Embed Size (px)
DESCRIPTION
Medical surgical nursing
Citation preview

CARDIOLOGY NURSING
THE CARDIOVASCULAR SYSTEM
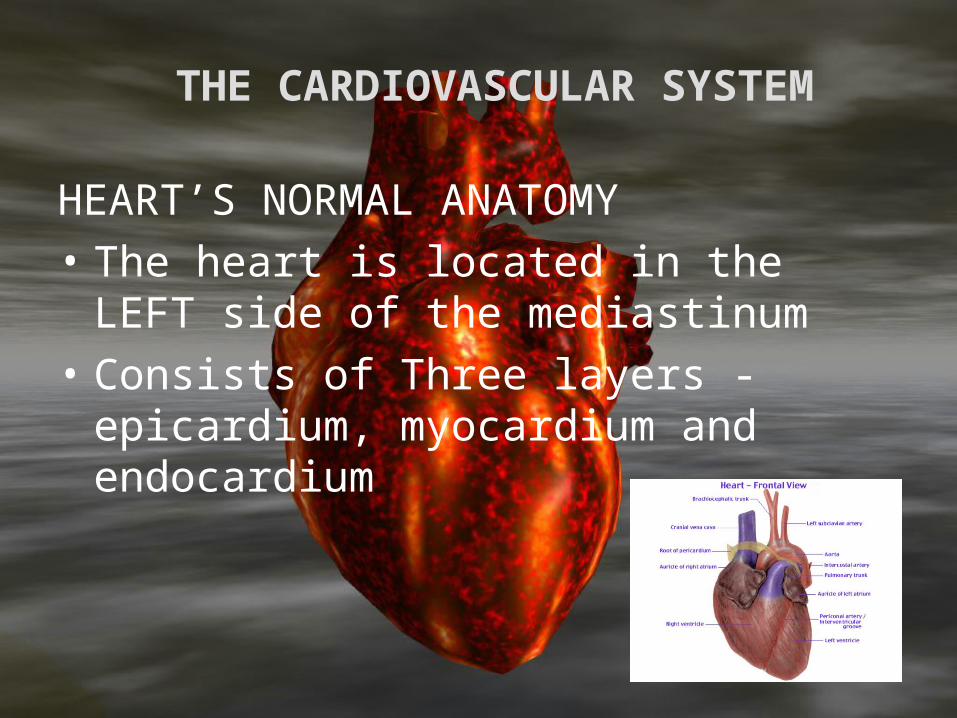
HEART’S NORMAL ANATOMY
• The heart is located in the LEFT side of the mediastinum
• Consists of Three layers - epicardium, myocardium and endocardium

THE CARDIOVASCULAR SYSTEM
• The epicardium covers the outer surface of the heart
• The myocardium is the middle muscular layer of the heart
• The endocardium lines the chambers and the valves

THE CARDIOVASCULAR SYSTEM
• The layer that covers the heart is the PERICARDIUM
• There are two parts - parietal and visceral pericardium
• The space between the two pericardial layers is the pericardial space

THE CARDIOVASCULAR SYSTEM
• The heart also has four chambers - two atria and two ventricles
• The Left atrium and the right atrium
• The left ventricle and the right ventricle

The Cardiovascular System
The heart chambers are guarded by valves
• The atrio-ventricular valves - tricuspid and bicuspid
• The semi-lunar valves - pulmonic and aortic valves

The Cardiovascular System
The Blood supply of the heart comes from the Coronary arteries
1. Right coronary artery supplies the RIGHT atrium and RIGHT ventricle, inferior portion of the LEFT ventricle, the POSTERIOR septal wall and the two nodes - AV (90%) and SA node (55%)

The Cardiovascular System
2. Left coronary artery- branches into the LAD and the circumflex branch
• The LAD supplies blood to the anterior wall of the LEFT ventricle, the anterior septum and the Apex of the left ventricle
• The CIRCUMFLEX branch supplies the left atrium and the posterior LEFT ventricle


The Cardiovascular System
The CONDUCTING SYSTEM OF THE HEART
Consists of the• 1. SA node- the pacemaker• 2. AV node- slowest conduction• 3. Bundle of His – branches into the Right
and the Left bundle branch• 4. Purkinje fibers- fastest conduction


The Cardiovascular System
The Heart sounds
• 1. S1- due to closure of the AV valves
• 2. S2- due to the closure of the semi-lunar valves
• 3. S3- due to increased ventricular filling
• 4. S4- due to forceful atrial contraction

The Cardiovascular System
Heart rate
• Normal range is 60-100 beats per minute
• Tachycardia is greater than 100 bpm
• Bradycardia is less than 60 bpm
• Sympathetic system INCREASES HR
• Parasympathetic system (Vagus) DECREASES HR

The Cardiovascular System
Blood pressure• Cardiac output X peripheral resistance• Control is neural (central and
peripheral) and hormonal• Baroreceptors in the carotid and aorta• Hormones- ADH, aldosterone,
epinephrine can increase BP; ANF can decrease BP

The Cardiovascular System
• The vascular system consists of the arteries, veins and capillaries
• The arteries are vessels that carry blood away from the heart to the periphery
• The veins are the vessels that carry blood to the heart
• The capillaries are lined with squamos cells, they connect the veins and arteries

The Cardiovascular System
• The lymphatic system also is part of the vascular system and the function of this system is to collect the extravasated fluid from the tissues and returns it to the blood

The Cardiovascular System
Cardiac Assessment

The Cardiovascular System
Laboratory Test Rationale
• 1. To assist in diagnosing MI
• 2. To identify abnormalities
• 3. To assess inflammation

The Cardiovascular System
Laboratory Test Rationale• 4. To determine baseline value• 5. To monitor serum level of
medications• 6. To assess the effects of
medications

The Cardiovascular SystemLABORATORY PROCEDURES
CARDIAC Proteins and enzymes
CK- MB ( creatine kinase)Elevates in MI within 4 hours, peaks in 18 hours and then declines till 3 days

The Cardiovascular SystemLABORATORY PROCEDURES
CARDIAC Proteins and enzymes
CK- MB ( creatine kinase)Normal value is 0-7 U/L

The Cardiovascular SystemLABORATORY PROCEDURES
CARDIAC Proteins and enzymes
Lactic Dehydrogenase (LDH)Elevates in MI in 24 hours, peaks in 48-72 hours
Normally LDH1 is greater than LDH2

The Cardiovascular SystemLABORATORY PROCEDURES
CARDIAC Proteins and enzymes
Lactic Dehydrogenase (LDH)MI- LDH2 greater than LDH1 (flipped LDH pattern)
Normal value is 70-200 IU/L

The Cardiovascular SystemLABORATORY PROCEDURES
CARDIAC Proteins and enzymes
MyoglobinRises within 1-3 hoursPeaks in 4-12 hoursReturns to normal in a day

The Cardiovascular SystemLABORATORY PROCEDURES
CARDIAC Proteins and enzymes
MyoglobinNot used aloneMuscular and RENAL disease
can have elevated myoglobin
The Cardiovascular SystemLABORATORY PROCEDURES
Troponin I and T• Troponin I is usually utilized
for MI• Elevates within 3-4 hours,
peaks in 4-24 hours and persists for 7 days to 3 weeks!
• Normal value for Troponin I is less than 0.6 ng/mL

The Cardiovascular SystemLABORATORY PROCEDURES
Troponin I and T• REMEMBER to AVOID IM injections before obtaining blood sample!
• Early and late diagnosis can be made!

