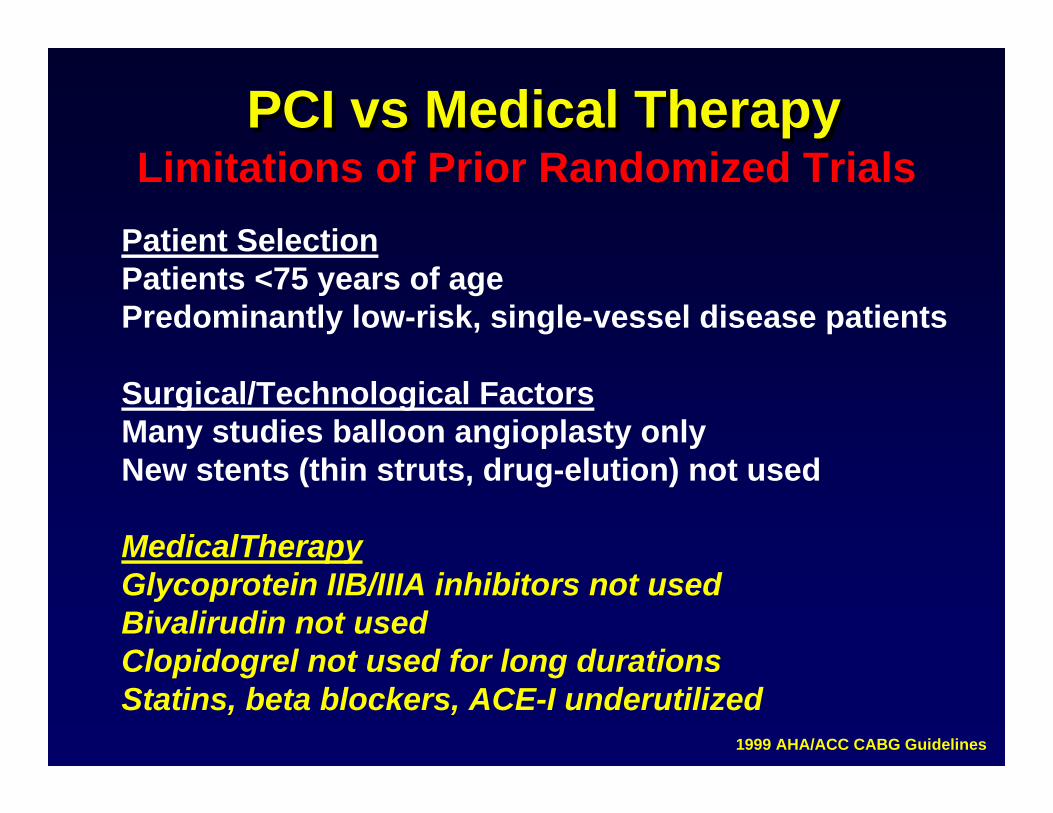
PCI vs Medical TherapyPCI vs Medical TherapyPCI vs Medical Therapy
Patient SelectionPatients <75 years of agePredominantly low-risk, single-vessel disease patients
Surgical/Technological FactorsMany studies balloon angioplasty onlyNew stents (thin struts, drug-elution) not used
MedicalTherapyGlycoprotein IIB/IIIA inhibitors not usedBivalirudin not usedClopidogrel not used for long durationsStatins, beta blockers, ACE-I underutilized
Optimal Medical Therapy for Stable CAD
