Embed Size (px)
Citation preview

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 1/92
Enteral
andParenteral
NutritionDiane Mendoza, RND, MSCN

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 2/92
Enteral and Parenteral Nutrition
OUTLI
NE:Introduction
Enteral Nutrition:
DefinitionIndications and Contraindications
Feeding Routes
Formula SelectionAdministration
Considerations
Monitoring

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 3/92
Enteral and Parenteral Nutrition
Parenteral Nutrition:Definition
Indications and Contraindications
Feeding AccessComponents of PN
Complications
MonitoringTransitional feeding and Discontinuation

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 4/92
³ The Skeleton in theHospital Closet´
Body Height not recorded in56%
Body Weight not Recordedin 23%
61% of those with recorded
weigh
t loss > 6 kg 37% had albumin < 3.0 gm/dl
Butterworth, CE, Nutr, Today 1974, April 4-8
Introduction:
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 5/92
Prevalence of Malnutrition
30 ± 50% of Hospitalized Patients worldwide
> In the US 30 ± 50 %
> In Britain 20 ± 48 %
> In Brazil 46 %
In the Philippines
> Private Hospital (SLMC) 48 %
>Gov¶t. Hospital (Amang Rodriguez)52%
Introduction:

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 6/92
NORMAL Starvation:
Lean bodymass
Gluconeo-genesis
ProteinCatabolism
NegativeN2 Balance
Water & MineralDepletion
Adjustment toNew Metabolic
State
Introduction:

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 7/92
Enteral and Parenteral Nutrition
FOODS
GIT
CELLS
LIVER
NORMAL PHYSIOLOGIC ROUTE OF FOOD

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 8/92
Enteral and Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 9/92
Enteral and Parenteral Nutrition
PROPER NUTRITION INTERVENTION
WHAT CAN WE DO?...

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 10/92
Enteral and Parenteral Nutrition
From: Dr. Jeff inciong
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 11/92
Enteral Nutrition
Supplementation or total nutrition feeding directlyinto the GIT using a feeding tube.
Beneficial effect on maintenance of intestinalstructure and function.
Enhanced utilization of nutrients, ease and safetyof administration and cost efficiency.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 12/92
Enteral Nutrition
From: Dr. Jeff inciong

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 13/92
Enteral and Parenteral Nutrition
If the gut isWORKING;
USE IT!

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 14/92
Indication for Use:
ASPEN GUIDELINES FOR USE OF ENTERAL TUBE FEEDINGS
patients with PEM with inadequate oral intake for the previous5 days;
With < 50% of required needs for the previous 7 to 10 days
Severe dysphagia
Major full thickness burns
Short gut
Psychiatric/eating disorders Impaired swallowing
Increased nut¶l losses (sepsis)

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 15/92
ASPEN GUIDELINES FOR USE OF ENTERAL TUBE FEEDINGS:
LIMITED OR UNLIMITED VALUE
Px receiving intensive therapy;
Px with acute enteritis secondary to radiation, acute infectionor active inflammatory bowel disease;
Px with <10% remaining small intestines
Indication for Use:

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 16/92
ASPEN GUIDELINES FOR USE OF ENTERAL TUBE FEEDINGS:
CONTRAINDICATED
Px with complete or small bowel obstruction;
Px with ileus or intestinal hypomotility
Px with severe diarrhea resistant to pharmocologic tx
Severe pancreatitis
Shock
Gastrointestinal bleeding
Legal matters
Contraindications:

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 17/92
FEEDING ROUTES
NASOENTERIC FEEDING
Feeding Routes:

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 18/92
Feeding Routes:
ENTEROSTOMYFEEDING

