-
8/10/2019 Kuliah pneumonia 25-5-12
1/75
-
8/10/2019 Kuliah pneumonia 25-5-12
2/75
Definition
Pneumonia is an acuteinfection of the
parenchyma of thelung, caused by
bacteria, virus, parasiteetc.
Pneumonia may also be
caused by other factors
including X-ray,chemical, allergen
-
8/10/2019 Kuliah pneumonia 25-5-12
3/75
Epidemiology
The morbidity and mortality of pneumonia
are high especially in old people.
-
8/10/2019 Kuliah pneumonia 25-5-12
4/75
Classification by acquired
environmentCommunity acquired pneumoniaCAP
Hospital acquired pneumoniaHAPNP
Nursing home acquired pneumonia,NHAP
Immunocompromised host pneumonia,(ICAP)
-
8/10/2019 Kuliah pneumonia 25-5-12
5/75
CAP
CAPrefers to pneumonia acquired outside of
hospitals or extended-care facilities .
Streptococcus pneumoniae remains the mostcommonly identified
pathogen.
Other pathogens include Haemophilus influenzae,
mycoplasma pneumoniae, Chlamydophilia
pneumoniae, Moraxella catarrhalis and ects.
Drug resistance streptococcus pneumoniae(DRSP)
-
8/10/2019 Kuliah pneumonia 25-5-12
6/75
Community Acquired
Pneumonia Epidemiology:
4-5 million cases annually
~500,000 hospitalizations
~45,000 deaths
Mortality 2-30%
-
8/10/2019 Kuliah pneumonia 25-5-12
7/75
-
8/10/2019 Kuliah pneumonia 25-5-12
8/75
EPIDEMIOLOGY
HAP is the most common infection occurring inpatients requiring
care in an intensive care unit(ICU), with incidence rates ranging
from 6% up to
52%, much higher than the 0.5% to 2% incidencereported for
hospitalized patients as a whole.
This increased incidence is due to the fact thatpatients located
in an ICU often require
mechanical ventilation, and mechanicallyventilated patients are
6 to 21 times more likely todevelop HAP than are nonventilated
patients.Mechanical ventilation is associated
-
8/10/2019 Kuliah pneumonia 25-5-12
9/75
ICHP
Pneumonia in an immunocompromised host
describes a lung infection that occurs in
a person whose ability to fight infection is
greatly impaired.
(Non-HIV-ICH)
-
8/10/2019 Kuliah pneumonia 25-5-12
10/75
Causes, incidence, and risk factors
Immunosuppression can be caused by HIV
infection, leukemia, organ transplantation, bone
marrow transplant, and medications to treat cancer.
Microorganisms include all kinds of bacteria and
virus(CMV), candida and aspergilosis.
pneumocystis carinii
-
8/10/2019 Kuliah pneumonia 25-5-12
11/75
Epidemiology: (contd)
fewest cases in 18-24 yr group probably highest incidence in
65
yrs
mortality disproportionately high in >65 yrs
Community Acquired
Pneumonia
Adeel A. Butt, MD
-
8/10/2019 Kuliah pneumonia 25-5-12
12/75
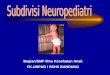
Community Acquired Pneumonia
Adeel A. Butt, MD
898
1071
83
1171 1207
684
0
200
400
600
800
1000
1200
1400
65
# of cases
# in
1000s
Incidence
-
8/10/2019 Kuliah pneumonia 25-5-12
13/75
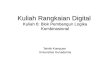
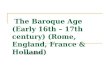
Community Acquired Pneumonia
Adeel A. Butt, MD
25.7
74.9
0
10
20
30
40
50
60
70
80
65
# of deaths# in
1000s
Mortality
-
8/10/2019 Kuliah pneumonia 25-5-12
14/75
-
8/10/2019 Kuliah pneumonia 25-5-12
15/75
Etiology
There are two factors
involved in the
formation ofpneumonia , including
pathogens and host
defenses.
