Embed Size (px)
DESCRIPTION
Lobo & Galloway (2012) Enhanced Handling and Positioning in Early Infancy Advances Development Throughout the First Year CopyLobo & Galloway (2012) Enhanced Handling and Positioning in Early Infancy Advances Development Throughout the First Year CopyLobo & Galloway (2012) Enhanced Handling and Positioning in Early Infancy Advances Development Throughout the First Year Copy
Citation preview

Enhanced Handling and Positioning in Early Infancy AdvancesDevelopment Throughout the First Year
Michele A. Lobo and James C. GallowayThe University of Delaware
Behaviors emerge, in part, from the interplay of infant abilities and caregiver–infant interactions. Cross-cultural and developmental studies suggest caregiver handling and positioning influence infant development.In this prospective, longitudinal study, the effects of 3 weeks of enhanced handling and positioning experiencesprovided to 14 infants versus control experiences provided to 14 infants at 2 months of age were assessedwith follow-up through 15 months of age. Behaviors in prone were immediately advanced. Short-termadvancements occurred in multiple behaviors, including prone, head control, reaching, and sitting behaviors.Longer term advancements, up to 12 months after the experience period, occurred in object transfer, crawlingand walking behaviors. This suggests broad and long-lasting changes can arise via brief periods of change incaregiver–infant interactions.
The role of daily experience in the typical develop-ment of early behaviors is of interest to severaldisciplines. For developmental psychology andearly education, studies that quantify the effects ofdaily experiences provide an empirical test of keytheoretical principles of how infants gain the foun-dational skills for increasingly complex behaviors.For example, this study tests the notion of embod-ied development, which states that developmentalabilities do not emerge de novo but emerge from arich history of exploration and daily interactionsbetween caregivers, young infants, and the physi-cal environment (Adolph & Berger, 2006; Lock-man, 2001). For pediatric rehabilitation, studiesthat quantify the effect of caregiver–infant inter-actions provide an important foundation for newassessment and intervention strategies and high-light the potential benefits of family-centered inter-ventions (Bamm & Rosenbaum, 2008). The generalpurpose of this project was to determine if a rela-tively short period of caregiver–infant interactionswould impact longer term changes in develop-ment.
Specifically, we aimed to determine the develop-mental consequences of a 3-week caregiver-pro-vided enhanced handling and positioning program.
These activities were ‘‘enhanced’’ because theyinvolved behaviors that are not typical of daily lifefor young infants born into Western cultures. Thesebehaviors included supported sitting and standing,encouragement of independent head and trunkcontrol, and emphasis on prone positioning (Kuo,Liao, Chen, Hsieh, & Hwang, 2008). Our previousresearch suggested that enhancing caregiver–infantinteractions immediately advances the emergenceof reaching, as well as object exploration and prob-lem-solving development weeks to months afterstopping the enhanced experiences (Lobo & Gallo-way, 2008; Lobo, Galloway, & Savelsbergh, 2004).The current study focused on quantifying evenlonger term changes through the onset of walkingaround 1 year of age. This study is the first to use aprospective experimental design to assess the effectsof early, prescribed changes in caregiver handlingand positioning practices on infant motor develop-ment into the 2nd year of life. We hypothesized2-month-old infants provided enhanced handlingand positioning experiences would display moreadvanced development throughout the 1st yearof life.
Our hypothesis is supported by cross-culturalstudies suggesting that differences in handling andpositioning can affect infant development. ‘‘Han-dling’’ is those behaviors that occur when caregiversThis research was supported in part by fellowships from The
University of Delaware and The Foundation for Physical Ther-apy.
Correspondence concerning this article should be addressed toMichele A. Lobo, Department of Physical Therapy, 329 McKinlyBuilding, The University of Delaware, Newark, DE 19716. Elec-tronic mail may be sent to [email protected].
Child Development, July/August 2012, Volume 83, Number 4, Pages 1290–1302
! 2012 The AuthorsChild Development ! 2012 Society for Research in Child Development, Inc.All rights reserved. 0009-3920/2012/8304-0014DOI: 10.1111/j.1467-8624.2012.01772.x

are in physical contact with young infants. Differ-ences in handling practices across cultures have beenassociated with differences in the development ofadaptive behaviors, motor behaviors, early commu-nication, and cognitive development (Adolph,Karasik, & Tamis-LeMonda, 2010; Bril & Sabatier,1986; Hopkins & Westra, 1988). For instance, inareas of Kenya, Nigeria, and West India, formal han-dling techniques to encourage sitting and walkingfrom birth have resulted in infants sitting andwalking months earlier than those in Western cul-tures. Non-Western caregivers using similar formalhandling techniques have infants with better headcontrol at 1 month and advanced sitting and stand-ing at 6 months of age compared to infants born tomothers not using such practices (Hopkins & Westra,1989).
Young, immobile infants also spend consider-able time being placed in positions by caregivers.Descriptive studies suggest that greater experiencein multiple positions in the months after birth isassociated with better development in the 1st yearfor healthy infants and those born preterm and atrisk for delays (Fetters & Huang, 2007). Reducedexperience in the months after birth in the proneposition, a position that is especially challengingfor young infants and that most caregivers avoidor utilize very little, is associated with delayeddevelopment in certain skills in the 1st year of life(Kuo et al., 2008; Majnemer, 2007). Therefore,theoretical and cross-cultural work suggests thatcaregivers facilitate infants’ development throughtheir everyday handling and positioning inter-actions. This prospective, longitudinal, multiple-group study specifically tested this proposal. Ourgoal was to build upon these findings from acrosscultures and within Western cultures to create anenhanced handling and positioning programaimed at advancing future development.