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 19/92
Summary of Enteral Access Sites:
SITE INDICATIONS ADVANTAGES DISADVANTAGES
NASOGASTRIC normal GI function uses and stimulate GI aspiration
flexibility in administration discomfort
medications can be placed nasal irritation
tube insertion at bedside tube displacement
NASODUODENAL normal small intestine tube insertion at bedside discomfort
need to bypass stomach tube displacement
NASOJEJUNAL normal small intestine tube insertion at bedside discomfortneed to bypass stomach tube displacement
GASTROSTOMY normal GI funx. Long term feeding access surgical procedurebypass the upper GI reduced risk of displacement irritation
allows bolus feeding infection on sitePEG normal GI outpatient procedure irritation and infection
bypass the upper GI long term feeding access for insertion siteless expensive; reduced riskfor tube displacement
JEJUNOSTOMY normal GI function increased tolerance for early surgical procedurebut need to bypass initiation of EN risk for irritationcomponents of GI tract and infection, risk of
clogging may be greater

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 20/92
Formula Selection:

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 21/92
Formula Selection: Substrate Sources
POLYMERIC FORMULA composed of intact proteins, disaccharides and
polysaccharides variable amounts of fat, residue and lactose. osmolality of polymeric
formulas is usually lower thanthe osmolality of ³elemental´formulas.
In general, these formulasrequire a functioning
gastrointestinal tract fordigestion and absorption of nutrients.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 22/92
Enteral and Parenteral Nutrition
PREDIGESTED
FORMULA
composed of low molecular
weight nutrients minimal residue are thought to
lead to less stimulation of pancreatic and gastrointestinalsecretions
less allergenic th
an oth
erformula.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 23/92
Enteral and Parenteral Nutrition
MODULAR PRODUCTS
individual micronutrient
modules such as glucosepolymers, protein, orlipids are available asadditives to food andenteral formulas to
ch
ange overall fuelcomposition.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 24/92
Enteral and Parenteral Nutrition
SPECIAL DISEASE-SPECIFIC
FORMULASthese products are designed
for patients who have specific
medical conditions that may
require nutrient modification.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 25/92
Enteral and Parenteral Nutrition
DIETARY FIBER
Fiber-containing enteral formulas are most viscous
and may require a larger diameter feeding tube foradequate flow.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 26/92
Formula Selection: Osmolality
Measure of the oncotic pressure exerted by a solution;
What determines osmolality?Number and
Size of : electrolytes, CHO; minerals; CHONFactors that can increase osmolality?
Concentration of formulas; (energy:volume)Addition of modular products
Formulas with higher osmolality may induce the shiftof free water into the intestinal space; thus may
cause rapid transit diarrhea.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 27/92
Administration:
Continuous feeding ±constant, steady rate over a 16-24hour period, Cyclic Feeding ± delivered by continuous drip method at
an increased rate over 8 to 16 hours, Intermittent feeding- can be infused at specific intervalsthroughout the day, Bolus feeding- rapid administration of feeding

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 28/92
Administration:
Conversion to glucose as a majorenergy source
Insulin release
Cellular Glucose Uptake, Protein synthesis
Clinical Symptoms of refeedingsyndrome
Depletion of Phosphate, K+ & Mg
Refeeding Syndrome:

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 29/92
Initiation and Special Considerations
INITIATION
can be started at 10-40 ml/hr, then progressuntil desired rate.
CONSIDERATIONS:Temperature
Bacterial Contamination
Prevention of aspiration
Patency
Medications

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 30/92
Complications: Gastrointestinal
Diarrhea
Hyperosmolar formula
Malabsorption
Bolus feeding, volume overload, rapid
administration
PEM
Hypoalbuminemia
Medications
Nausea or vomiting
Constipation
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 31/92
Complications:Mechanical
Mechanical Problems:
Occlusion or clogging of the tube
Misplacement of the tube
Skin irritation around ostomy site
Metabolic problems
Electrolyte and metabolic abnormalities
deh
ydration

