Embed Size (px)
Citation preview
Lecture 15-18 Anemia in CKD Cho
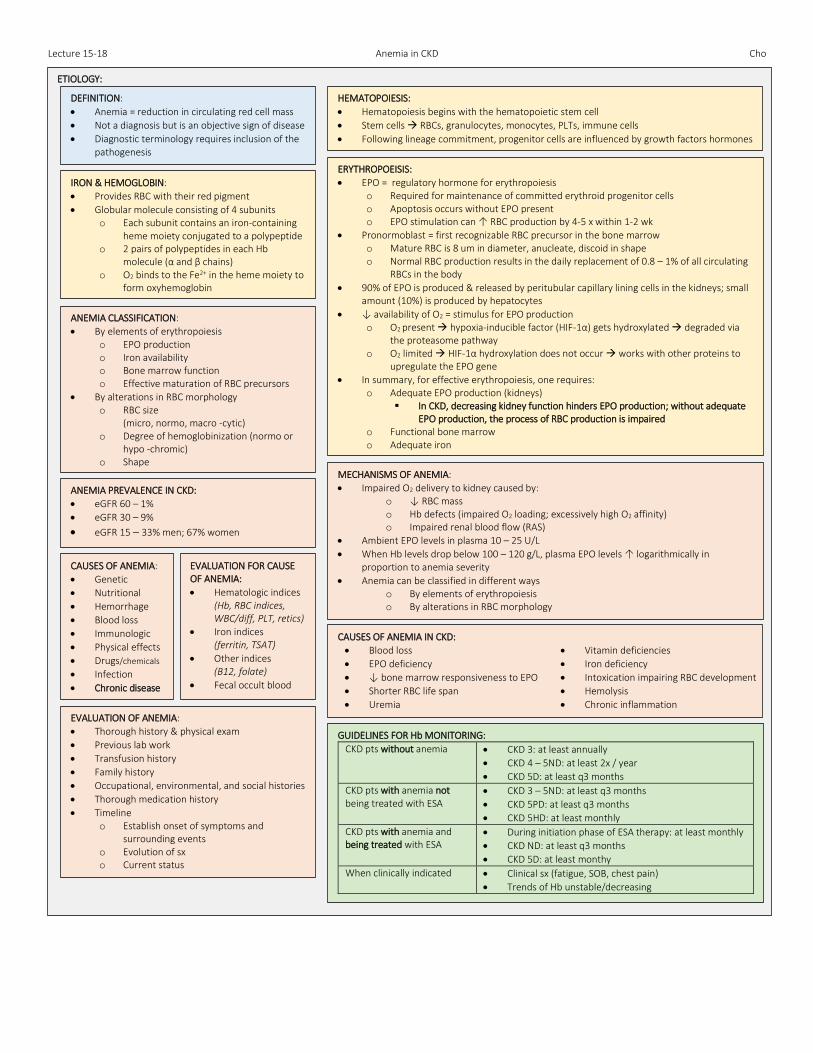
ETIOLOGY:
DEFINITION:
Anemia = reduction in circulating red cell mass
Not a diagnosis but is an objective sign of disease
Diagnostic terminology requires inclusion of the pathogenesis
HEMATOPOIESIS:
Hematopoiesis begins with the hematopoietic stem cell
Stem cells RBCs, granulocytes, monocytes, PLTs, immune cells
Following lineage commitment, progenitor cells are influenced by growth factors hormones
ERYTHROPOEISIS:
EPO = regulatory hormone for erythropoiesis o Required for maintenance of committed erythroid progenitor cells o Apoptosis occurs without EPO present o EPO stimulation can ↑ RBC production by 4-5 x within 1-2 wk
Pronormoblast = first recognizable RBC precursor in the bone marrow o Mature RBC is 8 um in diameter, anucleate, discoid in shape o Normal RBC production results in the daily replacement of 0.8 – 1% of all circulating
RBCs in the body
90% of EPO is produced & released by peritubular capillary lining cells in the kidneys; small amount (10%) is produced by hepatocytes
↓ availability of O2 = stimulus for EPO production o O2 present hypoxia-inducible factor (HIF-1α) gets hydroxylated degraded via
the proteasome pathway o O2 limited HIF-1α hydroxylation does not occur works with other proteins to
upregulate the EPO gene
In summary, for effective erythropoiesis, one requires: o Adequate EPO production (kidneys)
In CKD, decreasing kidney function hinders EPO production; without adequate EPO production, the process of RBC production is impaired
o Functional bone marrow o Adequate iron
IRON & HEMOGLOBIN:
Provides RBC with their red pigment
Globular molecule consisting of 4 subunits o Each subunit contains an iron-containing
heme moiety conjugated to a polypeptide o 2 pairs of polypeptides in each Hb
molecule (α and β chains) o O2 binds to the Fe2+ in the heme moiety to
form oxyhemoglobin
MECHANISMS OF ANEMIA:
Impaired O2 delivery to kidney caused by: o ↓ RBC mass o Hb defects (impaired O2 loading; excessively high O2 affinity) o Impaired renal blood flow (RAS)
Ambient EPO levels in plasma 10 – 25 U/L
