Embed Size (px)
Citation preview
Lawrence J. Hirsch, MDProfessor of Clinical Neurology
Director of Clinical NeurophysiologyNeurological InstituteColumbia UniversityNew York, New York
ICUEEG Monitoring: When and Why
Disclosures
Name of Commercial Interest Type of Financial RelationshipCortiCare Advisory boardEisai Research fundingGlaxoSmithKline Speakers bureau
HonorariaLundbeck Speakers bureau
Advisory boardHonoraria
Research fundingPfizer Inc Research fundingUCB –Pharma Speakers bureau
HonorariaResearch funding
Why Do cVEEG in ICUs?
• To detect seizures– Usually nonconvulsive in ICUs
• To define nature of spells, including autonomic• To quantify seizures• To detect hypoxia / ischemia and other brain
events• Prognostication• Other
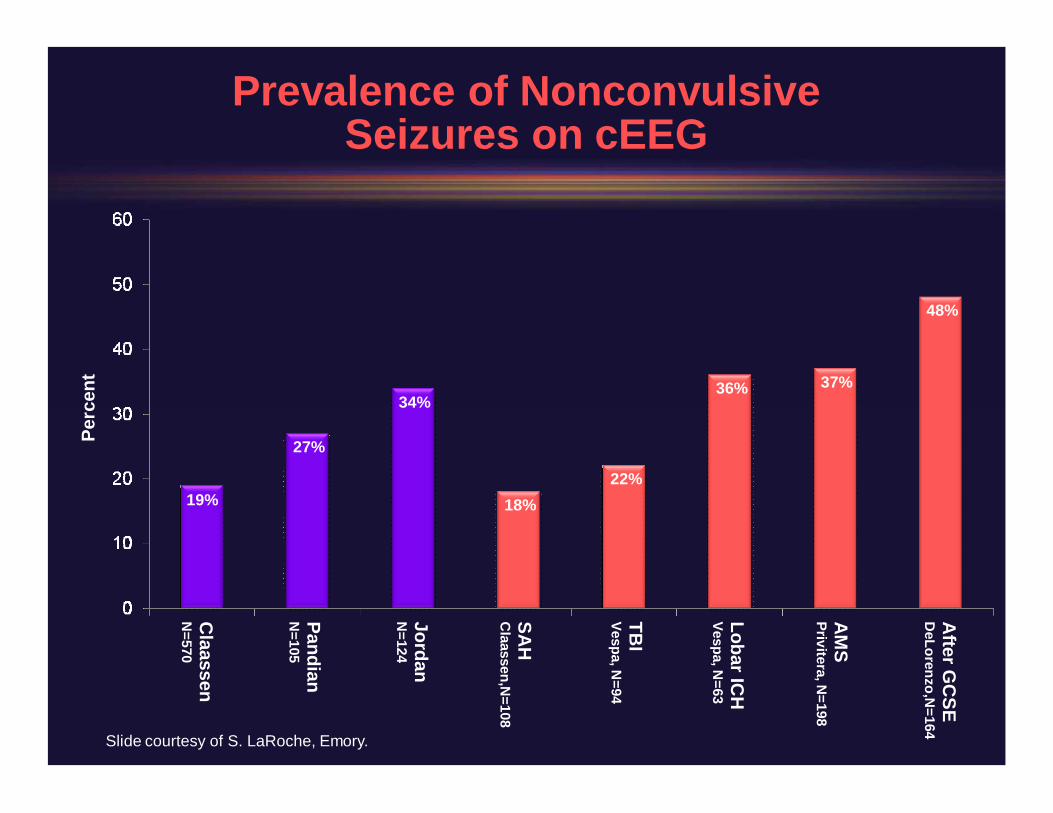
Prevalence of NonconvulsiveSeizures on cEEG
Perc
ent
Claassen
N=570
PandianN
=105
JordanN
=124
19%
27%
34%
SAH
Claassen,N
=108
TBI
Vespa, N=94
AM
SPrivitera, N
=198
Lobar ICH
Vespa, N=63
After G
CSE
DeLorenzo,N
=164
18%22%
36% 37%
48%
Slide courtesy of S. LaRoche, Emory.
Risk Factors for NonconvulsiveSeizures and NCSE
• Husain et al. JNNP. 2003– Severely impaired mental status– Oculomotor abnormalities§ Nystagmus§ Sustained eye deviation§ Hippus
– Remote risk factors for epilepsy
• Claassen et al. Neurology. 2004: 570 consecutivepatients undergoing cEEG monitoring– 110 (19%) with seizures
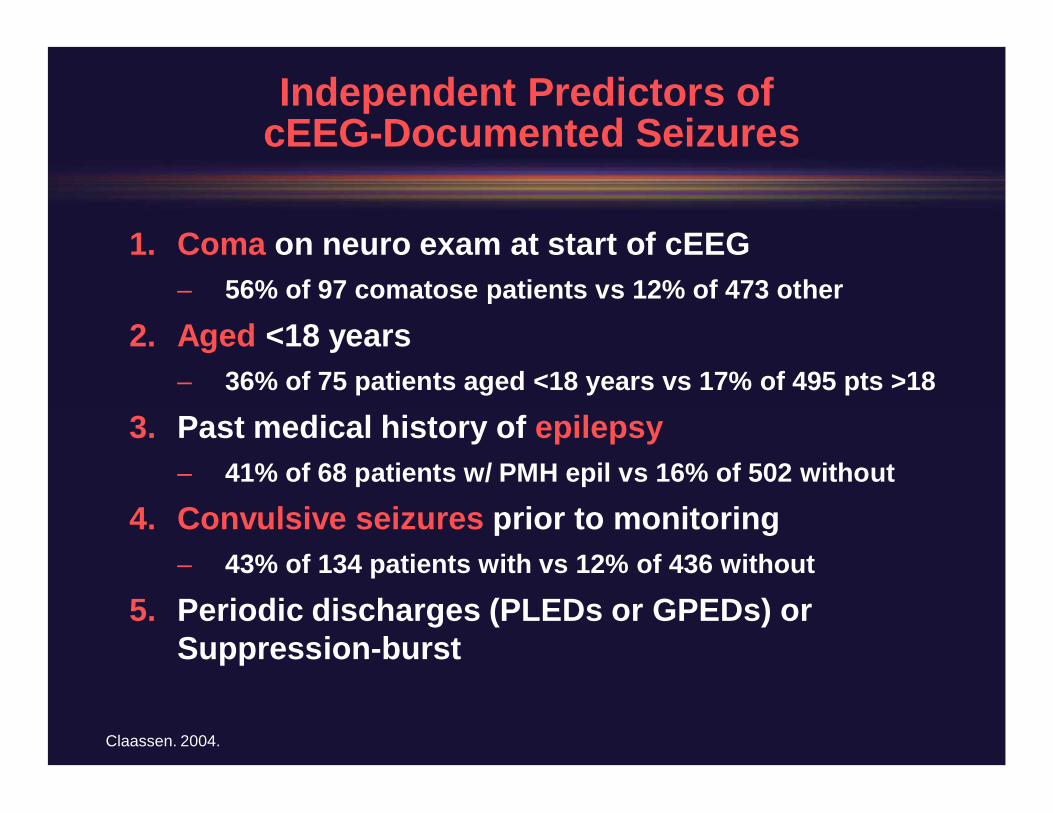
Independent Predictors ofcEEGDocumented Seizures
1. Coma on neuro exam at start of cEEG– 56% of 97 comatose patients vs 12% of 473 other
2. Aged <18 years– 36% of 75 patients aged <18 years vs 17% of 495 pts >18
3. Past medical history of epilepsy– 41% of 68 patients w/ PMH epil vs 16% of 502 without
4. Convulsive seizures prior to monitoring– 43% of 134 patients with vs 12% of 436 without
5. Periodic discharges (PLEDs or GPEDs) orSuppressionburst
Claassen. 2004.
Most patients (101/110) hadexclusively nonconvulsive seizures

Sample video cases from 2 consecutive days ofCEEG
47, possible encephalitis, coma
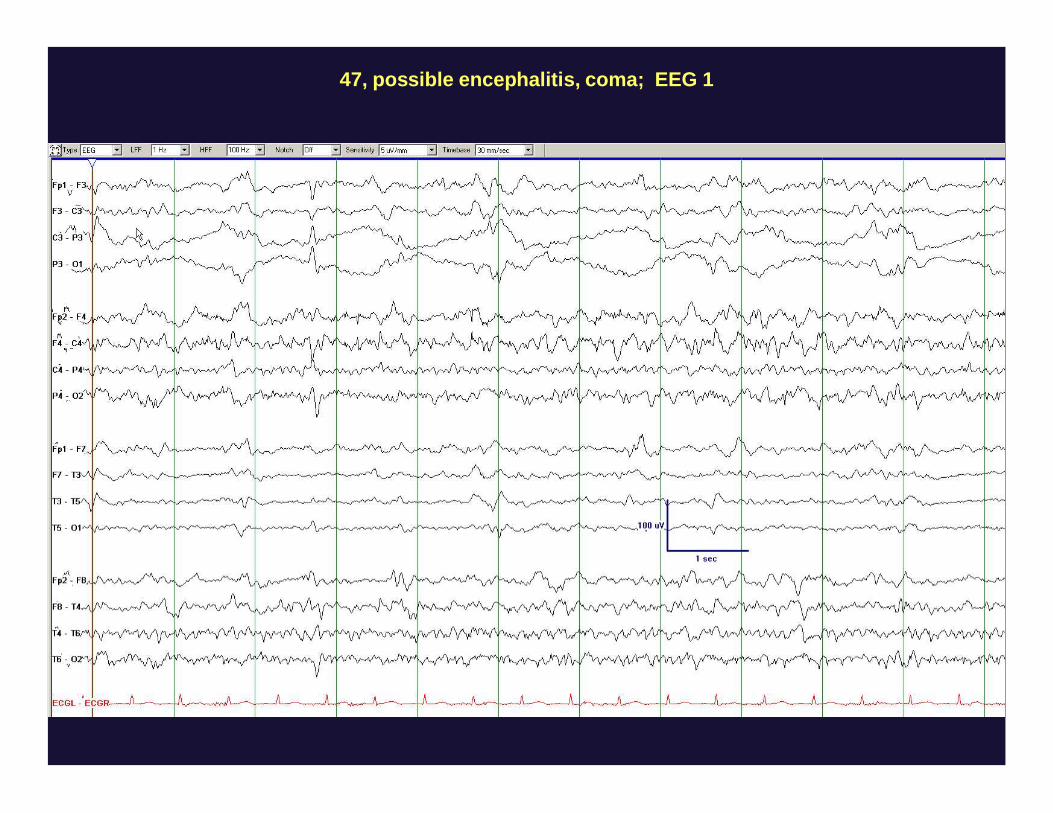
