Embed Size (px)
Citation preview
Liam E Marshall, PhD Research & Academics Division and Provincial Forensics Waypoint Centre for Mental Health Care
Evidence-based interventions in forensic mental health and correctional settings
Introduction
• Rationale • Administrative Components • Therapeutic features • Evaluation • Future Directions
INTRODUCTION • Goals
– Provide evidence-based psychological treatments to reduce problems associated with mental illness
– Provide evidence-based psychological treatments to reduce risk and criminogenic needs
• Objectives – to meet these goals in empirically supported ways which are respectful toward the client and promote positive patient-staff relations
Rationale: RNR • RISK:
– Treating mental illness only, does not reduce risk for future offending
– Client’s risk for future offending and risk to cause harm to self and others, needs to be considered
• NEEDS: – Mentally ill offenders can profit from addressing empirically
identified criminogenic needs • RESPONSIVITY:
– There is typically less motivation for treatment in mentally ill offenders than in clients who seek treatment
– Skilled & supported facilitators are more effective
3/25/2015 4
Challenges • Choice of interventions • Choice of therapeutic style/model of
intervention • Staff to run interventions • Assessment procedures • Content and process • Over reliance on manuals • Infrastructure • Facility support
3/25/2015 5
Considerations
• Number of patients suitable for psychotherapy
• Range and skill of staff: choice of training • Other responsibilities of treatment staff • Who is the customer?