The Cardiovascular SystemLABORATORY PROCEDURES
SERUM LIPIDS• Lipid profile measures the
serum cholesterol, triglycerides and lipoprotein levels
• Cholesterol= 200 mg/dL• Triglycerides- 40- 150 mg/dL
The Cardiovascular SystemLABORATORY PROCEDURES
SERUM LIPIDS
• LDH- 130 mg/dL
• HDL- 30-70- mg/dL
• NPO post midnight (usually 12 hours)

The Cardiovascular SystemLABORATORY PROCEDURES
ELECTROCARDIOGRAM (ECG)
• A non-invasive procedure that evaluates the electrical activity of the heart
• Electrodes and wires are attached to the patient



The Cardiovascular SystemLABORATORY PROCEDURESHolter Monitoring• A non-invasive test in which the client wears a Holter monitor and an ECG tracing recorded continuously over a period of 24 hours

The Cardiovascular SystemLABORATORY PROCEDURES
Holter Monitoring• Instruct the client to resume normal activities and maintain a diary of activities and any symptoms that may develop


The Cardiovascular SystemLABORATORY PROCEDURES
ECHOCARDIOGRAM• Non-invasive test that studies
the structural and functional changes of the heart with the use of ultrasound
• No special preparation is needed


The Cardiovascular SystemLABORATORY PROCEDURES
Stress Test• A non-invasive test that
studies the heart during activity and detects and evaluates CAD
• Exercise test, pharmacologic test and emotional test

The Cardiovascular SystemLABORATORY PROCEDURES
Stress Test
• Treadmill testing is the most commonly used stress test
• Used to determine CAD, Chest pain causes, drug effects and dysrhythmias in exercise

The Cardiovascular SystemLABORATORY PROCEDURES
Stress Test• Pre-test: consent may be required, adequate rest , eat a light meal or fast for 4 hours and avoid smoking, alcohol and caffeine

The Cardiovascular SystemLABORATORY PROCEDURES
• Post-test: instruct client to notify the physician if any chest pain, dizziness or shortness of breath . Instruct client to avoid taking a hot shower for 10-12 hours after the test
The Cardiovascular SystemLABORATORY PROCEDURES
Pharmacological stress test
• Use of dipyridamole• Maximally dilates coronary artery
• Side-effect: flushing of face

The Cardiovascular SystemLABORATORY PROCEDURES
Pharmacological stress test
• Pre-test: 4 hours fasting, avoid alcohol, caffeine
• Post test: report symptoms of chest pain

The Cardiovascular SystemLABORATORY PROCEDURES• CARDIAC catheterization• Insertion of a catheter into
the heart and surrounding vessels
• Determines the structure and performance of the heart valves and surrounding vessels

The Cardiovascular SystemLABORATORY PROCEDURES• CARDIAC catheterization• Used to diagnose CAD, assess coronary atery patency and determine extent of atherosclerosis

The Cardiovascular SystemLABORATORY PROCEDURES
• Pretest: Ensure Consent, assess for allergy to seafood and iodine, NPO, document weight and height, baseline VS, blood tests and document the peripheral pulses

The Cardiovascular SystemLABORATORY PROCEDURES
• Pretest: Fast for 8-12 hours, teachings, medications to allay anxiety

The Cardiovascular SystemLABORATORY PROCEDURES
• Intra-test: inform patient of a fluttery feeling as the catheter passes through the heart; inform the patient that a feeling of warmth and metallic taste may occur when dye is administered

The Cardiovascular SystemLABORATORY PROCEDURES
• Post-test: Monitor VS and cardiac rhythm
• Monitor peripheral pulses, color and warmth and sensation of the extremity distal to insertion site
• Maintain sandbag to the insertion site if required to maintain pressure
• Monitor for bleeding and hematoma formation

The Cardiovascular SystemLABORATORY PROCEDURES
• Maintain strict bed rest for 6-12 hours
• Client may turn from side to side but bed should not be elevated more than 30 degrees and legs always straight
• Encourage fluid intake to flush out the dye
• Immobilize the arm if the antecubital vein is used
• Monitor for dye allergy

The Cardiovascular SystemLABORATORY PROCEDURES
CVP• The CVP is the pressure
within the SVC• Reflects the pressure under
which blood is returned to the SVC and right atrium

The Cardiovascular SystemLABORATORY PROCEDURES
CVP• Normal CVP is 0 to 8 mmHg/ 4-10 cm
H2O• Elevated CVP indicates increase in
blood volume, excessive IVF or heart/renal failure
• Low CVP may indicated hypovolemia, hemorrhage and severe vasodilatation

The Cardiovascular SystemLABORATORY PROCEDURES
Measuring CVP• 1. Position the client supine with
bed elevated at 45 degrees• 2. Position the zero point of the CVP
line at the level of the right atrium. Usually this is at the MAL, 4th ICS
• 3. Instruct the client to be relaxed and avoid coughing and straining.


CARDIAC ASSESSMENT
ASSESSMENT1. Health History• Obtain description of present
illness and the chief complaint
• Chest pain, SOB, Edema, etc.• Assess risk factors

CARDIAC ASSESSMENT
2. Physical examination • Vital signs- BP, PP, MAP• Inspection of the skin• Inspection of the thorax• Palpation of the PMI, pulses• Auscultation of the heart sounds


CARDIAC ASSESSMENT
• 3. Laboratory and diagnostic studies• CBC • cardiac catheterization• Lipid profile • arteriography• Cardiac enzymes and proteins• CXR • CVP• EEG• Holter monitoring• Exercise ECG

CARDIAC IMPLEMENTATION
1. Assess the cardio-pulmonary status
VS, BP, Cardiac assessment
2. Enhance cardiac output
– Establish IV line to administer fluids

CARDIAC IMPLEMENTATION
3. Promote gas exchange
–Administer O2
–Position client in SEMI-Fowler’s
–Encourage coughing and deep breathing exercises

CARDIAC IMPLEMENTATION
4. Increase client activity tolerance–Balance rest and activity periods–Assist in daily activities
5. Promote client comfort–Assess the client’s description of
pain and chest discomfort–Administer medication as
prescribed

CARDIAC IMPLEMENTATION
6. Promote adequate sleep7. Prevent infection
–Monitor skin integrity of lower extremities
–Assess skin site for edema, redness and warmth
–Monitor for fever–Change position frequently