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 32/92
Termination of Tube Feeding
Gradual weaning;
Increased oral intake
Decreasing the volume of the formula
can eat/drink the formula that was earlier on the
tube
Monitor oral intake.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 33/92
Monitoring:
Tube placement
Daily weight
Intake and output
CBG (DM, px w/ steroids)
Gastric residuals (esp. if h
igh
risk foraspiration)
Bowel movements and consistency
Feeding tolerance
ElectrolytesBaseline and weely reassesment of nut.indeceswith appropriate adjustments
Daily feeding tube site care

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 34/92
How to Compute for NutritionalHow to Compute for NutritionalRequirements:Requirements:
Given Data:Given Data:
Ht 5¶4´ Ht 5¶4´
Age 54 years oldAge 54 years old
Wt 78 kgs.Wt 78 kgs.
Diet RxDiet Rx 35 kcal/ kg BW 1.2 gms CHON 60%35 kcal/ kg BW 1.2 gms CHON 60%HBV No Sources of Simple SugarsHBV No Sources of Simple SugarsLow PotassiumLow Potassium

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 35/92
To Compute :To Compute :
DBW= 5 x 12 = 60DBW= 5 x 12 = 6060 + 4 = 6460 + 4 = 6464 x 2.54=162.5664 x 2.54=162.56162.56162.56 ±± 100 =62.56100 =62.56-- 6.256 (10%)6.256 (10%)
= 56.31 kg DBW= 56.31 kg DBW

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 36/92
ExampleExample
To Assess:To Assess:
% IDW= 78 kg% IDW= 78 kg
56.31 kg56.31 kg
= 1.39 x 100 = 139 %= 1.39 x 100 = 139 %
Interpretation:Interpretation:
Patient is Obese class 1Patient is Obese class 1

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 37/92
To follow diet Rx:
CHON= 56.31 x1.2x=67.84 ~ 68 gm CHON68 x 4=272 kcal
TER= 35 x 56.31 = 1970.85 kcal
NPC = 1970.85 ± 272 = 1698.85
1698.85 x 0.6 = 1019.31 kcal / 4=254.83 ~ 255 gm CHO
1698.85 x 0.4 = 679.54 / 9= 75.51 ~75 gm FATS

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 38/92
Complete Diet RX
TER= 1970.85 kcal/ day255 gm CHO / day
68 gm CHO
N/ day75 gm Fats /day

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 39/92
Food Item Exchanges CHO
gm
CHON
gm
Fats
gm
Kcal
Vegetables 2 6 2 - 32
Fruit 2 20 - - 80
Milk, low
Fat 2 24 16 10 250
Rice 9 207 18 - 900
Meat/EW 4 - 32 4 164
Fats 12 - - 60 540
Total - 257 68 74 1966
Computation based on FELComputation based on FEL

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 40/92
Enteral and Parenteral Nutrition
Enteral Formula Scoop perCan
1 CUP 1 SCOOP
CHO PRO FAT KCAL CHO PRO FAT KCAL
Ensure 1 kg (Vanilla) 112 (1000) 72.8 19.74 17.5 1056 5.20 1.41 1.25 37.72
Nutren Fiber 49 (400) 57.85 18.3 17.4 458.25 4.45 1.41 1.34 35.25
Nutren Optimum 54 (400) 63.56 20.16 19.18 503.3 4.54 1.44 1.37 35.95
Nutren Diabetes 43 (400) 55.08 18.84 21.72 491.16 4.59 1.57 1.81 40.93
Nutren Junior 51 (400) 63.44 14.17 18.72 476.58 4.88 1.09 1.44 36.66
Peptamen 48 (400) 72.15 23.25 22.65 586.2 4.81 1.55 1.51 39.08
Peptamen Junior 51 (500) 4.97 1.08 1.37 36.09
Nutricomp Protein 100 (250) 0 59.8 6.5 245.18 0 2.3 .25 9.43
Nutricomp Caloric 90 (450) 121.5 0 0 513 4.5 0 0 19
Nutricomp Renal - 55.75 20.67 28.37 559.99 *44.8 *16.
6
*22.8 *450
Impact CHON 30 (453.7) 1.65 11.7
5
.32 53
polycose 94 - - - 5.64/tbsp _ - -
Resource 50(400) 4.9 1.25 1.25 35.7
Aminoleban EN - 31.05* 13.5*
3.5* 210*
Glucerna SR 48 (400) 62.92 23.79 17.29 477.88 4.84 1.83 1.33 36.76
Prosure 46(380) 81 27 10 502.5