-
8/10/2019 Kuliah pneumonia 25-5-12
16/75
-
8/10/2019 Kuliah pneumonia 25-5-12
17/75
pathogenesis
Pneumococci usually
reach the lungs by
inhalation oraspiration. They lodge
in the bronchioles,
proliferation and
initiate aninflammatory process.
-
8/10/2019 Kuliah pneumonia 25-5-12
18/75
Bacter ia are introduced into the
lungs by the four routes Source Route Response Outcome
colonization aspiration
Air inhalation
Non-pulmonary blood lung pneu.
infection stream defenses
Contiguous direct infection extention
-
8/10/2019 Kuliah pneumonia 25-5-12
19/75
Legionnaires disease is acquriedby inhaling aerosolized
watercontaining Legionellaorganisms or possibly bypulmonary
aspiration ofcontaminated water.
The contaminated water arederived from humidifiers,shower heads,
respiratorytherapy equipment, industrailcooling water.
Because of the frequently use ofair conditioner,
Legionnaiespneumonia is also seen inCAP
-
8/10/2019 Kuliah pneumonia 25-5-12
20/75
-
8/10/2019 Kuliah pneumonia 25-5-12
21/75
Classification
Classification of anatomy
Classification of pathogen
Classification of acquired environment
-
8/10/2019 Kuliah pneumonia 25-5-12
22/75
.Classif ication by pathogen
Pathogen classification is the most useful
to treat the patients by choosing effective
antimicrobial agents
-
8/10/2019 Kuliah pneumonia 25-5-12
23/75
-
8/10/2019 Kuliah pneumonia 25-5-12
24/75
-
8/10/2019 Kuliah pneumonia 25-5-12
25/75
Risk Factors Elderly (not agingper
sebut its associations)
Swallowing difficulty
Use of sedativemedications
Depressed cough reflex
Dementia
Reduced consciousness
Pharyngeal anesthesia
Protracted vomiting
Large volume tube
feedings
Feeding gastrostomy
Recumbent position
-
8/10/2019 Kuliah pneumonia 25-5-12
26/75
-
8/10/2019 Kuliah pneumonia 25-5-12
27/75
Bacter ial pneumonia
(1) Aerobic Gram-positive bacteria,such
as streptococcus pneumoniae, staphy-
lococcus aureus, Group A hemolytic
streptococci
(2) Aerobic Gram-negative bacteria, such
as klebsiella pneumoniae, Hemophilus
influenzae, Escherichia coli
(3) Anaerobic bacteria
-
8/10/2019 Kuliah pneumonia 25-5-12
28/75
Atypical pneumonia
Including Legionnaies pneumonia ,
Mycoplasmal pneumonia ,chlamydia pneumonia.
-
8/10/2019 Kuliah pneumonia 25-5-12
29/75
Fungal pneumonia
Fungal pneumonia is commonly caused by
candida and aspergilosis.
pneumocystis jiroveci
-
8/10/2019 Kuliah pneumonia 25-5-12
30/75
Legionellae are small,gram-negative,obligately aerobic
baclli.
.
-
8/10/2019 Kuliah pneumonia 25-5-12
31/75
Viral pneumonia
Viral pneumonia may be caused by
adenoviruses, respiratory syncytial
virus, influenza, cytomegalovirus,
herpes simplex
-
8/10/2019 Kuliah pneumonia 25-5-12
32/75
Pneumonia caused byother pathogen
Rickettsias (a fever rickettsia),
parasites
protozoa
-
8/10/2019 Kuliah pneumonia 25-5-12
33/75
.Classif ication by anatomy
1. Lobar: Involvement of an entire lobe
2. Lobular: Involvement of parts of the lobe only,
segmental or of alveoli contiguous to
bronchi(bronchopneumonia).