Process by Which Handling and Positioning WereExpected to Affect Developmental Change
We expected a relatively brief period of enhancedhandling and positioning would have longerlasting effects for two reasons. First, the alteredhandling and positioning activities were expectedto advance infants’ foundational abilities that aredevelopmentally linked to future skills. Forinstance, being placed in a range of positionsallows infants to experience a variety of possibili-ties for action, views of the world, levels of arousaland social interaction, and postural and strengthrequirements (Fogel, Messinger, Dickson, & Hsu,
1999). These opportunities were expected to leadto corresponding changes in infants’ potential toperceive, act, and attend within their world. Sec-ond, we expected caregivers would adapt to theirinfants’ emerging abilities and continue advancingtheir interactions even outside of and after thehome experience period. A cycle would occur inwhich changes in caregivers or infants would inturn create change in the other (Bronfenbrenner,1979). For instance, our work and others’ suggestthat once caregivers observe their infants attempt-ing to reach for objects, they begin to presentobjects to infants more often within reach soinfants have greater opportunities daily for objectexploration (Fogel, 1997; Lobo & Galloway, 2008;Reed & Bril, 1996). This ongoing cycle of changesupports the emergence of novel behaviors indevelopment and the maintenance of gains whendevelopment is advanced through early interven-tion (Gottlieb, 1983; Ramey & Ramey, 1998). Thepresent study aimed to accelerate this cycle byeducating caregivers to use handling and position-ing techniques to facilitate developmental advance-ments that were expected to continue well into thefuture.
We expected the handling and positioning expe-riences to have broad developmental effectsbecause they aimed at enhancing early perceptual-motor experiences across a variety of postures andactivities. Some literature suggests that the effectsof early experiences are specific. For instance, task-specific activities focused on advancing targetskills, like sitting or stepping, can advance the onsetof those target skills (Vereijken & Thelen, 1997;Zelazo, Zelazo, Cohen, & Zelazo, 1993). Similarly,perception of traversibility of slopes has been dem-onstrated to be dependent upon specific experiencewith each mode of locomotion, such as creeping onhands and knees and walking (Adolph, Tamis-LeMonda, Ishak, Karasik, & Lobo, 2008). On thecontrary, other studies have suggested that theeffects of experiences can be much broader. Forinstance, sitting ability has been shown to advanceknowledge about object properties (Soska, Adolph,& Johnson, 2010). Early experiences to advancereach onset also advance future object explorationand means–end problem-solving ability (Lobo &Galloway, 2008). And early experiences in proneadvance the future ability to crawl on hands andknees (Adolph, Vereijken, & Denny, 1998). Thepresent study aimed to utilize a variety of earlyexperiences in order to advance the development ofthose skills practiced as well as to advance thedevelopment of future related skills.
Handling and Positioning Advance Development 1291

Method
Participants
Twenty-eight families with infants born full-termwere recruited from the local community at2 months of age. Inclusion criteria were typicaldevelopment and no medical diagnoses. Twenty-six of the infants were Caucasian and 2 wereAfrican American. Caregivers provided informedconsent. Three additional families were excludedfrom the study because they did not meet the mini-mum experience performance criterion (see belowfor details).
Experience Groups
Infants were randomly assigned to either thesocial experience (control) group or the handlingand positioning experience (experimental) group.Infants were matched for gender so each group hadseven males and seven females.
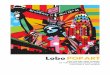
Experiences were provided to infants by caregiv-ers 15 min daily the first 3 weeks of the 60-weekstudy when infants were in an awake and alertstate. Caregivers were informed they could performthe experiences in shorter segments throughout theday if necessary to ensure infants remained in apositive behavioral state during the activities. Care-givers received an illustrated manual and trainingfrom an experimenter at the first study visit (seeFigure 1). They were given a diary to chronicle thefrequency, duration, and content of their sessions.There was a minimum experience performancecriterion of 60% of the days for inclusion in thestudy. Each participant’s diary was examined afterthe prescribed home experience period and anyonenot meeting the 60% criterion was excluded fromthe study at that point. The same experimenter, alicensed pediatric physical therapist, trained allfamilies and conducted the visits.
At the second study visit caregivers were offeredthe opportunity to ask questions, were asked todemonstrate the home experiences without refer-ring to the manual, and were offered any sugges-tions to improve the provision of the activities ifthey deviated from the instructions. After the endof the experience period (third study visit), caregiv-ers were no longer required to perform the activi-ties with their infants.
Social Experience (Control)
Caregivers in the control group were asked toplace their infants in supine and engage them in
face-to-face interaction for 15 min daily (seeFigure 2a for related image and online supportinginformation Appendix S1 for more detail). The aimof these experiences was to control for the socialinteraction and associated general movements thatinfants in the experimental group would receive.Therefore, the social experiences chosen were typi-cal for this developmental period and incorporatedthe social and supine general movement compo-nents of the experimental experiences. Caregiverswere asked to use minimal physical interaction andno objects during these interactions and to use theirface and voice to encourage infants to attend tothem. We did not choose more advanced socialexperiences because it was likely that such experi-ences would accelerate development in other ways.
Handling and Positioning Experience (Experimental)
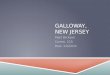
Caregivers in the experimental group were askedto perform advanced handling and positioningactivities with their infants 15 min daily. The spe-cific activities involved caregivers encouraging andassisting infants: (a) by placing them in prone onthe floor or caregiver while encouraging them topush up to lift their head, (b) by pulling them upand lowering them down slowly between sittingand supine while assisting them to keep their headin line with their body, (c) by supporting them insitting and standing while swaying them slowly indifferent directions while encouraging them toweight bear and to reorient their body upright withrespect to gravity, and (d) by moving their hands tomidline for play to encourage a shift from lateral tomore midline arm placement (see Figure 2b–g forrelated images and online supporting information
Figure 1. Time line showing the schedule of home experience,assessments, and home visits in relation to the ages ofparticipants.
1292 Lobo and Galloway

Appendix S2 for more detail). These activities pro-vided enhanced perceptual-motor experience acrosspositions in order to promote abilities includingstrength, postural control, and midline hand behav-ior. These activities also involved a fair amount ofsocial interaction between caregivers and infants.
Procedure
Assessments in the Home
The same experimenter, a licensed pediatricphysical therapist, visited families in their homes for6 visits across the first 3 months of the study. Theaverage age of infants at each visit was 9, 10.5, 12,15, 18, and 21 weeks of age (see Figure 1 for assess-ment schedule). There were no differences in theages of infants in each group at the start of the studyor at subsequent visits (age in weeks Visit 1: control8.7 ± 0.9, experimental 8.9 ± 0.7; Visit 2: control 10.3± 0.9, experimental 10.6 ± 0.8; Visit 3: control 11.8 ±0.8, experimental 11.9 ± 0.7; Visit 4: control 14.8 ±0.7, experimental 14.9 ± 0.9; Visit 5: control 17.9 ± 0.8,experimental 17.9 ± 0.9; Visit 6: control 20.6 ± 0.8,
experimental 20.8 ± 1.0). Visits were documentedvia video recordings so coders blind to groupassignment and not present for visits could code theassessments described below. The visits were con-ducted when infants were in an awake and alertstate. The first and second visits also included train-ing activities for caregivers as aforementioned.