When Hb levels drop below 100 – 120 g/L, plasma EPO levels ↑ logarithmically in proportion to anemia severity
Anemia can be classified in different ways o By elements of erythropoiesis o By alterations in RBC morphology
ANEMIA CLASSIFICATION:
By elements of erythropoiesis o EPO production o Iron availability o Bone marrow function o Effective maturation of RBC precursors
By alterations in RBC morphology o RBC size
(micro, normo, macro -cytic) o Degree of hemoglobinization (normo or
hypo -chromic) o Shape
ANEMIA PREVALENCE IN CKD:
eGFR 60 – 1%
eGFR 30 – 9%
eGFR 15 – 33% men; 67% women
CAUSES OF ANEMIA IN CKD:
Blood loss
EPO deficiency
↓ bone marrow responsiveness to EPO
Shorter RBC life span
Uremia
Vitamin deficiencies
Iron deficiency
Intoxication impairing RBC development
Hemolysis
Chronic inflammation EVALUATION OF ANEMIA:
Thorough history & physical exam
Previous lab work
Transfusion history
Family history
Occupational, environmental, and social histories
Thorough medication history
Timeline o Establish onset of symptoms and
surrounding events o Evolution of sx o Current status
EVALUATION FOR CAUSE OF ANEMIA:
Hematologic indices (Hb, RBC indices, WBC/diff, PLT, retics)
Iron indices (ferritin, TSAT)
Other indices (B12, folate)
Fecal occult blood
CAUSES OF ANEMIA:
Genetic
Nutritional
Hemorrhage
Blood loss
Immunologic
Physical effects
Drugs/chemicals
Infection
Chronic disease
GUIDELINES FOR Hb MONITORING:
CKD pts without anemia CKD 3: at least annually
CKD 4 – 5ND: at least 2x / year
CKD 5D: at least q3 months
CKD pts with anemia not being treated with ESA
CKD 3 – 5ND: at least q3 months
CKD 5PD: at least q3 months
CKD 5HD: at least monthly
CKD pts with anemia and being treated with ESA
During initiation phase of ESA therapy: at least monthly
CKD ND: at least q3 months
CKD 5D: at least monthy
When clinically indicated Clinical sx (fatigue, SOB, chest pain)
Trends of Hb unstable/decreasing
Lecture 15-18 Anemia in CKD Cho
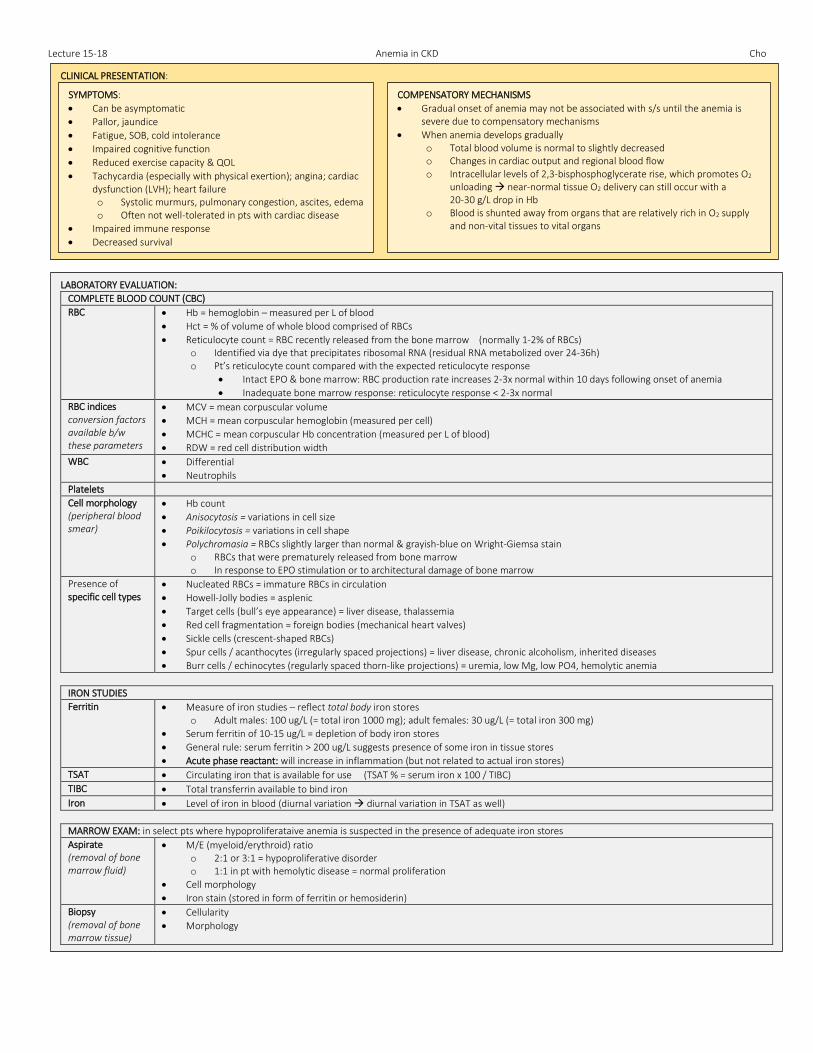
CLINICAL PRESENTATION:
SYMPTOMS:
Can be asymptomatic
Pallor, jaundice
Fatigue, SOB, cold intolerance
Impaired cognitive function
Reduced exercise capacity & QOL