Optimal Medical Therapy Optimal Medical Therapy for Stable CADfor Stable CAD
Drugs proven to reduce death and MI•beta-blockers•aspirin•statins•ACE inhibitors•eplerenone•thienopyridines
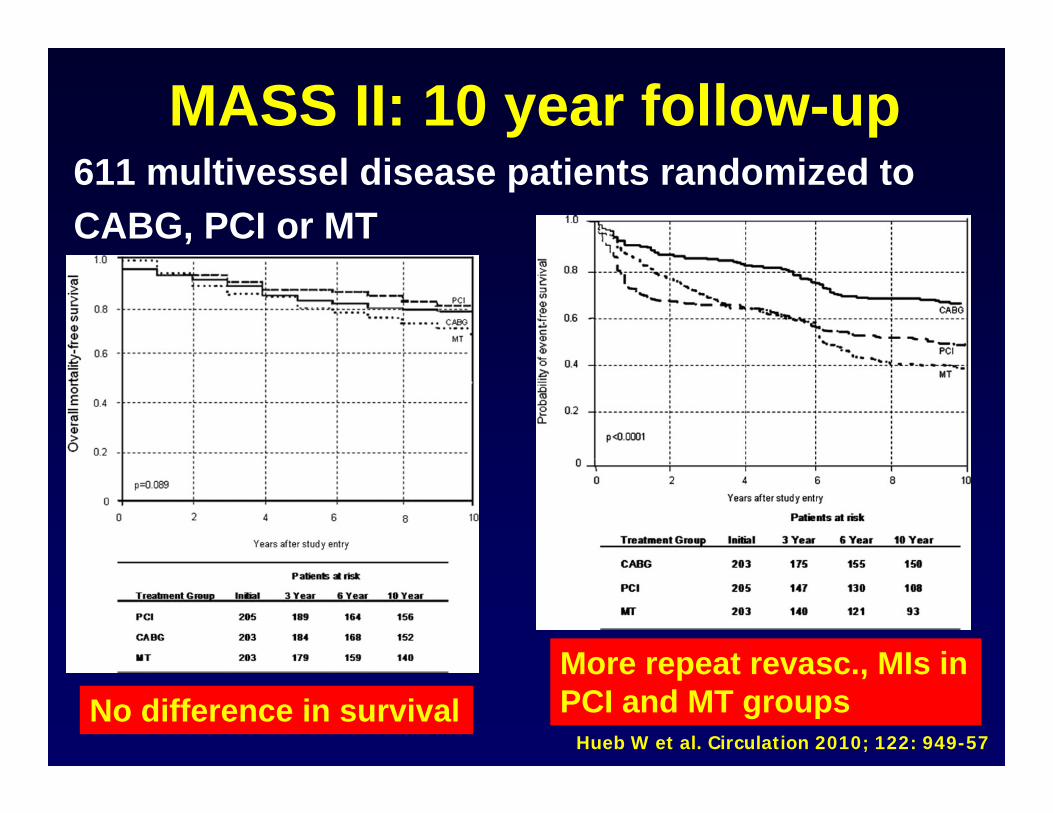
MASS II: 10 year follow-up611 multivessel disease patients randomized to CABG, PCI or MT
Hueb W et al. Circulation 2010; 122: 949-57No difference in survival
More repeat revasc., MIs inPCI and MT groups
MASS II Trial Limitations• Small number of subjects
• Single-center study
• Post-angiography selection bias
• No glycoprotein IIB/IIIA inhibitors