CARDIAC IMPLEMENTATION
8. Minimize patient anxiety–Encourage verbalization of feelings, fears and concerns
–Answer client questions. Provide information about procedures and medications

CARDIAC DISEASES
• Coronary Artery Disease• Myocardial Infarction• Congestive Heart Failure• Infective Endocarditis• Cardiac Tamponade• Cardiogenic Shock

VASCULAR DISEASES
• Hypertension• Buerger’s disease• Varicose veins• Deep vein thrombosis• Aneurysm
CAD
• CAD results from the focal narrowing of the large and medium-sized coronary arteries due to deposition of atheromatous plaque in the vessel wall

CADRISK FACTORS• 1. Age above 45/55 and Sex- Males and
post-menopausal females• 2. Family History• 3. Hypertension• 4. DM• 5. Smoking• 6. Obesity• 7. Sedentary lifestyle• 8. Hyperlipedimia

CADRISK FACTORS
Most important MODIFIABLE factors:
• Smoking
• Hypertension
• Diabetes
• Cholesterol abnormalities

CAD
Pathophysiology• Fatty streak formation in the
vascular intima T-cells and monocytes ingest lipids in the area of deposition atheroma narrowing of the arterial lumen reduced coronary blood flow myocardial ischemia

CAD
Pathophysiology• There is decreased perfusion of
myocardial tissue and inadequate myocardial oxygen supply
• If 50% of the left coronary arterial lumen is reduced or 75% of the other coronary artery, this becomes significant
• Potential for Thrombosis and embolism

Angina Pectoris
•Chest pain resulting from coronary atherosclerosis or myocardial ischemia

Angina Pectoris: Clinical Syndromes
Three Common Types of ANGINA
1. STABLE ANGINA–The typical angina that occurs during exertion, relieved by rest and drugs and the severity does not change

Angina Pectoris: Clinical Syndromes
Three Common Types of ANGINA
2. Unstable angina–Occurs unpredictably during exertion and emotion, severity increases with time and pain may not be relieved by rest and drug

Angina Pectoris: Clinical Syndromes
Three Common Types of ANGINA
3. Variant angina–Prinzmetal angina, results from coronary artery VASOSPASMS, may occur at rest

Angina Pectoris
ASSESSMENT FINDINGS1. Chest pain- ANGINA• The most characteristic symptom• PAIN is described as mild to
severe retrosternal pain, squeezing, tightness or burning sensation
• Radiates to the jaw and left arm
Angina Pectoris
ASSESSMENT FINDINGS
1. Chest pain- ANGINA• Precipitated by Exercise, Eating
heavy meals, Emotions like excitement and anxiety and Extremes of temperature
• Relieved by REST and Nitroglycerin
Angina Pectoris
ASSESSMENT FINDINGS• 2. Diaphoresis• 3. Nausea and vomiting• 4. Cold clammy skin• 5. Sense of apprehension and
doom• 6. Dizziness and syncope

Angina Pectoris
LABORATORY FINDINGS1. ECG may show normal tracing if patient
is pain-free. Ischemic changes may show ST depression and T wave inversion
2. Cardiac catheterization–Provides the MOST DEFINITIVE source
of diagnosis by showing the presence of the atherosclerotic lesions

Angina Pectoris
NURSING MANAGEMENT1. Administer prescribed medications• Nitrates- to dilate the coronary arteries• Aspirin- to prevent thrombus formation• Beta-blockers- to reduce BP and HR• Calcium-channel blockers- to dilate
coronary artery and reduce vasospasm
2. Teach the patient management of anginal attacks
• Advise patient to stop all activities • Put one nitroglycerin tablet under the tongue• Wait for 5 minutes• If not relieved, take another tablet and wait for 5
minutes• Another tablet can be taken (third tablet)• If unrelieved after THREE tablets seek medical
attention
Angina Pectoris
3. Obtain a 12-lead ECG4. Promote myocardial perfusion• Instruct patient to maintain bed rest• Administer O2 @ 3 lpm• Advise to avoid valsalva maneuvers• Provide laxatives or high fiber diet
to lessen constipation• Encourage to avoid increased
physical activities

Angina Pectoris
5. Assist in possible treatment modalities• PTCA- percutaneous transluminal
coronary angioplasty–To compress the plaque against the
vessel wall, increasing the arterial lumen
• CABG- coronary artery bypass graft–To improve the blood flow to the
myocardial tissue


Angina Pectoris
6. Provide information to family members to minimize anxiety and promote family cooperation
7. Assist client to identify risk factors that can be modified
8. Refer patient to proper agencies

Myocardial infarction
• Death of myocardial tissue in regions of the heart with abrupt interruption of coronary blood supply


Myocardial infarction
ETIOLOGY and Risk factors• 1. CAD• 2. Coronary vasospasm• 3. Coronary artery occlusion by
embolus and thrombus• 4. Conditions that decrease
perfusion- hemorrhage, shock
Myocardial infarction
Risk factors• 1. Hypercholesterolemia• 2. Smoking• 3. Hypertension• 4. Obesity• 5. Stress• 6. Sedentary lifestyle

Myocardial infarction
PATHOPHYSIOLOGY• Interrupted coronary blood flow
myocardial ischemia anaerobic myocardial metabolism for several hours myocardial death depressed cardiac function triggers autonomic nervous system response further imbalance of myocardial O2 demand and supply

Myocardial infarction
ASSESSMENT findings1. CHEST PAIN• Chest pain is described as
severe, persistent, crushing substernal discomfort
• Radiates to the neck, arm, jaw and back

Myocardial infarction
ASSESSMENT findings1. CHEST PAIN• Occurs without cause, primarily
early morning• NOT relieved by rest or
nitroglycerin• Lasts 30 minutes or longer

Myocardial infarction
Assessment findings• 2. Dyspnea• 3. Diaphoresis• 4. cold clammy skin• 5. N/V• 6. restlessness, sense of doom• 7. tachycardia or bradycardia• 8. hypotension• 9. S3 and dysrhythmias

Myocardial infarction
Laboratory findings• 1. ECG- the ST segment is ELEVATED.
T wave inversion, presence of Q wave• 2. Myocardial enzymes- elevated CK-
MB, LDH and Troponin levels• 3. CBC- may show elevated WBC count • 4. Test after the acute stage- Exercise
tolerance test, thallium scans, cardiac catheterization


Myocardial infarctionNursing Interventions
1. Provide Oxygen at 2 lpm, Semi-fowler’s2. Administer medications
–Morphine to relieve pain– nitrates, thrombolytics, aspirin and
anticoagulants–Stool softener and hypolipidemics
3. Minimize patient anxiety–Provide information as to procedures and
drug therapy

Myocardial infarction
4. Provide adequate rest periods
5. Minimize metabolic demands
–Provide soft diet
–Provide a low-sodium, low cholesterol and low fat diet
6. Minimize anxiety
–Reassure client and provide information as needed
Myocardial infarction
7. Assist in treatment modalities such as PTCA and CABG
8. Monitor for complications of MI- especially dysrhythmias, since ventricular tachycardia can happen in the first few hours after MI
9. Provide client teaching


