Embed Size (px)
Citation preview

1
Literature review: Forensic Mental Health Models of Care
Overview
In late 2019 the Commission engaged Professor Kimberlie Dean, University of NSW, to undertake a literature review of forensic mental health systems and models of care. The literature review following has informed the Living Well Mid Term Review and strategic planning process following the review.
Summary of method and scope
The review focussed on models of care for forensic patients within and beyond forensic mental health systems. Models of mental health care for individuals in custody and on release from custody were briefly considered. The author undertook a search of the peer-reviewed and grey online literature on models of care for forensic patients and consulted colleagues working within forensic mental health services in NSW.
Summary of findings
Section 2.1 summarises peer-reviewed evidence in key topics. The review found that no internationally agreed standard exists for forensic mental health services, pathways or models of care. In the absence of randomised controlled trial evidence, the precise model for community forensic mental health services best supported by evidence is unclear. Some approaches and elements are common to several jurisdictions, including in Australia. These include:
• secure inpatient mental health units covering a range of security levels (i.e. high, medium, and low)
• prison mental health services • diversion services, particularly in court-based settings • community forensic mental health services, including with supported community-
based accommodation options.
Emerging evidence supports the notion that successful forensic mental health services or systems require all elements (above) to be present and integrated for optimal functioning. Delays, and sometimes complete blockages to progression, represent the main challenge facing forensic mental health services. This can occur in transition from prison to hospital and between one level of forensic secure inpatient care to another, usually due to lack of available places. Section 2.2 details recommendations from several Australian and international reviews of forensic mental health systems. Section 2.3 lists comments drawn from consultations with key informants. Section 2.4 describes the literature on post-release outcomes of prisoners discharged from forensic mental health care.

2
Section 3.1 canvasses the principles and concepts related to prison models of care, with equivalence of care being an important concept. Public health implications post release, complexity of mental health issues and rates of Aboriginal incarceration and mental health issues are also detailed in section 3.1. Section 3.2 details some models of mental health care provision in prisons that vary along a spectrum from those where external health providers provide occasional out-patient style clinics within prisons to those where the healthcare providers are embedded in the prison environment on a full-time basis providing primary and secondary care with ‘in-reach’ services (analogous to community mental health team models outside hospital) and sometimes hospital-type care (analogous to inpatient psychiatric care). Very limited research exists, beyond providing descriptions of health needs, models of care and audits of provision in some settings, to support the effectiveness of any specific models of mental health service provision to prisoners.

Literature Review: Forensic Mental Health Models of Care
A report for the NSW Mental Health Commission
Prepared by:
Professor Kimberlie Dean1, 2
Chair of Forensic Mental Health and Clinical Academic Forensic Psychiatrist
1 School of Psychiatry, University of New South Wales 2 Justice Health and Forensic Mental Health Network, NSW
May 2020

i
Contents
Approach taken to review report .............................................................................................. 1
1. Background ......................................................................................................................... 2
Terminology ........................................................................................................................... 3
2. Models of care for forensic patients .................................................................................. 4
2.1. Summary of peer-review evidence on key topics ........................................................... 4
2.1.1. Transition delays .................................................................................................. 4
2.1.2. Community forensic mental health services ....................................................... 5
2.2. Key documents identified outside the peer-reviewed literature ................................... 7
2.3. Informal consultation with senior forensic mental health professionals ..................... 10
2.4. Post-release outcomes for forensic patients ................................................................ 11
2.5. Research exploring other outcomes for forensic patients ........................................... 13
3. Prison Mental Health Models of Care (extracted from Fazel et al 2016 review) ................ 15
3.1 Principles and concepts relevant to prison models of care ........................................... 15
3.1.1 The principle of equivalence of care .................................................................. 15
3.1.2 The public health implications of prison health ................................................ 16
3.1.3 Acknowledging the complexity .......................................................................... 17
3.1.4 Indigenous Australian prisoners ........................................................................ 18
3.2 Review of prison mental health models of care literature ....................................... 20
3.2.1 Prison mental healthcare models in Australia ................................................... 20
3.2.2 Mental health screening .................................................................................... 21
3.2.3 The role of primary and secondary care ............................................................ 22
3.2.4 Evaluations of within-prison models ................................................................. 24
References ............................................................................................................................... 25
Appendix 1 ............................................................................................................................... 28
Appendix 2 ............................................................................................................................... 29

1
Approach taken to review report This review is focused on providing a snapshot overview of literature relevant to the
development of forensic mental health models of care. Given the breadth of the field under
review, a systematic review methodology has not been adopted. As requested by the New
South Wales (NSW) Mental Health Commission, the review focuses on models of care for
forensic patients within and beyond forensic mental health systems. Models of mental health
care for individuals in custody and on release from custody are also briefly considered.
Regarding models of care for forensic patients, the author undertook a search of the peer-
reviewed and grey online literature and consulted colleagues working in within forensic
mental health services in NSW. The Prison mental health models of care section is based on a
review undertaken in 2016 for Justice Health and Forensic Mental Health Network
(JH&FMHN) in NSW. The author proposes no key findings or recommendations.

2
1. Background People in contact with the criminal justice system are well known to have high rates of mental
illness, including severe mental illnesses such as schizophrenia (1). A systematic review of
prison studies across 24 countries revealed a pooled prevalence of psychosis of 3.6% (95%
Confidence Interval (CI) 3.1–4.2) in male prisoners and 3.9% (95% CI 2.7–5.0) in female
prisoners). In NSW, the prevalence of mental illness amongst prisoners has also been
established to be much higher than in the general population (2). This burden of mental illness
has led to the development of diversionary programs and services, particularly at courts but
also at police stations and in prison. Such programs aim to identify those offenders
experiencing mental disorder who need treatment and facilitate their access to mental health
services.
A sub-group of offenders who have typically committed serious violent offences and have
severe mental illnesses such as schizophrenia may be found Not Guilty by reason of Mental
Illness (NGMI) at court. Along with those found mentally unfit to plead or stand trial, NGMI
forensic patients form the sub-group of mentally ill offenders typically managed by forensic
mental health services (including in NSW). In many jurisdictions, including in Australia and in
the United Kingdom (UK), another group of prisoners (on remand or sentenced) who become
mentally ill and require treatment (termed ‘correctional patients’ in NSW) can also be
transferred out of prison and treated by forensic mental health services in secure settings.
The extent to which this is possible is often limited because of the unavailability of secure
hospital beds in the system. While NSW legislation supports such treatment for correctional
patients, in practice it is very often not available.
The prevalence of mental health problems in the wider population of individuals in prison in
NSW has recently been updated in the 2015 Network Patient Health Survey (3) and 2015
Young People in Custody Health Survey (3). The author notes that international evidence has
been almost entirely in the form of prevalence studies, providing a cross-sectional snapshot
of mental health need. Much less is known about the longitudinal course of mental illness
among prisoners, research that would better inform development of interventions and
service delivery models.
No internationally agreed standard exists for forensic mental health services, pathways or
models of care. There are, however, approaches common to several jurisdictions, including in

3
Australia. While the specific nature of enabling legislation and associated policies and
procedures may vary, forensic mental health services are typically comprised of secure
inpatient facilities (ideally with varying levels of security to safely facilitate rehabilitation),
complemented by prison-based mental health services, court-based diversion and/or liaison
services, and community-based services (that may or may not include the case management
of forensic patients).
Terminology
It is important to clarify the meaning of ‘forensic patient’ as used in this review since use of
the term varies internationally. In many jurisdictions, including the UK where medico-legal
concepts relevant to the NSW context originate, ‘forensic patient’ is a term commonly used
to refer to any mentally ill offender. That is any person who has engaged in offending
behaviour or is at risk of doing so and has significant mental health problems. Such individuals
may or may not be in contact with the criminal justice system and are not necessarily defined
by any specific legislation. They may be in contact with forensic mental health services,
including inpatient secure care. As a result of the local legal and health service arrangements
in NSW, the term is often used more specifically to refer to those deemed to be Forensic
Patients under the Mental Health (Forensic Provisions) Act 1990, which includes the following
three groups of people with mental or cognitive impairment (4):
• those who have been accused of committing a crime and have been refused bail after
having been found unfit to be tried, or
• those who have been found unfit to be tried, had a special hearing, found to have
committed one or more offence(s) and been ordered to be detained for not longer
than a ‘limiting term’ nominated by the court, or
• those who have been found NGMI of one or more offence(s) after a trial or special
hearing, and either detained or conditionally released (NGMI forensic patients)
Readers should note that most forensic patients in NSW belong to the third category NGMI,
although a substantial proportion of NGMI forensic patients have been found unfit at some
point during their contact with the criminal justice system. This literature review will refer to
research involving forensic patients in other jurisdictions where the term may be used more
generally but where the research is still relevant to forensic patients in NSW.

