Embed Size (px)
Citation preview

Instructions for use
Title Effects of coronary revascularization on global coronary flow reserve in stable coronary artery disease
Author(s)Aikawa Tadao Naya Masanao Obara Masahiko Manabe Osamu Magota Keiichi Koyanagawa KazuhiroAsakawa Naoya Ito Yoichi M Shiga Tohru Katoh Chietsugu Anzai Toshihisa Tsutsui Hiroyuki MurthyVenkatesh L Tamaki Nagara
Citation Cardiovascular Research 115(1) 119-129httpsdoiorg101093cvrcvy169
Issue Date 2019-01-01
Doc URL httphdlhandlenet211572289
Rights(URL) httpcreativecommonsorglicensesby-nc40
Type article
Additional Information There are other files related to this item in HUSCAP Check the above URL
File Information cvy169pdf
Hokkaido University Collection of Scholarly and Academic Papers HUSCAP
Effects of coronary revascularization on
global coronary flow reserve in stable
coronary artery disease
Tadao Aikawa1 Masanao Naya1 Masahiko Obara1 Osamu Manabe2
Keiichi Magota3 Kazuhiro Koyanagawa1 Naoya Asakawa1 Yoichi M Ito4
Tohru Shiga2 Chietsugu Katoh5 Toshihisa Anzai1 Hiroyuki Tsutsui6
Venkatesh L Murthy7 and Nagara Tamaki8
1Department of Cardiovascular Medicine Faculty of Medicine Graduate School of Medicine Hokkaido University Kita-15 Nishi-7 Kita-ku Sapporo 060-8638 Japan 2Department ofNuclear Medicine Faculty of Medicine and Graduate School of Medicine Hokkaido University Kita-15 Nishi-7 Kita-ku Sapporo 060-8638 Japan 3Division of Medical Imaging andTechnology Hokkaido University Hospital Sapporo Japan Kita-14 Nishi-5 Kita-ku Sapporo 060-8648 Japan 4Department of Biostatistics Faculty of Medicine Graduate School ofMedicine Hokkaido University Kita-15 Nishi-7 Kita-ku Sapporo 060-8638 Japan 5Department of Biomedical Science and Engineering Faculty of Health Sciences Hokkaido UniversityKita-12 Nishi-5 Kita-ku Sapporo 060-0812 Japan 6Department of Cardiovascular Medicine Kyushu University 3-1-1 Maidashi Higashi-ku Fukuoka 812-8582 Japan 7Divisions ofNuclear Medicine Cardiothoracic Imaging and Cardiovascular Medicine Departments of Medicine and Radiology University of Michigan 1500 E Medical Center Ann Arbor MI 48109USA and 8Department of Radiology Kyoto Prefectural University of Medicine Kajii-cho Kawaramachi-Hirokoji Kamigyo-ku Kyoto 602-8566 Japan
Received 11 April 2018 revised 14 June 2018 editorial decision 28 June 2018 accepted 9 July 2018 online publish-ahead-of-print 10 July 2018
Time for primary review 27 days
Aims Coronary flow reserve (CFR) is an integrated measure of the entire coronary vasculature and is a powerfulprognostic marker in coronary artery disease (CAD) The extent to which coronary revascularization can improveCFR is unclear This study aimed to evaluate the impact of percutaneous coronary intervention (PCI) and coronaryartery bypass grafting (CABG) on CFR in patients with stable CAD
Methodsand results
In a prospective multicentre observational study CFR was measured by 15O-water positron emission tomography asthe ratio of stress to rest myocardial blood flow at baseline and 6 months after optimal medical therapy (OMT) alonePCI or CABG Changes in the SYNTAX and Leaman scores were angiographically evaluated as indicators of com-pleteness of revascularization Follow-up was completed by 75 (25 OMT alone 28 PCI and 22 CABG) out of 82patients The median SYNTAX and Leaman scores and baseline CFR were 145 [interquartile range (IQR) 8ndash245]55 (IQR 25ndash125) and 194 (IQR 167ndash266) respectively Baseline CFR was negatively correlated with theSYNTAX (q = -040 P lt 0001) and Leaman scores (q = -033 P = 0004) Overall only CABG was associated with asignificant increase in CFR [167 (IQR 114ndash196) vs 198 (IQR 160ndash239) P lt 0001] Among patients with CFR lt20(n = 41) CFR significantly increased in the PCI [170 (IQR 142ndash179) vs 221 (IQR 178ndash249) P = 0002 P lt 0001for interaction between time and CFR] and CABG groups [128 (IQR 113ndash180) vs 186 (IQR 157ndash222) P lt 0001]The reduction in SYNTAX or Leaman scores after PCI or CABG was independently associated with the percent in-crease in CFR after adjusting for baseline characteristics (P = 0012 and P = 0011 respectively)
Conclusion Coronary revascularization ameliorated reduced CFR in patients with obstructive CAD The degree of
improvement in angiographic CAD burden by revascularization was correlated with magnitude of improvementin CFR
Keywords Coronary artery disease bull Coronary flow reserve bull Percutaneous coronary intervention bull Coronary artery by-pass grafting bull 15O-water positron emission tomography
Corresponding author Tel thorn81 11 706 6973 fax thorn81 11 706 7874 E-mail nayamedhokudaiacjp
VC The Author(s) 2018 Published by Oxford University Press on behalf of the European Society of CardiologyThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (httpcreativecommonsorglicensesby-nc40) whichpermits non-commercial re-use distribution and reproduction in any medium provided the original work is properly cited For commercial re-use please contactjournalspermissionsoupcom
Cardiovascular Research (2019) 115 119ndash129doi101093cvrcvy169
Dow
nloaded from httpsacadem
icoupcomcardiovascresarticle-abstract11511195051230 by H
okkaido University Library user on 08 January 2019
1 Introduction
Quantitative coronary flow reserve (CFR) calculated as the ratio ofhyperaemic to resting myocardial blood flow (MBF) estimated using dy-namic positron emission tomography (PET) data has emerged as a pow-erful marker of the risk for adverse cardiovascular outcomes includingdeath1ndash3 However the extent to which CFR can be used to select ap-propriate patients with coronary artery disease (CAD) for optimal medi-cal therapy (OMT) percutaneous coronary intervention (PCI) orcoronary artery bypass grafting (CABG) remains unclear Since CFR isan integrated measure of the entire coronary vasculature reflecting epi-cardial coronary anatomy and microvascular dysfunction4 both coro-nary revascularization and medical therapy may increase CFRImportantly several studies have demonstrated that coronaryrevascularization for CAD is associated with early post-proceduralimprovements in regional CFR5ndash8 Conversely in one single-centre ret-rospective study a prognostic difference seen between CABG and PCIwas seen only among patients with very low CFR3 Importantly the in-termediate and long-term effects of PCI or CABG on global CFR andtheir effects on outcomes have not been well explored Therefore weconducted a prospective multicentre observational study to determinethe effects of OMT PCI and CABG on global CFR over 6 months inpatients with CAD
2 Methods
Between July 2015 and August 2017 patients diagnosed with obstructiveCAD defined as a gt_50 diameter stenosis in at least one coronary ar-tery with a reference diameter of gt_15 mm by visual estimation on inva-sive coronary angiography were prospectively identified and recruitedat four centres in Japan Patients with acute coronary syndrome second-or third-degree atrioventricular block bronchial asthma or known orsuspected pregnancy were excluded The study protocol was approvedby the ethics committee of each institution and registered with theUniversity Hospital Medical Information Network clinical trials registry(UMIN000018160 httpwwwuminacjpctrindexhtm) Written in-formed consent was obtained from all patients in accordance with theDeclaration of Helsinki
All patients received guideline-directed OMT9 for patients with ob-structive CAD Stress myocardial perfusion imaging or invasive assess-ment of fractional flow reserve was performed at the cardiologistrsquosdiscretion based on standards of care using previously described meth-ods10 Patients with evidence of ischaemia determined by fractional flowreserve lt_08 or reversible perfusion defects on stress myocardial perfu-sion imaging were considered for coronary revascularization Indicationsfor PCI and CABG were determined based on a heart-team approach ateach institution blinded to the results of MBF and CFR assessmentsPatients undergoing PCI were premedicated with dual antiplatelet ther-apy and treated according to standard practice primarily with drug-eluting stents Patients undergoing CABG received mainly internal mam-mary artery grafts with cardiopulmonary bypass (n = 5) or off-pump(n = 21) All CABG patients were given post-operative aspirinindefinitely
The primary aim of the study was to assess changes in CFR on PET be-fore and 6 months after treatment across treatment groups of OMTalone PCI and CABG in the entire cohort The secondary aim was toidentify significant predictors of change in CFR among baseline character-istics and revascularized CAD burden
21 Positron emission tomographyAll patients were imaged on a whole-body PETcomputed tomography(CT) scanner (Gemini TF 64 Philips Healthcare Cleveland OH USA) atHokkaido University Hospital before and after treatment MBF was mea-sured at rest and during hyperaemia as described previously11 In briefpatients were instructed to fast for at least 4 h and to refrain from caf-feine- and methylxanthine-containing products for at least 24 h Routineantianginal medications were continued A prospectively electrocardio-graphically gated CT scan for coronary artery calcium scoring was per-formed before the PET scan After a low-dose CT scan to correct forattenuation and scatter a 6-min list-mode acquisition was started withconcomitant administration of 500 MBq of 15O-water After a 10-min in-terval for tracer decay an identical scan was repeated during adenosinetriphosphate infusion (016 mgkgmin) Adenosine triphosphate was ini-tiated 3 min before the scan and tracer infusion Heart rate blood pres-sure and 12-lead electrocardiography were recorded at baseline andevery minute during pharmacological stress The emission data werereconstructed using a 3D row-action-maximum-likelihood algorithminto 24 frames (18 10-s and 6 30-s) The estimated radiation expo-sure per examination was 42 mSv including lt01 mSv for the scoutscan 12 mSv for the CT for coronary artery calcium scoring 07 mSvfor the CT for attenuation correction and 11 mSv for each PET scanPET images were analysed using in-house developed software1112 in ablinded fashion MBF (mLgmin) was calculated using a single tissue com-partment model with correction for spillover from the myocardium tothe blood CFR was calculated as the ratio of hyperaemic to resting MBFGlobal CFR lt20 was considered reduced which has been reported asan indicator of high-risk CAD patients12 This value is lower than an-other cut-off point of 25 for detecting haemodynamically significantCAD13 Regional CFR was assessed in the three main coronary arteriesusing the American Heart Association 17-segment model to evaluateCFR in the culprit coronary artery A segment was considered to have is-chaemia when the regional hyperaemic MBF was lt23 which is more di-agnostically accurate than using regional CFR lt25 as the criterion13 Theextent of myocardial ischaemia was expressed as the percentage of theleft ventricle (LV) In addition relative flow reserve defined as the ratioof hyperaemic MBF in a stenotic area (lesion diameter stenosis gt_50) tohyperaemic MBF in a remote area was also calculated in patients withone- or two-vessel disease to minimize the impact of microvascular dys-function on perfusion values1415
22 Angiographic assessmentThe SYNTAX score16 at baseline was calculated in a blinded fashionSince the SYNTAX score was developed for patients without CABGthe CABG SYNTAX score17 was used in patients with CABG An angio-graphically successful PCI was defined as lt50 residual stenosis of thetarget lesion after the procedure The residual SYNTAX score18 orCABG SYNTAX score after revascularization was calculated fromfollow-up angiography If patients did not undergo follow-up angiogra-phy we calculated the residual SYNTAX score from angiography duringPCI and the CABG SYNTAX score from the surgical report in conjunctionwith the baseline angiogram before CABG The pre- and post-procedureanatomical Leaman score was also calculated as previously described19
23 Assessment of left ventricular systolicfunctionEchocardiography was performed by experienced sonographers whowere blinded to the PET results Left ventricular ejection fraction was
120 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
calculated using the biplane method of disks Interpretation was per-formed by cardiologists blinded to the PET results
24 Assessment of cardiovascular riskfactor controlCardiovascular risk factor control for hypertension diabetes hyperlipi-daemia and smoking were performed and assessed on the basis of theBARI 2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes)trial protocol20
25 Statistical analysisContinuous variables are presented as medians with interquartile range(IQR) Categorical variables are presented as absolute numbers withpercentages The sample size calculation was based on the assumptionthat the change in CFR before and after treatment would be 07 withstandard deviation of 10 To detect this change with gt_85 power and asignificance level of 005 each group needed to comprise gt_20 patientsThis sample size was calculated using Power and Sample Size Calculationversion 312 (httpbiostatmcvanderbilteduwikiMainPowerSampleSize) Differences between groups were evaluated using the Wilcoxonrank sum test followed by the Steel-Dwass test for continuous data andthe Fisher exact test for categorical data Differences between paireddata were evaluated using the Wilcoxon signed rank test or theMcNemar test as appropriate A two-way analysis of variance with re-peated measures was used to determine interaction effects BivariateSpearmanrsquos rank correlation coefficients (q) were calculated betweenbaseline CFR and changes in CFR and angiographic indices and theirchanges Before a multivariate regression analysis variables wereassessed for normality by the ShapirondashWilk test and log transformationapplied to correct for skewness as appropriate such as in changes in theLeaman score between pre- and post-revascularization (DLeamanscore) Linear regression analysis was used to examine the associationbetween changes in CFR and revascularized CAD burden [Model 1 in-cluded changes in the SYNTAX score between pre- and post-revascularization (DSYNTAX score) Model 2 included log (1-DLeamanscore)] adjusted for important covariates including the pretest likeli-hood of obstructive CAD history of PCI or CABG and the presence ofleft ventricular systolic dysfunction (left ventricular ejection fractionlt50) selected based on clinical relevance3 and the CABG group Totest the relative contribution of revascularization with CABG on changesin CFR a linear interaction term (DSYNTAX score the CABG group)was added to Model 1 (Model 3) Because of the nonrandomized natureof the study we used percent change as the dependent variable to mini-mize the differences in baseline CFR between groups The pretest likeli-hood of obstructive CAD was estimated using the Duke clinical riskscore21 calculated using age sex type of angina history of myocardial in-farction electrocardiographic Q and ST-T wave changes smokinghyperlipidaemia diabetes and interaction terms (age sex history ofmyocardial infarction electrocardiographic Q wave age smokingage hyperlipidaemia and sex smoking) The assumption of linearityfor continuous covariates was evaluated by plotting the residuals againstthe fitted values As an exploratory analysis propensity score matchingwas used to account for differences in baseline SYNTAX scoresbetween the PCI and CABG groups Propensity scores were calculatedusing a logistic regression model including baseline SYNTAX score andthe same covariates in the multivariate Model 1 (the pretest likelihoodof obstructive CAD history of PCI or CABG and left ventricularejection fraction lt50) A propensity score-matched cohort was
generated by 11 nearest available matching without replacement using acalliper width equal to 02 of the standard deviation of the logit of thepropensity score22 Propensity score matching was performed using theJMP add-in program (httpswwwjmpcomja_jpsupporttechnical-documentshtml) A two-tailed P-value of lt005 was considered statisticallysignificant All statistical analyses were performed using JMP Pro 1310(SAS Institute Inc Cary NC USA)
3 Results
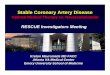
31 Patient characteristicsWe prospectively recruited 82 patients to the study of whom 30 under-went PCI and 26 underwent CABG Of the remaining 26 patients whowere treated with OMT alone 21 had significant comorbidities (eg ad-vanced cancer or severely atheromatous aorta) or unsuitable coronaryanatomy for coronary revascularization three preferred medical ther-apy and two had fixed perfusion defects in the target area on myocardialperfusion imaging We excluded seven patients from the final analysesone patient in the OMT group developed advanced atrioventricularblock during adenosine triphosphate infusion at baseline PET and sixpatients (two in the PCI group and four in the CABG group) withdrewconsent during the follow-up period (Figure 1) Thus the final study co-hort consisted of 75 patients who completed the second PET
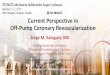
Baseline clinical characteristics are detailed in Table 1 The median ageof the patients was 70 (63ndash75) years 63 patients (84) were men andthe median pretest likelihood of obstructive CAD was 94 (78ndash98)Of these patients 24 (32) had one-vessel disease 22 (29) had two-vessel disease and 29 (39) had three-vessel or left main disease In gen-eral the baseline clinical characteristics were similar between the threegroups The CABG group however had higher SYNTAX and Leamanscores and total ischaemic burden with lower stress MBF and CFR thanthe OMT and PCI groups which reflected the non-randomized study de-sign Figure 2 shows three representative cases
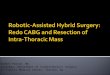
Baseline CFR was negatively correlated with the SYNTAX (q = -040P lt 0001) and Leaman scores (q = -033 P = 0004) (Figure 3) Likewisestress MBF was negatively correlated with the SYNTAX (q = -048P lt 0001) and Leaman scores (q = -044 P lt 0001) whereas rest MBFwas not significantly correlated with either angiographic score(Supplementary material online Figure S1)
32 Changes in coronary risk factor controland angiographic CAD burdenTable 2 shows changes in coronary risk factor control and angiographicCAD burden during a median follow-up duration of 61 (56ndash63)months Overall the number of risk factors achieving the targets washigh at baseline The CABG group showed a significant increase in thepercentage of patients achieving gt_5 risk factor targets which did not dif-fer significantly between the three groups at follow-up Medications atfollow-up are shown in Supplementary material online Table S1