Tachycardia (especially with physical exertion); angina; cardiac dysfunction (LVH); heart failure o Systolic murmurs, pulmonary congestion, ascites, edema o Often not well-tolerated in pts with cardiac disease
Impaired immune response
Decreased survival
COMPENSATORY MECHANISMS
Gradual onset of anemia may not be associated with s/s until the anemia is severe due to compensatory mechanisms
When anemia develops gradually o Total blood volume is normal to slightly decreased o Changes in cardiac output and regional blood flow o Intracellular levels of 2,3-bisphosphoglycerate rise, which promotes O2
unloading near-normal tissue O2 delivery can still occur with a 20-30 g/L drop in Hb
o Blood is shunted away from organs that are relatively rich in O2 supply and non-vital tissues to vital organs
LABORATORY EVALUATION:
COMPLETE BLOOD COUNT (CBC)
RBC Hb = hemoglobin – measured per L of blood
Hct = % of volume of whole blood comprised of RBCs
Reticulocyte count = RBC recently released from the bone marrow (normally 1-2% of RBCs) o Identified via dye that precipitates ribosomal RNA (residual RNA metabolized over 24-36h) o Pt’s reticulocyte count compared with the expected reticulocyte response
Intact EPO & bone marrow: RBC production rate increases 2-3x normal within 10 days following onset of anemia
Inadequate bone marrow response: reticulocyte response < 2-3x normal
RBC indices conversion factors available b/w these parameters
MCV = mean corpuscular volume
MCH = mean corpuscular hemoglobin (measured per cell)
MCHC = mean corpuscular Hb concentration (measured per L of blood)
RDW = red cell distribution width
WBC Differential
Neutrophils
Platelets
Cell morphology (peripheral blood smear)
Hb count
Anisocytosis = variations in cell size
Poikilocytosis = variations in cell shape
Polychromasia = RBCs slightly larger than normal & grayish-blue on Wright-Giemsa stain o RBCs that were prematurely released from bone marrow o In response to EPO stimulation or to architectural damage of bone marrow
Presence of specific cell types
Nucleated RBCs = immature RBCs in circulation
Howell-Jolly bodies = asplenic
Target cells (bull’s eye appearance) = liver disease, thalassemia