Alberta Infant Motor Scale (AIMS). At every homevisit, infants’ general motor ability was assessedusing the AIMS. This is a valid and reliable assess-ment tool that compares young infants’ motor per-formance with a normative sample. It consists ofobservation of infants’ weight bearing, posture, andantigravity movement in four positions ⁄ subscales:supine, prone, sitting, and standing (Piper, Pinnell,Darrah, Maguire, & Byrne, 1992). Each subscaleconsists of a series of behaviors infants may beobserved to progress through developmentally. Forinstance, in prone, infants may progress throughpushing up on their arms with their elbows behindtheir shoulders, then with their elbows in line withtheir shoulders, and then may demonstrate the abil-ity to lift their heads higher and shift their weight.Infants receive a score of 1 for behaviors they are
a b c
d e
f g
Figure 2. Caregivers in the social experience (control) group (a) were asked to place their infants in supine and engage them in face-to-face interaction without objects for 15 min daily. Caregivers in the handling and positioning experience (experimental) group wereasked to perform activities for 15 min daily to encourage and assist pushing up in prone (b, c), pulling up and lowering down betweensupine and sitting (d), maintaining head and upper body control in assisted sitting and standing (e, f), and moving hands to midline (g).
Handling and Positioning Advance Development 1293

observed performing and a 0 for more advanceditems they were not observed performing. There-fore, each point received reflects an infant’s abilityto behave at a new level within each position.
Reaching. At every home visit, infants’ reachingability was assessed in supine and seated in a cus-tom chair. In each position, infants were given one3-min trial to interact with a stationary, midline toyheld an arm’s length away at chest level.
Caregiver Questionnaire
Caregivers were provided written questionnairesat the start of the study and at the final home visitat 5 months of age. The questionnaires assessedinfants’ sleeping position and if and how caregiversreportedly changed the ways they interacted withtheir infants as a result of participation in this study(see online supporting information Appendix S2).
Follow-up Developmental Assessment
From the end of the home assessments at5 months of age until the onset of independentwalking between 10 and 15 months of age, infantswere followed using a reliable and valid ParentMilestone Report Form (Adolph, Robinson, Young,& Gill-Alvarez, 2008; Bodnarchuk & Eaton, 2004).Caregivers were asked to track their infant’s devel-opment on behaviors from reaching through creep-ing on hands and knees and walking. Once weeklythey documented whether they observed theirinfant performing each of the behaviors. Then atthe end of each month, an experimenter blind togroup assignment collected these data from thecaregiver by phone and recorded them.
Variables
Assessments in the Home
Alberta Infant Motor Scale. A trained experimenterwho did not perform the home visits and was blindto group assignment and the details of the studyscored the AIMS assessments from video. A secondscorer, also blind to group assignment and not pres-ent at visits, scored 20% of the assessments to ensureinterrater reliability with the primary scorer. Thenumber of item scores agreed and disagreed on wasdetermined and the percentage of reliability wascalculated using the equation: [agreed ⁄ (agreed + dis-agreed)] · 100. Interrater reliability between the twoscorers was 94%. Infants received a score for eachsubscale (supine, prone, sitting, and standing) as well
as a total score (sum of the four subscale scores). Weanalyzed scores at Visit 1 to ensure groups were simi-lar at the start of the study. We analyzed changes inAIMS scores for infants in each group during the 3-week experience period (2–3 months of age) andthroughout the home assessment period (through5 months of age) to assess the immediate and short-term effects of the home experiences.
Reaching. Two trained experimenters blind togroup assignment coded the number of timesinfants contacted the midline object from thereaching assessment videos. Each time the infant’shand came in contact with the object, a contactwas coded. From these data, we calculated thevisit of reach onset for each infant, or the first visitwhen the infant contacted the midline object morethan 10 times total (total contacts supine andseated in the chair) and the number of object con-tacts for all subsequent visits remained greaterthan this value.
Coding reliability was assessed for 20% of thecoded data across age using the equation describedabove. Intrarater reliabilities were 95% and 96% foreach coder. Interrater reliability was 92% betweencoders.
Caregiver Questionnaire
Caregiver responses were categorized for statisti-cal analyses by two experimenters blind to groupassignment. Interrater agreement for categorizationwas Kappa = 1.00 (p < .001). Sleeping position wascategorized into supine, prone, or sidelying. Studyparticipation was categorized as either having aneffect or having no effect on caregiver–infant inter-actions. For those who reported participation didaffect their interactions, the ways in which theirinteractions were affected were categorized asincreased social interaction (responses such as‘‘looking,’’ ‘‘attention,’’ or ‘‘talking’’), increased han-dling and positioning interaction (responses such as‘‘postures,’’ ‘‘strength,’’ or ‘‘continued with experi-ence activities’’), or increased play with objects(responses such as ‘‘toys,’’ ‘‘reach,’’ or ‘‘hold’’). Allresponses fell into one of these three categories.
Follow-up Developmental Assessment
The weekly milestone tracking was used to deter-mine the week of each milestone’s onset in relationto the week the infant had his or her first study visit.When infants were first observed performing abehavior 3 weeks consecutively, the onset of thebehavior was defined as the first of these weeks. For
1294 Lobo and Galloway

instance, if an infant was observed by his or hercaregiver transferring objects from hand to hand at15, 16, and 17 weeks after the week of the infant’sfirst visit, the onset of this behavior was recorded ashappening at 15 weeks after the first visit. To pro-vide readers with a better perspective of develop-mental time, these results are reported both in termsof weeks from the first visit as well in terms ofinfants’ ages in months.
Data Analysis
Mann–Whitney U nonparametric tests were usedto compare the two groups for all variables. Medianfollowed by minimum and maximum values inparentheses and effect size using Cohen’s correla-tion coefficient (r) are reported for all comparisons,with r = 0.10 representing a small effect, r = 0.30representing a medium effect, and r = 0.50 repre-senting a large effect (Cohen, 1992). One-tailed testswere utilized for variables we hypothesized wouldbe different as a result of the experiences, such aschange in AIMS score after enhanced experience.Two-tailed tests were used for the remainder of thevariables, such as age at the first visit. Only resultswith significance values £ 0.05 are reported. To bet-ter describe these significant group changes, wealso report individual counts of behaviors. To testthe robustness of the findings, all analyses werealso performed using parametric independent sam-ple t tests with Levene’s test for equality of vari-ances. The parametric and nonparametric findingswere consistent but the nonparametric findings arereported here because many of the variables areordinal and our sample sizes are modest.