During the follow-up period none of the patients had adverse cardiacevents The symptoms disappeared after the treatment of CAD in 72 of75 patients (96) (Table 2) All 28 patients in the PCI group underwentan angiographically successful PCI In 17 patients undergoing PCI andscheduled follow-up angiography at a median time of 251 (169ndash279)days after PCI 16 had no significant restenosis and one had developedrestenosis and underwent repeated PCI after the second PET In 19patients undergoing CABG and post-operative angiography at a mediantime of 9 (8ndash14) days after CABG one had early saphenous vein graft
Effects of coronary revascularization on global CFR 121D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
occlusion after CABG and underwent additional PCI in the native coro-nary artery before the second PET The SYNTAX and Leaman scores inboth the PCI and CABG groups significantly decreased at follow-up(Table 2) There was no significant difference in the proportion ofpatients with low post-revascularization SYNTAX scores (0ndash8) acrossthe two revascularization groups and the OMT group (Table 2)
33 Changes in CFR and its association withangiographic CAD burdenIn the CABG group stress MBF significantly increased from baseline tofollow-up [122 (095ndash148) mLgmin vs 149 (129ndash169) mLgminP lt 0001] resulting in increased CFR [167 (114ndash196) vs 198 (160ndash239) P lt 0001] (Figure 4AndashC) Conversely both stress MBF and CFR didnot significantly change in the OMT and PCI groups (P gt 005 for all)(Figure 4B and C) Importantly despite baseline differences in CFR CFRat follow-up was not significantly different between the three groups[OMT group 242 (174ndash265) vs PCI group 223 (181ndash250) vs CABGgroup 198 (160ndash239) P = 020] After excluding patients with priormyocardial infarction or coronary revascularization (n = 34) the CFR sig-nificantly increased only in the CABG group [n = 13 171 (117ndash209) vs217 (163ndash242) P = 0002] Supplementary material online Table S2summarizes the haemodynamic characteristics of all patients during eachPET scan
When patients with baseline CFR lt20 (n = 41) were analysed CFRwas found to be significantly increased from baseline to follow-up bothin the PCI group [170 (142ndash179) vs 221 (178ndash249) P = 0002] and inthe CABG group [128 (113ndash180) vs 186 (157ndash222) P lt 0001](Figure 4D) This beneficial effect of PCI on CFR was only observed inpatients with baseline CFR lt20 (P lt 0001 for interaction) (Figure 4D
and 4E) These relationships did not change substantially when patientswere stratified by CFR lt25 and gt_25
When patients with a baseline SYNTAX score gt_23 (n = 23) were ana-lysed CFR was found to be significantly increased from baseline tofollow-up both in the PCI and CABG groups (Figure 4F) while there wasno significant interaction between time and baseline SYNTAX score inthe PCI and CABG groups (P = 011 and P = 099 respectively) Theseresults did not change substantially when patients were categorised intothree SYNTAX subgroups (0ndash22 23ndash32 and gt_33) (Supplementary ma-terial online Table S3)
Among 46 patients with one- or two-vessel disease in this study 17(37) had regional CFR lt20 in a remote area reflecting coronary mi-crovascular dysfunction In nine patients with coronary microvasculardysfunction who underwent PCI (n = 6) or CABG (n = 3) three (one inthe PCI group and two in the CABG group) had global CFR lt20 atfollow-up indicating that their coronary microvascular dysfunction per-sisted after revascularization The small number of patients with one- ortwo-vessel disease prevented a meaningful analysis based on relativeflow reserve values
Figure 5 shows changes in CFR and angiographic CAD burden in thePCI and CABG groups The percent changes in CFR were negatively cor-related with DSYNTAX score (q = -042 P lt 0001) and DLeaman score(q = -044 P lt 0001) The percent changes in CFR and stress MBF werenot significantly correlated with coronary artery calcium scores at base-line (P = 090 and P = 052 respectively)
On a per-vessel basis the percent change in regional CFR after treat-ment was significantly higher in coronary territories receiving CABG[213 (64ndash532)] than those receiving OMT alone [lt50 stenosis-21 (-209ndash182) P lt 0001 and 50ndash100 stenosis -11 (-215ndash
Figure 1 Study flowchart ATP adenosine triphosphate AV atrioventricular CABG coronary artery bypass grafting CAD coronary artery diseaseOMT optimal medical therapy PCI percutaneous coronary intervention PET positron emission tomography
122 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Table 1 Baseline characteristics of the study patients
Variables OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P-value
Age (years) 71 (64ndash79) 71 (65ndash78) 66 (55ndash74) 009
Male 23 (92) 23 (82) 17 (77) 035
Body mass index (kgm2) 234 (201ndash267) 236 (224ndash244) 265 (223ndash290) 010
Pretest likelihood of obstructive CAD () 95 (81ndash99) 90 (78ndash97) 94 (76ndash98) 043
Anginal symptoms 033
Typical angina 13 (52) 13 (46) 11 (50)
Atypical angina 6 (24) 2 (7) 2 (9)
Non-anginal chest pain 1 (4) 1 (4) 0 (0)
Hypertension 19 (76) 20 (71) 19 (86) 048
Diabetes 10 (40) 16 (57) 16 (73) 008
Hyperlipidaemia 18 (72) 22 (79) 18 (82) 078
Family history of CAD 2 (8) 2 (7) 1 (5) 100
Current smoker 4 (16) 4 (14) 5 (23) 074
Prior myocardial infarction 12 (48) 7 (25) 6 (27) 018
Prior PCI 10 (40) 9 (32) 4 (18) 026
Prior CABG 2 (8) 4 (14) 0 (0) 023
Systolic blood pressure (mmHg) 118 (106ndash136) 126 (112ndash137) 120 (108ndash132) 043
Diastolic blood pressure (mmHg) 60 (55ndash75) 64 (58ndash73) 64 (58ndash73) 056
Laboratory data
Total cholesterol (mgdL) 160 (133ndash186) 162 (136ndash184) 161 (138ndash178) 098
HDL cholesterol (mgdL) 52 (42ndash63) 45 (36ndash49) 44 (37ndash54) 013
LDL cholesterol (mgdL) 76 (58ndash110) 89 (68ndash111) 81 (74ndash115) 067
Triglycerides (mgdL) 111 (87ndash150) 122 (87ndash184) 113 (78ndash172) 086
Non-HDL cholesterol (mgdL) 102 (87ndash134) 116 (99ndash140) 107 (95ndash139) 059
Haemoglobin A1c () 60 (56ndash65) 60 (57ndash76) 69 (60ndash74) 024
Echocardiographic LV ejection fraction () 57 (47ndash64) 62 (51ndash67) 59 (34ndash64) 009
Vessels involved lt0001
1-vessel disease 15 (60) 8 (29) 1 (5)
2-vessel disease 7 (28) 12 (43) 3 (14)
3-vessel disease 3 (12) 7 (25) 13 (59)
Left main disease 0 (0) 1 (4) 5 (23)
SYNTAX score 9 (5ndash15) 14 (7ndash22) 29 (23ndash34) lt0001
Leaman score 4 (2ndash7) 4 (2ndash8) 14 (7ndash19) lt0001
Coronary artery calcium score (n = 50) 01ndash400gt400 0510 0413 0711 069
Rest myocardial blood flow (mLgmin) 086 (067ndash101) 080 (060ndash112) 076 (065ndash088) 038
Stress myocardial blood flow (mLgmin) 186 (172ndash235) 174(131ndash214) 122 (095ndash148) lt0001
Coronary flow reserve 238 (183ndash280) 203 (170ndash278) 167 (114ndash196) 0002
Myocardial ischaemia extent (LV) 94 (47ndash100) 94 (65ndash100) 100 (100ndash100) 0005
Medications
Antiplatelet agents 23 (92) 27 (96) 18 (82) 024
Angiotensin inhibitors 16 (64) 18 (64) 14 (64) 100
Beta-blockers 18 (72) 15 (54) 13 (59) 037
Calcium-channel blockers 13 (52) 13 (46) 9 (41) 077
Statins 24 (96) 25 (89) 19 (86) 054
Nitrates 11 (44) 7 (25) 11 (50) 015
Diuretics 8 (32) 6 (21) 8 (36) 051
Insulin 2 (8) 7 (25) 4 (18) 027
Warfarin 2 (8) 2 (7) 1 (5) 100
Data are represented median (interquartile range) or n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL high-density lipoprotein LDL low-density lipoprotein LV left ventricular OMT optimal medical ther-apy PCI percutaneous coronary interventionP lt 005 vs the OMT groupP lt 005 vs the PCI group
Effects of coronary revascularization on global CFR 123D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Figure 2 Eighty-two-year-old man treated with optimal medical therapy alone (A B) A global CFR of 264 at baseline (A) was slightly decreased to 257 atfollow-up (B) Sixty-six-year-old man receiving PCI (C D) The polar map of CFR at baseline (C) shows a regional decrease in the anterior to lateral wallGlobal CFR was modestly increased from 170 to 182 (D) after PCI to the LCX (yellow arrows) Seventy-eight-year-old man receiving CABG (E F) A globalCFR of 123 at baseline (E) was increased to 220 (F) after CABG using a RITA graft to the LAD a left internal thoracic artery graft to the LCX and a SVGgraft from the aorta to the RCA and LCX All grafts were patent 8 days after the CABG (F) CABG coronary artery bypass grafting LAD left anteriordescending artery LCX left circumflex artery LMT left main trunk PCI percutaneous coronary intervention RCA right coronary artery RITA right inter-nal thoracic artery SVG saphenous vein graft
124 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
313) P = 0002] (Figure 6) There was no significant difference in per-cent change in regional CFR between coronary territories receiving PCI[193 (-119ndash407)] and OMT alone (Figure 6) In addition thepercent change in regional CFR after PCI did not differ betweenstenoses with fractional flow reserve lt_08 and those with ischaemia onstress perfusion imaging [-37 (-309ndash654) vs 194 (-116ndash400)P = 086]
34 Predictors of changes in CFR inresponse to coronary revascularizationThe characteristics of patients with increased CFR from baseline tofollow-up compared with those without improvement are summarizedin Supplementary material online Table S4 Independent predictors ofchanges in CFR between baseline and follow-up PET are summarized inTable 3 The DSYNTAX score (Model 1) and DLeaman score (Model 2)were independently associated with changes in CFR Importantly the ex-tent of improvement in angiographic disease burden but not the pretestlikelihood or left ventricular ejection fraction was independently associ-ated with changes in CFR There was no significant interaction between
DSYNTAX score and revascularization with CABG (Model 3) indicatingthat CABG did not amplify the effects of revascularization on CFR
35 Propensity score-matched analysisSupplementary material online Table S5 shows the clinical characteristicsof the matched cohort The two groups (n = 9 in each group) were wellmatched at baseline The CABG group showed a significant increase inCFR [164 (113ndash207) vs 187 (152ndash248) P = 0004] while the PCIgroup did not [178 (147ndash246) vs 234 (147ndash274) P = 050] Althoughthere was no significant interaction between time and the tworevascularization groups (P = 069) probably due to small sample sizethe tendency was consistent with the unmatched cohort
4 Discussion
In this prospective multicentre study we demonstrated thatrevascularization of obstructive CAD improved CFR and stress MBF andthat the degree of improvement was correlated with the degree of re-duction of epicardial CAD burden Importantly these changes were
Figure 3 Relationship between CFR and the SYNTAX score (A) or the Leaman score (B) (A) The vertical dotted line indicates a SYNTAX score of 23
Table 2 Proportion of patients achieving risk factor targets and angiographic completeness of revascularization during thestudy period
OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P (between groups
at follow-up)Baseline Follow-up P Baseline Follow-up P Baseline Follow-up P
Systolic blood pressure lt130 mmHg 17 (68) 16 (64) 071 17 (61) 17 (61) 100 13 (55) 16 (73) 026 072
Diastolic blood pressure lt80 mmHg 22 (88) 21 (84) 065 26 (93) 25 (89) 065 21 (95) 21 (95) 100 052
Non-diabeteshaemoglobin A1c lt70 22 (88) 22 (88) 100 19 (68) 20 (71) 056 13 (59) 16 (73) 018 027
Triglycerides lt150 mgdL 19 (76) 16 (67) 041 19 (68) 19 (68) 100 15 (75) 16 (80) 065 064
Non-HDL-C lt130 mgdL 19 (76) 17 (68) 056 20 (71) 23 (82) 026 16 (73) 19 (86) 026 051
No smoking 21 (84) 22 (88) 032 24 (86) 25 (89) 032 17 (77) 21 (95) 0046 070
Achieving gt_5 risk factor targets 18 (72) 14 (64) 016 13 (46) 19 (68) 008 11 (50) 17 (77) 0034 029
SYNTAX score 0ndash8 12 (48) NA NA 8 (29) 19 (68) lt0001 0 (0) 10 (45) lt0001 022a
Leaman score = 0 3 (12) NA NA 2 (7) 16 (57) lt0001 0 (0) 16 (73) lt0001 lt0001a
Anginal symptoms 20 (80) 2 (8) lt0001 16 (57) 0 (0) lt0001 13 (59) 1 (8) lt0001 038
Values are represented as n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL-C high-density lipoprotein cholesterol LV left ventricular NA not applicable OMT optimal medicaltherapy PCI percutaneous coronary interventionaComparison between the OMT group at baseline and the PCI and CABG groups at follow-up
Effects of coronary revascularization on global CFR 125D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

Effects of coronary revascularization on
global coronary flow reserve in stable
coronary artery disease
Tadao Aikawa1 Masanao Naya1 Masahiko Obara1 Osamu Manabe2
Keiichi Magota3 Kazuhiro Koyanagawa1 Naoya Asakawa1 Yoichi M Ito4
Tohru Shiga2 Chietsugu Katoh5 Toshihisa Anzai1 Hiroyuki Tsutsui6
Venkatesh L Murthy7 and Nagara Tamaki8
1Department of Cardiovascular Medicine Faculty of Medicine Graduate School of Medicine Hokkaido University Kita-15 Nishi-7 Kita-ku Sapporo 060-8638 Japan 2Department ofNuclear Medicine Faculty of Medicine and Graduate School of Medicine Hokkaido University Kita-15 Nishi-7 Kita-ku Sapporo 060-8638 Japan 3Division of Medical Imaging andTechnology Hokkaido University Hospital Sapporo Japan Kita-14 Nishi-5 Kita-ku Sapporo 060-8648 Japan 4Department of Biostatistics Faculty of Medicine Graduate School ofMedicine Hokkaido University Kita-15 Nishi-7 Kita-ku Sapporo 060-8638 Japan 5Department of Biomedical Science and Engineering Faculty of Health Sciences Hokkaido UniversityKita-12 Nishi-5 Kita-ku Sapporo 060-0812 Japan 6Department of Cardiovascular Medicine Kyushu University 3-1-1 Maidashi Higashi-ku Fukuoka 812-8582 Japan 7Divisions ofNuclear Medicine Cardiothoracic Imaging and Cardiovascular Medicine Departments of Medicine and Radiology University of Michigan 1500 E Medical Center Ann Arbor MI 48109USA and 8Department of Radiology Kyoto Prefectural University of Medicine Kajii-cho Kawaramachi-Hirokoji Kamigyo-ku Kyoto 602-8566 Japan
Received 11 April 2018 revised 14 June 2018 editorial decision 28 June 2018 accepted 9 July 2018 online publish-ahead-of-print 10 July 2018
Time for primary review 27 days
Aims Coronary flow reserve (CFR) is an integrated measure of the entire coronary vasculature and is a powerfulprognostic marker in coronary artery disease (CAD) The extent to which coronary revascularization can improveCFR is unclear This study aimed to evaluate the impact of percutaneous coronary intervention (PCI) and coronaryartery bypass grafting (CABG) on CFR in patients with stable CAD
Methodsand results
In a prospective multicentre observational study CFR was measured by 15O-water positron emission tomography asthe ratio of stress to rest myocardial blood flow at baseline and 6 months after optimal medical therapy (OMT) alonePCI or CABG Changes in the SYNTAX and Leaman scores were angiographically evaluated as indicators of com-pleteness of revascularization Follow-up was completed by 75 (25 OMT alone 28 PCI and 22 CABG) out of 82patients The median SYNTAX and Leaman scores and baseline CFR were 145 [interquartile range (IQR) 8ndash245]55 (IQR 25ndash125) and 194 (IQR 167ndash266) respectively Baseline CFR was negatively correlated with theSYNTAX (q = -040 P lt 0001) and Leaman scores (q = -033 P = 0004) Overall only CABG was associated with asignificant increase in CFR [167 (IQR 114ndash196) vs 198 (IQR 160ndash239) P lt 0001] Among patients with CFR lt20(n = 41) CFR significantly increased in the PCI [170 (IQR 142ndash179) vs 221 (IQR 178ndash249) P = 0002 P lt 0001for interaction between time and CFR] and CABG groups [128 (IQR 113ndash180) vs 186 (IQR 157ndash222) P lt 0001]The reduction in SYNTAX or Leaman scores after PCI or CABG was independently associated with the percent in-crease in CFR after adjusting for baseline characteristics (P = 0012 and P = 0011 respectively)
Conclusion Coronary revascularization ameliorated reduced CFR in patients with obstructive CAD The degree of
improvement in angiographic CAD burden by revascularization was correlated with magnitude of improvementin CFR
Keywords Coronary artery disease bull Coronary flow reserve bull Percutaneous coronary intervention bull Coronary artery by-pass grafting bull 15O-water positron emission tomography
Corresponding author Tel thorn81 11 706 6973 fax thorn81 11 706 7874 E-mail nayamedhokudaiacjp
VC The Author(s) 2018 Published by Oxford University Press on behalf of the European Society of CardiologyThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (httpcreativecommonsorglicensesby-nc40) whichpermits non-commercial re-use distribution and reproduction in any medium provided the original work is properly cited For commercial re-use please contactjournalspermissionsoupcom
Cardiovascular Research (2019) 115 119ndash129doi101093cvrcvy169
Dow
nloaded from httpsacadem
icoupcomcardiovascresarticle-abstract11511195051230 by H
okkaido University Library user on 08 January 2019
1 Introduction
Quantitative coronary flow reserve (CFR) calculated as the ratio ofhyperaemic to resting myocardial blood flow (MBF) estimated using dy-namic positron emission tomography (PET) data has emerged as a pow-erful marker of the risk for adverse cardiovascular outcomes includingdeath1ndash3 However the extent to which CFR can be used to select ap-propriate patients with coronary artery disease (CAD) for optimal medi-cal therapy (OMT) percutaneous coronary intervention (PCI) orcoronary artery bypass grafting (CABG) remains unclear Since CFR isan integrated measure of the entire coronary vasculature reflecting epi-cardial coronary anatomy and microvascular dysfunction4 both coro-nary revascularization and medical therapy may increase CFRImportantly several studies have demonstrated that coronaryrevascularization for CAD is associated with early post-proceduralimprovements in regional CFR5ndash8 Conversely in one single-centre ret-rospective study a prognostic difference seen between CABG and PCIwas seen only among patients with very low CFR3 Importantly the in-termediate and long-term effects of PCI or CABG on global CFR andtheir effects on outcomes have not been well explored Therefore weconducted a prospective multicentre observational study to determinethe effects of OMT PCI and CABG on global CFR over 6 months inpatients with CAD
2 Methods
Between July 2015 and August 2017 patients diagnosed with obstructiveCAD defined as a gt_50 diameter stenosis in at least one coronary ar-tery with a reference diameter of gt_15 mm by visual estimation on inva-sive coronary angiography were prospectively identified and recruitedat four centres in Japan Patients with acute coronary syndrome second-or third-degree atrioventricular block bronchial asthma or known orsuspected pregnancy were excluded The study protocol was approvedby the ethics committee of each institution and registered with theUniversity Hospital Medical Information Network clinical trials registry(UMIN000018160 httpwwwuminacjpctrindexhtm) Written in-formed consent was obtained from all patients in accordance with theDeclaration of Helsinki