Red cell fragmentation = foreign bodies (mechanical heart valves)
Sickle cells (crescent-shaped RBCs)
Spur cells / acanthocytes (irregularly spaced projections) = liver disease, chronic alcoholism, inherited diseases
Burr cells / echinocytes (regularly spaced thorn-like projections) = uremia, low Mg, low PO4, hemolytic anemia
IRON STUDIES
Ferritin Measure of iron studies – reflect total body iron stores o Adult males: 100 ug/L (= total iron 1000 mg); adult females: 30 ug/L (= total iron 300 mg)
Serum ferritin of 10-15 ug/L = depletion of body iron stores
General rule: serum ferritin > 200 ug/L suggests presence of some iron in tissue stores
Acute phase reactant: will increase in inflammation (but not related to actual iron stores)
TSAT Circulating iron that is available for use (TSAT % = serum iron x 100 / TIBC)
TIBC Total transferrin available to bind iron
Iron Level of iron in blood (diurnal variation diurnal variation in TSAT as well)
MARROW EXAM: in select pts where hypoproliferataive anemia is suspected in the presence of adequate iron stores
Aspirate (removal of bone marrow fluid)
M/E (myeloid/erythroid) ratio o 2:1 or 3:1 = hypoproliferative disorder o 1:1 in pt with hemolytic disease = normal proliferation
Cell morphology
Iron stain (stored in form of ferritin or hemosiderin)
Biopsy (removal of bone marrow tissue)
Cellularity
Morphology
Lecture 15-18 Anemia in CKD Cho
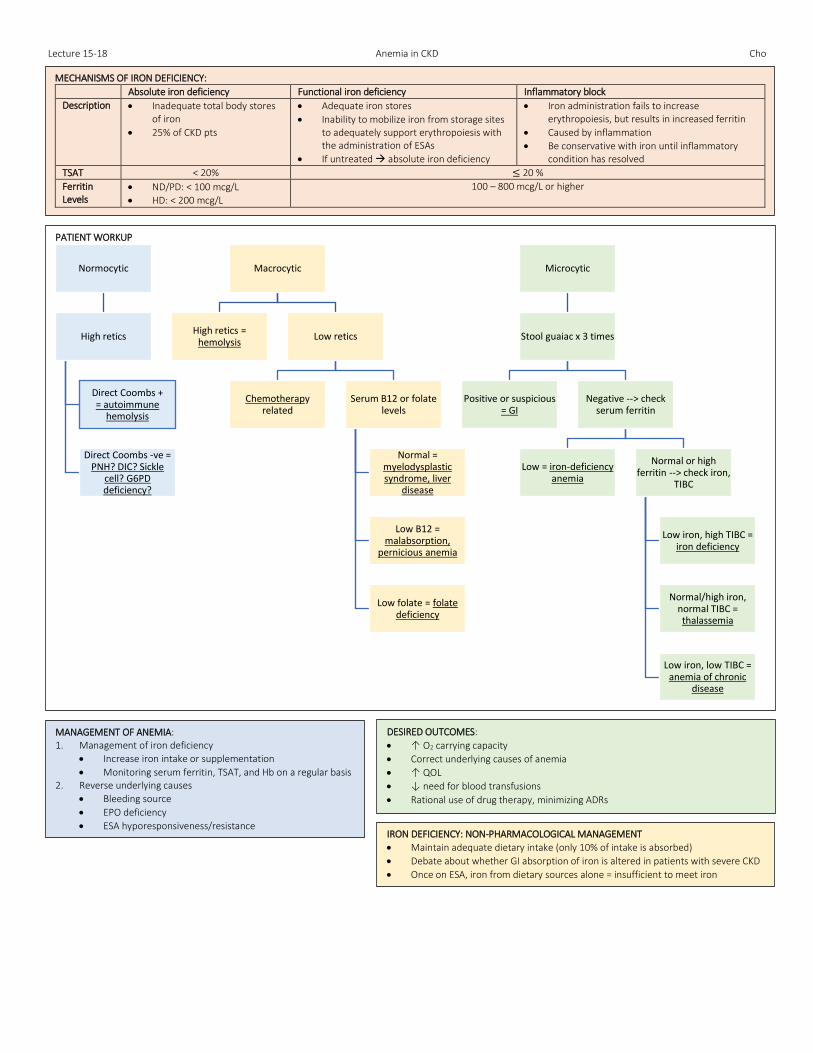
MECHANISMS OF IRON DEFICIENCY:
Absolute iron deficiency Functional iron deficiency Inflammatory block
Description Inadequate total body stores of iron
25% of CKD pts
Adequate iron stores
Inability to mobilize iron from storage sites to adequately support erythropoiesis with the administration of ESAs
If untreated absolute iron deficiency
Iron administration fails to increase erythropoiesis, but results in increased ferritin
Caused by inflammation
Be conservative with iron until inflammatory condition has resolved
TSAT < 20% ≤ 20 %
Ferritin Levels
ND/PD: < 100 mcg/L
HD: < 200 mcg/L
100 – 800 mcg/L or higher
PATIENT WORKUP
Normocytic
High retics
Direct Coombs + = autoimmune
hemolysis
Direct Coombs -ve = PNH? DIC? Sickle
cell? G6PD deficiency?