CDCP: Replicating Effective Programs (REP) project • Systematic and effective strategies to prepare HIV
interventions for dissemination • Four phases:
– Pre-conditions (e.g., identifying need, target population, and suitable intervention)
– Pre-implementation (e.g., intervention packaging and community input)
– Implementation (e.g., package dissemination, training, technical assistance, and evaluation)
– Maintenance and evolution (e.g., preparing the intervention for sustainability)
7
How to Successfully Implement Evidence-Based Social Programs: A Brief Overview for Policymakers and Program Providers. (Gorman-Smith, 2006)
• Step 1: Select an appropriate evidence-based intervention
• Step 2: Identify resources that can help with successful implementation
• Step 3: Identify appropriate implementation sites • Step 4: Identify key features of the intervention that
must be closely adhered to and monitored • Step 5: Implement a system to ensure close
adherence to these key features
8
March 25, 2015 9
Example of an Implementation Strategy in Forensic & Correctional Settings
• Oversight: intervention committee & 3 sub-committees • Required “core” interventions
– Criminogenic: emotional self-regulation & substance abuse (sexual self-regulation, prosocial cognition, domestic violence, relaxation/mindfulness, leisure awareness and skills, self-esteem)
– Others: illness related interventions (e.g., medication & symptom management, CBT for psychosis DBT for BPD)
• Assessments for interventions: only on issues actually addressed in interventions
3/25/2015 10