• First-generation stent technology (no DES)Hueb W et al. Circulation 2010; 122: 949-57
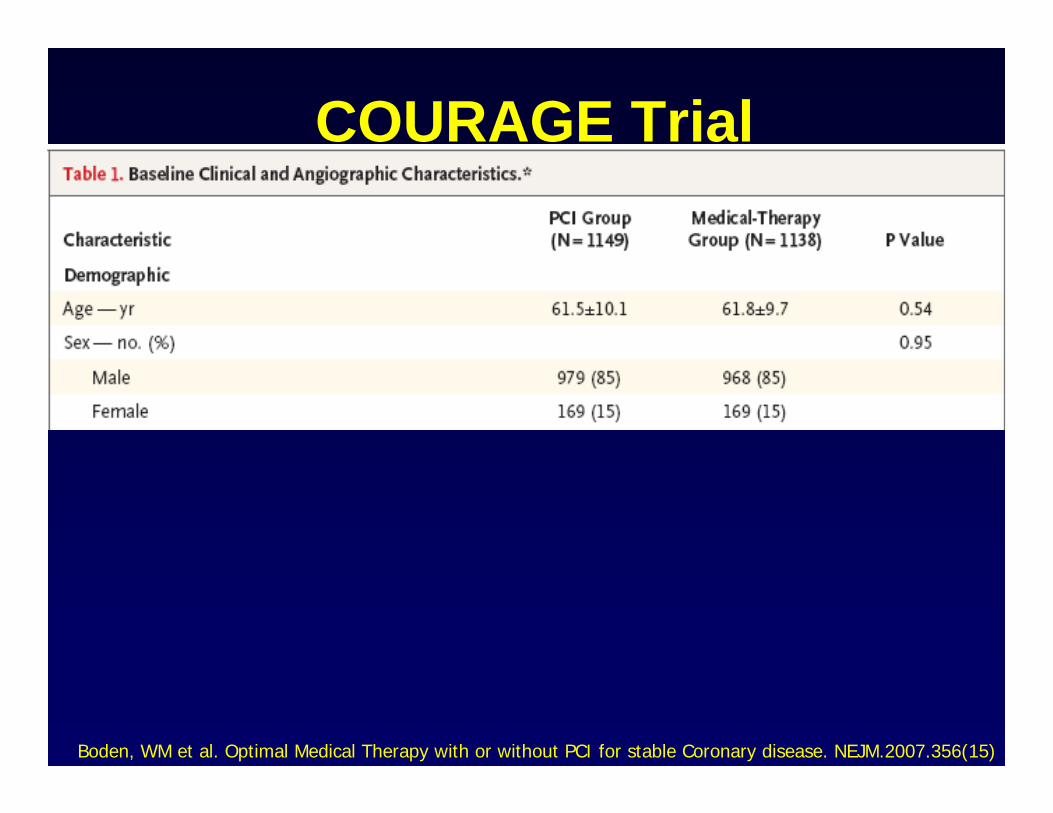
COURAGE Trial• Multi-center, multi-nation study• 2,287 patients (mean age 62y) with stable
CAD– at least one vessel with > 70% stenosisAND– evidence of ischemia by non-invasive testing
(ECG, MPI, DSE) Or
– stenosis > 80% with classic angina
Boden, WM et al. NEJM.2007.356(15)

COURAGE Trial
• Excluded: – CCS class IV angina– ≥50 percent left main – LVEF less than 30%.– Refractory CHF– Early positive treadmill (Stage I Bruce)
