Embed Size (px)
Citation preview

Latent Autoimmune Diabetes in Adults
A Case Study Report
Written by Angelica Adragna
Sodexo Dietetic Intern 2013
Introduction: As a dietetic intern with an emphasis in diabetes, I knew my case study topic
would be related to diabetes. I wanted it to be a topic that I knew little about and something that I
would gain good knowledge from for my future career goal as Certified Diabetes Educator
(CDE). During my diabetes outpatient clinical days at an endocrinology pediatric clinic, my
preceptor told me about a patient who initially presented with childhood type 2 diabetes, but oral
medications were not helping. Eventually, the physician ran more tests and diagnosed him as
type 1. I began to think that with the rise in childhood obesity and subsequent rise in childhood
type 2 diabetes, this situation may be more common than it used to be.
According to the International Diabetes Federation, there has been an annual 3% increase
in incidence of type 1 diabetes since 2011. Diabetes as a whole is projected to increase from 366
million people (2011) to 552 million people by 2030. The term “juvenile” diabetes is considered
to not be used anymore because type 1 can also be diagnosed in adulthood. After pondering this
evolvement of diabetes diagnoses, I realized that I was not too familiar of the diagnostic
laboratory values used for differentiating between diabetes type 1 and 2. Although I know the
difference between the two, I wanted to research more on the diagnostic tools for these types of
patients who would typically be one type, but due to other physiological causes, they may also fit
the signs and symptoms for another type of diabetes. Familiarizing myself with the diagnostic
criteria for type 1 and type 2 diabetes is important for my future career in diabetes.
I began researching this epidemic of type 2 diabetes in children and type 1 diabetes in
older adults and came across the “type 1.5.” This new type is also more formally called latent
autoimmune diabetes of adults, or LADA. This subject includes every aspect of diabetes that I

was interested in researching so I then found a patient at the outpatient Helwig Health Diabetes
Center who was diagnosed LADA and researched how lab values, signs and symptoms can help
health care practitioners decide whether their patient is type 1, type 2, or the more uncommon
type 1.5.
Abstract: Diabetes is a growing epidemic worldwide. There are different types of diabetes
that may confuse not only the general population, but the medical world as well. The main types
of diabetes are type 1, type 2, gestational diabetes, and now a new type termed “type 1.5.” It is
more formally titled latent autoimmune diabetes of adults (LADA) and is a very rare type of
diabetes that occurs in older adults, but reflects more similar features to that of type 1 diabetes,
which is more prevalent in youth and young adults.
The purpose of this paper is to review how LADA compares to the more common type 2
and type 1 diabetes. It will address the difficulty in diagnosing LADA as it often presents
similarly to type 2 diabetes. It will review the definition of each type, the diagnostic criteria, and
the treatment. The medical nutrition therapy for diabetes is similar for each type, focusing on
carbohydrate counting and overall healthy eating for weight loss or maintenance. This paper will
also introduce a case study patient who was found to have LADA. The case study will include
the patient’s background history and physical, discussion of the outpatient office visits, the
nutrition care and medications prescribed to the patient.
Discussion of Medical Condition: Diabetes is a very prominent disease in the United States.
With obesity on the rise, diabetes affects 25.8 million Americans, which is 8.3% of the
population as of 2011 (1). There are about 1.9 million new cases of diabetes a year. Because
there are different types of diabetes—type 1, type 2, gestational, and now latent autoimmune
adult onset—the diagnostic tools used are important to differentiate between.

Diabetes is defined by the American Diabetes Association (ADA) as a group of diseases
where the body cannot utilize or produce insulin correctly, which results in elevated blood sugar
levels (1). There are several different types of diabetes characterized by the differences in the
inability to use or make insulin. Insulin is a key hormone in glucose metabolism (1). When
carbohydrates from foods we eat enter the blood stream, the digestive tract breaks down the
carbohydrates into glucose that is used for energy. Insulin is needed to bring glucose from the
blood into the cells to be metabolized properly (1). Without insulin, glucose builds up in the
blood stream and causes hyperglycemia, or high blood sugar (1).
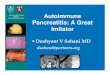
Specifically, type 1 diabetes mellitus (T1DM) is a disease where the body can no longer
make insulin due to the loss of beta cell production (1). Beta cells are made by the islet of
Langerhans in the pancreas (2). Beta cells release insulin in
response to an increase of blood glucose (2). Without the beta
cells, there is no insulin to help maintain normal blood glucose
levels—causing T1DM. In T1DM, there is an overcompensation
of the immune system, which attacks the body and terminates the
pancreas’ ability to make insulin (1). Thus, T1DM is an
autoimmune disease. Type 1 diabetes is termed insulin-dependent
diabetes and was previously known as “juvenile diabetes”
because it was most prevalent in children. Due to an increase in average age of diagnosis of
diabetes, it is no longer called “juvenile diabetes” (1).
Type 1 diabetes is most common among children and young adults (1). Caucasians,
especially Scandinavians have the highest prevalence compared to other ethnicities (3). It is
especially rare among ethnicities such as African and Asians (3). Diabetes is more prevalent in

