Embed Size (px)
Citation preview
Duke Advanced Heart Failure
Symposium Michel G. Khouri, MD
October 5, 2013
Cardio-‐Oncology
Disclosures • None
Cardio-‐Oncology • An emerging field to keep pace with the rapid evoluDon of cancer therapies and the incidence, magnitude and consequences of their CV side effects
• Relevant to cancer survivorship: i. Early CV toxiciDes arising during treatment may
interfere with compleDon of very therapies needed to enhance survivorship
ii. CV issues arising aPer cancer therapy compleDon • New fronDer in medicine
• CV toxiciDes of novel targeted cancer therapies
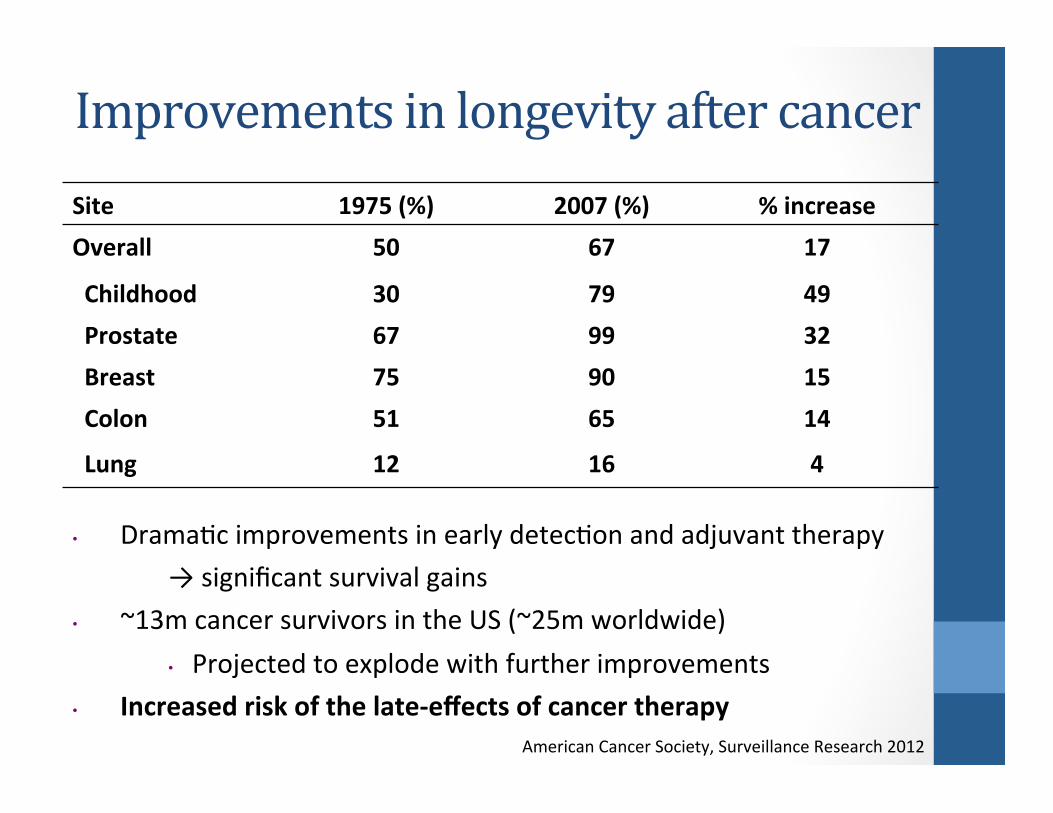
Site 1975 (%) 2007 (%) % increase Overall 50 67 17
Childhood 30 79 49 Prostate 67 99 32 Breast 75 90 15 Colon 51 65 14
Lung 12 16 4
• DramaDc improvements in early detecDon and adjuvant therapy → significant survival gains
• ~13m cancer survivors in the US (~25m worldwide) • Projected to explode with further improvements
• Increased risk of the late-‐effects of cancer therapy
Improvements in longevity after cancer
American Cancer Society, Surveillance Research 2012
Cancer Therapy and the Heart Cardiotoxicity I. Is there a problem? II. How serious is the problem? III. Why is there a problem? IV. What can we do about the problem?
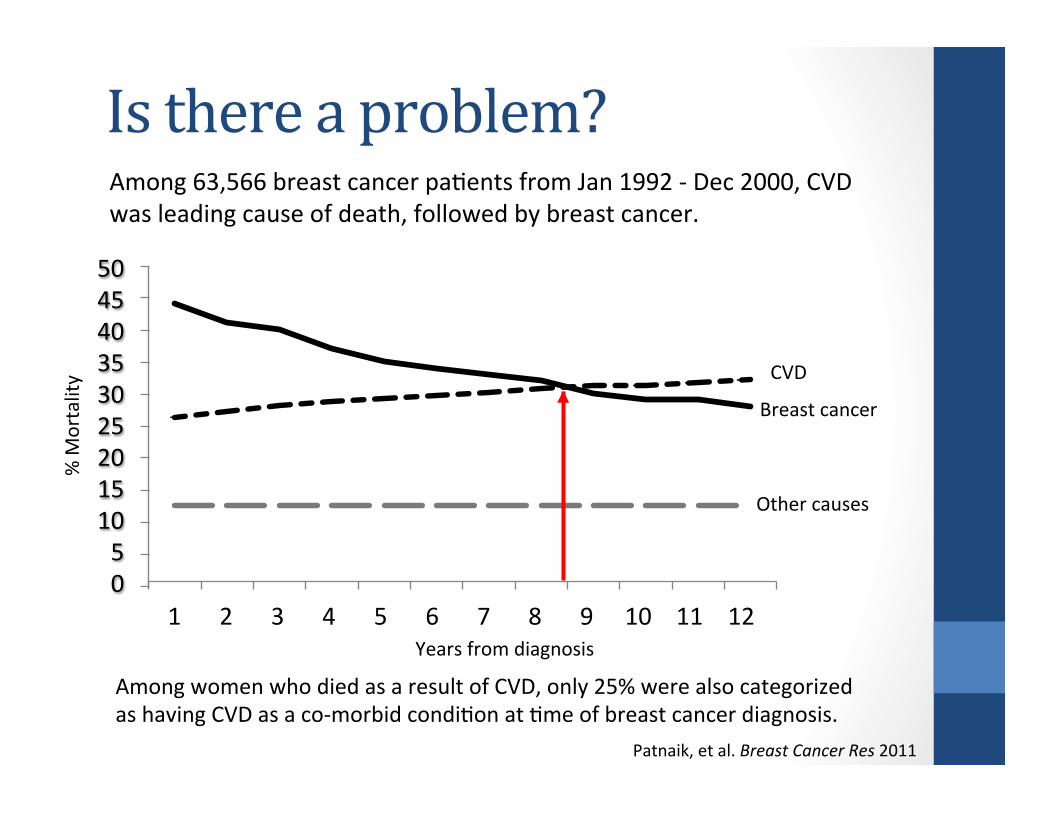
Is there a problem? Among 63,566 breast cancer paDents from Jan 1992 -‐ Dec 2000, CVD was leading cause of death, followed by breast cancer.
Patnaik, et al. Breast Cancer Res 2011
Among women who died as a result of CVD, only 25% were also categorized as having CVD as a co-‐morbid condiDon at Dme of breast cancer diagnosis.
0 5 10 15 20 25 30 35 40 45 50
1 2 3 4 5 6 7 8 9 10 11 12 Years from diagnosis
% M
ortality
Other causes
CVD
Breast cancer
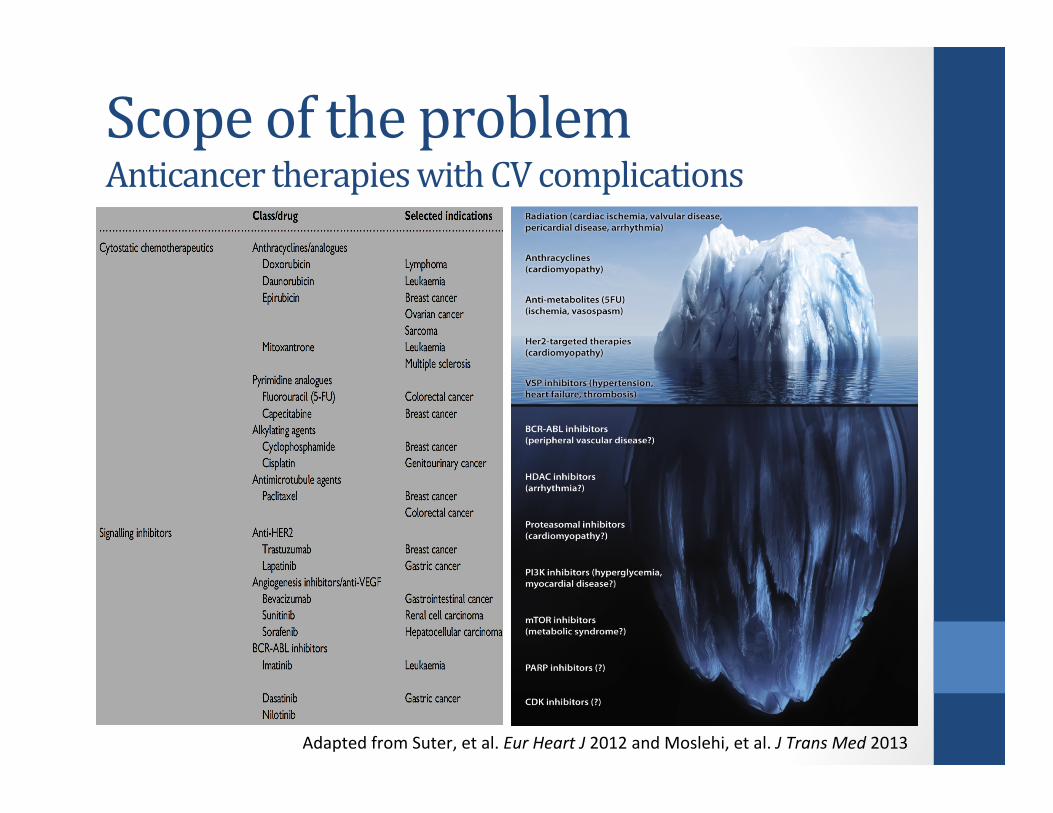
Scope of the problem Anticancer therapies with CV complications
Adapted from Suter, et al. Eur Heart J 2012 and Moslehi, et al. J Trans Med 2013
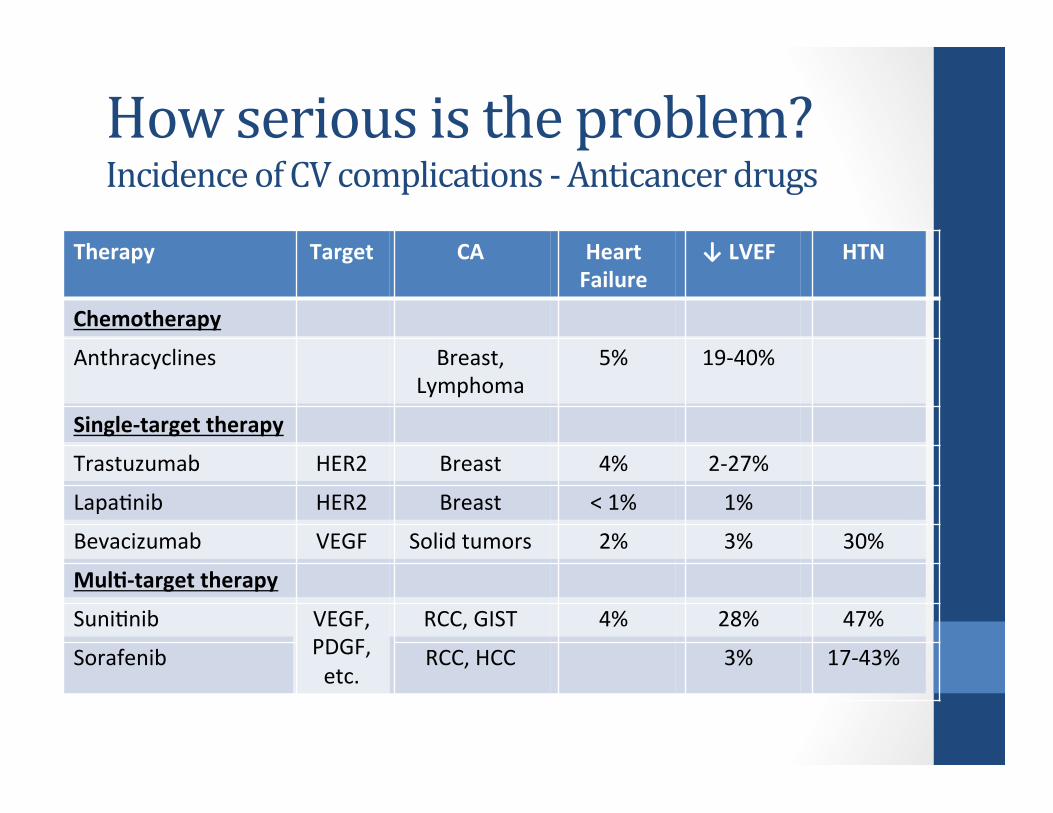
How serious is the problem? Incidence of CV complications -‐ Anticancer drugs
Therapy Target CA Heart Failure
↓ LVEF HTN
Chemotherapy
Anthracyclines Breast, Lymphoma
5% 19-‐40%
Single-‐target therapy
Trastuzumab HER2 Breast 4% 2-‐27%
LapaDnib HER2 Breast < 1% 1%
Bevacizumab VEGF Solid tumors 2% 3% 30%
MulT-‐target therapy
SuniDnib VEGF, PDGF, etc.