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 41/92
Computation using Nutritional andComputation using Nutritional andmodularmodular
Diet Rx 35 kcal/ kg BW 1.2 gms CHON 60% HBV NoDiet Rx 35 kcal/ kg BW 1.2 gms CHON 60% HBV NoSources of Simple Sugars Low PotassiumSources of Simple Sugars Low Potassium
255 gmCHO
68 gmCHON
75 gmFats K,mg
Nutren Db 3.5 c -192.78 -65.94 -76.02 2184
difference 62.22 2.06 -1.08 -
Polycose 11 tbsp -62.04 - - -
NutricompProtein 0.18 2.3 - -
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 42/92
Computation using Nutritional and naturalComputation using Nutritional and naturalfoodsfoods
255 gmCHO
68gmCHON
75 gmFats K, mg
Nutren Db, 2 c 110.16 37.68 43.44 1248
difference 144.84 30.32 31.56 -Veg, 1 c. 6 2 95
fruit, 2 's 20 160
bread, 5's 115 10 175
Eggwhite, 4's 16 2 190oil, 6 tsp 30 138
TOTAL 251.16 65.68 75.44 2006
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 43/92
Enteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 44/92
Parenteral Nutrition
WHEN ENTERAL INTAKE ISu
uIMPOSSIBLE
...IMPROBABLE uINADVISABLE
uHAZARDOUS
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 45/92
Parenteral Nutrition
PARENTERAL NUTRITION ± is the provision of nutrients into the bloodstream intravenously.
para=
outsideenteron = intestine
intra = within
vena = vein

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 46/92
Indications:
cancer px w/ GI problems
Preoperative PN
Acute inflammatory
bowel diseaseRenal failure
Hepatic disease
Acute pancreatitis
Critical care
Short bowelsyndrome
Eating disorders