All patients received guideline-directed OMT9 for patients with ob-structive CAD Stress myocardial perfusion imaging or invasive assess-ment of fractional flow reserve was performed at the cardiologistrsquosdiscretion based on standards of care using previously described meth-ods10 Patients with evidence of ischaemia determined by fractional flowreserve lt_08 or reversible perfusion defects on stress myocardial perfu-sion imaging were considered for coronary revascularization Indicationsfor PCI and CABG were determined based on a heart-team approach ateach institution blinded to the results of MBF and CFR assessmentsPatients undergoing PCI were premedicated with dual antiplatelet ther-apy and treated according to standard practice primarily with drug-eluting stents Patients undergoing CABG received mainly internal mam-mary artery grafts with cardiopulmonary bypass (n = 5) or off-pump(n = 21) All CABG patients were given post-operative aspirinindefinitely
The primary aim of the study was to assess changes in CFR on PET be-fore and 6 months after treatment across treatment groups of OMTalone PCI and CABG in the entire cohort The secondary aim was toidentify significant predictors of change in CFR among baseline character-istics and revascularized CAD burden
21 Positron emission tomographyAll patients were imaged on a whole-body PETcomputed tomography(CT) scanner (Gemini TF 64 Philips Healthcare Cleveland OH USA) atHokkaido University Hospital before and after treatment MBF was mea-sured at rest and during hyperaemia as described previously11 In briefpatients were instructed to fast for at least 4 h and to refrain from caf-feine- and methylxanthine-containing products for at least 24 h Routineantianginal medications were continued A prospectively electrocardio-graphically gated CT scan for coronary artery calcium scoring was per-formed before the PET scan After a low-dose CT scan to correct forattenuation and scatter a 6-min list-mode acquisition was started withconcomitant administration of 500 MBq of 15O-water After a 10-min in-terval for tracer decay an identical scan was repeated during adenosinetriphosphate infusion (016 mgkgmin) Adenosine triphosphate was ini-tiated 3 min before the scan and tracer infusion Heart rate blood pres-sure and 12-lead electrocardiography were recorded at baseline andevery minute during pharmacological stress The emission data werereconstructed using a 3D row-action-maximum-likelihood algorithminto 24 frames (18 10-s and 6 30-s) The estimated radiation expo-sure per examination was 42 mSv including lt01 mSv for the scoutscan 12 mSv for the CT for coronary artery calcium scoring 07 mSvfor the CT for attenuation correction and 11 mSv for each PET scanPET images were analysed using in-house developed software1112 in ablinded fashion MBF (mLgmin) was calculated using a single tissue com-partment model with correction for spillover from the myocardium tothe blood CFR was calculated as the ratio of hyperaemic to resting MBFGlobal CFR lt20 was considered reduced which has been reported asan indicator of high-risk CAD patients12 This value is lower than an-other cut-off point of 25 for detecting haemodynamically significantCAD13 Regional CFR was assessed in the three main coronary arteriesusing the American Heart Association 17-segment model to evaluateCFR in the culprit coronary artery A segment was considered to have is-chaemia when the regional hyperaemic MBF was lt23 which is more di-agnostically accurate than using regional CFR lt25 as the criterion13 Theextent of myocardial ischaemia was expressed as the percentage of theleft ventricle (LV) In addition relative flow reserve defined as the ratioof hyperaemic MBF in a stenotic area (lesion diameter stenosis gt_50) tohyperaemic MBF in a remote area was also calculated in patients withone- or two-vessel disease to minimize the impact of microvascular dys-function on perfusion values1415
22 Angiographic assessmentThe SYNTAX score16 at baseline was calculated in a blinded fashionSince the SYNTAX score was developed for patients without CABGthe CABG SYNTAX score17 was used in patients with CABG An angio-graphically successful PCI was defined as lt50 residual stenosis of thetarget lesion after the procedure The residual SYNTAX score18 orCABG SYNTAX score after revascularization was calculated fromfollow-up angiography If patients did not undergo follow-up angiogra-phy we calculated the residual SYNTAX score from angiography duringPCI and the CABG SYNTAX score from the surgical report in conjunctionwith the baseline angiogram before CABG The pre- and post-procedureanatomical Leaman score was also calculated as previously described19
23 Assessment of left ventricular systolicfunctionEchocardiography was performed by experienced sonographers whowere blinded to the PET results Left ventricular ejection fraction was
120 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
calculated using the biplane method of disks Interpretation was per-formed by cardiologists blinded to the PET results
24 Assessment of cardiovascular riskfactor controlCardiovascular risk factor control for hypertension diabetes hyperlipi-daemia and smoking were performed and assessed on the basis of theBARI 2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes)trial protocol20
25 Statistical analysisContinuous variables are presented as medians with interquartile range(IQR) Categorical variables are presented as absolute numbers withpercentages The sample size calculation was based on the assumptionthat the change in CFR before and after treatment would be 07 withstandard deviation of 10 To detect this change with gt_85 power and asignificance level of 005 each group needed to comprise gt_20 patientsThis sample size was calculated using Power and Sample Size Calculationversion 312 (httpbiostatmcvanderbilteduwikiMainPowerSampleSize) Differences between groups were evaluated using the Wilcoxonrank sum test followed by the Steel-Dwass test for continuous data andthe Fisher exact test for categorical data Differences between paireddata were evaluated using the Wilcoxon signed rank test or theMcNemar test as appropriate A two-way analysis of variance with re-peated measures was used to determine interaction effects BivariateSpearmanrsquos rank correlation coefficients (q) were calculated betweenbaseline CFR and changes in CFR and angiographic indices and theirchanges Before a multivariate regression analysis variables wereassessed for normality by the ShapirondashWilk test and log transformationapplied to correct for skewness as appropriate such as in changes in theLeaman score between pre- and post-revascularization (DLeamanscore) Linear regression analysis was used to examine the associationbetween changes in CFR and revascularized CAD burden [Model 1 in-cluded changes in the SYNTAX score between pre- and post-revascularization (DSYNTAX score) Model 2 included log (1-DLeamanscore)] adjusted for important covariates including the pretest likeli-hood of obstructive CAD history of PCI or CABG and the presence ofleft ventricular systolic dysfunction (left ventricular ejection fractionlt50) selected based on clinical relevance3 and the CABG group Totest the relative contribution of revascularization with CABG on changesin CFR a linear interaction term (DSYNTAX score the CABG group)was added to Model 1 (Model 3) Because of the nonrandomized natureof the study we used percent change as the dependent variable to mini-mize the differences in baseline CFR between groups The pretest likeli-hood of obstructive CAD was estimated using the Duke clinical riskscore21 calculated using age sex type of angina history of myocardial in-farction electrocardiographic Q and ST-T wave changes smokinghyperlipidaemia diabetes and interaction terms (age sex history ofmyocardial infarction electrocardiographic Q wave age smokingage hyperlipidaemia and sex smoking) The assumption of linearityfor continuous covariates was evaluated by plotting the residuals againstthe fitted values As an exploratory analysis propensity score matchingwas used to account for differences in baseline SYNTAX scoresbetween the PCI and CABG groups Propensity scores were calculatedusing a logistic regression model including baseline SYNTAX score andthe same covariates in the multivariate Model 1 (the pretest likelihoodof obstructive CAD history of PCI or CABG and left ventricularejection fraction lt50) A propensity score-matched cohort was
generated by 11 nearest available matching without replacement using acalliper width equal to 02 of the standard deviation of the logit of thepropensity score22 Propensity score matching was performed using theJMP add-in program (httpswwwjmpcomja_jpsupporttechnical-documentshtml) A two-tailed P-value of lt005 was considered statisticallysignificant All statistical analyses were performed using JMP Pro 1310(SAS Institute Inc Cary NC USA)
3 Results
31 Patient characteristicsWe prospectively recruited 82 patients to the study of whom 30 under-went PCI and 26 underwent CABG Of the remaining 26 patients whowere treated with OMT alone 21 had significant comorbidities (eg ad-vanced cancer or severely atheromatous aorta) or unsuitable coronaryanatomy for coronary revascularization three preferred medical ther-apy and two had fixed perfusion defects in the target area on myocardialperfusion imaging We excluded seven patients from the final analysesone patient in the OMT group developed advanced atrioventricularblock during adenosine triphosphate infusion at baseline PET and sixpatients (two in the PCI group and four in the CABG group) withdrewconsent during the follow-up period (Figure 1) Thus the final study co-hort consisted of 75 patients who completed the second PET
Baseline clinical characteristics are detailed in Table 1 The median ageof the patients was 70 (63ndash75) years 63 patients (84) were men andthe median pretest likelihood of obstructive CAD was 94 (78ndash98)Of these patients 24 (32) had one-vessel disease 22 (29) had two-vessel disease and 29 (39) had three-vessel or left main disease In gen-eral the baseline clinical characteristics were similar between the threegroups The CABG group however had higher SYNTAX and Leamanscores and total ischaemic burden with lower stress MBF and CFR thanthe OMT and PCI groups which reflected the non-randomized study de-sign Figure 2 shows three representative cases
Baseline CFR was negatively correlated with the SYNTAX (q = -040P lt 0001) and Leaman scores (q = -033 P = 0004) (Figure 3) Likewisestress MBF was negatively correlated with the SYNTAX (q = -048P lt 0001) and Leaman scores (q = -044 P lt 0001) whereas rest MBFwas not significantly correlated with either angiographic score(Supplementary material online Figure S1)
32 Changes in coronary risk factor controland angiographic CAD burdenTable 2 shows changes in coronary risk factor control and angiographicCAD burden during a median follow-up duration of 61 (56ndash63)months Overall the number of risk factors achieving the targets washigh at baseline The CABG group showed a significant increase in thepercentage of patients achieving gt_5 risk factor targets which did not dif-fer significantly between the three groups at follow-up Medications atfollow-up are shown in Supplementary material online Table S1
During the follow-up period none of the patients had adverse cardiacevents The symptoms disappeared after the treatment of CAD in 72 of75 patients (96) (Table 2) All 28 patients in the PCI group underwentan angiographically successful PCI In 17 patients undergoing PCI andscheduled follow-up angiography at a median time of 251 (169ndash279)days after PCI 16 had no significant restenosis and one had developedrestenosis and underwent repeated PCI after the second PET In 19patients undergoing CABG and post-operative angiography at a mediantime of 9 (8ndash14) days after CABG one had early saphenous vein graft
Effects of coronary revascularization on global CFR 121D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
occlusion after CABG and underwent additional PCI in the native coro-nary artery before the second PET The SYNTAX and Leaman scores inboth the PCI and CABG groups significantly decreased at follow-up(Table 2) There was no significant difference in the proportion ofpatients with low post-revascularization SYNTAX scores (0ndash8) acrossthe two revascularization groups and the OMT group (Table 2)
33 Changes in CFR and its association withangiographic CAD burdenIn the CABG group stress MBF significantly increased from baseline tofollow-up [122 (095ndash148) mLgmin vs 149 (129ndash169) mLgminP lt 0001] resulting in increased CFR [167 (114ndash196) vs 198 (160ndash239) P lt 0001] (Figure 4AndashC) Conversely both stress MBF and CFR didnot significantly change in the OMT and PCI groups (P gt 005 for all)(Figure 4B and C) Importantly despite baseline differences in CFR CFRat follow-up was not significantly different between the three groups[OMT group 242 (174ndash265) vs PCI group 223 (181ndash250) vs CABGgroup 198 (160ndash239) P = 020] After excluding patients with priormyocardial infarction or coronary revascularization (n = 34) the CFR sig-nificantly increased only in the CABG group [n = 13 171 (117ndash209) vs217 (163ndash242) P = 0002] Supplementary material online Table S2summarizes the haemodynamic characteristics of all patients during eachPET scan
When patients with baseline CFR lt20 (n = 41) were analysed CFRwas found to be significantly increased from baseline to follow-up bothin the PCI group [170 (142ndash179) vs 221 (178ndash249) P = 0002] and inthe CABG group [128 (113ndash180) vs 186 (157ndash222) P lt 0001](Figure 4D) This beneficial effect of PCI on CFR was only observed inpatients with baseline CFR lt20 (P lt 0001 for interaction) (Figure 4D
and 4E) These relationships did not change substantially when patientswere stratified by CFR lt25 and gt_25
When patients with a baseline SYNTAX score gt_23 (n = 23) were ana-lysed CFR was found to be significantly increased from baseline tofollow-up both in the PCI and CABG groups (Figure 4F) while there wasno significant interaction between time and baseline SYNTAX score inthe PCI and CABG groups (P = 011 and P = 099 respectively) Theseresults did not change substantially when patients were categorised intothree SYNTAX subgroups (0ndash22 23ndash32 and gt_33) (Supplementary ma-terial online Table S3)
Among 46 patients with one- or two-vessel disease in this study 17(37) had regional CFR lt20 in a remote area reflecting coronary mi-crovascular dysfunction In nine patients with coronary microvasculardysfunction who underwent PCI (n = 6) or CABG (n = 3) three (one inthe PCI group and two in the CABG group) had global CFR lt20 atfollow-up indicating that their coronary microvascular dysfunction per-sisted after revascularization The small number of patients with one- ortwo-vessel disease prevented a meaningful analysis based on relativeflow reserve values
Figure 5 shows changes in CFR and angiographic CAD burden in thePCI and CABG groups The percent changes in CFR were negatively cor-related with DSYNTAX score (q = -042 P lt 0001) and DLeaman score(q = -044 P lt 0001) The percent changes in CFR and stress MBF werenot significantly correlated with coronary artery calcium scores at base-line (P = 090 and P = 052 respectively)
On a per-vessel basis the percent change in regional CFR after treat-ment was significantly higher in coronary territories receiving CABG[213 (64ndash532)] than those receiving OMT alone [lt50 stenosis-21 (-209ndash182) P lt 0001 and 50ndash100 stenosis -11 (-215ndash
Figure 1 Study flowchart ATP adenosine triphosphate AV atrioventricular CABG coronary artery bypass grafting CAD coronary artery diseaseOMT optimal medical therapy PCI percutaneous coronary intervention PET positron emission tomography
122 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Table 1 Baseline characteristics of the study patients
Variables OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P-value
Age (years) 71 (64ndash79) 71 (65ndash78) 66 (55ndash74) 009
Male 23 (92) 23 (82) 17 (77) 035
Body mass index (kgm2) 234 (201ndash267) 236 (224ndash244) 265 (223ndash290) 010
Pretest likelihood of obstructive CAD () 95 (81ndash99) 90 (78ndash97) 94 (76ndash98) 043
Anginal symptoms 033
Typical angina 13 (52) 13 (46) 11 (50)
Atypical angina 6 (24) 2 (7) 2 (9)
Non-anginal chest pain 1 (4) 1 (4) 0 (0)
Hypertension 19 (76) 20 (71) 19 (86) 048
Diabetes 10 (40) 16 (57) 16 (73) 008
Hyperlipidaemia 18 (72) 22 (79) 18 (82) 078
Family history of CAD 2 (8) 2 (7) 1 (5) 100
Current smoker 4 (16) 4 (14) 5 (23) 074
Prior myocardial infarction 12 (48) 7 (25) 6 (27) 018
Prior PCI 10 (40) 9 (32) 4 (18) 026
Prior CABG 2 (8) 4 (14) 0 (0) 023
Systolic blood pressure (mmHg) 118 (106ndash136) 126 (112ndash137) 120 (108ndash132) 043
Diastolic blood pressure (mmHg) 60 (55ndash75) 64 (58ndash73) 64 (58ndash73) 056
Laboratory data
Total cholesterol (mgdL) 160 (133ndash186) 162 (136ndash184) 161 (138ndash178) 098
HDL cholesterol (mgdL) 52 (42ndash63) 45 (36ndash49) 44 (37ndash54) 013
LDL cholesterol (mgdL) 76 (58ndash110) 89 (68ndash111) 81 (74ndash115) 067
Triglycerides (mgdL) 111 (87ndash150) 122 (87ndash184) 113 (78ndash172) 086
Non-HDL cholesterol (mgdL) 102 (87ndash134) 116 (99ndash140) 107 (95ndash139) 059
Haemoglobin A1c () 60 (56ndash65) 60 (57ndash76) 69 (60ndash74) 024
Echocardiographic LV ejection fraction () 57 (47ndash64) 62 (51ndash67) 59 (34ndash64) 009
Vessels involved lt0001
1-vessel disease 15 (60) 8 (29) 1 (5)
2-vessel disease 7 (28) 12 (43) 3 (14)
3-vessel disease 3 (12) 7 (25) 13 (59)
Left main disease 0 (0) 1 (4) 5 (23)
SYNTAX score 9 (5ndash15) 14 (7ndash22) 29 (23ndash34) lt0001
Leaman score 4 (2ndash7) 4 (2ndash8) 14 (7ndash19) lt0001
Coronary artery calcium score (n = 50) 01ndash400gt400 0510 0413 0711 069
Rest myocardial blood flow (mLgmin) 086 (067ndash101) 080 (060ndash112) 076 (065ndash088) 038
Stress myocardial blood flow (mLgmin) 186 (172ndash235) 174(131ndash214) 122 (095ndash148) lt0001
Coronary flow reserve 238 (183ndash280) 203 (170ndash278) 167 (114ndash196) 0002
Myocardial ischaemia extent (LV) 94 (47ndash100) 94 (65ndash100) 100 (100ndash100) 0005
Medications
Antiplatelet agents 23 (92) 27 (96) 18 (82) 024
Angiotensin inhibitors 16 (64) 18 (64) 14 (64) 100
Beta-blockers 18 (72) 15 (54) 13 (59) 037
Calcium-channel blockers 13 (52) 13 (46) 9 (41) 077
Statins 24 (96) 25 (89) 19 (86) 054
Nitrates 11 (44) 7 (25) 11 (50) 015
Diuretics 8 (32) 6 (21) 8 (36) 051
Insulin 2 (8) 7 (25) 4 (18) 027
Warfarin 2 (8) 2 (7) 1 (5) 100
Data are represented median (interquartile range) or n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL high-density lipoprotein LDL low-density lipoprotein LV left ventricular OMT optimal medical ther-apy PCI percutaneous coronary interventionP lt 005 vs the OMT groupP lt 005 vs the PCI group