men than women (1). According to the ADA, 13.0 million men have diabetes, compared to 12.6
million women (1). There are many other factors that may increase the risk of developing type 1
diabetes such as breastfeeding and other environmental triggers (1).
Self-administration of insulin is the main treatment for type 1 diabetes; however it is not
a cure. Children and adults with T1DM need to take insulin throughout the day to maintain as
close to normal blood glucose levels as possible and must account for carbohydrates consumed.
Therefore, people with T1DM need to count their carbohydrates and calculate insulin doses
needed to maintain normal blood sugar levels. Insulin can be administered through subcutaneous
injections or with the use of an insulin pump. With tight control, health risks caused by type 1
diabetes can be minimized.
There are two main types of insulin—rapid acting and long acting. Rapid acting insulin is
used to correct high blood sugars using a calculated amount. For example, some diabetics may
take 1 unit of rapid acting insulin for every 50 mg/dl over their goal blood sugar, called an
insulin sensitivity factor. Rapid acting insulin medications include Humalog, Novalog, and
Apidra (4). Rapid acting insulin begins working within 15 minutes of injection. Peak time can
last between 30 and 90 minutes. This insulin can also be used for carbohydrate coverage. Similar
to blood sugar corrections, diabetics may also have a carbohydrate coverage calculation. For
example, a carbohydrate to insulin ratio may be determined for every 15 grams of carbohydrates,
1 unit of insulin may be administered. Long acting insulin is the other main type that serves as a
basal rate that lasts 24 hours to maintain insulin levels and to keep blood sugar levels as close to
normal as possible throughout the day. Lantus and Levemir are two examples of long acting
insulin medications that are normally administered subcutaneously once a day (4). If a patient
were using an insulin pump, only rapid acting insulin would be used. Patients can administer a

bolus for food coverage and blood sugar correction. The ratios are programmed into the pump,
simplifying dosing for the pumper. Instead of taking a long acting insulin such as Lantus, the
pump has a setting for a basal rate that can be manipulated over 24 hours to maintain blood
glucose levels.
Signs and symptoms for undiagnosed T1DM include weight loss, thirst, hunger, fatigue
and frequent urination (1). Weight loss is caused by the body’s reaction to having insufficient
insulin. The body needs glucose in the cells—not in the blood--to be used as energy. The body
reacts by going in to starvation mode, utilizing protein and fat as energy sources since the
glucose is not available (1). Ketones can be produced and weight loss can occur. Diabetic
ketoacidosis (DKA) is often present at time of diagnosis of T1DM, where the body is breaking
down fat for energy, creating a byproduct of ketones (1). Patients can become very ill when this
happens. Side effects of ketones in extreme cases can result in a diabetes coma, or even death.
The diagnostic criteria for T1DM includes positive tests results for islet cell antibodies.
Insulin autoantibodies are often detected as well as islet antigen 2 in newly diagnosed patients.
GAD antibodies are commonly found at diagnosis for adults, not as much for children. Insulin/C-
peptide levels are very low at diagnoses (5). Other markers of diabetes include certain antibodies,
autoantibodies, insulin levels, specific gene markers, and C-peptide levels. Without the beta
cells, the body cannot produce the insulin needed to control blood glucose levels. Therefore,
screening for T1DM often includes testing antibody levels. Insulin levels are also tested because
if a patient is type 1 diabetic, their insulin levels will be low. C-peptide is an amino acid that
reflects endogenous insulin levels because it is a byproduct of insulin. Because C-peptide reflects
insulin levels, it can also help diagnose T1DM because it shows that the body is not making
insulin (5).

The antibody tested to diagnose T1DM is called glutamic acid decarboxylase
autoantibody (GAD). GAD is often a predictor of insulin dependency because if there is a
presence of GAD antibody it reacts with pancreatic islet cell antigens, leading to beta cell
damage and interferes with insulin production (6).
Type 2 diabetes (T2DM) is most commonly linked to obesity and occurs when the body
makes the insulin needed, but does not use it properly or resists it (1). T2DM accounts for 90-
95% of people with diabetes and only 5-10% of people with diabetes have type 1 (1). According
to the International Diabetes Federation, there is an annual 3% increase in incidence of type 1
diabetes which accounts for over 475,000 children under the age of fourteen, worldwide, with
type 1 diabetes (3). In comparison to the 475,000 who have type 1 diabetes in the world; 15
million of people have type 2 diabetes, just in the United States (1,2).
T2DM normally occurs in adulthood and is characterized by either insufficient
production of insulin and/or insulin resistance. Although people with T2DM still produce insulin,
the liver, fat, and muscle cells do not use insulin properly (4). Without sufficient amount of
insulin or if the insulin is not properly utilized to compensate for the amount of insulin secreted,
hyperglycemia occurs and can cause damage to the nerves resulting in co-morbidities such as
cardiovascular diseases, neuropathy and nephropathy (1).
T2DM can be caused by different factors. Genetics play a major role in the risk of
developing T2DM (4). Some researchers have found that the combination of certain genes can
cause the development of diabetes (4). Certain ethnic groups are also found to have higher risk
for T2DM (4). Obesity is another main factor in T2DM. Central obesity, where there is excess
fat around the middle stomach, can cause insulin resistance because the adipose tissue produces
hormones that cause damage to the blood vessels (4). The combination of damage to the blood