4
2. Models of care for forensic patients
2.1. Summary of peer-review evidence on key topics
As noted earlier, there is no internationally agreed and/or empirically supported single model
of care for forensic patients or for forensic mental health services. However, models of care
have been developed in a range of jurisdictions which have several common elements,
including:
• secure inpatient mental health units covering a range of security levels (i.e. high,
medium, and low)
• prison mental health services (see section 3 of this review)
• diversion services, particularly in court-based settings
• community forensic mental health services, including with supported community-
based accommodation options.
Jurisdictions differ in the precise nature and combination of these elements. But evidence is
emerging to support the notion that successful forensic mental health services or systems
require all elements and that optimal functioning requires the elements to be integrated.
Delays, and sometimes complete blockages to progression, represent the main challenge
facing forensic mental health services.
2.1.1. Transition delays
Delays for forensic patients transitioning through different elements of the forensic mental
health system have been documented in several jurisdictions. Legislative, administrative and
resource-level factors have been cited as the main barriers to efficient forensic patient
progress. Transfers from prison to hospital have frequently been described as unacceptably
delayed. In one study of two London prisons, the average transfer wait was reported to have
been between 93 and 102 days (5). More recently, the UK Government set a target for prison-
to-hospital transfer of 14 days. One study subsequently examining transfers between 2011
and 2014 still reported a mean wait time of 76 days (6).
In many jurisdictions, it is not legally possible for forensic patients found NGMI (or equivalent)
to be detained in custody awaiting bed availability in hospital. In those jurisdictions where
such waiting is possible, delays in transfer of up to several years have been reported. Findings

5
from the NSW Forensic Patient Database on delays in transfer from prison to hospital for
NGMI forensic patients will be published separately and potentially add to this evidence.
Other transition periods, such as from one level of forensic secure inpatient care to another,
have also been cited as subject to considerable delays. Again, administrative, legal and, in
some jurisdictions, financial factors have been cited as potential causes of such delays. Up to
one-third of forensic patients in secure services have been described as ‘long-stay’ patients
(7) and while a number of individual patient characteristics are known to predict longer
periods of forensic inpatient care (8), limitations in models of care and other service-
dependent factors are also likely to influence admission duration.
One such service-dependent factor likely to influence length of stay and the occurrence of
transition delays is the relative provision of elements within forensic mental health services.
A lack of beds in one or more of the high, medium or low secure settings relative to need can
result in bottle-necks and delays proximal to the level with a relative lack of provision. In NSW,
patients requiring medium or low security were found to be waiting in high security in large
numbers with the relative lack of provision at medium and low security levels being cited as
the key cause (9, 10).
Another key consideration regarding transition delays in forensic mental health services
relates to the difficulty in ensuring adequately catering for special groups. Subgroups within
the wider forensic patient population such as women, older adults, and those with significant
cognitive impairments and/or personality disorder are unlikely to have access to the full range
of forensic mental health service elements. They may experience greater than average
transition delays as a result.
2.1.2. Community forensic mental health services
In addition to the need for supported accommodation for forensic patients transitioning from
secure hospital care to the community, the benefits of community-based forensic mental
health services have been under scrutiny in the peer-reviewed literature. One of the key
questions to be answered is whether stand-alone parallel community forensic mental health
teams managing a case load of forensic and/or other high-risk patients has advantages over
liaison-only models or over management of such patients by general community mental
health services. While randomised controlled trial (RCT) evidence is lacking, some studies

6
have demonstrated apparent advantages for parallel community forensic mental health
teams, including those using an assertive-outreach model of care. In a key study conducted
in the UK over a decade ago, individuals discharged from medium security to forensic services
did no better than those discharged to general adult services with regard to re-offending or
re-hospitalisation outcomes but the mortality rate was lower amongst those referred to
community forensic services (11). While the study’s authors did not find evidence that
forensic services were referred patients who presented a greater risk than those referred to
general services, the lack of randomisation raises concerns about this possibility given this
sort of difference has been shown in other community samples (12). In another UK study
comparing outcomes for forensic patients discharged to forensic compared to general adult
community services (from one particular medium secure unit), the median time to
reconviction was actually significantly lower for those discharged to forensic teams, despite
similar clinical and forensic characteristics at discharge between the two groups (13). Just as
with the latter study, concerns were noted about the true similarity of the two groups in the
absence of randomisation.
In another UK study comparing the characteristics and needs of forensic and general adult
community patients, forensic community services were defined as either parallel or
integrated (the latter being integrated with general adult community teams) (14). The authors
detailed the arguments for and against these two models of community forensic mental
health service as including:
• In favour of parallel community forensic mental health teams: enables continuity of
care from inpatient secure to community care, concentration of staff with forensic
skills and experience, potential for assertive outreach and reduced caseloads
• In favour of integrated community forensic mental health services (forensic staff
embedded within geographically-defined general community mental health teams): if
readmission is required the opportunity for least restrictive care may be greater
(automatic readmission to secure care may be avoided), potential for increasing the
forensic-relevant skills and experience of general community team staff.
In the absence of RCT evidence, the precise model for community forensic mental health
services best supported by evidence is unclear. Where such services undertake case
management (rather than assessment and liaison only), an integrated approach (that is,

7
integrated with general community mental health services) may have merit over a completely
parallel model.
2.2. Key documents identified outside the peer-reviewed literature
Several reports were identified outside the peer-reviewed literature that comment on
forensic mental health models of care, often in the context of a review of the model operating
in a jurisdiction. A summary of recommendations arising from these key reports/reviews
appears below:
• Joint Commissioning Panel for Mental Health, NHS England Guide for the Commissioners
of Forensic Mental Health (FMH) Services, January 2013, contained 10 key messages:
1. FMH services are provided for individuals with a mental disorder who pose, or
have posed, risks to others and where that risk usually related to their mental
disorder
2. Patients must be at the centre of care; a dual emphasis on promoting and enabling
individual recovery and independence, while ensuring protection of the public (not
mutually exclusive)
3. FMH services are ‘low volume and high cost’ and the following should be ensured:
that patients make progress through the care pathway according to their risk and
mental health stability, that services are flexible enough to meet individual
complex needs in any setting, that administrative barriers are kept to a minimum
to avoid blocking of care pathways, and that mental health care in prisons is
equivalent to community care
4. A safe environment to enable therapeutic work to be undertaken should be
provided without over-reliance on physical security
5. Integrated pathways of care should be commissioned to avoid administrative
delays at service interfaces
6. Co-ordination of commissioning required
7. The ‘equivalence of care’ principle should guide prison mental health services
8. All services should be part of the Quality Network for Forensic Mental Health
Services (QNFMHS). The Network has been successful in raising standards in
medium security (and should be extended to prison, low secure and community
services)