MI
• Medical Management
• 1. ANALGESIC–The choice is MORPHINE
–It reduces pain and anxiety
–Relaxes bronchioles to enhance oxygenation

MI
• Medical Management
• 2. ACE–Prevents formation of
angiotensin II
–Limits the area of infarction

MI
• Medical Management
• 3. Thrombolytics–Streptokinase, Alteplase
–Dissolve clots in the coronary artery allowing blood to flow

Myocardial infarction
NURSING INTERVENTIONS AFTER ACUTE EPISODE
• 1. Maintain bed rest for the first 3 days
• 2. Provide passive ROM exercises
• 3. Progress with dangling of the feet at side of bed

Myocardial infarction
NURSING INTERVENTIONS AFTER ACUTE EPISODE
• 4. Proceed with sitting out of bed, on the chair for 30 minutes TID
• 5. Proceed with ambulation in the room toilet hallway TID

Myocardial infarction
NURSING INTERVENTIONS AFTER ACUTE EPISODE
Cardiac rehabilitation• To extend and improve quality of
life• Physical conditioning• Patients who are able to walk 3-4
mph are usually ready to resume sexual activities

CARDIOMYOPATHIES
• Heart muscle disease associated with cardiac dysfunction

CARDIOMYOPATHIES
• 1. Dilated Cardiomyopathy• 2. Hypertrophic
Cardiomyopathy• 3. Restrictive cardiomyopathy

DILATED CARDIOMYOPATHY
ASSOCIATED FACTORS
• 1. Heavy alcohol intake
• 2. Pregnancy
• 3. Viral infection
• 4. Idiopathic

DILATED CARDIOMYOPATHY
PATHOPHYSIOLOGY• Diminished contractile
proteins poor contraction decreased blood ejection increased blood remaining in the ventricle ventricular stretching and dilatation.
• SYSTOLIC DYSFUNCTION

HYPERTROPHIC CARDIOMYOPATHY
• Associated factors:
• 1. Genetic
• 2. Idiopathic

HYPERTROPHIC CARDIOMYOPATHY
• Pathophysiology
• Increased size of myocardium reduced ventricular volume increased resistance to ventricular filling diastolic dysfunction

RESTRICTIVE CARDIOMYOPATHY
• Associated factors• 1. Infiltrative diseases like
AMYLOIDOSIS• 2. Idiopathic

RESTRICTIVE CARDIOMYOPATHY
• Pathophysiology• Rigid ventricular wall
impaired stretch and diastolic filling decreased output
• Diastolic dysfunction

CARDIOMYOPATHIES
Assessment findings
• 1. PND
• 2. Orthopnea
• 3. Edema
• 4. Chest pain
• 5. Palpitations
• 6. dizziness
• 7. Syncope with exertion

CARDIOMYOPATHIES
• Laboratory Findings• 1. CXR- may reveal
cardiomegaly• 2. ECHOCARDIOGRAM• 3. ECG• 4. Myocardial Biopsy

CARDIOMYOPATHIES
• Medical Management
• 1. Surgery
• 2. pacemaker insertion
• 3. Pharmacological drugs for symptom relief

CARDIOMYOPATHIES
• Nursing Management
1.Improve cardiac output
• Adequate rest
• Oxygen therapy
• Low sodium diet

CARDIOMYOPATHIES
• Nursing Management
2. Increase patient tolerance
• Schedule activities with rest periods in between

CARDIOMYOPATHIES
• Nursing Management3. Reduce patient anxiety• Support• Offer information about
transplantations• Support family in anticipatory
grieving

Infective endocarditis
• Infection of the heart valves and the endothelial surface of the heart
• Can be acute or chronic

Infective endocarditis
• Etiologic factors• 1. Bacteria- Organism
depends on several factors• 2. Fungi

Infective endocarditis
Risk factors• 1. Prosthetic valves• 2. Congenital malformation• 3. Cardiomyopathy• 4. IV drug users• 5. Valvular dysfunctions

Infective endocarditis
Pathophysiology• Direct invasion of microbes
microbes adhere to damaged valve surface and proliferate damage attracts platelets causing clot formation erosion of valvular leaflets and vegetation can embolize

Infective endocarditis
Assessment findings• 1. Intermittent HIGH fever• 2. anorexia, weight loss• 3. cough, back pain and joint
pain• 4. splinter hemorrhages
under nails

Infective endocarditis
• Assessment findings• 5. Osler’s nodes- painful
nodules on fingerpads• 6. Roth’s spots- pale
hemorrhages in the retina

Infective endocarditis
• Assessment findings• 7. Heart murmurs• 8. Heart failure

Infective endocarditis
• Prevention• Antibiotic prophylaxis if
patient is undergoing procedures like dental extractions, bronchoscopy, surgery, etc.

Infective endocarditis
• LABORATORY EXAM• Blood Cultures to
determine the exact organism

Infective endocarditis
Nursing management• 1. regular monitoring of
temperature, heart sounds • 2. manage infection• 3. long-term antibiotic
therapy

Infective endocarditis
Medical management• 1. Pharmacotherapy• IV antibiotic for 2-6 weeks• Antifungal agents are
given – amphotericin B

Infective endocarditis
Medical management• 2. Surgery• Valvular replacement

CHF
• A syndrome of congestion of both pulmonary and systemic circulation caused by inadequate cardiac function and inadequate cardiac output to meet the metabolic demands of tissues

CHF
• Inability of the heart to pump sufficiently
• The heart is unable to maintain adequate circulation to meet the metabolic needs of the body
• Classified according to the major ventricular dysfunction- Left or Right


CHFEtiology of CHF
• 1. CAD• 2. Valvular heart diseases• 3. Hypertension• 4. MI• 5. Cardiomyopathy• 6. Lung diseases• 7. Post-partum• 8. Pericarditis and cardiac tamponade

New York Heart Association
Class 1• Ordinary physical activity does
NOT cause chest pain and fatigue
• No pulmonary congestion• Asymptomatic• NO limitation of ADLs
New York Heart Association
Class 2• SLIGHT limitation of ADLs• NO symptom at rest• Symptom with INCREASED
activity• Basilar crackles and S3

New York Heart Association
Class 3
• Markedly limitation on ADLs
• Comfortable at rest BUT symptoms present in LESS than ordinary activity

New York Heart Association
Class 4
• SYMPTOMS are present at rest

CHF
PATHOPHYSIOLOGY• LEFT Ventricular pump
failure back up of blood into the pulmonary veins increased pulmonary capillary pressure pulmonary congestion

CHF
PATHOPHYSIOLOGY• LEFT ventricular failure
decreased cardiac output decreased perfusion to the brain, kidney and other tissues oliguria, dizziness

CHF
PATHOPHYSIOLOGY• RIGHT ventricular failure
blood pooling in the venous circulation increased hydrostatic pressure peripheral edema

