Embed Size (px)
Citation preview

Quando Passare dagli Inotropi all�Assistenza Meccanica
Sulle Sponde del Ticino, Emoclinic Symposium Stresa, Regina Palace Hotel, 9 Maggio 2014
FABRIZIO OLIVA
Lo Scompenso Cardiaco Grave

Circ Heart Fail 2010;3;314-325
3. Terapia acuta in base al profilo emodinamico

IN-HF Outcome Acute HF: All-cause mortality by SBP (Quartiles)
(n. 1855) (n. 524) (n. 469) (n. 420) (n. 425)
SBP is available for 1838 pts
24.0%
35.9%
20.3% 20.5% 16.9%
SBP (mmHg)
Oliva F et al Eur J Heart Fail 2012

IN-HF Outcome Acute HF: baseline characteristics (n. 1868 pts)
Total (n. 1868)
Worsening HF (n. 1059)
De Novo (n. 809)
p
Age ≥70 years, % 64.7 66.0 62.9 0.17 Age (years), mean±SD 72±12 72±11 72±13 0.13 Females, % 39.7 37.3 42.9 0.01 Ischemic etiology, % 42.3 45.5 38.2 0.002 BMI ≥30 (kg/m2), % 27.5 27.1 28.1 0.71 BMI (kg/m2), mean±SD 27.6±5.5 27.3±5.5 27.9±5.4 0.09 SBP <110 mmHg, % 20.1 23.9 15.1 <.0001 SBP (mmHg), mean±SD 134±33 129±30 141±35 <.0001 HR (bpm), mean±SD 93±26 89±24 99±26 <.0001 EF (%) in the previous 6 months, available, % 33.5 45.1 18.3 <.0001
EF (%) in the previous 6 months, mean±SD 36.1±12.5 34.6±12.2 41.2±12.0 <.0001
Oliva F et al Eur J Heart Fail 2012

IN-HF Outcome Acute HF: physical examination (n. 1868 pts)
Total (n. 1868)
Worsening HF (n. 1059)
De Novo (n. 809)
p
Pulmonary congestion, % 78.3 76.0 81.3 0.006 Peripheral congestion, % 56.2 61.6 49.1 <.0001 Pulmonary and/or peripheral congestion, % 88.4 87.9 89.1 0.42
Peripheral hypoperfusion, % 12.0 12.5 11.5 0.52 Cold, % 11.2 11.4 10.9 0.71 Somnolent, confused, sedated, % 11.5 9.7 13.8 0.006
Oliva F et al Eur J Heart Fail 2012

IN-HF Outcome Acute HF: acute treatment(n. 1868 pts)
Total (n. 1868)
Worsening HF (n. 1059)
De Novo (n. 809)
p
IV Furosemide, % 98.1 97.8 98.4 0.38 IV Furosemide, median [IQR] daily dosage 80 [40-240] 100 [50-250] 80 [40-125] <.0001
Oral Furosemide, % 79.3 80.6 77.8 0.14 Oral Furosemide, median [IQR] daily dosage
75 [50-125] 100 [50-125] 50 [50-100] <.0001
Furosemide (IV or oral), % 99.4 99.6 99.0 0.10 IV diuretics, % 99.0 99.2 98.8 0.41 Other IV diuretics, % 15.7 18.1 12.5 0.0009 IV nitrates, % 30.0 26.2 35.0 <.0001 Inotropes, % Dopamine, % Dobutamine, % Levosimendan, %
19.3 13.8 7.7 3.9
21.3 14.5 9.4 3.6
16.7 13.0 5.4 4.3
0.01 0.36
0.001 0.41
Oliva F et al Eur J Heart Fail 2012
Nei pz con Shock 75%



G Ital Cardiol 2009
PAS 90-100 mmHg
Eziologia ischemica
Levosimendan*
Scompenso de novo Eziologia non ischemica
Dobutamina Enoximone
(Levosimendan*)
Scompenso cronico riacutizzato
e/o in -bloccante
Congestione persistente e/o ipoperfusione, per svezzare da Dobutamina
* No bolo
Il Trattamento con Inotropi: revisione delle evidenze scientifiche e cliniche per i �vecchi� e �nuovi� farmaci
Giuseppe Ambrosioa , Andrea Di Lenardab ,Francesco Fedele c, Domenico Gabriellid, Marco Metrae, Fabrizio Olivaf, Gianpiero Pernad, Michele Sennig , Renata De Mariah