vessels and insulin resistance greatly increases the risk for T2DM and cardiovascular diseases
(4). Another risk factor is abnormal glucose production by the liver. Normally, the pancreas
produces glucagon when glucose levels in the blood are low.
Glucagon then stimulates the liver to release glucose into the
blood to avoid hypoglycemia (4). When carbohydrates are
consumed and glucose levels rise, the liver stores the extra
glucose to use later. Sometimes the liver continues to release
glucose when it is not necessary, but researchers do not fully
understand why (4). The extra glucose causes hyperglycemia
and can lead to T2DM.
According to the ADA, the diagnostic criteria for
T2DM includes fasting plasma glucose ≥126 mg/dl, oral glucose tolerance test (OGTT) ≥200
mg/dl, or a hemoglobin A1C ≥6.5% (1). Patients with T2DM do not show positive results for
islet cell antibodies or insulin autoantibodies and rarely screen positive for glutamic acid
decarboxylase (GAD) antibody.
FPG is a glucose test taken after the patient has fasted for at least 8 hours and is most
commonly used to test for diabetes because it is the most convenient. An OGTT is given after the
patient has fasted for 8 hours and two hours after the patient is given 75g of glucose dissolved in
water. A hemoglobin A1C is a blood test that reflects a patient’s blood glucose control over the
last 3 months. The result is given as a percentage and shows glycated hemoglobin in the blood
(1). Most physicians or endocrinologists aim for patients to have an A1C ≤ 7%.

Signs and symptoms for T2DM are similar to those of T1DM including thirst, hunger,
fatigue and frequent urination. However, weight loss is not a symptom of T2DM because there is
still insulin present. Symptoms of T2DM appear more gradually and are more subtle than T1DM
so T2DM may go undiagnosed for some time (4).
Although diet and physical activity can improve the control of blood sugars, treatment of
T2DM usually begins with the use of oral medications. There are many different categories of
oral medications used. Three of the main types are biguanides, sulfonylureas, and
thiazolidinediones. Biguanides are distributed as Metformin, Glucophage, and other brand
names. There mode of action includes inhibiting the release of glucose from the liver and
improve sensitivity to insulin (7). Sulfonylureas stimulate the release of insulin and are sold in
the brand names of Glipizide, Glimepiride, and Glyburide. Because they stimulate insulin, one
risk of this medication is hypoglycemia (7). Patients on these medications must not skip meals to
avoid hypoglycemia. Thiazolidinediones are sold as Avandia and Actos. There mode of action
includes improving sensitivity to insulin and inhibiting the release of glucose from the liver (7).
Dipeptidy peptidase-4 D (DDP-4) inhibitors act similarly to thiazolidinediones and is popularly
sold as Januvia (7). Some oral medications can be combined to achieve best glycemic control.
When oral medications are not enough to achieve glycemic control, insulin may be added as part
of the regimen.
Latent autoimmune diabetes in adults was first discovered by doctors in the 1970s (8). It
is said that doctors found LADA by accident while studying ways to detect autoantibodies that
are used to diagnose people with type 1 diabetes (8). LADA is sometimes called type 1.5
diabetes and accounts for 10% of phenotypic type 2 diabetics (8). Many are calling it a
combination of both type 1 and type 2. As of recent, there is uncertainty about how to diagnose

LADA. Because these patients are adults, most assume T2DM. Oral medications are then
prescribed, but do not always help. Once further lab work is done, it is shown that these patients
also have autoantibodies, similar to a type 1 diabetic. These patients will slowly become insulin
dependent, usually within 6 months (8). These patients have autoantibodies, such as GAD, and
relatively low C-peptide levels, proving that they are not producing enough insulin. They have a
higher rate of developing insulin dependency than a type 2 diabetic (8). LADA shares features of
both type 1 and type 2 diabetes, which makes it difficult to diagnose.
Because LADA is a blend of the two types of diabetes, the question arises how to
diagnose LADA. When an adult patient shows signs or symptoms of diabetes, physicians may
see one or more parameter such as an A1C, FPG, or OGTT and diagnose them with T2DM.
These patients are prescribed oral medications that would normally benefit a type 2 diabetic,
such as a sulfonylurea or biguanide, but because these patients do not have only T2DM
pathophysiology, the oral meds do not help and they are then put on insulin. If patients were
screened for autoantibodies at time of diagnosis, they could be detected earlier for LADA and
treated properly initially. Because LADA is so rare, patients are not normally screened for
autoantibodies.

How to diagnose LADA: In a Polish study done by Gorska, et al. in 2012, researchers aimed
to distinguish the characteristics and incidence of LADA (9). Researchers observed the
population of Bialystok, Poland (188,738). Information was obtained from primary care
physicians. Subjects were aged 20-64 years old and were followed from January to December of
2003. Results showed that 231subjects presented with new cases of diabetes in 2003, however
only 212 of those participated in the study. Of those, 54.2% were male. The mean HbA1C was
7.2% and body mass index (BMI) in the diabetic population was 29. Researchers also looked
insulin and C-peptide levels, GAD antibody (GADA), anti-insulin antibody (IAA).
Results also showed that 10.3% of participants were IAA/GADA positive. There were
7% positive for anti-glumatic acid carboxylase antibody and 4.5% for IAA. There were some
interesting correlations found with patients diagnosed with LADA. Those who had the presence
of autoantibody were also lower in age, had a lower BMI, C-peptide, insulin, and beta cell
function when compared to those with type 2 diabetes. They were also less resistant to insulin.
Interestingly, 3.3% of diabetics were diagnosed with type 1. Three of these tested positive for
autoimmune antibody and 4 tested negative.
Overall in this community, LADA was detected in 10 per year per 100,000 people and
accounted for 8.9% of newly diagnosed cases with diabetes. These results are similar to those of
studies done in Whales, Finland and Sweden. The researchers used GAD to identify LADA and
believe that although most believe that LADA is a blend of T1DM and T2DM, LADA can be
distinguished simply by antiautobodies and not a combination of parameters (9). When
compared to type 2 diabetic patients, the LADA patients had similar fasting plasma glucose