Suggestions for Implementation
• 1 staff member (psychologist) as over-seer of interventions
• Allocate according to interest and expertise • Empirical, collaborative, reflexive, approach to
program development • Ongoing support through weekly or bi-weekly
clinic meetings with each team and as a unit • Opportunities for immediate debrief when needed
Suggestions for Implementation
Recommended initial approach for groups • Closed format – move to open format when comfortable with
material and process • Minimum two facilitators – Primary & Secondary • Small groups (4+ participants) • Separate groups or individual counseling appropriate for
functioning level of clients (average, low, very low) • Number of sessions/week (min 2, max 3) dependent on risk
and needs • Length (# hours) of sessions – dependent of client
functioning level; i.e., shorter for lower functioning. • Completion criteria: Dependent on goals and objectives • Evaluation: Dependent on goals and objectives
1. Assessment & Triage – Choice of assessment tools – Assignment to intervention
2. Interventions & Reporting – Criminogenic & Mental Health needs – Therapist support & effective reporting
3. Tracking & Evaluation – Completions, dropouts, refusers – Targets of treatment, recidivism, client perspective
3/25/2015 13
Components of Intervention Implementation
ASSESSMENTS • RATIONALE:
– Need to identify each client’s personal Risk, Needs, & Responsivity, issues
– Need to be trauma-informed – Provides tracking of significant treatment-related
trends – Informs treatment decisions – Allows for measurement of treatment-related