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 47/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 48/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 49/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 50/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 51/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 52/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 53/92
Parenteral NutritionParenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 54/92
Parenteral NutritionParenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 55/92
Parenteral NutritionParenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 56/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 57/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 58/92
Parenteral Nutrition
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 59/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 60/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 61/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 62/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 63/92
Parenteral Nutrition
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 64/92
Parenteral Nutrition
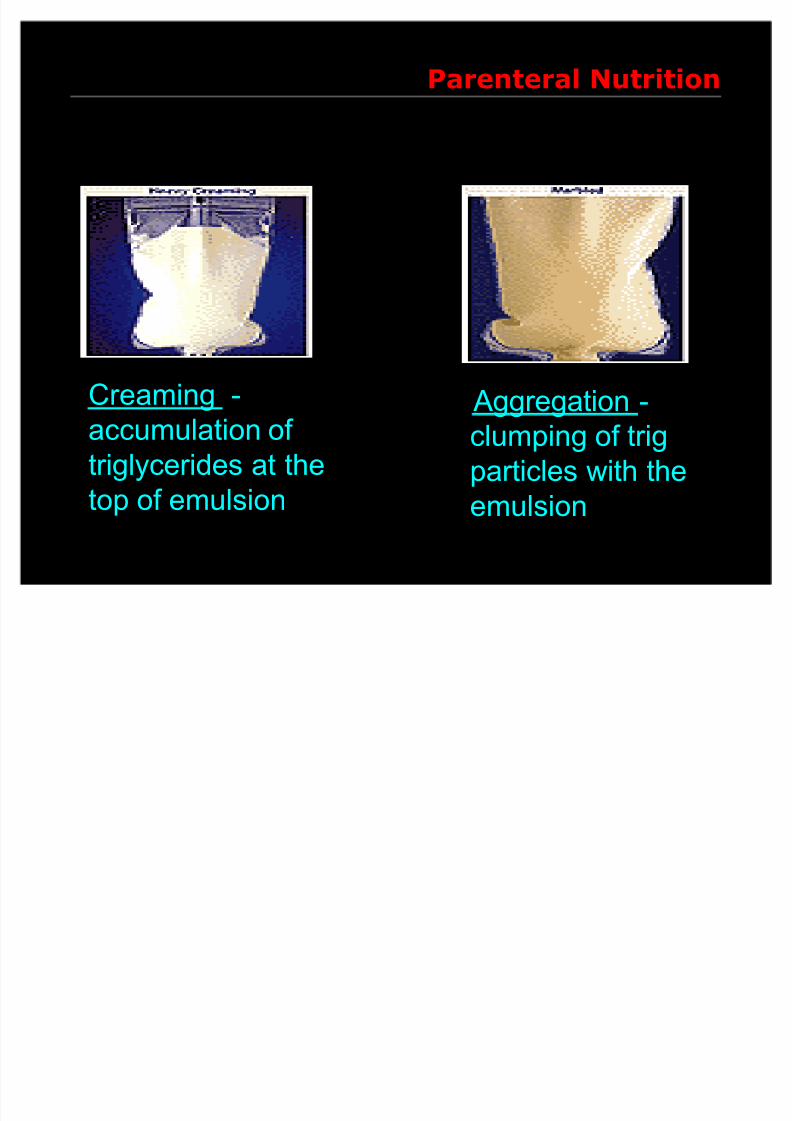
Aggregation -
clumping of trig
particles with the
emulsion
Creaming -
accumulation of triglycerides at the
top of emulsion
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 65/92
Parenteral Nutrition
Cracking ±
separation of the oil andwater components of
the emulsion
Coalescence -
fusion of small trigparticles into larger
particles

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 66/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 67/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 68/92
Parenteral Nutrition

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 69/92
Parenteral Nutrition
Macronutrient Concentrations in PN

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 70/92
Macronutrient Concentrations in PNSolutions
Macronutrient concentrations (%) = thegrams of solute/100 ml of fluid
D70 has 70 grams of dextrose per 100 ml.
10% amino acid solution has 10 gramsamino acids/100 ml of solution
20% lipids has 20 grams of lipid/100 ml of solution

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 71/92
Parenteral Nutrition
Protein Content Calculations
To calculate the
grams of protein
supplied by a TPN solution, multiply the
total volume of
amino acid solution
(in ml*) supplied in aday by the amino
acid concentration.
Example Protein
Calculation
1000 ml of 8%amino acids:
1000 ml x 8 g/100
ml = 80g
Or 1000 x .08 = 80 g

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 72/92
Parenteral Nutrition
Calculation of Dextrose Calories Calculate grams of dextrose:
± Multiply the total volume of dextrose soln(in ml) supplied in a day by the dextrose
concentration. This gives you grams of dextrose supplied in a day.
Multiply the grams of dextrose by 3.4 (there
are 3.4 kcal/g dextrose) to determinekcalories supplied by dextrose in a day.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 73/92
Parenteral Nutrition
Sample Dextrose Calculation
1000 ml of D50W (50% dextrose)
± 1000 ml x 50g / 100 ml = 500g dextrose
± OR 1000 ml x .50 = 500g dextrose
500g dextrose x 3.4 kcal/g = 1700 kcal