Boden, WM et al. NEJM.2007.356(15)
COURAGE Trial
• Randomized to:– optimal medical therapy (OMT) alone vs. OMT
plus PCI
• Follow-up: – 2.5 – 7 years– Mean f/u = 4.6 years
Boden, WM et al. Optimal Medical Therapy with or without PCI for stable Coronary disease. NEJM.2007.356(15)
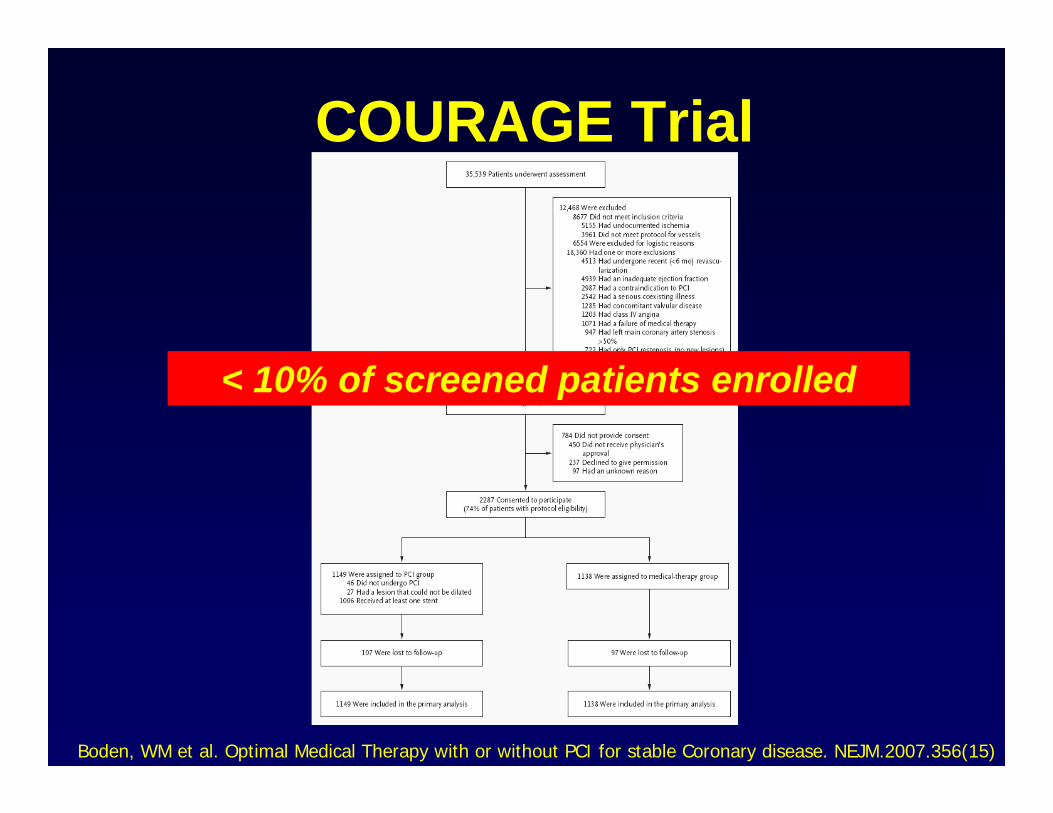
COURAGE Trial
Boden, WM et al. Optimal Medical Therapy with or without PCI for stable Coronary disease. NEJM.2007.356(15)
< 10% of screened patients enrolled
COURAGE Trial