8
9. Recommendations of the 2009 Bradley Report should be considered
10. The highest risk time for individuals is during the transition between different parts
of the pathway and thus transitions should be managed safely and securely.
The Guide describes forensic mental health services in the UK, the principles
underlying aims to improve such services, and the history of their development. The
Guide is intended to assist those commissioning forensic mental health services in
regions across the UK.
• Royal Australian and New Zealand College of Psychiatrists (RANZCP) 2016 Principles for
the treatment of persons found not criminally responsible or not fit for trial due to mental
illness or cognitive disability outlined six principles:
1. Forensic patients must receive equity of access to health care and legal
representation
2. Forensic patients must be managed by mental health services not correctional
services
3. Decisions regarding detention, release or transfer must be made by courts or
independent statutory bodies
4. Treatment must be in the least restrictive environment appropriate, consistent
with individual circumstances and the safety of the community
5. The level of security required for any individual should be based on a valid
professional risk assessment
6. Rehabilitation and effective treatment is required to decrease recidivism.
• ‘National Statement of Principles for Forensic Mental Health’ Australian Health Ministers
Advisory Council, under the COAG Health Council 2006 contained 13 principles articulated
under the following headings:
o equivalence to the non-offender, safe and secure treatment, responsibilities of the
Health, Justice and Correctional Systems, Access and Early Intervention,
Comprehensive forensic mental health systems, integration and linkages, ethical
standards, staff knowledge, attitudes and skills, individualized care, quality and
effectiveness, transparency and accountability, judicial determination of
detention/release, legal reform.

9
• Treatment Advocacy Center, Virginia, USA Emptying the ‘New Asylums: A Beds-Capacity
Model to Reduce Mental Illness Behind Bars, January 2017
• Review of the South Australian Forensic Mental Health Service 2015
The terms of reference encompassed consideration of the ‘management, culture and
standards of care within the service’.
Priority recommendations:
o Urgent transfer of small number of forensic patients detained in prison for
prolonged periods
o Commissioning of additional beds in the rehabilitation unit
o Review of staffing model in high secure unit to be reviewed to support a clinical
approach to risk management and least restrictive practice
Other recommendations were also made regarding: program components,
strategic/relationship matters, and legislation
Stakeholder feedback highlighted issues including the view that the detention of
forensic patients in custody is ‘inappropriate’ and the problems of access to mental
health care arising from inadequate patient flow (ultimately leading to forensic
patients being detained in custody)
The review noted that the ‘time for the forensic patients currently awaiting transfer
to the (HSIS) High Secure Inpatient Service extends from 13 days to over 5 years’
• Report on the review of Forensic Mental Health and Disability Services within the Northern
Territory, January 2019
21 recommendations made to support the development of an adequately resourced and
contemporary forensic mental health system
• ACT Forensic Mental Health Services Model of Care (June 2019 draft review and proposed
changes)
Principles of Care:
o High quality, person-centred, recovery-oriented care
o Timely and responsive service access and provision
o Provision of a comprehensive service in which care pathways are integrated,
multidisciplinary and evidence-based

10
o Service provision is ethical, transparent and accountable
2.3. Informal consultation with senior forensic mental health professionals
For this review, the author sought the views of several key senior forensic mental health
professionals in NSW. The following themes reflect their responses to questions about models
of care for forensic patients and what changes might be beneficial in NSW.
• NSW has a shortage of forensic mental health beds, particularly when the national context
of bed numbers relative to population size is considered
• Medium and low secure beds, and supported housing are most needed
• A community forensic team that holds a case-load would be of benefit
• Secure/supported beds for long-stay patients are needed
• A more fluid model between custody and secure forensic care would enable patients to
move between secure hospital care and custody as needed
• The Housing and Accommodation Support Initiative (HASI) HASI-plus model of supported
housing should be supported and expanded, preserving the capacity for 24-hour support,
supervision of medication, provision of group activities. Good support from local
community mental health services is also required to ensure the success of this model.
The evaluation of the HASI-plus program in NSW is highly anticipated.
• ‘Step-down cottages’ connected to medium or low security facilities can be effective in
safely testing individuals prior to formal conditional release into the community
• The role of National Disability Insurance Scheme (NDIS) should be considered in terms of
facilitating community placement. It may need amending in light of the needs and
contexts for forensic patients
• Access to appropriately supported nursing homes in the community is needed for the
successful placement of older forensic patients
• A more flexible rather than linear patient-flow model (based primarily on patients’
needs/risk) should be adopted
• NSW needs greater integration between elements of the forensic mental health system
(e.g. between different medium secure units, between forensic and general mental health
services)
• Models of care within elements of the forensic mental health system could benefit from
greater consistency
11
• Civil patients who are at risk of becoming forensic patients also need to be considered,
patients with major mental illness leaving custody and high risk civil patients
• Earlier transfer of prisoners with severe mental illness (including likely future forensic
patients) is important for ensuring early assessment (temporally close to the index
offence) and early establishment of therapeutic relationships (avoiding long waiting
periods in custodial settings)
• Interpretation of insanity criteria (key to defining which individuals become forensic
patients) should be reviewed and might benefit from a systematic approach (for example,
through instruction of court-appointed or independent psychiatry experts, or through use
of early transfer to hospital for assessment prior to forensic status determination)
• Support for court diversion is needed, including increasing the capacity of general mental
health services to manage diverted patients
• The Mental Health Review Tribunal (MHRT) needs to be appropriately resourced in order
that the timing of hearings and decisions does not unnecessarily delay patient progress
through the system
• Resourcing gaps in general mental health services (inpatient and community) also impact
on the forensic mental health service (related to opportunities to preventing individuals
becoming forensic patients, delays in discharging forensic patients from secure settings,
and the likelihood of discharged forensic patients returning to hospital or custody)
• A centralised assessment and treatment planning process is needed for forensic patients,
with treatment plans/goals agreed early and commenced in settings with the appropriate
level of security (based on individualised assessments of risk and security needs).
2.4. Post-release outcomes for forensic patients
In the context of evaluating models of care for forensic patients, it is important to consider
the evidence supporting outcomes for individuals following care and treatment in forensic
mental health services. Whilst the many differences between jurisdictions internationally and
nationally make generalisations difficult, several studies attempt to examine rates of
reoffending in forensic patients following release into the community from secure care.
Reoffending is not the only factor to consider when evaluating the outcomes of forensic
mental health care, but it is an important one.