RCC, GIST 4% 28% 47%
Sorafenib RCC, HCC 3% 17-‐43%
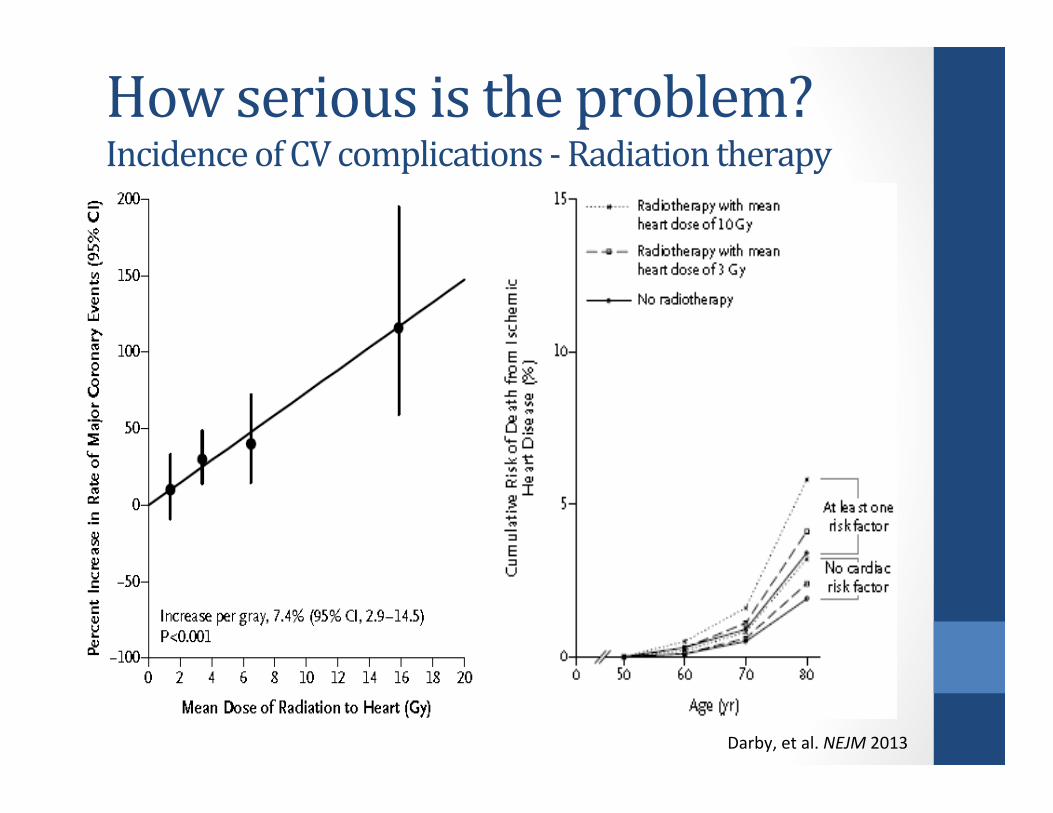
How serious is the problem? Incidence of CV complications -‐ Radiation therapy
Darby, et al. NEJM 2013
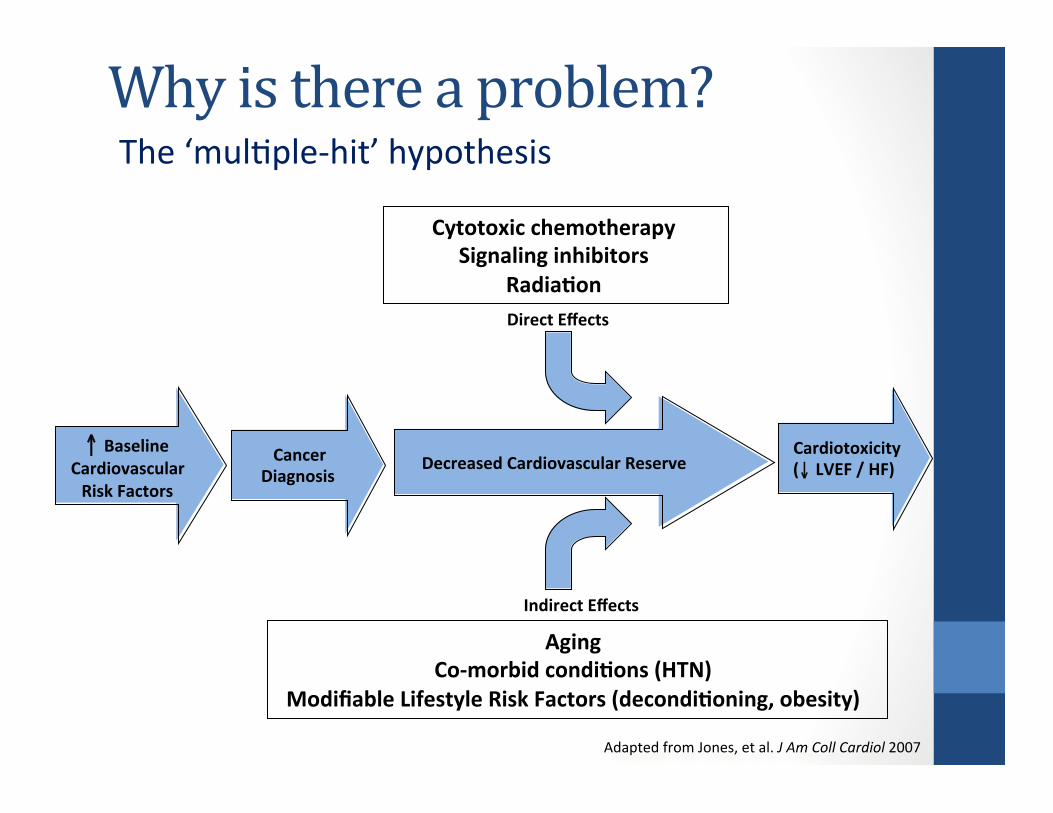
Decreased Cardiovascular Reserve
Cytotoxic chemotherapy Signaling inhibitors
RadiaTon Direct Effects
Indirect Effects
Aging Co-‐morbid condiTons (HTN)
Modifiable Lifestyle Risk Factors (decondiToning, obesity)
↑ Baseline Cardiovascular Risk Factors
Cancer Diagnosis
Cardiotoxicity (↓ LVEF / HF)
Adapted from Jones, et al. J Am Coll Cardiol 2007
Why is there a problem? The ‘mulDple-‐hit’ hypothesis
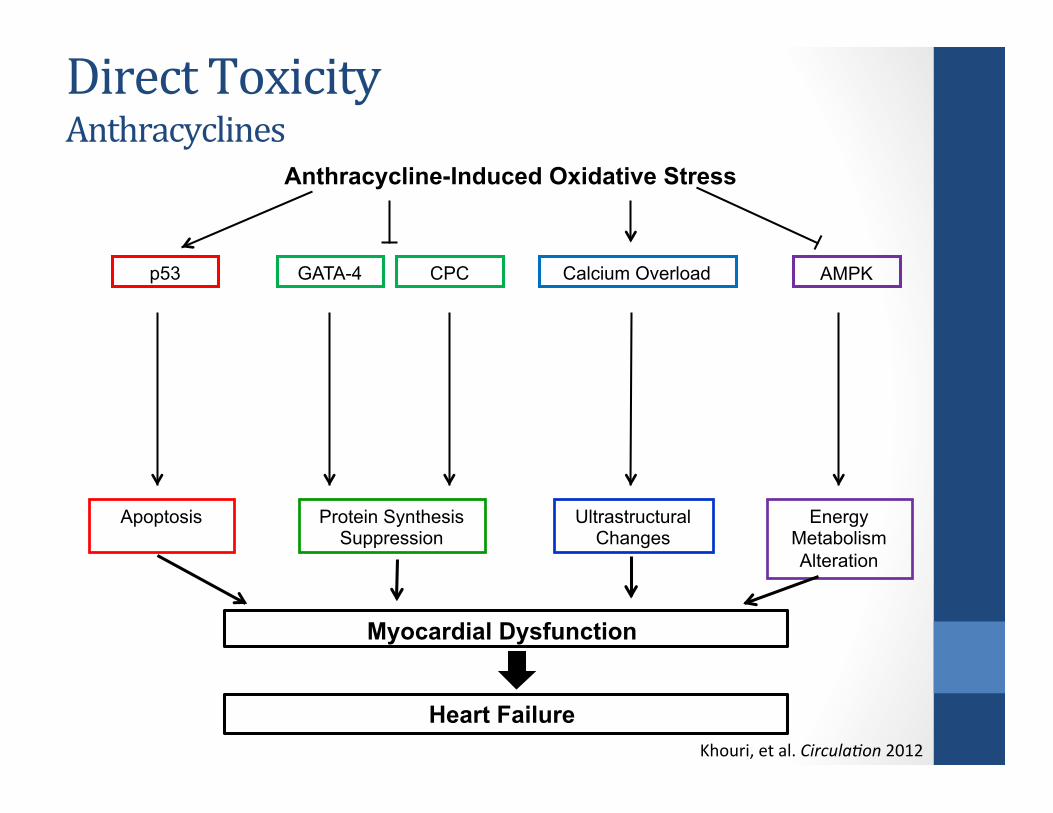
p53
Apoptosis Protein Synthesis Suppression
Ultrastructural Changes
Energy Metabolism Alteration
Anthracycline-Induced Oxidative Stress
GATA-4 CPC Calcium Overload AMPK
Myocardial Dysfunction
Heart Failure
Khouri, et al. Circula9on 2012
Direct Toxicity Anthracyclines
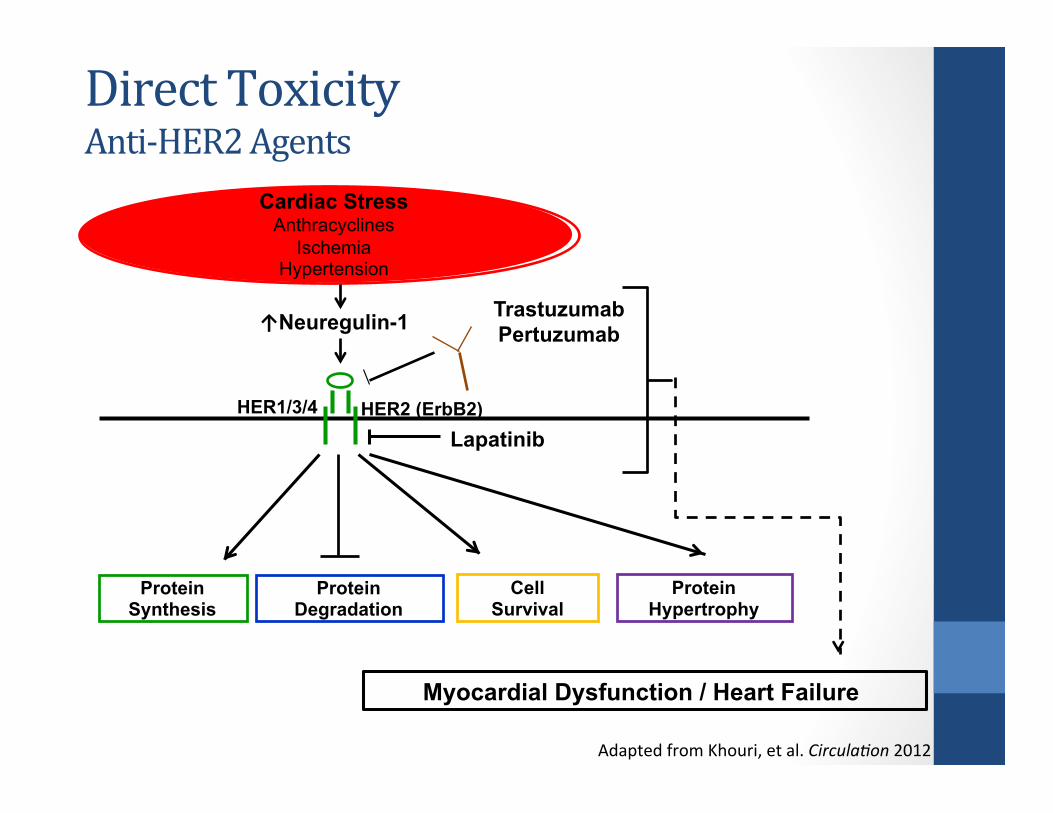
Direct Toxicity Anti-‐HER2 Agents
Adapted from Khouri, et al. Circula9on 2012
HER1/3/4
Cardiac Stress Anthracyclines
Ischemia Hypertension
Protein Synthesis
Protein Degradation
Protein Hypertrophy
Cell Survival
HER2 (ErbB2)
↑Neuregulin-1 Trastuzumab Pertuzumab
Lapatinib
Myocardial Dysfunction / Heart Failure
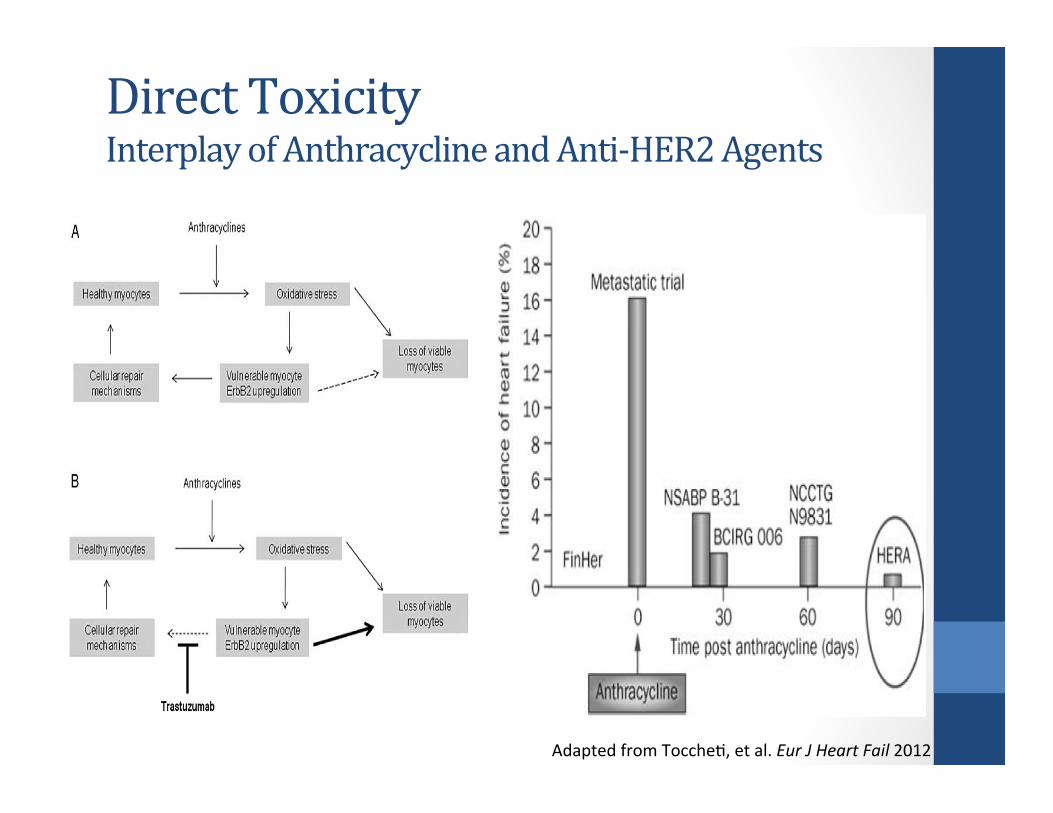