Results
Groups Began the Study at a Similar Age andDevelopmental Level
Infants were similar at the start of the study. Allinfants were born full-term and there was no differ-ence in weight at birth between groups. Infants ineach group started the study at the same age:con-trol Mdn 8.4 (7.7, 11.0), experimental Mdn 8.7 (8.1,11.2) weeks old, U = 72.50, ns, r = )0.22. There wasno reported difference in sleeping position ofinfants (U = 82.50, ns, r = )0.22). The majority ofinfants in each group slept in supine. Sleep positiondifferences between groups could have been animportant confound because motor development inthe 1st year of life may be delayed in infants who
sleep supine compared to infants who sleep prone(Davis, Moon, Sachs, & Ottolini, 1998).
At the start of the study, the control and experi-mental groups had similar total AIMS scores:con-trol Mdn 9 (8, 13), experimental Mdn 9 (7, 13); andsimilar scores for the supine:control Mdn 3 (2, 5),experimental Mdn 3 (2, 5); sitting:control Mdn 1 (1,2), experimental Mdn 1 (1, 2); and standing:controlMdn 2 (1, 2), experimental Mdn 2 (2, 2); AIMSsubscales (total U = 60.50, ns, r = )0.35; supineU = 92.00, ns, r = )0.06; sitting U = 98.00, ns,r = .00; standing U = 77.00, ns, r = )0.34). Controlinfants did have better prone subscale scores at thisvisit, about 1 point higher:control Mdn 3 (2, 6),experimental Mdn 2 (1, 6) (U = 53.50, p £ .05,r = )0.41). Because the difference was in favor ofour control group and we believed our experienceswould advance development for the experimentalgroup beyond this difference, this small differenceat the start of the study was acceptable. Infants’median total AIMS scores were at the 50th percen-tile for both groups at the start of the study.
Groups Had Similar Amounts of Home Experience
During the 3-week home experience period, bothgroups had a similar number of days of experi-ence:control Mdn 17.5 (14, 25), experimental Mdn18.5 (17, 23) days (U = 63.00, ns, r = )0.31) and sim-ilar total minutes of experience:control Mdn 267.5(210, 795), experimental Mdn 268 (182.5, 403) totalminutes; control Mdn 15 (13.4, 31.8), experimentalMdn 13.8 (10.3, 19.19) min ⁄ day (U = 81.50, ns,r = )0.14).
Immediate Effects of the Experiences: Advancements inProne Abilities
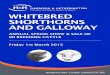
At the end of the 3-week home experience periodwhen infants were 3 months old, infants in theexperimental group were already making develop-mental advances compared to control infants (seeFigure 3). From 2 to 3 months of age they hadgreater increases in their AIMS prone subscalescores:control Mdn 1 (0, 4), experimental Mdn 2(0, 5) points change (U = 47.50, p £ .01, r = )0.45).This manifested from greater advancements in theirability to push up on their forearms and extendedarms, to shift their weight for early mobility, and toraise one arm to reach for objects and people in theprone position. After the home experience, controlinfants’ median total AIMS score was at the 65thpercentile, while experimental infants’ medianscore increased to the 80th percentile.
Handling and Positioning Advance Development 1295

Short-Term Effects of the Experiences: Advancementsin Global Motor Abilities, Hand Movement, Object
Interaction, and Head Righting
After the 3-week home experience period, care-givers were no longer asked to perform the homeactivities, yet experimental infants continued todemonstrate advancements. Specifically, from 3 to5 months of age, experimental infants demonstratedadvanced midline hand movement ability, objectinteraction abilities, head righting abilities, and glo-bal motor development. They began to rest theirhands in midline rather than lateral in supine, anitem on the AIMS, earlier than control infants (at3 months: 8 of 14 control infants; 12 of 14 experi-mental infants, U = 70.00, p £ .05, r = )0.31; at4 months: 10 of 14 control infants; all 14 experimen-tal infants, U = 70.00, p £ .05, r = )0.40). Next, theyreached for objects earlier in the reaching assess-ment:control Mdn 18 (12, 21), experimental Mdn13.5 (10.5, 21) weeks of age (U = 59.00, p £ .05,r = )0.34). Control infants were reaching in themiddle of the typical age expected (3–5 months ofage) by about 4.2 months of age, while experimen-tal infants were reaching at the early end by about3.1 months of age (Thelen, Corbetta, & Spencer,1996). At the first visit no infants were reachers. Atthe second and third visits (around 2.5 and then3 months old), no control infants and 4 experimen-tal infants were reachers (Visit 2: U = 28.00, p £ .05,r = 0.4; Visit 3: U = 28.00, p £ .05, r = 0.4). At the
fourth visit (around 3.75 months old), 6 control and9 experimental infants were reachers. At the fifthvisit (around 4.5 months old), 10 control and 12experimental infants were reachers. At the lasthome visit (around 5.25 months old), 13 controland all 14 experimental infants were reachers. Afterreach onset, experimental infants were able to righttheir heads earlier by keeping it in line with theirtrunk when pulled by the hands from supine to sit-ting, another item on the AIMS (at 4 months: 5 of14 control infants, 10 of 14 experimental infants,U = 63.00, p £ .05, r = )0.35; at 5 months: 9 of 14control infants, 13 of 14 experimental infants,U = 70.00, p £ .05, r = )0.34).
Infants in the experimental group were makinggreater global motor developmental advances com-pared to control infants (see Figure 4). Through5 months of age they had greater increases in theirAIMS total scores, prone subscale scores, andsitting subscale scores—points change total: controlMdn 8 (5, 12), experimental Mdn 11 (8, 18)(U = 45.50, p £ .01, r = )0.46); prone: control Mdn 3(2, 6), experimental Mdn 5 (3, 9) (U = 42.50, p £ .01,r = )0.45); sitting:control Mdn 2 (0, 4), experimentalMdn 3 (1, 7) (U = 62.00, p £ .05, r = )0.34). At5 months of age, control infants’ median total AIMSscores were at the 30th percentile, while experimen-tal infants’ scores were at the 50th percentile.