12
In 2016, Fazel et al (15) published an important systematic review and meta-analysis of
patient outcomes following discharge from secure psychiatric hospitals. Searching across 11
computer-based literature indexes up until March 2013, they identified 35 studies from 10
countries. Importantly, they considered reoffending as an outcome of release, but they also
examined mortality rates, suicide rates, and readmission rates. For inclusion in the review,
studies had to involve follow-up of patients discharged from a secure hospital (high, medium
or low security) and had to provide sufficient quantitative information to be included in the
meta-analysis. The authors also considered possible comparison groups (community
psychiatric patients, prisoners and forensic patients sentenced to community-based
interventions). The total sample included 12,056 patients (75% male) with a mean age of 34.5
years and an average length of admission of three years. Most studies were from England and
Wales (18 investigations). The follow-up period after discharge ranged from 1.5 to 13.6 years
for the reoffending analysis.
Thirty papers considered reoffending following discharge and reported criminal outcomes
with crude reoffending rates ranging from 0 to 24,244 per 100,000 person-years. The pooled
estimate across studies was 4,484 repeat offences per 100,000 person-years (95% CI 3,679-
5,287). The authors identified substantial heterogeneity across studies, partly explained by
the higher rates reported by earlier studies. But they did not find evidence that study findings
differed due to differences in the age of patients, geographical region, type of index offence,
duration of admission, Mental Health Act status or history of in-patient treatment. Ten studies
reported reoffending rates for comparison populations (released prisoners, offenders with
personality disorder, mentally disordered offenders and offenders with mental illness). Rates
for these comparison populations ranged from 4,535 to 36,964 repeat offences per 100,000
person years, and all were higher than the reoffending rate reported for the forensic patient
sample in each of the studies. Fifteen studies reported findings for violent reoffending
specifically and the pooled estimate was found to be 3,902 violent re-offences per 100,000
person years (95% CI 2,671-5,187) again with substantial heterogeneity identified. This rate
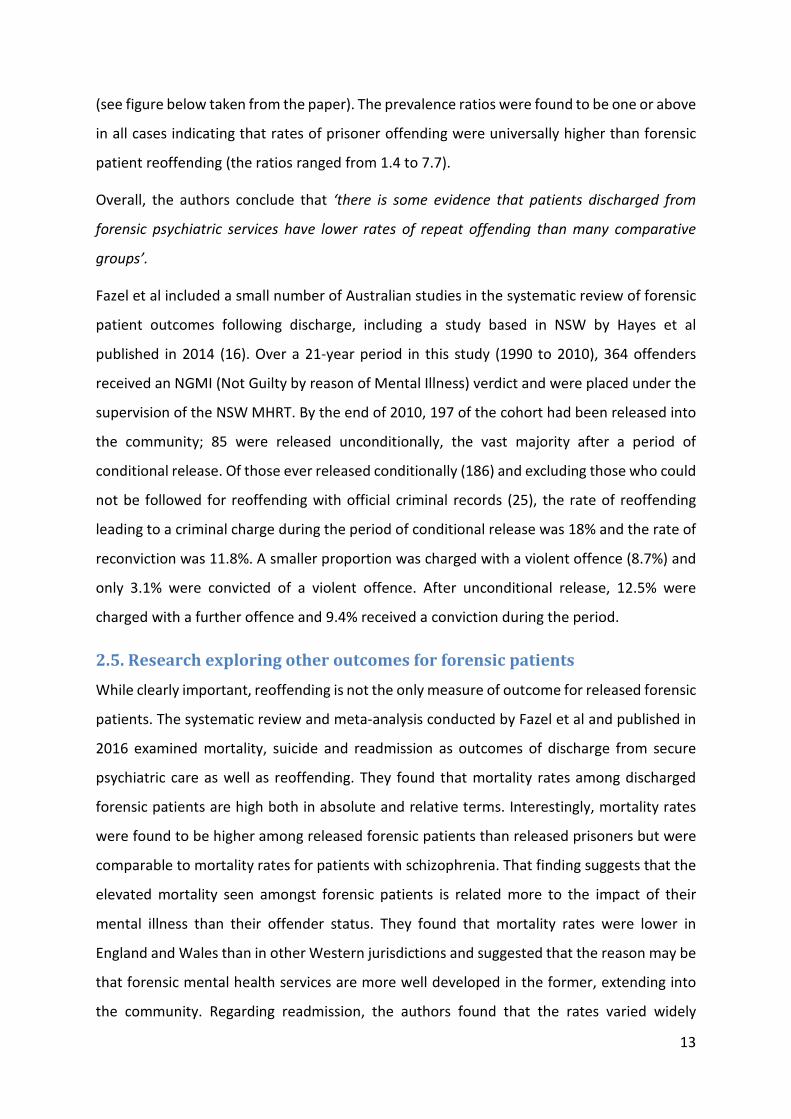
of violent reoffending compares favourably to released prisoners (7,200 US; 25,494 UK). Fazel
et al also undertook comparisons between reoffending rates for discharged forensic patients
reported in the studies and the reoffending rates obtained for prisoners using data from the
same country, similar calendar period, same gender, and similar age bands where possible
13
(see figure below taken from the paper). The prevalence ratios were found to be one or above
in all cases indicating that rates of prisoner offending were universally higher than forensic
patient reoffending (the ratios ranged from 1.4 to 7.7).
Overall, the authors conclude that ‘there is some evidence that patients discharged from
forensic psychiatric services have lower rates of repeat offending than many comparative
groups’.
Fazel et al included a small number of Australian studies in the systematic review of forensic
patient outcomes following discharge, including a study based in NSW by Hayes et al
published in 2014 (16). Over a 21-year period in this study (1990 to 2010), 364 offenders
received an NGMI (Not Guilty by reason of Mental Illness) verdict and were placed under the
supervision of the NSW MHRT. By the end of 2010, 197 of the cohort had been released into
the community; 85 were released unconditionally, the vast majority after a period of
conditional release. Of those ever released conditionally (186) and excluding those who could
not be followed for reoffending with official criminal records (25), the rate of reoffending
leading to a criminal charge during the period of conditional release was 18% and the rate of
reconviction was 11.8%. A smaller proportion was charged with a violent offence (8.7%) and
only 3.1% were convicted of a violent offence. After unconditional release, 12.5% were
charged with a further offence and 9.4% received a conviction during the period.
2.5. Research exploring other outcomes for forensic patients
While clearly important, reoffending is not the only measure of outcome for released forensic
patients. The systematic review and meta-analysis conducted by Fazel et al and published in
2016 examined mortality, suicide and readmission as outcomes of discharge from secure
psychiatric care as well as reoffending. They found that mortality rates among discharged
forensic patients are high both in absolute and relative terms. Interestingly, mortality rates
were found to be higher among released forensic patients than released prisoners but were
comparable to mortality rates for patients with schizophrenia. That finding suggests that the
elevated mortality seen amongst forensic patients is related more to the impact of their
mental illness than their offender status. They found that mortality rates were lower in
England and Wales than in other Western jurisdictions and suggested that the reason may be
that forensic mental health services are more well developed in the former, extending into
the community. Regarding readmission, the authors found that the rates varied widely

14
between jurisdictions and comparative data for psychiatric patients is largely lacking. They
called for future research to examine readmission but also to examine outcomes for forensic
patients more broadly, including markers of functioning and quality of life.

15
3. Prison Mental Health Models of Care (extracted from Fazel et al 2016 review)
3.1 Principles and concepts relevant to prison models of care
3.1.1 The principle of equivalence of care
The principle of ‘equivalence of care’ refers to the notion that those individuals in contact
with the criminal justice system, particularly prisoners, should receive the same level and
quality of health care as they would have access to in the community. This principle has guided
the evolution of health care provision, including mental health care provision, to prisoners in
various jurisdictions and has, in recent times, been formally adopted by some.
The ‘Basic principles for the treatment of prisoners’ resolution was adopted by the United
Nations General Assembly in 1990 with one of the 11 principles describing a right to
equivalence of care – ‘Prisoners shall have access to the health services available in the
country without discrimination on the grounds of their legal situation’ (17).
In line with protection of other related human rights for prisoners, the principle of
equivalence in this context supports the notion that discrimination on the grounds of legal
situation cannot be used to justify denial of rights. In the UK, the principle of equivalence of
care has been formally enshrined in documents governing healthcare arrangements for
prisoners for well over a decade and predated the transition from prison service to National
Health Service responsibility for prison healthcare in 2003 (18, 19). In this context equivalence
was considered relevant to ‘policy, standards and delivery’. Despite formal adoption of the
equivalence of care principle in some jurisdictions, minimum standards for healthcare
provision to prisoners to ensure equivalence are rarely formally set or monitored. However,
in 2015, the UK Quality Network for Prison Mental Health Services published standards for
mental health services (20), the standards having been explicitly developed on a foundation
of care equivalence.
In Australia, one of the barriers to formal national adoption of the principle of care
equivalence is the fact that prison services and healthcare provision within prisons is the
responsibility of states and territories. There is currently no national organisation tasked with
setting standards and monitoring the quality of healthcare provision to prisoners and others
in contact with the criminal justice system. Arrangements for healthcare provision vary
between jurisdictions. While the Australian Institute of Health and Welfare coordinates a