Direct Toxicity Interplay of Anthracycline and Anti-‐HER2 Agents
Adapted from ToccheD, et al. Eur J Heart Fail 2012

Direct Toxicity Angiogenesis (VSP) Inhibitors
Adapted from Khouri, et al. Circula9on 2012
↑VEGF Ischemia Hypertension
VEGFR (1/2/3)
Sunitinib Sorafenib Pazopanib
Axitinib Vandetanib
Bevacizumab
C-Kit PDGFR
HIFα ↑PDGF
Cell survival Vasodilation (NO production)
Angiogenesis Prostaglandin production
Hypertension Thromboembolism (VTE, ATE)
Myocardial Dysfunction / Heart Failure
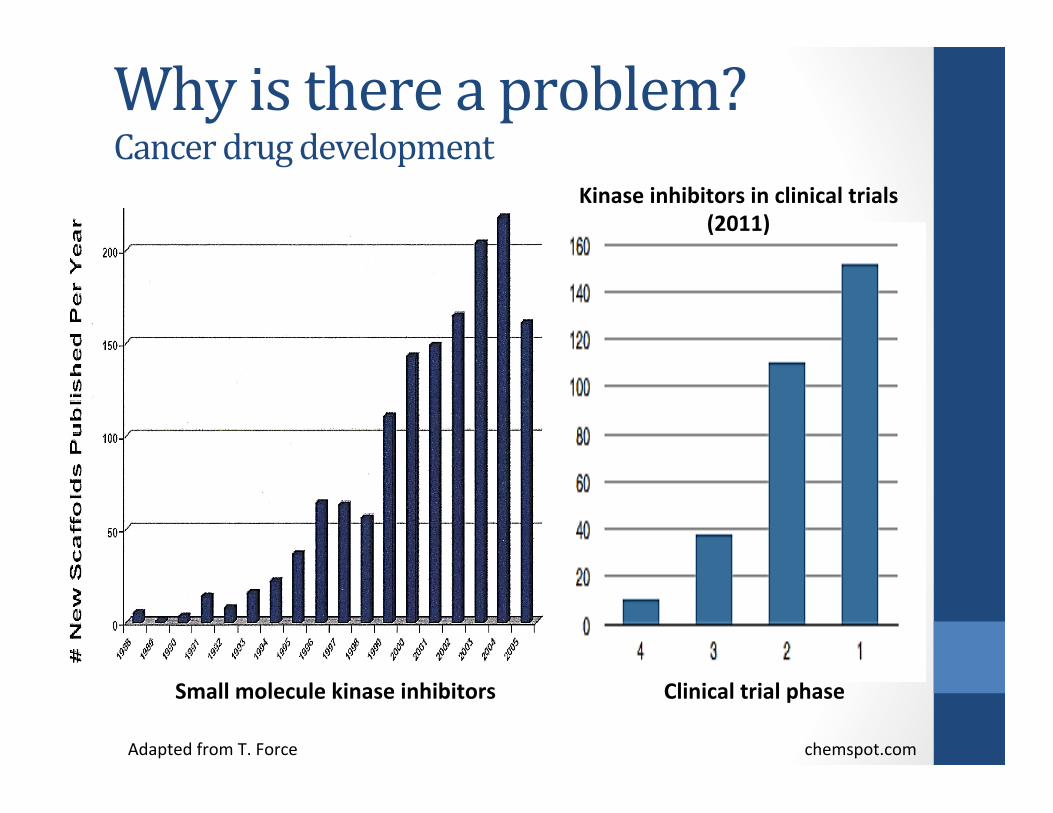
Why is there a problem? Cancer drug development
Clinical trial phase
Kinase inhibitors in clinical trials (2011)
Small molecule kinase inhibitors
Adapted from T. Force chemspot.com
Summary I • Advancements in diagnosDc tools and therapies have dramaDcally improved cancer-‐specific survival
• Adverse cardiac effects of convenDonal therapies remain • Newer adjuvant therapies interfere with molecular pathways crucial to normal cardiovascular health • Numerous more drugs are in the pipeline
• The cancer survivor populaDon is aging with a higher prevalence of tradiDonal CVD risk factors
• If these current trends conDnue, further improvements in cancer-‐specific and overall survival may be offset by increased therapy-‐associated CV mortality
What can we do about the problem?
Yoon, et al. JACC 2010
Smiseth, et al. JACC 2013
What can we do about the problem?