Boden, WM et al. Optimal Medical Therapy with or without PCI for stable Coronary disease. NEJM.2007.356(15)
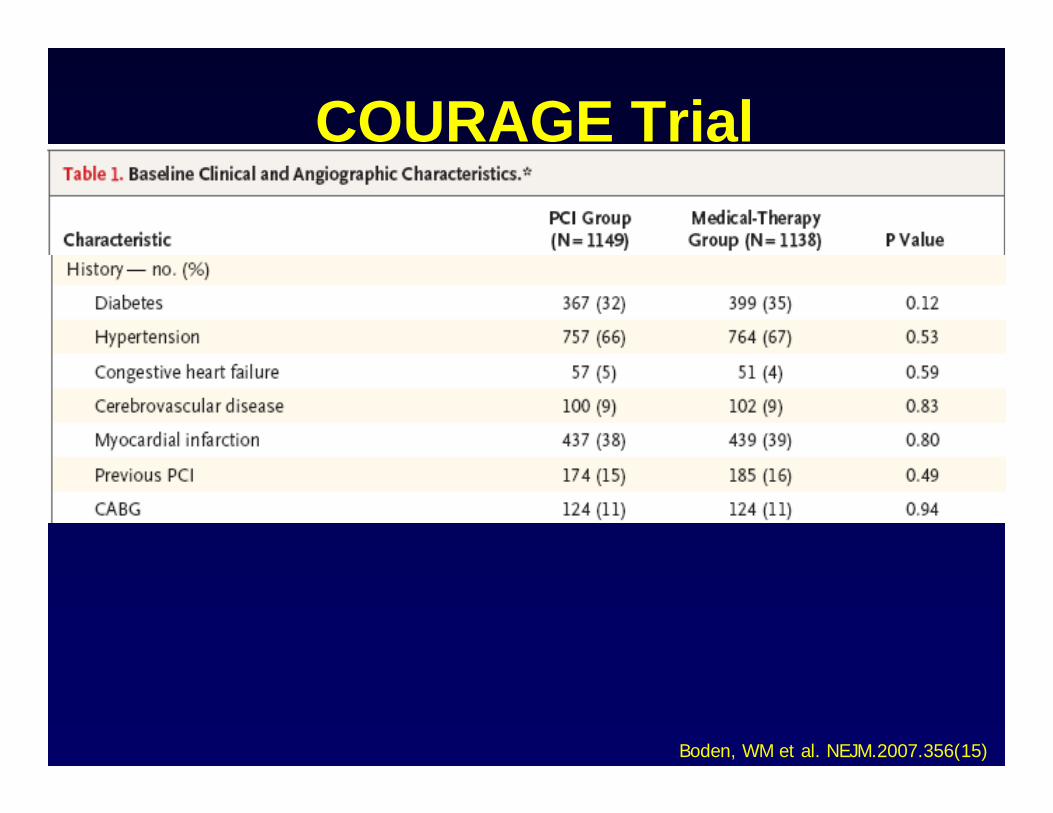
COURAGE Trial
Boden, WM et al. NEJM.2007.356(15)
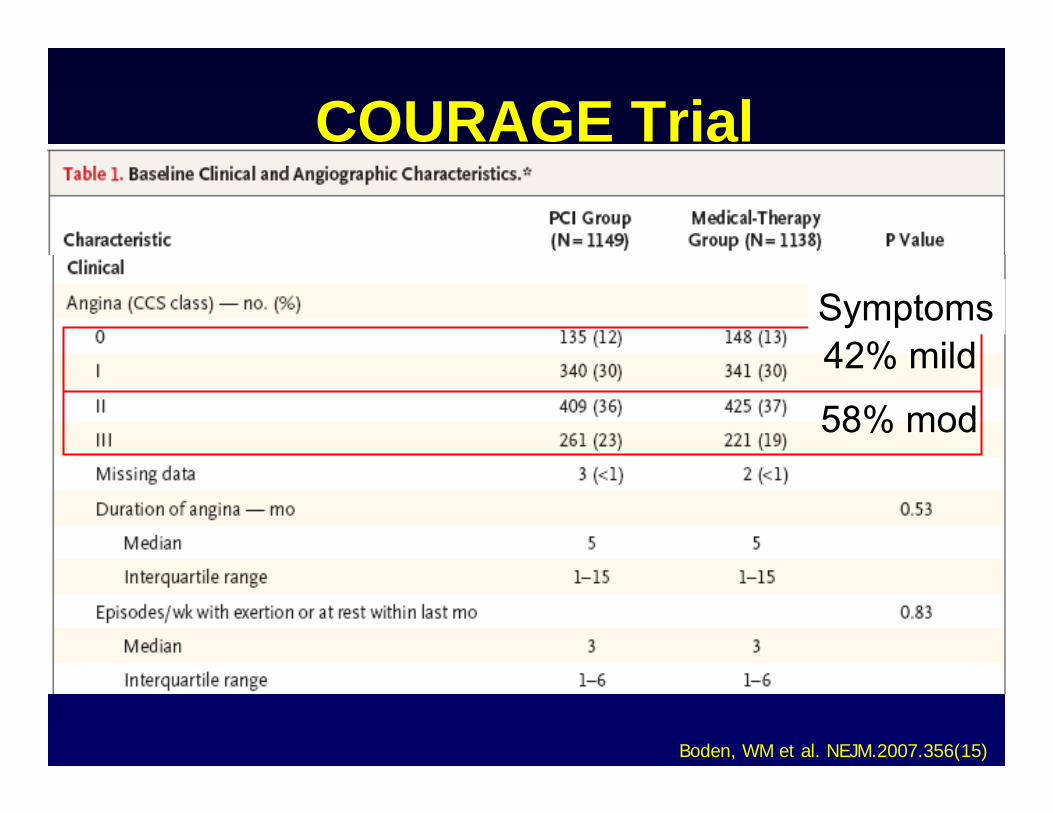
COURAGE Trial
Boden, WM et al. NEJM.2007.356(15)
42% mild
58% mod
Symptoms
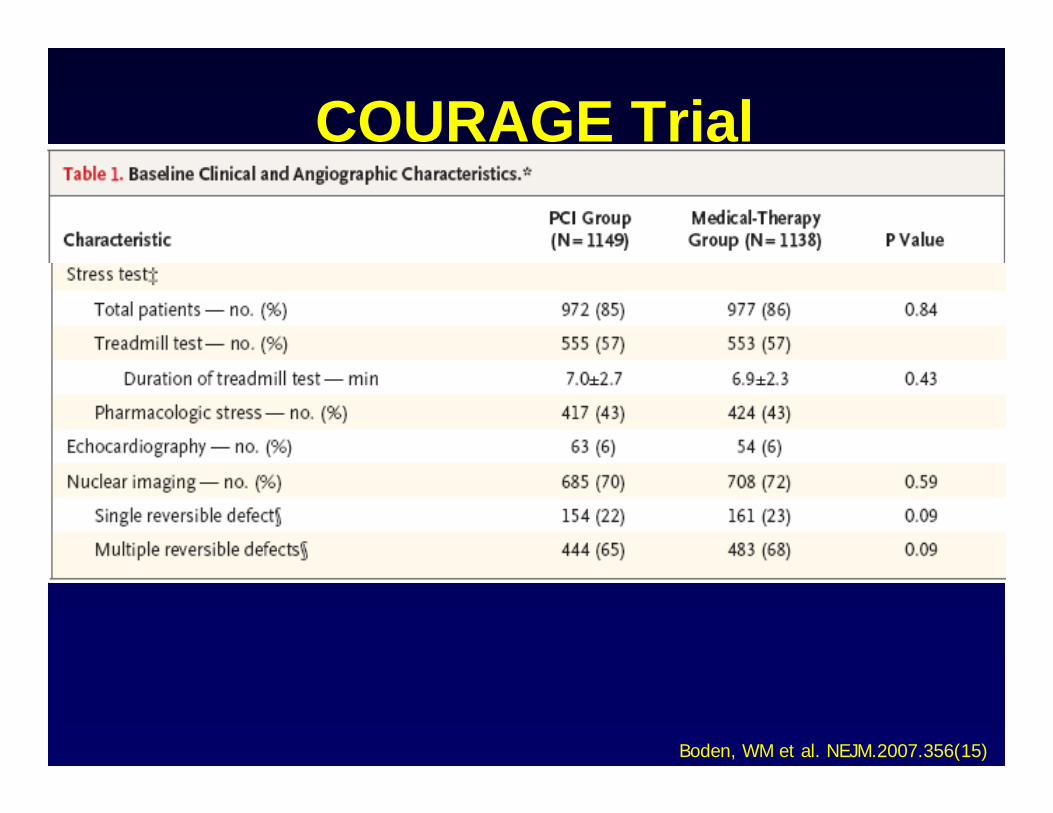
COURAGE Trial
Boden, WM et al. NEJM.2007.356(15)
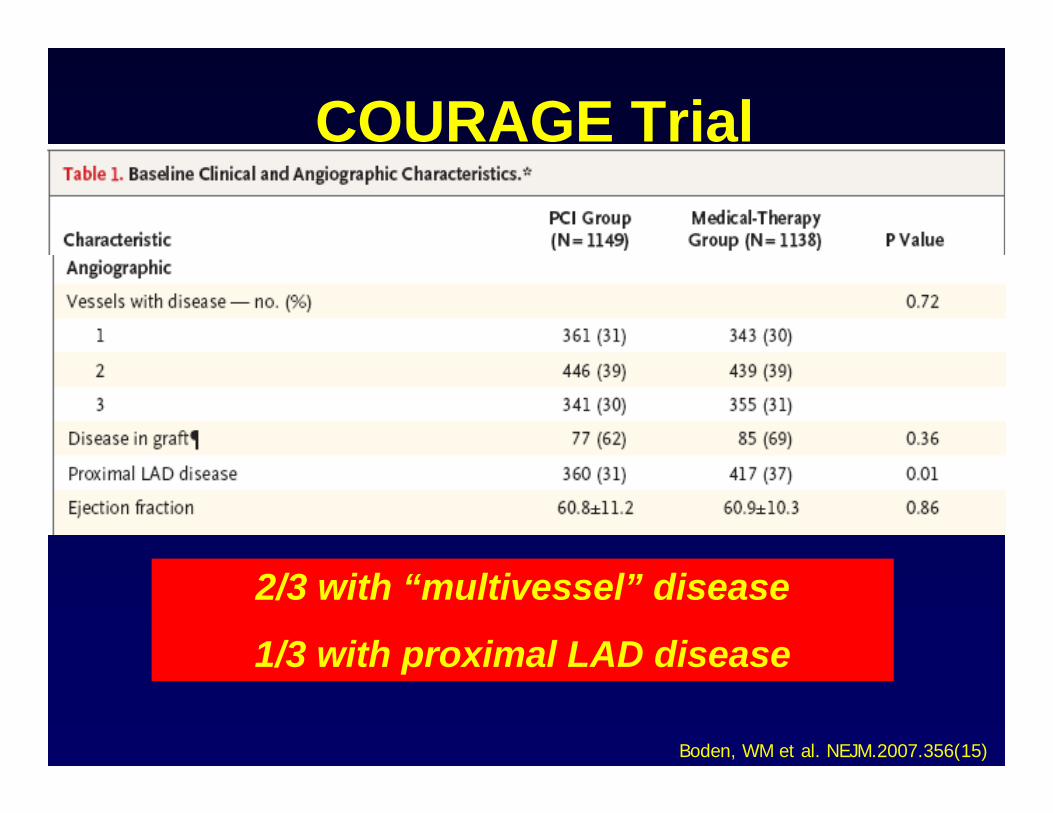
COURAGE Trial
Boden, WM et al. NEJM.2007.356(15)
2/3 with “multivessel” disease
1/3 with proximal LAD disease