47, possible encephalitis, coma; EEG 1
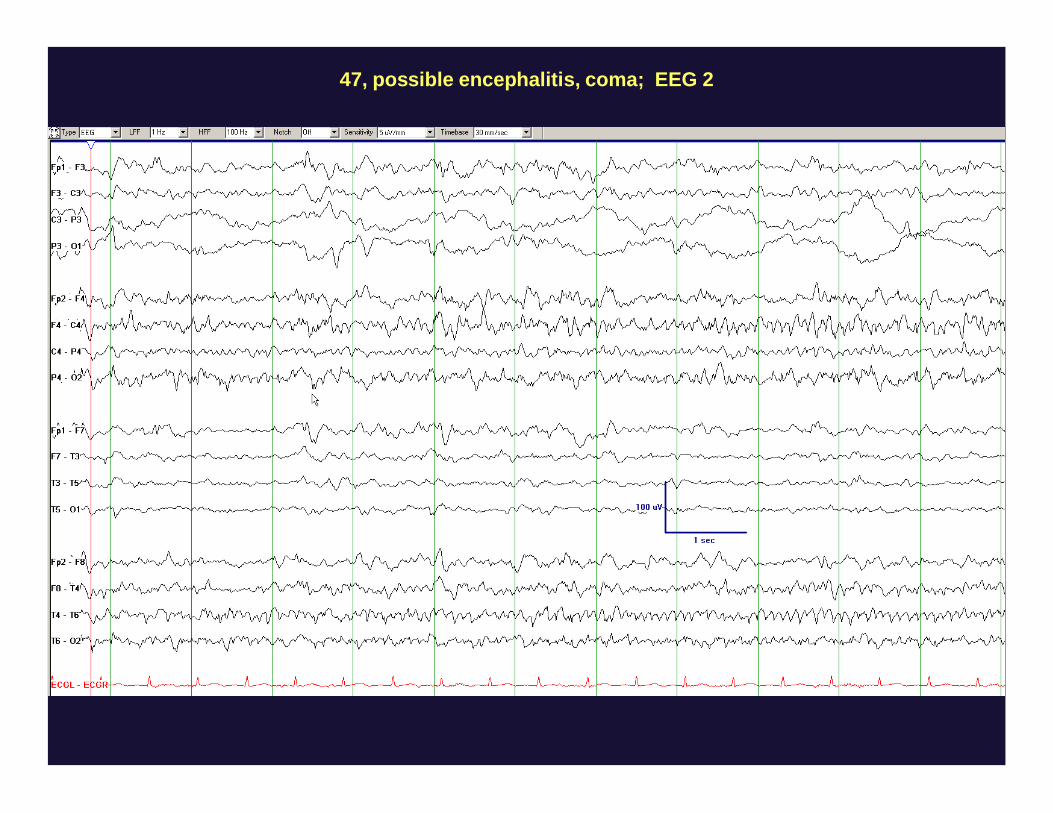
47, possible encephalitis, coma; EEG 2
83, grade I SAH and aneurysm clipping. No clinical seizures. “Because of persistent alteredmental status and difficulty speaking, cEEG was started”
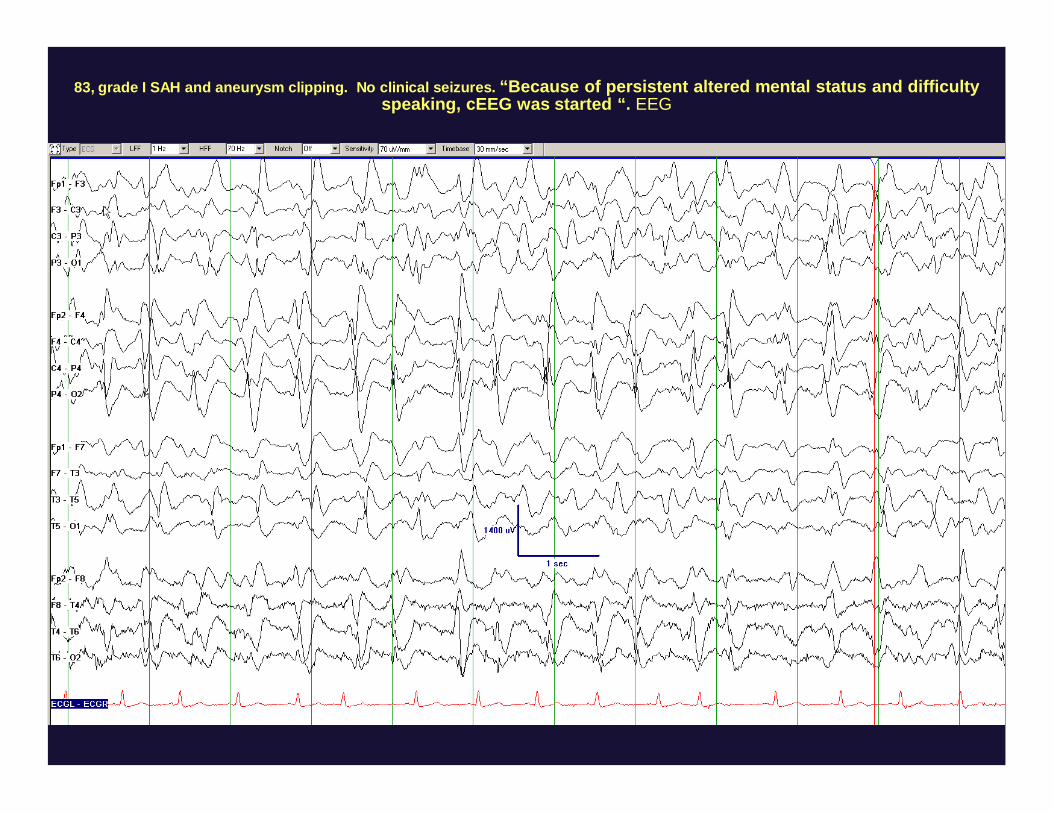
83, grade I SAH and aneurysm clipping. No clinical seizures. “Because of persistent altered mental status and difficultyspeaking, cEEG was started “. EEG
73, astrocytomaresection, csf leak,
meningitis, rare clinicalseizures
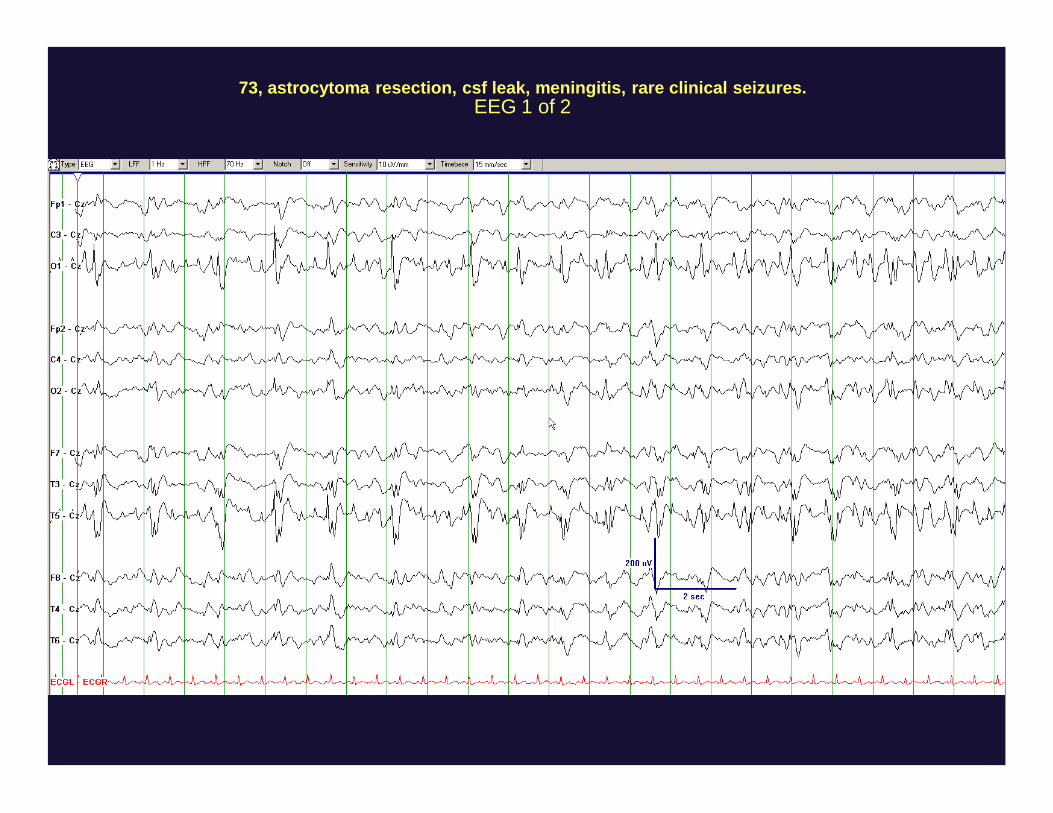
73, astrocytoma resection, csf leak, meningitis, rare clinical seizures.EEG 1 of 2
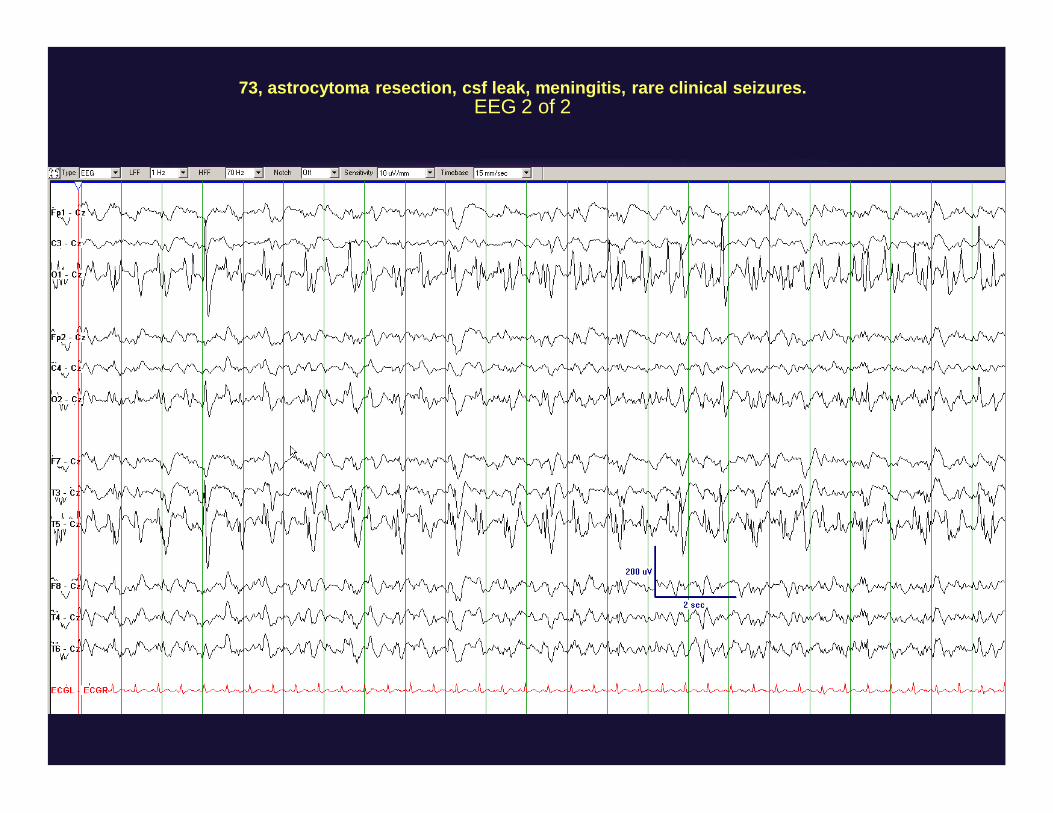
73, astrocytoma resection, csf leak, meningitis, rare clinical seizures.EEG 2 of 2
29, amyloidosis, prior encephalitis and epilepsy, multiple medical probs, now with fever,pneumonia, decreased mental status, no recent clinical seizures
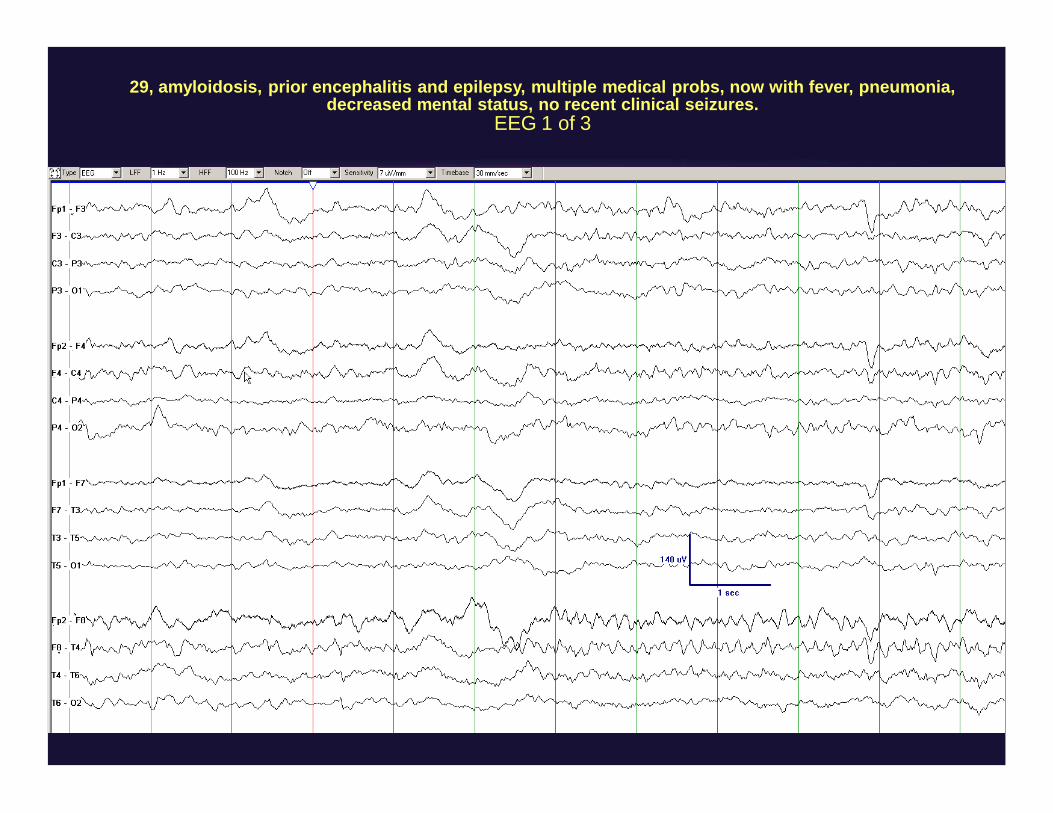
29, amyloidosis, prior encephalitis and epilepsy, multiple medical probs, now with fever, pneumonia,decreased mental status, no recent clinical seizures.
EEG 1 of 3
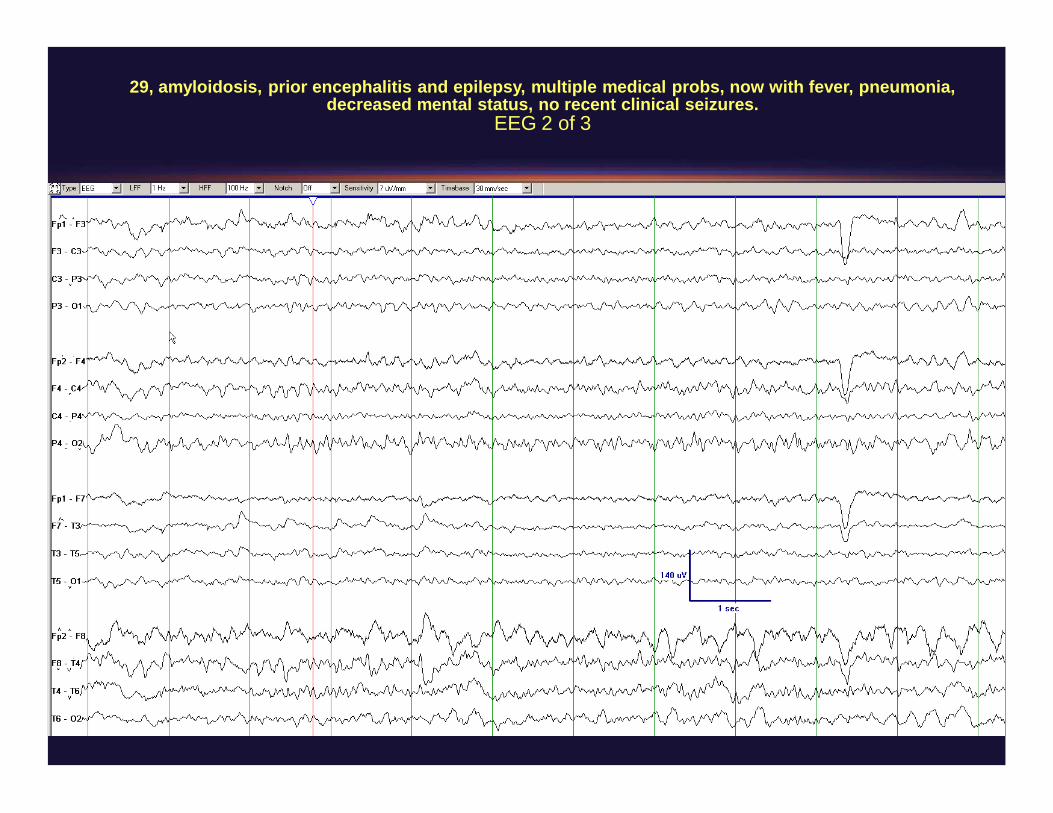
29, amyloidosis, prior encephalitis and epilepsy, multiple medical probs, now with fever, pneumonia,decreased mental status, no recent clinical seizures.
EEG 2 of 3
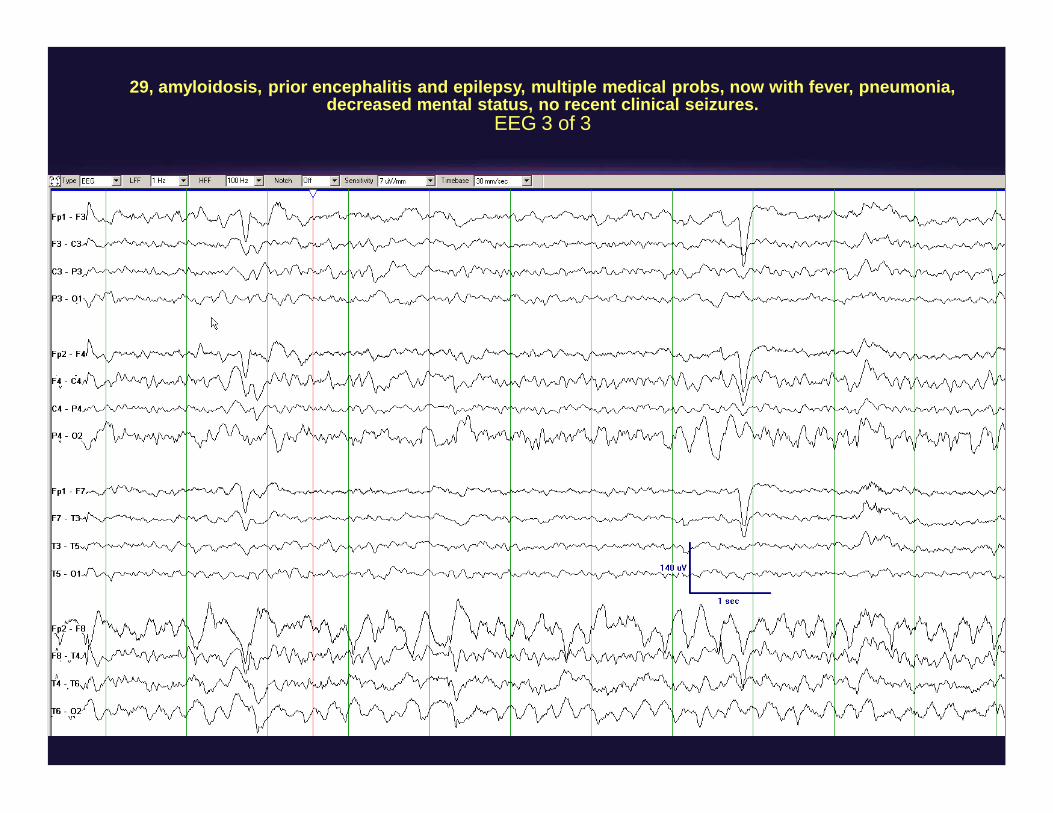
29, amyloidosis, prior encephalitis and epilepsy, multiple medical probs, now with fever, pneumonia,decreased mental status, no recent clinical seizures.
EEG 3 of 3
“25 month old F with developmental delay, intractable epilepsy, admittedfor increased seizure frequency. Pt now lethargic, most likely from Ativangiven in ED”
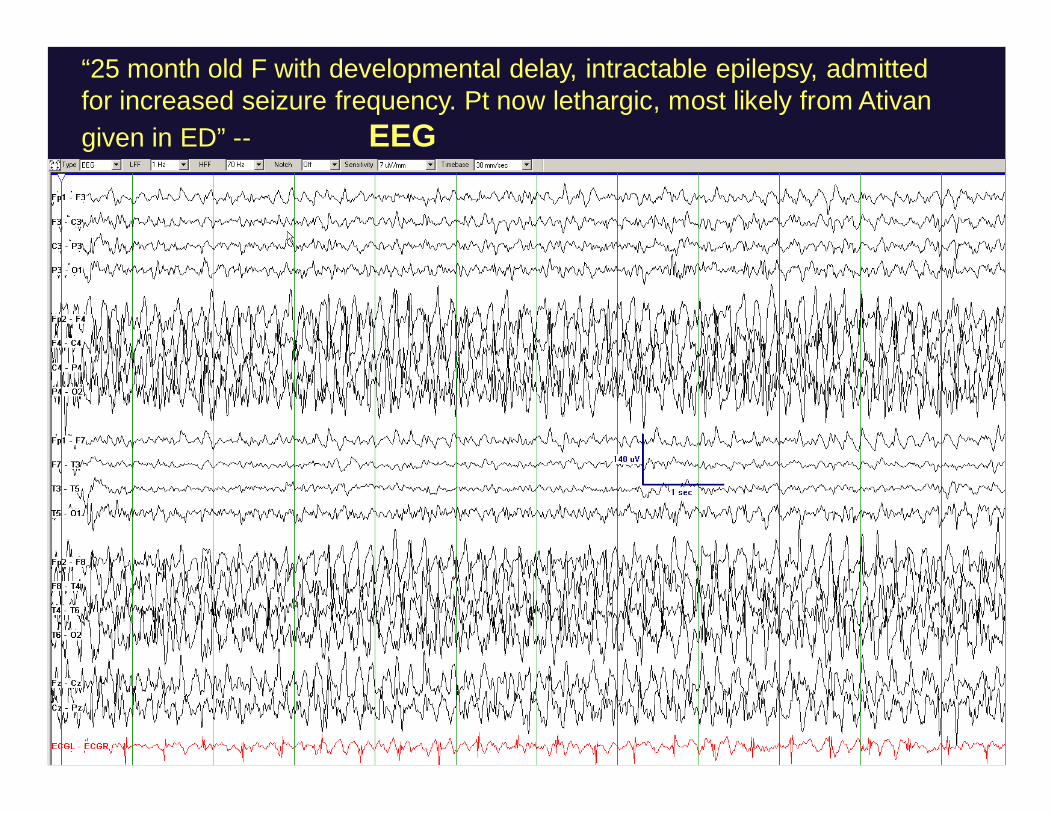
“25 month old F with developmental delay, intractable epilepsy, admittedfor increased seizure frequency. Pt now lethargic, most likely from Ativangiven in ED” EEG
Digital VideoEEG Monitoring in theNeurologicalNeurosurg ICU
Pandian AJD, Cascino GD, So EL, Manno E, Fulgham JRArch Neurol. July 2004.