IN-HF Outcome Acute HF: Independent predictors of all-cause in-hospital death
(clinical variables and laboratory measures and treatments)
OR 95%CI p Age ≥75 years 2.98 1.87-4.76 <.0001 Somnolent, confused, sedated 3.98 2.53-6.25 <.0001 eGFR <50 vs ≥50 (ml/min/1.73m2) 2.75 1.68-4.51 <.0001 eGFR missing ≥50 (ml/min/1.73m2) 8.20 2.32-29.00 0.001 Sodium <136 mEq/L 1.85 1.16-2.95 0.009 IV inotropes 7.18 4.62-11.18 <.0001
Oliva F et al Eur J Heart Fail 2012

11
58%
24,5%
17,5% 19.4%
Terapia con Inotropi Registro italiano IN-HF Outcome – Scompenso Acuto
Mortara A, Oliva F, Metra M et al J Heart Lung Transplant, accepted

Inotropes
Yes (n=360 )
Inotropes SBP <110 (n=206 )
Inotropes SBP 111-130
(n=87)
Inotropes SBP >130 (n=62 )
Length of Hospital stay, days 14 [8-23] 15 [8-26] 12 [7-19] 14 [10-21]
Admission in CCU, % 73.9 70.4 79.3 77.4
In Hospital all cause death, % 21.4 22.8 25.3 11.3
1-yr hospitalization for HF, % 23.7 28.9 21.5 12.7*
1-yr all cause mortality rate, % 50.6 56.3 43.7 40.3
1-yr CV mortality rate, % 41.9 45.2 39.1 33.9
1-yr all cause mortality+ 1-yr hospitalization rate for HF, %
61.7 70.4 51.7* 46.8*
Outcome of patients taking inotropes according with blood pressure profile at entry
Mortara A, Oliva F, Metra M et al J Heart Lung Transplant, accepted

1"
2"
3"
4"5"
6"
7"
Dying/MOF"
Crash"&"Burn"
Sliding"fast"
Stable"dependent"
ResCng"symptoms"home"on"oral"therapy"
ExerCon"intolerant"(Housebound)""
ExerCon"limited"(Walking/wounded)"
Advanced"NYHA"III"%1RYears"Survival"100%"
50%"25%"10%"
O%"
Severity"of"EndRStage"Heart"Failure"INTERMACS"Levels"
*Does"not"account"for"arrhythmia"

INTERMACS"Levels"Ho
spita
lRICC
U"
Ambu
latory"

Cardiogenic Shock F. Oliva
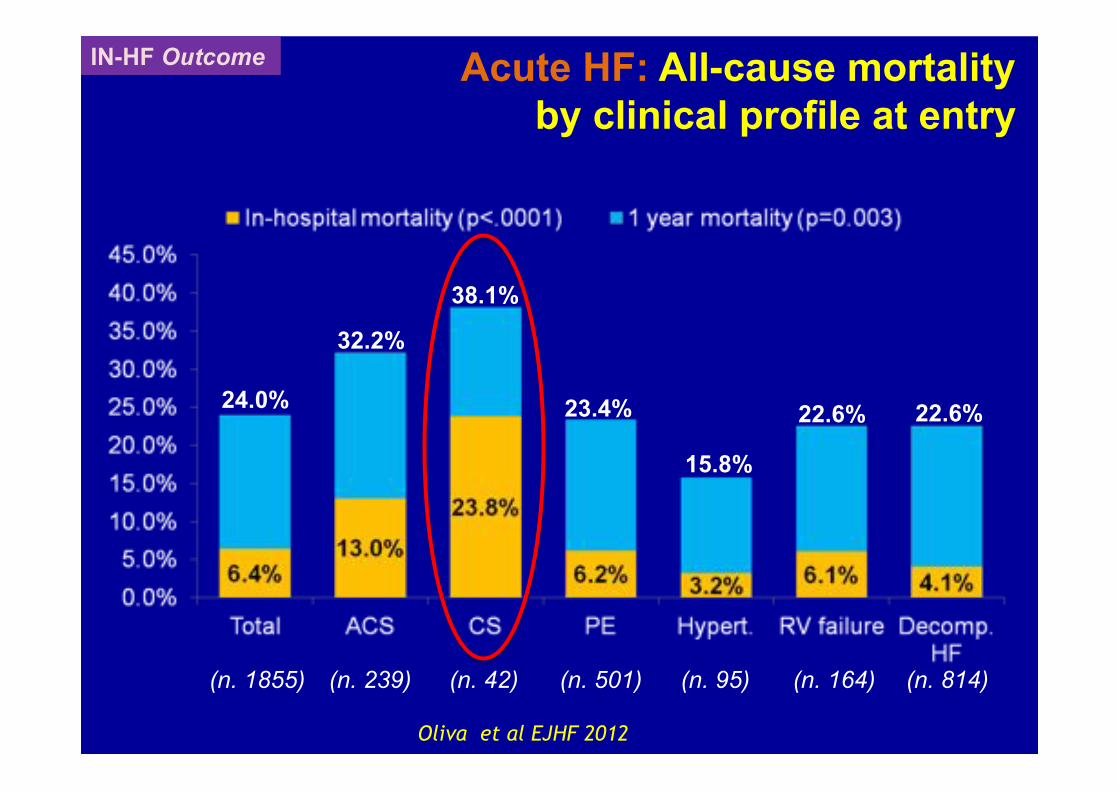
IN-HF Outcome Acute HF: All-cause mortality by clinical profile at entry
24.0%
32.2%
38.1%
23.4%
15.8%
22.6% 22.6%
(n. 1855) (n. 239) (n. 42) (n. 501) (n. 95) (n. 164) (n. 814)
Oliva et al EJHF 2012