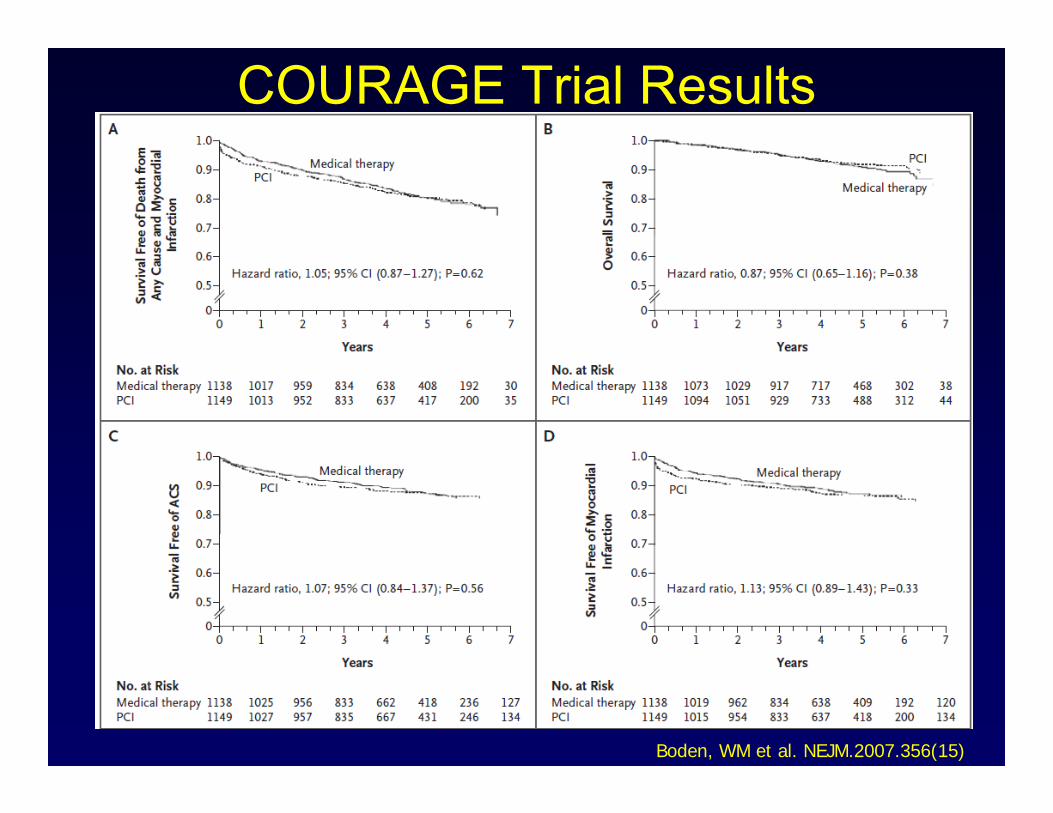
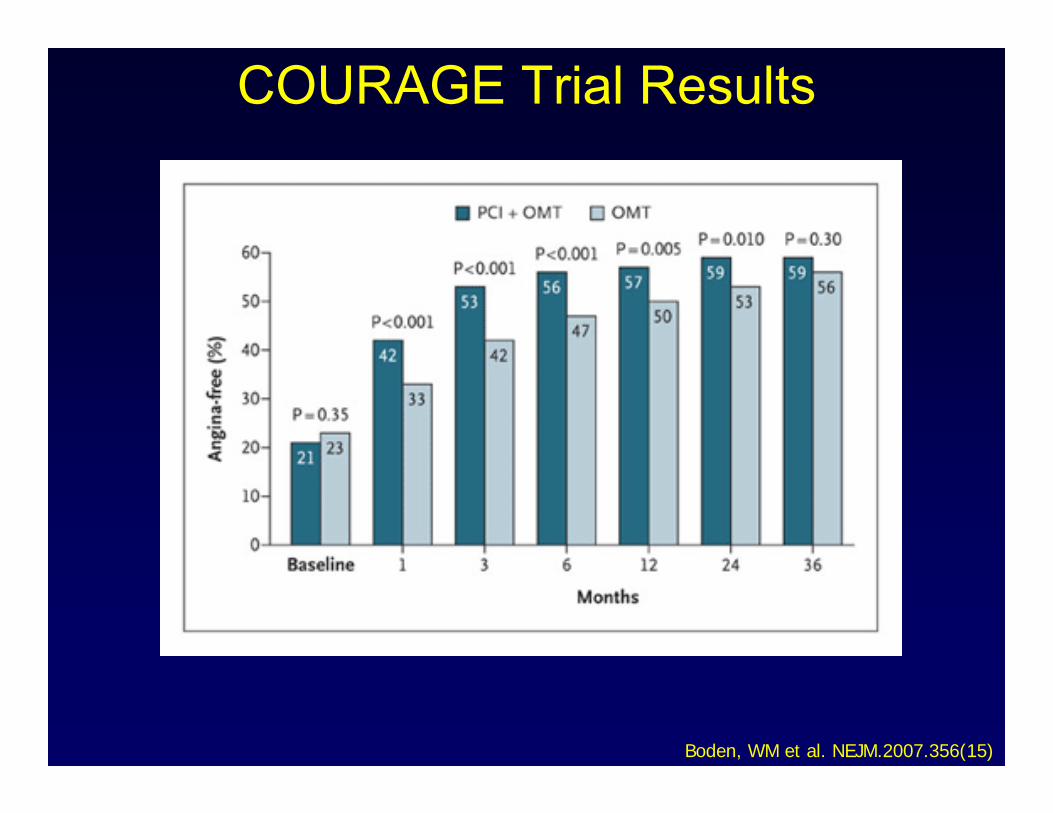
COURAGE Trial Results
Boden, WM et al. NEJM.2007.356(15)
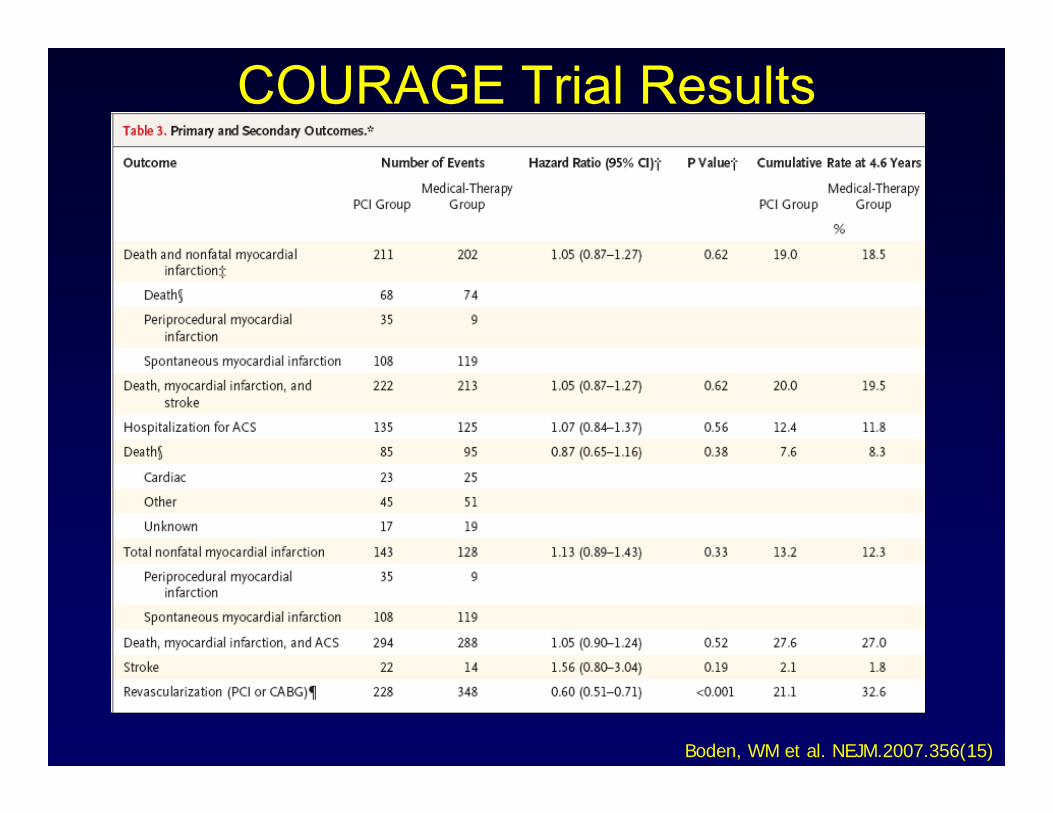
COURAGE Trial Results
Boden, WM et al. NEJM.2007.356(15)
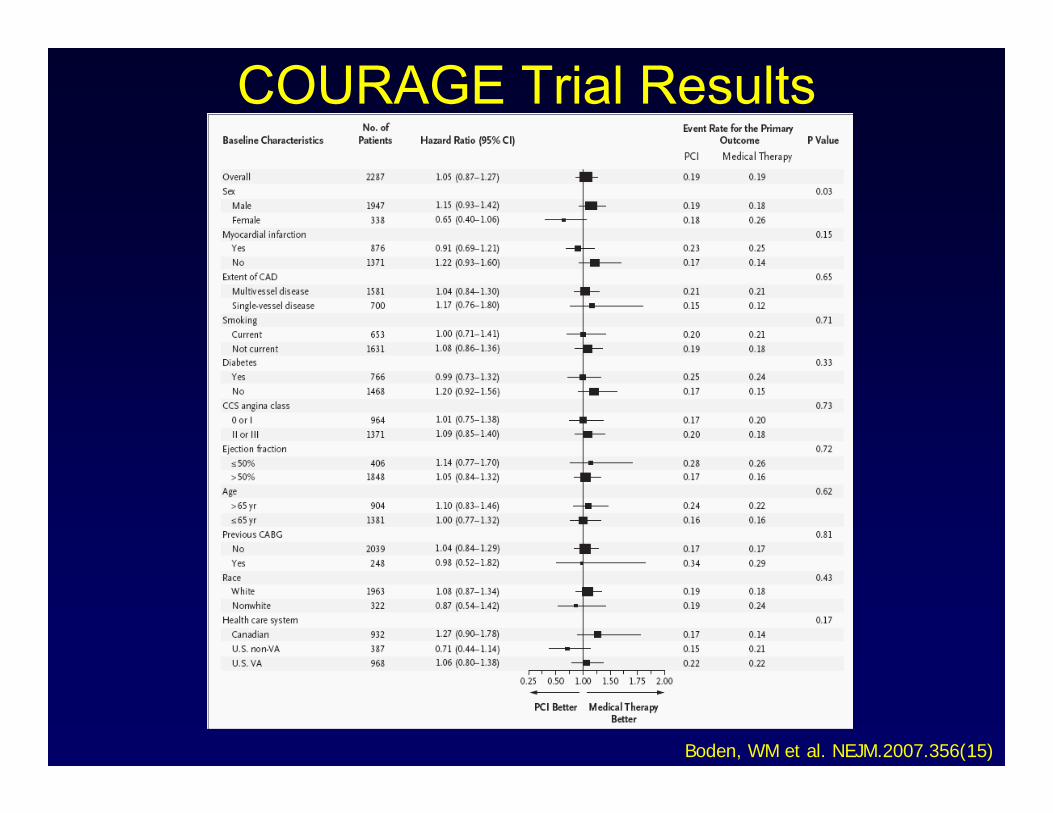
COURAGE Trial Results
Boden, WM et al. NEJM.2007.356(15)
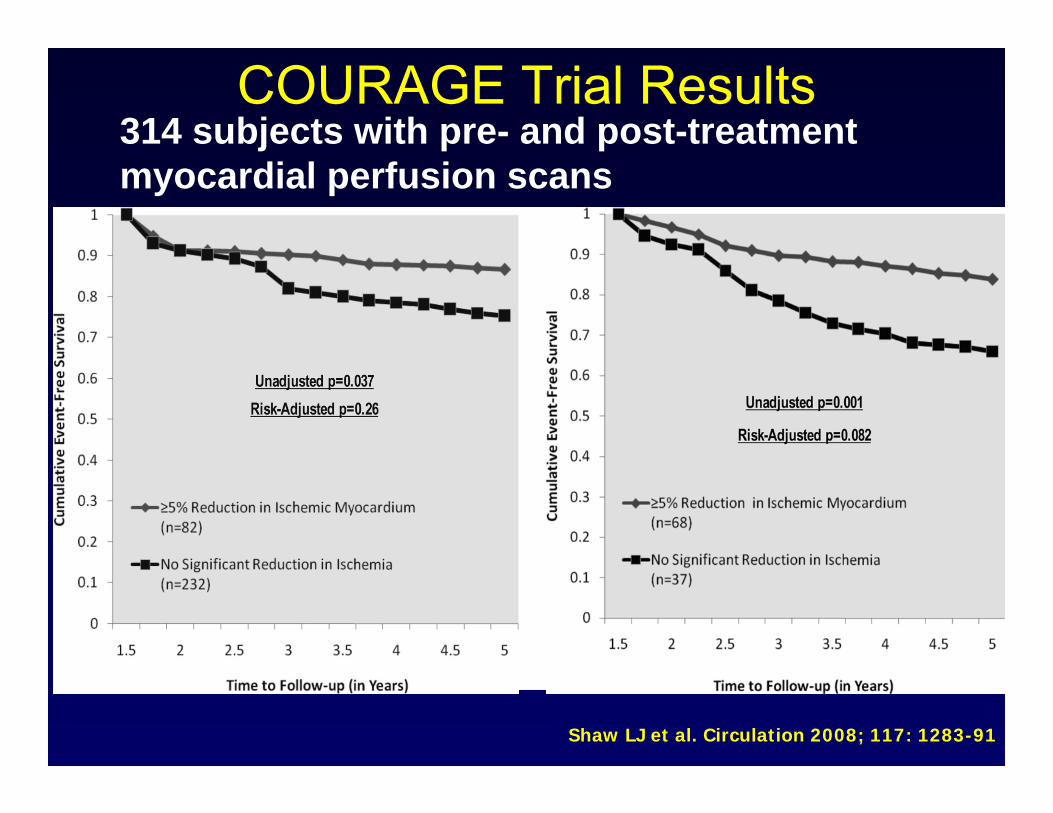
COURAGE Trial Results
Shaw LJ et al. Circulation 2008; 117: 1283-91
314 subjects with pre- and post-treatment myocardial perfusion scans
COURAGE Trial Results
Boden, WM et al. NEJM.2007.356(15)
COURAGE Trial Limitations• <10% of screened patients enrolled• Post-angiography selection bias• OMT superior to “real-life” therapy• 32% of OMT patients “crossed over” to PCI• < 2% patients received drug-eluting stents• > 2/3rds received only single-vessel PCI
(multivessel disease patients undertreated?)
COURAGE Conclusions
When treating patients with chronic stable CAD, an initial strategy of OMT alone:
• Improves anginal symptoms• NOT associated with excess death or MI
(i.e. safe)
compared to OMT+PCI.