CHF
PATHOPHYSIOLOGY• RIGHT ventricular failure blood pooling venous congestion in the kidney, liver and GIT

LEFT SIDED CHFASSESSMENT FINDINGS
• 1. Dyspnea on exertion• 2. PND• 3. Orthopnea• 4. Pulmonary crackles/rales• 5. cough with Pinkish, frothy
sputum• 6. Tachycardia

LEFT SIDED CHFASSESSMENT FINDINGS
• 7. Cool extremities• 8. Cyanosis• 9. decreased peripheral pulses• 10. Fatigue• 11. Oliguria• 12. signs of cerebral anoxia

RIGHT SIDED CHFASSESSMENT FINDINGS
• 1. Peripheral dependent, pitting edema
• 2. Weight gain• 3. Distended neck vein• 4. hepatomegaly• 5. Ascites

RIGHT SIDED CHFASSESSMENT FINDINGS
• 6. Body weakness
• 7. Anorexia, nausea
• 8. Pulsus alternans
CHF
LABORATORY FINDINGS• 1. CXR may reveal
cardiomegaly• 2. ECG may identify Cardiac
hypertrophy• 3. Echocardiogram may
show hypokinetic heart
CHF
LABORATORY FINDINGS• 4. ABG and Pulse oximetry may
show decreased O2 saturation• 5. PCWP is increased in LEFT
sided CHF and CVP is increased in RIGHT sided CHF

CHF
NURSING INTERVENTIONS• 1. Assess patient's cardio-
pulmonary status• 2. Assess VS, CVP and
PCWP. Weigh patient daily to monitor fluid retention

CHF
NURSING INTERVENTIONS
• 3. Administer medications- usually cardiac glycosides are given- DIGOXIN or DIGITOXIN, Diuretics, vasodilators and hypolipidemics are prescribed

CHF
NURSING INTERVENTIONS• 4. Provide a LOW sodium
diet. Limit fluid intake as necessary
• 5. Provide adequate rest periods to prevent fatigue

CHF
NURSING INTERVENTIONS• 6. Position on semi-fowler’s
to fowler’s for adequate chest expansion
• 7. Prevent complications of immobility
CHF
NURSING INTERVENTION AFTER THE ACUTE STAGE
• 1. Provide opportunities for verbalization of feelings
• 2. Instruct the patient about the medication regimen- digitalis, vasodilators and diuretics
• 3. Instruct to avoid OTC drugs, Stimulants, smoking and alcohol

CHF
NURSING INTERVENTION AFTER THE ACUTE STAGE
• 4. Provide a LOW fat and LOW sodium diet
• 5. Provide potassium supplements
• 6. Instruct about fluid restriction

CHF
NURSING INTERVENTION AFTER THE ACUTE STAGE
• 7. Provide adequate rest periods and schedule activities
• 8. Monitor daily weight and report signs of fluid retention

CARDIOGENIC SHOCK
• Heart fails to pump adequately resulting to a decreased cardiac output and decreased tissue perfusion
ETIOLOGY• 1. Massive MI• 2. Severe CHF• 3. Cardiomyopathy• 4. Cardiac trauma• 5. Cardiac tamponade

CARDIOGENIC SHOCK
ASSESSMENT FINDINGS• 1. HYPOTENSION• 2. oliguria (less than 30 ml/hour)• 3. tachycardia• 4. narrow pulse pressure• 5. weak peripheral pulses• 6. cold clammy skin• 7. changes in sensorium/LOC• 8. pulmonary congestion

CARDIOGENIC SHOCK
• LABORATORY FINDINGS
• Increased CVP–Normal is 4-10 cmH2O

CARDIOGENIC SHOCK
NURSING INTERVENTIONS• 1. Place patient in a modified
Trendelenburg (shock ) position• 2. Administer IVF, vasopressors and
inotropics such as DOPAMINE and DOBUTAMINE
• 3. Administer O2• 4. Morphine is administered to decreased
pulmonary congestion and to relieve pain

CARDIOGENIC SHOCK
• 5. Assist in intubation, mechanical ventilation, PTCA, CABG, insertion of Swan-Ganz cath and IABP
• 6. Monitor urinary output, BP and pulses
• 7. cautiously administer diuretics and nitrates

CARDIAC TAMPONADE
• A condition where the heart is unable to pump blood due to accumulation of fluid in the pericardial sac (pericardial effusion)

CARDIAC TAMPONADE
• This condition restricts ventricular filling resulting to decreased cardiac output
• Acute tamponade may happen when there is a sudden accumulation of more than 50 ml fluid in the pericardial sac

CARDIAC TAMPONADE
Causative factors
• 1. Cardiac trauma
• 2. Complication of Myocardial infarction
• 3. Pericarditis
• 4. Cancer metastasis

CARDIAC TAMPONADE
ASSESSMENT FINDINGS
• 1. BECK’s Triad- Jugular vein distention, hypotension and distant/muffled heart sound
• 2. Pulsus paradoxus
• 3. Increased CVP
• 4. decreased cardiac output
CARDIAC TAMPONADE
• ASSESSMENT FINDINGS
• 5. Syncope
• 6. anxiety
• 7. dyspnea
• 8. Percussion- Flatness across the anterior chest

CARDIAC TAMPONADE
• Laboratory FINDINGS• 1. Echocardiogram• 2. Chest X-ray

CARDIAC TAMPONADE
NURSING INTERVENTIONS• 1. Assist in PERICARDIOCENTESIS• 2. Administer IVF• 3. Monitor ECG, urine output and BP• 4. Monitor for recurrence of
tamponade

Pericardiocentesis
• Patient is monitored by ECG • Maintain emergency equipments• Elevate head of bed 45-60 degrees• Monitor for complications-
coronary artery rupture, dysrhythmias, pleural laceration and myocardial trauma
HYPERTENSION
• A systolic BP greater than 140 mmHg and a diastolic pressure greater than 90 mmHg over a sustained period, based on two or more BP measurements.