Figure 3. Immediate changes in development for each groupduring the experience period represented by changes in totaland subscale scores on the Alberta Infant Motor Scale (AIMS).Note. The time frame represents 3 weeks between 2 and3 months of age in this box plot.*p £ .05.
Figure 4. Short-term changes in development for each groupduring the home assessment period represented by changes intotal and subscale scores on the Alberta Infant Motor Scale(AIMS).Note. The time frame represents 3 months from 2 to 5 months ofage in this box plot.*p £ .05.
1296 Lobo and Galloway

Longer-Term Effects of the Experiences: Advancementsin Object Manipulation and Locomotor Abilities
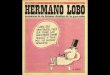
In the 7–12 months following the 3-week homeexperience period, experimental infants continuedto show important advances in object manipulationand locomotion abilities (see Figure 5). Infants in theexperimental group transferred objects from onehand to the other 2.5 weeks earlier, explored theirenvironment by creeping or crawling on their handsand knees 5 weeks earlier, walked supported side-ways holding on to furniture or forward holding onto an adult’s hands 2.5 weeks earlier, and walkedalone less than 10 ft 6 weeks earlier—weeks fromthe first study visit object transfer:control Mdn 15.5(10, 24), experimental Mdn 13 (4, 18) (U = 57.50,p £ .05, r = )0.35); creeping on hands and knees:control Mdn 29 (16, 35), experimental Mdn 24 (11,38) (U = 58.00, p £ .05, r = )0.30); walking with sup-port: control Mdn 33 (28, 46), experimental Mdn 30.5(24, 43) (U = 60.00, p £ .05, r = )0.33); walking inde-pendently: control Mdn 45 (37, 67), experimentalMdn 39 (31, 55) (U = 57.50, p £ .05, r = )0.35).
Transferring objects from hand to hand typicallyemerges between 5 and 6 months of age and wasdefined in the parent report form as when the ‘‘babycan pass a small toy, cookie, or other object fromhand to hand.’’ This behavior emerged in controland experimental infants within the typical range at5.5 months of age and 5.3 months of age, respec-
tively. Creeping on hands and knees typicallyemerges around 8–10 months of age and wasdefined in the parent report form as crawling morethan 10 ft using only the hands and knees for sup-port, with the back straight, the knees under thehips, and the elbows under the shoulders. Thisbehavior emerged for control infants within the typi-cal range at 8.7 months of age and for experimentalinfants a bit earlier at 7.5 months of age. Walkingwith support typically emerges between 10 and11 months of age and was defined in the parentreport form as the infant supporting his or her ownweight and taking several steps but receiving assis-tance to balance by holding furniture and steppingsideways or holding an adults’ hands and steppingforward. This behavior emerged for control infantsjust before the typical range at 9.7 months of age andfor experimental infants a bit earlier at 9.1 months ofage. Walking independently typically emergesaround 12 months of age and was defined in theparent report form as the infant taking at least onestep alone with each foot without the support of oth-ers or objects (Haywood & Getchell, 2009; Long &Cintas, 1995; Piek, 2006). This behavior emerged forcontrol infants at the typical age of 12.4 months andfor experimental infants a bit earlier at 11 months.
The Experiences Elicited Different Changes inCaregiver-Infant Interactions
A similar majority of caregivers in each groupreported on the parent questionnaire that participa-tion in the study did affect the way they interactedwith their infants (12 of 14 control infants, all 14experimental infants). However, the specific wayscaregivers reported their interactions were affectedwere quite different between groups (U = 175.00,p < .01, r = 0.78). Thirteen of the 14 experimentalcaregivers reported that they handled or positionedtheir infants differently. In contrast, 10 of the con-trol caregivers who reported their interactions withtheir infants were affected reported that theyplayed more socially with their infants. The remain-ing families in each group reported greater increasein interest playing with toys.
Discussion
Infants who received enhanced handling and posi-tioning experiences at 2 months of age showedadvanced abilities that began immediately and con-tinued through 12 months after the experiences.Behaviors in prone were immediately advanced,
Figure 5. Longer term changes in age of milestone emergence forinfants in each group based on the reaching assessment andcaregiver report form.Note. Milestones represented are reaching for midline objects(reach), transferring objects between the hands (transfer),creeping on hands and knees (creep), walking with support(walk sup), and walking independently (walk ind).*p £ .05.
Handling and Positioning Advance Development 1297

followed by advancements in prone, head control,midline hand control, reaching, and sitting behav-iors. Longer term advancements occurred in objecttransfer, creeping on hands and knees, and walkingbehaviors.
How did a relatively short period of advancedexperience lead to such lasting and widespreadadvancements in infants’ motor abilities? How didinfants improve not only on tasks experienced,such as hands to midline and head righting, butalso on other tasks, such as reaching and transfer-ring objects? To answer these questions, we firstdiscuss the interrelation of the skills advanced. Sec-ond, we discuss some key changes in infants, care-givers, and caregiver–infant interactions that likelycreated and maintained this advanced developmen-tal trajectory.
Skills Advanced Share Common Thread
Infants in the experimental group were advancedin skills ranging from floor play to object manipula-tion and locomotion. Although these skills mayat first glance seem very different, they all sharea common thread. These skills do not emerge denovo but from a rich history of perceptual-motorexperience (Kamm, Thelen, & Jensen, 1990). All arealso important vehicles for exploration and thedevelopment of embodied cognition (Adolph &Berger, 2006; Lockman, 2001). Behavioral develop-ment in infancy can often be linked to previousexperience with seemingly unrelated activities. Forinstance, a certain level of experience and control inprone and supine precedes the onset of indepen-dent sitting (Green, Mulcahy, & Pountney, 1995).Prone experience is connected to the developmentof creeping on hands and knees as it allows infantsto coordinate the co-occurrences of head orienting,reaching, and kicking (Goldfield, 1989). Therefore,advancements in development so far after ourexperience period ended were likely related toexperimental infants’ enriched perceptual-motorhistory. We now discuss some mechanisms throughwhich these experiences may have advanced devel-opment.
Changes Within Infants
The likely consequence of experimental infants’early experiences was enhanced priming of theirperception-action and cognitive systems. Below wedescribe some ways experience may have advancedthe development of experimental infants’ percep-tion-action and cognitive systems.