levels and HbA1C levels. Researchers say this may suggest that there is a slow progression and
maybe asymptomatic onset of LADA (9).
Because 36% of patients with LADA tested positive for IAA, researchers say it may be
useful in diagnosing patients (9). Overall, LADA presented very similar to type 2 diabetes,
except with significant beta cell dysfunction, proven by the GAD, and lower insulin resistance.
The study concluded that testing type 2 diabetics for autoantibodies and IAA may be beneficial
in detecting LADA earlier, especially in those who have a lower BMI and who are younger (9).
This study brings up a valid point of how to diagnose LADA. It is commonly accepted
that the presence of autoantibodies in adults who appear to have type 2 diabetes differentiates
them to be LADA, but not all physicians will screen all type 2 patients. It is important that
patients with LADA often have a lower BMI, C-peptide, and insulin resistance and that insulin
dependence will be necessary in time. The sooner physicians recognize that the patient has
LADA rather than type 2 diabetes, the sooner they can begin proper treatment.
In a review article titled “Latent autoimmune diabetes of adults: From oral hypoglycemic
agents to early insulin,” written by Resham R. Poudel published in the Indian Journal of
Endocrinology and Metabolism in 2012, the treatment and diagnosis of LADA is discussed (10).
Poudel discusses that when patients are initially treated with oral hypoglycemic agents (OHA)
and patients fail with OHA, it gives a clue that this patient may actually have LADA. Five
clinical features from a retrospective study (11) were used to help identify LADA:

The younger age and lower BMI agree with the Polish study findings as far as clinical
markers for LADA (11). Fourlanos’ markers also include the normal acute symptoms of diabetes
including thirst, increased urination and unintentional weight loss, as well as a personal or family
history of autoimmune disease. The HLA gene marker is another clinical feature that is being
researched in being linked to type 1 diabetes. Specifically, the human leukocyte antigen (HLA)-
DR3 or HLA-DR4 has been found to be common in whites with type 1 diabetes (11). Research
has shown that an environmental factor can trigger the HLA gene to be expressed, which is
linked to the overcompensation of the immune system, leading to the beta cell’s inability to
produce insulin in type 1diabetes (10).
In a study by Andersen, et al in 2010, researchers looked at the differences between
patients over the age of 35 who were diagnosed with type 1 diabetes, type 2 diabetes, and LADA
(12). LADA was defined in this study to be diabetic patients that were GADA positive who did
not have insulin therapy for the first 6 months. This research was conducted by combining
cohorts of two separate studies. One group included patients older than 35 who were diagnosed
with LADA, patients less than age 20 with type 1 diabetes, and GADA positive type 2 diabetics
(from the Botnia study group). The other group observed was from the FinnDiane study; type 1
diabetics over the age of 35. All patients underwent OGTT, serum insulin, C-peptide levels,

lipids, and GADA screenings. A series of HLA alleles were also tested to be able to distinguish
the different genetic makeup between the diabetic patients.
When comparing the four genotypes, 82.1% of T1DM <20 years of age had two or more
risk genotypes followed by 74.4% of T1DM >35 years of age, LADA patients 54.1%, and
T2DM 38.7%. LADA patients also had a higher BMI than TIDM >35 year old and higher lipid
concentrations of T1DM >35 years old. When compared to T2DM, LADA had lower insulin,
lipids and BMI. The higher the GAD in LADA patients, the more significant trend toward lower
insulin secretion, BMI, and lipid levels. LADA patients with higher amounts of GAD had higher
amounts of C-peptide when compared to T1DM >35 years of age and LADA patients with lower
amounts of GAD had lower C-peptide levels than T2DM. There were no significant differences
in the two groups of T1DM, aged <20 and >35 (12).
This study proved that there are genetic differences in T1DM, LADA, and type 2
diabetes. Specifically, there is a genetic difference between T1DM diagnosed after age 35 and

LADA. This is important because it will help future medical professionals differentiate between
LADA and type 1 and 2 when an older adult is diagnosed with diabetes, needing insulin within 6
months and has a lower BMI. The study concluded that LADA with high GADA were more
similar to type 1 diabetes, but not identical. LADA with low GADA were more similar to type 2
diabetics. These are all key findings in defining LADA based on the most current research.
LADA is less recognized and under-diagnosed because it is rare and not as obvious in its
characteristics as type 1 or type 2 may be. It has characteristics from both types and because
most LADA patients are adults, it is not apparent to check autoantibodies or C-peptide levels at
diagnosis. Patients with LADA will experience a decline in their beta cell function, causing
insulin dependency within 6 months of diagnosis whereas type 2 diabetics will only need insulin
if oral medications are not sufficient enough to achieve glycemic control. The main difference
between type 2 and LADA is the presence of autoantibodies and low C-peptide levels in LADA
(13).
To summarize, LADA is a rare type of diabetes where the beta cells eventually lose their
ability to produce insulin, causing hyperglycemia. LADA is commonly mistaken for T2DM, due
to the late onset of age >30 years. Oral medications may not help control blood glucose levels,
because the liver and insulin resistance are not the main culprits causing hyperglycemia. Patients
with LADA test positive for autoantibodies and lower C-peptides levels proving that it is beta
cell malfunction, opposed to insulin resistance and/or over production and release of glucose
from the liver. Individuals with LADA will have better glucose control if they are put on an
insulin regimen in the earlier stages of diagnosis opposed to oral medications. Risk factors for
LADA include a family history of autoimmune diseases, a lower BMI (<25 kg/m2), and age <50.