16
national census of prisoner health which provides an internationally unique picture of the
state of health of Australian prisoners, there is no national approach to setting and monitoring
adherence to standards of healthcare provision. In addition, prisoners in Australian states and
territories are not entitled to access the federally administered Medicare insurance system
which inevitably limits the extent to which access to healthcare is equivalent to that available
in the community.
Challenges to the principle of care equivalence have focused on the barriers to full
implementation of the principle and on the fact that the striking level and complexity of
health need presented by those coming in contact with the criminal justice system actually
necessitates more than an ‘equivalent’ level of healthcare provision (21). Barriers to provision
of equivalent care include the limitations inherent in delivering healthcare in an environment
that by its nature and culture is not designed to facilitate healthcare delivery. This important
barrier to achieving equivalence arises both from the nature of the custodial environment,
including the policies/practices which impact on healthcare provision, as well as the higher-
level design of criminal justice systems within jurisdictions. The latter is reflected in the fact
that the availability of appropriate local health services is not normally a key consideration in
determining the location of individual prisons. Such geographical isolation of prisons is
prominent in jurisdictions such as NSW where relevant distances are also vast. The challenge
to care equivalence which arises from the level and complexity of mental health need
presented by prisoners is further nuanced by the fact that prisoners do not simply present
with more of the same type and mix of health needs – mental health needs are
disproportionately apparent for example. Importing community-based models wholesale into
the prison setting with the intent of achieving equivalence is thus flawed not only in the extent
to which the models may not be appropriate but on the basis that prisoner needs do not
simply reflect those of a community sample. A focus on the extent to which prison healthcare
provision is equivalent in terms simply of such process issues rather than being outcomes or
at least needs-based has been raised as a concern in the discourse around the principle of
care equivalence (22).
3.1.2 The public health implications of prison health
Prisoners come from the community and will, in nearly all cases, return to the community –
an obvious fact which is often lost in the discourse surrounding prisoner health. Given the

17
high level of morbidity and the poor history of community healthcare access for most
prisoners, a period in prison can be seen as an opportunity to identify health needs and
provide appropriate treatment that may well have positive public health impacts (23). The
impact on the individual, their families and the wider community is likely to be significant.
This point is most easily made when considering infectious diseases, but the principle can also
apply to chronic diseases including mental ill health.
The extent to which identification of mental health need and appropriate treatment provision
for those in contact with the justice system improves the health of the whole community is
essentially unknown but the potential is clear. One of the implications of such a potential is
that improving the mental health of offenders may well also have economic benefits – a
notion which is again untested. The public health implications of improving offender health
rely on continuity of care between the justice system and the community, particularly as
mental illness may be chronic. There would seem to be limited benefit in adequately
addressing mental ill health among prisoners only to release prisoners without ongoing
treatment and support in the community with the inevitable risk of deterioration. Thus
whatever models of mental health care provision are adopted in prison, these need to be
capable of integrating with community systems, including community-based primary care
(24), to ensure satisfactory aftercare following release.
3.1.3 Acknowledging the complexity
As noted earlier in relation to challenges to the equivalent care principle, it is generally
recognised that when individuals with a mental illness encounter the criminal justice system
the health needs they present are very often complex. This may be both in terms of the
increased risk of co-occurring health disorders, both mental and physical, and the typical
pattern of poor prior health service utilisation. The co-occurring disorders may include dual
diagnoses (i.e. additional substance use disorders), additional mental health and personality
disorders, cognitive disability and a range of physical health disorders including infectious
diseases and/or chronic conditions such as diabetes.
While there remains a paucity of research examining the nature and extent of health
complexity for those people with mental illness in contact with the criminal justice system, it
is well recognised that a high proportion of mentally disordered offenders have at least a
coexisting substance use disorder (25). A cross sectional study in metropolitan Victoria

18
identified a third of police detainees, for example, had a dual-diagnosis (26). Significant
mental health co-morbidity was identified in the 2001 NSW Inmate Mental Health survey with
945 diagnoses (of psychotic symptoms, affective disorder or anxiety disorder) recorded for
624 individuals (27). Regarding evidence of poor health service use prior to incarceration, the
2012 Australian prisoner health survey report notes that 39% of prison entrants needed to
see a health professional in the community during the prior 12 months and did not (28).
Those people in contact with the criminal justice system are also well known to have high
rates of cognitive disability (29-32). A recent prison cohort and data-linkage study based in
NSW (33) identified 1463 individuals with a cognitive disability who had contact with the
criminal justice system. Of those, 66% were found to have complex needs which included
having an additional substance use disorder and/or additional mental health diagnoses.
Complexity of healthcare needs may well be the norm for those in contact with the criminal
justice system. This notion has clear implications for the development of effective and
appropriate interventions and service delivery models and challenges the principle of care
‘equivalence’. The development of forensic mental health services in most Western settings
particularly secure inpatient forensic units, reflects an acknowledgement that ‘more than
equivalent’ levels of mental health care may be needed to effectively assess and manage
mentally disordered offenders. Such services are of course focused most often on individuals
with severe mental illnesses who have committed serious violence offences and present
significant ongoing risks.
3.1.4 Indigenous Australian prisoners
The incarceration rate for Indigenous Australians is significantly higher than non-Indigenous
Australians across all Australian jurisdictions. As at 30 June 2012, there were 7,979 prisoners
in Australia who identified as Indigenous, representing 27% of the total prisoner population
(34). The incarceration rate for Indigenous Australians was 1,914 per 100,000 compared to
129 per 100,000 for non-Indigenous Australians, an extraordinary relative risk of almost 15.
Western Australia recorded the highest rate of incarceration for Indigenous Australians
compared to non-Indigenous Australians (20 times higher) and Tasmania reported the lowest
rate of incarceration compared to non-Indigenous Australians (four times higher). Since 2002,
an increase in the rate of incarceration has been observed for both Indigenous and non-
Indigenous Australians (1,262 per 100,000 and 123 per 100,000 respectively). These figures

19
represent some of the worst relative incarceration rates for any minority population in the
Western world.
Prison health surveys indicated that Indigenous prisoners may be less likely to report a prior
history or prior treatment for mental illness than other prisoners (28). While these findings
appear to suggest Indigenous prisoners are less likely to suffer mental health problems
compared to non-Indigenous prisoners, caution should be exercised when interpreting these
data, particularly given that community-based studies indicate an elevated risk of mental
disorder for Indigenous Australians. The prevalence of mental disorders among Indigenous
Australians has been estimated to represent 15.5% of the total burden of disease in the
community. Furthermore, compared to their non-Indigenous counterparts, Indigenous
Australians are reported to be twice as likely to be hospitalised for a mental disorder (35). The
relatively low rates of self-reported mental health problems among Indigenous prisoners
entering prison may reflect a reluctance to report previous mental health problems and/or a
history of poor engagement with health services for mental health problems whilst in the
community. Indigenous prisoners, along with others at socio-economic disadvantage are
more often incarcerated for relatively short periods for minor offending. One consequence of
this is a more limited opportunity to have their mental health needs identified and addressed.
As noted earlier, a period of incarceration can provide an important opportunity for
individuals to access and receive healthcare services, including treatment. This is of particular
importance for those with a prior history of poor health care contact in the community and
evidence suggests Indigenous prisoners may benefit to a significant extent when offered
treatment for mental health problems (28).
Some dedicated programs have been established to provide culturally specific or sensitive
general health and mental health care to Indigenous prisoners to improve access and service
use. These include the training and employment of Aboriginal health workers in prison health
clinics and in-reach consultation and treatment provided by visiting Aboriginal health services
usually based in the community. However, the available evidence suggests that these
programs are not always sufficiently embedded within prison healthcare service provision
across all Australian jurisdictions. And where they are available, they appear to be under-
utilised by Indigenous prisoners (36). The patterns of mental health need and service use for
Indigenous Australians in the community and in prison, and the underlying factors giving rise