progress – All of which, informs the improvement of clinical
services
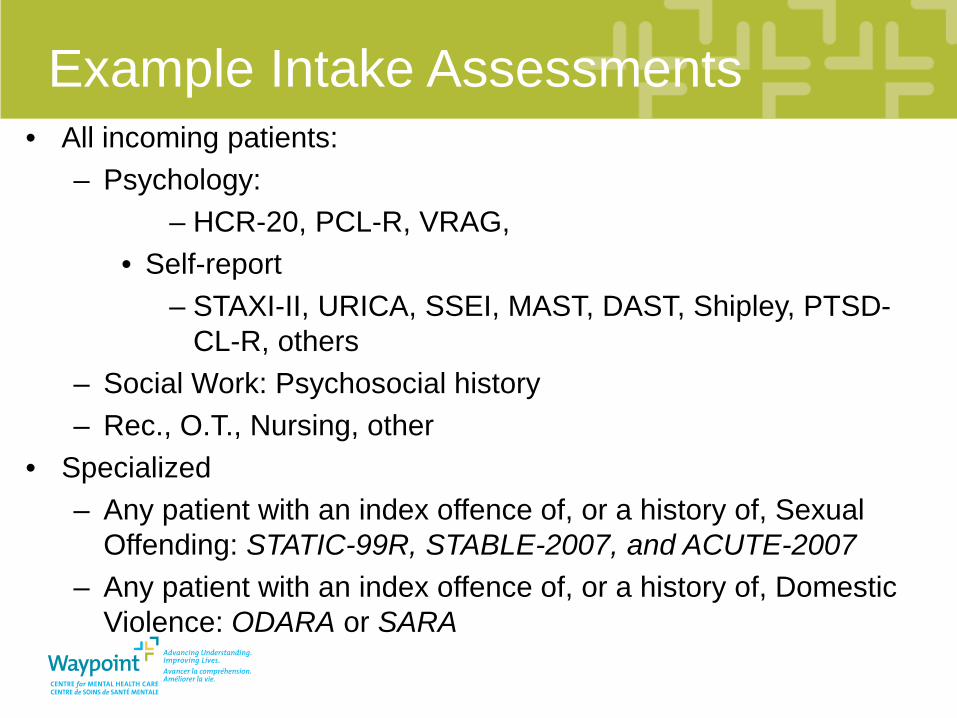
Example Intake Assessments • All incoming patients:
– Psychology: – HCR-20, PCL-R, VRAG,
• Self-report – STAXI-II, URICA, SSEI, MAST, DAST, Shipley, PTSD-
CL-R, others – Social Work: Psychosocial history – Rec., O.T., Nursing, other
• Specialized – Any patient with an index offence of, or a history of, Sexual
Offending: STATIC-99R, STABLE-2007, and ACUTE-2007 – Any patient with an index offence of, or a history of, Domestic
Violence: ODARA or SARA
16
2. Intervention & Reporting • Intervention design and implementation
– Theoretical orientation – Manuals – Training for facilitators
• Supervision – maintaining treatment focus and integrity – Depth & type of supervision
• Reporting results of interventions – Outcome of intervention – Consider stakeholders needs – Structure and length of reports
17
18
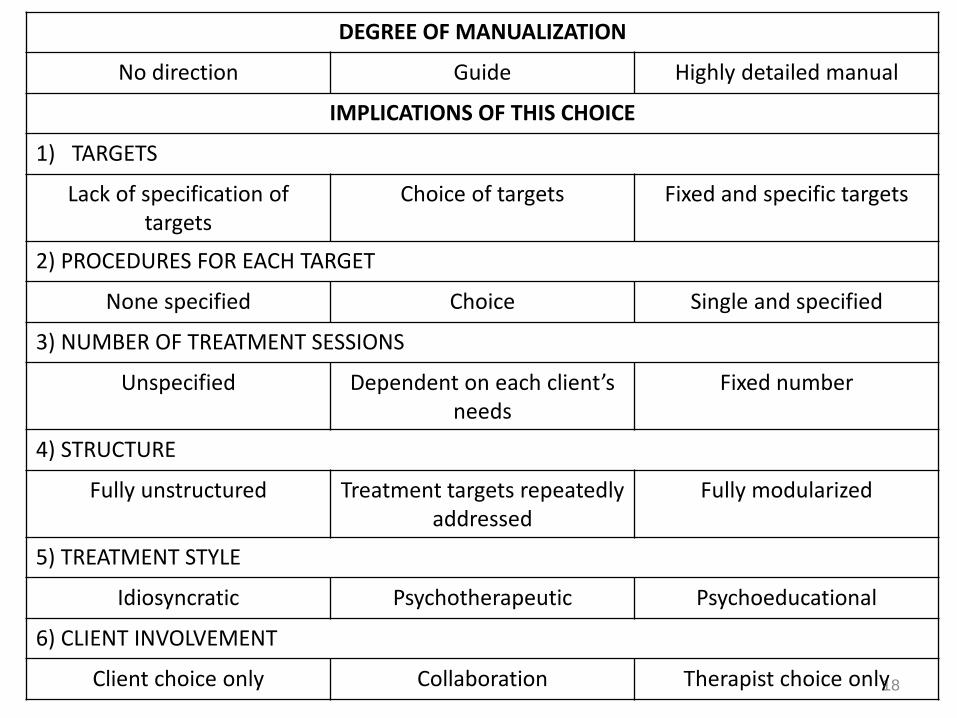
DEGREE OF MANUALIZATION
No direction Guide Highly detailed manual
IMPLICATIONS OF THIS CHOICE
1) TARGETS
Lack of specification of targets
Choice of targets Fixed and specific targets
2) PROCEDURES FOR EACH TARGET
None specified Choice Single and specified
3) NUMBER OF TREATMENT SESSIONS
Unspecified Dependent on each client’s needs
Fixed number
4) STRUCTURE
Fully unstructured Treatment targets repeatedly addressed
Fully modularized
5) TREATMENT STYLE
Idiosyncratic Psychotherapeutic Psychoeducational
6) CLIENT INVOLVEMENT
Client choice only Collaboration Therapist choice only
19
3. Tracking & Evaluation
• Successful completions, refusers, dropouts