Discussion of Medical Nutrition Therapy: Medical nutrition therapy for LADA is similar to
that of treating type 1 and 2 diabetes. The goal for diabetics is to achieve glycemic control as
close to normal as possible. Depending on the type of diabetes, treatment can be approached in
several different ways including nutrition therapy, insulin therapy, exercise, and other
medications.
Nutrition is a key component in treating all types of diabetes. Carbohydrates can play a
big role in controlling blood glucose levels because they increase BGs. Carbohydrate counting is
a method taught to diabetics by dietitians, nurses, and certified diabetes educators. One serving
of carbohydrates is considered to be 15 grams (g) (14). Each individual will have a different goal
of carbohydrate limits per day and per meal. A typical pattern would be a range of 45-60g per
meal and 15-20g per snack (14). Diabetics are taught how to count carbohydrates using portion
sizes, nutrition labels and other resources. Along with being consistent with the amount of
carbohydrates consumed, the type of carbohydrates is also helpful in controlling BGs. Complex
carbohydrates take longer for the body to digest and cause less of a spike and drop in BGs than
simple carbohydrates do (Figure
1).
Similar to all well-
balanced meals, a healthy diabetes
calorie intake can be estimated as
50-60% carbohydrate, 20-30%
protein, and roughly 20% fat.
Protein intake should be focused on lean proteins such as lean meats (chicken, turkey, fish), low-
fat dairy and legumes. Foods that are low in saturated fats, higher in mono- and polyunsaturated

fats and no trans fats are also recommended. These well-balanced diet recommendations will
help lower body fat and decrease risks for cardiac diseases that are often seen with diabetes (13).
Physical activity can also help control BG levels among other benefits (1). Aerobic
exercise can help improve cardiovascular health by increasing heart and breathing rates, and
working other major muscle groups (1). The cardiovascular benefits of physical exercise are
especially helpful in the treatment of diabetes and in decreasing risks associated with
complications of diabetes. Strength training is another form of physical exercise that has a major
benefit of helping lower BG levels as it fatigues and works muscles. This also helps build strong
bones and burns calories (1). Flexibility training also focuses on muscles by strengthening and
stretching them. Having flexible muscles helps prevent injury.
Insulin therapy is always needed in cases of T1DM and sometimes with T2DM. In cases
of LADA, insulin is usually needed within 6 months of diagnosis due to the slow progression of
beta cell dysfunction. Insulin therapy with type 1 diabetics is initiated at diagnosis (15). Insulin
doses for LADA are similar to those of T1DM described earlier.
In a Swedish study done by Thunander, et al published in 2011in the European Journal of
Endocrinology the treatment of LADA was examined. In this three year long, randomized
controlled study, 37 patients were divided into two groups (13). All participants were taken from
Lund and Kronoberg counties in Southern Sweden and were adults ≥30 years old, diagnosed
with diabetes, and were considered non-insulin requiring at diagnosis. They were all GAD and/or
ICA positive, which would put them in the LADA category. One group was treated as the
intervention group and consisted of 20 participants. These participants were started on early
insulin therapy of an injection of 2-6 units of Lantus every evening. The other 17 participants

served as the control group and received regular treatment of diet modification and oral
medications such as Metformin. Both groups had the same BG goal ranges for pre- and post-
prandial BGs. Both groups received insulin or medication adjustments at the discretion of the
physician. If the one injection of Lantus was not sufficient in treating BGs, doses were increased
in increments and/or fast-acting insulin was added to be administered before meals (13).
Results of this study showed that A1C levels in the control group increased significantly
after 36 months. In the intervention group, A1C levels had no significant difference after 36
months. The preservation of beta cell function could not be determined; however autoantibody
and C-peptide results were similar in both groups. Although this study was small, it agrees with
other studies an effective treatment for LADA patients is early insulin therapy. Early insulin
therapy helped glycemic control more than oral medications alone. Since LADA has
autoimmune components that prove to slowly decline beta cell function, it makes sense that early
insulin therapy is most effective because these patients will eventually not be able to produce
their own insulin and will need synthetic administration (13).
Treatment of LADA is not yet fully agreed upon, but more studies are coming out that
are ending with a recommendation of early insulin therapy. Because we have a good amount of
evidenced based research on how to treat type 1 and 2 diabetes, LADA patients may need a
combination of these two treatment plans, including early insulin therapy.
Presentation of Patient: The patient chosen for this case study was from Helwig Health
Diabetes Center, seen as an outpatient. My case study was done a bit differently than planned. I
chose my topic of LADA because it was a topic that I thought would be a great learning
experience, and was something I wanted to understand more thoroughly. I had not seen a patient