Areas of InvesDgaDon / Improvement I. Defining Cardiotoxicity II. DetecDon III. PrevenDon / Treatment
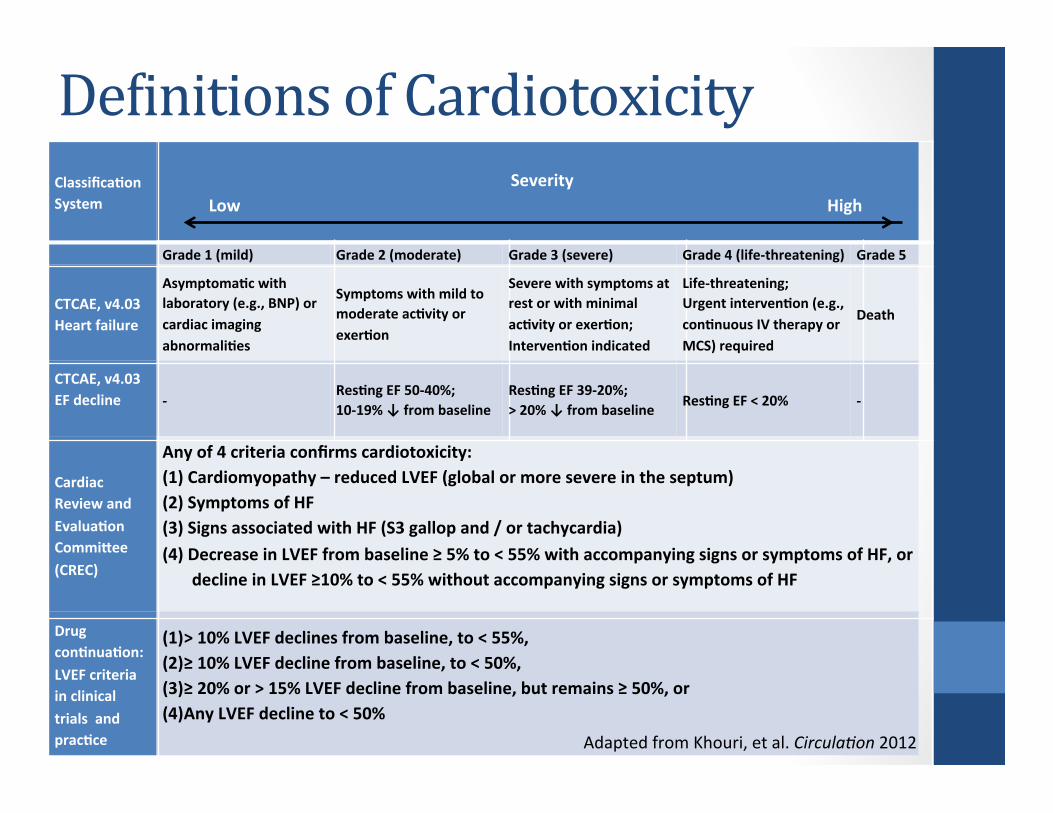
DeLinitions of Cardiotoxicity ClassificaTon System
Severity
Low High
Grade 1 (mild) Grade 2 (moderate) Grade 3 (severe) Grade 4 (life-‐threatening) Grade 5
CTCAE, v4.03 Heart failure
AsymptomaTc with laboratory (e.g., BNP) or cardiac imaging abnormaliTes
Symptoms with mild to moderate acTvity or exerTon
Severe with symptoms at rest or with minimal acTvity or exerTon; IntervenTon indicated
Life-‐threatening; Urgent intervenTon (e.g., conTnuous IV therapy or MCS) required
Death
CTCAE, v4.03 EF decline
-‐ ResTng EF 50-‐40%; 10-‐19% ↓ from baseline
ResTng EF 39-‐20%; > 20% ↓ from baseline ResTng EF < 20% -‐
Cardiac Review and EvaluaTon Commigee (CREC)
Any of 4 criteria confirms cardiotoxicity: (1) Cardiomyopathy – reduced LVEF (global or more severe in the septum) (2) Symptoms of HF (3) Signs associated with HF (S3 gallop and / or tachycardia) (4) Decrease in LVEF from baseline ≥ 5% to < 55% with accompanying signs or symptoms of HF, or decline in LVEF ≥10% to < 55% without accompanying signs or symptoms of HF
Drug conTnuaTon: LVEF criteria in clinical trials and pracTce
(1) > 10% LVEF declines from baseline, to < 55%, (2) ≥ 10% LVEF decline from baseline, to < 50%, (3) ≥ 20% or > 15% LVEF decline from baseline, but remains ≥ 50%, or (4) Any LVEF decline to < 50% Adapted from Khouri, et al. Circula9on 2012
Implications of current deLinitions
• Differing LVEF parameters hinder accurate assessment of the frequency and magnitude of drug-‐induced LV dysfuncDon
• Clinical importance of current definiDons of cardiotoxicity remains unknown
• Long-‐term natural history of LVEF during and post-‐ therapy remains unknown • What degree of LVEF decline is important?
Detection of Cardiotoxicity • ResDng LVEF = Standard of Care