Cardiogenic Shock F. Oliva


Shock F.Oliva

Cardiogenic Shock F. Oliva
Cardiogenic Shock (CS) – TREATMENT Fluid, Vasopressors, Inotropes
• Initial stabilization with volume expansion to obtain optimal filling pressures.
• The choice of vasopressor and inotropic therapy is based on individual experience, institutional policy and pathophysiological considerations1,2.
• Recent trial: dopamine was associated with more adverse events3.
1. Antman Circulation 2004 2. Wan Der Weerf Eur Heart J 2008 3. De Backer N Engl J Med 2010

Cardiogenic Shock F. Oliva
Rivalutazione dopo 2 h
Adeguamento terapeutico Monitoraggio avanzato
Adrenalina >0,05γ/Kg/min + altro inotropo >6 PVC< 12 mmHg VAM se indicata
Swan-Ganz - ECO
Contattare: Cardiologo Rianimatore Cardiochirurgo
In presenza di indicatori clinici e strumentali di SBP* che permangono dopo cauto test volemico
*Raccolta parametri clinici e lab se pz
esterno
Protocollo Operativo per lo Shock Cardiogeno

Cardiogenic Shock F. Oliva International Journal of Cardiology 2011, 149: 384

Cardiogenic Shock F. Oliva
• PAS < 100 mmHg O PAM < 70 mmHg nonostante adeguato riempimento volemico (almeno 1000 ml di cristalloidi o 500 ml di colloidi) o in presenza di segni di incrementata pressione venosa centrale (> 12 mmHg) o incremento della pressioni di occlusione capillare polmonare (>14 mmHg).
• Sat. venosa mista < 60%
• Lattati arteriosi > 2
• Oliguria < 0.5 ml/Kg/h
Criteri di Inclusione ( almeno 2 )
Protocollo Shock