diagnosed with LADA during my internship so during my time spent at Helwig Health Diabetes
Center as the diabetes emphasis intern, I asked the staff if there was a recent patient they had
seen with LADA that I could research. Unfortunately, I was unable to meet and speak with the
patient, however I was given access to look through her medical chart to learn how the diagnosis
of LADA occurred and how her treatment plan was altered as they changed her diagnosis from
T2DM to LADA.
Patient is CK, a 63 year old female who was diagnosed T2DM and hypothyroidism in
August of 2011. CK is 149.86cm, or 59 inches. Weight history includes: 164 pounds in
September 2011, 168 pounds in February 2012, and 173 pounds in December 2012. From
September 2011 to December 2012, the patient gained a total of nine pounds. The patient’s past
medical history includes hyperlipidemia, hypertension, hypercholesterolemia, hypothyroidism,
arthritis, and uncontrolled diabetes (type 2 in August 2011). CK’s past surgical history is
insignificant with a c-section in 1974. Her family history includes that her mother passed away
with CVA at age 78 and her father passed away post operation at age 78 as well. She has three
sons, one with Celiac disease. It was noted that Celiac disease is an autoimmune disease, so
family history is positive for autoimmune diseases. Her social history as of August 2011 shows
that she consumes alcohol occasionally, does not exercise regularly, does not use drugs, no
caffeine and has never smoked. Her current BMI is 33 kg/m2. She has a regular pulse of
78/minute with a blood pressure of 138/82.
During CK’s first follow-up visit in September 2011, her complete medication list was as
follows:
1) Cozaar 50 Mg Tabs (Losartan potassium) .... Daily
2) Synthroid 50 Mcg Tabs (Levothyroxine sodium) .... Daily

3) Famotidine 20 Mg Tabs (Famotidine) .... Daily
4) Hydrochlorothiazide 25 Mg Tabs (Hydrochlorothiazide) .... 1 daily
5) Aspirin Adult Low Strength 81 Mg Tbec (Aspirin) .... Daily
6) Ferrex 150 Plus Caps (Fe-succ ac-c-thre ac caps) .... Daily
7) Metoprolol Tartrate 25 Mg Tabs (Metoprolol tartrate) .... Daily
8) Simvastatin 40 Mg Tabs (Simvastatin) .... Daily
9) Potassium Chloride Cr 10 Meq Cr-tabs (Potassium chloride) .... Daily
10) Nexium 40 Mg Cpdr (Esomeprazole magnesium) .... Prn
11) One Touch Delica Lancets Misc (Lancets) .... Tests 2 times daily. dx code:250.02
12) Onetouch Ultra Test Strp (Glucose blood) .... Tests 2 times daily. dx code:250.02
13) Metformin Hcl 1000 Mg Tabs (Metformin hcl) .... Take one tablet twice a day
14) Lantus Solostar 100 Unit/ml Soln (Insulin glargine) .... 30 units hs (This was added at first
follow up appointment). 15) Bd Disp Needles 30g X 1/2" Misc (Needle (disp)) .... Use daily
During this visit, Glimepiride 2mg tablets that was previously prescribed to be taken
twice a day was stopped and Lantus insulin therapy was initiated. All other physical
examinations appeared normal. No retinopathy was noted from previous medical chart. No
laboratory values were noted to be abnormal other than an A1C on November 15, 2012 of
11.3%. No other previous A1C is found. I did not have any records of blood glucose levels
recorded.
Discussion of Medical/Surgical Hospital Course: The patient was seen in the clinic on
September 18, 2011 by Dr. Donald Barilla for a diabetes follow-up. On this date, the patient
denied any polyuria, polydipsia, or polyphagia. She denies self-managed hypoglycemia,
nocturnal hypoglycemia, fatigue, and blurred vision. The patient denies any parasthesia,
neuropathic pain, angina, edema, skin ulceration, SOB, nausea, vomiting, diarrhea, constipation,
orthostatic symptoms, eating disorder, and intermittent claudication. Since the last visit, the
patient admits to home blood glucose monitor (HBGM) testing, carbohydrate counting, and
dietary compliance is good. Patient notes eye care since last visit including been seen by eye
physician and no retinopathy. The patient also presented today for a hypothyroidism. The patient

denies cold intolerance, weight gain, weakness, dry skin, constipation, lethargy, and facial
swelling, which are all possible side effects or symptoms of either disease or medications used.
Patient denies depression, anxiety, chest pain, sense of neck fullness, difficulty swallowing,
coarse hair, and dry skin. Previous evaluation includes lab studies and + TPO AB. Risk factors
for hypothyroidism include FH Hashimoto's.
At this time, the patient had been diagnosed two months prior with T2DM and was
prescribed Metformin and Glimepiride. The patient tested her blood sugars twice a day and had a
“very acceptable diet.” With an elevated A1C and with little success in controlling blood glucose
levels with oral agents, more labs were drawn. Laboratory values were reviewed during this visit,
and the patient tested positive for GAD antibody at 250, with normal ranges being under 3 and
C-peptide was 1.1. At this point, the patient was said to have “slowly evolving form of one
diabetes, LADA which will require insulin.” CK was taught how to use insulin and was told to
test her blood glucose levels twice a day and to send in her record of blood sugars every two
weeks. Her Lantus was started at 15 units at bedtime and was instructed to increase by 15 units
in one week if blood sugars in the morning were over 150 mg/dL. Glimepiride was removed
from her medication list.
The patient was seen for a follow-up three months later. CK complained of weight gain
and fatigue, which may be related to hypothyroidism if it is not under control, but denies
polyuria, polydipsia, polyphagia, nocturia, and blurred vision. The patient again denies any
parasthesia, neuropathic pain, angina, edema, skin ulceration, SOB, nausea, vomiting, diarrhea,
constipation, orthostatic symptoms, and eating disorder. Since the last visit the patient admits to
HBGM testing, carbohydrate counting, and dietary compliance is good. Patient notes eye care