• 2D Echo or MUGA • LimitaDons of LVEF
• InsensiDve measure of subclinical cardiac injury • CompensaDon masks chemo-‐induced early myocyte damage
• Decline evident only once significant damage has occurred • Too late to avert irreversible cardiomyopathy
• LimitaDons of current detecDon approaches • No evidence-‐based guidelines of Dming / frequency • Unchanged LVEF oPen equated to a lack of cardiotoxicity
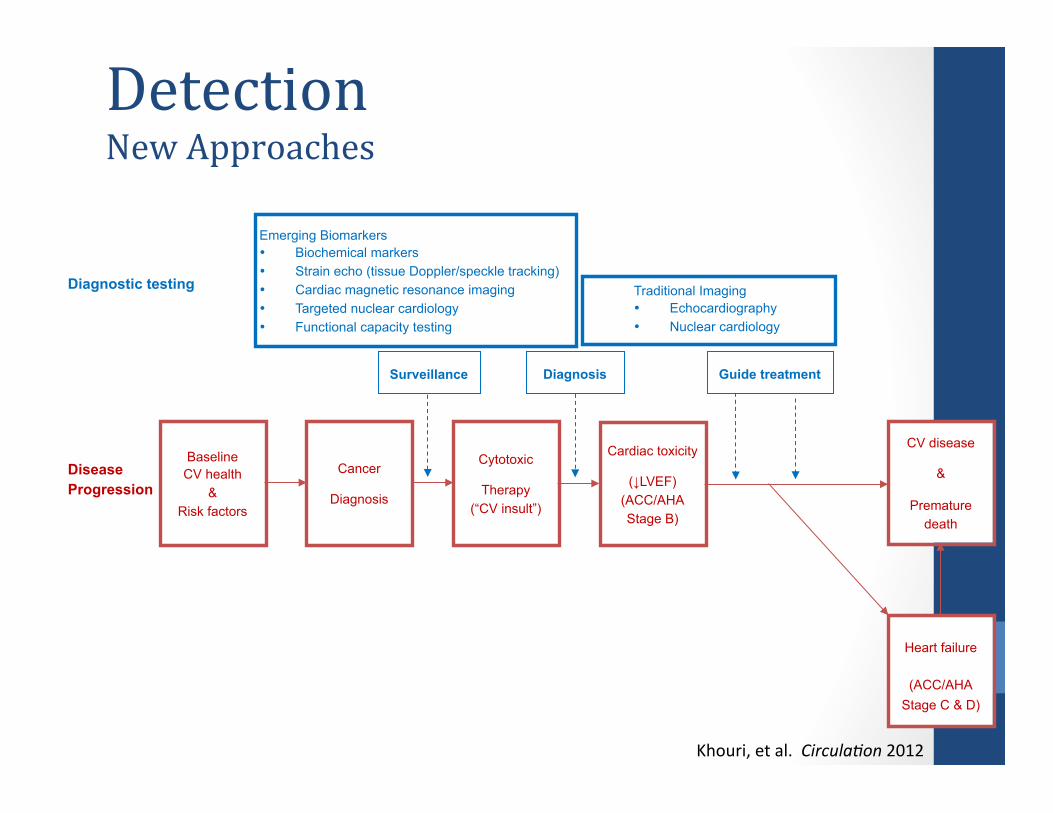
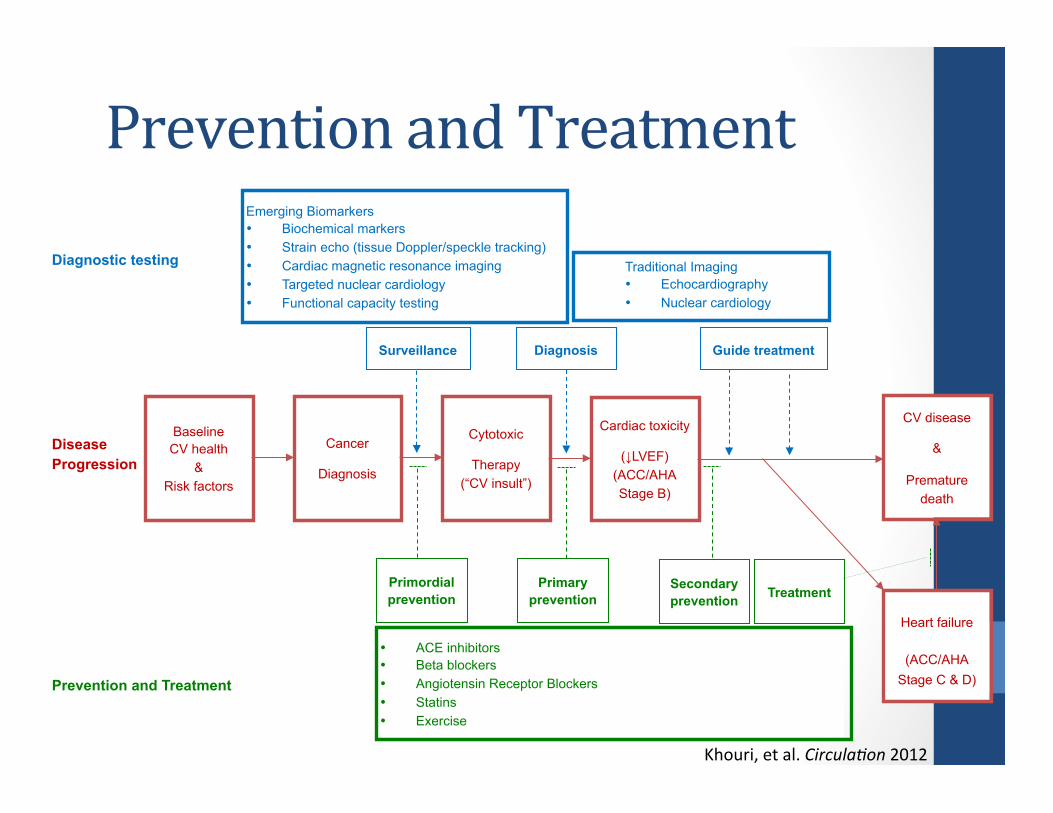
Diagnostic testing
Emerging Biomarkers • Biochemical markers • Strain echo (tissue Doppler/speckle tracking) • Cardiac magnetic resonance imaging • Targeted nuclear cardiology • Functional capacity testing
Surveillance
Traditional Imaging • Echocardiography • Nuclear cardiology
Diagnosis Guide treatment
Baseline CV health
& Risk factors
Cancer
Diagnosis
Cytotoxic
Therapy (“CV insult”)
Cardiac toxicity
(↓LVEF) (ACC/AHA Stage B)
Heart failure
(ACC/AHA
Stage C & D)
CV disease
&
Premature death
Disease Progression
Detection New Approaches
Khouri, et al. Circula9on 2012
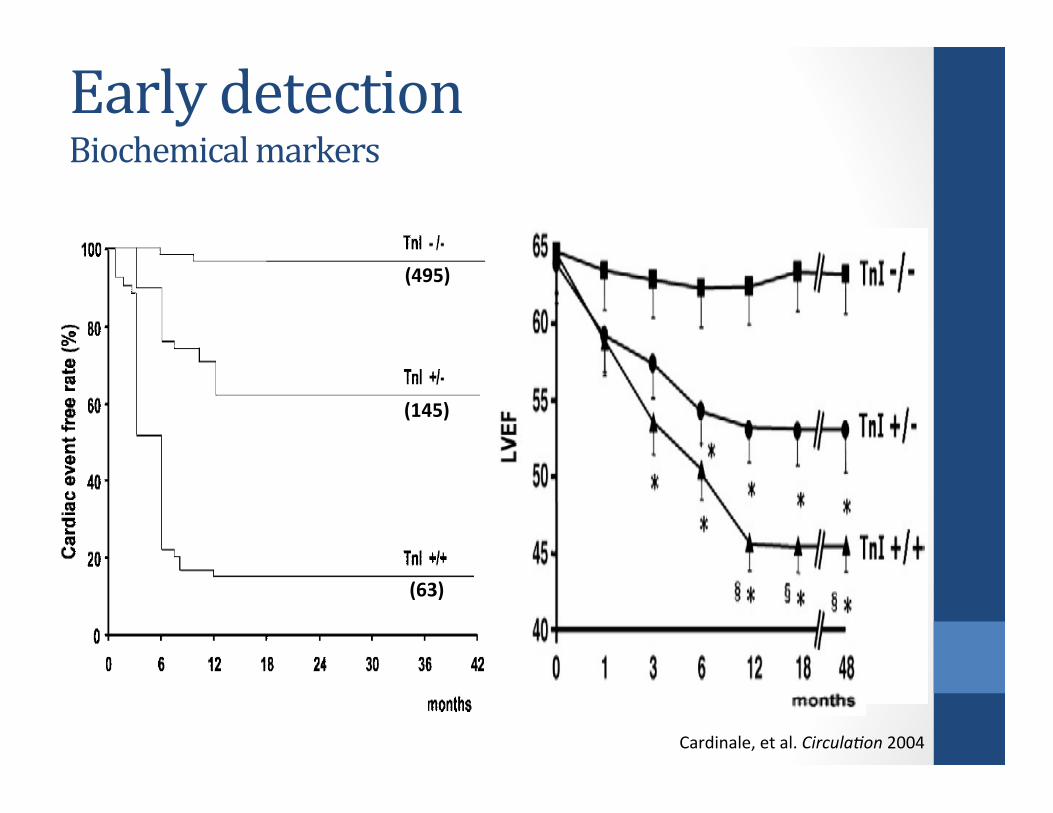
Early detection Biochemical markers
Cardinale, et al. Circula9on 2004
(495)
(145)
(63)
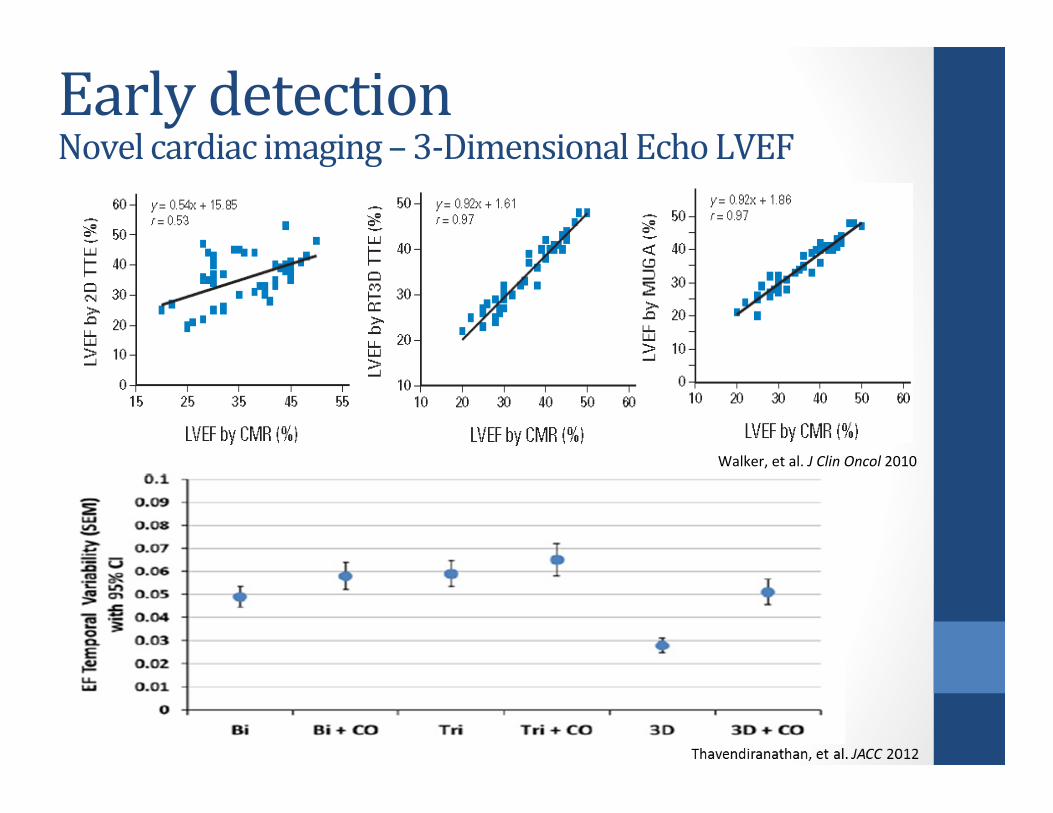
Early detection Novel cardiac imaging – 3-‐Dimensional Echo LVEF
Walker, et al. J Clin Oncol 2010
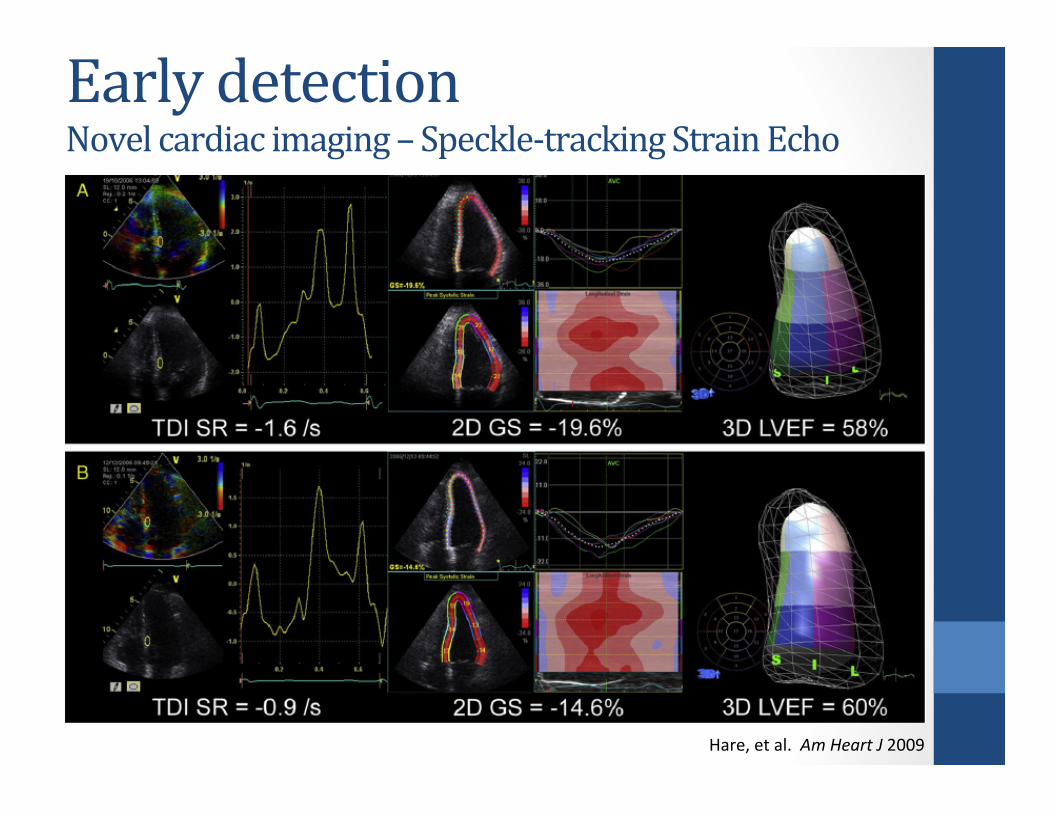
Early detection Novel cardiac imaging – Speckle-‐tracking Strain Echo
Hare, et al. Am Heart J 2009
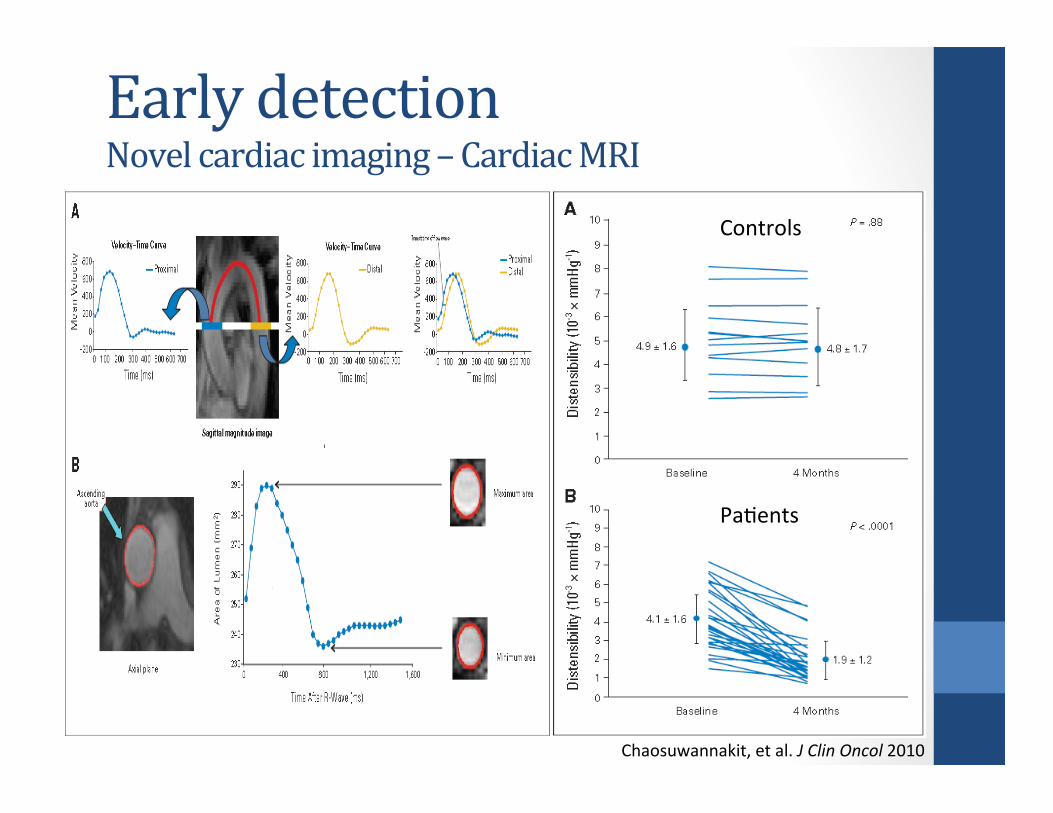
Controls
PaDents
Early detection Novel cardiac imaging – Cardiac MRI
Chaosuwannakit, et al. J Clin Oncol 2010
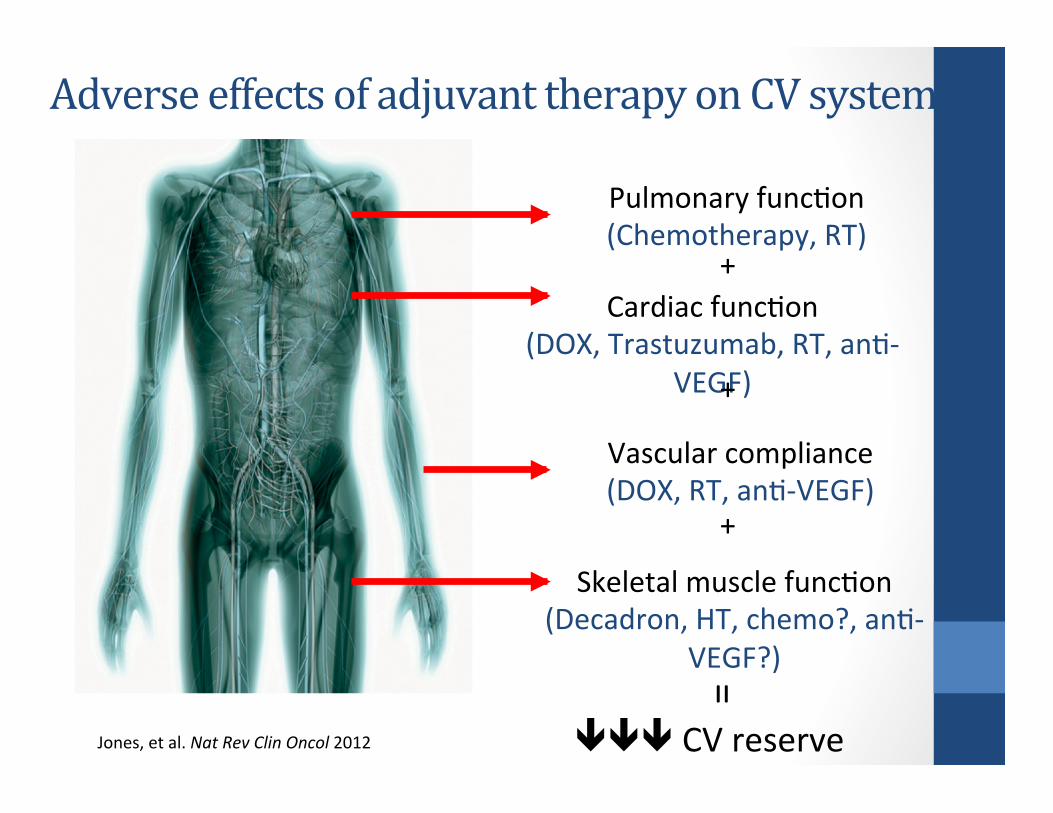
Pulmonary funcDon (Chemotherapy, RT)
Cardiac funcDon (DOX, Trastuzumab, RT, anD-‐
VEGF)
Vascular compliance (DOX, RT, anD-‐VEGF)
Skeletal muscle funcDon (Decadron, HT, chemo?, anD-‐
VEGF?)