Macrocytic
High retics = hemolysis
Low retics
Chemotherapy related
Serum B12 or folate levels
Normal = myelodysplastic syndrome, liver
disease
Low B12 = malabsorption,
pernicious anemia
Low folate = folate deficiency
Microcytic
Stool guaiac x 3 times
Positive or suspicious = GI
Negative --> check serum ferritin
Low = iron-deficiency anemia
Normal or high ferritin --> check iron,
TIBC
Low iron, high TIBC = iron deficiency
Normal/high iron, normal TIBC = thalassemia
Low iron, low TIBC = anemia of chronic
disease
IRON DEFICIENCY: NON-PHARMACOLOGICAL MANAGEMENT
Maintain adequate dietary intake (only 10% of intake is absorbed)
Debate about whether GI absorption of iron is altered in patients with severe CKD
Once on ESA, iron from dietary sources alone = insufficient to meet iron requirements
MANAGEMENT OF ANEMIA: 1. Management of iron deficiency
Increase iron intake or supplementation
Monitoring serum ferritin, TSAT, and Hb on a regular basis 2. Reverse underlying causes
Bleeding source
EPO deficiency
ESA hyporesponsiveness/resistance
DESIRED OUTCOMES:
↑ O2 carrying capacity
Correct underlying causes of anemia
↑ QOL
↓ need for blood transfusions
Rational use of drug therapy, minimizing ADRs
Lecture 15-18 Anemia in CKD Cho
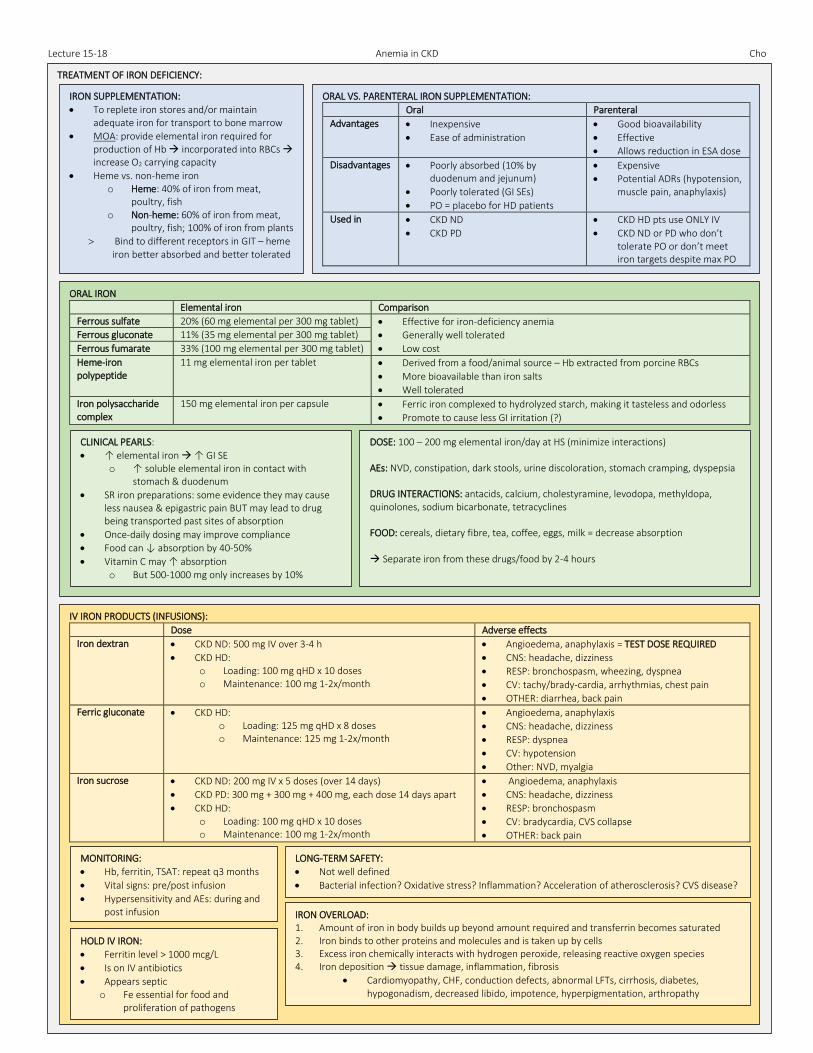
TREATMENT OF IRON DEFICIENCY: IRON SUPPLEMENTATION:
To replete iron stores and/or maintain adequate iron for transport to bone marrow
MOA: provide elemental iron required for production of Hb incorporated into RBCs increase O2 carrying capacity
Heme vs. non-heme iron o Heme: 40% of iron from meat,
poultry, fish o Non-heme: 60% of iron from meat,
poultry, fish; 100% of iron from plants
Bind to different receptors in GIT – heme iron better absorbed and better tolerated
ORAL VS. PARENTERAL IRON SUPPLEMENTATION:
Oral Parenteral
Advantages Inexpensive
Ease of administration
Good bioavailability
Effective
Allows reduction in ESA dose
Disadvantages Poorly absorbed (10% by duodenum and jejunum)
Poorly tolerated (GI SEs)
PO = placebo for HD patients
Expensive
Potential ADRs (hypotension, muscle pain, anaphylaxis)
Used in CKD ND
CKD PD
CKD HD pts use ONLY IV
CKD ND or PD who don’t tolerate PO or don’t meet iron targets despite max PO
ORAL IRON
Elemental iron Comparison
Ferrous sulfate 20% (60 mg elemental per 300 mg tablet) Effective for iron-deficiency anemia
Generally well tolerated