Effects of coronary revascularization on global CFR 123D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Figure 2 Eighty-two-year-old man treated with optimal medical therapy alone (A B) A global CFR of 264 at baseline (A) was slightly decreased to 257 atfollow-up (B) Sixty-six-year-old man receiving PCI (C D) The polar map of CFR at baseline (C) shows a regional decrease in the anterior to lateral wallGlobal CFR was modestly increased from 170 to 182 (D) after PCI to the LCX (yellow arrows) Seventy-eight-year-old man receiving CABG (E F) A globalCFR of 123 at baseline (E) was increased to 220 (F) after CABG using a RITA graft to the LAD a left internal thoracic artery graft to the LCX and a SVGgraft from the aorta to the RCA and LCX All grafts were patent 8 days after the CABG (F) CABG coronary artery bypass grafting LAD left anteriordescending artery LCX left circumflex artery LMT left main trunk PCI percutaneous coronary intervention RCA right coronary artery RITA right inter-nal thoracic artery SVG saphenous vein graft
124 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
313) P = 0002] (Figure 6) There was no significant difference in per-cent change in regional CFR between coronary territories receiving PCI[193 (-119ndash407)] and OMT alone (Figure 6) In addition thepercent change in regional CFR after PCI did not differ betweenstenoses with fractional flow reserve lt_08 and those with ischaemia onstress perfusion imaging [-37 (-309ndash654) vs 194 (-116ndash400)P = 086]
34 Predictors of changes in CFR inresponse to coronary revascularizationThe characteristics of patients with increased CFR from baseline tofollow-up compared with those without improvement are summarizedin Supplementary material online Table S4 Independent predictors ofchanges in CFR between baseline and follow-up PET are summarized inTable 3 The DSYNTAX score (Model 1) and DLeaman score (Model 2)were independently associated with changes in CFR Importantly the ex-tent of improvement in angiographic disease burden but not the pretestlikelihood or left ventricular ejection fraction was independently associ-ated with changes in CFR There was no significant interaction between
DSYNTAX score and revascularization with CABG (Model 3) indicatingthat CABG did not amplify the effects of revascularization on CFR
35 Propensity score-matched analysisSupplementary material online Table S5 shows the clinical characteristicsof the matched cohort The two groups (n = 9 in each group) were wellmatched at baseline The CABG group showed a significant increase inCFR [164 (113ndash207) vs 187 (152ndash248) P = 0004] while the PCIgroup did not [178 (147ndash246) vs 234 (147ndash274) P = 050] Althoughthere was no significant interaction between time and the tworevascularization groups (P = 069) probably due to small sample sizethe tendency was consistent with the unmatched cohort
4 Discussion
In this prospective multicentre study we demonstrated thatrevascularization of obstructive CAD improved CFR and stress MBF andthat the degree of improvement was correlated with the degree of re-duction of epicardial CAD burden Importantly these changes were
Figure 3 Relationship between CFR and the SYNTAX score (A) or the Leaman score (B) (A) The vertical dotted line indicates a SYNTAX score of 23
Table 2 Proportion of patients achieving risk factor targets and angiographic completeness of revascularization during thestudy period
OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P (between groups
at follow-up)Baseline Follow-up P Baseline Follow-up P Baseline Follow-up P
Systolic blood pressure lt130 mmHg 17 (68) 16 (64) 071 17 (61) 17 (61) 100 13 (55) 16 (73) 026 072
Diastolic blood pressure lt80 mmHg 22 (88) 21 (84) 065 26 (93) 25 (89) 065 21 (95) 21 (95) 100 052
Non-diabeteshaemoglobin A1c lt70 22 (88) 22 (88) 100 19 (68) 20 (71) 056 13 (59) 16 (73) 018 027
Triglycerides lt150 mgdL 19 (76) 16 (67) 041 19 (68) 19 (68) 100 15 (75) 16 (80) 065 064
Non-HDL-C lt130 mgdL 19 (76) 17 (68) 056 20 (71) 23 (82) 026 16 (73) 19 (86) 026 051
No smoking 21 (84) 22 (88) 032 24 (86) 25 (89) 032 17 (77) 21 (95) 0046 070
Achieving gt_5 risk factor targets 18 (72) 14 (64) 016 13 (46) 19 (68) 008 11 (50) 17 (77) 0034 029
SYNTAX score 0ndash8 12 (48) NA NA 8 (29) 19 (68) lt0001 0 (0) 10 (45) lt0001 022a
Leaman score = 0 3 (12) NA NA 2 (7) 16 (57) lt0001 0 (0) 16 (73) lt0001 lt0001a
Anginal symptoms 20 (80) 2 (8) lt0001 16 (57) 0 (0) lt0001 13 (59) 1 (8) lt0001 038
Values are represented as n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL-C high-density lipoprotein cholesterol LV left ventricular NA not applicable OMT optimal medicaltherapy PCI percutaneous coronary interventionaComparison between the OMT group at baseline and the PCI and CABG groups at follow-up
Effects of coronary revascularization on global CFR 125D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

1 Introduction
Quantitative coronary flow reserve (CFR) calculated as the ratio ofhyperaemic to resting myocardial blood flow (MBF) estimated using dy-namic positron emission tomography (PET) data has emerged as a pow-erful marker of the risk for adverse cardiovascular outcomes includingdeath1ndash3 However the extent to which CFR can be used to select ap-propriate patients with coronary artery disease (CAD) for optimal medi-cal therapy (OMT) percutaneous coronary intervention (PCI) orcoronary artery bypass grafting (CABG) remains unclear Since CFR isan integrated measure of the entire coronary vasculature reflecting epi-cardial coronary anatomy and microvascular dysfunction4 both coro-nary revascularization and medical therapy may increase CFRImportantly several studies have demonstrated that coronaryrevascularization for CAD is associated with early post-proceduralimprovements in regional CFR5ndash8 Conversely in one single-centre ret-rospective study a prognostic difference seen between CABG and PCIwas seen only among patients with very low CFR3 Importantly the in-termediate and long-term effects of PCI or CABG on global CFR andtheir effects on outcomes have not been well explored Therefore weconducted a prospective multicentre observational study to determinethe effects of OMT PCI and CABG on global CFR over 6 months inpatients with CAD
2 Methods
Between July 2015 and August 2017 patients diagnosed with obstructiveCAD defined as a gt_50 diameter stenosis in at least one coronary ar-tery with a reference diameter of gt_15 mm by visual estimation on inva-sive coronary angiography were prospectively identified and recruitedat four centres in Japan Patients with acute coronary syndrome second-or third-degree atrioventricular block bronchial asthma or known orsuspected pregnancy were excluded The study protocol was approvedby the ethics committee of each institution and registered with theUniversity Hospital Medical Information Network clinical trials registry(UMIN000018160 httpwwwuminacjpctrindexhtm) Written in-formed consent was obtained from all patients in accordance with theDeclaration of Helsinki
All patients received guideline-directed OMT9 for patients with ob-structive CAD Stress myocardial perfusion imaging or invasive assess-ment of fractional flow reserve was performed at the cardiologistrsquosdiscretion based on standards of care using previously described meth-ods10 Patients with evidence of ischaemia determined by fractional flowreserve lt_08 or reversible perfusion defects on stress myocardial perfu-sion imaging were considered for coronary revascularization Indicationsfor PCI and CABG were determined based on a heart-team approach ateach institution blinded to the results of MBF and CFR assessmentsPatients undergoing PCI were premedicated with dual antiplatelet ther-apy and treated according to standard practice primarily with drug-eluting stents Patients undergoing CABG received mainly internal mam-mary artery grafts with cardiopulmonary bypass (n = 5) or off-pump(n = 21) All CABG patients were given post-operative aspirinindefinitely
The primary aim of the study was to assess changes in CFR on PET be-fore and 6 months after treatment across treatment groups of OMTalone PCI and CABG in the entire cohort The secondary aim was toidentify significant predictors of change in CFR among baseline character-istics and revascularized CAD burden
21 Positron emission tomographyAll patients were imaged on a whole-body PETcomputed tomography(CT) scanner (Gemini TF 64 Philips Healthcare Cleveland OH USA) atHokkaido University Hospital before and after treatment MBF was mea-sured at rest and during hyperaemia as described previously11 In briefpatients were instructed to fast for at least 4 h and to refrain from caf-feine- and methylxanthine-containing products for at least 24 h Routineantianginal medications were continued A prospectively electrocardio-graphically gated CT scan for coronary artery calcium scoring was per-formed before the PET scan After a low-dose CT scan to correct forattenuation and scatter a 6-min list-mode acquisition was started withconcomitant administration of 500 MBq of 15O-water After a 10-min in-terval for tracer decay an identical scan was repeated during adenosinetriphosphate infusion (016 mgkgmin) Adenosine triphosphate was ini-tiated 3 min before the scan and tracer infusion Heart rate blood pres-sure and 12-lead electrocardiography were recorded at baseline andevery minute during pharmacological stress The emission data werereconstructed using a 3D row-action-maximum-likelihood algorithminto 24 frames (18 10-s and 6 30-s) The estimated radiation expo-sure per examination was 42 mSv including lt01 mSv for the scoutscan 12 mSv for the CT for coronary artery calcium scoring 07 mSvfor the CT for attenuation correction and 11 mSv for each PET scanPET images were analysed using in-house developed software1112 in ablinded fashion MBF (mLgmin) was calculated using a single tissue com-partment model with correction for spillover from the myocardium tothe blood CFR was calculated as the ratio of hyperaemic to resting MBFGlobal CFR lt20 was considered reduced which has been reported asan indicator of high-risk CAD patients12 This value is lower than an-other cut-off point of 25 for detecting haemodynamically significantCAD13 Regional CFR was assessed in the three main coronary arteriesusing the American Heart Association 17-segment model to evaluateCFR in the culprit coronary artery A segment was considered to have is-chaemia when the regional hyperaemic MBF was lt23 which is more di-agnostically accurate than using regional CFR lt25 as the criterion13 Theextent of myocardial ischaemia was expressed as the percentage of theleft ventricle (LV) In addition relative flow reserve defined as the ratioof hyperaemic MBF in a stenotic area (lesion diameter stenosis gt_50) tohyperaemic MBF in a remote area was also calculated in patients withone- or two-vessel disease to minimize the impact of microvascular dys-function on perfusion values1415
22 Angiographic assessmentThe SYNTAX score16 at baseline was calculated in a blinded fashionSince the SYNTAX score was developed for patients without CABGthe CABG SYNTAX score17 was used in patients with CABG An angio-graphically successful PCI was defined as lt50 residual stenosis of thetarget lesion after the procedure The residual SYNTAX score18 orCABG SYNTAX score after revascularization was calculated fromfollow-up angiography If patients did not undergo follow-up angiogra-phy we calculated the residual SYNTAX score from angiography duringPCI and the CABG SYNTAX score from the surgical report in conjunctionwith the baseline angiogram before CABG The pre- and post-procedureanatomical Leaman score was also calculated as previously described19
23 Assessment of left ventricular systolicfunctionEchocardiography was performed by experienced sonographers whowere blinded to the PET results Left ventricular ejection fraction was
120 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
calculated using the biplane method of disks Interpretation was per-formed by cardiologists blinded to the PET results
24 Assessment of cardiovascular riskfactor controlCardiovascular risk factor control for hypertension diabetes hyperlipi-daemia and smoking were performed and assessed on the basis of theBARI 2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes)trial protocol20
25 Statistical analysisContinuous variables are presented as medians with interquartile range(IQR) Categorical variables are presented as absolute numbers withpercentages The sample size calculation was based on the assumptionthat the change in CFR before and after treatment would be 07 withstandard deviation of 10 To detect this change with gt_85 power and asignificance level of 005 each group needed to comprise gt_20 patientsThis sample size was calculated using Power and Sample Size Calculationversion 312 (httpbiostatmcvanderbilteduwikiMainPowerSampleSize) Differences between groups were evaluated using the Wilcoxonrank sum test followed by the Steel-Dwass test for continuous data andthe Fisher exact test for categorical data Differences between paireddata were evaluated using the Wilcoxon signed rank test or theMcNemar test as appropriate A two-way analysis of variance with re-peated measures was used to determine interaction effects BivariateSpearmanrsquos rank correlation coefficients (q) were calculated betweenbaseline CFR and changes in CFR and angiographic indices and theirchanges Before a multivariate regression analysis variables wereassessed for normality by the ShapirondashWilk test and log transformationapplied to correct for skewness as appropriate such as in changes in theLeaman score between pre- and post-revascularization (DLeamanscore) Linear regression analysis was used to examine the associationbetween changes in CFR and revascularized CAD burden [Model 1 in-cluded changes in the SYNTAX score between pre- and post-revascularization (DSYNTAX score) Model 2 included log (1-DLeamanscore)] adjusted for important covariates including the pretest likeli-hood of obstructive CAD history of PCI or CABG and the presence ofleft ventricular systolic dysfunction (left ventricular ejection fractionlt50) selected based on clinical relevance3 and the CABG group Totest the relative contribution of revascularization with CABG on changesin CFR a linear interaction term (DSYNTAX score the CABG group)was added to Model 1 (Model 3) Because of the nonrandomized natureof the study we used percent change as the dependent variable to mini-mize the differences in baseline CFR between groups The pretest likeli-hood of obstructive CAD was estimated using the Duke clinical riskscore21 calculated using age sex type of angina history of myocardial in-farction electrocardiographic Q and ST-T wave changes smokinghyperlipidaemia diabetes and interaction terms (age sex history ofmyocardial infarction electrocardiographic Q wave age smokingage hyperlipidaemia and sex smoking) The assumption of linearityfor continuous covariates was evaluated by plotting the residuals againstthe fitted values As an exploratory analysis propensity score matchingwas used to account for differences in baseline SYNTAX scoresbetween the PCI and CABG groups Propensity scores were calculatedusing a logistic regression model including baseline SYNTAX score andthe same covariates in the multivariate Model 1 (the pretest likelihoodof obstructive CAD history of PCI or CABG and left ventricularejection fraction lt50) A propensity score-matched cohort was
generated by 11 nearest available matching without replacement using acalliper width equal to 02 of the standard deviation of the logit of thepropensity score22 Propensity score matching was performed using theJMP add-in program (httpswwwjmpcomja_jpsupporttechnical-documentshtml) A two-tailed P-value of lt005 was considered statisticallysignificant All statistical analyses were performed using JMP Pro 1310(SAS Institute Inc Cary NC USA)
3 Results
31 Patient characteristicsWe prospectively recruited 82 patients to the study of whom 30 under-went PCI and 26 underwent CABG Of the remaining 26 patients whowere treated with OMT alone 21 had significant comorbidities (eg ad-vanced cancer or severely atheromatous aorta) or unsuitable coronaryanatomy for coronary revascularization three preferred medical ther-apy and two had fixed perfusion defects in the target area on myocardialperfusion imaging We excluded seven patients from the final analysesone patient in the OMT group developed advanced atrioventricularblock during adenosine triphosphate infusion at baseline PET and sixpatients (two in the PCI group and four in the CABG group) withdrewconsent during the follow-up period (Figure 1) Thus the final study co-hort consisted of 75 patients who completed the second PET
Baseline clinical characteristics are detailed in Table 1 The median ageof the patients was 70 (63ndash75) years 63 patients (84) were men andthe median pretest likelihood of obstructive CAD was 94 (78ndash98)Of these patients 24 (32) had one-vessel disease 22 (29) had two-vessel disease and 29 (39) had three-vessel or left main disease In gen-eral the baseline clinical characteristics were similar between the threegroups The CABG group however had higher SYNTAX and Leamanscores and total ischaemic burden with lower stress MBF and CFR thanthe OMT and PCI groups which reflected the non-randomized study de-sign Figure 2 shows three representative cases
Baseline CFR was negatively correlated with the SYNTAX (q = -040P lt 0001) and Leaman scores (q = -033 P = 0004) (Figure 3) Likewisestress MBF was negatively correlated with the SYNTAX (q = -048P lt 0001) and Leaman scores (q = -044 P lt 0001) whereas rest MBFwas not significantly correlated with either angiographic score(Supplementary material online Figure S1)
32 Changes in coronary risk factor controland angiographic CAD burdenTable 2 shows changes in coronary risk factor control and angiographicCAD burden during a median follow-up duration of 61 (56ndash63)months Overall the number of risk factors achieving the targets washigh at baseline The CABG group showed a significant increase in thepercentage of patients achieving gt_5 risk factor targets which did not dif-fer significantly between the three groups at follow-up Medications atfollow-up are shown in Supplementary material online Table S1
During the follow-up period none of the patients had adverse cardiacevents The symptoms disappeared after the treatment of CAD in 72 of75 patients (96) (Table 2) All 28 patients in the PCI group underwentan angiographically successful PCI In 17 patients undergoing PCI andscheduled follow-up angiography at a median time of 251 (169ndash279)days after PCI 16 had no significant restenosis and one had developedrestenosis and underwent repeated PCI after the second PET In 19patients undergoing CABG and post-operative angiography at a mediantime of 9 (8ndash14) days after CABG one had early saphenous vein graft
Effects of coronary revascularization on global CFR 121D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