CV reserve
+
+
+
=
Jones, et al. Nat Rev Clin Oncol 2012
Adverse effects of adjuvant therapy on CV system
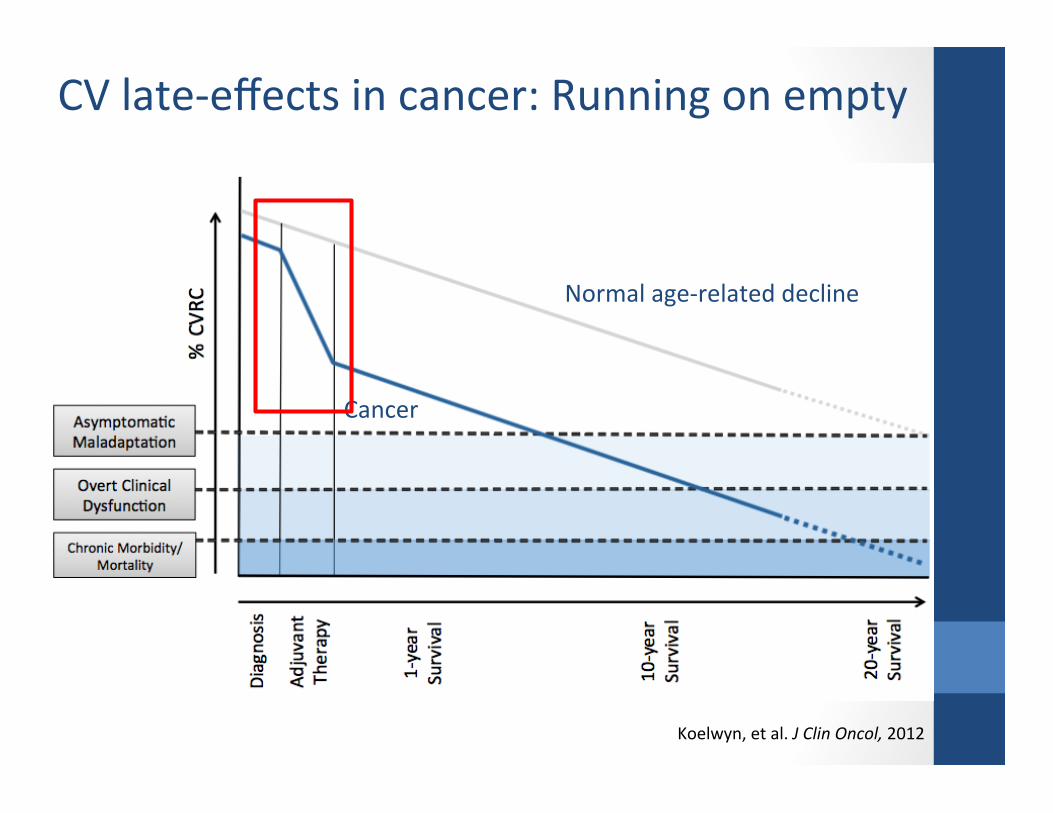
Koelwyn, et al. J Clin Oncol, 2012
CV late-‐effects in cancer: Running on empty
Cancer
Normal age-‐related decline
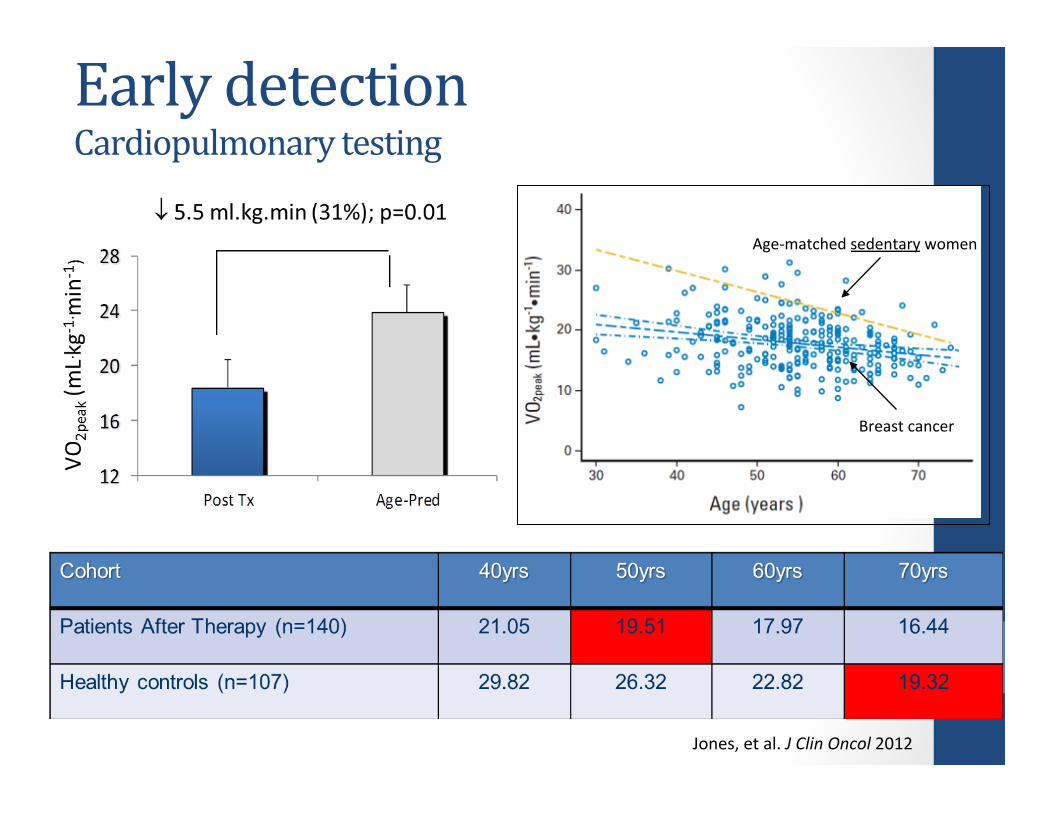
Early detection Cardiopulmonary testing
Breast cancer
Age-‐matched sedentary women
Jones, et al. J Clin Oncol 2012
50
55
60
65
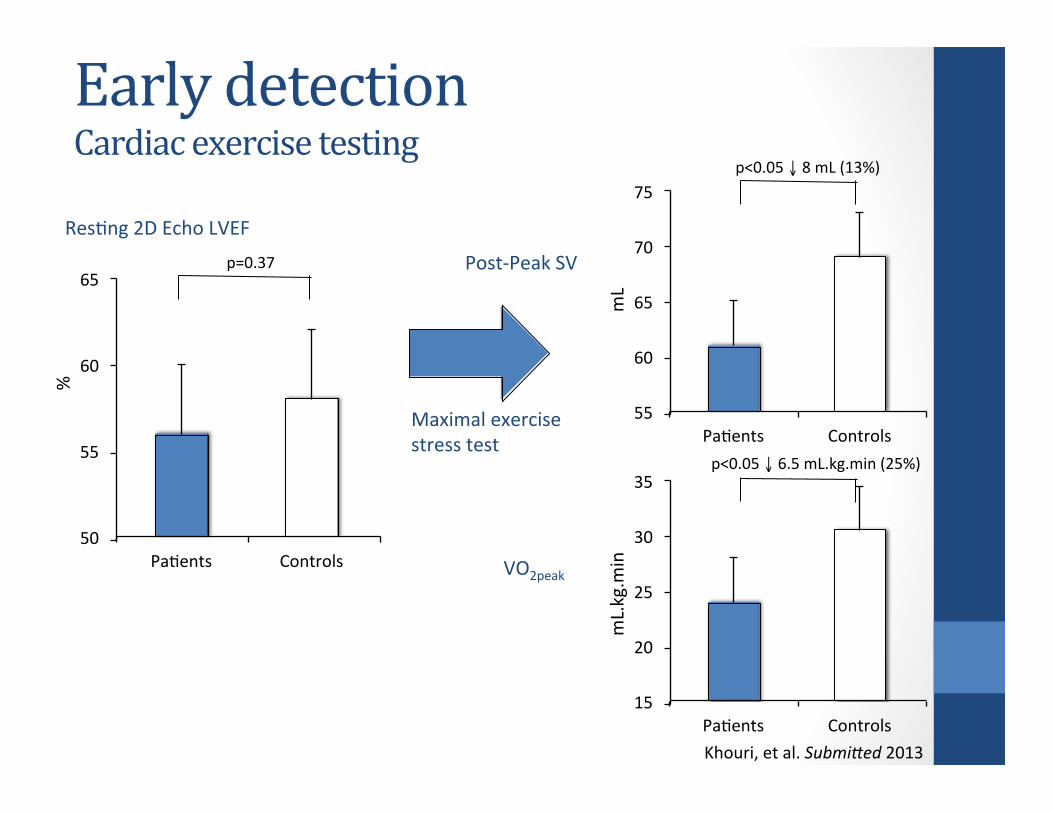
PaDents Controls
p=0.37
%
ResDng 2D Echo LVEF
Maximal exercise stress test
55
60
65
70
75
PaDents Controls
Post-‐Peak SV
mL
p<0.05 ↓ 8 mL (13%)
15
20
25
30
35
PaDents Controls
VO2peak
mL.kg.m
in
p<0.05 ↓ 6.5 mL.kg.min (25%)
Early detection Cardiac exercise testing
Khouri, et al. SubmiAed 2013
Baseline CV health
& Risk factors
Cancer
Diagnosis
Cytotoxic
Therapy (“CV insult”)
Cardiac toxicity
(↓LVEF) (ACC/AHA Stage B)
Heart failure
(ACC/AHA
Stage C & D)
CV disease
&
Premature death
Diagnostic testing
Disease Progression
Emerging Biomarkers • Biochemical markers • Strain echo (tissue Doppler/speckle tracking) • Cardiac magnetic resonance imaging • Targeted nuclear cardiology • Functional capacity testing
Surveillance
Traditional Imaging • Echocardiography • Nuclear cardiology
Diagnosis Guide treatment
Prevention and Treatment
• ACE inhibitors • Beta blockers • Angiotensin Receptor Blockers • Statins • Exercise
Primordial prevention
Primary prevention
Secondary prevention Treatment
Prevention and Treatment
Khouri, et al. Circula9on 2012
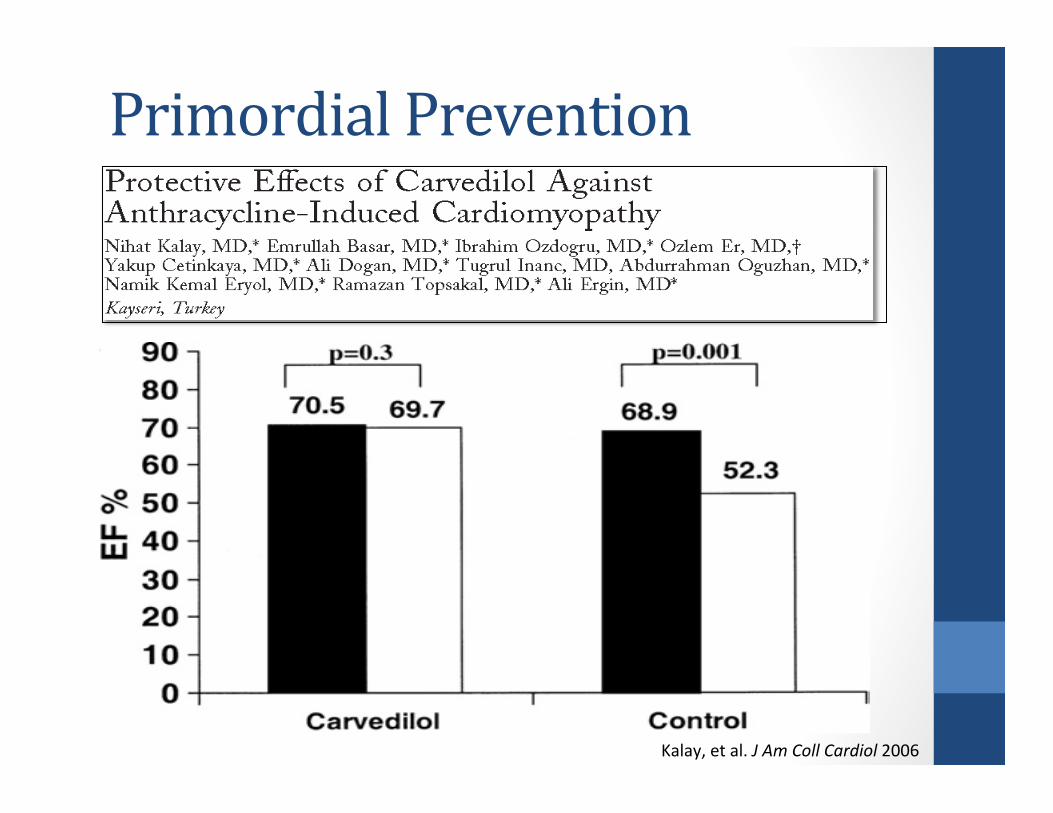
Primordial Prevention