• 105 patients• All patients had routine EEG for at least 30 min at
start of study• Mean duration of DVEEG: 2.9 days
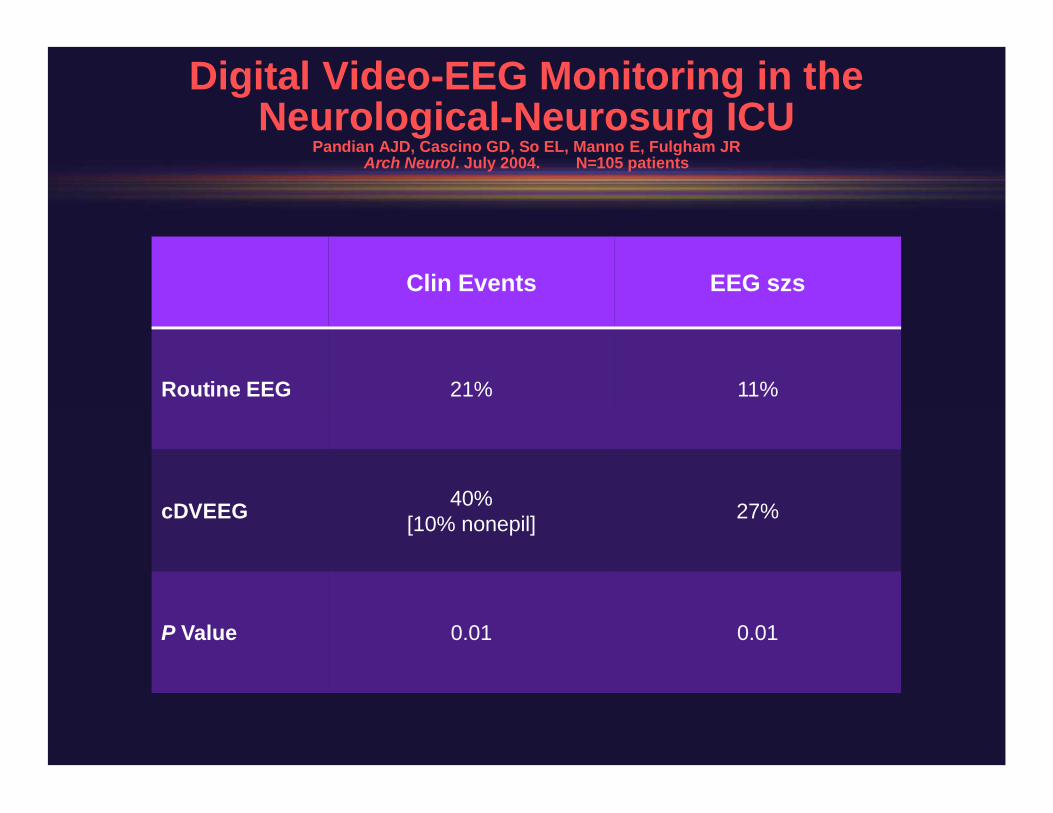
Digital VideoEEG Monitoring in theNeurologicalNeurosurg ICU
Pandian AJD, Cascino GD, So EL, Manno E, Fulgham JRArch Neurol. July 2004. N=105 patients
Clin Events EEG szs
Routine EEG 21% 11%
cDVEEG 40%[10% nonepil] 27%
P Value 0.01 0.01
Clinical TakeHome Messages
• The majority of seizures in ICU patients arenonconvulsive (92% in Claassen et al. 2004)
• NEED EEG after convulsive status epilepticus if thepatient does not wake up
• Need EEG in unexplained coma (and in many casesof explained coma)
Why do we care aboutnonconvulsive seizures?
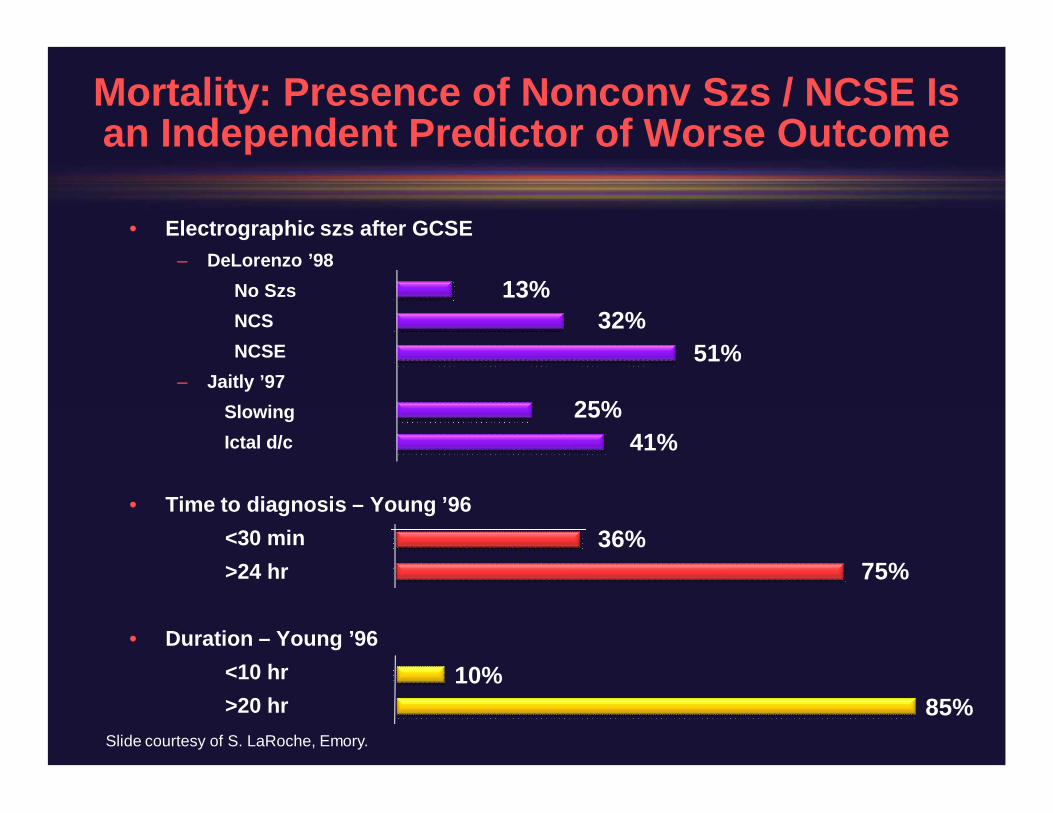
Mortality: Presence of Nonconv Szs / NCSE Isan Independent Predictor of Worse Outcome
• Electrographic szs after GCSE– DeLorenzo ’98
No SzsNCSNCSE
– Jaitly ’97SlowingIctal d/c
• Time to diagnosis –Young ’96<30 min>24 hr
• Duration –Young ’96<10 hr>20 hr
51%32%
13%
41%25%
75%36%
Slide courtesy of S. LaRoche, Emory.
10%85%
Evidence That Seizures, IncludingNonconvulsive Ones, Are Causing Further Harm
(cont)
• Rare cases of prolonged nonconvulsive seizureswithout acute brain injury and permanent CNSinjury / worsening (Krumholz 1995)– >36 hours
• NCszs alone can cause elevated NSE. Highest NSEis in those with acute brain injury + subtle szs;(DiGiorgio ’95 + ’99)– From animal studies: NSE correlates w/ szrelated
histologic damage
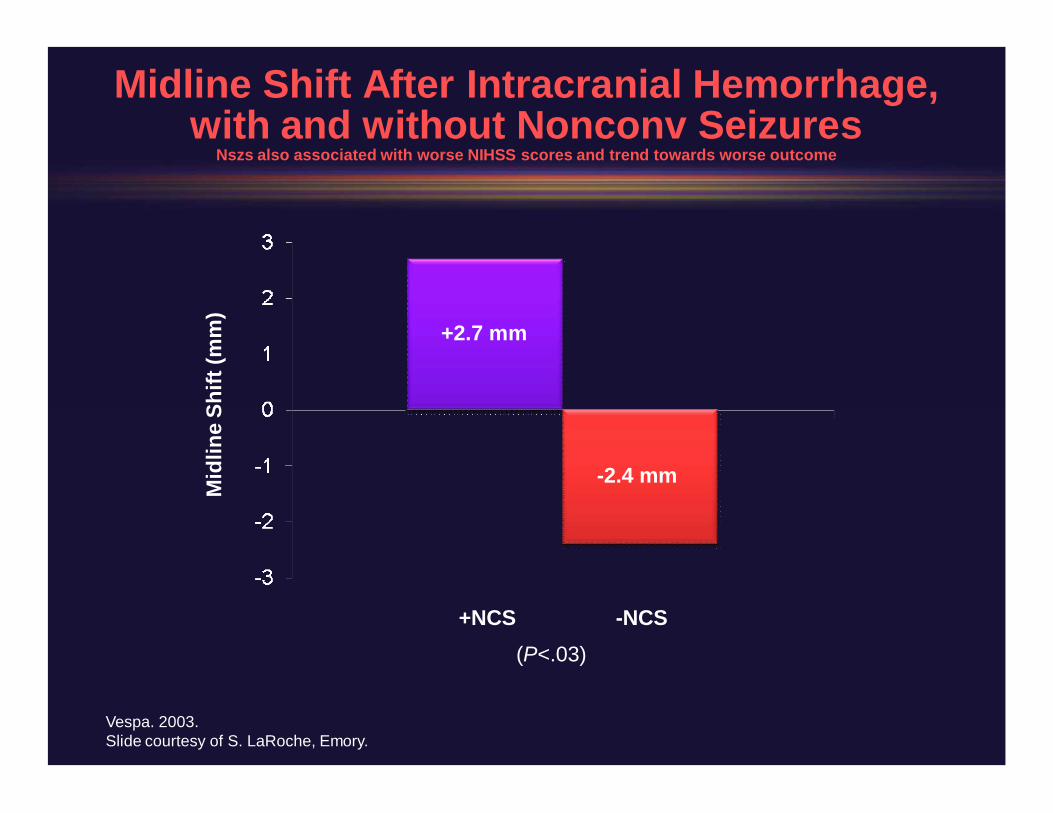
Midline Shift After Intracranial Hemorrhage,with and without Nonconv Seizures
Nszs also associated with worse NIHSS scores and trend towards worse outcome
+NCS NCS(P<.03)
+2.7 mm
2.4 mmMid
line
Shift
(mm
)
Vespa. 2003.Slide courtesy of S. LaRoche, Emory.
Other Evidence That Seizures, IncludingNonconvulsive Ones, Are Causing Further Harm
(cont)
• Microdialysis– Szs can cause glutamate spikes on microdialysis, incl to
known neurotoxic levels, elevated glycerol (membranebreakdown), elevated lactate (Vespa 1998, 2002, 2007)
• Seizures cause elevations in CBF, ICP (animals andhumans), lactate, and metabolic demand, all ofwhich can be harmful in the acutely injured brain
• Seizures may trigger periinjury depolarizations
Evidence That Seizures, IncludingNonconvulsive Ones, Are Causing Further Harm
(cont)
• Rat MCA occlusion model supports secondaryinjury from seizures, both with regard to infarctsize and mortality (Williams AJ. J Pharmacol & ExpTherap. 2004)
• Rat CPSE model (lowdose pilocarpine) showspermanent neurologic (motor and social),histologic (cortex), and physiologic (hippocampus)dysfunction (Krsek. Epilepsia. 2001; Epil & Behav.2004)
“Nonconvulsive Electrographic Seizures After TBI Result ina Delayed, Prolonged Increase in ICP and Metabolic Crisis”
Vespa P et al. Crit Care Med. Dec 2007
• 10 patients with modsevere TBI undergoing cEEGx 7 days and microdialysis WITH EEG szs– All szs were nonconvulsive
• 10 TBI controls matched for age, CT scan, andGCS, but WITHOUT EEG szs
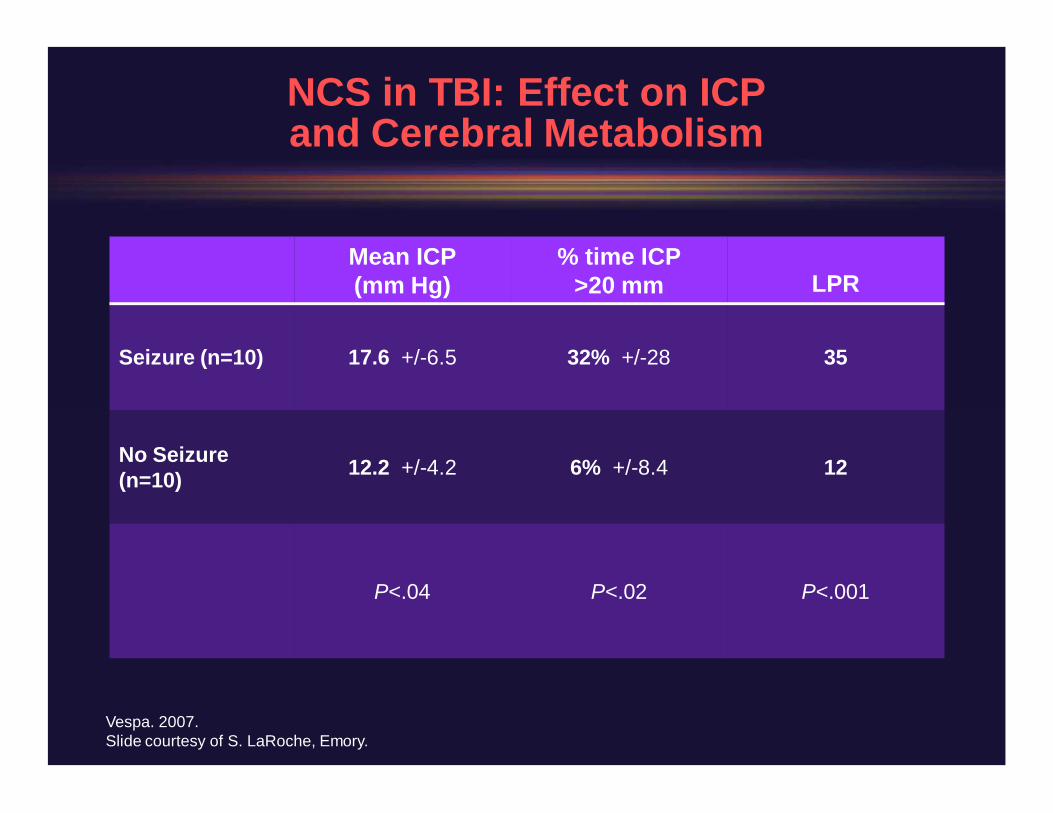
NCS in TBI: Effect on ICPand Cerebral Metabolism
Vespa. 2007.Slide courtesy of S. LaRoche, Emory.
Mean ICP(mm Hg)
% time ICP>20 mm LPR
Seizure (n=10) 17.6 +/6.5 32% +/28 35
No Seizure(n=10) 12.2 +/4.2 6% +/8.4 12
P<.04 P<.02 P<.001
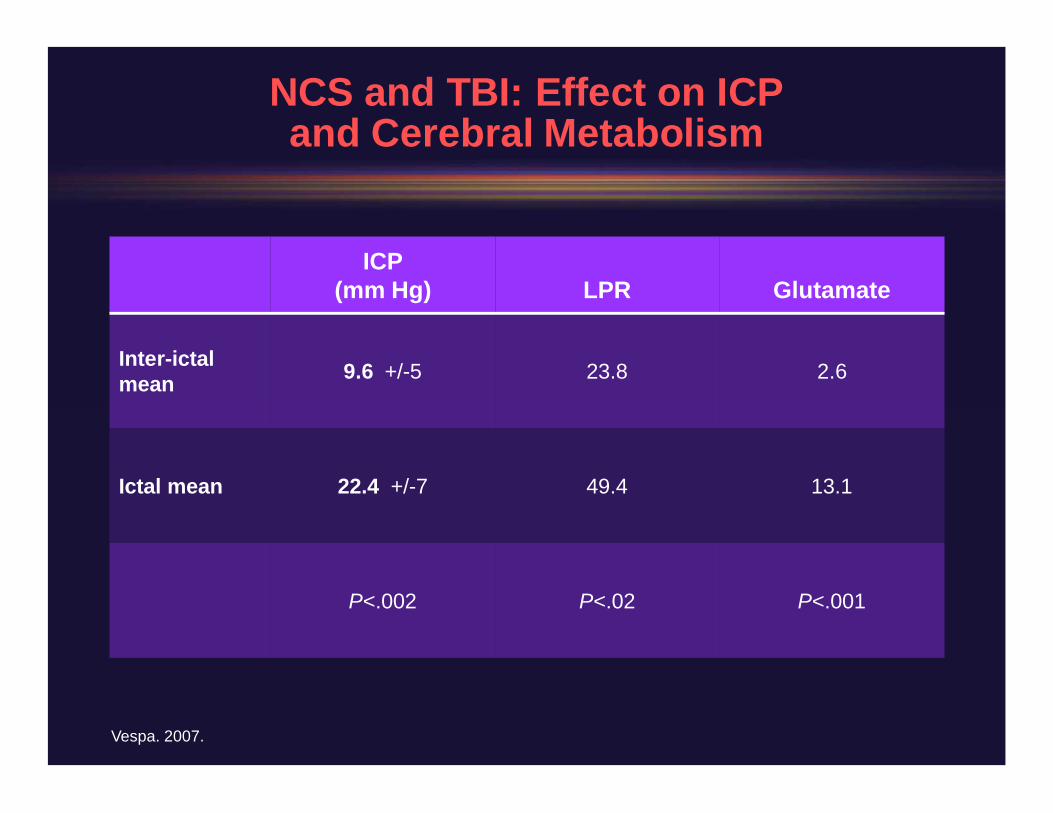
NCS and TBI: Effect on ICPand Cerebral Metabolism
ICP(mm Hg) LPR Glutamate
Interictalmean 9.6 +/5 23.8 2.6
Ictal mean 22.4 +/7 49.4 13.1
P<.002 P<.02 P<.001
Vespa. 2007.
“Nonconvulsive Seizures After Traumatic Brain InjuryAre Associated with Hippocampal Atrophy”
• 6 TBI patients with seizures had greaterhippocampal atrophy as compared to 10 matchedTBI patients without seizures (21 +/ 9 vs 12 +/ 6%,P = 0.017)
• Hippocampi ipsilateral to the electrographic seizurefocus demonstrated a greater degree of volumetricatrophy as compared with nonseizure hippocampi(28 +/ 5 vs 13 +/ 9%, P = 0.007)
Vespa PM et al. Neurology. 2010.