occlusion after CABG and underwent additional PCI in the native coro-nary artery before the second PET The SYNTAX and Leaman scores inboth the PCI and CABG groups significantly decreased at follow-up(Table 2) There was no significant difference in the proportion ofpatients with low post-revascularization SYNTAX scores (0ndash8) acrossthe two revascularization groups and the OMT group (Table 2)
33 Changes in CFR and its association withangiographic CAD burdenIn the CABG group stress MBF significantly increased from baseline tofollow-up [122 (095ndash148) mLgmin vs 149 (129ndash169) mLgminP lt 0001] resulting in increased CFR [167 (114ndash196) vs 198 (160ndash239) P lt 0001] (Figure 4AndashC) Conversely both stress MBF and CFR didnot significantly change in the OMT and PCI groups (P gt 005 for all)(Figure 4B and C) Importantly despite baseline differences in CFR CFRat follow-up was not significantly different between the three groups[OMT group 242 (174ndash265) vs PCI group 223 (181ndash250) vs CABGgroup 198 (160ndash239) P = 020] After excluding patients with priormyocardial infarction or coronary revascularization (n = 34) the CFR sig-nificantly increased only in the CABG group [n = 13 171 (117ndash209) vs217 (163ndash242) P = 0002] Supplementary material online Table S2summarizes the haemodynamic characteristics of all patients during eachPET scan
When patients with baseline CFR lt20 (n = 41) were analysed CFRwas found to be significantly increased from baseline to follow-up bothin the PCI group [170 (142ndash179) vs 221 (178ndash249) P = 0002] and inthe CABG group [128 (113ndash180) vs 186 (157ndash222) P lt 0001](Figure 4D) This beneficial effect of PCI on CFR was only observed inpatients with baseline CFR lt20 (P lt 0001 for interaction) (Figure 4D
and 4E) These relationships did not change substantially when patientswere stratified by CFR lt25 and gt_25
When patients with a baseline SYNTAX score gt_23 (n = 23) were ana-lysed CFR was found to be significantly increased from baseline tofollow-up both in the PCI and CABG groups (Figure 4F) while there wasno significant interaction between time and baseline SYNTAX score inthe PCI and CABG groups (P = 011 and P = 099 respectively) Theseresults did not change substantially when patients were categorised intothree SYNTAX subgroups (0ndash22 23ndash32 and gt_33) (Supplementary ma-terial online Table S3)
Among 46 patients with one- or two-vessel disease in this study 17(37) had regional CFR lt20 in a remote area reflecting coronary mi-crovascular dysfunction In nine patients with coronary microvasculardysfunction who underwent PCI (n = 6) or CABG (n = 3) three (one inthe PCI group and two in the CABG group) had global CFR lt20 atfollow-up indicating that their coronary microvascular dysfunction per-sisted after revascularization The small number of patients with one- ortwo-vessel disease prevented a meaningful analysis based on relativeflow reserve values
Figure 5 shows changes in CFR and angiographic CAD burden in thePCI and CABG groups The percent changes in CFR were negatively cor-related with DSYNTAX score (q = -042 P lt 0001) and DLeaman score(q = -044 P lt 0001) The percent changes in CFR and stress MBF werenot significantly correlated with coronary artery calcium scores at base-line (P = 090 and P = 052 respectively)
On a per-vessel basis the percent change in regional CFR after treat-ment was significantly higher in coronary territories receiving CABG[213 (64ndash532)] than those receiving OMT alone [lt50 stenosis-21 (-209ndash182) P lt 0001 and 50ndash100 stenosis -11 (-215ndash
Figure 1 Study flowchart ATP adenosine triphosphate AV atrioventricular CABG coronary artery bypass grafting CAD coronary artery diseaseOMT optimal medical therapy PCI percutaneous coronary intervention PET positron emission tomography
122 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Table 1 Baseline characteristics of the study patients
Variables OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P-value
Age (years) 71 (64ndash79) 71 (65ndash78) 66 (55ndash74) 009
Male 23 (92) 23 (82) 17 (77) 035
Body mass index (kgm2) 234 (201ndash267) 236 (224ndash244) 265 (223ndash290) 010
Pretest likelihood of obstructive CAD () 95 (81ndash99) 90 (78ndash97) 94 (76ndash98) 043
Anginal symptoms 033
Typical angina 13 (52) 13 (46) 11 (50)
Atypical angina 6 (24) 2 (7) 2 (9)
Non-anginal chest pain 1 (4) 1 (4) 0 (0)
Hypertension 19 (76) 20 (71) 19 (86) 048
Diabetes 10 (40) 16 (57) 16 (73) 008
Hyperlipidaemia 18 (72) 22 (79) 18 (82) 078
Family history of CAD 2 (8) 2 (7) 1 (5) 100
Current smoker 4 (16) 4 (14) 5 (23) 074
Prior myocardial infarction 12 (48) 7 (25) 6 (27) 018
Prior PCI 10 (40) 9 (32) 4 (18) 026
Prior CABG 2 (8) 4 (14) 0 (0) 023
Systolic blood pressure (mmHg) 118 (106ndash136) 126 (112ndash137) 120 (108ndash132) 043
Diastolic blood pressure (mmHg) 60 (55ndash75) 64 (58ndash73) 64 (58ndash73) 056
Laboratory data
Total cholesterol (mgdL) 160 (133ndash186) 162 (136ndash184) 161 (138ndash178) 098
HDL cholesterol (mgdL) 52 (42ndash63) 45 (36ndash49) 44 (37ndash54) 013
LDL cholesterol (mgdL) 76 (58ndash110) 89 (68ndash111) 81 (74ndash115) 067
Triglycerides (mgdL) 111 (87ndash150) 122 (87ndash184) 113 (78ndash172) 086
Non-HDL cholesterol (mgdL) 102 (87ndash134) 116 (99ndash140) 107 (95ndash139) 059
Haemoglobin A1c () 60 (56ndash65) 60 (57ndash76) 69 (60ndash74) 024
Echocardiographic LV ejection fraction () 57 (47ndash64) 62 (51ndash67) 59 (34ndash64) 009
Vessels involved lt0001
1-vessel disease 15 (60) 8 (29) 1 (5)
2-vessel disease 7 (28) 12 (43) 3 (14)
3-vessel disease 3 (12) 7 (25) 13 (59)
Left main disease 0 (0) 1 (4) 5 (23)
SYNTAX score 9 (5ndash15) 14 (7ndash22) 29 (23ndash34) lt0001
Leaman score 4 (2ndash7) 4 (2ndash8) 14 (7ndash19) lt0001
Coronary artery calcium score (n = 50) 01ndash400gt400 0510 0413 0711 069
Rest myocardial blood flow (mLgmin) 086 (067ndash101) 080 (060ndash112) 076 (065ndash088) 038
Stress myocardial blood flow (mLgmin) 186 (172ndash235) 174(131ndash214) 122 (095ndash148) lt0001
Coronary flow reserve 238 (183ndash280) 203 (170ndash278) 167 (114ndash196) 0002
Myocardial ischaemia extent (LV) 94 (47ndash100) 94 (65ndash100) 100 (100ndash100) 0005
Medications
Antiplatelet agents 23 (92) 27 (96) 18 (82) 024
Angiotensin inhibitors 16 (64) 18 (64) 14 (64) 100
Beta-blockers 18 (72) 15 (54) 13 (59) 037
Calcium-channel blockers 13 (52) 13 (46) 9 (41) 077
Statins 24 (96) 25 (89) 19 (86) 054
Nitrates 11 (44) 7 (25) 11 (50) 015
Diuretics 8 (32) 6 (21) 8 (36) 051
Insulin 2 (8) 7 (25) 4 (18) 027
Warfarin 2 (8) 2 (7) 1 (5) 100
Data are represented median (interquartile range) or n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL high-density lipoprotein LDL low-density lipoprotein LV left ventricular OMT optimal medical ther-apy PCI percutaneous coronary interventionP lt 005 vs the OMT groupP lt 005 vs the PCI group
Effects of coronary revascularization on global CFR 123D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Figure 2 Eighty-two-year-old man treated with optimal medical therapy alone (A B) A global CFR of 264 at baseline (A) was slightly decreased to 257 atfollow-up (B) Sixty-six-year-old man receiving PCI (C D) The polar map of CFR at baseline (C) shows a regional decrease in the anterior to lateral wallGlobal CFR was modestly increased from 170 to 182 (D) after PCI to the LCX (yellow arrows) Seventy-eight-year-old man receiving CABG (E F) A globalCFR of 123 at baseline (E) was increased to 220 (F) after CABG using a RITA graft to the LAD a left internal thoracic artery graft to the LCX and a SVGgraft from the aorta to the RCA and LCX All grafts were patent 8 days after the CABG (F) CABG coronary artery bypass grafting LAD left anteriordescending artery LCX left circumflex artery LMT left main trunk PCI percutaneous coronary intervention RCA right coronary artery RITA right inter-nal thoracic artery SVG saphenous vein graft
124 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
313) P = 0002] (Figure 6) There was no significant difference in per-cent change in regional CFR between coronary territories receiving PCI[193 (-119ndash407)] and OMT alone (Figure 6) In addition thepercent change in regional CFR after PCI did not differ betweenstenoses with fractional flow reserve lt_08 and those with ischaemia onstress perfusion imaging [-37 (-309ndash654) vs 194 (-116ndash400)P = 086]
34 Predictors of changes in CFR inresponse to coronary revascularizationThe characteristics of patients with increased CFR from baseline tofollow-up compared with those without improvement are summarizedin Supplementary material online Table S4 Independent predictors ofchanges in CFR between baseline and follow-up PET are summarized inTable 3 The DSYNTAX score (Model 1) and DLeaman score (Model 2)were independently associated with changes in CFR Importantly the ex-tent of improvement in angiographic disease burden but not the pretestlikelihood or left ventricular ejection fraction was independently associ-ated with changes in CFR There was no significant interaction between
DSYNTAX score and revascularization with CABG (Model 3) indicatingthat CABG did not amplify the effects of revascularization on CFR
35 Propensity score-matched analysisSupplementary material online Table S5 shows the clinical characteristicsof the matched cohort The two groups (n = 9 in each group) were wellmatched at baseline The CABG group showed a significant increase inCFR [164 (113ndash207) vs 187 (152ndash248) P = 0004] while the PCIgroup did not [178 (147ndash246) vs 234 (147ndash274) P = 050] Althoughthere was no significant interaction between time and the tworevascularization groups (P = 069) probably due to small sample sizethe tendency was consistent with the unmatched cohort
4 Discussion
In this prospective multicentre study we demonstrated thatrevascularization of obstructive CAD improved CFR and stress MBF andthat the degree of improvement was correlated with the degree of re-duction of epicardial CAD burden Importantly these changes were
Figure 3 Relationship between CFR and the SYNTAX score (A) or the Leaman score (B) (A) The vertical dotted line indicates a SYNTAX score of 23
Table 2 Proportion of patients achieving risk factor targets and angiographic completeness of revascularization during thestudy period
OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P (between groups
at follow-up)Baseline Follow-up P Baseline Follow-up P Baseline Follow-up P
Systolic blood pressure lt130 mmHg 17 (68) 16 (64) 071 17 (61) 17 (61) 100 13 (55) 16 (73) 026 072
Diastolic blood pressure lt80 mmHg 22 (88) 21 (84) 065 26 (93) 25 (89) 065 21 (95) 21 (95) 100 052
Non-diabeteshaemoglobin A1c lt70 22 (88) 22 (88) 100 19 (68) 20 (71) 056 13 (59) 16 (73) 018 027
Triglycerides lt150 mgdL 19 (76) 16 (67) 041 19 (68) 19 (68) 100 15 (75) 16 (80) 065 064
Non-HDL-C lt130 mgdL 19 (76) 17 (68) 056 20 (71) 23 (82) 026 16 (73) 19 (86) 026 051
No smoking 21 (84) 22 (88) 032 24 (86) 25 (89) 032 17 (77) 21 (95) 0046 070
Achieving gt_5 risk factor targets 18 (72) 14 (64) 016 13 (46) 19 (68) 008 11 (50) 17 (77) 0034 029
SYNTAX score 0ndash8 12 (48) NA NA 8 (29) 19 (68) lt0001 0 (0) 10 (45) lt0001 022a
Leaman score = 0 3 (12) NA NA 2 (7) 16 (57) lt0001 0 (0) 16 (73) lt0001 lt0001a
Anginal symptoms 20 (80) 2 (8) lt0001 16 (57) 0 (0) lt0001 13 (59) 1 (8) lt0001 038
Values are represented as n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL-C high-density lipoprotein cholesterol LV left ventricular NA not applicable OMT optimal medicaltherapy PCI percutaneous coronary interventionaComparison between the OMT group at baseline and the PCI and CABG groups at follow-up
Effects of coronary revascularization on global CFR 125D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

calculated using the biplane method of disks Interpretation was per-formed by cardiologists blinded to the PET results
24 Assessment of cardiovascular riskfactor controlCardiovascular risk factor control for hypertension diabetes hyperlipi-daemia and smoking were performed and assessed on the basis of theBARI 2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes)trial protocol20
25 Statistical analysisContinuous variables are presented as medians with interquartile range(IQR) Categorical variables are presented as absolute numbers withpercentages The sample size calculation was based on the assumptionthat the change in CFR before and after treatment would be 07 withstandard deviation of 10 To detect this change with gt_85 power and asignificance level of 005 each group needed to comprise gt_20 patientsThis sample size was calculated using Power and Sample Size Calculationversion 312 (httpbiostatmcvanderbilteduwikiMainPowerSampleSize) Differences between groups were evaluated using the Wilcoxonrank sum test followed by the Steel-Dwass test for continuous data andthe Fisher exact test for categorical data Differences between paireddata were evaluated using the Wilcoxon signed rank test or theMcNemar test as appropriate A two-way analysis of variance with re-peated measures was used to determine interaction effects BivariateSpearmanrsquos rank correlation coefficients (q) were calculated betweenbaseline CFR and changes in CFR and angiographic indices and theirchanges Before a multivariate regression analysis variables wereassessed for normality by the ShapirondashWilk test and log transformationapplied to correct for skewness as appropriate such as in changes in theLeaman score between pre- and post-revascularization (DLeamanscore) Linear regression analysis was used to examine the associationbetween changes in CFR and revascularized CAD burden [Model 1 in-cluded changes in the SYNTAX score between pre- and post-revascularization (DSYNTAX score) Model 2 included log (1-DLeamanscore)] adjusted for important covariates including the pretest likeli-hood of obstructive CAD history of PCI or CABG and the presence ofleft ventricular systolic dysfunction (left ventricular ejection fractionlt50) selected based on clinical relevance3 and the CABG group Totest the relative contribution of revascularization with CABG on changesin CFR a linear interaction term (DSYNTAX score the CABG group)was added to Model 1 (Model 3) Because of the nonrandomized natureof the study we used percent change as the dependent variable to mini-mize the differences in baseline CFR between groups The pretest likeli-hood of obstructive CAD was estimated using the Duke clinical riskscore21 calculated using age sex type of angina history of myocardial in-farction electrocardiographic Q and ST-T wave changes smokinghyperlipidaemia diabetes and interaction terms (age sex history ofmyocardial infarction electrocardiographic Q wave age smokingage hyperlipidaemia and sex smoking) The assumption of linearityfor continuous covariates was evaluated by plotting the residuals againstthe fitted values As an exploratory analysis propensity score matchingwas used to account for differences in baseline SYNTAX scoresbetween the PCI and CABG groups Propensity scores were calculatedusing a logistic regression model including baseline SYNTAX score andthe same covariates in the multivariate Model 1 (the pretest likelihoodof obstructive CAD history of PCI or CABG and left ventricularejection fraction lt50) A propensity score-matched cohort was
generated by 11 nearest available matching without replacement using acalliper width equal to 02 of the standard deviation of the logit of thepropensity score22 Propensity score matching was performed using theJMP add-in program (httpswwwjmpcomja_jpsupporttechnical-documentshtml) A two-tailed P-value of lt005 was considered statisticallysignificant All statistical analyses were performed using JMP Pro 1310(SAS Institute Inc Cary NC USA)
3 Results
31 Patient characteristicsWe prospectively recruited 82 patients to the study of whom 30 under-went PCI and 26 underwent CABG Of the remaining 26 patients whowere treated with OMT alone 21 had significant comorbidities (eg ad-vanced cancer or severely atheromatous aorta) or unsuitable coronaryanatomy for coronary revascularization three preferred medical ther-apy and two had fixed perfusion defects in the target area on myocardialperfusion imaging We excluded seven patients from the final analysesone patient in the OMT group developed advanced atrioventricularblock during adenosine triphosphate infusion at baseline PET and sixpatients (two in the PCI group and four in the CABG group) withdrewconsent during the follow-up period (Figure 1) Thus the final study co-hort consisted of 75 patients who completed the second PET
Baseline clinical characteristics are detailed in Table 1 The median ageof the patients was 70 (63ndash75) years 63 patients (84) were men andthe median pretest likelihood of obstructive CAD was 94 (78ndash98)Of these patients 24 (32) had one-vessel disease 22 (29) had two-vessel disease and 29 (39) had three-vessel or left main disease In gen-eral the baseline clinical characteristics were similar between the threegroups The CABG group however had higher SYNTAX and Leamanscores and total ischaemic burden with lower stress MBF and CFR thanthe OMT and PCI groups which reflected the non-randomized study de-sign Figure 2 shows three representative cases
Baseline CFR was negatively correlated with the SYNTAX (q = -040P lt 0001) and Leaman scores (q = -033 P = 0004) (Figure 3) Likewisestress MBF was negatively correlated with the SYNTAX (q = -048P lt 0001) and Leaman scores (q = -044 P lt 0001) whereas rest MBFwas not significantly correlated with either angiographic score(Supplementary material online Figure S1)
32 Changes in coronary risk factor controland angiographic CAD burdenTable 2 shows changes in coronary risk factor control and angiographicCAD burden during a median follow-up duration of 61 (56ndash63)months Overall the number of risk factors achieving the targets washigh at baseline The CABG group showed a significant increase in thepercentage of patients achieving gt_5 risk factor targets which did not dif-fer significantly between the three groups at follow-up Medications atfollow-up are shown in Supplementary material online Table S1
During the follow-up period none of the patients had adverse cardiacevents The symptoms disappeared after the treatment of CAD in 72 of75 patients (96) (Table 2) All 28 patients in the PCI group underwentan angiographically successful PCI In 17 patients undergoing PCI andscheduled follow-up angiography at a median time of 251 (169ndash279)days after PCI 16 had no significant restenosis and one had developedrestenosis and underwent repeated PCI after the second PET In 19patients undergoing CABG and post-operative angiography at a mediantime of 9 (8ndash14) days after CABG one had early saphenous vein graft
Effects of coronary revascularization on global CFR 121D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
occlusion after CABG and underwent additional PCI in the native coro-nary artery before the second PET The SYNTAX and Leaman scores inboth the PCI and CABG groups significantly decreased at follow-up(Table 2) There was no significant difference in the proportion ofpatients with low post-revascularization SYNTAX scores (0ndash8) acrossthe two revascularization groups and the OMT group (Table 2)