Kalay, et al. J Am Coll Cardiol 2006
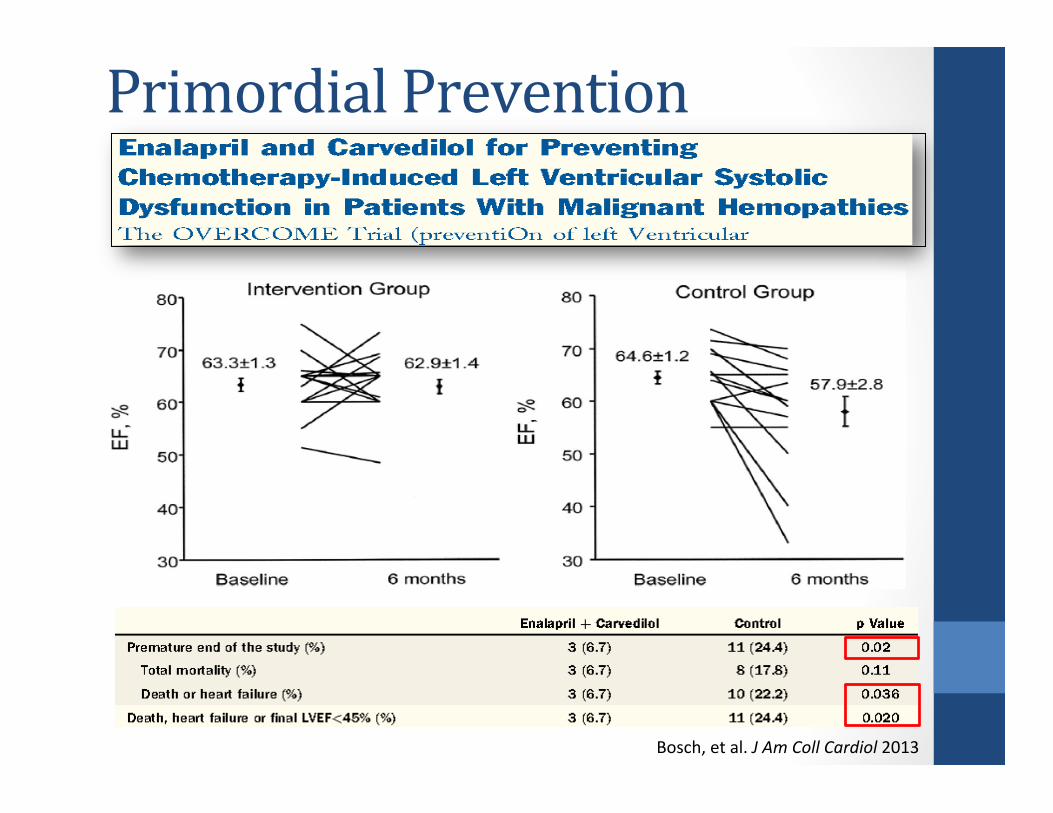
Primordial Prevention
Bosch, et al. J Am Coll Cardiol 2013
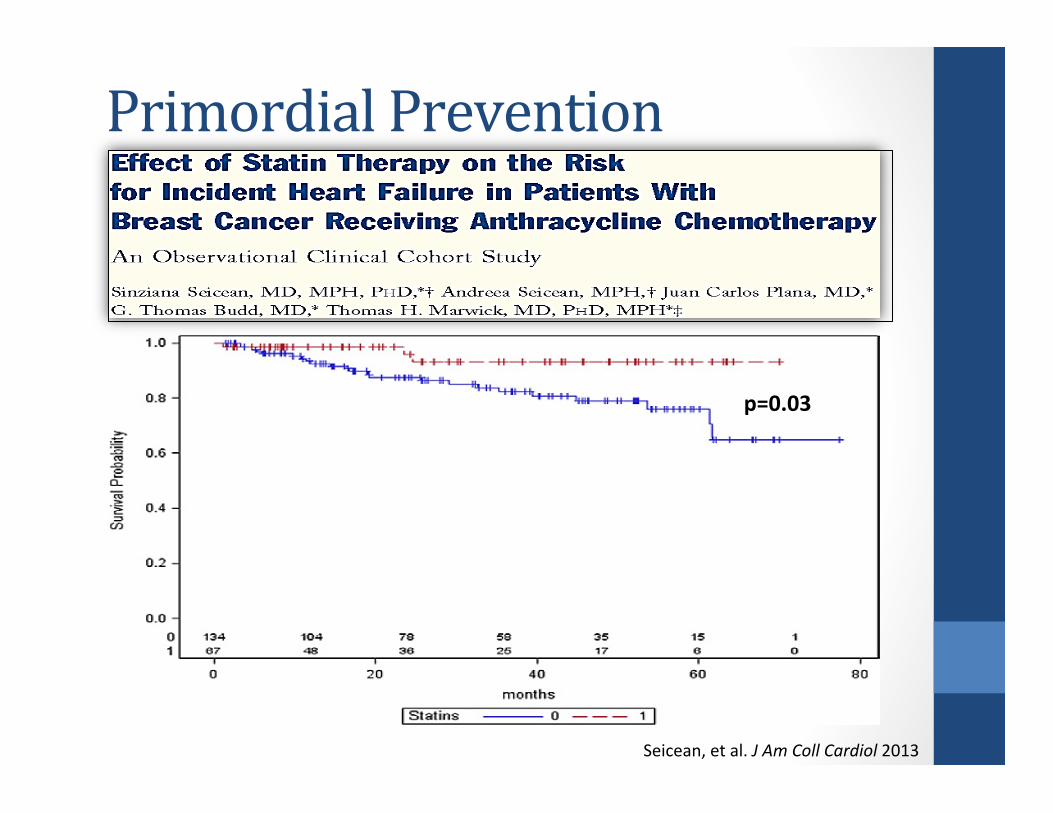
Primordial Prevention
p=0.03
Seicean, et al. J Am Coll Cardiol 2013
LVEF (%
)
Controls ACEI-‐group
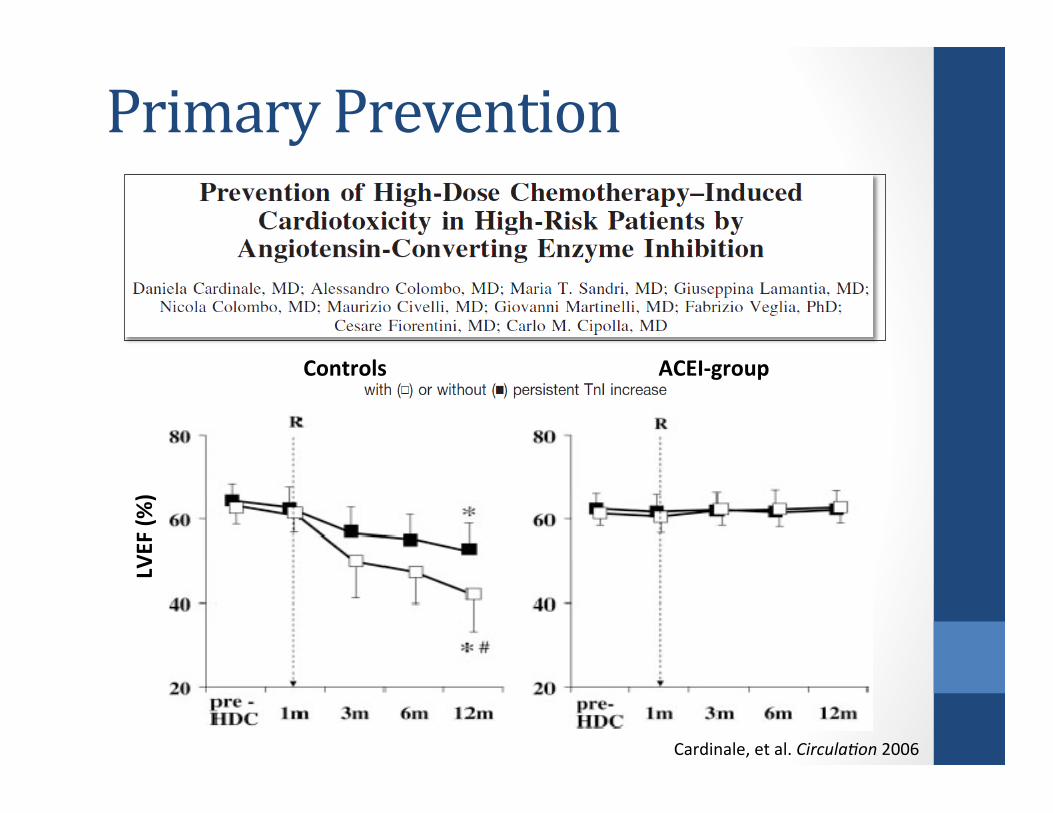
Primary Prevention
Cardinale, et al. Circula9on 2006
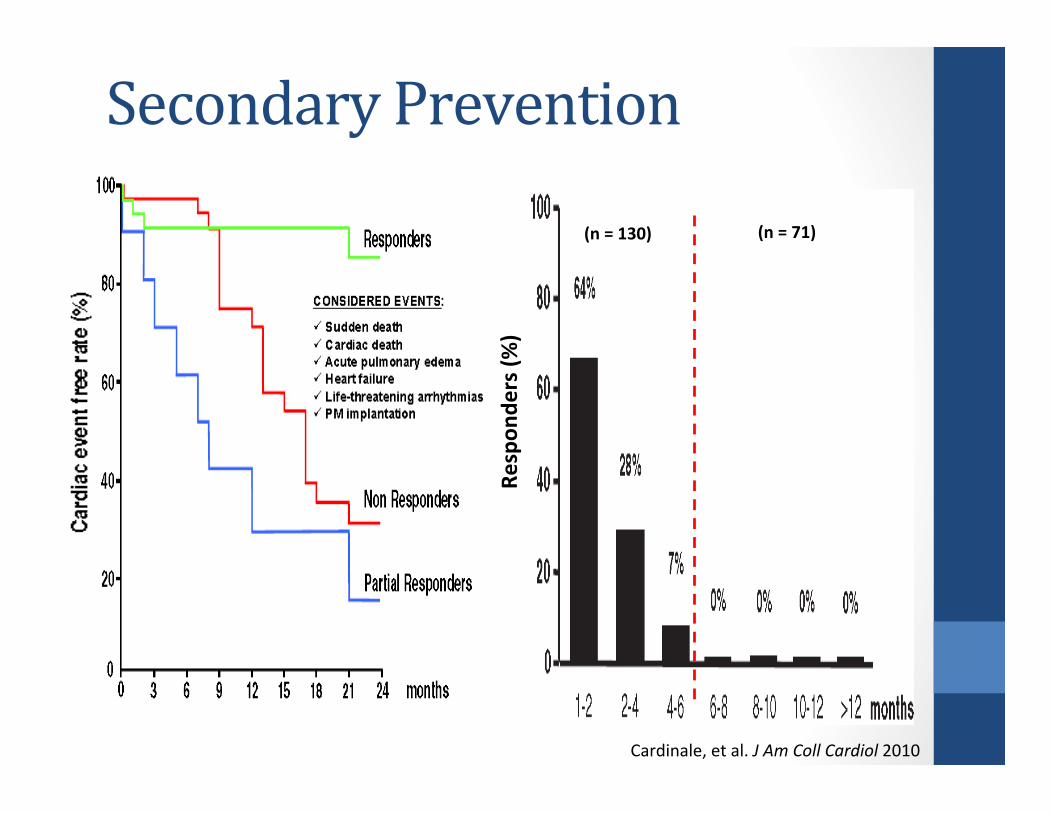
Secondary Prevention
Cardinale, et al. J Am Coll Cardiol 2010
Respon
ders (%
)
(n = 130) (n = 71)
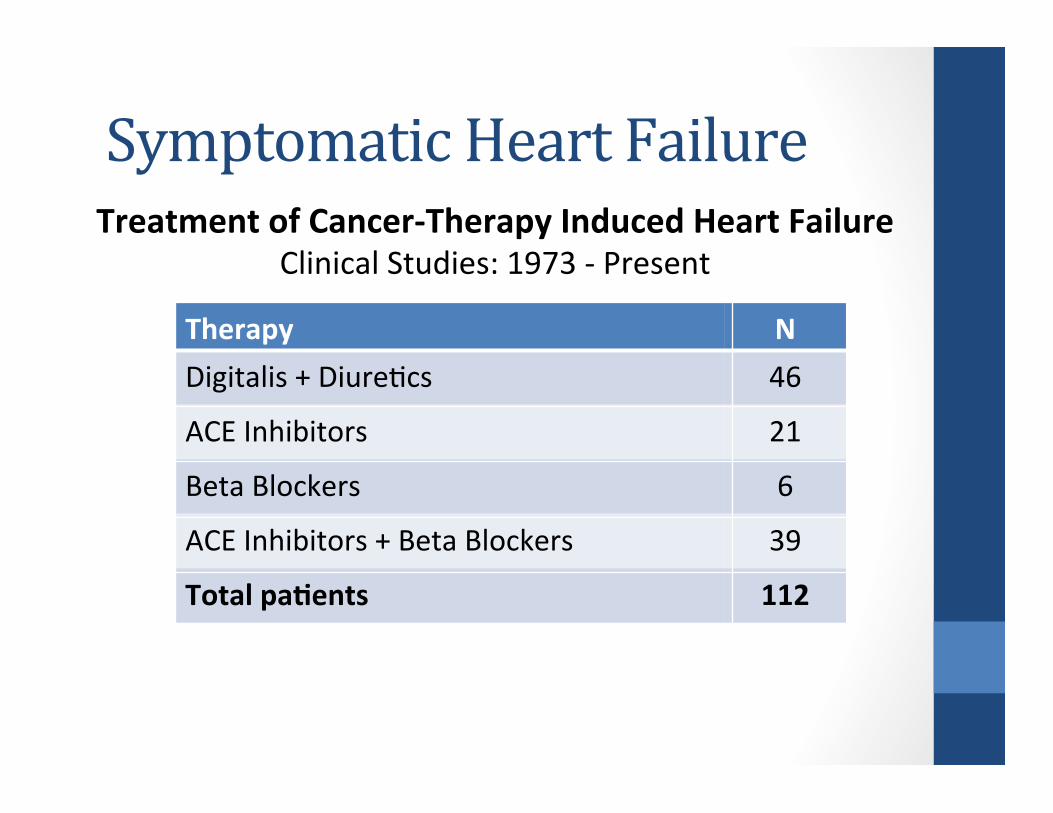
Symptomatic Heart Failure
Therapy N Digitalis + DiureDcs 46
ACE Inhibitors 21
Beta Blockers 6
ACE Inhibitors + Beta Blockers 39
Total paTents 112
Treatment of Cancer-‐Therapy Induced Heart Failure Clinical Studies: 1973 -‐ Present
Summary II • Lack of a universal definiDon of cardiotoxicity
• Limits understanding of true incidence • DetecDon
• Troponin (I, T, hs) has promising predicDve abiliDes • Small trials and variable Dming of assessments limit applicaDon
• Strain and strain rate imaging may detect subclinical cardiac dysfuncDon • PredicDve value remains uncertain
• Abnormal cardiorespiratory fitness may be early mortality risk predictor • CPET may be limited by availability
• Treatment / PrevenDon • Current state of the art therapies – ACE inhibitors and Beta blockers • Evidence limited in CA paDents; based mostly on general HF guidelines • OpDmal Dming and duraDon of medical therapies uncertain • Studies ongoing to evaluate exercise as intervenDon
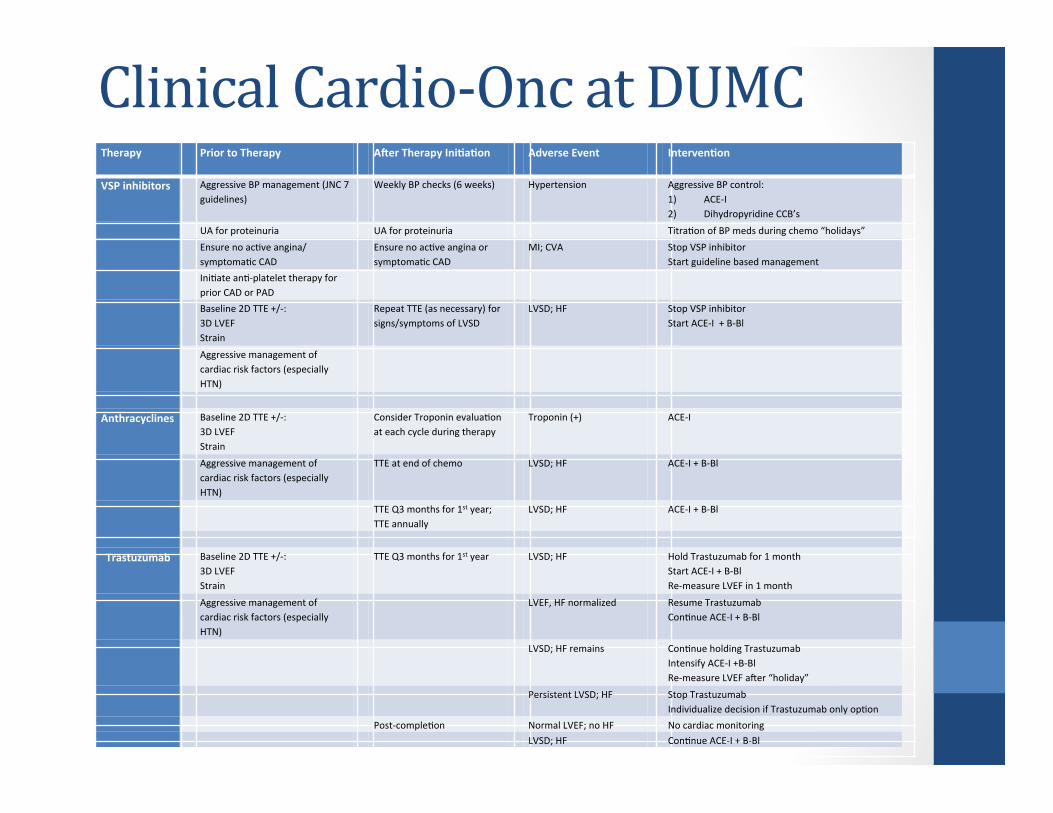
Clinical Cardio-‐Onc at DUMC Therapy Prior to Therapy