First, infants in the experimental group likelydeveloped advanced postural control. Posturalcontrol is important for each of the skills wemeasured and develops as a result of movementand experience in a variety of positions (Bertenthal& Von Hofsten, 1998; Chen, Metcalfe, Chang, Jeka,& Clark, 2008). For instance, the postural controlrequired to manipulate objects develops, in part,from earlier experiences maintaining balance inreaction to perturbations from spontaneous armmovements (Thelen & Spencer, 1998). The posturalcontrol required to manipulate objects while sittingor standing is not present when infants begin toindependently assume these positions but developsthrough exploratory play in various positions (vander Fits, Klip, van Eykern, & Hadders-Algra, 1999).As experimental infants explored their perception-action possibilities across positions they likely con-structed a range of complex anticipatory reactionsto maintain balance and body alignment (Metcalfe& Clark, 2000).
Second, experimental infants may have physio-logically primed their neuromuscular systems to bebetter prepared for action. The experimental groupwas exposed to various positions and movementexperiences that required head, trunk and limbmuscles to work against gravity, which is known toincrease muscular strength (Kleyweg, Vandermeche,& Schmitz, 1991). Experiencing movements acrosspositions also likely taught them to coordinatetheir muscular forces along with inertial forcesfrom distant joints and gravity to produce smooth,functionally adaptive movements (Galloway &Koshland, 2002). In addition, the neuromuscularactivity associated with the handling and position-ing experiences may have guided the pruning andstrengthening of neuronal connections, the pruningand strengthening of one neuronal innervation permuscle fiber, and the development of the corticospi-nal system, all processes shaped by perception-action experience (Eyre, Taylor, Villagra, Smith, &Miller, 2001; IJkema-Paassen & Gramsbergen, 2005;Martin, Choy, Pullman, & Meng, 2004). Conse-quently, experimental infants may have acceleratedthese processes so their neuromuscular systemswere physiologically better equipped to executeactions across a variety of positions.
Third, experimental infants may have primedtheir perceptual systems to better process sensoryinformation. Many perceptual systems are notmature at birth but develop, in part, as a result ofexperience. Each position an infant is held orplaced in allows for different actions and accompa-nying perceptual experiences. For instance, more
1298 Lobo and Galloway

kicking behavior occurs in supine and more hand-to-mouth behavior occurs in sidelying (Geerdink,Hopkins, Beek, & Heriza, 1996; Rocha & Tudella,2008). Changing head position with respect to grav-ity also provides a variety of visual and vestibularexperiences (Shumway-Cook, 1992). Experience isimportant in the development of the visual andvestibular systems as infants must learn to keeptheir heads stable in order to receive reliable per-ceptual information (Pozzo, Levik, & Berthoz,1995). Experience is also crucial for infants to learnhow to accurately perceive information from thesesystems. For instance, when infants begin toassume a standing position, this novel uprightexperience allows them to adapt their otolithicresponses and sensitivities so they can detect move-ment of the body in planes not previously experi-enced through crawling and rolling (Bril & Ledebt,1998). Therefore, experimental infants likely hadenhanced ability to detect and process perceptualinformation across positions.
Changes in Caregivers and Caregiver–Infant Interactions
The interplay between caregivers’ perceptionsand actions and infants’ abilities underlies the devel-opmental process and was a focus of this study.Even in the first months of life, typical developmentinvolves a cooperative process of communicationand interaction between caregivers and infants asinfants facilitate and regulate their own learningin conjunction with guidance from more experi-enced caregivers. Caregivers who are more sensitiveat reading infants’ cues and adapting their interac-tions to match infants’ abilities and needs haveinfants with better social-emotional and cognitivedevelopment at 1–2 years of age (Forcada-Guex,Pierrehumbert, Borghini, Moessinger, & Muller-Nix,2006; Treyvaud et al., 2009).
The changes we observed in infants’ abilitiesmost likely resulted from an interaction betweenchanges in infants’ abilities and in caregivers’ per-ceptions and interactions. Interestingly, caregiversin the two groups reported different effects of par-ticipation in the study on their everyday interac-tions with their infants. Control group caregiversreported greater social play and improved visualattention for their infants, while experimentalgroup caregivers reported greater handling andpositioning play and improved strength and pos-tural control for their infants. These reports suggestthat the changes in infants’ developmental abilitieswere not simply the result of 15 min of isolatedexperience across 3 weeks in time but that they
were also the result of changes in caregivers’ per-ceptions and the everyday play interactionsbetween caregivers and infants that extended wellbeyond the prescribed experience period.
Significance of the Findings
The findings of this study have important impli-cations for developmental psychology and earlychildhood education. First, they provide compre-hensive support for the proposal that caregiver han-dling and positioning behaviors can instill broadand long-lasting developmental changes. Second,they provide additional empirical support for theproposal that behaviors emerge, evolve, andbecome increasing adaptive as a function of a com-plex history of experiences dependent upon theinterplay of infant abilities, caregiver–infant inter-actions, and environment. Third, they help us betterunderstand the complex process of developmentand provide the foundation for more specifichypothesis testing. For instance, many basic ques-tions remain, such as what are the cues caregiversrespond to as they provide more advanced opportu-nities for their infants in development; what sourcestypically inform and guide caregivers’ perceptionsabout how to handle, position, and play with theirinfants; and how does attainment of novel behaviorssuch as reaching, sitting, crawling, or walking affectdaily interactions between caregivers and infantsand the structuring of their environment.
The findings of this study also have importantimplications for medical professionals and earlyeducators working with populations with specialneeds. The findings support that caregivers, theirinteractions with infants, and the environment theycocreate with infants are all critical components ofthe developmental process and are important com-ponents of early assessment and interventionprograms (Wilder & Granlund, 2003). The findingssuggest early interventions should be jointly aimedat educating caregivers and enabling infants(Cotnoir-Bichelman, Thompson, McKerchar, &Haremza, 2006). Therefore, the results support thenotion that a key component of early interventionshould be focused caregiver education targetedtoward advancing foundational abilities at develop-mentally appropriate times (Mahoney, Robinson, &Perales, 2004).