33 Changes in CFR and its association withangiographic CAD burdenIn the CABG group stress MBF significantly increased from baseline tofollow-up [122 (095ndash148) mLgmin vs 149 (129ndash169) mLgminP lt 0001] resulting in increased CFR [167 (114ndash196) vs 198 (160ndash239) P lt 0001] (Figure 4AndashC) Conversely both stress MBF and CFR didnot significantly change in the OMT and PCI groups (P gt 005 for all)(Figure 4B and C) Importantly despite baseline differences in CFR CFRat follow-up was not significantly different between the three groups[OMT group 242 (174ndash265) vs PCI group 223 (181ndash250) vs CABGgroup 198 (160ndash239) P = 020] After excluding patients with priormyocardial infarction or coronary revascularization (n = 34) the CFR sig-nificantly increased only in the CABG group [n = 13 171 (117ndash209) vs217 (163ndash242) P = 0002] Supplementary material online Table S2summarizes the haemodynamic characteristics of all patients during eachPET scan
When patients with baseline CFR lt20 (n = 41) were analysed CFRwas found to be significantly increased from baseline to follow-up bothin the PCI group [170 (142ndash179) vs 221 (178ndash249) P = 0002] and inthe CABG group [128 (113ndash180) vs 186 (157ndash222) P lt 0001](Figure 4D) This beneficial effect of PCI on CFR was only observed inpatients with baseline CFR lt20 (P lt 0001 for interaction) (Figure 4D
and 4E) These relationships did not change substantially when patientswere stratified by CFR lt25 and gt_25
When patients with a baseline SYNTAX score gt_23 (n = 23) were ana-lysed CFR was found to be significantly increased from baseline tofollow-up both in the PCI and CABG groups (Figure 4F) while there wasno significant interaction between time and baseline SYNTAX score inthe PCI and CABG groups (P = 011 and P = 099 respectively) Theseresults did not change substantially when patients were categorised intothree SYNTAX subgroups (0ndash22 23ndash32 and gt_33) (Supplementary ma-terial online Table S3)
Among 46 patients with one- or two-vessel disease in this study 17(37) had regional CFR lt20 in a remote area reflecting coronary mi-crovascular dysfunction In nine patients with coronary microvasculardysfunction who underwent PCI (n = 6) or CABG (n = 3) three (one inthe PCI group and two in the CABG group) had global CFR lt20 atfollow-up indicating that their coronary microvascular dysfunction per-sisted after revascularization The small number of patients with one- ortwo-vessel disease prevented a meaningful analysis based on relativeflow reserve values
Figure 5 shows changes in CFR and angiographic CAD burden in thePCI and CABG groups The percent changes in CFR were negatively cor-related with DSYNTAX score (q = -042 P lt 0001) and DLeaman score(q = -044 P lt 0001) The percent changes in CFR and stress MBF werenot significantly correlated with coronary artery calcium scores at base-line (P = 090 and P = 052 respectively)
On a per-vessel basis the percent change in regional CFR after treat-ment was significantly higher in coronary territories receiving CABG[213 (64ndash532)] than those receiving OMT alone [lt50 stenosis-21 (-209ndash182) P lt 0001 and 50ndash100 stenosis -11 (-215ndash
Figure 1 Study flowchart ATP adenosine triphosphate AV atrioventricular CABG coronary artery bypass grafting CAD coronary artery diseaseOMT optimal medical therapy PCI percutaneous coronary intervention PET positron emission tomography
122 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Table 1 Baseline characteristics of the study patients
Variables OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P-value
Age (years) 71 (64ndash79) 71 (65ndash78) 66 (55ndash74) 009
Male 23 (92) 23 (82) 17 (77) 035
Body mass index (kgm2) 234 (201ndash267) 236 (224ndash244) 265 (223ndash290) 010
Pretest likelihood of obstructive CAD () 95 (81ndash99) 90 (78ndash97) 94 (76ndash98) 043
Anginal symptoms 033
Typical angina 13 (52) 13 (46) 11 (50)
Atypical angina 6 (24) 2 (7) 2 (9)
Non-anginal chest pain 1 (4) 1 (4) 0 (0)
Hypertension 19 (76) 20 (71) 19 (86) 048
Diabetes 10 (40) 16 (57) 16 (73) 008
Hyperlipidaemia 18 (72) 22 (79) 18 (82) 078
Family history of CAD 2 (8) 2 (7) 1 (5) 100
Current smoker 4 (16) 4 (14) 5 (23) 074
Prior myocardial infarction 12 (48) 7 (25) 6 (27) 018
Prior PCI 10 (40) 9 (32) 4 (18) 026
Prior CABG 2 (8) 4 (14) 0 (0) 023
Systolic blood pressure (mmHg) 118 (106ndash136) 126 (112ndash137) 120 (108ndash132) 043
Diastolic blood pressure (mmHg) 60 (55ndash75) 64 (58ndash73) 64 (58ndash73) 056
Laboratory data
Total cholesterol (mgdL) 160 (133ndash186) 162 (136ndash184) 161 (138ndash178) 098
HDL cholesterol (mgdL) 52 (42ndash63) 45 (36ndash49) 44 (37ndash54) 013
LDL cholesterol (mgdL) 76 (58ndash110) 89 (68ndash111) 81 (74ndash115) 067
Triglycerides (mgdL) 111 (87ndash150) 122 (87ndash184) 113 (78ndash172) 086
Non-HDL cholesterol (mgdL) 102 (87ndash134) 116 (99ndash140) 107 (95ndash139) 059
Haemoglobin A1c () 60 (56ndash65) 60 (57ndash76) 69 (60ndash74) 024
Echocardiographic LV ejection fraction () 57 (47ndash64) 62 (51ndash67) 59 (34ndash64) 009
Vessels involved lt0001
1-vessel disease 15 (60) 8 (29) 1 (5)
2-vessel disease 7 (28) 12 (43) 3 (14)
3-vessel disease 3 (12) 7 (25) 13 (59)
Left main disease 0 (0) 1 (4) 5 (23)
SYNTAX score 9 (5ndash15) 14 (7ndash22) 29 (23ndash34) lt0001
Leaman score 4 (2ndash7) 4 (2ndash8) 14 (7ndash19) lt0001
Coronary artery calcium score (n = 50) 01ndash400gt400 0510 0413 0711 069
Rest myocardial blood flow (mLgmin) 086 (067ndash101) 080 (060ndash112) 076 (065ndash088) 038
Stress myocardial blood flow (mLgmin) 186 (172ndash235) 174(131ndash214) 122 (095ndash148) lt0001
Coronary flow reserve 238 (183ndash280) 203 (170ndash278) 167 (114ndash196) 0002
Myocardial ischaemia extent (LV) 94 (47ndash100) 94 (65ndash100) 100 (100ndash100) 0005
Medications
Antiplatelet agents 23 (92) 27 (96) 18 (82) 024
Angiotensin inhibitors 16 (64) 18 (64) 14 (64) 100
Beta-blockers 18 (72) 15 (54) 13 (59) 037
Calcium-channel blockers 13 (52) 13 (46) 9 (41) 077
Statins 24 (96) 25 (89) 19 (86) 054
Nitrates 11 (44) 7 (25) 11 (50) 015
Diuretics 8 (32) 6 (21) 8 (36) 051
Insulin 2 (8) 7 (25) 4 (18) 027
Warfarin 2 (8) 2 (7) 1 (5) 100
Data are represented median (interquartile range) or n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL high-density lipoprotein LDL low-density lipoprotein LV left ventricular OMT optimal medical ther-apy PCI percutaneous coronary interventionP lt 005 vs the OMT groupP lt 005 vs the PCI group
Effects of coronary revascularization on global CFR 123D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Figure 2 Eighty-two-year-old man treated with optimal medical therapy alone (A B) A global CFR of 264 at baseline (A) was slightly decreased to 257 atfollow-up (B) Sixty-six-year-old man receiving PCI (C D) The polar map of CFR at baseline (C) shows a regional decrease in the anterior to lateral wallGlobal CFR was modestly increased from 170 to 182 (D) after PCI to the LCX (yellow arrows) Seventy-eight-year-old man receiving CABG (E F) A globalCFR of 123 at baseline (E) was increased to 220 (F) after CABG using a RITA graft to the LAD a left internal thoracic artery graft to the LCX and a SVGgraft from the aorta to the RCA and LCX All grafts were patent 8 days after the CABG (F) CABG coronary artery bypass grafting LAD left anteriordescending artery LCX left circumflex artery LMT left main trunk PCI percutaneous coronary intervention RCA right coronary artery RITA right inter-nal thoracic artery SVG saphenous vein graft
124 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
313) P = 0002] (Figure 6) There was no significant difference in per-cent change in regional CFR between coronary territories receiving PCI[193 (-119ndash407)] and OMT alone (Figure 6) In addition thepercent change in regional CFR after PCI did not differ betweenstenoses with fractional flow reserve lt_08 and those with ischaemia onstress perfusion imaging [-37 (-309ndash654) vs 194 (-116ndash400)P = 086]
34 Predictors of changes in CFR inresponse to coronary revascularizationThe characteristics of patients with increased CFR from baseline tofollow-up compared with those without improvement are summarizedin Supplementary material online Table S4 Independent predictors ofchanges in CFR between baseline and follow-up PET are summarized inTable 3 The DSYNTAX score (Model 1) and DLeaman score (Model 2)were independently associated with changes in CFR Importantly the ex-tent of improvement in angiographic disease burden but not the pretestlikelihood or left ventricular ejection fraction was independently associ-ated with changes in CFR There was no significant interaction between
DSYNTAX score and revascularization with CABG (Model 3) indicatingthat CABG did not amplify the effects of revascularization on CFR
35 Propensity score-matched analysisSupplementary material online Table S5 shows the clinical characteristicsof the matched cohort The two groups (n = 9 in each group) were wellmatched at baseline The CABG group showed a significant increase inCFR [164 (113ndash207) vs 187 (152ndash248) P = 0004] while the PCIgroup did not [178 (147ndash246) vs 234 (147ndash274) P = 050] Althoughthere was no significant interaction between time and the tworevascularization groups (P = 069) probably due to small sample sizethe tendency was consistent with the unmatched cohort
4 Discussion
In this prospective multicentre study we demonstrated thatrevascularization of obstructive CAD improved CFR and stress MBF andthat the degree of improvement was correlated with the degree of re-duction of epicardial CAD burden Importantly these changes were
Figure 3 Relationship between CFR and the SYNTAX score (A) or the Leaman score (B) (A) The vertical dotted line indicates a SYNTAX score of 23
Table 2 Proportion of patients achieving risk factor targets and angiographic completeness of revascularization during thestudy period
OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P (between groups
at follow-up)Baseline Follow-up P Baseline Follow-up P Baseline Follow-up P
Systolic blood pressure lt130 mmHg 17 (68) 16 (64) 071 17 (61) 17 (61) 100 13 (55) 16 (73) 026 072
Diastolic blood pressure lt80 mmHg 22 (88) 21 (84) 065 26 (93) 25 (89) 065 21 (95) 21 (95) 100 052
Non-diabeteshaemoglobin A1c lt70 22 (88) 22 (88) 100 19 (68) 20 (71) 056 13 (59) 16 (73) 018 027
Triglycerides lt150 mgdL 19 (76) 16 (67) 041 19 (68) 19 (68) 100 15 (75) 16 (80) 065 064
Non-HDL-C lt130 mgdL 19 (76) 17 (68) 056 20 (71) 23 (82) 026 16 (73) 19 (86) 026 051
No smoking 21 (84) 22 (88) 032 24 (86) 25 (89) 032 17 (77) 21 (95) 0046 070
Achieving gt_5 risk factor targets 18 (72) 14 (64) 016 13 (46) 19 (68) 008 11 (50) 17 (77) 0034 029
SYNTAX score 0ndash8 12 (48) NA NA 8 (29) 19 (68) lt0001 0 (0) 10 (45) lt0001 022a
Leaman score = 0 3 (12) NA NA 2 (7) 16 (57) lt0001 0 (0) 16 (73) lt0001 lt0001a
Anginal symptoms 20 (80) 2 (8) lt0001 16 (57) 0 (0) lt0001 13 (59) 1 (8) lt0001 038
Values are represented as n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL-C high-density lipoprotein cholesterol LV left ventricular NA not applicable OMT optimal medicaltherapy PCI percutaneous coronary interventionaComparison between the OMT group at baseline and the PCI and CABG groups at follow-up
Effects of coronary revascularization on global CFR 125D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

occlusion after CABG and underwent additional PCI in the native coro-nary artery before the second PET The SYNTAX and Leaman scores inboth the PCI and CABG groups significantly decreased at follow-up(Table 2) There was no significant difference in the proportion ofpatients with low post-revascularization SYNTAX scores (0ndash8) acrossthe two revascularization groups and the OMT group (Table 2)
33 Changes in CFR and its association withangiographic CAD burdenIn the CABG group stress MBF significantly increased from baseline tofollow-up [122 (095ndash148) mLgmin vs 149 (129ndash169) mLgminP lt 0001] resulting in increased CFR [167 (114ndash196) vs 198 (160ndash239) P lt 0001] (Figure 4AndashC) Conversely both stress MBF and CFR didnot significantly change in the OMT and PCI groups (P gt 005 for all)(Figure 4B and C) Importantly despite baseline differences in CFR CFRat follow-up was not significantly different between the three groups[OMT group 242 (174ndash265) vs PCI group 223 (181ndash250) vs CABGgroup 198 (160ndash239) P = 020] After excluding patients with priormyocardial infarction or coronary revascularization (n = 34) the CFR sig-nificantly increased only in the CABG group [n = 13 171 (117ndash209) vs217 (163ndash242) P = 0002] Supplementary material online Table S2summarizes the haemodynamic characteristics of all patients during eachPET scan
When patients with baseline CFR lt20 (n = 41) were analysed CFRwas found to be significantly increased from baseline to follow-up bothin the PCI group [170 (142ndash179) vs 221 (178ndash249) P = 0002] and inthe CABG group [128 (113ndash180) vs 186 (157ndash222) P lt 0001](Figure 4D) This beneficial effect of PCI on CFR was only observed inpatients with baseline CFR lt20 (P lt 0001 for interaction) (Figure 4D
and 4E) These relationships did not change substantially when patientswere stratified by CFR lt25 and gt_25
When patients with a baseline SYNTAX score gt_23 (n = 23) were ana-lysed CFR was found to be significantly increased from baseline tofollow-up both in the PCI and CABG groups (Figure 4F) while there wasno significant interaction between time and baseline SYNTAX score inthe PCI and CABG groups (P = 011 and P = 099 respectively) Theseresults did not change substantially when patients were categorised intothree SYNTAX subgroups (0ndash22 23ndash32 and gt_33) (Supplementary ma-terial online Table S3)
Among 46 patients with one- or two-vessel disease in this study 17(37) had regional CFR lt20 in a remote area reflecting coronary mi-crovascular dysfunction In nine patients with coronary microvasculardysfunction who underwent PCI (n = 6) or CABG (n = 3) three (one inthe PCI group and two in the CABG group) had global CFR lt20 atfollow-up indicating that their coronary microvascular dysfunction per-sisted after revascularization The small number of patients with one- ortwo-vessel disease prevented a meaningful analysis based on relativeflow reserve values
Figure 5 shows changes in CFR and angiographic CAD burden in thePCI and CABG groups The percent changes in CFR were negatively cor-related with DSYNTAX score (q = -042 P lt 0001) and DLeaman score(q = -044 P lt 0001) The percent changes in CFR and stress MBF werenot significantly correlated with coronary artery calcium scores at base-line (P = 090 and P = 052 respectively)
On a per-vessel basis the percent change in regional CFR after treat-ment was significantly higher in coronary territories receiving CABG[213 (64ndash532)] than those receiving OMT alone [lt50 stenosis-21 (-209ndash182) P lt 0001 and 50ndash100 stenosis -11 (-215ndash
Figure 1 Study flowchart ATP adenosine triphosphate AV atrioventricular CABG coronary artery bypass grafting CAD coronary artery diseaseOMT optimal medical therapy PCI percutaneous coronary intervention PET positron emission tomography
122 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Table 1 Baseline characteristics of the study patients
Variables OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P-value
Age (years) 71 (64ndash79) 71 (65ndash78) 66 (55ndash74) 009
Male 23 (92) 23 (82) 17 (77) 035
Body mass index (kgm2) 234 (201ndash267) 236 (224ndash244) 265 (223ndash290) 010
Pretest likelihood of obstructive CAD () 95 (81ndash99) 90 (78ndash97) 94 (76ndash98) 043
Anginal symptoms 033
Typical angina 13 (52) 13 (46) 11 (50)
Atypical angina 6 (24) 2 (7) 2 (9)
Non-anginal chest pain 1 (4) 1 (4) 0 (0)
Hypertension 19 (76) 20 (71) 19 (86) 048
Diabetes 10 (40) 16 (57) 16 (73) 008
Hyperlipidaemia 18 (72) 22 (79) 18 (82) 078
Family history of CAD 2 (8) 2 (7) 1 (5) 100
Current smoker 4 (16) 4 (14) 5 (23) 074
Prior myocardial infarction 12 (48) 7 (25) 6 (27) 018
Prior PCI 10 (40) 9 (32) 4 (18) 026
Prior CABG 2 (8) 4 (14) 0 (0) 023
Systolic blood pressure (mmHg) 118 (106ndash136) 126 (112ndash137) 120 (108ndash132) 043
Diastolic blood pressure (mmHg) 60 (55ndash75) 64 (58ndash73) 64 (58ndash73) 056
Laboratory data
Total cholesterol (mgdL) 160 (133ndash186) 162 (136ndash184) 161 (138ndash178) 098
HDL cholesterol (mgdL) 52 (42ndash63) 45 (36ndash49) 44 (37ndash54) 013
LDL cholesterol (mgdL) 76 (58ndash110) 89 (68ndash111) 81 (74ndash115) 067
Triglycerides (mgdL) 111 (87ndash150) 122 (87ndash184) 113 (78ndash172) 086
Non-HDL cholesterol (mgdL) 102 (87ndash134) 116 (99ndash140) 107 (95ndash139) 059
Haemoglobin A1c () 60 (56ndash65) 60 (57ndash76) 69 (60ndash74) 024
Echocardiographic LV ejection fraction () 57 (47ndash64) 62 (51ndash67) 59 (34ndash64) 009
Vessels involved lt0001
1-vessel disease 15 (60) 8 (29) 1 (5)
2-vessel disease 7 (28) 12 (43) 3 (14)
3-vessel disease 3 (12) 7 (25) 13 (59)
Left main disease 0 (0) 1 (4) 5 (23)
SYNTAX score 9 (5ndash15) 14 (7ndash22) 29 (23ndash34) lt0001
Leaman score 4 (2ndash7) 4 (2ndash8) 14 (7ndash19) lt0001
Coronary artery calcium score (n = 50) 01ndash400gt400 0510 0413 0711 069
Rest myocardial blood flow (mLgmin) 086 (067ndash101) 080 (060ndash112) 076 (065ndash088) 038
Stress myocardial blood flow (mLgmin) 186 (172ndash235) 174(131ndash214) 122 (095ndash148) lt0001
Coronary flow reserve 238 (183ndash280) 203 (170ndash278) 167 (114ndash196) 0002
Myocardial ischaemia extent (LV) 94 (47ndash100) 94 (65ndash100) 100 (100ndash100) 0005
Medications
Antiplatelet agents 23 (92) 27 (96) 18 (82) 024
Angiotensin inhibitors 16 (64) 18 (64) 14 (64) 100
Beta-blockers 18 (72) 15 (54) 13 (59) 037
Calcium-channel blockers 13 (52) 13 (46) 9 (41) 077
Statins 24 (96) 25 (89) 19 (86) 054
Nitrates 11 (44) 7 (25) 11 (50) 015
Diuretics 8 (32) 6 (21) 8 (36) 051
Insulin 2 (8) 7 (25) 4 (18) 027
Warfarin 2 (8) 2 (7) 1 (5) 100
Data are represented median (interquartile range) or n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL high-density lipoprotein LDL low-density lipoprotein LV left ventricular OMT optimal medical ther-apy PCI percutaneous coronary interventionP lt 005 vs the OMT groupP lt 005 vs the PCI group
Effects of coronary revascularization on global CFR 123D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Figure 2 Eighty-two-year-old man treated with optimal medical therapy alone (A B) A global CFR of 264 at baseline (A) was slightly decreased to 257 atfollow-up (B) Sixty-six-year-old man receiving PCI (C D) The polar map of CFR at baseline (C) shows a regional decrease in the anterior to lateral wallGlobal CFR was modestly increased from 170 to 182 (D) after PCI to the LCX (yellow arrows) Seventy-eight-year-old man receiving CABG (E F) A globalCFR of 123 at baseline (E) was increased to 220 (F) after CABG using a RITA graft to the LAD a left internal thoracic artery graft to the LCX and a SVGgraft from the aorta to the RCA and LCX All grafts were patent 8 days after the CABG (F) CABG coronary artery bypass grafting LAD left anteriordescending artery LCX left circumflex artery LMT left main trunk PCI percutaneous coronary intervention RCA right coronary artery RITA right inter-nal thoracic artery SVG saphenous vein graft