Aler Therapy IniTaTon Adverse Event IntervenTon
VSP inhibitors Aggressive BP management (JNC 7 guidelines)
Weekly BP checks (6 weeks) Hypertension Aggressive BP control: 1) ACE-‐I 2) Dihydropyridine CCB’s
UA for proteinuria UA for proteinuria TitraDon of BP meds during chemo “holidays”
Ensure no acDve angina/symptomaDc CAD
Ensure no acDve angina or symptomaDc CAD
MI; CVA Stop VSP inhibitor Start guideline based management
IniDate anD-‐platelet therapy for prior CAD or PAD
Baseline 2D TTE +/-‐: 3D LVEF Strain
Repeat TTE (as necessary) for signs/symptoms of LVSD
LVSD; HF Stop VSP inhibitor Start ACE-‐I + B-‐Bl
Aggressive management of cardiac risk factors (especially HTN)
Anthracyclines
Baseline 2D TTE +/-‐: 3D LVEF Strain
Consider Troponin evaluaDon at each cycle during therapy
Troponin (+) ACE-‐I
Aggressive management of cardiac risk factors (especially HTN)
TTE at end of chemo LVSD; HF ACE-‐I + B-‐Bl
TTE Q3 months for 1st year; TTE annually
LVSD; HF ACE-‐I + B-‐Bl
Trastuzumab Baseline 2D TTE +/-‐: 3D LVEF Strain
TTE Q3 months for 1st year LVSD; HF Hold Trastuzumab for 1 month Start ACE-‐I + B-‐Bl Re-‐measure LVEF in 1 month
Aggressive management of cardiac risk factors (especially HTN)
LVEF, HF normalized Resume Trastuzumab ConDnue ACE-‐I + B-‐Bl
LVSD; HF remains ConDnue holding Trastuzumab Intensify ACE-‐I +B-‐Bl Re-‐measure LVEF aPer “holiday”
Persistent LVSD; HF Stop Trastuzumab Individualize decision if Trastuzumab only opDon
Post-‐compleDon Normal LVEF; no HF No cardiac monitoring LVSD; HF ConDnue ACE-‐I + B-‐Bl





