Although the results of this study provideimportant insights into development, limitations inthe design leave several questions open for futureinvestigation. First, participants enrolled in thestudy by showing motivation to respond to recruit-
Handling and Positioning Advance Development 1299

ment letters and to perform daily play activitieswith their infants so our volunteer demographicmay not represent all caregivers in the general pop-ulation. Although we did not collect data on socio-economic status from families, the neighborhoodsand occupations we observed suggest none of ourparticipating families had low socioeconomic sta-tus. All of the infants in the study were healthy andtypically developing. Therefore, future research isnecessary to determine how these experiencesapply across contexts and populations, especially aspotential interventions to advance development inchildren born with biological or environmental riskfactors (Dodge, 2011). In addition, future researchwith larger, more diverse sample groups is neces-sary to answer important questions, such as forwhom do these experiences have no effect and whyand are there subgroups of caregivers less likely toperform the experiences. Finally, there remainimportant unanswered questions about dosageeffects to better understand the timing and amountof experience provision that is most effective atadvancing development. In the same vein, we needto better understand the constraints that may limitdevelopment, such as development of the neuro-muscular system, as well as the reasons why theamount of variability in typical development is solarge. For instance, the typical age range for theonset of walking is anywhere from 9 to 17 monthsof age (Haywood & Getchell, 2009). A better under-standing of the sources of this variability and theconstraints that must be overcome for the emer-gence of novel behaviors is critical for designingeffective early interventions for individuals at riskfor developmental delays and learning disabilities.
References
Adolph, K. E., & Berger, S. E. (2006). Motor development.In W. Damon & R. Lerner (Eds.), Handbook of child psy-chology: Vol. 2. Cognition, perception, and language (6thed., pp. 161–213). New York: Wiley.
Adolph, K. E., Karasik, L. B., & Tamis-LeMonda, C. S.(2010). Moving between cultures: Cross-culturalresearch on motor development. In M. Bornstein (Ed.),Handbook of cross-cultural developmental science: Domainsof development across cultures (Vol. 1, pp. 61–88). Mah-wah, NJ: Erlbaum.
Adolph, K. E., Robinson, S. R., Young, J. W., & Gill-Alvarez, F. (2008). What is the shape of developmentalchange? Psychological Review, 115, 527–543.
Adolph, K. E., Tamis-LeMonda, C. S., Ishak, S., Karasik,L. B., & Lobo, S. A. (2008). Locomotor experience anduse of social information are posture specific. Develop-mental Psychology, 44, 1705–1714.
Adolph, K. E., Vereijken, B., & Denny, M. A. (1998).Learning to crawl. Child Development, 69, 1299–1312.
Bamm, E. L., & Rosenbaum, P. (2008). Family-centeredtheory: Origins, development, barriers, and supports toimplementation in rehabilitation medicine. Archives ofPhysical Medicine and Rehabilitation, 89, 1618–1624.
Bertenthal, B., & Von Hofsten, C. (1998). Eye, head andtrunk control: The foundation for manual development.Neuroscience And Biobehavioral Reviews, 22, 515–520.
Bodnarchuk, J. L., & Eaton, W. O. (2004). Can parentreports be trusted? Validity of daily checklists of grossmotor milestone attainment. Journal of Applied Develop-mental Psychology, 25, 481–490.
Bril, B., & Ledebt, A. (1998). Head coordination as ameans to assist sensory integration in learning to walk.Neuroscience and Biobehavioral Reviews, 22, 555–563.
Bril, B., & Sabatier, C. (1986). The cultural context ofmotor development: Postural manipulations in thedaily life of Bambara babies (Mali). International Journalof Behavioral Development, 9, 439–453.
Bronfenbrenner, U. (1979). The ecology of human develop-ment: Experiments by nature and design. Cambridge, MA:Harvard University Press.
Chen, L. C., Metcalfe, J. S., Chang, T. Y., Jeka, J. J., &Clark, J. E. (2008). The development of infant uprightposture: Sway less or sway differently? ExperimentalBrain Research, 186, 293–303.
Cohen, J. (1992). A power primer. Psychological Bulletin,112, 155–159.
Cotnoir-Bichelman, N. M., Thompson, R. H., McKerchar,P. M., & Haremza, J. L. (2006). Training student teach-ers to reposition infants frequently. Journal of AppliedBehavior Analysis, 39, 489–494.
Davis, B. E., Moon, R. Y., Sachs, H. C., & Ottolini, M. C.(1998). Effects of sleep position on infant motor devel-opment. Pediatrics, 102, 1135–1140.
Dodge, K. A. (2011). Context matters in child and familypolicy. Child Development, 82, 433–442.
Eyre, J. A., Taylor, J. P., Villagra, F., Smith, M., & Miller,S. (2001). Evidence of activity-dependent withdrawal ofcorticospinal projections during human development.Neurology, 57, 1543–1554.
Fetters, L., & Huang, H. H. (2007). Motor developmentand sleep, play, and feeding positions in very-low-birth-weight infants with and without white matter disease.Developmental Medicine and Child Neurology, 49, 807–813.
Fogel, A. (1997). Information, creativity, and culture. InC. D.-R. P. Zukow-Goldring (Ed.), Evolving explanationsof development (pp. 413–443). Washington, DC: Ameri-can Psychological Association.
Fogel, A., Messinger, D. S., Dickson, K. L., & Hsu, H. C.(1999). Posture and gaze in early mother-infantcommunication: Synchronization of developmental tra-jectories. Developmental Science, 2, 325–332.
Forcada-Guex, M., Pierrehumbert, B., Borghini, A., Moes-singer, A., & Muller-Nix, C. (2006). Early dyadicpatterns of mother-infant interactions and outcomes ofprematurity at 18 months. Pediatrics, 118, E107–E114.
1300 Lobo and Galloway
Galloway, J. C., & Koshland, G. F. (2002). General coordi-nation of shoulder, elbow and wrist dynamics duringmultijoint arm movements. Experimental Brain Research,142, 163–180.
Geerdink, J. J., Hopkins, B., Beek, W. J., & Heriza, C. B.(1996). The organization of leg movements in pretermand full-term infants after term age. Developmental Psy-chobiology, 29, 335–351.
Goldfield, E. C. (1989). Transition from rocking to crawl-ing: Postural constraints on infant movement. Develop-mental Psychology, 25, 913–919.
Gottlieb, G. (1983). The psychobiological approach todevelopmental issues. In P. Mussen (Ed.), Handbook ofchild psychology: Infancy and developmental psychobiology(pp. 1–26). New York: Wiley.