124 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
313) P = 0002] (Figure 6) There was no significant difference in per-cent change in regional CFR between coronary territories receiving PCI[193 (-119ndash407)] and OMT alone (Figure 6) In addition thepercent change in regional CFR after PCI did not differ betweenstenoses with fractional flow reserve lt_08 and those with ischaemia onstress perfusion imaging [-37 (-309ndash654) vs 194 (-116ndash400)P = 086]
34 Predictors of changes in CFR inresponse to coronary revascularizationThe characteristics of patients with increased CFR from baseline tofollow-up compared with those without improvement are summarizedin Supplementary material online Table S4 Independent predictors ofchanges in CFR between baseline and follow-up PET are summarized inTable 3 The DSYNTAX score (Model 1) and DLeaman score (Model 2)were independently associated with changes in CFR Importantly the ex-tent of improvement in angiographic disease burden but not the pretestlikelihood or left ventricular ejection fraction was independently associ-ated with changes in CFR There was no significant interaction between
DSYNTAX score and revascularization with CABG (Model 3) indicatingthat CABG did not amplify the effects of revascularization on CFR
35 Propensity score-matched analysisSupplementary material online Table S5 shows the clinical characteristicsof the matched cohort The two groups (n = 9 in each group) were wellmatched at baseline The CABG group showed a significant increase inCFR [164 (113ndash207) vs 187 (152ndash248) P = 0004] while the PCIgroup did not [178 (147ndash246) vs 234 (147ndash274) P = 050] Althoughthere was no significant interaction between time and the tworevascularization groups (P = 069) probably due to small sample sizethe tendency was consistent with the unmatched cohort
4 Discussion
In this prospective multicentre study we demonstrated thatrevascularization of obstructive CAD improved CFR and stress MBF andthat the degree of improvement was correlated with the degree of re-duction of epicardial CAD burden Importantly these changes were
Figure 3 Relationship between CFR and the SYNTAX score (A) or the Leaman score (B) (A) The vertical dotted line indicates a SYNTAX score of 23
Table 2 Proportion of patients achieving risk factor targets and angiographic completeness of revascularization during thestudy period
OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P (between groups
at follow-up)Baseline Follow-up P Baseline Follow-up P Baseline Follow-up P
Systolic blood pressure lt130 mmHg 17 (68) 16 (64) 071 17 (61) 17 (61) 100 13 (55) 16 (73) 026 072
Diastolic blood pressure lt80 mmHg 22 (88) 21 (84) 065 26 (93) 25 (89) 065 21 (95) 21 (95) 100 052
Non-diabeteshaemoglobin A1c lt70 22 (88) 22 (88) 100 19 (68) 20 (71) 056 13 (59) 16 (73) 018 027
Triglycerides lt150 mgdL 19 (76) 16 (67) 041 19 (68) 19 (68) 100 15 (75) 16 (80) 065 064
Non-HDL-C lt130 mgdL 19 (76) 17 (68) 056 20 (71) 23 (82) 026 16 (73) 19 (86) 026 051
No smoking 21 (84) 22 (88) 032 24 (86) 25 (89) 032 17 (77) 21 (95) 0046 070
Achieving gt_5 risk factor targets 18 (72) 14 (64) 016 13 (46) 19 (68) 008 11 (50) 17 (77) 0034 029
SYNTAX score 0ndash8 12 (48) NA NA 8 (29) 19 (68) lt0001 0 (0) 10 (45) lt0001 022a
Leaman score = 0 3 (12) NA NA 2 (7) 16 (57) lt0001 0 (0) 16 (73) lt0001 lt0001a
Anginal symptoms 20 (80) 2 (8) lt0001 16 (57) 0 (0) lt0001 13 (59) 1 (8) lt0001 038
Values are represented as n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL-C high-density lipoprotein cholesterol LV left ventricular NA not applicable OMT optimal medicaltherapy PCI percutaneous coronary interventionaComparison between the OMT group at baseline and the PCI and CABG groups at follow-up
Effects of coronary revascularization on global CFR 125D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

Table 1 Baseline characteristics of the study patients
Variables OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P-value
Age (years) 71 (64ndash79) 71 (65ndash78) 66 (55ndash74) 009
Male 23 (92) 23 (82) 17 (77) 035
Body mass index (kgm2) 234 (201ndash267) 236 (224ndash244) 265 (223ndash290) 010
Pretest likelihood of obstructive CAD () 95 (81ndash99) 90 (78ndash97) 94 (76ndash98) 043
Anginal symptoms 033
Typical angina 13 (52) 13 (46) 11 (50)
Atypical angina 6 (24) 2 (7) 2 (9)
Non-anginal chest pain 1 (4) 1 (4) 0 (0)
Hypertension 19 (76) 20 (71) 19 (86) 048
Diabetes 10 (40) 16 (57) 16 (73) 008
Hyperlipidaemia 18 (72) 22 (79) 18 (82) 078
Family history of CAD 2 (8) 2 (7) 1 (5) 100
Current smoker 4 (16) 4 (14) 5 (23) 074
Prior myocardial infarction 12 (48) 7 (25) 6 (27) 018
Prior PCI 10 (40) 9 (32) 4 (18) 026
Prior CABG 2 (8) 4 (14) 0 (0) 023
Systolic blood pressure (mmHg) 118 (106ndash136) 126 (112ndash137) 120 (108ndash132) 043
Diastolic blood pressure (mmHg) 60 (55ndash75) 64 (58ndash73) 64 (58ndash73) 056
Laboratory data
Total cholesterol (mgdL) 160 (133ndash186) 162 (136ndash184) 161 (138ndash178) 098
HDL cholesterol (mgdL) 52 (42ndash63) 45 (36ndash49) 44 (37ndash54) 013
LDL cholesterol (mgdL) 76 (58ndash110) 89 (68ndash111) 81 (74ndash115) 067
Triglycerides (mgdL) 111 (87ndash150) 122 (87ndash184) 113 (78ndash172) 086
Non-HDL cholesterol (mgdL) 102 (87ndash134) 116 (99ndash140) 107 (95ndash139) 059
Haemoglobin A1c () 60 (56ndash65) 60 (57ndash76) 69 (60ndash74) 024
Echocardiographic LV ejection fraction () 57 (47ndash64) 62 (51ndash67) 59 (34ndash64) 009
Vessels involved lt0001
1-vessel disease 15 (60) 8 (29) 1 (5)
2-vessel disease 7 (28) 12 (43) 3 (14)
3-vessel disease 3 (12) 7 (25) 13 (59)
Left main disease 0 (0) 1 (4) 5 (23)
SYNTAX score 9 (5ndash15) 14 (7ndash22) 29 (23ndash34) lt0001
Leaman score 4 (2ndash7) 4 (2ndash8) 14 (7ndash19) lt0001
Coronary artery calcium score (n = 50) 01ndash400gt400 0510 0413 0711 069
Rest myocardial blood flow (mLgmin) 086 (067ndash101) 080 (060ndash112) 076 (065ndash088) 038
Stress myocardial blood flow (mLgmin) 186 (172ndash235) 174(131ndash214) 122 (095ndash148) lt0001
Coronary flow reserve 238 (183ndash280) 203 (170ndash278) 167 (114ndash196) 0002
Myocardial ischaemia extent (LV) 94 (47ndash100) 94 (65ndash100) 100 (100ndash100) 0005
Medications
Antiplatelet agents 23 (92) 27 (96) 18 (82) 024
Angiotensin inhibitors 16 (64) 18 (64) 14 (64) 100
Beta-blockers 18 (72) 15 (54) 13 (59) 037
Calcium-channel blockers 13 (52) 13 (46) 9 (41) 077
Statins 24 (96) 25 (89) 19 (86) 054
Nitrates 11 (44) 7 (25) 11 (50) 015
Diuretics 8 (32) 6 (21) 8 (36) 051
Insulin 2 (8) 7 (25) 4 (18) 027
Warfarin 2 (8) 2 (7) 1 (5) 100
Data are represented median (interquartile range) or n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL high-density lipoprotein LDL low-density lipoprotein LV left ventricular OMT optimal medical ther-apy PCI percutaneous coronary interventionP lt 005 vs the OMT groupP lt 005 vs the PCI group
Effects of coronary revascularization on global CFR 123D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Figure 2 Eighty-two-year-old man treated with optimal medical therapy alone (A B) A global CFR of 264 at baseline (A) was slightly decreased to 257 atfollow-up (B) Sixty-six-year-old man receiving PCI (C D) The polar map of CFR at baseline (C) shows a regional decrease in the anterior to lateral wallGlobal CFR was modestly increased from 170 to 182 (D) after PCI to the LCX (yellow arrows) Seventy-eight-year-old man receiving CABG (E F) A globalCFR of 123 at baseline (E) was increased to 220 (F) after CABG using a RITA graft to the LAD a left internal thoracic artery graft to the LCX and a SVGgraft from the aorta to the RCA and LCX All grafts were patent 8 days after the CABG (F) CABG coronary artery bypass grafting LAD left anteriordescending artery LCX left circumflex artery LMT left main trunk PCI percutaneous coronary intervention RCA right coronary artery RITA right inter-nal thoracic artery SVG saphenous vein graft
124 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
313) P = 0002] (Figure 6) There was no significant difference in per-cent change in regional CFR between coronary territories receiving PCI[193 (-119ndash407)] and OMT alone (Figure 6) In addition thepercent change in regional CFR after PCI did not differ betweenstenoses with fractional flow reserve lt_08 and those with ischaemia onstress perfusion imaging [-37 (-309ndash654) vs 194 (-116ndash400)P = 086]
34 Predictors of changes in CFR inresponse to coronary revascularizationThe characteristics of patients with increased CFR from baseline tofollow-up compared with those without improvement are summarizedin Supplementary material online Table S4 Independent predictors ofchanges in CFR between baseline and follow-up PET are summarized inTable 3 The DSYNTAX score (Model 1) and DLeaman score (Model 2)were independently associated with changes in CFR Importantly the ex-tent of improvement in angiographic disease burden but not the pretestlikelihood or left ventricular ejection fraction was independently associ-ated with changes in CFR There was no significant interaction between
DSYNTAX score and revascularization with CABG (Model 3) indicatingthat CABG did not amplify the effects of revascularization on CFR
35 Propensity score-matched analysisSupplementary material online Table S5 shows the clinical characteristicsof the matched cohort The two groups (n = 9 in each group) were wellmatched at baseline The CABG group showed a significant increase inCFR [164 (113ndash207) vs 187 (152ndash248) P = 0004] while the PCIgroup did not [178 (147ndash246) vs 234 (147ndash274) P = 050] Althoughthere was no significant interaction between time and the tworevascularization groups (P = 069) probably due to small sample sizethe tendency was consistent with the unmatched cohort
4 Discussion
In this prospective multicentre study we demonstrated thatrevascularization of obstructive CAD improved CFR and stress MBF andthat the degree of improvement was correlated with the degree of re-duction of epicardial CAD burden Importantly these changes were
Figure 3 Relationship between CFR and the SYNTAX score (A) or the Leaman score (B) (A) The vertical dotted line indicates a SYNTAX score of 23
Table 2 Proportion of patients achieving risk factor targets and angiographic completeness of revascularization during thestudy period
OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P (between groups
at follow-up)Baseline Follow-up P Baseline Follow-up P Baseline Follow-up P
Systolic blood pressure lt130 mmHg 17 (68) 16 (64) 071 17 (61) 17 (61) 100 13 (55) 16 (73) 026 072
Diastolic blood pressure lt80 mmHg 22 (88) 21 (84) 065 26 (93) 25 (89) 065 21 (95) 21 (95) 100 052
Non-diabeteshaemoglobin A1c lt70 22 (88) 22 (88) 100 19 (68) 20 (71) 056 13 (59) 16 (73) 018 027
Triglycerides lt150 mgdL 19 (76) 16 (67) 041 19 (68) 19 (68) 100 15 (75) 16 (80) 065 064
Non-HDL-C lt130 mgdL 19 (76) 17 (68) 056 20 (71) 23 (82) 026 16 (73) 19 (86) 026 051
No smoking 21 (84) 22 (88) 032 24 (86) 25 (89) 032 17 (77) 21 (95) 0046 070
Achieving gt_5 risk factor targets 18 (72) 14 (64) 016 13 (46) 19 (68) 008 11 (50) 17 (77) 0034 029
SYNTAX score 0ndash8 12 (48) NA NA 8 (29) 19 (68) lt0001 0 (0) 10 (45) lt0001 022a
Leaman score = 0 3 (12) NA NA 2 (7) 16 (57) lt0001 0 (0) 16 (73) lt0001 lt0001a
Anginal symptoms 20 (80) 2 (8) lt0001 16 (57) 0 (0) lt0001 13 (59) 1 (8) lt0001 038
Values are represented as n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL-C high-density lipoprotein cholesterol LV left ventricular NA not applicable OMT optimal medicaltherapy PCI percutaneous coronary interventionaComparison between the OMT group at baseline and the PCI and CABG groups at follow-up
Effects of coronary revascularization on global CFR 125D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

Figure 2 Eighty-two-year-old man treated with optimal medical therapy alone (A B) A global CFR of 264 at baseline (A) was slightly decreased to 257 atfollow-up (B) Sixty-six-year-old man receiving PCI (C D) The polar map of CFR at baseline (C) shows a regional decrease in the anterior to lateral wallGlobal CFR was modestly increased from 170 to 182 (D) after PCI to the LCX (yellow arrows) Seventy-eight-year-old man receiving CABG (E F) A globalCFR of 123 at baseline (E) was increased to 220 (F) after CABG using a RITA graft to the LAD a left internal thoracic artery graft to the LCX and a SVGgraft from the aorta to the RCA and LCX All grafts were patent 8 days after the CABG (F) CABG coronary artery bypass grafting LAD left anteriordescending artery LCX left circumflex artery LMT left main trunk PCI percutaneous coronary intervention RCA right coronary artery RITA right inter-nal thoracic artery SVG saphenous vein graft
124 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
313) P = 0002] (Figure 6) There was no significant difference in per-cent change in regional CFR between coronary territories receiving PCI[193 (-119ndash407)] and OMT alone (Figure 6) In addition thepercent change in regional CFR after PCI did not differ betweenstenoses with fractional flow reserve lt_08 and those with ischaemia onstress perfusion imaging [-37 (-309ndash654) vs 194 (-116ndash400)P = 086]
34 Predictors of changes in CFR inresponse to coronary revascularizationThe characteristics of patients with increased CFR from baseline tofollow-up compared with those without improvement are summarizedin Supplementary material online Table S4 Independent predictors ofchanges in CFR between baseline and follow-up PET are summarized inTable 3 The DSYNTAX score (Model 1) and DLeaman score (Model 2)were independently associated with changes in CFR Importantly the ex-tent of improvement in angiographic disease burden but not the pretestlikelihood or left ventricular ejection fraction was independently associ-ated with changes in CFR There was no significant interaction between
DSYNTAX score and revascularization with CABG (Model 3) indicatingthat CABG did not amplify the effects of revascularization on CFR
35 Propensity score-matched analysisSupplementary material online Table S5 shows the clinical characteristicsof the matched cohort The two groups (n = 9 in each group) were wellmatched at baseline The CABG group showed a significant increase inCFR [164 (113ndash207) vs 187 (152ndash248) P = 0004] while the PCIgroup did not [178 (147ndash246) vs 234 (147ndash274) P = 050] Althoughthere was no significant interaction between time and the tworevascularization groups (P = 069) probably due to small sample sizethe tendency was consistent with the unmatched cohort
4 Discussion
In this prospective multicentre study we demonstrated thatrevascularization of obstructive CAD improved CFR and stress MBF andthat the degree of improvement was correlated with the degree of re-duction of epicardial CAD burden Importantly these changes were
Figure 3 Relationship between CFR and the SYNTAX score (A) or the Leaman score (B) (A) The vertical dotted line indicates a SYNTAX score of 23
Table 2 Proportion of patients achieving risk factor targets and angiographic completeness of revascularization during thestudy period
OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P (between groups
at follow-up)Baseline Follow-up P Baseline Follow-up P Baseline Follow-up P
Systolic blood pressure lt130 mmHg 17 (68) 16 (64) 071 17 (61) 17 (61) 100 13 (55) 16 (73) 026 072
Diastolic blood pressure lt80 mmHg 22 (88) 21 (84) 065 26 (93) 25 (89) 065 21 (95) 21 (95) 100 052
Non-diabeteshaemoglobin A1c lt70 22 (88) 22 (88) 100 19 (68) 20 (71) 056 13 (59) 16 (73) 018 027
Triglycerides lt150 mgdL 19 (76) 16 (67) 041 19 (68) 19 (68) 100 15 (75) 16 (80) 065 064
Non-HDL-C lt130 mgdL 19 (76) 17 (68) 056 20 (71) 23 (82) 026 16 (73) 19 (86) 026 051
No smoking 21 (84) 22 (88) 032 24 (86) 25 (89) 032 17 (77) 21 (95) 0046 070
Achieving gt_5 risk factor targets 18 (72) 14 (64) 016 13 (46) 19 (68) 008 11 (50) 17 (77) 0034 029
SYNTAX score 0ndash8 12 (48) NA NA 8 (29) 19 (68) lt0001 0 (0) 10 (45) lt0001 022a
Leaman score = 0 3 (12) NA NA 2 (7) 16 (57) lt0001 0 (0) 16 (73) lt0001 lt0001a
Anginal symptoms 20 (80) 2 (8) lt0001 16 (57) 0 (0) lt0001 13 (59) 1 (8) lt0001 038
Values are represented as n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL-C high-density lipoprotein cholesterol LV left ventricular NA not applicable OMT optimal medicaltherapy PCI percutaneous coronary interventionaComparison between the OMT group at baseline and the PCI and CABG groups at follow-up
Effects of coronary revascularization on global CFR 125D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

313) P = 0002] (Figure 6) There was no significant difference in per-cent change in regional CFR between coronary territories receiving PCI[193 (-119ndash407)] and OMT alone (Figure 6) In addition thepercent change in regional CFR after PCI did not differ betweenstenoses with fractional flow reserve lt_08 and those with ischaemia onstress perfusion imaging [-37 (-309ndash654) vs 194 (-116ndash400)P = 086]
34 Predictors of changes in CFR inresponse to coronary revascularizationThe characteristics of patients with increased CFR from baseline tofollow-up compared with those without improvement are summarizedin Supplementary material online Table S4 Independent predictors ofchanges in CFR between baseline and follow-up PET are summarized inTable 3 The DSYNTAX score (Model 1) and DLeaman score (Model 2)were independently associated with changes in CFR Importantly the ex-tent of improvement in angiographic disease burden but not the pretestlikelihood or left ventricular ejection fraction was independently associ-ated with changes in CFR There was no significant interaction between
DSYNTAX score and revascularization with CABG (Model 3) indicatingthat CABG did not amplify the effects of revascularization on CFR
35 Propensity score-matched analysisSupplementary material online Table S5 shows the clinical characteristicsof the matched cohort The two groups (n = 9 in each group) were wellmatched at baseline The CABG group showed a significant increase inCFR [164 (113ndash207) vs 187 (152ndash248) P = 0004] while the PCIgroup did not [178 (147ndash246) vs 234 (147ndash274) P = 050] Althoughthere was no significant interaction between time and the tworevascularization groups (P = 069) probably due to small sample sizethe tendency was consistent with the unmatched cohort
4 Discussion
In this prospective multicentre study we demonstrated thatrevascularization of obstructive CAD improved CFR and stress MBF andthat the degree of improvement was correlated with the degree of re-duction of epicardial CAD burden Importantly these changes were