3. Interstitial
-
8/10/2019 Kuliah pneumonia 25-5-12
34/75
Pembagian Berdasarkan Lokasi
Pneumonia Lobaris
Pneumonia Interstitial
Pneumonia Lobularis (Bronkopneumonia)
-
8/10/2019 Kuliah pneumonia 25-5-12
35/75
Lobar pneumonia
-
8/10/2019 Kuliah pneumonia 25-5-12
36/75
-
8/10/2019 Kuliah pneumonia 25-5-12
37/75
-
8/10/2019 Kuliah pneumonia 25-5-12
38/75
Lobular pneumonia
-
8/10/2019 Kuliah pneumonia 25-5-12
39/75
Diagnosis
Give a definite diagnosis of pneumonia
To evaluate the degree of the pneumonia
To definite the pathogen of the pneumonia
-
8/10/2019 Kuliah pneumonia 25-5-12
40/75
Diagnosis
Clinical diagnosis
Pathogen diagnosis
Evaluate the severity degree of pneumonia
-
8/10/2019 Kuliah pneumonia 25-5-12
41/75
Diagnosis
History and physical
examination(5W)
X-ray examination
Pathogen identification
-
8/10/2019 Kuliah pneumonia 25-5-12
42/75
Pathogen identification
Sputum: More than 25 white blood cells
(WBCs) and less than 10 epithelial cells.
Nasotracheal suctioning
Blood culture or pleural effusion culture
Serologic testing (immunological testing)
Molecular Techniques
-
8/10/2019 Kuliah pneumonia 25-5-12
43/75
-
8/10/2019 Kuliah pneumonia 25-5-12
44/75
The diagnostic standard of severe
pneumonia
Altered mental status
Pa02
-
8/10/2019 Kuliah pneumonia 25-5-12
45/75
-
8/10/2019 Kuliah pneumonia 25-5-12
46/75
signs
Consolidation signs
Moist rales
Respiratory rate or heart rate
-
8/10/2019 Kuliah pneumonia 25-5-12
47/75
-
8/10/2019 Kuliah pneumonia 25-5-12
48/75
-
8/10/2019 Kuliah pneumonia 25-5-12
49/75
Pathology
Red hepatilization
-
8/10/2019 Kuliah pneumonia 25-5-12
50/75
Abstraction
Pneumococcal
pneumonia is produced
by
streptococcal
pneumoniae
It is the most commonly
occurring bacterial
pneumonia
-
8/10/2019 Kuliah pneumonia 25-5-12
51/75
Clinical mani festations
-
8/10/2019 Kuliah pneumonia 25-5-12
52/75
Clinical manifestations (1)
Many patients have had an upper respiratory
infection for several days before the onset of
pneumonia Onset usually is sudden, half cases with a
shaking chill
The temperature rises during the first few
hours to 39-40
-
8/10/2019 Kuliah pneumonia 25-5-12
53/75
Clinical manifestations (2)
Typically, patients have the symptoms of
high fever , shaking chill, sharp chest
pain, cough, dyspnea and blood-fleckedsputum.
But in some cases, especially those at age
extremes symptoms may be moreinsidious.
Cli i l if i (3)
-
8/10/2019 Kuliah pneumonia 25-5-12
54/75
The pulse accelerates
Sharp pain in the involved hemi thorax
The cough is initially dry with pinkish or
blood-flecked sputum
Gastrointestinal symptoms such as,
anorexia, nausea, vomiting abdominal
pain, diarrhea may be mistaken as acuteabdominal
inflammation
Clinical manifestations (3)
-
8/10/2019 Kuliah pneumonia 25-5-12
55/75
Signs 1
The acutely ill patient is tachypneic, and
may be observed to use accessory muscles
for respiration, and even to exhibit nasal
flaring
Fever and tachycardia are present, frank
shock is unusual, except in the later stages
of infection or DIC
-
8/10/2019 Kuliah pneumonia 25-5-12
56/75
Signs 2
Auscultation of the chest reveals
bronchovesicular or tubular breath
sounds and wet rales over theinvolved lung
A consolidation occurs, vocal and
tactile fremitus are increased
-
8/10/2019 Kuliah pneumonia 25-5-12
57/75
Laboratory examinations
-
8/10/2019 Kuliah pneumonia 25-5-12
58/75
-
8/10/2019 Kuliah pneumonia 25-5-12
59/75
-
8/10/2019 Kuliah pneumonia 25-5-12
60/75
X-ray examination
Usually lobar or
segmental
consolidation
suggests a bacterial
cause for pneumonia
If blunting of the
costophrenic angle isnoted, pleural
effusion may be exist.