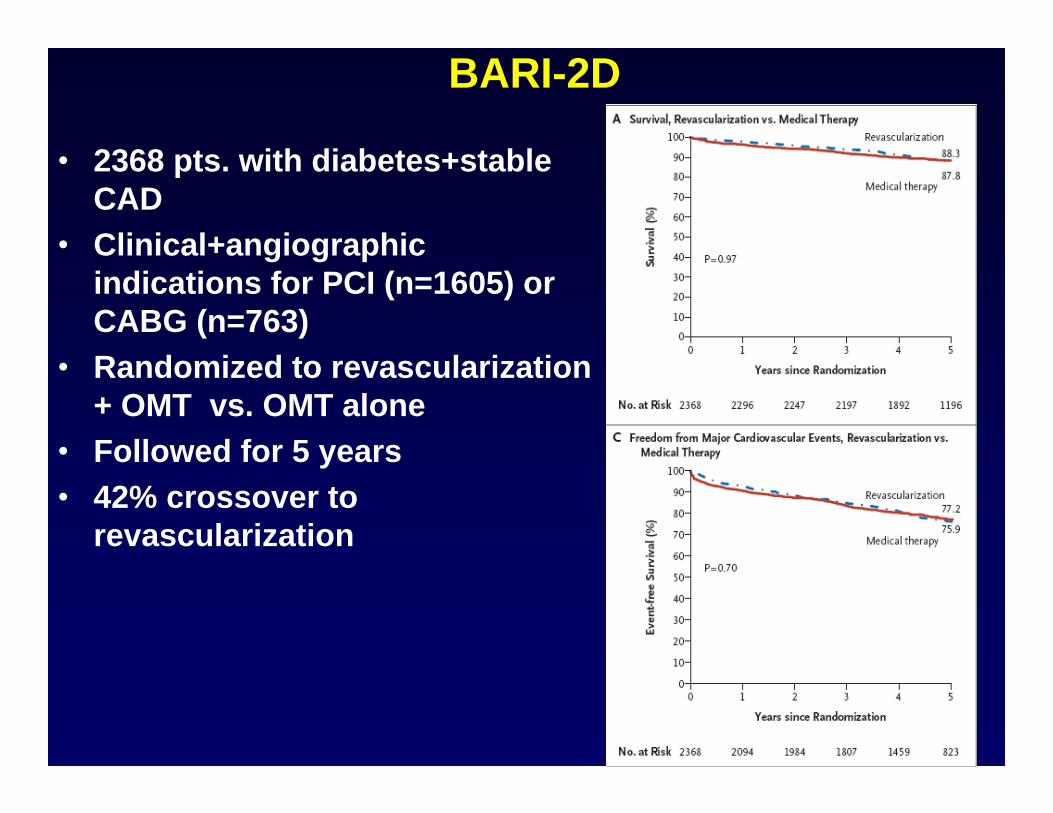
BARI-2D
• 2368 pts. with diabetes+stable CAD
• Clinical+angiographic indications for PCI (n=1605) or CABG (n=763)
• Randomized to revascularization + OMT vs. OMT alone
• Followed for 5 years• 42% crossover to
revascularization
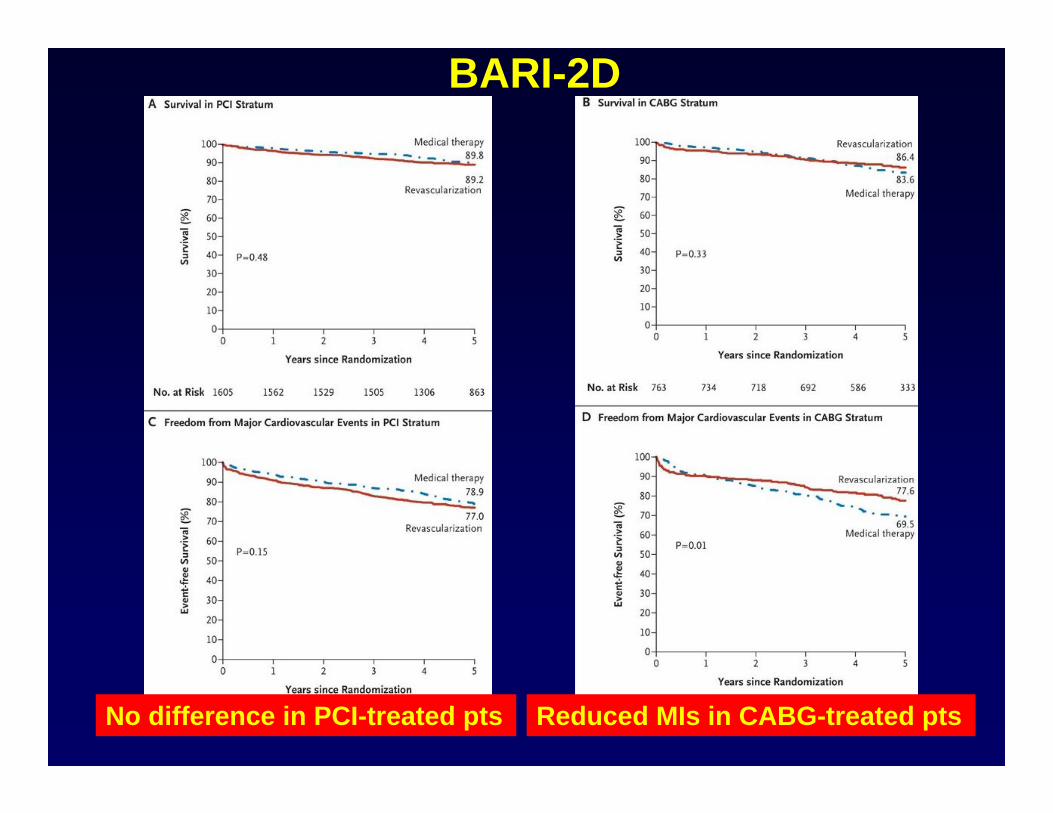
BARI-2D
Reduced MIs in CABG-treated ptsNo difference in PCI-treated pts
BARI 2D Trial Limitations• Post-angiography selection bias• Unknown % of patients screened were actually
enrolled• Relatively low risk patients (mild angina, normal
LVEF)• Low use of DES (35%) and clopidogrel (21%)• CABG vs medical therapy a subgroup analysis of a
negative study (although it was prespecified)
BARI-2D
• OMT alone is a safe initial treatment strategy in patients with diabetes and stable CAD
• CABG, in addition to OMT, may reduce non-fatal MI in clinically-selected patients with diabetes and multi-vessel CAD
Conclusions
OMT vs Revascularization
• OMT alone is a safe initial strategy for many stable CAD patients
• Consider early revascularization in:– Left main > 50%– LVEF < 40%– Persistent/worsening anginal symptoms– 3 vessel disease patients with DM– Large burdens of ischemia on MPI
Conclusions