Figure 3 Relationship between CFR and the SYNTAX score (A) or the Leaman score (B) (A) The vertical dotted line indicates a SYNTAX score of 23
Table 2 Proportion of patients achieving risk factor targets and angiographic completeness of revascularization during thestudy period
OMT (n 5 25) PCI (n 5 28) CABG (n 5 22) P (between groups
at follow-up)Baseline Follow-up P Baseline Follow-up P Baseline Follow-up P
Systolic blood pressure lt130 mmHg 17 (68) 16 (64) 071 17 (61) 17 (61) 100 13 (55) 16 (73) 026 072
Diastolic blood pressure lt80 mmHg 22 (88) 21 (84) 065 26 (93) 25 (89) 065 21 (95) 21 (95) 100 052
Non-diabeteshaemoglobin A1c lt70 22 (88) 22 (88) 100 19 (68) 20 (71) 056 13 (59) 16 (73) 018 027
Triglycerides lt150 mgdL 19 (76) 16 (67) 041 19 (68) 19 (68) 100 15 (75) 16 (80) 065 064
Non-HDL-C lt130 mgdL 19 (76) 17 (68) 056 20 (71) 23 (82) 026 16 (73) 19 (86) 026 051
No smoking 21 (84) 22 (88) 032 24 (86) 25 (89) 032 17 (77) 21 (95) 0046 070
Achieving gt_5 risk factor targets 18 (72) 14 (64) 016 13 (46) 19 (68) 008 11 (50) 17 (77) 0034 029
SYNTAX score 0ndash8 12 (48) NA NA 8 (29) 19 (68) lt0001 0 (0) 10 (45) lt0001 022a
Leaman score = 0 3 (12) NA NA 2 (7) 16 (57) lt0001 0 (0) 16 (73) lt0001 lt0001a
Anginal symptoms 20 (80) 2 (8) lt0001 16 (57) 0 (0) lt0001 13 (59) 1 (8) lt0001 038
Values are represented as n ()CABG coronary artery bypass grafting CAD coronary artery disease HDL-C high-density lipoprotein cholesterol LV left ventricular NA not applicable OMT optimal medicaltherapy PCI percutaneous coronary interventionaComparison between the OMT group at baseline and the PCI and CABG groups at follow-up
Effects of coronary revascularization on global CFR 125D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

observed in the context of aggressive risk factor control Finally the ben-efit of PCI for improving CFR was confined to patients with baseline CFRlt20 whereas CABG was beneficial regardless of baseline CFR
The findings of this study extend previous cross-sectional correlationsbetween CFR and angiographic findings3 and prognostic studies of CFR1ndash3
to further understand how coronary revascularization impacts this markerWhile the nuclear substudy of the COURAGE trial evaluated the impact ofrevascularization and OMT on single-photon emission CT findings ofischaemia23 this modality is relatively insensitive compared to CFR Ourstudy represents the first multicentre prospective study to demonstrate
that revascularization improves overall myocardial perfusion and coronaryvasomotor function as measured by PET CFR and stress MBF
The significant association between reduction in angiographic CADburden and improvement in CFR has important clinical implications es-pecially for planning coronary revascularization when multiple stenoticlesions are present Farooq et al18 reported that a greater reduction inthe post-procedure residual SYNTAX score was associated with a bet-ter outcome Our findings support this and offer potential mechanisticinsights into the underlying pathophysiology of the observation thatmore complete revascularization is associated with better prognosis
Figure 4 Comparisons of change in quantitative myocardial perfusion Resting MBF (A) stress MBF (B) and global CFR (C) Individual changes in CFRfrom baseline (BL) to follow-up (FL) in patients with CFR lt20 (D) or gt_20 (E) and in patients with baseline SYNTAX score gt_23 (F) Vertical barsrepresent medians with interquartile ranges CABG coronary artery bypass grafting OMT optimal medical therapy PCI percutaneous coronary interven-tion P = 0025 for interaction between time and CFR daggerP lt 0001 for interaction between time and CFR
Figure 5 Relationship between changes in CFR and the SYNTAX score (A) or the Leaman score (B) CABG coronary artery bypass grafting OMT opti-mal medical therapy PCI percutaneous coronary intervention
126 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

Our study suggests that baseline CFR could be helpful in selecting themanagement strategy in patients with obstructive CAD The resultsfrom multivariate analyses highlight the importance of completerevascularization in ameliorating reduced CFR This adds to data fromTaqueti et al3 suggesting that CABG may be more beneficial than PCI inpatients with severely reduced CFR While the International Study ofComparative Health Effectiveness with Medical and Invasive Approaches(ISCHEMIA trial ClinicalTrialsgov number NCT01471522) is evaluatinghow relative measures of ischaemia should be used to select treatmentstrategy for CAD it is unlikely to directly address the question ofwhether CFR has a role in this decision-making process Our data pro-vide the basis for further studies directly aimed at this question
Our findings may help to explain the results of the ORBITA trial24 Inthe ORBITA trial all patients were pretreated with OMT atrandomization and PCI for single-vessel stenosis did not significantly
increase exercise time over a placebo procedure One reason for thismay be the lack of significant increase in global CFR by PCI for single-vessel stenosis
The moderately strong correlation between CFR and angiographicCAD burden in the present study was in line with previous studies usingthe CAD prognostic index3 The Leaman score19 and CAD prognosticindex3 only take into account the number of diseased vessels and the se-verity of stenosis while the SYNTAX score16 includes not only thesefactors but also coronary lesion complexity (eg bifurcation lesions longlesions heavy calcification) The robustness of these results across angio-graphic scores supports the generality of the relationship between CFRand the anatomic extent of CAD Importantly the residual variability inCFR among patients with obstructive CAD may be explained by diffusedisease and microvascular dysfunction Importantly patients with re-duced CFR and SYNTAX score lt23 for whom microvascular dysfunc-tion may have been a major contributor to CFR reduction comprised29 of the cohort (Figure 3)
41 Study limitationsIn contrast to other PET studies highlighting the benefits of OMT (includ-ing statins beta-blockers and nitrates) and risk factor modification onCFR25 this study found no effects for OMT on myocardial perfusionOne reason for this is that a relatively high prevalence of patients alreadyon OMT before inclusion in the study which reflects evidence-basedpractice in the modern era In addition CFR values were not providedon PET reports to referring cardiologists therefore the impact of thesemetrics on cardiologistsrsquo decision making cannot be determined We didnot assess myocardial viability and changes in left ventricular ejectionfraction in all the study patients which may affect the change in CFR aftertreatment However the appropriateness of coronary revascularizationwas evaluated with conventional myocardial perfusion imaging or inva-sive fractional flow reserve Most critically our findings are subject to se-lection bias and confounding because of the observational nature of thestudy which may introduce bias where the OMT group was reservedfor either very mild or very severe CAD whereas PCI would be per-formed for less advanced CAD compared with CABG The results ofthe subgroup analysis of patients with baseline CFR lt20 while interest-ing may be not robust due to the relatively small sample sizeNonetheless the change with treatment observed in this small cohort isconsistent with the results of the COURAGE nuclear substudy23 Dueto the multicentre observational nature of the study there are some
Figure 6 Per-vessel relationship between changes in regional CFRand coronary arteries categorized by diameter stenosis and treatmentCABG coronary artery bypass grafting OMT optimal medical therapyPCI percutaneous coronary intervention
Table 3 Multivariate linear regression analysis for predicting the percent change in global coronary flow reserve in responseto coronary revascularization
Model 1 Model 2 Model 3
b 95 CI P b 95 CI P b 95 CI P
Intercept -157 -516 to 203 039 -139 -495 to 218 044 -226 -601 to 149 023
Pretest likelihood of obstructive CAD (per 10) 22 -20 to 63 030 24 -23 to 59 038 28 -15 to 70 020
History of PCI or CABG -88 -248 to 72 028 -110 -269 to 48 017 -101 -261 to 60 022
Left ventricular ejection fraction lt50 -17 -178 to 145 084 -18 -179 to 144 083 -25 -187 to 137 076
CABG group 27 -192 to 247 080 11 -217 to 239 092 208 -152 to 568 025
DSYNTAX score -14 -25 to -03 0012 ndash ndash ndash -20 -34 to -06 0007
Interaction (DSYNTAX score CABG group) ndash ndash ndash ndash ndash ndash 14 -08 to 37 021
Log (1 - DLeaman score) (per 1) ndash ndash ndash 118 27 to 208 0011 ndash ndash ndash
CABG coronary artery bypass grafting CAD coronary artery disease CI confidence interval PCI percutaneous coronary intervention
Effects of coronary revascularization on global CFR 127D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

variations in baseline CFR between groups and in follow-up proceduresafter coronary revascularization between hospitals The significance ofthe coronary haemodynamic findings after revascularization needs to beevaluated in patients with a similar atherosclerotic burden and a prede-fined procedure of follow-up angiography Finally we did not assess theassociation between changes in CFR after treatment and the patientsrsquooutcomes Further long-term follow-up studies are needed to determinewhether an increase in CFR leads to better outcomes in patients withCAD
5 Conclusion
Coronary revascularization ameliorated reduced CFR in patients withobstructive CAD Improvement in CFR was proportionate to reductionin angiographic CAD burden by coronary revascularization Theseresults suggest that patients with reduced CFR and high-risk CAD mayhave greater potential to benefit from coronary revascularization
Supplementary material
Supplementary material is available at Cardiovascular Research online
AcknowledgementsThe authors thank Yuuki Tomiyama PhD and Keisuke Kawauchi fortechnical assistance We acknowledge the contributions of the followingcardiologists who participated in this study Hisashi Matsuo (KeiwakaiEbetsu Hospital) Yoichi Yamada Mitsunori Otsubo (ShinSapporoHospital of Cardiology) and Tetsuro Kohya (Sapporo City GeneralHospital)
Conflict of interest none declared
FundingThis work was supported by the Japan Heart Foundation amp Astellas Grantfor Research on Atherosclerosis Update the Uehara Memorial Foundation[to TA] a Grant-in-Aid for Scientific Research from the Japan Society forthe Promotion of Science [grant number JP16K10264 to MN] and theTakeda Science Foundation [to MN]
References1 Murthy VL Naya M Foster CR Hainer J Gaber M Di Carli G Blankstein R Dorbala
S Sitek A Pencina MJ Di Carli MF Improved cardiac risk assessment with noninva-sive measures of coronary flow reserve Circulation 20111242215ndash2224
2 Ziadi MC Dekemp RA Williams KA Guo A Chow BJ Renaud JM Ruddy TDSarveswaran N Tee RE Beanlands RS Impaired myocardial flow reserve onrubidium-82 positron emission tomography imaging predicts adverse outcomes inpatients assessed for myocardial ischemia J Am Coll Cardiol 201158740ndash748
3 Taqueti VR Hachamovitch R Murthy VL Naya M Foster CR Hainer J Dorbala SBlankstein R Di Carli MF Global coronary flow reserve is associated with adversecardiovascular events independently of luminal angiographic severity and modifiesthe effect of early revascularization Circulation 201513119ndash27
4 Camici PG Crea F Coronary microvascular dysfunction N Engl J Med 2007356830ndash840
5 Wilson RF White CW Does coronary artery bypass surgery restore normal maxi-mal coronary flow reserve The effect of diffuse atherosclerosis and focal obstructivelesions Circulation 198776563ndash571
6 Pizzuto F Voci P Mariano E Puddu PE Sardella G Nigri A Assessment of flow ve-locity reserve by transthoracic Doppler echocardiography and venous adenosine in-fusion before and after left anterior descending coronary artery stenting J Am CollCardiol 200138155ndash162
7 Nijjer SS Petraco R van de Hoef TP Sen S van Lavieren MA Foale RA MeuwissenM Broyd C Echavarria-Pinto M Al-Lamee R Foin N Sethi A Malik IS Mikhail GWHughes AD Mayet J Francis DP Di Mario C Escaned J Piek JJ Davies JE Change incoronary blood flow after percutaneous coronary intervention in relation to baselinelesion physiology results of the JUSTIFY-PCI study Circ Cardiovasc Interv 20158e001715
8 Driessen RS Danad I Stuijfzand WJ Schumacher SP Knuuti J Maki M LammertsmaAA van Rossum AC van Royen N Raijmakers PG Knaapen P Impact of revasculari-zation on absolute myocardial blood flow as assessed by serial [15O]H2O positronemission tomography imaging a comparison with fractional flow reserve CircCardiovasc Imaging 201811e007417
9 Task Force Members Montalescot G Sechtem U Achenbach S Andreotti F ArdenC Budaj A Bugiardini R Crea F Cuisset T Di Mario C Ferreira JR Gersh BJ GittAK Hulot JS Marx N Opie LH Pfisterer M Prescott E Ruschitzka F Sabate MSenior R Taggart DP van der WEE Vrints CJ ESC Committee for PracticeGuidelines Zamorano JL Achenbach S Baumgartner H Bax JJ Bueno H Dean VDeaton C Erol C Fagard R Ferrari R Hasdai D Hoes AW Kirchhof P Knuuti JKolh P Lancellotti P Linhart A Nihoyannopoulos P Piepoli MF Ponikowski P SirnesPA Tamargo JL Tendera M Torbicki A Wijns W Windecker S DocumentReviewers Knuuti J Valgimigli M Bueno H Claeys MJ Donner-Banzhoff N Erol CFrank H Funck-Brentano C Gaemperli O Gonzalez-Juanatey JR Hamilos M HasdaiD Husted S James SK Kervinen K Kolh P Kristensen SD Lancellotti P MaggioniAP Piepoli MF Pries AR Romeo F Ryden L Simoons ML Sirnes PA Steg PGTimmis A Wijns W Windecker S Yildirir A Zamorano JL 2013 ESC guidelines onthe management of stable coronary artery disease the Task Force on the manage-ment of stable coronary artery disease of the European Society of Cardiology EurHeart J 2013342949ndash3003
10 Kamiya K Sakakibara M Asakawa N Yamada S Yoshitani T Iwano H Komatsu HNaya M Chiba S Yamada S Manabe O Kikuchi Y Oyama-Manabe N Oba KTsutsui H Cardiac magnetic resonance performs better in the detection of function-ally significant coronary artery stenosis compared to single-photon emission com-puted tomography and dobutamine stress echocardiography Circ J 2014782468ndash2476
11 Manabe O Naya M Aikawa T Obara M Magota K Kroenke M Oyama-Manabe NHirata K Shinyama D Katoh C Tamaki N PETCT scanning with 3D acquisition isfeasible for quantifying myocardial blood flow when diagnosing coronary artery dis-ease EJNMMI Res 2017752
12 Naya M Tsukamoto T Morita K Katoh C Furumoto T Fujii S Tamaki N Tsutsui HOlmesartan but not amlodipine improves endothelium-dependent coronary dilationin hypertensive patients J Am Coll Cardiol 2007501144ndash1149
13 Danad I Uusitalo V Kero T Saraste A Raijmakers PG Lammertsma AA HeymansMW Kajander SA Pietila M James S Sorensen J Knaapen P Knuuti J Quantitativeassessment of myocardial perfusion in the detection of significant coronary arterydisease cutoff values and diagnostic accuracy of quantitative [15O]H2O PET imagingJ Am Coll Cardiol 2014641464ndash1475
14 De Bruyne B Baudhuin T Melin JA Pijls NH Sys SU Bol A Paulus WJ HeyndrickxGR Wijns W Coronary flow reserve calculated from pressure measurements inhumans Validation with positron emission tomography Circulation 1994891013ndash1022
15 Stuijfzand WJ Uusitalo V Kero T Danad I Rijnierse MT Saraste A Raijmakers PGLammertsma AA Harms HJ Heymans MW Huisman MC Marques KM KajanderSA Pietila M Sorensen J Royen N V Knuuti J Knaapen P Relative flow reserve de-rived from quantitative perfusion imaging may not outperform stress myocardialblood flow for identification of hemodynamically significant coronary artery diseaseCirc Cardiovasc Imaging 20158e002400
16 Serruys PW Onuma Y Garg S Sarno G van den Brand M Kappetein AP Van DyckN Mack M Holmes D Feldman T Morice MC Colombo A Bass E Leadley KDawkins KD van Es GA Morel MA Mohr FW Assessment of the SYNTAX score inthe Syntax study EuroIntervention 2009550ndash56
17 Farooq V Girasis C Magro M Onuma Y Morel MA Heo JH Garcia-Garcia HKappetein AP van den Brand M Holmes DR Mack M Feldman T Colombo AStahle E James S Carrie D Fournial G van Es GA Dawkins KD Mohr FW MoriceMC Serruys PW The CABG SYNTAX Score - an angiographic tool to grade thecomplexity of coronary disease following coronary artery bypass graft surgery fromthe SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy EuroIntervention201381277ndash1285
18 Farooq V Serruys PW Bourantas CV Zhang Y Muramatsu T Feldman T HolmesDR Mack M Morice MC Stahle E Colombo A de Vries T Morel MA Dawkins KDKappetein AP Mohr FW Quantification of incomplete revascularization and its asso-ciation with five-year mortality in the synergy between percutaneous coronary inter-vention with taxus and cardiac surgery (SYNTAX) trial validation of the residualSYNTAX score Circulation 2013128141ndash151
19 Leaman DM Brower RW Meester GT Serruys P van den Brand M Coronary arteryatherosclerosis severity of the disease severity of angina pectoris and compromisedleft ventricular function Circulation 198163285ndash299
20 Bittner V Bertolet M Barraza Felix R Farkouh ME Goldberg S Ramanathan KBRedmon JB Sperling L Rutter MK BARI 2D Group Comprehensive cardiovascularrisk factor control improves survival the BARI 2D trial J Am Coll Cardiol 201566765ndash773
128 T Aikawa et alD
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019
21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019

21 Pryor DB Shaw L McCants CB Lee KL Mark DB Harrell FE Jr Muhlbaier LH Califf
RM Value of the history and physical in identifying patients at increased risk for coro-nary artery disease Ann Intern Med 199311881ndash90
22 Austin PC An introduction to propensity score methods for reducing the effects ofconfounding in observational studies Multivariate Behav Res 201146399ndash424
23 Shaw LJ Berman DS Maron DJ Mancini GB Hayes SW Hartigan PM WeintraubWS OrsquoRourke RA Dada M Spertus JA Chaitman BR Friedman J Slomka P HellerGV Germano G Gosselin G Berger P Kostuk WJ Schwartz RG Knudtson MVeledar E Bates ER McCallister B Teo KK Boden WE COURAGE InvestigatorsOptimal medical therapy with or without percutaneous coronary intervention to
reduce ischemic burden results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE) trial nuclearsubstudy Circulation 20081171283ndash1291
24 Al-Lamee R Thompson D Dehbi HM Sen S Tang K Davies J Keeble T MielewczikM Kaprielian R Malik IS Nijjer SS Petraco R Cook C Ahmad Y Howard J Baker CSharp A Gerber R Talwar S Assomull R Mayet J Wensel R Collier D Shun-ShinM Thom SA Davies JE Francis DP Percutaneous coronary intervention in stable an-gina (ORBITA) a double-blind randomised controlled trial Lancet 201839131ndash40
25 Zoghbi GJ Dorfman TA Iskandrian AE The effects of medications on myocardialperfusion J Am Coll Cardiol 200852401ndash416
Effects of coronary revascularization on global CFR 129D
ownloaded from
httpsacademicoupcom
cardiovascresarticle-abstract11511195051230 by Hokkaido U
niversity Library user on 08 January 2019