since last visit including been seen by eye physician and no retinopathy. AIC is 11.3%. No other
medical or social history changed since the last visit.
CK had reached the 30 units of Lantus and was still experiencing hyperglycemia. The
physician added Janumet 50/1000mg twice a day to help with blood glucose control. Janumet is
a combination drug of Januvia (a DDP-4) and Metformin (a biguanide). The physician also
reordered a C-peptide in 6 months and an A1C in 3 and 6 months.
The next three month visit showed continued uncontrolled blood glucose levels and an
increased A1C of 13.1%. At this point, the physician decided to discontinue the Janumet and
initiated intensive insulin therapy and included a rapid-acting insulin, Humalog. The patient
received education on dosing and injecting insulin using a FlexPen rather than insulin vial and
syringe. CK was instructed to cover her meals using an insulin to carbohydrate ratio of 1 unit of
Humalog for every 10g of carbohydrate. She was also given an insulin sensitivity factor (ISF) of
1 unit of insulin for every 25 mg/dL over 120 mg/dL. Janumet was discontinued from her
medication list and she was asked to send in her records of blood sugars every month to touch
base with the educators. She was also asked to increase her blood sugar testing to four times a
day. No other significant change in medical history. Patient did report that she had started
physical activity on a regular basis. At the end of the charting reviewed, the patient was
discontinued from all oral medications to treat diabetes and was on intensive insulin therapy,
similar to a type 1 diabetic.
Discussion of Nutrition Care: The medical nutrition therapy for this patient includes
nutrition education on carbohydrate counting, weight loss, and nutrition-related laboratory
values. If I were to see this patient as an inpatient, I would have started with diabetes education
as a newly diagnosed diabetic. Calculated needs for this patient would be aimed for weight loss

since her BMI was 33 and the patient reported weight gain. I would estimate 1572-1965
calories/day based on 20-25 kcal/78.6 kg. Protein needs would be about 0.8g/kg for maintenance
and no acute stress or need for increased protein. This would equate to 63g of protein per day.
Fluid needs are about 25-30 ml/kg based on age and no increased/decreased needs, which equals
about 2000-2300 ml/day. Multiple PES statements could be made for this patient. If I were
assessing this patient, I would most likely prioritize her need for diabetes education and would
document my PES statement to be: Altered nutrition-related laboratory values related to
uncontrolled diabetes as evidenced by A1C 13% (increased from 11.3%), elevated BGs, C-
peptide 1.1 and positive GAD. My intervention term would be nutrition education. I would
monitor and evaluate the patient’s endocrine/blood glucose profile with a goal A1C of ≤7.0%
and to maintain blood sugars between 70 and 120.
If this were a patient seen in the hospital setting, I would provide her with the Sodexo
educational handout titled “Ready, Set, Carb Counting!” It is a good introduction to carbohydrate
counting and I find that when I go through and highlight the more important parts, patients are
able to follow along with me easily. The patient’s chart stated that she was compliant with
carbohydrate counting, so during the interview process, I would ask her if she has received
formal education on carb counting before, and if she would like a refresher on it. The main parts
reviewed include what food groups have carbs in them, the amount counted as a serving or
choice of carb, how to read a label, and carbohydrate goals for women at each meal and snack. I
would also explain the importance of consistent carbohydrate intake to maintain glycemic
control.
During the interview I would also ask the patient if she wanted any information on
weight loss since it was on her list of complaints documented in her chart. Managing her weight

would also be beneficial in her diabetes control. Weight loss includes monitoring intake of
calories, which would also help her monitor intake of carbohydrates. Overall healthy eating is
especially beneficial for people with diabetes. I would review a healthy overall diet and show the
visual of a plate—half the plate fruits and vegetables, a quarter of it grains and a quarter of it
protein. I could also to a 24-hour recall and then show other healthier options for her food
choices. I also would give resources to look up foods such as the Calorie King book or app for a
smart phone, as well as the MyFitnessPal app. Physical activity would also be a good topic to go
over with her, since it was something that was new to her and with diabetes, it is important to go
over signs and symptoms of hypoglycemia and how to treat it. To summarize, I would recap
what the A1C means, how to lower it to the goal, the importance of carb counting and insulin
administration, and tips on weight loss.
The doctor’s last list of medications were as follows:
1) Cozaar 50 Mg Tabs (Losartan potassium) .... Daily
2) Synthroid 50 Mcg Tabs (Levothyroxine sodium) .... Daily
3) Famotidine 20 Mg Tabs (Famotidine) .... Daily
4) Hydrochlorothiazide 25 Mg Tabs (Hydrochlorothiazide) .... 1 daily
5) Aspirin Adult Low Strength 81 Mg Tbec (Aspirin) .... Daily
6) Ferrex 150 Plus Caps (Fe-succ ac-c-thre ac caps) .... Daily
7) Metoprolol Tartrate 25 Mg Tabs (Metoprolol tartrate) .... Daily
8) Simvastatin 40 Mg Tabs (Simvastatin) .... Daily
9) Potassium Chloride Cr 10 Meq Cr-tabs (Potassium chloride) .... Daily
10) Nexium 40 Mg Cpdr (Esomeprazole magnesium) .... Prn
11) One Touch Delica Lancets Misc (Lancets) .... Tests __4__ times daily. dx code:250.02
12) Onetouch Ultra Test Strp (Glucose blood) .... Tests ___2___ times daily. dx code:250.02
13) Lantus Solostar 100 Unit/ml Soln (Insulin glargine) .... 30 units twice daily
14) Humalog Kwikpen 100 Unit/ml Soln (Insulin lispro (human)) .... 15 units tid
15) Bd Pen Needle Mini U/f 31g X 5 Mm Misc (Insulin pen needle) .... Use 4 daily
Summary: In summary, this patient was a good example of the diagnosis process that is most
likely typical for someone with LADA. Because the patient was age 62 and showed signs and
symptoms of diabetes, she was put on oral medication which was unsuccessful in achieving