HYPERTENSION
Types of Hypertension
1. Primary or ESSENTIAL–Most common type
2. Secondary –Due to other conditions like
Pheochromocytoma, renovascular hypertension, Cushing’s, Conn’s , SIADH
HYPERTENSION
• CLASSIFICATION OF HYPERTENSION by JNC-VII


HYPERTENSION
PATHOPHYSIOLOGY
• Multi-factorial etiology
• BP= CO (SV X HR) x TPR
• Any increase in the above parameters will increase BP
• 1. Increased sympathetic activity
• 2. Increased absorption of Sodium, and water in the kidney

HYPERTENSION
PATHOPHYSIOLOGY
• Multifactorial etiology
• BP= CO (SV X HR) x TPR
• Any increase in the above parameters will increase BP
• 3. Increased activity of the RAAS
• 4. Increased vasoconstriction of the peripheral vessels
• 5. insulin resistance

HYPERTENSION
• ASSESSMENT FINDINGS
• 1. Headache
• 2. Visual changes
• 3. chest pain
• 4. dizziness
• 5. N/V

HYPERTENSION
• Risk factors for Cardiovascular Problems in Hypertensive patients
Major Risk factors• 1. Smoking• 2. Hyperlipidemia• 3. DM• 4. Age older than 60 • 5. Gender- Male and post menopausal W• 6. Family History
HYPERTENSION
• DIAGNOSTIC STUDIES
• 1. Health history and PE
• 2. Routine laboratory- urinalysis, ECG, lipid profile, BUN, serum creatinine , FBS
• 3. Other lab- CXR, creatinine clearance, 24-huour urine protein

HYPERTENSION
• MEDICAL MANAGEMENT• 1. Lifestyle modification• 2. Drug therapy• 3. Diet therapy

HYPERTENSION
MEDICAL MANAGEMENTDrug therapy
• Diuretics• Beta blockers• Calcium channel blockers• ACE inhibitors• A2 Receptor blockers• Vasodilators

HYPERTENSION
• NURSING INTERVENTIONS• 1. Provide health teaching to
patient• Teach about the disease
process• Elaborate on lifestyle changes• Assist in meal planning to lose
weight

HYPERTENSION
• NURSING INTERVENTIONS• 1. Provide health teaching to the
patient• Provide list of LOW fat , LOW
sodium diet of less than 2-3 grams of Na/day
• Limit alcohol intake to 30 ml/day• Regular aerobic exercise• Advise to completely Stop smoking

HYPERTENSION
• Nursing Interventions• 2. Provide information about anti-
hypertensive drugs• Instruct proper compliance and not abrupt
cessation of drugs even if pt becomes asymptomatic/ improved condition
• Instruct to avoid over-the-counter drugs that may interfere with the current medication

HYPERTENSION
• Nursing Intervention• 3. Promote Home care management• Instruct regular monitoring of BP• Involve family members in care• Instruct regular follow-up• 4. Manage hypertensive emergency
and urgency properly

Vascular Diseases

ANEURYSM
• Dilation involving an artery formed at a weak point in the vessel wall

ANEURYSM
• Saccular= when one side of the vessel is affected
• Fusiform= when the entire segment becomes dilated

ANEURYSM
• RISK FACTORS
1. Atherosclerosis
2. Infection= syphilis
3. Connective tissue disorder
4. Genetic disorder= Marfan’s Syndrome

ANEURYSM
• PATHOPHYSIOLOGY
Damage to the intima and media weakness outpouching
Dissecting aneurysm tear in the intima and media with dissection of blood through the layers
ANEURYSM
• ASSESSMENT
1. Asymptomatic
2. Pulsatile sensation on the abdomen
3. Palpable bruit

ANEURYSM
LABORATORY:
• CT scan
• Ultrasound
• X-ray
• Aortography

ANEURYSM
Medical Management:
• Anti-hypertensives
• Synthetic graft
ANEURYSM
Nursing Management:
• Administer medications
• Emphasize the need to avoid increased abdominal pressure
• No deep abdominal palpation
• Remind patient the need for serial ultrasound to detect diameter changes

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Refers to arterial insufficiency of the extremities usually secondary to peripheral atherosclerosis.
• Usually found in males age 50 and above
• The legs are most often affected

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Risk factors for Peripheral Arterial occlusive disease
• Non-Modifiable
• 1. Age
• 2. gender
• 3. family predisposition

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Risk factors for Peripheral Arterial occlusive disease
Modifiable• 1. Smoking • 2. HPN• 3. Obesity• 4. Sedentary lifestyle• 5. DM• 6. Stress

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
ASSESSMENT FINDINGS• 1. INTERMITTENT CLAUDICATION-
the hallmark of PAOD• This is PAIN described as aching,
cramping or fatiguing discomfort consistently reproduced with the same degree of exercise or activity

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• ASSESSMENT FINDINGS• 1. INTERMITTENT
CLAUDICATION- the hallmark of PAOD
• This pain is RELIEVED by REST• This commonly affects the
muscle group below the arterial occlusion

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Assessment Findings• 2. Progressive pain on the
extremity as the disease advances
• 3. Sensation of cold and numbness of the extremities

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Assessment Findings• 4. Skin is pale when elevated
and cyanotic/ruddy when placed on a dependent position
• 5. Muscle atrophy, leg ulceration and gangrene

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Diagnostic Findings
• 1. Unequal pulses between the extremities
• 2. Duplex ultrasonography
• 3. Doppler flow studies

PAOD
• Medical Management
1. Drug therapy• Pentoxyfylline (Trental) reduces blood
viscosity and improves supply of O2 blood to muscles
• Cilostazol (Pletaal) inhibits platelet aggregation and increases vasodilatation
• 2. Surgery- Bypass graft and anastomoses

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Nursing Interventions
1. Maintain Circulation to the extremity• Evaluate regularly peripheral pulses,
temperature, sensation, motor function and capillary refill time
• Administer post-operative care to patient who underwent surgery

PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Nursing Interventions2. Monitor and manage complications• Note for bleeding, hematoma,
decreased urine output• Elevate the legs to diminish edema• Encourage exercise of the extremity
while on bed• Teach patient to avoid leg-crossing
PERIPHERAL ARTERIAL OCCLUSIVE DISEASE
• Nursing Interventions
3. Promote Home management
• Encourage lifestyle changes
• Instruct to AVOID smoking
• Instruct to avoid leg crossing

BUERGER’S DISEASE
• Thromboangiitis obliterans
• A disease characterized by recurring inflammation of the medium and small arteries and veins of the lower extremities
• Occurs in MEN ages 20-35
• RISK FACTOR: SMOKING!

BUERGER’S DISEASE
PATHOPHYSIOLOGY
• Cause is UNKNOWN
• Probably an Autoimmune disease
• Inflammation of the arteries thrombus formation occlusion of the vessels

BUERGER’S DISEASE
• ASSESSMENT FINDINGS
1. Leg PAIN• Foot cramps in the arch (instep
claudication) after exercise• Relieved by rest• Aggravated by smoking, emotional
disturbance and cold chilling
2. Digital rest pain not changed by activity or rest

BUERGER’S DISEASE
• ASSESSMENT FINDINGS
• 3. Intense RUBOR (reddish-blue discoloration), progresses to CYANOSIS as disease advances
• 4. Paresthesia

BUERGER’S DISEASE
• Diagnostic Studies• 1. Duplex ultrasonography• 2. Contrast angiography

BUERGER’S DISEASE
• Nursing Interventions
1. Assist in the medical and surgical management
• Bypass graft• amputation
2. Strongly advise to AVOID smoking
3. Manage complications appropriately

• Medical Management
1. Drug therapy• Pentoxyfylline (Trental) reduces blood
viscosity and improves supply of O2 blood to muscles
• Cilostazol (Pletaal) inhibits platelet aggregation and increases vasodilatation
• 2. Surgery- Bypass graft and anastomoses