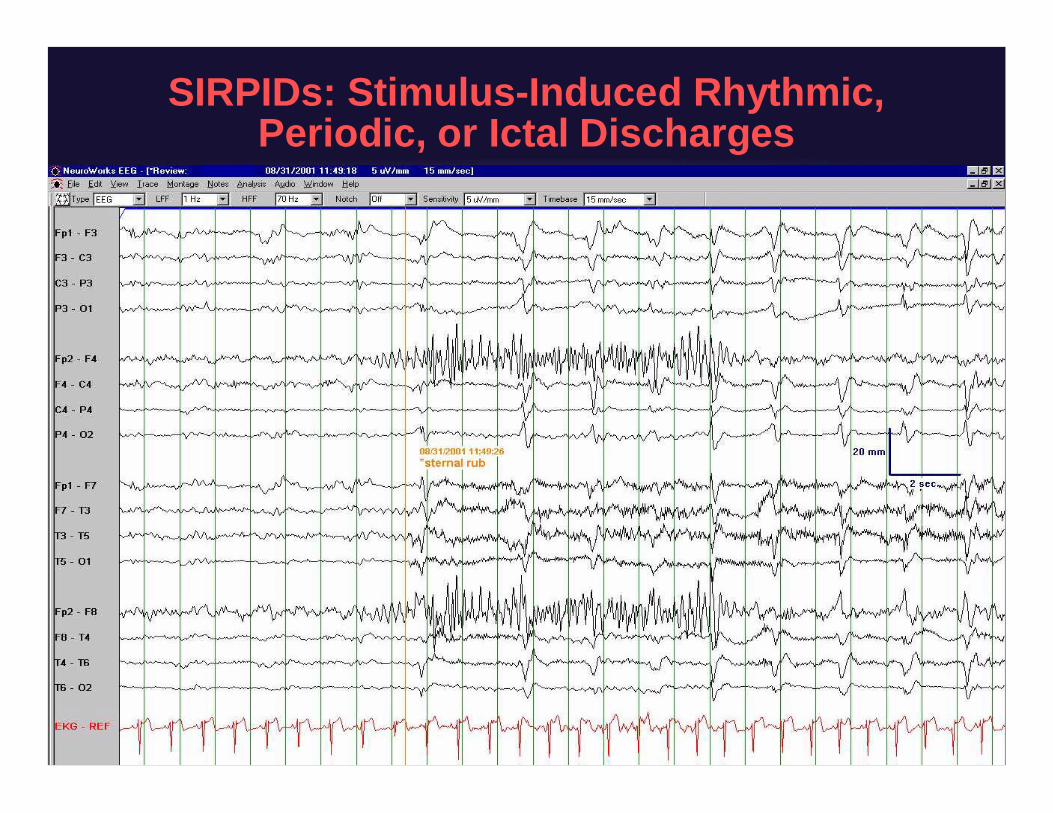
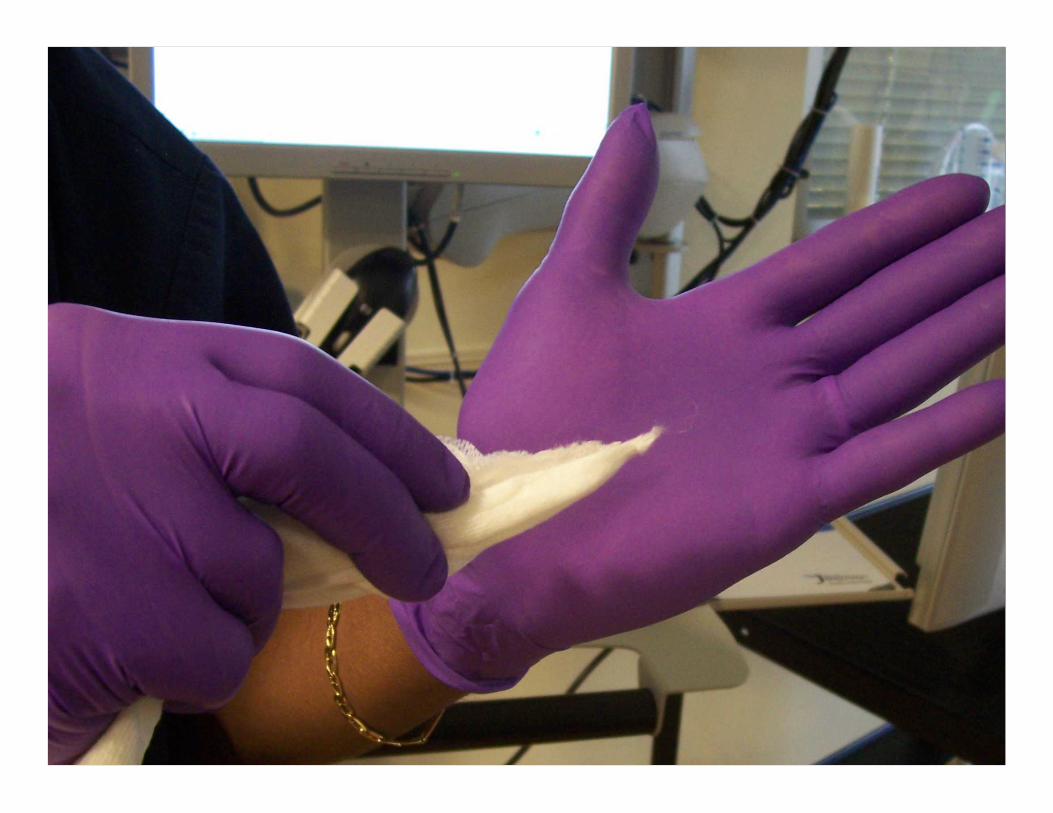
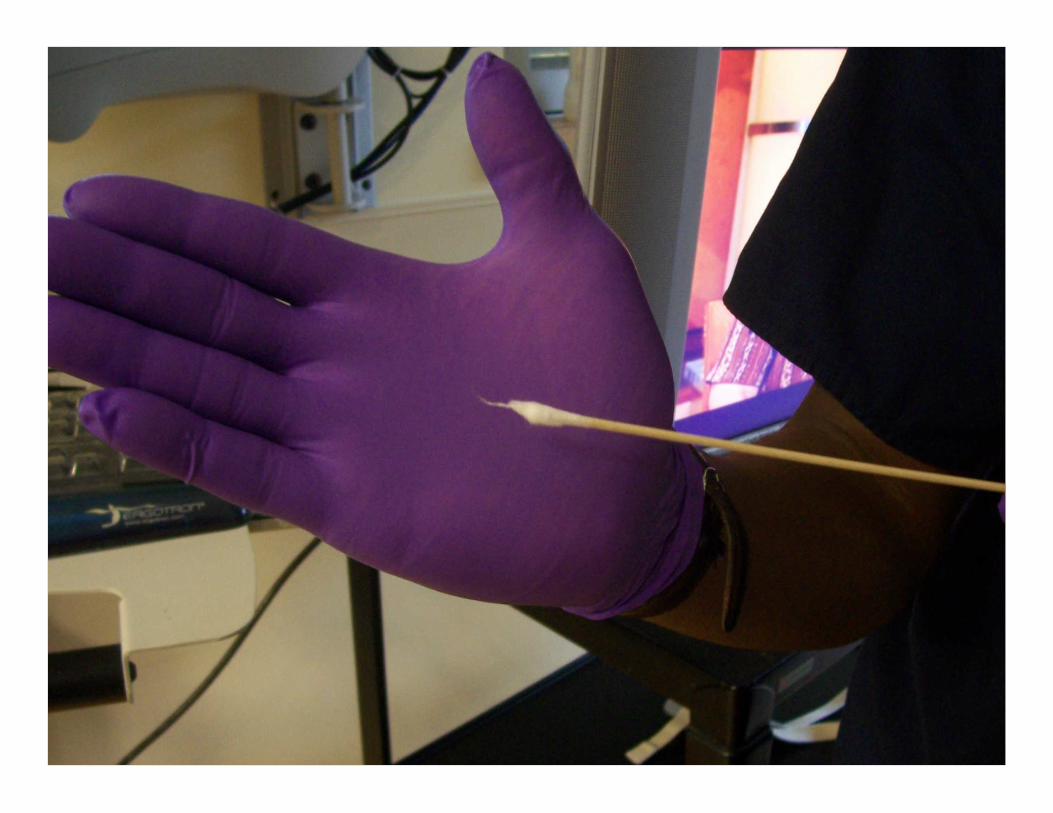
SIRPIDs: StimulusInduced Rhythmic,Periodic, or Ictal Discharges
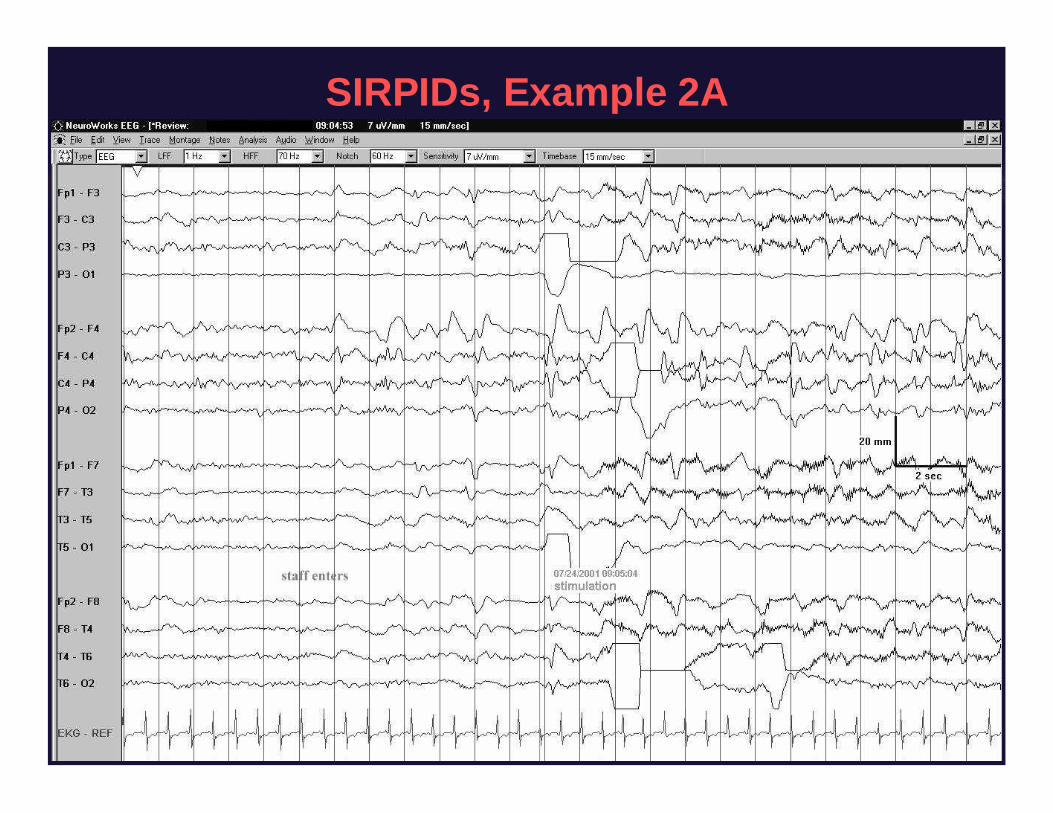
SIRPIDs, Example 2A
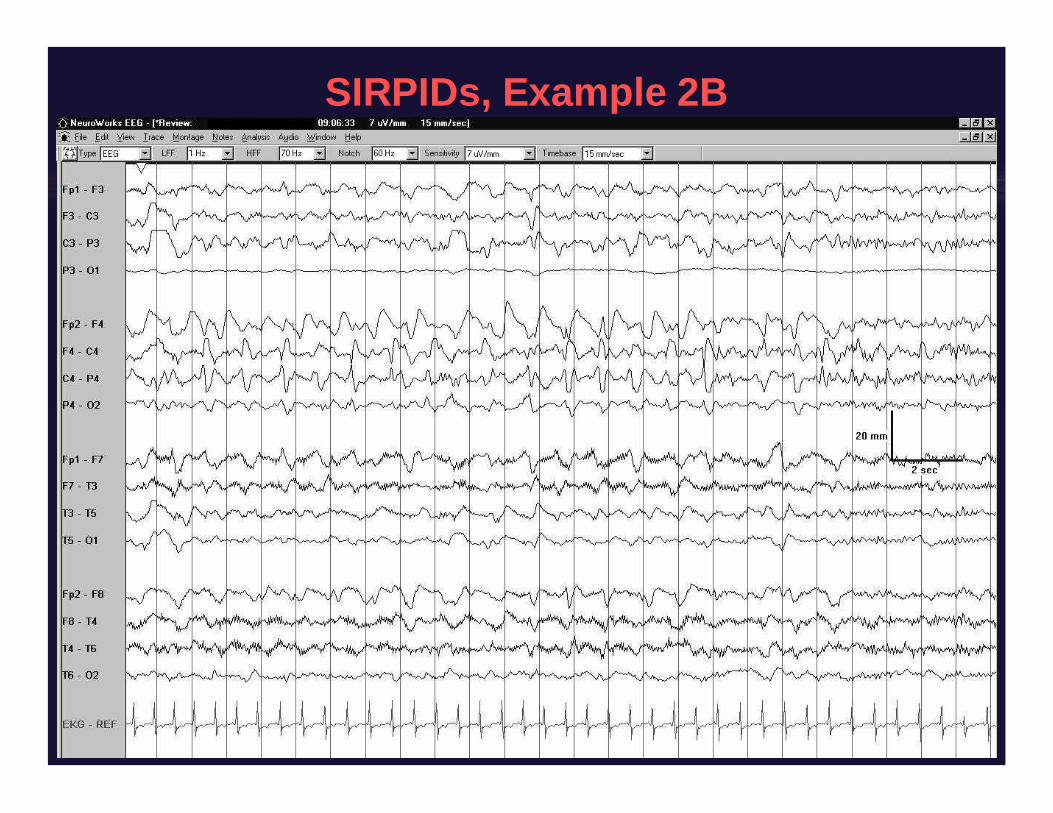
SIRPIDs, Example 2B

SIRPIDs w/ clin correlate

73 yo woman after cardiac arrest,developed bilateral watershed infarcts.
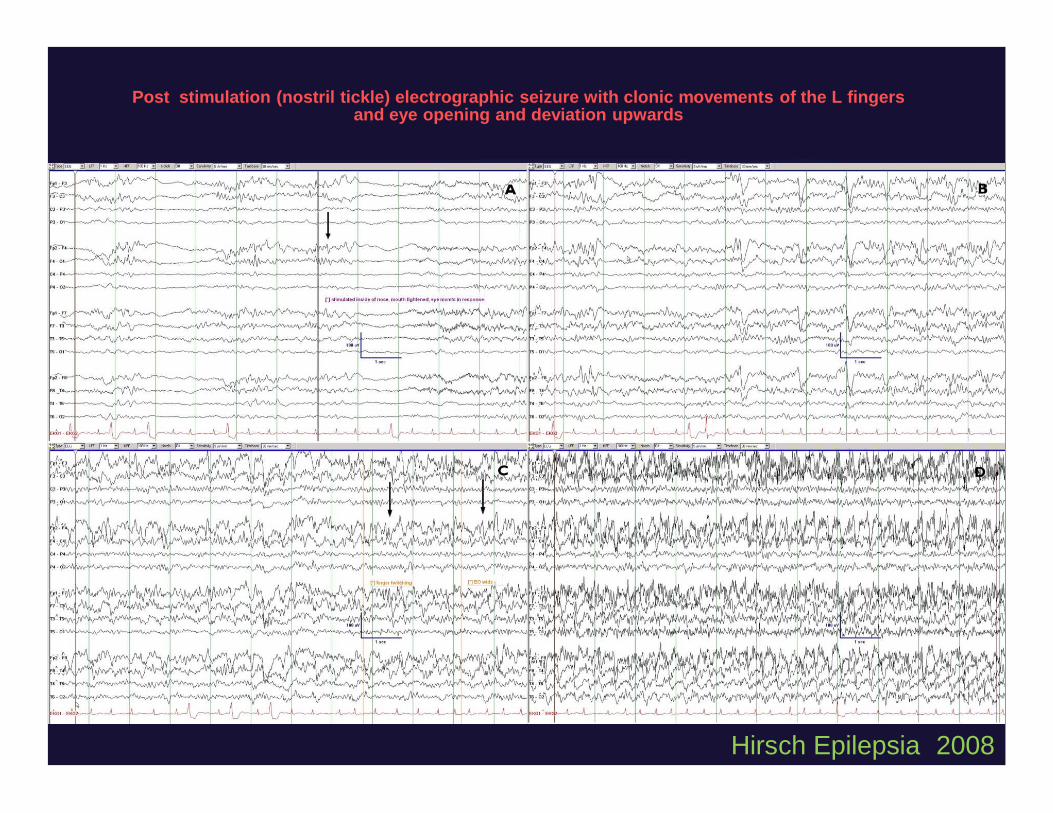
Post stimulation (nostril tickle) electrographic seizure with clonic movements of the L fingersand eye opening and deviation upwards
Hirsch Epilepsia 2008
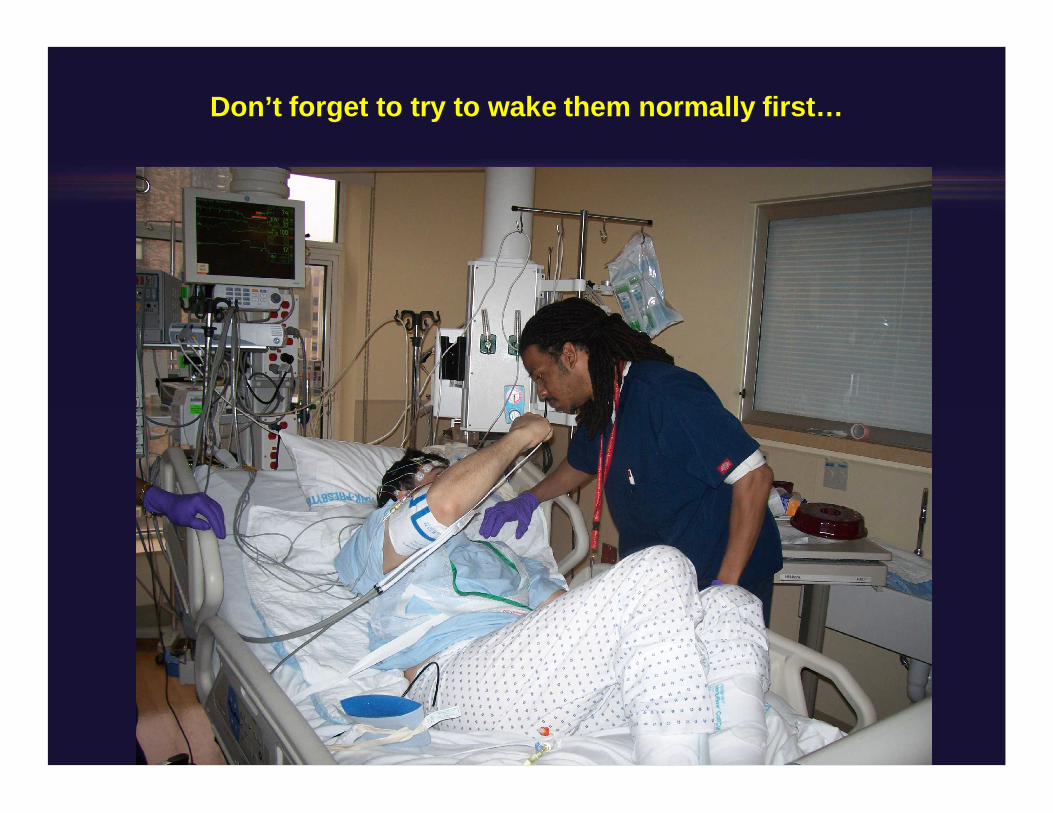
Don’t forget to try to wake them normally first…
MDZ
Dr. Mayer
Do Patients Wake Up After Treating NCSE?If So, When?