Green, E. M., Mulcahy, C. M., & Pountney, T. E. (1995).An investigation into the development of early posturalcontrol. Developmental Medicine and Child Neurology, 37,437–448.
Haywood, K. M., & Getchell, N. (2009). Life span motordevelopment (5th ed.). Champaign, IL: Human Kinetics.
Hopkins, B., & Westra, T. (1988). Maternal handling andmotor development: An intracultural study. GeneticSocial and General Psychology Monographs, 114, 377–408.
Hopkins, B., & Westra, T. (1989). Maternal expectationsof their infants’ development: Some cultural-differ-ences. Developmental Medicine and Child Neurology, 31,384–390.
IJkema-Paassen, J., & Gramsbergen, A. (2005). Develop-ment of postural muscles and their innervation. NeuralPlasticity, 12, 141–151.
Kamm, K., Thelen, E., & Jensen, J. L. (1990). A dynamic-systems approach to motor development. Physical Ther-apy, 70, 763–775.
Kleyweg, R. P., Vandermeche, F. G. A., & Schmitz, P. I.M. (1991). Interobserver agreement in the assessment ofmuscle strength and functional abilities in Guillain-Barre syndrome. Muscle and Nerve, 14, 1103–1109.
Kuo, Y. L., Liao, H. F., Chen, P. C., Hsieh, W. S., &Hwang, A. W. (2008). The influence of wakeful pronepositioning on motor development during the earlylife. Journal of Developmental and Behavioral Pediatrics, 29,367–376.
Lobo, M. A., & Galloway, J. C. (2008). Postural andobject-oriented experiences advance early reaching,object exploration, and means-end behavior. ChildDevelopment, 79, 1869–1890.
Lobo, M. A., Galloway, J. C., & Savelsbergh, G. J. P.(2004). General and task-related experiences affect earlyobject interaction. Child Development, 75, 1268–1281.
Lockman, J. J. (2001). An embodied theory of cognitivedevelopment: Within reach? Behavioral and Brain Sci-ences, 24, 48–48.
Long, T. M., & Cintas, H. L. (1995). Handbook of pediatricphysical therapy. Philadelphia: Williams & Wilkins.
Mahoney, G., Robinson, C., & Perales, F. (2004). Earlymotor intervention: The need for new treatment para-digms. Infants & Young Children, 17, 291–300.
Majnemer, A. (2007). Caregiver practices that influencemotor development: What are the next moves? Develop-mental Medicine and Child Neurology, 49, 807–813.
Martin, J. H., Choy, M., Pullman, S., & Meng, Z. (2004).Corticospinal system development depends on motorexperience. Journal of Neuroscience, 24, 2122–2132.
Metcalfe, J. S., & Clark, J. E. (2000). Sensory informationaffords exploration of posture in newly walking infantsand toddlers. Infant Behavior & Development, 23, 391–405.
Piek, J. P. (2006). Infant motor development. Champaign, IL:Human Kinetics.
Piper, M. C., Pinnell, L. E., Darrah, J., Maguire, T., &Byrne, P. J. (1992). Construction and validation of theAlberta Infant Motor Scale (AIMS). Canadian Journal ofPublic Health, 83, 46–50.
Pozzo, T., Levik, Y., & Berthoz, A. (1995). Head and trunkmovements in the frontal plane during complexdynamci equilibrium tasks in humans. ExperimentalBrain Research, 106, 327–338.
Ramey, C. T., & Ramey, S. L. (1998). Early interventionand early experience. American Psychologist, 53, 109–120.
Reed, E. S., & Bril, B. (1996). The primacy of action indevelopment. In M. L. L. M. T. Turvey (Ed.), Dexteriryand its development (pp. 431–451). Mahwah, NJ: Erlbaum.
Rocha, N., & Tudella, E. (2008). The influence of lyingpositions and postural control on hand-mouth andhand-hand behaviors in 0-4-month-old infants. InfantBehavior & Development, 31, 107–114.
Shumway-Cook, A. (1992). Role of the vestibular system inmotor development: Theoretical and clinical issues. InH. Forssberg & H. Hirschfield (Eds.), Movement disordersin children (pp. 209–216). Basel, Switzerland: Karger.
Soska, K. C., Adolph, K. E., & Johnson, S. P. (2010). Sys-tems in development: Motor skill acquisition facilitatesthree-dimensional object completion. Developmental Psy-chology, 46, 129–138.
Thelen, E., Corbetta, D., & Spencer, J. P. (1996). Develop-ment of reaching during the first year: Role of move-ment speed. Journal of Experimental Psychology: HumanPerception & Performance, 22, 1059–1076.
Thelen, E., & Spencer, J. P. (1998). Postural control duringreaching in young infants: A dynamic systems approach.Neuroscience and Biobehavioral Reviews, 22, 507–514.
Treyvaud, K., Anderson, V. A., Howard, K., Bear, M.,Hunt, R. W., Doyle, L. W., et al. (2009). Parentingbehavior is associated with the early neurobehavioraldevelopment of very preterm children. Pediatrics, 123,555–561.
van der Fits, I. B. M., Klip, A. W. J., van Eykern, L. A., &Hadders-Algra, M. (1999). Postural adjustments duringspontaneous and goal-directed arm movements in thefirst half year of life. Behavioural Brain Research, 106, 75–90.
Vereijken, B., & Thelen, E. (1997). Training infant tread-mill stepping: The role of individual pattern stability.Developmental Psychobiology, 30, 89–102.
Wilder, J., & Granlund, M. (2003). Behaviour style andinteraction between seven children with multiple
Handling and Positioning Advance Development 1301

disabilities and their caregivers. Child Care Health andDevelopment, 29, 559–567.
Zelazo, N. A., Zelazo, P. R., Cohen, K. M., & Zelazo, P. D.(1993). Specificity of practice effects on elementaryneuromotor patterns. Developmental Psychology, 29, 686–691.
Supporting Information
Additional supporting information may be foundin the online version of this article:
Appendix S1. Social Experience Manual.Appendix S2. Handling Positioning Manual.Please note: Wiley-Blackwell is not responsible
for the content or functionality of any supportingmaterials supplied by the authors. Any queries(other than missing material) should be directed tothe corresponding author for the article.
1302 Lobo and Galloway