Low cost
Ferrous gluconate 11% (35 mg elemental per 300 mg tablet)
Ferrous fumarate 33% (100 mg elemental per 300 mg tablet)
Heme-iron polypeptide
11 mg elemental iron per tablet Derived from a food/animal source – Hb extracted from porcine RBCs
More bioavailable than iron salts
Well tolerated
Iron polysaccharide complex
150 mg elemental iron per capsule Ferric iron complexed to hydrolyzed starch, making it tasteless and odorless
Promote to cause less GI irritation (?)
CLINICAL PEARLS:
↑ elemental iron ↑ GI SE o ↑ soluble elemental iron in contact with
stomach & duodenum
SR iron preparations: some evidence they may cause less nausea & epigastric pain BUT may lead to drug being transported past sites of absorption
Once-daily dosing may improve compliance
Food can ↓ absorption by 40-50%
Vitamin C may ↑ absorption o But 500-1000 mg only increases by 10%
DOSE: 100 – 200 mg elemental iron/day at HS (minimize interactions) AEs: NVD, constipation, dark stools, urine discoloration, stomach cramping, dyspepsia DRUG INTERACTIONS: antacids, calcium, cholestyramine, levodopa, methyldopa, quinolones, sodium bicarbonate, tetracyclines FOOD: cereals, dietary fibre, tea, coffee, eggs, milk = decrease absorption Separate iron from these drugs/food by 2-4 hours
IV IRON PRODUCTS (INFUSIONS):
Dose Adverse effects
Iron dextran CKD ND: 500 mg IV over 3-4 h
CKD HD: o Loading: 100 mg qHD x 10 doses o Maintenance: 100 mg 1-2x/month
Angioedema, anaphylaxis = TEST DOSE REQUIRED
CNS: headache, dizziness
RESP: bronchospasm, wheezing, dyspnea
CV: tachy/brady-cardia, arrhythmias, chest pain
OTHER: diarrhea, back pain
Ferric gluconate CKD HD: o Loading: 125 mg qHD x 8 doses o Maintenance: 125 mg 1-2x/month
Angioedema, anaphylaxis
CNS: headache, dizziness
RESP: dyspnea
CV: hypotension
Other: NVD, myalgia
Iron sucrose CKD ND: 200 mg IV x 5 doses (over 14 days)
CKD PD: 300 mg + 300 mg + 400 mg, each dose 14 days apart
CKD HD: o Loading: 100 mg qHD x 10 doses o Maintenance: 100 mg 1-2x/month
Angioedema, anaphylaxis
CNS: headache, dizziness
RESP: bronchospasm
CV: bradycardia, CVS collapse
OTHER: back pain
MONITORING:
Hb, ferritin, TSAT: repeat q3 months
Vital signs: pre/post infusion
Hypersensitivity and AEs: during and post infusion
LONG-TERM SAFETY:
Not well defined
Bacterial infection? Oxidative stress? Inflammation? Acceleration of atherosclerosis? CVS disease?