• 91 cases of seizures on EEG in ICU patients in BethIsrael Deaconess, Boston– (No neuro ICU)
• Of the 68 nonanoxic patients, 38 (56%) improved inalertness, including 25/52 comatose patients
• Improvement not immediate, but often same day• 21/38 responders survived vs 1/30 of others
Drislane et al, Aug 2008.
Effect of Seizure Detectionon Treatment Decisions
Kilbride RD et al. Arch Neurol. 2009.
• 300 consecutive patients undergoing cEEG– 189 in an ICU; 240 were adults– Median duration 52 hours
• EEG seizures found in 28%• Change in AED treatment in 28%
– 14% initiation of an AED– 33% AED modification– 5% AED discontinuation
ICU “pseudoseizures”1:15
Shortcut to ICUpseudoszleftarmB.C.743cf14dc3654680a09a32f974552cee_0002.avi.lnk
Shortcut to ICU pseudoszRightarmD.H._a8889b4ad19744ae94c022783039dacc_0003.avi.lnk
Shortcut to ICUpseudoszleftarmB.C.743cf14dc3654680a09a32f974552cee_0002.avi.lnk
ICU pseudosz: Video clip:51
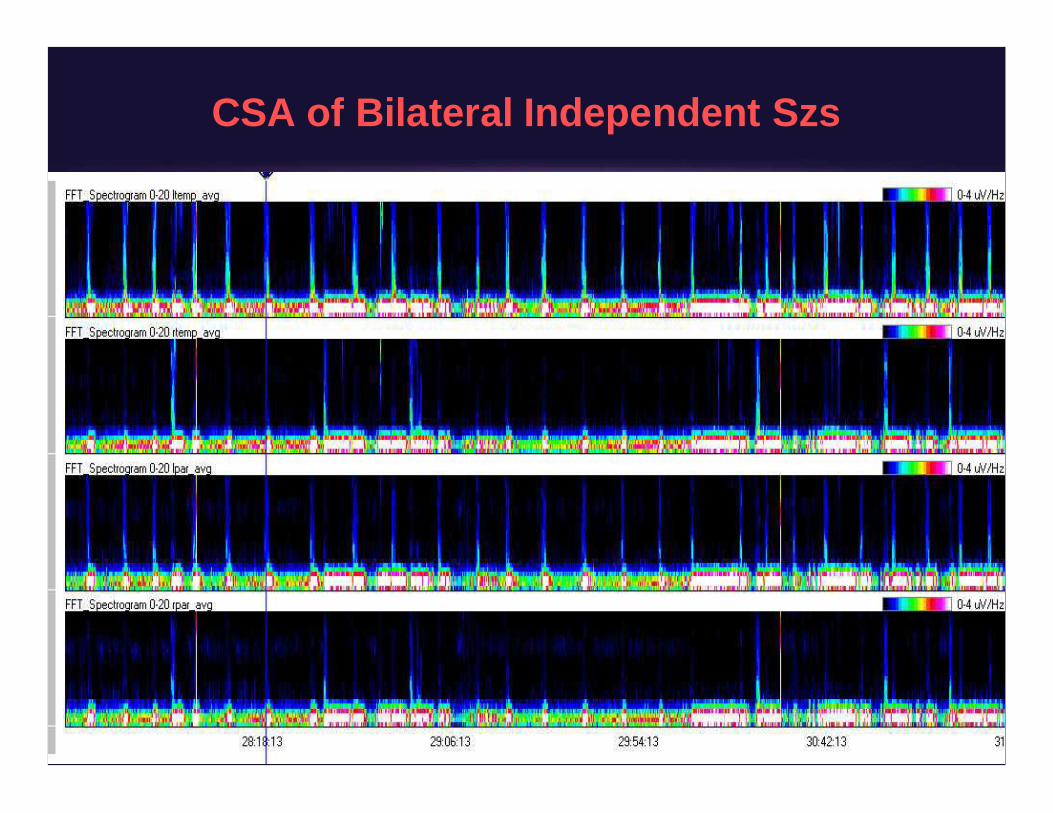
CSA of Bilateral Independent Szs
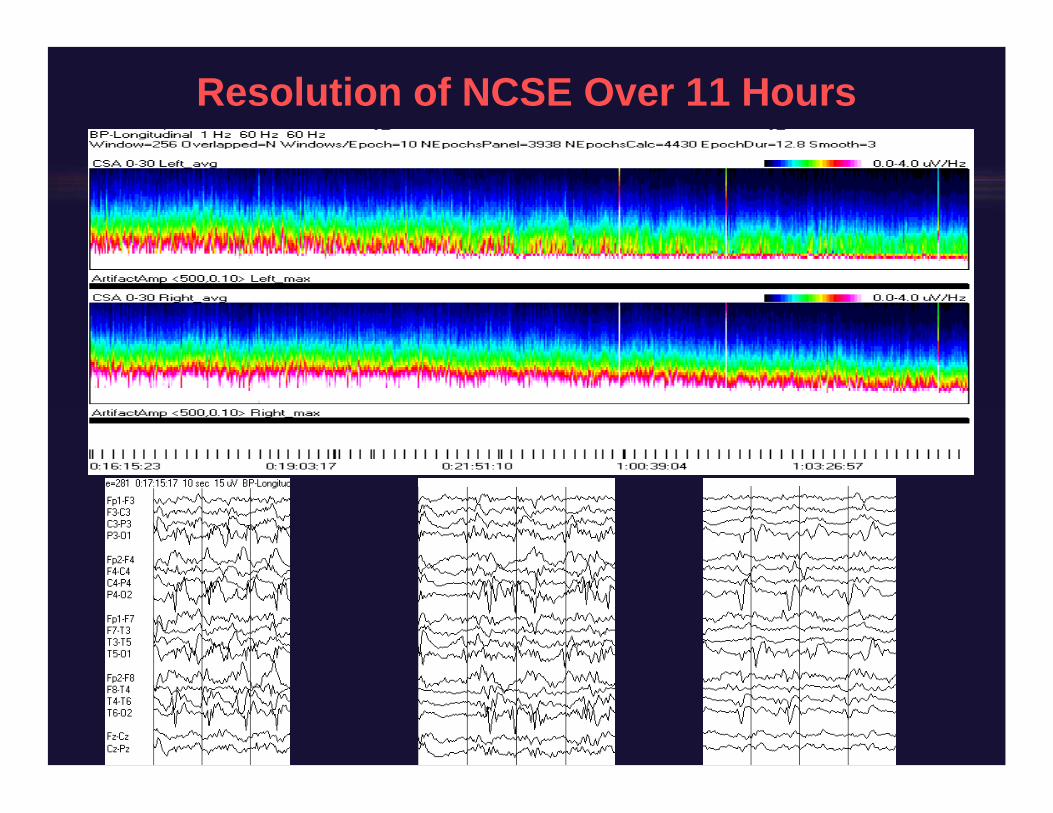
Resolution of NCSE Over 11 Hours
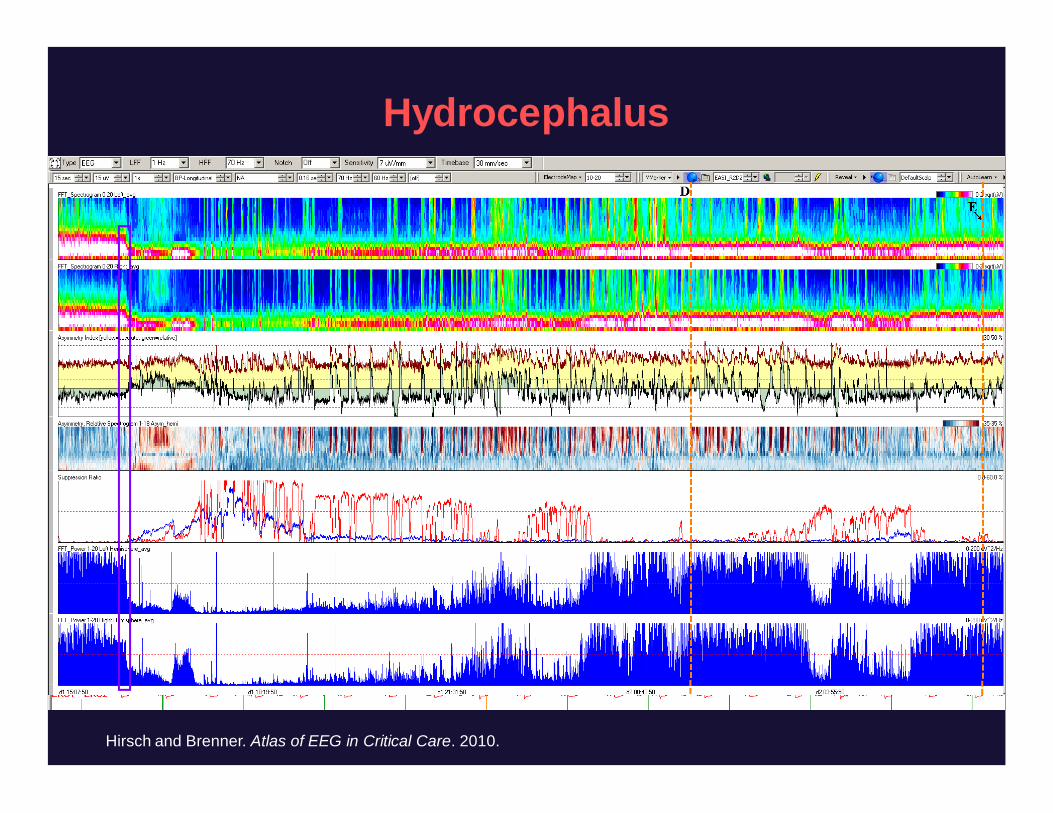
Hydrocephalus
Hirsch and Brenner. Atlas of EEG in Critical Care. 2010.
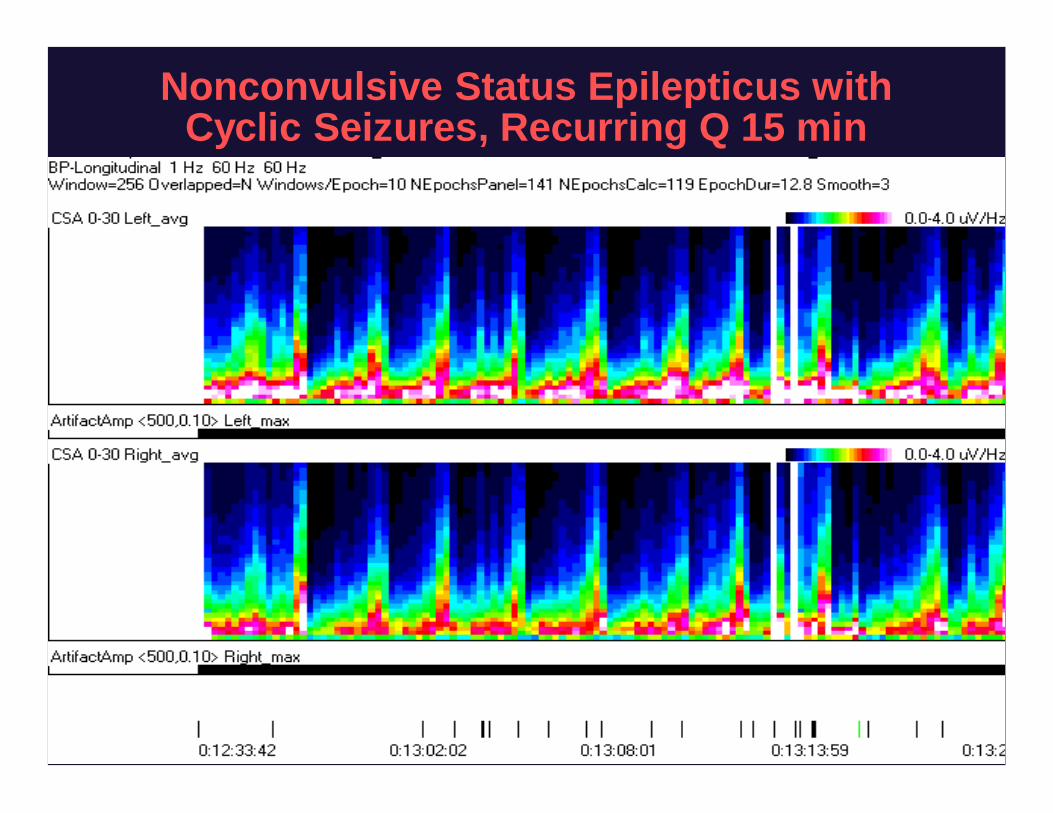
Nonconvulsive Status Epilepticus withCyclic Seizures, Recurring Q 15 min
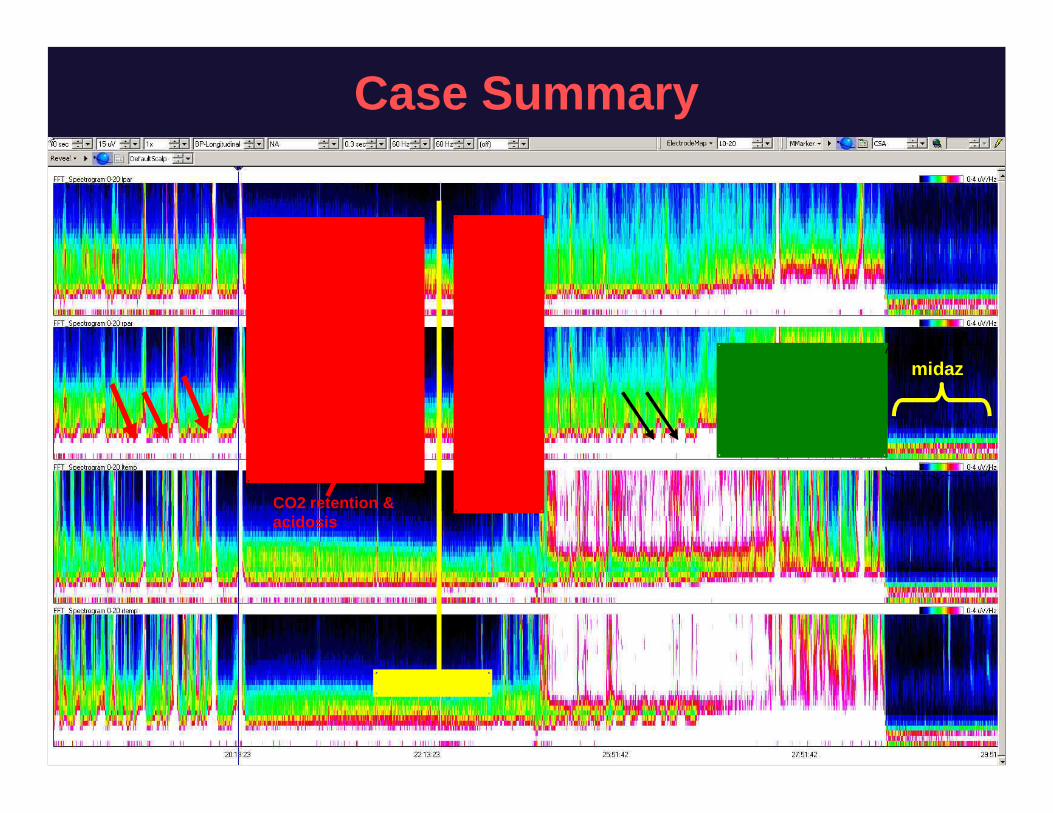
Case Summary
intubation
CO2 retention &acidosis
NCSE
midaz

CBF LEVEL(mL/100 gm/min)
EEGCHANGE
DEGREE OFNEURONAL INJURY
3570 NORMAL NO INJURY
2535 LOSS OF FAST BETA FREQUENCIES REVERSIBLE
1825 SLOWING OF BACKGROUND T0 57HZ THETA REVERSIBLE
1218 SLOWING TO 14HZ DELTA REVERSIBLE
<810 SUPPRESSION OF ALL FREQUENCIES NEURONAL DEATH
Jordan 2004.