20
to such patterns, are highly complex. Current evidence is insufficient to inform service
development and given the extraordinary incarceration rates and known extremes of
disadvantage faced by Indigenous Australians, gathering vital evidence and testing
interventions and service changes is an important priority.
3.2 Review of prison mental health models of care literature
Existing models of mental health care provision in prisons vary along a spectrum from those
where external health providers provide occasional out-patient style clinics within prisons to
those where the healthcare providers are embedded in the prison environment on a full-time
basis providing primary and secondary care with ‘in-reach’ services (analogous to community
mental health team models outside hospital) and sometimes hospital-type care (analogous
to inpatient psychiatric care). Healthcare providers may be employed by the prison service,
employed by the publicly funded health service or by a private provider contracted by the
state. The extent to which primary care clinicians and services provided in prisons are linked
or integrated into secondary-care-based prison mental health models of car also varies. Very
limited research exists, beyond providing descriptions of health needs, models of care and
audits of provision in some settings, to support the effectiveness of any specific models of
mental health service provision to prisoners.
3.2.1 Prison mental healthcare models in Australia
Levy (21) describes in detail the models for provision of mental healthcare to prisoners across
the various jurisdictions in Australia and in the context of international trends. A wide range
of approaches have evolved, both in terms of the funding and management arrangements,
and in terms of the models of provision. Many states and territories have also adopted a range
of approaches depending on local circumstances, with more remote prison facilities often
reliant on local or ‘fly in fly out’ healthcare professionals providing occasional care while the
larger metropolitan-based prisons have full-time in-reach mental health provision. The ‘prison
hospital wing’ concept which has long been the focus of debate nationally and internationally
also operates in Australian jurisdictions both with and without the ability to provide
healthcare with the support of mental health legislation enabling involuntary treatment.
Some people have seen the former as challenging the notion of equivalence of care since no
such model of care operates in the community (18) while others have opposed the

21
development of the latter on the grounds that prison hospitals intended to function as
community psychiatric hospitals are inherently unable to do so.
The mental health needs of prisoners are addressed by the individual Australian states or
territories which govern mental health funding and the nature of service provision such as
whether services are to be provided by corrective or health departments, outsourced to a third
party, or a combination of these (37). Across all Australian jurisdictions, mental health services to
individuals in contact with the criminal justice system are commonly provided by the health
sector, sometimes in partnership with the criminal justice system (for example, JH&FMHN in
NSW, Forensicare in Victoria, the State Forensic Mental Health Service in Western Australia).
Within the custodial environment, there may be dedicated prison clinics, prison hospital wings or
gazetted hospitals staffed by mental health professionals. The Mental Health Screening Unit
(MHSU) at the Metropolitan Reception and Remand Centre, NSW, is an example of a prison in-
reach service (which also has some of the properties of the ‘hospital wing in prison’) for those
with mental health problems or who pose a risk to themselves or others (38). Inmates presenting
with mental health problems at reception screening are seen by the in-reach mental health team
and/or Risk Assessment and Intervention Team and referred to the MHSU if necessary. Patients
remain in the MHSU until a diagnosis is made and a management plan is established following
multidisciplinary consultations with psychiatrists, general practitioners, psychologists, and
welfare officers. Several discharge pathways are available from the MHSU. For example, patients
can be transferred to a gazetted mental health facility for involuntary treatment, back into the
main jail to be followed up by in-reach mental health teams and/or primary care clinicians or be
diverted from the local court if the patient had been remanded for summary offences.
3.2.2 Mental health screening
Screening of new prisoners for the presence of known prior and unknown mental health need
is a common practice and of significant potential but has been little studied. There are no
consistent models or guidelines for prison mental health screening. Different jurisdictions
tend to use different approaches. In recent times screening tools developed and tested for
use specifically in prisons have appeared. A recent New Zealand study tested the Brief Jail
Mental Health Screening (BJMHS) and English Mental Health Screen (EMHS) tools for new
prison entrants and found the tools to be useful in identifying psychosis and in identifying
those likely to require urgent or semi-urgent psychiatric intervention (39). Given the rate of
false positives resulting from use of the tools, the authors of the study suggested that a

22
second stage screening process entailing a brief triage interview be used for those who screen
positive. Correctional Services in Canada recently implemented a Computerised Mental
Health Intake Screening System, which involves a 45-minute computerised interview typically
administered within 14 days of reception to facilitate timely referrals to other services (40).
The interview uses two psychological measures of distress and an additional attention deficit
and hyperactivity disorder and cognitive screening component. An iterative classification tree
methodology is used to interpret the screening outcome. The potential benefits of effective
screening with prompt access to treatment are multiple and include: guarding against adverse
outcomes (e.g. suicide and self-harm), improving prognosis of those who are acutely unwell,
reducing prison disturbance (as a result of better management of psychiatric symptoms), and
fostering initial engagement with mental healthcare among new entrants with a mental
illness (41). However, evidence suggests that the majority of psychiatric disorders are likely
to be missed during initial screening; routine screening in the UK has been shown to identify
only about 23-33% of prisoners with serious mental illness (42). For those whose illness is not
identified, the stress of incarceration can subsequently lead to worsening of symptoms or
development of additional morbidity (43).
3.2.3 The role of primary and secondary care
The roles of prison primary care clinicians and services in the model of care for provision of mental
health care in prisons has been little studied. Primary care clinicians (typically nurses) are often
tasked with undertaking structured mental health screening of new prisoners in the context of
screening for a wide range of health problems (see 2.4). But the extent to which primary care
clinicians are involved in mental health care beyond screening is unclear. The principle of
equivalence of care (see 3.1.1) would suggest that the models of care typically present in the
community might be replicated in the prison setting and the predominant model in the
community is a ‘Stepped Care Model’. This approach is the current recommended model for
addressing common mental health problems in the community according to UK National Institute
for Health and Clinical Excellence (NICE) guidelines (44). Appendix 1 includes a copy of a figure
taken from these guidelines that details the key elements of the stepped care model for common
mental disorders aimed at non-specialist mental health services. A review of the mental health of
adults in contact with the criminal justice system is currently being undertaken by NICE UK. The
UK-based Standards for Prison Mental Health Services (20) makes explicit reference to the
stepped care model. Of interest, the authors quote Stephen Shaw, a former UK prisons and

23
probation ombudsman, made in 2007 regarding primary care and specialist mental health
responsibilities in the context of prison mental healthcare provision:
…prisons are full of people not ill enough for secondary care but too difficult (or too
transient) for primary services. It is perhaps in that area that services for prisoners
with mental health problems are most in need of strengthening.
Many jurisdictions internationally have grappled with how to best provide mental health care for
prisoners and in the absence of rigorous evidence to favour specific models of care, consultation
exercises are often undertaken with clinicians and other staff. One Primary Care Trust in the UK
undertook such an exercise and concluded that with regard to mental health the stepped care
model is the best practice model for adoption within a prison setting (45). Regarding specialist
mental health specifically, among a range of recommendations, the principles of community-
based crisis resolution services were recommended for adoption to provide 24/7 intensive
assessment and treatment for acute mental health distress open to patients suffering a
severe/enduring mental illness, in mental health crisis and/or at imminent risk of suicide or self-
harm.
Given the stepped care model has been designed for and tested in a non-custodial community
setting, it is worthwhile considering developments in the community models for primary and
secondary mental health care provision beyond stepped care. Integrated care models have
recently been proposed to address the burden of mental and physical ill health co-morbidity
among those with mental illness in the community (46). Although prisoners are not specifically
considered in the proposal developed by the Kings Fund, a well-known healthcare think tank, the
justifications detailed have considerable relevance for those working in prisons. The report lists
trends in the development of integrated service models including both enhanced mental health
support in primary care (collaborative care) and integrated community multidisciplinary teams
which involve both primary and secondary care clinicians working together directly.
It is also important to note that the emphasis has been, perhaps appropriately, on prison models
of mental healthcare provision aimed at serious rather than common mental illnesses. That
emphasis may partly explain the lack of research and commentary on the role of primary versus
secondary mental health services.