HOLD IV IRON:
Ferritin level > 1000 mcg/L
Is on IV antibiotics
Appears septic o Fe essential for food and
proliferation of pathogens
IRON OVERLOAD: 1. Amount of iron in body builds up beyond amount required and transferrin becomes saturated 2. Iron binds to other proteins and molecules and is taken up by cells 3. Excess iron chemically interacts with hydrogen peroxide, releasing reactive oxygen species 4. Iron deposition tissue damage, inflammation, fibrosis
Cardiomyopathy, CHF, conduction defects, abnormal LFTs, cirrhosis, diabetes, hypogonadism, decreased libido, impotence, hyperpigmentation, arthropathy
Lecture 15-18 Anemia in CKD Cho
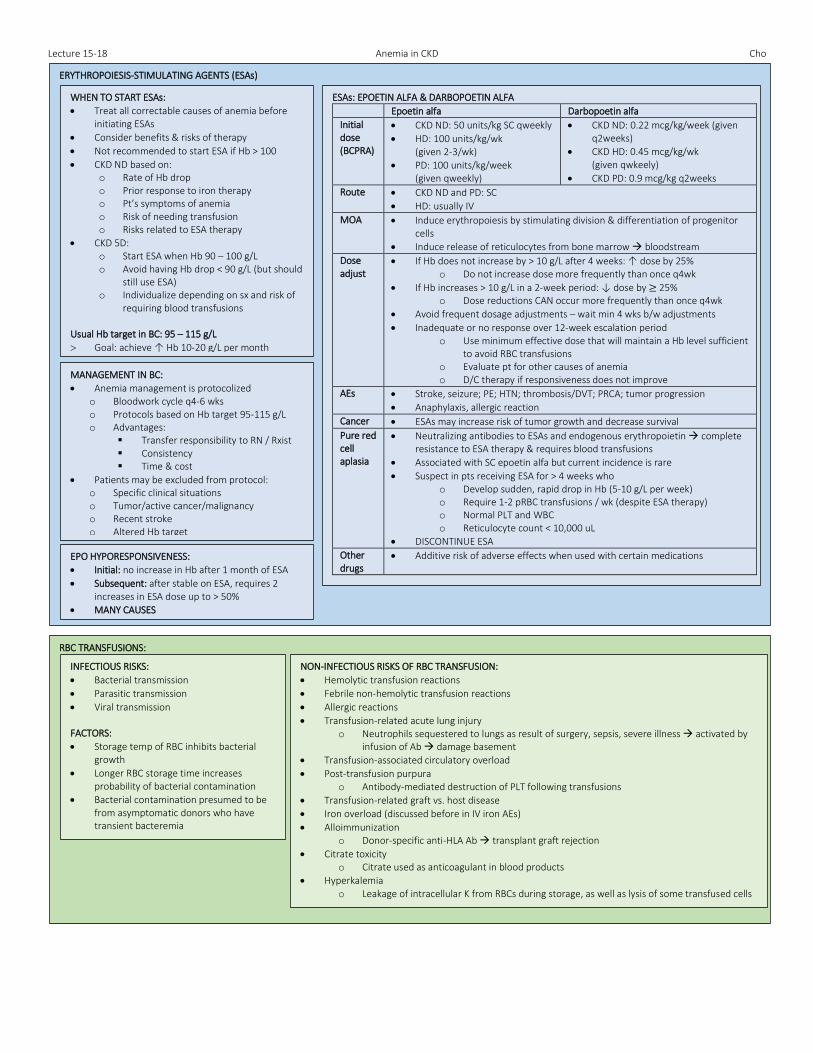
ERYTHROPOIESIS-STIMULATING AGENTS (ESAs)
WHEN TO START ESAs:
Treat all correctable causes of anemia before initiating ESAs
Consider benefits & risks of therapy
Not recommended to start ESA if Hb > 100
CKD ND based on: o Rate of Hb drop o Prior response to iron therapy o Pt’s symptoms of anemia o Risk of needing transfusion o Risks related to ESA therapy
CKD 5D: o Start ESA when Hb 90 – 100 g/L o Avoid having Hb drop < 90 g/L (but should
still use ESA) o Individualize depending on sx and risk of
requiring blood transfusions
Usual Hb target in BC: 95 – 115 g/L
Goal: achieve ↑ Hb 10-20 g/L per month
ESAs: EPOETIN ALFA & DARBOPOETIN ALFA
Epoetin alfa Darbopoetin alfa
Initial dose (BCPRA)
CKD ND: 50 units/kg SC qweekly
HD: 100 units/kg/wk (given 2-3/wk)
PD: 100 units/kg/week (given qweekly)
CKD ND: 0.22 mcg/kg/week (given q2weeks)
CKD HD: 0.45 mcg/kg/wk (given qwkeely)
CKD PD: 0.9 mcg/kg q2weeks
Route CKD ND and PD: SC
HD: usually IV
MOA Induce erythropoiesis by stimulating division & differentiation of progenitor cells
Induce release of reticulocytes from bone marrow bloodstream
Dose adjust
If Hb does not increase by > 10 g/L after 4 weeks: ↑ dose by 25% o Do not increase dose more frequently than once q4wk
If Hb increases > 10 g/L in a 2-week period: ↓ dose by ≥ 25% o Dose reductions CAN occur more frequently than once q4wk
Avoid frequent dosage adjustments – wait min 4 wks b/w adjustments
Inadequate or no response over 12-week escalation period o Use minimum effective dose that will maintain a Hb level sufficient
to avoid RBC transfusions o Evaluate pt for other causes of anemia o D/C therapy if responsiveness does not improve