Cardiogenic Shock F. Oliva
Dopo le prime due ore, gli obiettivi raggiunti dovranno essere tutti i seguenti:
• diuresi > 0.5 ml/Kg/h; • pressione arteriosa media> 65 mmHg; • indice cardiaco > 2.1 l/min; • lattati <2 mmol/L; • Sat venosa mista >60%; • rapporto Pa2/FiO2> 200; • adeguati scambi emogas-analitici: Sat O2> 90%, FR<
28-30 atti/min, PCO2 > 25 mmHg.
Cardiogenic Shock F. Oliva
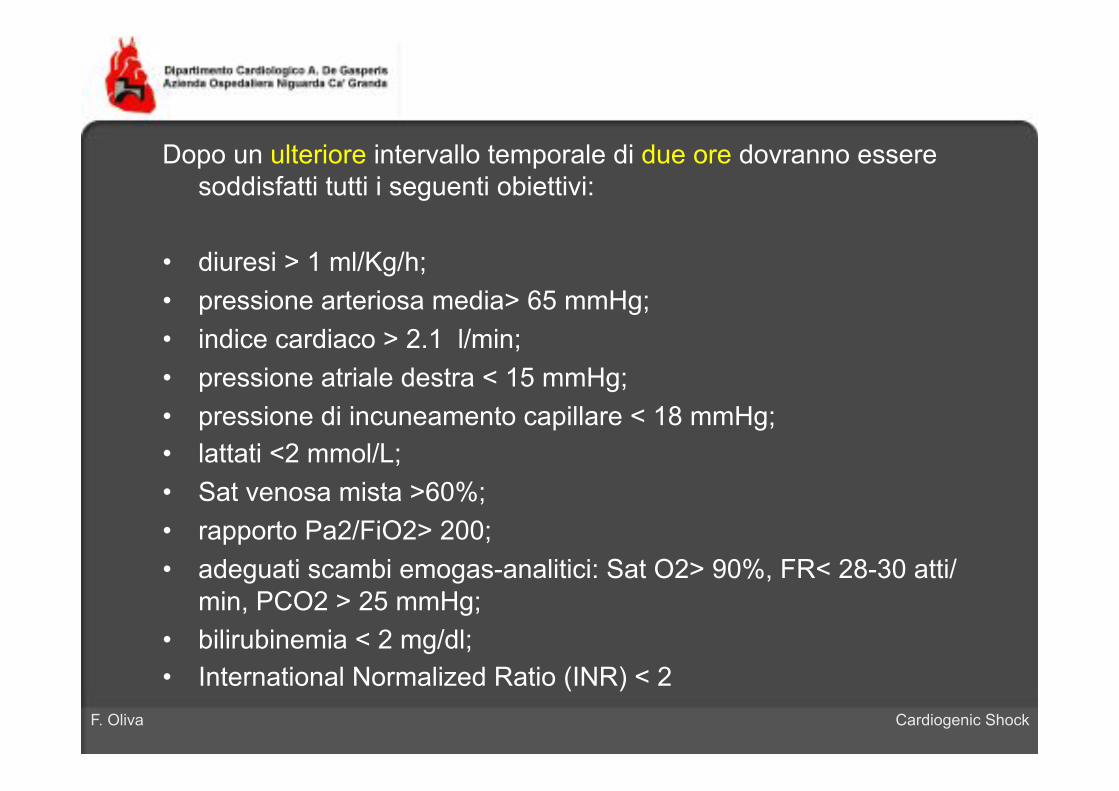
Dopo un ulteriore intervallo temporale di due ore dovranno essere soddisfatti tutti i seguenti obiettivi:
• diuresi > 1 ml/Kg/h; • pressione arteriosa media> 65 mmHg; • indice cardiaco > 2.1 l/min; • pressione atriale destra < 15 mmHg; • pressione di incuneamento capillare < 18 mmHg; • lattati <2 mmol/L; • Sat venosa mista >60%; • rapporto Pa2/FiO2> 200; • adeguati scambi emogas-analitici: Sat O2> 90%, FR< 28-30 atti/
min, PCO2 > 25 mmHg; • bilirubinemia < 2 mg/dl; • International Normalized Ratio (INR) < 2



Cardiogenic Shock F. Oliva
Cardiogenic Shock Mechanical Support: When?

Cardiogenic Shock F. Oliva
Miglioramento (Lattati/SVO2/QU)
Rivalutazione dopo 2 h
IABP Continua terapia
medica
Non miglioramento (Lattati/SVO2/QU)
Rivalutazione dopo 1 h
Protocollo Operativo per lo Shock Cardiogeno

Cardiogenic Shock F. Oliva

Cardiogenic Shock F. Oliva
Cardiogenic Shock (CS) – TREATMENT IABP
• The effects on cardiac output are only modest. • It�s the more widely used mechanical support device for
CS. • It�s reccomended ( class II A AHA/ACC, class II B ESC).
• Few randomized clinical trials. • Registries: conflicting results in mortality risk differences
– Pre-fibrinolytic era 28% favour IABP – Fibrinolytic era 18% favour IABP – PCI era 6% increase mortality for IABP

Cardiogenic Shock F. Oliva
Cardiogenic Shock (CS) – TREATMENT IABP
Thiele Eur Heart J 2010
Percentage of IABP used in selected trials and registries

Cardiogenic Shock F. Oliva
2006: IABP Use in ESC and Italian Registries
0,0
0,5
1,0
1,5
2,0
2,5
IABP
Eur 2006Ita 2006
Tavazzi et al, Eur Heart J 2006 Nieminen et al, Eur Heart J 2006
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
IABP (%Shock)
Eur 2006
Ita 2006