24
3.2.4 Evaluations of within-prison models
As noted earlier, rigorous evaluations of the effectiveness of prison mental health models of care
in prison are absent. Some people have argued that existing in-reach mental health services for
example are based on limited and idiosyncratic models of care (47) and typically involve small and
poorly resourced teams in practice (48). The National Evaluation of Prison Mental Health In-Reach
report (49), a UK survey, found that while in-reach team leaders supported the idea of in-reach
services, they also thought that these services were poorly resourced and implemented.
Furthermore, in line with criticism focused on court diversion/liaison services, most clinical
activity for in-reach teams is focused on assessment and liaison/support rather than face-to-face
and ongoing intervention. Some newly developed in-reach teams have strayed from providing
specific targeted interventions for serious mental illnesses to broad primary care level mental
health care, perhaps by necessity in the absence of primary care provision (47). There have been
more concerted attempts to replicate a fully functional community mental health service in a
prison setting and to implement established models of community care such as Assertive
Community Treatment, although such efforts have been met with significant difficulties (50).
Reviews of existing models of care have raised concerns about the significant number of people
in the criminal justice system still receiving little or no care (51). Prison clinics are often unable
to cope with influx of prisoners with complex health needs, and often rely on prisoners to
self-report health conditions. Therefore, only those who present with overt and salient
psychiatric symptoms or request mental health treatment would likely receive attention from
prison clinic staff (52).
There have been some positive outcomes reported to be a result of prison mental health in-
reach services including a reduction in the stigma associated with mental illness for prisoners
and the opportunity for establishing continuity of care after release (49). In a recent New
Zealand study, a new model of care for prisoners with serious mental illness was formally
trialled and evaluated with the new model resulting in increased prisoner numbers across
screening, referral, treatment and engagement (53). Appendix 2 includes a diagram detailing
the steps involved in the new model of care. The role of primary care in the model is at the
level of screening and triage and thus reflects an enhancement but not substantial deviation
away from the stepped care model. The focus of the approach is on serious mental illness
predominantly.

25
References
1. Fazel S, Seewald K. Severe mental illness in 33 588 prisoners worldwide: systematic review and meta-regression analysis. The British Journal of Psychiatry. 2012;200(5):364-73. 2. Butler T, Andrews G, Allnutt S, Sakashita C, Smith NE, Basson J. Mental disorders in Australian prisoners: a comparison with a community sample. The Australian and New Zealand journal of psychiatry. 2006;40(3):272-6. 3. JHFMHN_JJNSW. 2015 Young People in Custody Health Survey: Full Report. Sydney: Justice Health & Forensic Mental Health Network, and Juvenile Justice NSW; 2017. 4. MHRT N. Forensic Guidelines: Version 4. New South Wales Mental Health Review Tribunal; 2017. 5. Forrester A, Henderson C, Wilson S, Cumming I, Spyrou M, Parrott JJPB. A suitable waiting room? Hospital transfer outcomes and delays from two London prisons. 2009;33(11):409-12. 6. Wilson S. Compulsory treatment in prison. Commentary on… The Mental Capacity Act and mental healthcare in prison. The Psychiatrist. 2012;36(7):243-4. 7. Völlm BA, Edworthy R, Huband N, Talbot E, Majid S, Holley J, et al. Characteristics and Pathways of Long-Stay Patients in High and Medium Secure Settings in England; A Secondary Publication From a Large Mixed-Methods Study. Front Psychiatry. 2018;9:140. 8. Davoren M, Byrne O, O'Connell P, O'Neill H, O'Reilly K, Kennedy HG. Factors affecting length of stay in forensic hospital setting: need for therapeutic security and course of admission. BMC Psychiatry. 2015;15:301. 9. Adams J, Thomas S, Mackinnon T, Eggleton DJAP. How secure are the secure psychiatric units in New South Wales? 2019;27(1):32-5. 10. Adams J, Thomas SD, Mackinnon T, Eggleton DJBp. The risks, needs and stages of recovery of a complete forensic patient cohort in an Australian state. 2018;18(1):35. 11. Coid JW, Hickey N, Yang MJTBJoP. Comparison of outcomes following after-care from forensic and general adult psychiatric services. 2007;190(6):509-14. 12. Humber N, Hayes A, Wright S, Fahy T, Shaw JJJoFP, Psychology. A comparative study of forensic and general community psychiatric patients with integrated and parallel models of care in the UK. 2011;22(2):183-202. 13. Sahota S, Davies S, Duggan C, Clarke MJTJoFP, Psychology. The fate of medium secure patients discharged to generic or specialised services. 2009;20(1):74-84. 14. Humber N, Hayes A, Wright S, Fahy T, Shaw J. A comparative study of forensic and general community psychiatric patients with integrated and parallel models of care in the UK. The Journal of Forensic Psychiatry & Psychology. 2011;22(2):183-202. 15. Fazel S, Fiminska Z, Cocks C, Coid J. Patient outcomes following discharge from secure psychiatric hospitals: systematic review and meta-analysis. Br J Psychiatry. 2016;208(1):17-25. 16. Hayes H, Kemp RI, Large MM, Nielssen OB. A 21-year retrospective outcome study of New South Wales forensic patients granted conditional and unconditional release. The Australian and New Zealand journal of psychiatry. 2014;48(3):259-82. 17. United-Nations. Basic principles for the treatment of prisoners. Office of the High Commission for Human Rights; 1990. 18. Wilson S. The principle of equivalence and the future of mental health care in prisons. The British Journal of Psychiatry. 2004;184(1):5-7. 19. Brooker C, Ullman B. Out of Sight, Out of Mind. The state of mental healthcare in prison.; 2008. 20. Georgiou M, Souza R, Holder S, Stone H, Davies S. Standards for Prison Mental Health Services: Quality Network for Prison Mental Health Services. London: Royal College of Psychiatrists; 2015. 21. Levy M. Prisoner health care provision: Reflections from Australia. International Journal of Prisoner Health. 2005;1(1):65-73.