• Pre & Post testing • Client satisfaction • Recidivism
20
21
March 25, 2015 22
Sample Outcomes
Example outcomes: Facility “A”
Pre • Few programs running, no structure, no oversight,
outdated approach, conflict between medical and allied health staff
• Low staff morale and difficulty recruiting Strategy: provide training to interested staff members,
implement one intervention, then expand
23
Example outcomes: Facility “A” Post • Every Allied Health team member running at least one
criminogenic need-related group intervention with evaluation and reporting processes in place
• Medical staff (physicians & nurses) also running groups • Clients’ perspectives canvassed • Achievement of targets of treatment
24
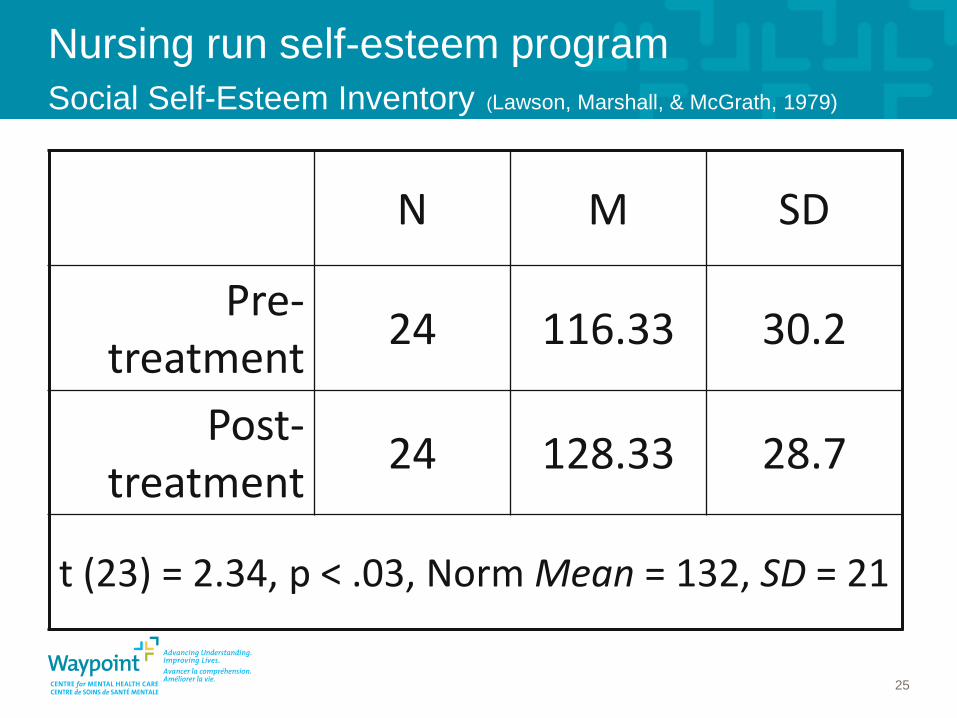
Nursing run self-esteem program Social Self-Esteem Inventory (Lawson, Marshall, & McGrath, 1979)
N M SD
Pre-treatment 24 116.33 30.2
Post-treatment 24 128.33 28.7
t (23) = 2.34, p < .03, Norm Mean = 132, SD = 21
25
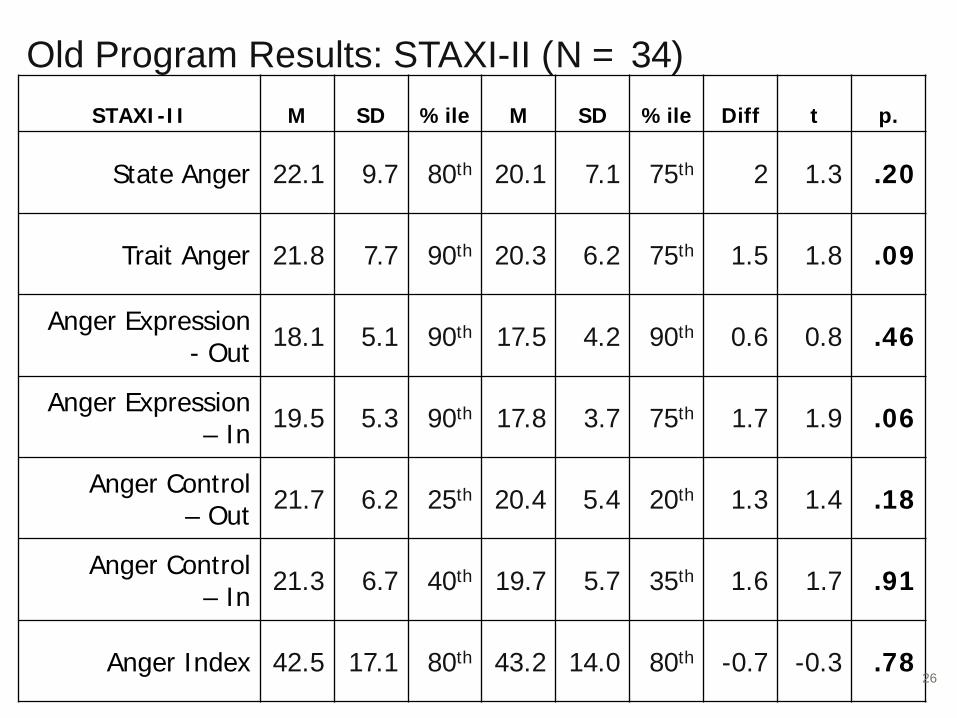
Old Program Results: STAXI-II (N = 34) STAXI-II M SD %ile M SD %ile Diff t p.
State Anger 22.1 9.7 80th 20.1 7.1 75th 2 1.3 .20
Trait Anger 21.8 7.7 90th 20.3 6.2 75th 1.5 1.8 .09
Anger Expression - Out 18.1 5.1 90th 17.5 4.2 90th 0.6 0.8 .46
Anger Expression – In 19.5 5.3 90th 17.8 3.7 75th 1.7 1.9 .06
Anger Control – Out 21.7 6.2 25th 20.4 5.4 20th 1.3 1.4 .18
Anger Control – In 21.3 6.7 40th 19.7 5.7 35th 1.6 1.7 .91
Anger Index 42.5 17.1 80th 43.2 14.0 80th -0.7 -0.3 .78 26
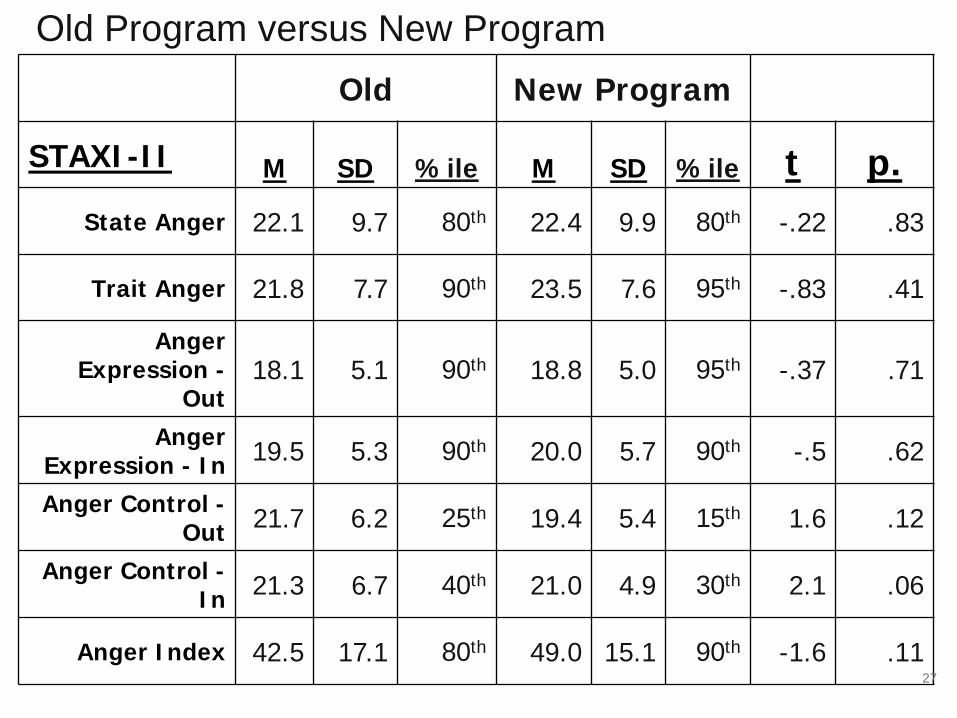
Old New Program