BUERGER’S DISEASE
• Nursing InterventionsPost-operative care: after amputation• Elevate stump for the FIRST 24 HOURS to
minimize edema and promote venous return
• Place patient on PRONE position after 24 hours
• Assess skin for bleeding and hematoma• Wrap the extremity with elastic bandage

RAYNAUD’S DISEASE
• A form of intermittent arteriolar VASOCONSTRICTION that results in coldness, pain and pallor of the fingertips or toes
• Cause : UNKNOWN• Most commonly affects WOMEN,
16- 40 years old
RAYNAUD’S DISEASE
• ASSESSMENT FINDINGS1. Raynaud’s phenomenon• A localized episode of
vasoconstriction of the small arteries of the hands and feet that causes color and temperature changes

RAYNAUD’S DISEASE
• W-B-R• Pallor- due to vasoconstriction,
then• Blue- due to pooling of
Deoxygenated blood• Red- due to exaggerated
reflow/hyperemia

RAYNAUD’S DISEASE
• ASSESSMENT FINDINGS2. tingling sensation
3. Burning pain on the hands and feet

RAYNAUD’S DISEASE
• Medical management• Drug therapy with the use of
CALCIUM channel blockers–To prevent vasospasms

RAYNAUD’S DISEASE
• Nursing Interventions• 1. instruct patient to avoid situations
that may be stressful• 2. instruct to avoid exposure to cold
and remain indoors when the climate is cold
• 3. instruct to avoid all kinds of nicotine• 4. instruct about safety. Careful
handling of sharp objects

Venous diseases

VARICOSE VEINS
• THESE are dilated veins usually in the lower extremities

VARICOSE VEINS
• Predisposing Factors–Pregnancy–Prolonged standing or sitting
–Constipation (for hemorrhoids)
–Incompetent venous valves

VARICOSE VEINS
• Pathophysiology–Factors venous stasis increased hydrostatic pressure edema

VARICOSE VEINS
• Assessment findings–Tortuous superficial veins on the legs
–Leg pain and Heaviness–Dependent edema

VARICOSE VEINS
• Laboratory findings–Venography–Duplex scan pletysmography

VARICOSE VEINS
• Medical management–Pharmacological therapy–Leg vein stripping–Anti-embolic stockings

VARICOSE VEINS
• Nursing management• 1. Advise patient to elevate
the legs• 2. Caution patient to avoid
prolonged standing or sitting
VARICOSE VEINS
• Nursing management• 3. Provide high-fiber foods
to prevent constipation• 4. Teach simple exercise to
promote venous return

VARICOSE VEINS
• Nursing management
• 5. Caution patient to avoid knee-length stockings and constrictive clothings

VARICOSE VEINS
• Nursing management• 6. Apply anti-embolic stockings as directed
• 7. Avoid massage on the affected area

DVT- Deep Vein Thrombosis
• Inflammation of the deep veins of the lower extremities and the pelvic veins
• The inflammation results to formation of blood clots in the area

DVT- Deep Vein Thrombosis
• Predisposing factors–Prolonged immobility
–Varicosities
–Traumatic procedures

DVT- Deep Vein Thrombosis
•Complication
–PULMONARY thromboembolism
DVT- Deep Vein Thrombosis
• Assessment findings
• Leg tenderness
• Leg pain and edema
• Positive HOMAN’s SIGN

DVT- Deep Vein Thrombosis
• Laboratory findings
• Venography
• Duplex scan

DVT- Deep Vein Thrombosis
• Medical management–Antiplatelets–Anticoagulants–Vein stripping and grafting–Anti-embolic stockings

DVT- Deep Vein Thrombosis
• Nursing management
• 1. Provide measures to avoid prolonged immobility
–Repositioning Q2
–Provide passive ROM
–Early ambulation

DVT- Deep Vein Thrombosis
• Nursing management• 2. Provide skin care to
prevent the complication of leg ulcers
• 3. Provide anti-embolic stockings

DVT- Deep Vein Thrombosis
• Nursing management• 4. Administer
anticoagulants as prescribed
• 5. Monitor for signs of pulmonary embolism


Blood disordersBlood disorders
AnemiaAnemiaNutritional anemiaNutritional anemiaHemolytic anemiaHemolytic anemiaAplastic anemiaAplastic anemiaSickle cell anemiaSickle cell anemia

ANEMIAANEMIA
A condition in A condition in which the which the hemoglobin hemoglobin concentration is concentration is lower than normallower than normal

ANEMIAANEMIA
Three broad categoriesThree broad categories1. Loss of RBC- occurs with 1. Loss of RBC- occurs with
bleedingbleeding2. Decreased RBC 2. Decreased RBC
productionproduction3. Increased RBC 3. Increased RBC
destructiondestruction

Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency AnemiaIron Deficiency Anemia–Results when the Results when the dietary intake of iron dietary intake of iron is inadequate to is inadequate to produce hemoglobinproduce hemoglobin
Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency AnemiaIron Deficiency Anemia–Etiologic FactorsEtiologic Factors–1. Bleeding- the most 1. Bleeding- the most common causecommon cause
–2. Mal-absorption2. Mal-absorption–3. Malnutrition3. Malnutrition–4. Alcoholism4. Alcoholism

Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency Iron Deficiency AnemiaAnemia
PathophysiologyPathophysiology–The body stores of iron The body stores of iron decrease, leading to decrease, leading to depletion of depletion of hemoglobin synthesishemoglobin synthesis

Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency AnemiaIron Deficiency AnemiaPathophysiologyPathophysiology
–The oxygen carrying The oxygen carrying capacity of hemoglobin is capacity of hemoglobin is reducedreduced tissue hypoxia tissue hypoxia

Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency AnemiaIron Deficiency AnemiaAssessment FindingsAssessment Findings1. Pallor of the skin and 1. Pallor of the skin and mucous membranemucous membrane
2. Weakness and fatigue2. Weakness and fatigue3. General malaise3. General malaise4. Pica4. Pica

Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency AnemiaIron Deficiency AnemiaAssessment FindingsAssessment Findings5. Brittle nails5. Brittle nails6. Smooth and sore 6. Smooth and sore tonguetongue
7. Angular cheilosis7. Angular cheilosis

Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency AnemiaIron Deficiency AnemiaLaboratory findingsLaboratory findings1. CBC- Low levels of Hct, 1. CBC- Low levels of Hct, Hgb and RBC countHgb and RBC count
2. low serum iron, low 2. low serum iron, low ferritinferritin
3. Bone marrow aspiration- 3. Bone marrow aspiration- MOST definitiveMOST definitive

Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency AnemiaIron Deficiency AnemiaMedical managementMedical management1. Hematinics1. Hematinics2. Blood transfusion2. Blood transfusion

Hypoproliferative AnemiaHypoproliferative Anemia
Iron Deficiency AnemiaIron Deficiency AnemiaNursing ManagementNursing Management1. Provide iron rich-foods1. Provide iron rich-foods
–Organ meats (liver)Organ meats (liver)–BeansBeans–Leafy green vegetablesLeafy green vegetables–Raisins and molassesRaisins and molasses