Monitoring CBF in Acute Stroke
•Quant EEG changes correlated withCBF and clinical exam during BP,hemodilution, and triple H therapy(Wood 1984; Jordan 1991; Suzuki 1990)
Ischemia and Vasospasm After SAH
• Decreased relative alpha variability:32 SAH patients Vespa 1997– QEEG was 100% sensitive for angiogramdefined vasospasm
(19/19); ppv=76%– QEEG changes preceded TCD or angio detection of vasospasm
by at least 2 days in 10/14 patients
• CPMC protocol: SAH grade IVV, monitored x 7 days, N=43– Poststim alpha / delta ratio was best predictor of ischemia from
vasospasm– Patients with ADR falling >10% below baseline in 6 consecutive
recordings: sensitivity 100%, specificity 76%– Or a single recording >50% below baseline: sensitivity 89%,
specificity 84% Claassen 2004
cEEG in the Medical ICUOddo M et al. Crit Care Med. 2009.
• 201 patients 20042007– Mean of 3 days of cEEG– 60% sepsis, 48% comatose
• 22% had seizures or PEDs• Seizures in 21 (10%)
– 67% patients with szs had nonconv szs only
• PEDs in 34 (17%)• Independent predictors of szs / PEDs
– Only sepsis (31% had szs or PEDs)
cEEG in the MICU (cont)Oddo M et al. Crit Care Med. 2009.
• Independent predictors of worse outcome– Electrographic szs– PEDs– Each assoc’d with double the rate of poor outcome
• Sepsis subgroup: 31% had szs or PEDs– In multivariate analysis, presence of szs or PEDs
remained highly significant predictor of worse outcome(O.R. 10, P<0.001)
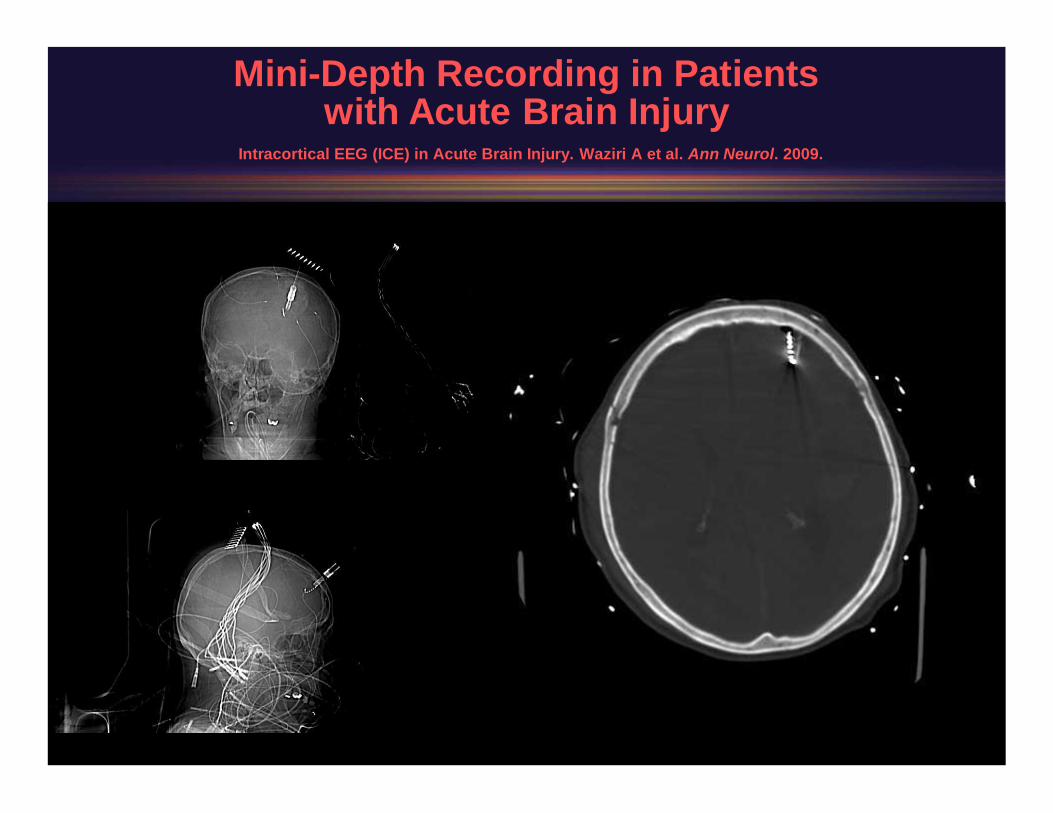
MiniDepth Recording in Patientswith Acute Brain Injury
Intracortical EEG (ICE) in Acute Brain Injury. Waziri A et al. Ann Neurol. 2009.
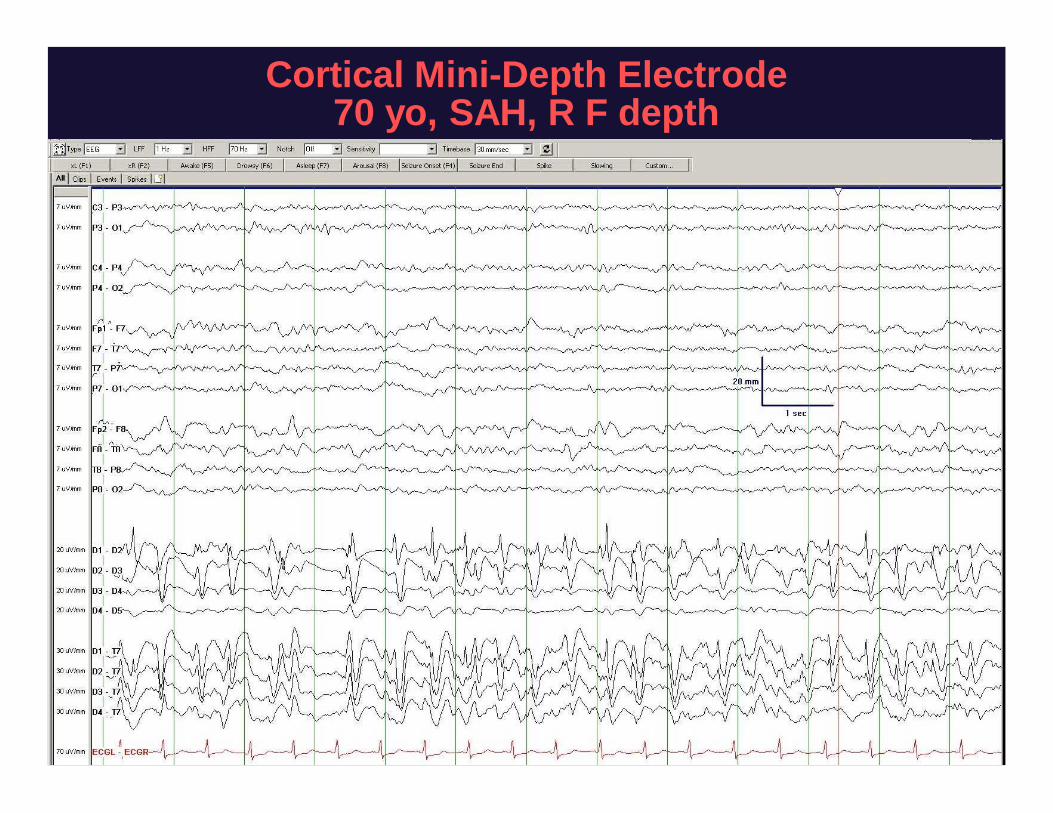
Cortical MiniDepth Electrode70 yo, SAH, R F depth
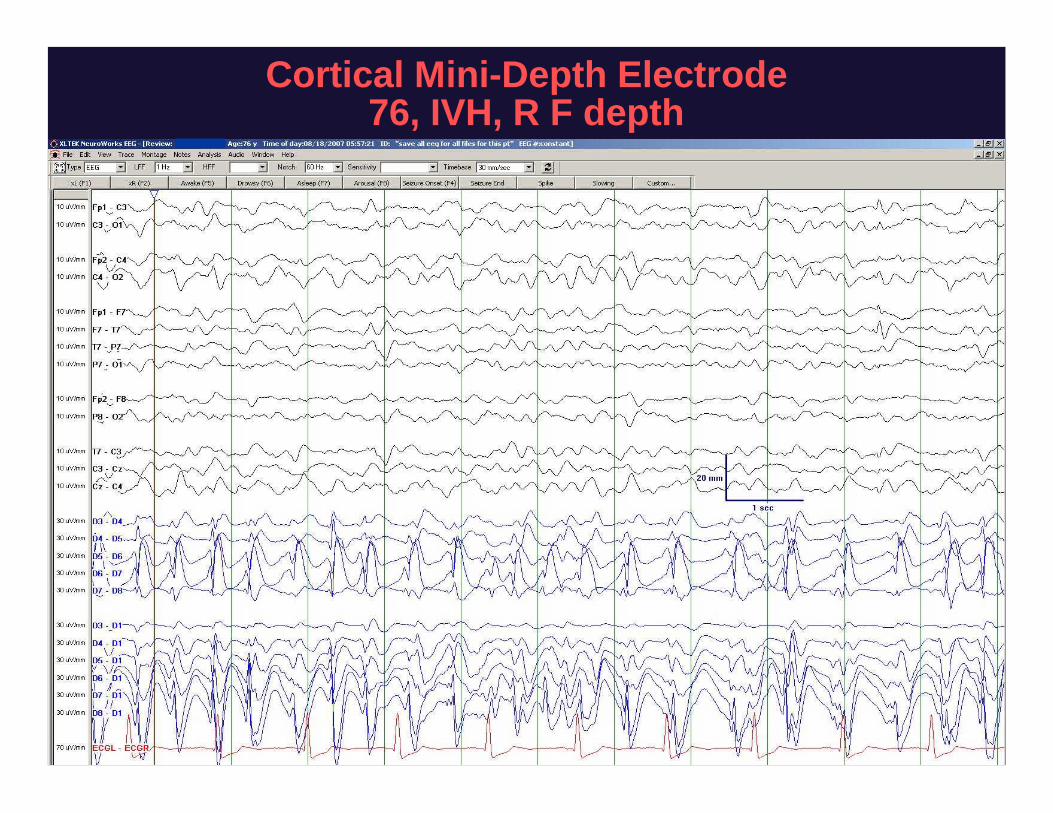
Cortical MiniDepth Electrode76, IVH, R F depth
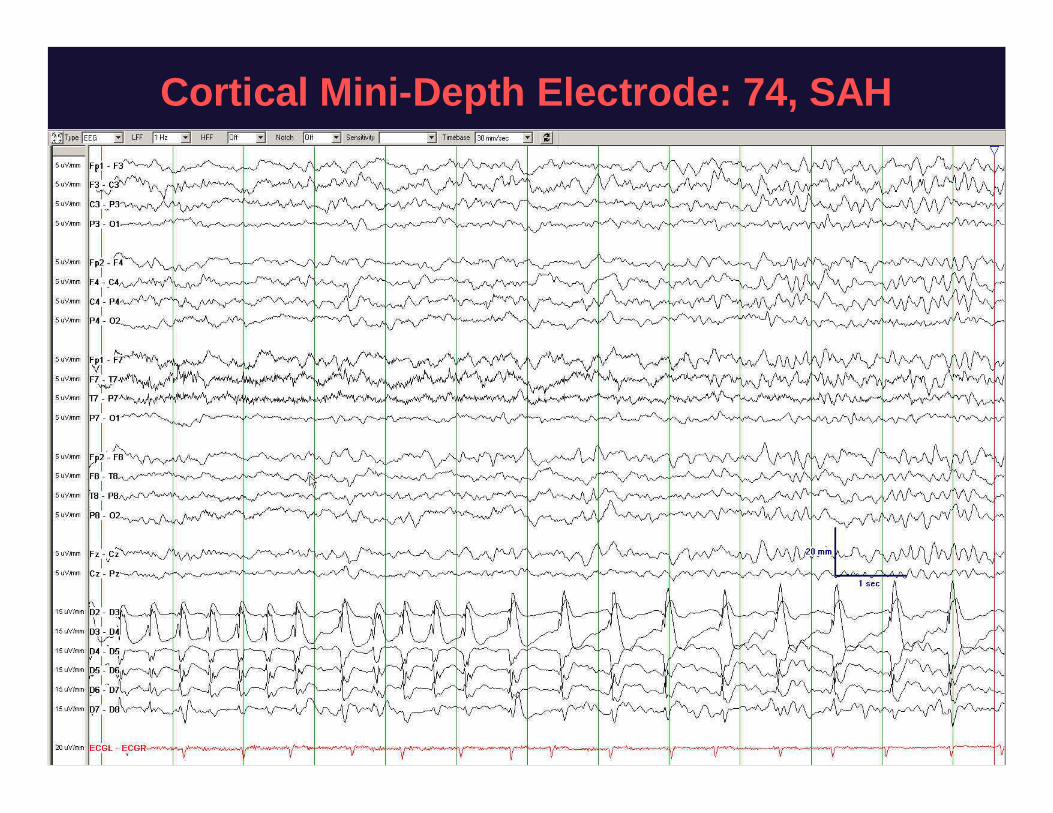
Cortical MiniDepth Electrode: 74, SAH
Summary of Findings withMiniDepth in NICU Patients
Intracortical EEG (ICE) in Acute Brain Injury.Waziri A et al. Ann Neurol. 2009.