STAXI-II M SD %ile M SD %ile t p. State Anger 22.1 9.7 80th 22.4 9.9 80th -.22 .83
Trait Anger 21.8 7.7 90th 23.5 7.6 95th -.83 .41
Anger Expression -
Out 18.1 5.1 90th 18.8 5.0 95th -.37 .71
Anger Expression - In 19.5 5.3 90th 20.0 5.7 90th -.5 .62
Anger Control - Out 21.7 6.2 25th 19.4 5.4 15th 1.6 .12
Anger Control - In 21.3 6.7 40th 21.0 4.9 30th 2.1 .06
Anger Index 42.5 17.1 80th 49.0 15.1 90th -1.6 .11
Old Program versus New Program
27
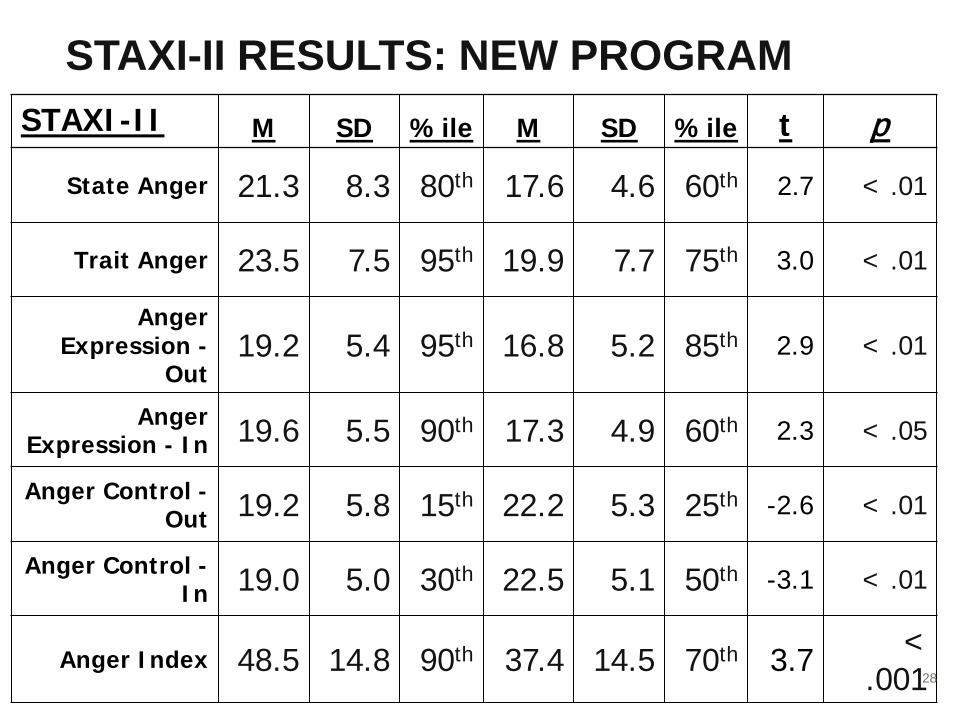
STAXI-II M SD %ile M SD %ile t p
State Anger 21.3 8.3 80th 17.6 4.6 60th 2.7 < .01
Trait Anger 23.5 7.5 95th 19.9 7.7 75th 3.0 < .01
Anger Expression -
Out 19.2 5.4 95th 16.8 5.2 85th 2.9 < .01
Anger Expression - In 19.6 5.5 90th 17.3 4.9 60th 2.3 < .05
Anger Control - Out 19.2 5.8 15th 22.2 5.3 25th -2.6 < .01
Anger Control - In 19.0 5.0 30th 22.5 5.1 50th -3.1 < .01
Anger Index 48.5 14.8 90th 37.4 14.5 70th 3.7 < .001
STAXI-II RESULTS: NEW PROGRAM
28
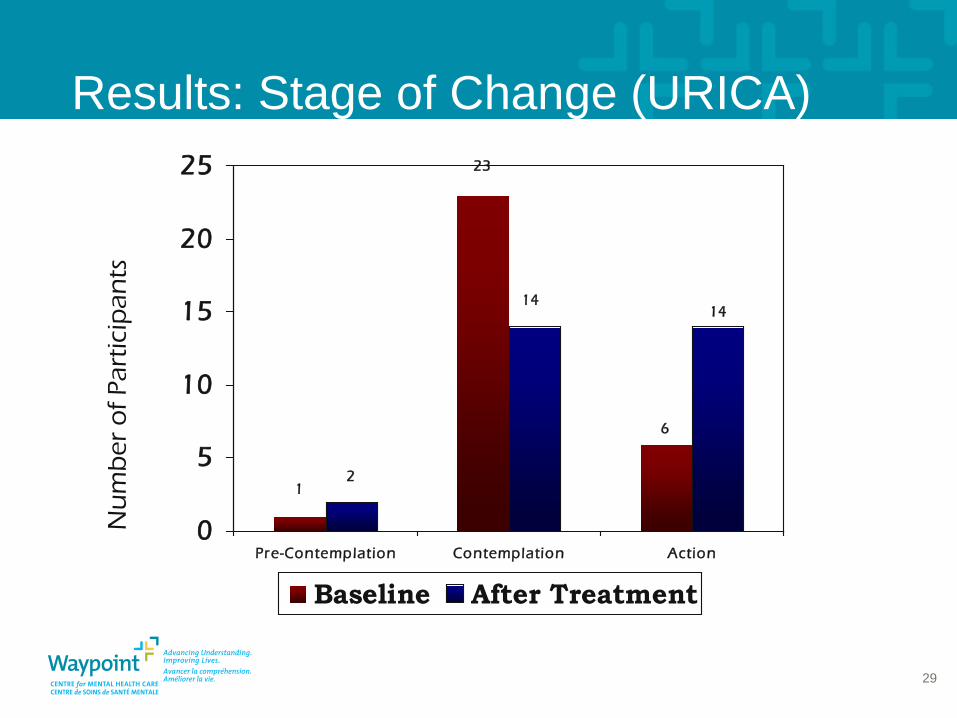
Results: Stage of Change (URICA)
6
14
1
23
2
14
0
5
10
15
20
25
Pre-Contemplation Contemplation Action
Baseline After Treatment
Nu
mb
er o
f Par
ticip
ants
29
30
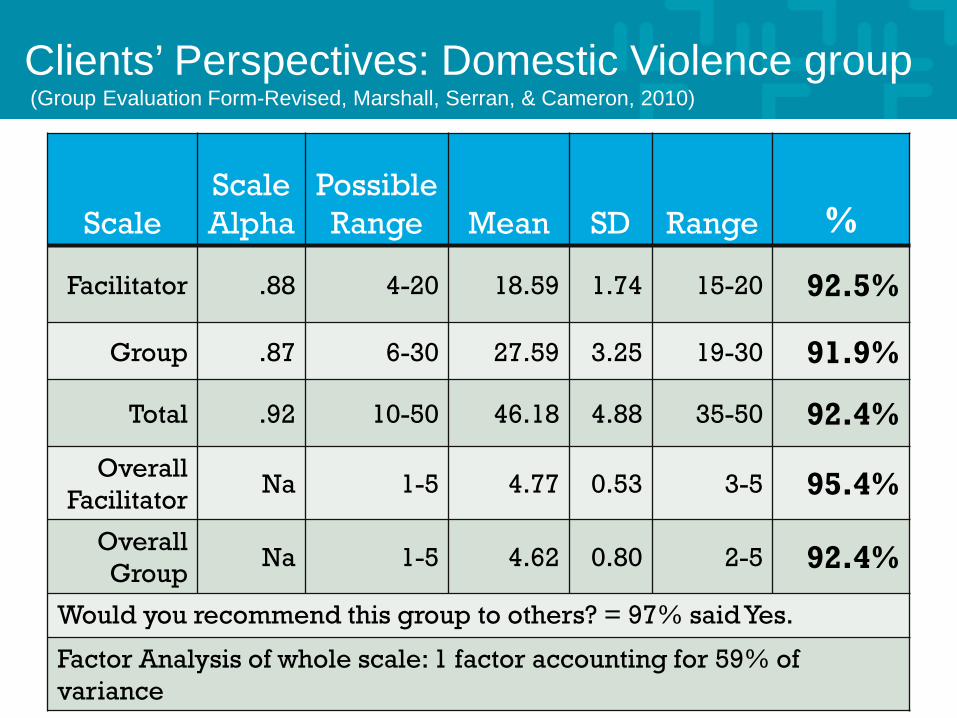
Clients’ Perspectives: Domestic Violence group (Group Evaluation Form-Revised, Marshall, Serran, & Cameron, 2010)
Scale Scale Alpha
Possible Range Mean SD Range %
Facilitator .88 4-20 18.59 1.74 15-20 92.5%
Group .87 6-30 27.59 3.25 19-30 91.9%
Total .92 10-50 46.18 4.88 35-50 92.4%
Overall Facilitator
Na 1-5 4.77 0.53 3-5 95.4%
Overall Group
Na 1-5 4.62 0.80 2-5 92.4%
Would you recommend this group to others? = 97% said Yes.