The features of CT
-
8/10/2019 Kuliah pneumonia 25-5-12
61/75
The features of CT
Air-bronchogram sign
-
8/10/2019 Kuliah pneumonia 25-5-12
62/75
Complications
sepsis
lung abscess or empyema
pleural effusionpleuritis
ARDS
ARF
pneumothorax
Extrapulmonary infections
-
8/10/2019 Kuliah pneumonia 25-5-12
63/75
Pleural Effusion
GenMed 3
-
8/10/2019 Kuliah pneumonia 25-5-12
64/75
Differential diagnosis
pulmonary tuberculosis
Other microbial pneumonias:
klebsiella pneumonia,
staphylococal pneumonia,
pneumonias due to G (-) bacilli,
viral and mycoplasmal
Acute lung abscess Bronchogenic carcinoma
Pulmonary infarction
-
8/10/2019 Kuliah pneumonia 25-5-12
65/75
Treatments
Antibiotics
Support therapy
Therapy of complications
-
8/10/2019 Kuliah pneumonia 25-5-12
66/75
-
8/10/2019 Kuliah pneumonia 25-5-12
67/75
Therapy
The therapy should always follow
confirmation of the diagnosis of pneumonia
and should always be accompanied by adiligent effort to identify
an etiologic agent.
Empiric therapy,(4-8h)
Combined empiric therapy to target therapy
-
8/10/2019 Kuliah pneumonia 25-5-12
68/75
Antibiotic therapy
Treatment with any effective agent
should be given for at least 5 to 7 day or
after the patients have been afebrile for2-3 days
-
8/10/2019 Kuliah pneumonia 25-5-12
69/75
Empiric therapy (1)
Outpatient
-
8/10/2019 Kuliah pneumonia 25-5-12
70/75
Supportive measure
Supportive measure are generally used in
the initial management of acute pneumo-
coccal pneumonia, such measures include
Bed rest
Monitoring vital signs and urine output
Administering an occasional analgesic to
relieve pleuritic pain
Replacing fluids, if the patient is dehydrated
Correcting electrolytes
Oxygen therapy
-
8/10/2019 Kuliah pneumonia 25-5-12
71/75
Treatment of complications
Empyema develops in appoximately 5% of patients
with pneumococcal pneumonia, although pleural
effusion commonly develop in 10%- 20% patients
Chest X-ray with lateral decubitus films are often
useful in the early recognition of pleural effusion,
pleural fluid that is removed should be subjected to
routing examination
If pneumococcal bacteremia occurs, extra pulmonary
complications such as arthritis, endocarditis must beexcluded,
because the therapy requires higher dosages
Treatment of infections shock
-
8/10/2019 Kuliah pneumonia 25-5-12
72/75
Therapy to Infectious Shock
Treatment in intensive care units
cardiac rhythm, blood pressure, cardiac performance, oxygen
delivery, and metabolic derangements can be monitored
Adequate oxygenation and ventilatory support
(sometimes mechanical ventilation)
Effective antibiotic therapy
Maintain blood pressure, including maintaincirculation blood
volume, use of dopamine
-
8/10/2019 Kuliah pneumonia 25-5-12
73/75
Prognosis
Prognosis is much better
Any of the following factors makes the prognosis
less favorable and convalescence more prolonged
elderly: involvement of 2 or more lobes
underlying chronic diseases (heart lung
kidney) normal temperature and WBC
count
-
8/10/2019 Kuliah pneumonia 25-5-12
74/75
Prevention
Release aspiration
Washing hands
vaccination
-
8/10/2019 Kuliah pneumonia 25-5-12
75/75
Prevention
The most important
preventive tool available
is using a poly valent
pneumococcal vaccine
in those with chronic
lung diseases, chronic
liver diseases,
splenectomy, diabetes
mellitus
and aged