• 10/14 patients had seizures on the minidepth• 6/10 never had scalp EEG correlate, 2 showed non
ictal appearing rhythmic delta on scalp, and 2showed scalp EEG correlate on occasion only
• Some but not all seizures / PEDs showedcorresponding microdialysis changes
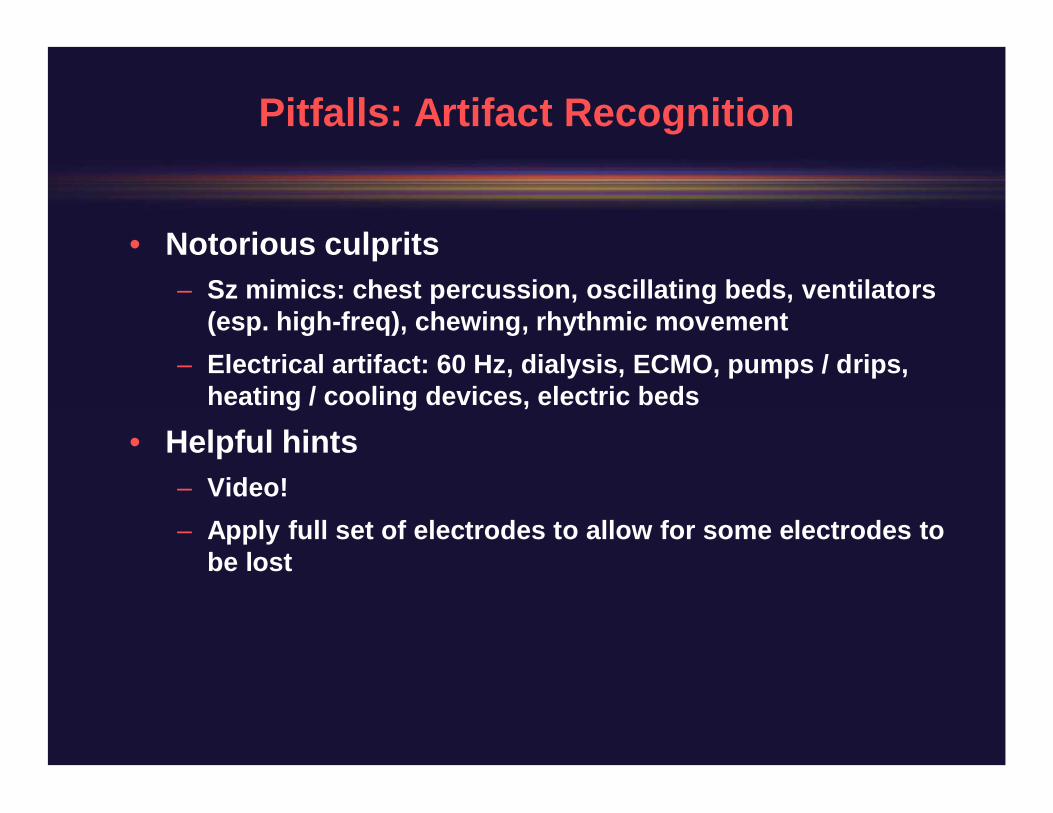
Pitfalls: Artifact Recognition
• Notorious culprits– Sz mimics: chest percussion, oscillating beds, ventilators
(esp. highfreq), chewing, rhythmic movement– Electrical artifact: 60 Hz, dialysis, ECMO, pumps / drips,
heating / cooling devices, electric beds
• Helpful hints– Video!– Apply full set of electrodes to allow for some electrodes to
be lost
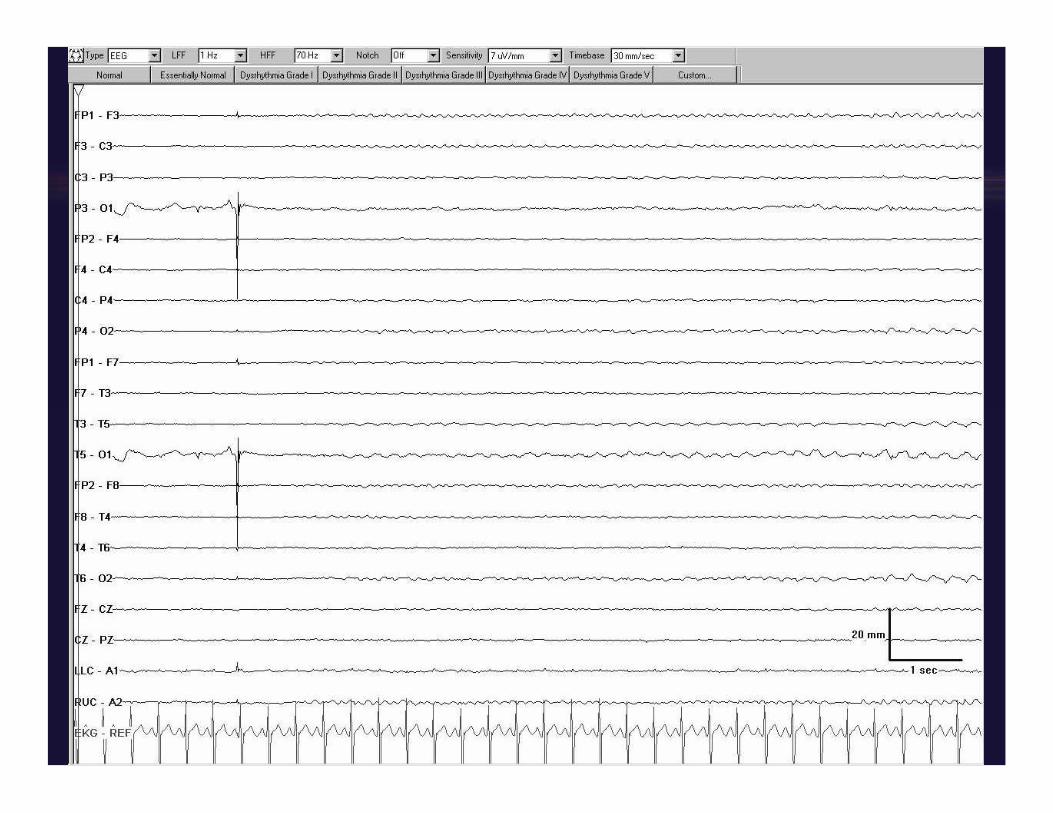
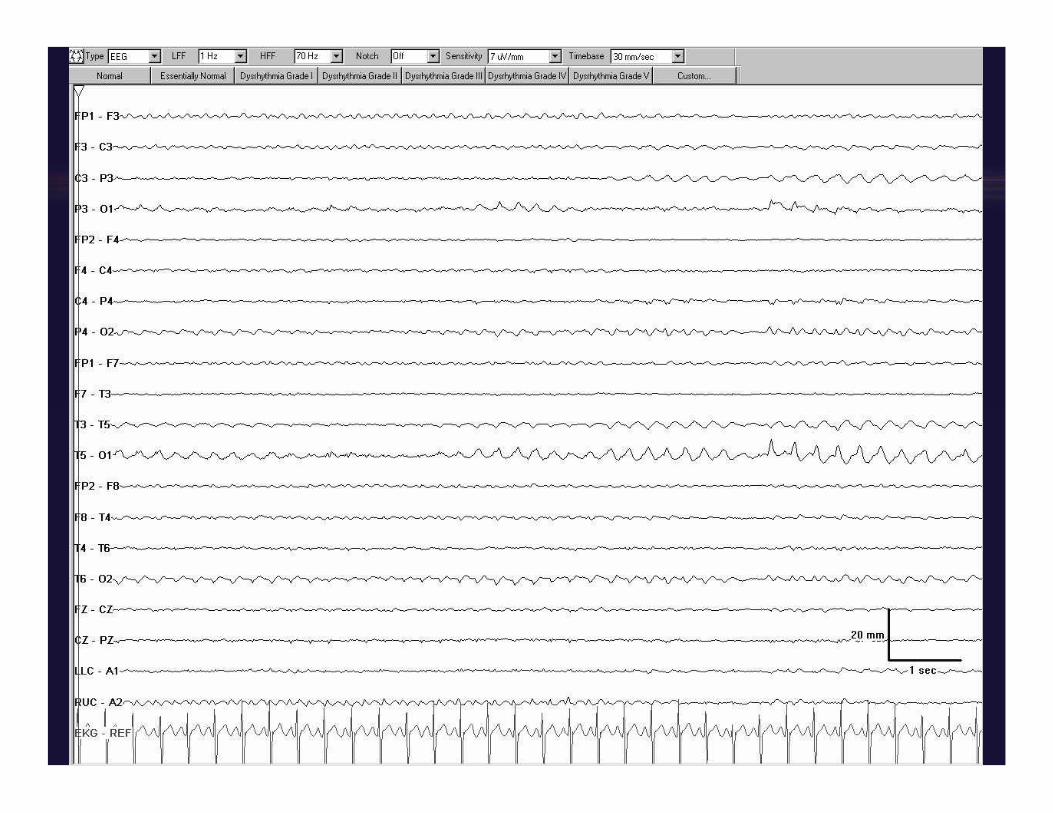
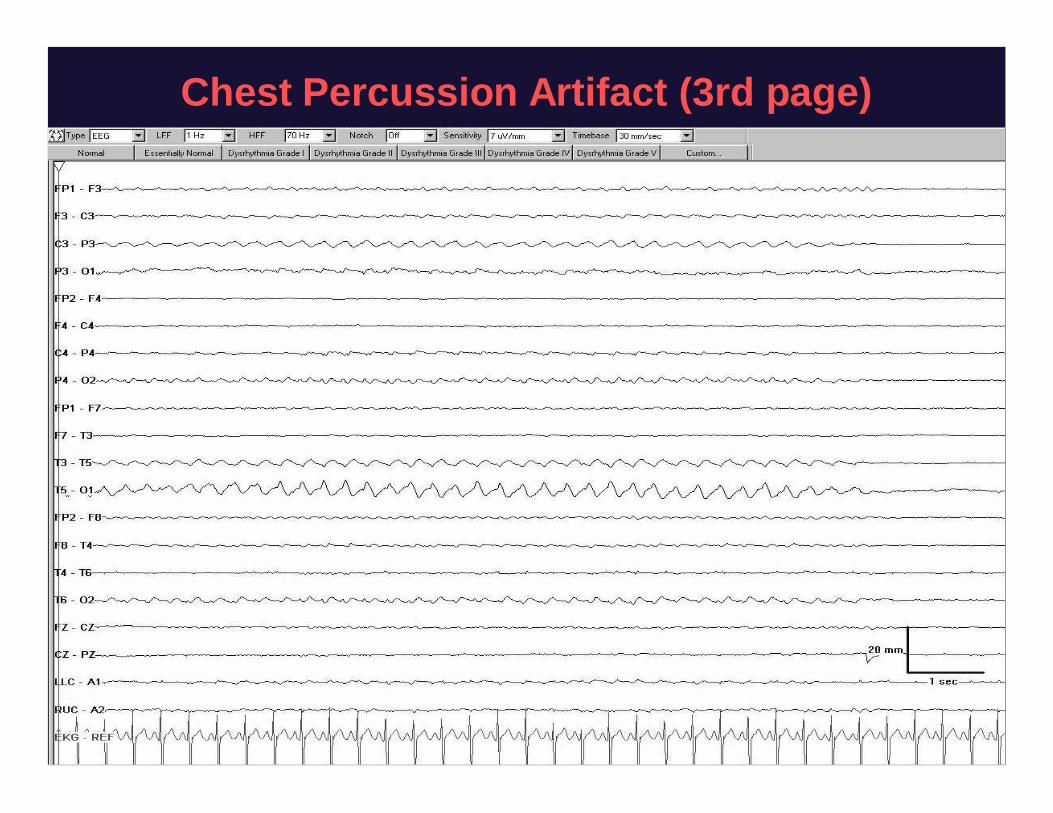
Chest Percussion Artifact (3rd page)
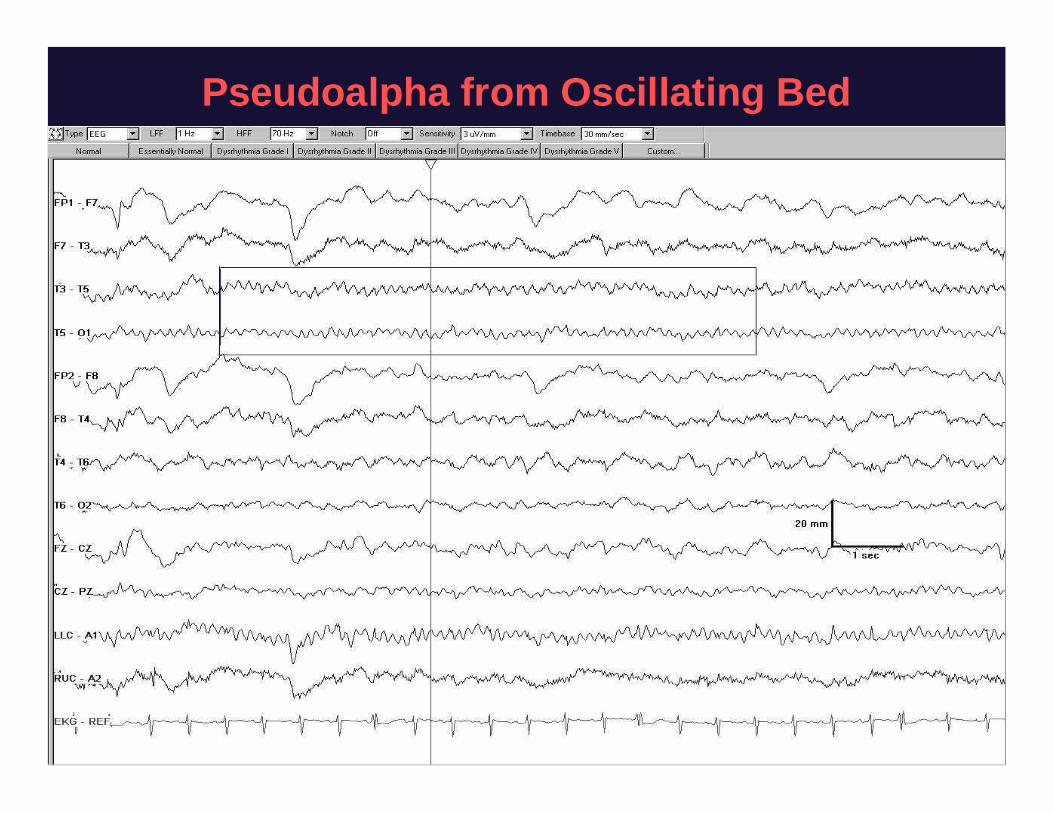
Pseudoalpha from Oscillating Bed
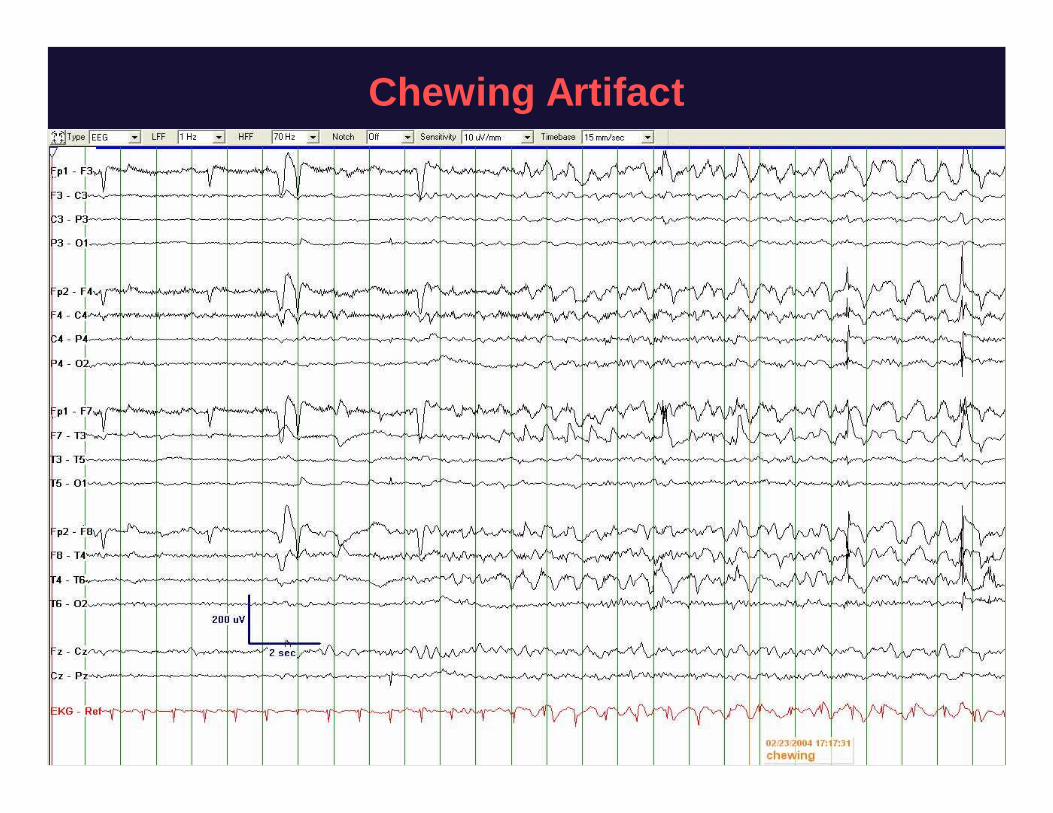
Chewing Artifact
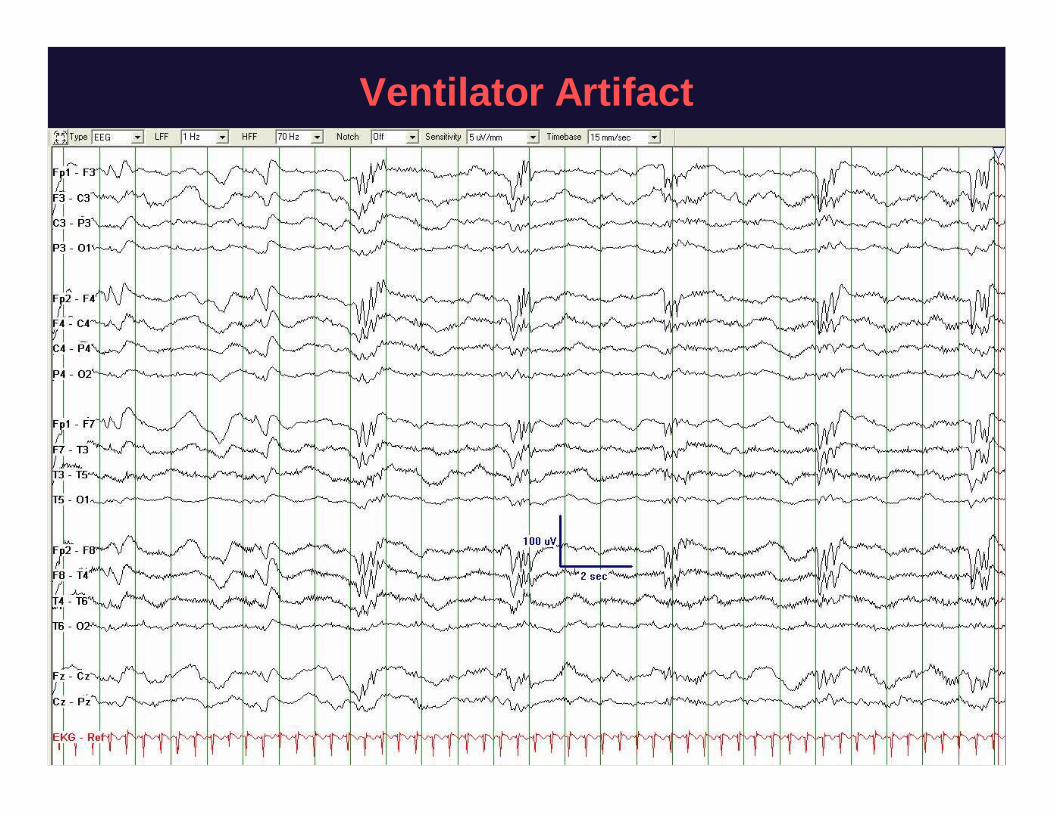
Ventilator Artifact
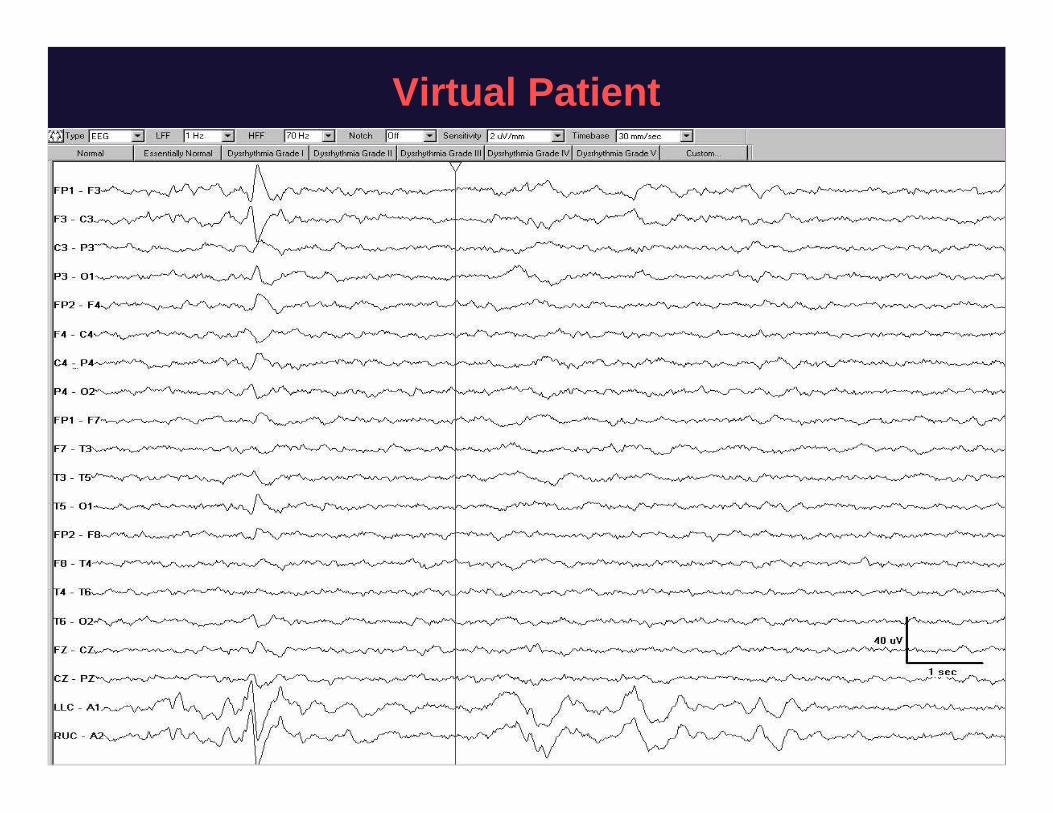
Virtual Patient

Summary of What We Now Know
• Nonconvulsive seizures are common in thecritically ill, including those without known braindisease
• Most seizures in the ICUs are nonconvulsive• There is extensive evidence (although no
prospective treatment trials) that seizures,including nonconvulsive ones, are harmful for thebrain, especially when superimposed on acutebrain injury
• EEG can detect many other acute brain processes
What We Now Need
• Realtime NEUROTELEMETRY– Ischemia– Hydrocephalus– Hemorrhage– Hypotension / hypoxia / CO2 retention / sepsis– Alarms feasible although require rapid review of raw
tracing§ Artifact detection and rejection in place§ 24 hour EEG techs in place (but not ones to read
continuously)§ Networking in place§ Imaging compatible electrodes— invisible on CT and MR
Other Conclusions
• A “routine” EEG will miss half to twothirds of patients that will goon to have nonconvulsive seizures
• Standard nomenclature and multicenter research consortium inplace
• Stimulation commonly elicits highly epileptiform or ictal EEGpatterns, occasionally with clinical correlate
• The era of NEUROTELEMETRY is almost here and there are MANYunanswered questions
• i.e., this is a great career opportunity!