Cardiogenic Shock F. Oliva Thiele N Engl J Med 2012

Cardiogenic Shock F. Oliva
• Scenario: CS complicating AMI, early revascularization planned.
• Slightly lower mortality compared other trials and registries.
• High rate of catecholamine use (90%) may offset the potential benefit of IABP.
• Exclusion criterion of onset shock > 12 h selected for a disease more amenable to revascularization.
• Benefit in severe CS is still unsettled. • No information about long-term outcomes.
BUT…

Cardiogenic Shock F. Oliva
MCS – ANMCO 2013
Classe IIa ( �can be useful�)
Classe IIb ( �may be considered�)

Cardiogenic Shock F. Oliva
Cardiogenic Shock (CS) – TREATMENT Percutaneous LV Assist Devices
• When ?
In many patients with severe depression of LV function, haemodynamic support and LV unloading derived from IABP is insufficient to reverse CS.
The use of percutaneous LV assist devices with active circulatory support might be beneficial in CS patients not responding to standard treatment including IABP support.
SEVERE REFRATORY CARDIOGENIC SHOCK (SRCS)

Cardiogenic Shock F. Oliva
IABP
Rivalutazione dopo 1 h
Non miglioramento (Lattati/SVO2/QU)
Miglioramento (Lattati/SVO2/QU)
ECMO/VAD Continua terapia medica
+ IABP
Idoneità a assistenza al circolo?
SI NO
Cardiogenic Shock F. Oliva
30 ����� 2012 ����� 2012
������: ����� � ��� � �������� � ������? ��� ? ����� : �� ������ ��
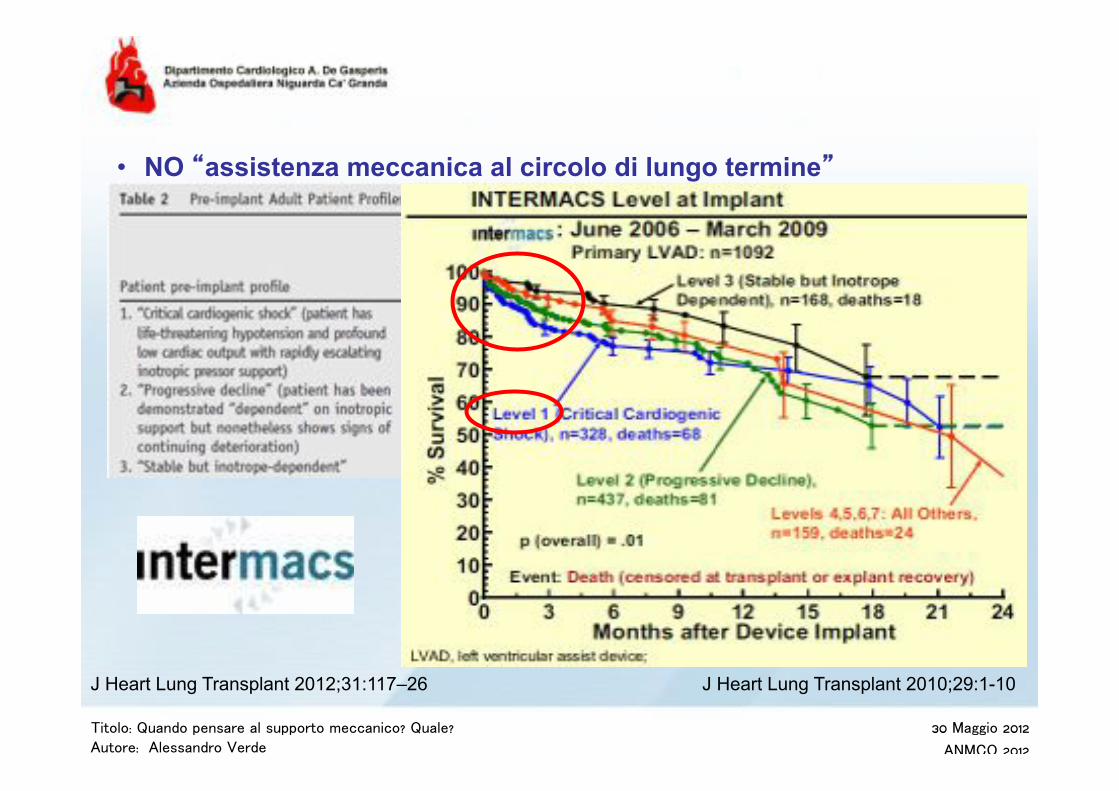
• NO �assistenza meccanica al circolo di lungo termine�
J Heart Lung Transplant 2012;31:117–26 J Heart Lung Transplant 2010;29:1-10