AEs Stroke, seizure; PE; HTN; thrombosis/DVT; PRCA; tumor progression
Anaphylaxis, allergic reaction
Cancer ESAs may increase risk of tumor growth and decrease survival
Pure red cell aplasia
Neutralizing antibodies to ESAs and endogenous erythropoietin complete resistance to ESA therapy & requires blood transfusions
Associated with SC epoetin alfa but current incidence is rare
Suspect in pts receiving ESA for > 4 weeks who o Develop sudden, rapid drop in Hb (5-10 g/L per week) o Require 1-2 pRBC transfusions / wk (despite ESA therapy) o Normal PLT and WBC o Reticulocyte count < 10,000 uL
DISCONTINUE ESA
Other drugs
Additive risk of adverse effects when used with certain medications
MANAGEMENT IN BC:
Anemia management is protocolized o Bloodwork cycle q4-6 wks o Protocols based on Hb target 95-115 g/L o Advantages:
Transfer responsibility to RN / Rxist Consistency Time & cost
Patients may be excluded from protocol: o Specific clinical situations o Tumor/active cancer/malignancy o Recent stroke o Altered Hb target
EPO HYPORESPONSIVENESS:
Initial: no increase in Hb after 1 month of ESA
Subsequent: after stable on ESA, requires 2 increases in ESA dose up to > 50%
MANY CAUSES
RBC TRANSFUSIONS:
INFECTIOUS RISKS:
Bacterial transmission
Parasitic transmission
Viral transmission FACTORS:
Storage temp of RBC inhibits bacterial growth
Longer RBC storage time increases probability of bacterial contamination
Bacterial contamination presumed to be from asymptomatic donors who have transient bacteremia
NON-INFECTIOUS RISKS OF RBC TRANSFUSION:
Hemolytic transfusion reactions
Febrile non-hemolytic transfusion reactions
Allergic reactions
Transfusion-related acute lung injury o Neutrophils sequestered to lungs as result of surgery, sepsis, severe illness activated by
infusion of Ab damage basement
Transfusion-associated circulatory overload
Post-transfusion purpura o Antibody-mediated destruction of PLT following transfusions
Transfusion-related graft vs. host disease
Iron overload (discussed before in IV iron AEs)
Alloimmunization o Donor-specific anti-HLA Ab transplant graft rejection
Citrate toxicity o Citrate used as anticoagulant in blood products
Hyperkalemia o Leakage of intracellular K from RBCs during storage, as well as lysis of some transfused cells