Thanks to…
• Stephan Mayer, MD• Ron Emerson, MD• Lew Kull, R.EEG.T• Jan Claassen, MD
EPILEPSY FELLOWS• Dan Friedman, MD• David Friedman, MD• John Wittman, MD• Gregory Kapinos, MD• Nathalie Jette, MD• Derek Chong, MD• Karine AbouKhaled, MD• Jeff Jirsch, MD• Bin Tu, MD, PhD• Elizabeth Gerard, MD• Brandon Foreman, MD
• Neuro ICU residents, fellows,nurses, and attendings
• EEG techs and supervisors– Especially Eddie Toro, Larry Reid
• Hiba Arif, MD• Mauro Oddo, MD• Emmanuel Carrera, MD• Michael Schmidt, MD• Sander Connolly, MD• Allen Waziri, MD• Morgan Stuart, MD• Pedro Kurtz, MD• Alexandra Svoronos

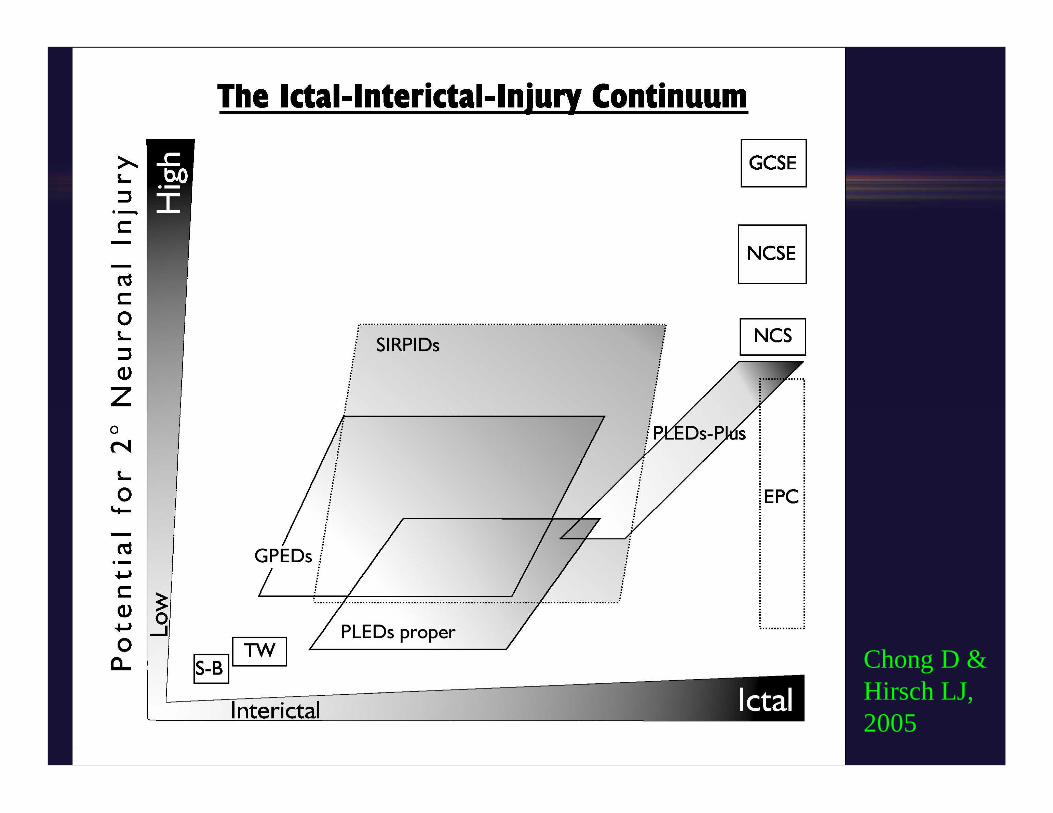
Chong D &Hirsch LJ,2005
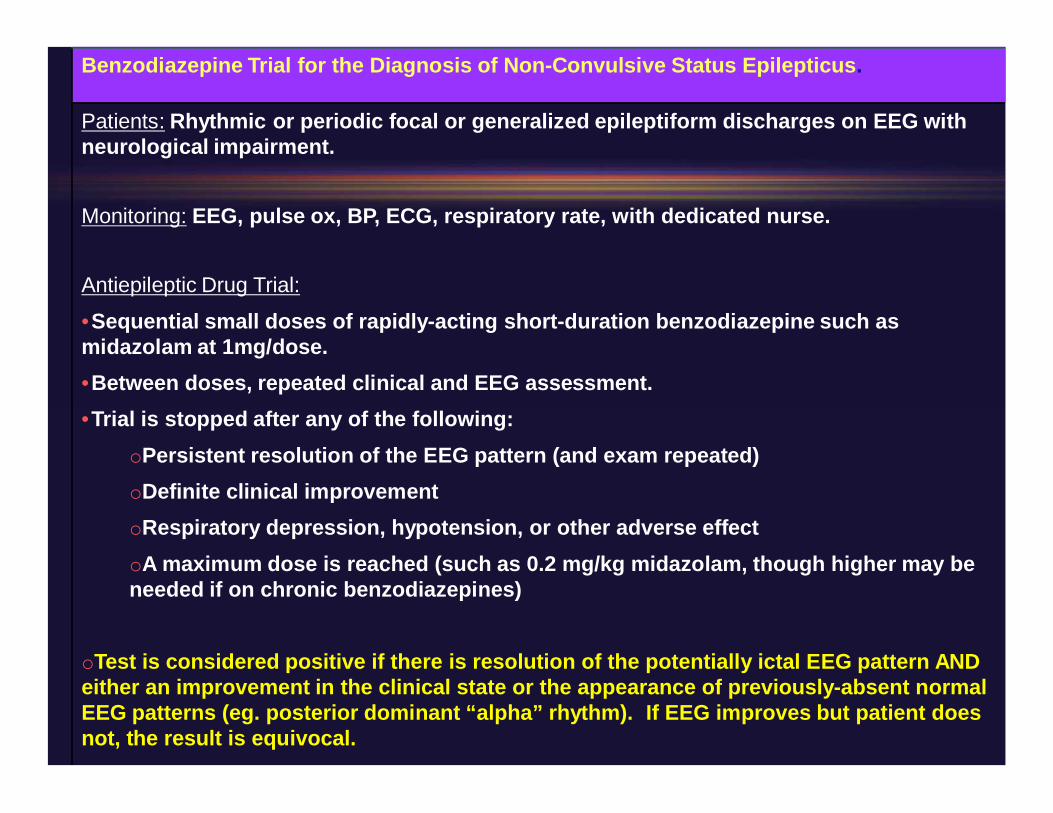
Benzodiazepine Trial for the Diagnosis of NonConvulsive Status Epilepticus.
Patients: Rhythmic or periodic focal or generalized epileptiform discharges on EEG withneurological impairment.
Monitoring: EEG, pulse ox, BP, ECG, respiratory rate, with dedicated nurse.
Antiepileptic Drug Trial:
•Sequential small doses of rapidlyacting shortduration benzodiazepine such asmidazolam at 1mg/dose.•Between doses, repeated clinical and EEG assessment.•Trial is stopped after any of the following:
oPersistent resolution of the EEG pattern (and exam repeated)oDefinite clinical improvementoRespiratory depression, hypotension, or other adverse effectoA maximum dose is reached (such as 0.2 mg/kg midazolam, though higher may beneeded if on chronic benzodiazepines)
oTest is considered positive if there is resolution of the potentially ictal EEG pattern ANDeither an improvement in the clinical state or the appearance of previouslyabsent normalEEG patterns (eg. posterior dominant “alpha” rhythm). If EEG improves but patient doesnot, the result is equivocal.
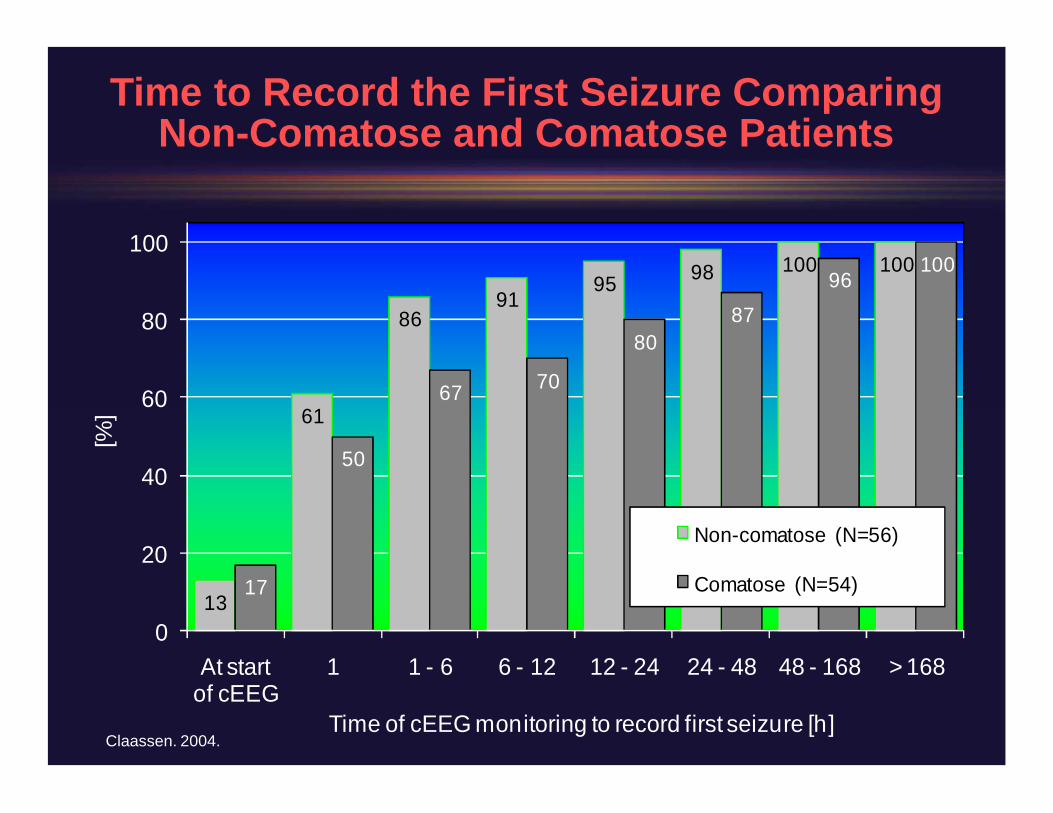
13
61
8691
95 98 100 100
17
50
67 70
8087
96100
0
20
40
60
80
100
At startof cEEG
1 1 6 6 12 12 24 24 48 48 168 > 168
[%]
Time of cEEG monitoring to record first seizure [h]
Noncomatose (N=56)
Comatose (N=54)
Claassen. 2004.
Time to Record the First Seizure ComparingNonComatose and Comatose Patients
How Long Should Patients Be Monitored?
• 24 hours if not comatose• 48 hours or more if comatose
– Longer if periodic discharges, withdrawing sedation orAEDs
• Routine EEG is not adequate in critically ill patients
MRICompatible Electrodes
• MRIcompatible disc electrodes– Mirsattari et al (w/ Ives), Clin Nphys 2004– 100 patients underwent MRI with their scalp disc electrode set
§ Pure silver with thick gold flash§ Bundled into 8 wires with one connector§ No heating at all§ No artifact that reached the intracranial compartment§ Also did fMRI successfully with these§ FDA approved
• Subdermal Wire electrodes– Ives J Clin Nphys 2005 and Young et al Clin Nphys 2006– Subdermal wire, AgAg/Cl electrodes (minisphenoidals)– MRI and CT compatible and minimal maintenance for long periods– Fewer artifacts and less 60 Hz in SWEs compared to disk+collodion (30/80 vs 10/80
electrodes in 10 comatose patients)– FDA approved in kids and adults
• Conductive plastic disc electrodes with a conductive silver epoxy coatdeveloped as well, FDA approved! Ives, Clin Nphys 2006
cEEG in ICH
• Claassen, Columbia series, N=102 pts w/ ICH– Szs in 31%
§ Cortical involvement: 29% had szs, vs 10% deep (P=0.015)
– During cEEG, 18% had szs§ Only 1 of 18 noticed at bedside clinically; the rest were CLUES
(CLinically Unrecognized Electrographic Szs)
– 17% had periodic discharges (PEDs— either GPEDs or PLEDs)– The only association with szs still present in multivariate: Szs
associated with expanding hemorrhages (szs in 36% withexpanding ICH, vs 14% without; P=0.048)
– PEDs associated with proximity to cortex and worse outcome(65% poor outcome vs 17%, P<0.001)§ Trend towards poor outcome with szs as well: 44% poor outcome vs
21%; P=0.03 univariate
Claassen J et al. Neurology. 2007.
Which QEEG Measure Is Best?“Seizure ID in the ICU using QEEG displays,” Stewart CP et al. Neurology. 2010.
• CDSA and aEEG (using 8 channels) approximatelyequal for sz detection in kids (raw EEG hidden)
• Both 81%83% sens and infrequent false positives• 20% seizures missed overall• There were some patients in whom seizures were
completely missed by both– Low ampl, focal, brief, or within frequent epileptiform
discharges
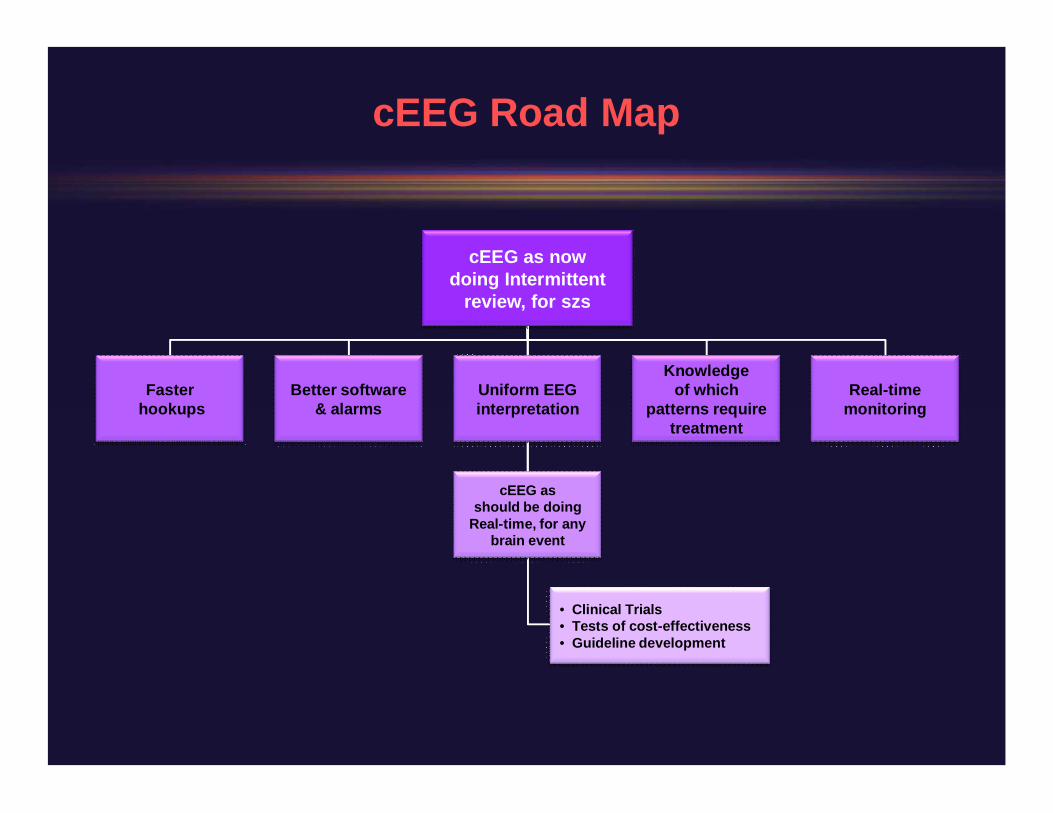
cEEG as nowdoing Intermittent
review, for szs
Fasterhookups
Better software& alarms
Uniform EEGinterpretation
cEEG asshould be doing
Realtime, for anybrain event
•Clinical Trials•Tests of costeffectiveness•Guideline development
Knowledgeof which
patterns requiretreatment
Realtimemonitoring
cEEG Road Map