Factor Analysis of whole scale: 1 factor accounting for 59% of variance
31
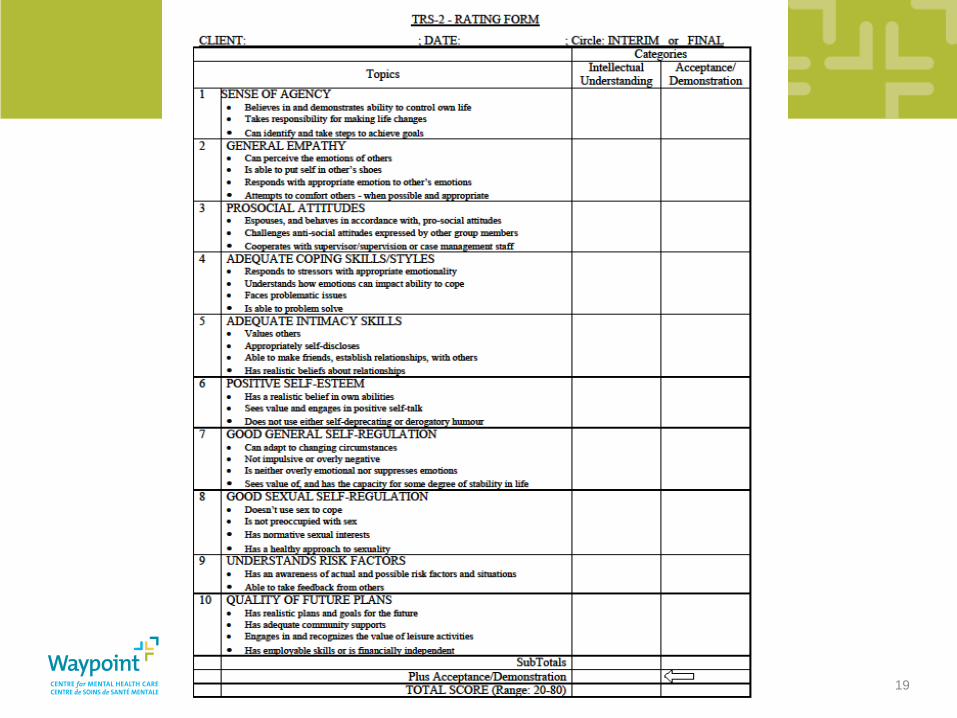
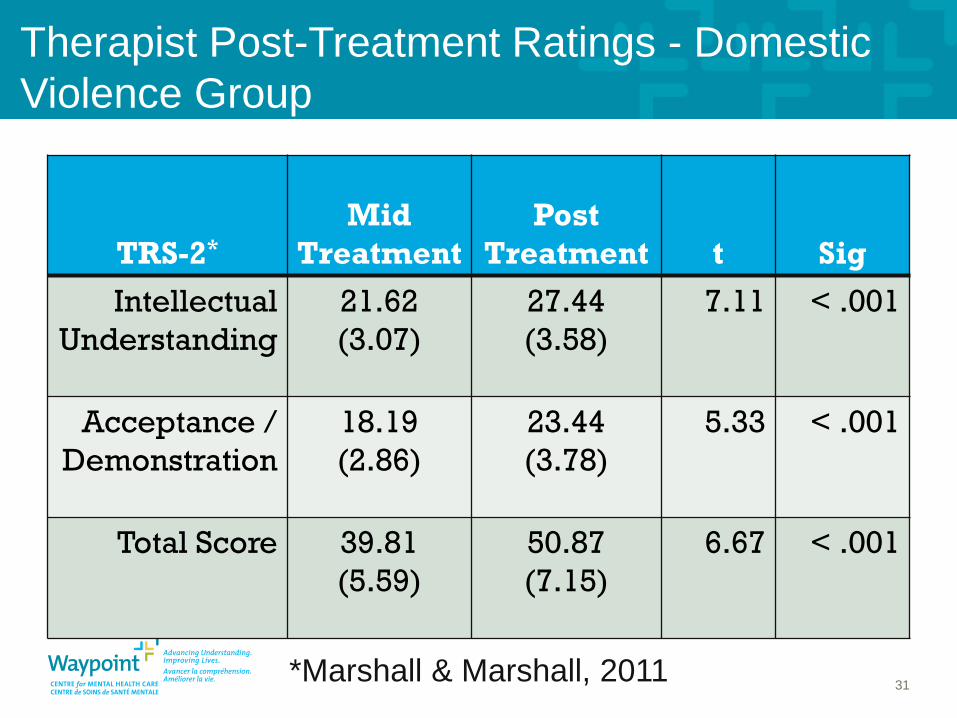
Therapist Post-Treatment Ratings - Domestic Violence Group
TRS-2* Mid
Treatment Post
Treatment t Sig Intellectual
Understanding 21.62 (3.07)
27.44 (3.58)
7.11 < .001
Acceptance / Demonstration
18.19 (2.86)
23.44 (3.78)
5.33 < .001
Total Score 39.81 (5.59)
50.87 (7.15)
6.67 < .001
*Marshall & Marshall, 2011
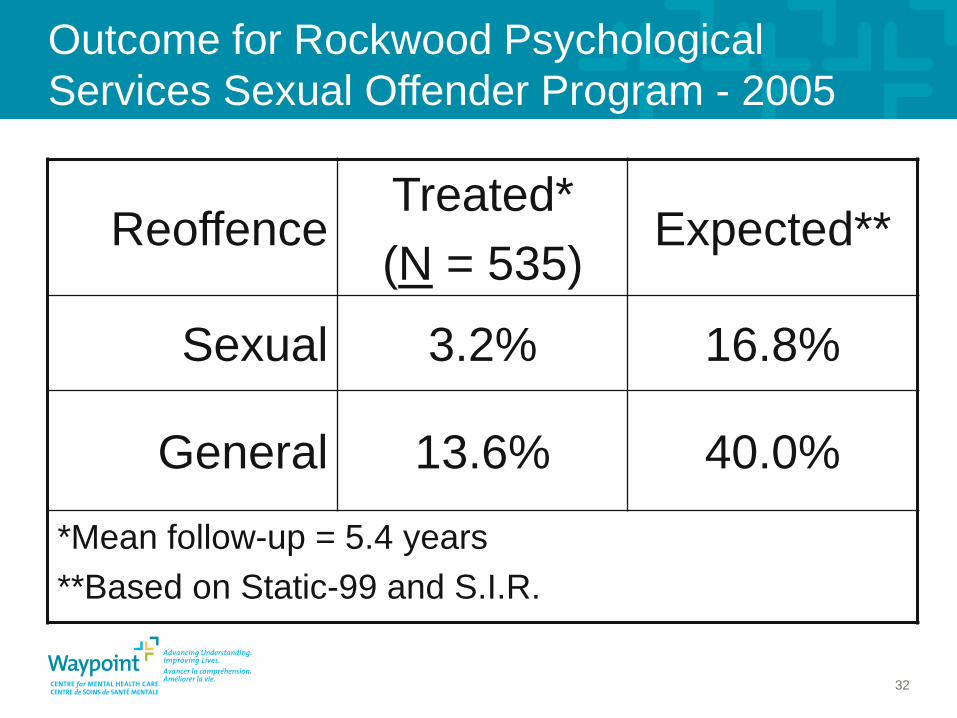
Outcome for Rockwood Psychological Services Sexual Offender Program - 2005
32
Reoffence Treated* (N = 535)
Expected**
Sexual 3.2% 16.8%
General 13.6% 40.0%
*Mean follow-up = 5.4 years **Based on Static-99 and S.I.R.
Summary • Interventions for mentally ill and other offenders can
be effective • Proposed structure meets needs of clients, justice
system, and other stakeholders – Provides treatment needed to move through
system – Helps to reduce reoffending – Efficient use of resources
33
Liam E Marshall, PhD Research & Academics Division and Provincial Forensics Division Waypoint Centre for Mental Health Care
Evidence-based interventions in forensic mental health and correctional settings
34