26
22. Charles A, Draper H. ‘Equivalence of care’ in prison medicine: is equivalence of process the right measure of equity? Journal of Medical Ethics. 2012;38(4):215-8. 23. Jacobi JV. Prison Health, Public Health: Obligations and Opportunities. American Journal of Law and Medicine. 2005;31(4):447-78. 24. Kinner SA, Young JT, Carroll M. The pivotal role of primary care in meeting the health needs of people recently released from prison. Australasian psychiatry : bulletin of Royal Australian and New Zealand College of Psychiatrists. 2015;23(6):650-3. 25. Weldon S, Ritchie G. Treatment of dual diagnosis in mentally disordered offenders: application of evidence from the mainstream. Advances in Dual Diagnosis. 2010;3(2):18-23. 26. Baksheev GN, Thomas SDM, Ogloff JRP. Psychiatric disorders and unmet needs in Australian police cells. Australian & New Zealand Journal of Psychiatry. 2010;44(11):1043-51. 27. Butler T, Allnutt S, Cain D, Owens D, Muller C. Mental Disorder in the New South Wales Prisoner Population. Australian and New Zealand Journal of Psychiatry. 2005;39(5):407-13. 28. AIHW. The health of Australia's prisoners 2012 Canberra: AIHW. Canberra; 2013. Contract No.: Cat. no. PHE 170. 29. Kavanagh L, Rowe D, Hersch J, Barnett K, Reznik R. Neurocognitive deficits and psychiatric disorders in a NSW prison population. International Journal of Law and Psychiatry. 2010;33(1):20-6. 30. Herrington V. Assessing the prevalence of intellectual disability among young male prisoners. Journal of Intellectual Disability Research. 2009;53(5):397-410. 31. Hayes S, Shackell P, Mottram P, Lancaster R. The prevalence of intellectual disability in a major UK prison. British Journal of Learning Disabilities. 2007;35(3):162-7. 32. Baldry E, Dowse L, Clarence M. Pathways to prison for mentally ill and cognitively impaired offenders. NSW District Court Annual Conference 2010: UNSW, School of Social Sciences and International Studies.; 2010. 33. Baldry E, Dowse L, Clarence M. People with intellectual and other cognitive disability in the criminal justice system. Sydney: University of New South Wales; 2012. 34. Australian Bureau of Statistics. Prisoners in Australia. In: Statistics ABo, editor. Canberra.: Australian Bureau of Statistics; 2012. 35. Butler C. Indigenous adolescent mental health: what is the role of primary health care? PHCRIS, Research Roundup. 2012(24). 36. Australian Institute of Health and Welfare. The health of Australia's prisoners 2012. Canberra: Australian Institute of Health and Welfare; 2013. 37. (AIHW) AIoHW. The mental health of prison entrants in Australia. Canberra2012. p. 1-24. 38. Adams J, Ellis A, Brown A, Owens D, Halsey R. A Prison Mental Health Screening Unit: a first for New South Wales. Australasian Psychiatry. 2009;17(2):90-6. 39. Evans C, Brinded P, Simpson A, Frampton C, Mulder R. Validation of brief screening tools for mental disorders among New Zealand prisoners. Psychiatric Services. 2010;61(9):923-8. 40. Martin MS, Wamboldt AD, O'Connor SL, Fortier J, Simpson AI. A comparison of scoring models for computerised mental health screening for federal prison inmates. Criminal Behaviour and Mental Health. 2013. 41. Birmingham L. Screening prisoners for psychiatric illness who benefits? Psychiatric Bulletin. 2001;25(12):462-4. 42. Birmingham L, Mason D, Grubin D. Prevalence of mental disorder in remand prisoners: consecutive case study. BMJ: British Medical Journal. 1996;313(7071):1521. 43. Birmingham L, Mason D, Grubin D. A follow-up study of mentally disordered men remanded to prison. Criminal Behaviour and Mental Health. 1998;8(3):202-13. 44. National-Collaborating-Centre-for-Mental-Health. Common mental health disorders: identification and pathways to care. The British Psychological Society and The Royal College of Psychiatrists; 2011. 45. South-Staffordshire-NHS-Primary-Care-Trust. Prison Health: Proposed models of care (adult male prisoners) - consultation exercise. 2009.

27
46. Naylor C, Das P, Ross S, Honeyman M, Thompson J, Gilburt H. Bringing together physical and mental health: a new frontier for integrated care. The Kings Fund; 2016. 47. Steel J, Thornicroft G, Birmingham L, Brooker C, Mills A, Harty M, et al. Prison mental health inreach services. The British Journal of Psychiatry. 2007;190(5):373-4. 48. Brooker C, Gojkovic D. The second national survey of mental health in-reach services in prisons. The Journal of Forensic Psychiatry & Psychology. 2009;20(S1):S11-S28. 49. Offender-Health-Research-Network. A national evaluation of prison mental health in-reach services. 2009. 50. Meiklejohn C, Hodges K, Capon D. Prisoners present a particular challenge for mental health nurses. MENTAL HEALTH NURSING-LONDON-. 2004;24(6):8-11. 51. Thomas JE. Diversion and support of offenders with a mental illness: Guidelines for best practice. In: Justice VDo, editor. Victoria: Justice Health, Victorian Government Department of Justice, and the National Justice Chief Executive Officers' Group; 2010. 52. Coid J, Ullrich S. Prisoners with psychosis in England and Wales: Diversion to psychiatric inpatient services? International Journal of Law and Psychiatry. 2011;34(2):99-108. 53. Pillai K, Rouse P, McKenna B, Skipworth J, Cavney J, Tapsell R, et al. From positive screen to engagement in treatment: a preliminary study of the impact of a new model of care for prisoners with serious mental illness. BMC Psychiatry. 2016;16(1):1-7.

28
Appendix 1 A stepped-care model (shown below) is used to organise the provision of services and to help people with common mental health disorders, their families, carers and healthcare professionals to choose the most effective interventions. The model presents an integrated overview of the key assessment and treatment interventions from this guideline. Recommendations focused solely on specialist mental health services are not included (these can be found in related guidance). Recommendation 1.5.1.3 sets out the components of a stepped-care model of service delivery, which should be included in the design of local care pathways for people with common mental health disorders. (44)
Focus of the intervention Nature of the intervention
Step 3: Persistent subthreshold depressive symptoms or mild to moderate depression that has not responded to a low-intensity intervention; initial presentation of moderate or severe depression; GAD with marked functional impairment or that has not responded to a low-intensity intervention; moderate to severe panic disorder; OCD with moderate or severe functional impairment; PTSD.
Depression: CBT, IPT, behavioural activation, behavioural couples therapy, counselling*, short-term psychodynamic psychotherapy*, antidepressants, combined interventions, collaborative care**, self-help groups.
GAD: CBT, applied relaxation, drug treatment, combined interventions, self-help groups.
Panic disorder: CBT, antidepressants, self-help groups.
OCD: CBT (including ERP), antidepressants, combined interventions and case management, self-help groups.
PTSD: Trauma-focused CBT, EMDR, drug treatment.
All disorders: Support groups, befriending, rehabilitation programmes, educational and employment support services; referral for further assessment and interventions.
Step 2: Persistent subthreshold depressive symptoms or mild to moderate depression; GAD; mild to moderate panic disorder; mild to moderate OCD; PTSD (including people with mild to moderate PTSD).
Depression: Individual facilitated self-help, computerised CBT, structured physical activity, group-based peer support (self-help) programmes**, non-directive counselling delivered at home†, antidepressants, self-help groups.
GAD and panic disorder: Individual non-facilitated and facilitated self-help, psychoeducational groups, self-help groups.
OCD: Individual or group CBT (including ERP), self-help groups.
PTSD: Trauma-focused CBT or EMDR.
All disorders: Support groups, educational and employment support services; referral for further assessment and interventions.
Step 1: All disorders – known and suspected presentations of common mental health disorders.
All disorders: Identification, assessment, psychoeducation, active monitoring; referral for further assessment and interventions.
* Discuss with the person the uncertainty of the effectiveness of counselling and psychodynamic psychotherapy in treating depression. ** For people with depression and a chronic physical health problem. † For women during pregnancy or the postnatal period. CBT, cognitive behavioural therapy; ERP, exposure and response prevention; EMDR, eye movement desensitisation and reprocessing; GAD, generalised anxiety disorder; OCD, obsessive compulsive disorder; IPT, interpersonal therapy; PTSD, post-traumatic stress disorder.

29
Appendix 2
A prison model of care, referral and treatment pathway (53)