Cardiogenic Shock F. Oliva

Cardiogenic Shock F. Oliva

“Bridge((to(Bridge”((• Temporary(support(
If(recovery((does(not(occur,(it’s(possible(to(switch(toward(a(Long(
Term(Device(
“Bridge(to(Recovery”(• AMI,(Fulminant(myocardiDs,(postEpartum(cardiomyopathy,(postEcardiotomy(shock((
To(allow(the(heart(to(rest,(expecDng(shortEterm(recover(
“Bridge(to(Transplant”("• Long(standing(HF,(Severa(AMI,(Giant(cells(myocardiDs(• Not(expected(to(recovery("To(allow(the(paDent(to(wait(for(
early(heart(transplant(

Cardiogenic Shock F. Oliva
Cardiogenic Shock F. Oliva

Cardiogenic Shock F. Oliva

Cardiogenic Shock F. Oliva

Cardiogenic Shock F. Oliva

Cardiogenic Shock F. Oliva

Cardiogenic Shock F. Oliva

J Thorac Cardiovasc Surg 2010;140:1416-21"
• Implanted"peripherally"in"8"cases"(53.4%)"and"centrally"in"the"remaining"7"(46.6%)."• Mean"venoRarterial"extracorporeal"membrane"oxygenaCon"duraCon"was"11.5"±"8.1"
days"(range,"1–30)"
Persistent low blood pressure (systolic blood pressure < 80 mm Hg for adults) and oliguria (< 0.5 mL/kg/hr) for at least 4 hours despite maximal inotropic support and IABP


Cardiogenic Shock F. Oliva
Cardiogenic Shock Percutaneous LVAD vs IABP
Cheng Eur Heart J 2009

Cardiogenic Shock F. Oliva
Cardiogenic Shock Percutaneous LVAD vs IABP
Cheng Eur Heart J 2009

Cardiogenic Shock F. Oliva
Cardiogenic Shock Percutaneous LVAD vs IABP
Cheng Eur Heart J 2009

Cardiogenic Shock F. Oliva
Management of Acute HF: 2013 Update and Perspectives
• IABP is a good hemodynamic option – Readily available in most centers – No impact on survival
• Need for friendly, versatile and powerfull device in hand – Impella
– Centrimag Survival rates ? – ECMO
When to Use A Balloon Pump or An Assist Device ?
Timely decision process is key No matter the device

Cardiogenic Shock F. Oliva
Cardiogenic Shock (CS) – TREATMENT Percutaneous LVAD
• To implant before deleterious effects of increasing pharmacological therapy and multiorgan failure ( avoid futile implants).
• To maintain MAP > 60 mmHg and mixed venous oxygen saturation > 70% ( adequate end-organ perfusion).
• To continuously assess clinical status and set goals for weaning off MCS.
• �Open� and �honest��communication with the families to discuss end of life issues in pts who are not likely to recover.

Cardiogenic Shock F. Oliva

Cardiogenic Shock F. Oliva
• Multidisciplinary team evaluation • (Cardiologist, Anesthesiologist, Cardiac
Surgeon) • Multi-system work-up
• Heart disease (Echo, Cath, etc.) • Respiratory function • Renal function • Liver function • Coagulation cascade and platelet
function

Cardiogenic Shock F. Oliva
I Level: UTIC IABP
II Level: UTIC IABP Cath Lab + Surg pMCS
III Level: Transplant or VAD Center pMCS VAD TC

Cardiogenic Shock F. Oliva
Cardiogenic Shock INFERENCES
• CS is a dramatic medical condition that requires a quick and multidisciplinary approach.
• All Cardiological Intensive Care Units should be able to implant a IABP when the drugs failed.
• In severe refractory cardiogenic shock ! emergency transfer to an experienced center ( Mobile Cardiac Assistance Unit) – pMCS first line therapy , insitution before MOF – pMCS as a bridge to… whatever seems reasonable – 20-40% of long-term survivors (poor oucomes if MOF) – Bigger devices ? Second line strategy if long term strategy is
required

![diapo Perucci[1] - Cochrane · Forme e complicazioni mal definite di cardiopatie 197 1.35 0.037 Altre forme di cardiopatia ischemica 128 1.35 0.001 Scompenso cardiaco 536 1.30 0.012](https://img.pdfslide.us/doc/110x75/5e651f8129483d01e633317a/diapo-perucci1-cochrane-forme-e-complicazioni-mal-definite-di-cardiopatie-197.jpg)