glycemic control even with an acceptable diet and eventually even regular exercise. Once the
patient was shown to be positive for GAD and had a C-peptide of 1.1, the physician discontinued
the Glimepiride, because it is known to be ineffective with a low C-peptide, but continued
Janumet and added Lantus. This was still unsuccessful and the patient actually had an increase in
her A1C. At that point the patient was finally put on intensive insulin therapy as a type 1 diabetic
would have. If I could see the latest chart entry, I would bet that the patient’s A1C has come
down since then. The fact that the patient was gaining weight may be due to the newly diagnosed
hypothyroidism, but I would assume that the physical activity and increase in glycemic control
would help her lose. Unfortunately, I do not have any further information on the patient at this
time. I did want to make mention that I thought it was interesting how this patient met some risk
factors that may separate her from type 2 to LADA. She has a family history of an autoimmune
disease, her son with celiac disease. She did have a BMI that qualified her as obese, but may still
be lower than the average BMI for T2DM. It would be interesting to test her genes to see if she
was positive for the HLA gene.
This case study had been a very beneficial learning experience for me. I feel that not only
did I gain knowledge on LADA, but now I am also more familiar with the diagnostic criteria for
T2DM and T1DM.
Medical Bibliography:
Medication Generic/Brand
name
Use Food/drug interactions
Levothyroxine sodium Synthroid Hypothyroidism Must take 1 hour before
food intake

Metformin (biguanide) Glucophage,
Fortamet
T2DM; decreases
liver glucose output,
some decrease
insulin resistance
May cause
nausea/diarrhea,
metallic taste. Do not
use with alcohol abuse,
avoid with liver and
renal disease.
Terminate at
pregnancy.
Ferrex Ferrex-150 Anemia Take on an empty
stomach
Potassium Chloride N/A Hypokalemia Take with food or right
after meal.
References
1. Diabetes Statistics. American Diabetes Association. 2011.
http://www.diabetes.org/diabetes-basics/diabetes-statistics/.
2. Beta Cell Biology Consortium. Insulin-From Secretion to Action. 2002-2013.
http://www.betacell.org/content/articleview/article_id/1/.
3. Genetic Health. (2011). Diabetes—What is Type I Diabetes.
http://www.genetichealth.com/dbts_what_is_type_1_diabetes.shtml.
4. U.S. Department of Health and Human Services. National Diabetes Information
Clearinghouse. Types of Insulin. 2012. http://diabetes.niddk.nih.gov.
5. Poudel, R. Latent autoimmune diabetes of adults: From oral hypoglycemic agents to early
insulin. Indian Journal of Endocrinology Metabolism. 2012. 16 Suppl 1:S41-46.
6. von Wartburg, L., Phillips, R. The Story of GAD. Diabetes Health. 2010.
http://diabeteshealth.com/read/2010/03/23/6611/the-story-of-gad/.
7. Type 2 Diabetes. Diabetes Treatment: Medications for type 2 diabetes. Mayo Clinic
Staff. 2011. http://www.mayoclinic.com/health/diabetes-treatment/DA00089.

8. Gebel, E. The Other Diabetes: LADA, or Type 1.5. Latent autoimmune diabetes in adults
is gradually being understood. Diabetes Forecast. 2010.
http://forecast.diabetes.org/magazine/features/other-diabetes-lada-or-type-15
9. Szepietowska, Gorska, Puch, Glebocka, Szelachowska. Latent autoimmune diabetes in
adults in a population-based cohort of Polish patients with newly diagnosed diabetes
mellitus. Archives of Medical Science. 2012. 8(3): 491-5.
10. Poudel. Latent autoimmune diabetes of adults: From oral hypoglycemic agents to early
insulin. Indian Journal of Endocrinology Metaobolism. 2012. 16(Suppl1):S41-S46.
11. Fourlanos, Perry, Stein, Stankovich, Harrison, Colman. A clinical screening tool
identifies autoimmune diabetes in adults. Diabetes Care. 2006. 29(5): 970-975.
12. Anderson, Lundgren, Tuomi. Latenet Autoimmune Diabetes in Adults Differs
Genetically from Classical Type 1 Diabetes Diagnosed After the Age of 35 Years.
Diabetes Care. 2010. 33(9): 2062-2064.
13. Thunander, Thorgeirsson, Torn, Petersson, Landin-Olsson. B-cell function and metabolic
control in latent autoimmue diabetes in adults with early insulin versus conventional
treatment: a 3-year follow-up. European Journal of Endocrinology. 2011. 164(2): 239-
45.
14. Academy of Nutrition and Dietetics. Carbohydrate counting for people with diabetes.
2012.
15. Brophy, Davies, Mannan, Brunt, Williams. Interventions for latent autoimmune diabetes
in adults (LADA). Cochrane Database of Systematic Reviews. 2011. (9): CD0006165.