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 74/92
Parenteral Nutrition
Calculation of Lipid Content
To determine kcalories supplied by lipid*,multiply the volume of 10% lipid (in ml) by1.1; multiply the volume of 20% lipid (in ml)by 2.0.
If lipids are not given daily, divide totalkcalories supplied by fat in one week by 7 toget an estimate of the average fat kcaloriesper day.
*Lipid emulsions contain glycerol, so lipid emulsion does
not have 9 kcal per gram as it would if it were pure fat.
Some use 10 kcal/gm for lipid emulsions.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 75/92
Parenteral Nutrition
500 ml of 10% lipid
± 500 ml x 1.1 kcal/ml = 550 kcal
500 ml 20% lipid
± 500 ml x 2.0 kcal/ml = 1000 kcal
Or, alternatively, 500 ml of 10% lipid = 50grams lipid x 10 kcal/g or 500 kcal

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 76/92
Parenteral Nutrition
Calculation of Dextrose/AA with
Piggyback Lipids (2-in-1)
Determine patient's kcalorie, protein,and fluid needs.
Determine lipid volume and rate for"piggy back" administration. ± Determine kcals to be supplied from lipid.
(Usually 30% of total kcals).
± Divide lipid kcals by 1.1 kcal/cc if you areusing 10% lipids; divide lipid kcals by 2kcal/cc if you are using 20% lipids. This isthe total volume.
± Divide total volume of lipid by 24 hr to
determine rate in cc/hr.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 77/92
Parenteral Nutrition
Example Calculation
Nutrient Needs:
Kcals: 1800. Protein: 88 g. Fluid: 2000 cc
1800 kcal x 30% = 540 kcal from
lipidLipid (10%):
±540 kcal/1.1 (kcal/cc) = 491 cc/24 hr=
20 cc/hr 10% lipid (round to 480 ml)
Remaining fluid needs: 2000cc - 480cc= 1520cc

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 78/92
Parenteral Nutrition
Determine Protein concentration
Subtract volume of lipid from total fluidrequirement to determine remainingfluid needs.
Divide protein requirement (in grams)by remaining fluid requirement andmultiply by 100. This gives you theamino acid concentration in %.
Multiply protein requirement in grams x4 to determine calories from protein
8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 79/92
Parenteral Nutrition
Protein Calculations
Protein: 88 g / 1520 cc x 100 =5.8% amino acid solution
88 g. x 4 kcal/gm =352 kcals fromprotein
Remaining kcal needs: 1800 ± (528 +
352)=
920 kcal

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 80/92
Parenteral Nutrition
Determine dextrose concentration.
Subtract kcals of lipid + calories fromprotein from total kcals to determineremaining kcal needs.
Divide "remaining kcals" by 3.4 kcal/gto determine grams of dextrose. Divide dextrose grams by remaining
fluid needs (in protein calculations) and
multiply by 100 to determine dextroseconcentration. Determine rate of AA/dex solution by
dividing "remaining fluid needs´ by 24hr.

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 81/92
Parenteral Nutrition
Dextrose Concentration
920 kcal/3.4 kcal/g = 270 g dextrose
270 g / 1520 cc x 100=
17.
7%dextrose solution Rate of Amino Acid / Dextrose: 1520 cc / 24hr = 63 cc/hrT
PN recommendation: Suggest two-in-one PN 17.7% dextrose, 5.8% a.a. @63 cc/hr with 10% lipids piggyback @20 cc/hr

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 82/92
Parenteral Nutrition
Re-check calculations
TPN recommendation: Suggest two-in-one PN 17.7% dextrose, 5.8% a.a. @63 cc/hr with 10% lipids piggyback @
20 cc/hr63 cc/hr x 24 = 1512 ml
1512 * (.177) = 268 g D X 3.4 kcals= 911 kcals
1512 * (.058) = 88 g a.a. x 4 kcals = 352
20 cc/hr lipids*24 = 480*1.1 kcals/cc = 528

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 83/92
Parenteral Nutrition
Evaluation of a PN OrderPN 15% dextrose, 4.5% A.A., 3% lipid @
100 cc/hour
Total volume = 2400
Dextrose: 15g/100 ml * 2400 ml = 360g
360 g x 3.4 kcal/gram = 1224 kcals
Lipids 3 g/100 ml x 2400 ml = 72 glipids
72 x 10 kcals/gram = 720 kcals

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 84/92
Parenteral Nutrition
Evaluation of a PN Order
Amino acids: 4.5 grams/100 ml * 2400ml = 108 grams protein
108 x 4 = 432 kcals
1224 + 720 + 432 = 2376 total kcals Lipid is 30% of total calories
Dextrose is 51.5% of total calories
Protein is 18% of total calories

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 85/92
Monitoring for Complications
Malnourished patients at risk for refeedingsyndrome should have serum phosphorus,magnesium, potassium, and glucose levelsmonitored closely at initiation of SNS. (B)
In patients with diabetes or risk factors forglucose intolerance, SNS should be initiatedwith a low dextrose infusion rate and bloodand urine glucose monitored closely. (C)
Blood glucose should be monitored
frequently upon initiation of SNS, upon anychange in insulin dose, and untilmeasurements are stable. (B)
ASPEN BOD. Guidelines for the use of enteral and parenteral nutrition in adult and pediatric
patients. JPEN 26;41SA, 2002
ASPEN BOD. Guidelines for the use of enteral and parenteral nutrition in adult andpediatric patients. JPEN 26;41SA, 2002

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 86/92
Parenteral Nutrition
Serum electrolytes (sodium, potassium,chloride, and bicarbonate) should bemonitored frequently upon initiation of SNSuntil measurements are stable. (B)
Patients receiving intravenous fat emulsionsshould have serum triglyceride levelsmonitored until stable and when changes aremade in the amount of fat administered. (C)
Liver function tests should be monitoredperiodically in patients receiving PN. (A)

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 87/92
Parenteral Nutrition
Acute Inpatient PN Monitoring
Parameter Daily
Frequency
3x/week Weekly
Glucose Initially ¥
Electrolytes Initially ¥
Phos, Mg,BUN, Cr, Ca
Initially ¥
TG ¥
Fluid/Is & Os ¥
Temperature ¥
Adapted from K&M, p. 549

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 88/92
Parenteral Nutrition
Inpatient Monitoring PN
Parameter Daily
Frequency
Weekly PRN
Body Weight Initially ¥
Nitrogen Balance Initially ¥
HGB, HCT ¥
Catheter Site ¥ Lymphocyte Count ¥ ¥
Clinical Status

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 89/92
Parenteral Nutrition
TRANSITIONAL FEEDING ANDDISCONTINUATION:
GIT-Functional?
Reduction in PN can be made as enteral ororal feedings are increased.
clumping of trig particles with the emulsion
ASPEN BOD. Guidelines for the use of enteral and parenteral nutrition in adult andpediatric patients. JPEN 26;41SA, 2002

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 90/92
Parenteral Nutrition
Maintain full PN support until pt is tolerating1/3 of needs via enteral route
Decrease TPN by 50% and continue to taperas the enteral feeding is advanced to total
TPN can reduce appetite if >25% of calorieneeds are met via PN TPN can be tapered when pt is consuming
greater than 500 calories/d and d-c¶d whenmeeting 60% of goal
TPN can be rapidly d-c¶d if pt is receivingenteral feeding in amount great enough tomaintain blood glucose levels

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 91/92
Parenteral Nutrition
Cessation of TPN
Rebound hypoglycemia is a potentialcomplication
Decrease the volume by 50% for 1-2 hoursbefore discontinuing the solution to minimizerisk
PPN can be stopped without concern for
hypoglycemia

8/3/2019 Lecture on en and PN
http://slidepdf.com/reader/full/lecture-on-en-and-pn 92/92
DIANE MENDOZA, RNDgRaciAs!





