Hypoproliferative AnemiaHypoproliferative Anemia
Nursing ManagementNursing Management2. Administer iron 2. Administer iron Oral preparations tablets- Fe Oral preparations tablets- Fe
fumarate, sulfate and gluconatefumarate, sulfate and gluconate Advise to take iron ONE hour Advise to take iron ONE hour
before mealsbefore meals Take it with vitamin CTake it with vitamin C Continue taking it for several Continue taking it for several
monthsmonths

Hypoproliferative AnemiaHypoproliferative AnemiaNursing ManagementNursing Management2. Administer iron 2. Administer iron Oral preparations- liquidOral preparations- liquid It stains teethIt stains teeth Drink it with a strawDrink it with a straw Stool may turn blackish- dark Stool may turn blackish- dark
in colorin color Advise to eat high-fiber diet to Advise to eat high-fiber diet to
counteract constipationcounteract constipation

Hypoproliferative AnemiaHypoproliferative AnemiaNursing ManagementNursing Management2. Administer iron 2. Administer iron IM preparationIM preparation Administer DEEP IM using the Administer DEEP IM using the
Z-track methodZ-track method Avoid vigorous rubbingAvoid vigorous rubbing Can cause local pain and Can cause local pain and
stainingstaining

APLASTIC ANEMIAAPLASTIC ANEMIA
A condition A condition characterized by characterized by decreased number decreased number of RBC as well as of RBC as well as WBC and plateletsWBC and platelets

APLASTIC ANEMIAAPLASTIC ANEMIA
CAUSATIVE FACTORSCAUSATIVE FACTORS1. Environmental toxins- 1. Environmental toxins-
pesticides, benzenepesticides, benzene2. Certain drugs- 2. Certain drugs-
Chemotherapeutic agents, Chemotherapeutic agents, chloramphenicol, chloramphenicol, phenothiazines, Sulfonamidesphenothiazines, Sulfonamides
3. Heavy metals3. Heavy metals4. Radiation4. Radiation

APLASTIC ANEMIAAPLASTIC ANEMIA
PathophysiologyPathophysiologyToxins cause a direct bone Toxins cause a direct bone marrow depressionmarrow depression acellualr bone marrowacellualr bone marrow decreased production of decreased production of blood elementsblood elements
APLASTIC ANEMIAAPLASTIC ANEMIA
ASSESSMENT FINDINGSASSESSMENT FINDINGS1. fatigue1. fatigue2. pallor2. pallor3. dyspnea3. dyspnea4. bruising4. bruising5. splenomegaly5. splenomegaly6. retinal hemorrhages6. retinal hemorrhages

APLASTIC ANEMIAAPLASTIC ANEMIA
LABORATORY FINDINGSLABORATORY FINDINGS1. CBC- decreased blood 1. CBC- decreased blood cell numberscell numbers
2. Bone marrow 2. Bone marrow aspiration confirms the aspiration confirms the anemia- hypoplastic or anemia- hypoplastic or acellular marrow acellular marrow replaced by fatsreplaced by fats

APLASTIC ANEMIAAPLASTIC ANEMIA
Medical ManagementMedical Management1. Bone marrow 1. Bone marrow transplantationtransplantation
2. Immunosupressant 2. Immunosupressant drugsdrugs
3. Rarely, steroids3. Rarely, steroids4. Blood transfusion4. Blood transfusion

APLASTIC ANEMIAAPLASTIC ANEMIA
Nursing managementNursing management1. Assess for signs of 1. Assess for signs of bleeding and bleeding and infectioninfection
2. Instruct to avoid 2. Instruct to avoid exposure to offending exposure to offending agentsagents

Megaloblastic AnemiasMegaloblastic Anemias
Anemias characterized Anemias characterized by abnormally large RBC by abnormally large RBC secondary to impaired secondary to impaired DNA synthesis due to DNA synthesis due to deficiency of Folic acid deficiency of Folic acid and/or vitamin B12 and/or vitamin B12

Megaloblastic AnemiasMegaloblastic Anemias
Folic Acid deficiencyFolic Acid deficiencyCausative factorsCausative factors1. Alcoholism1. Alcoholism2. Mal-absorption2. Mal-absorption3. Diet deficient in 3. Diet deficient in uncooked vegetablesuncooked vegetables

Megaloblastic AnemiasMegaloblastic AnemiasPathophysiology of Folic acid Pathophysiology of Folic acid
deficiencydeficiencyDecreased folic acidDecreased folic acid impaired impaired
DNA synthesis in the bone DNA synthesis in the bone marrowmarrow impaired RBC impaired RBC development, impaired nuclear development, impaired nuclear maturation but CYTOplasmic maturation but CYTOplasmic maturation continuesmaturation continues large large sizesize

Megaloblastic AnemiasMegaloblastic Anemias
Vitamin B12 deficiencyVitamin B12 deficiencyCausative factorsCausative factors1. Strict vegetarian diet1. Strict vegetarian diet2. Gastrointestinal 2. Gastrointestinal
malabsorptionmalabsorption3. Crohn's disease3. Crohn's disease4. gastrectomy4. gastrectomy

Megaloblastic AnemiasMegaloblastic Anemias
Vitamin B12 deficiencyVitamin B12 deficiency
Pernicious AnemiaPernicious Anemia Due to the absence of intrinsic Due to the absence of intrinsic
factor secreted by the parietal factor secreted by the parietal cells cells
Intrinsic factor binds with Vit. Intrinsic factor binds with Vit. B12 to promote absorptionB12 to promote absorption

Megaloblastic AnemiasMegaloblastic Anemias
Assessment findingsAssessment findings 1. weakness1. weakness 2. fatigue2. fatigue 3. listless3. listless 4. neurologic manifestations 4. neurologic manifestations
are present only in Vit. B12 are present only in Vit. B12 deficiencydeficiency

Megaloblastic AnemiasMegaloblastic Anemias
Assessment findingsAssessment findings Pernicious AnemiaPernicious Anemia
– Beefy, red, swollen tongueBeefy, red, swollen tongue– Mild diarrheaMild diarrhea– Extreme pallorExtreme pallor– Paresthesias in the extremitiesParesthesias in the extremities

Megaloblastic AnemiasMegaloblastic Anemias
Laboratory findingsLaboratory findings 1. Peripheral blood smear- 1. Peripheral blood smear-
shows giant RBCs, WBCs with shows giant RBCs, WBCs with giant hypersegmented nucleigiant hypersegmented nuclei
2. Very high MCV2. Very high MCV 3. Schilling’s test3. Schilling’s test 4. Intrinsic factor antibody test4. Intrinsic factor antibody test

Megaloblastic AnemiasMegaloblastic Anemias
Medical ManagementMedical Management 1. Vitamin supplementation1. Vitamin supplementation
– Folic acid 1 mg dailyFolic acid 1 mg daily 2. Diet supplementation2. Diet supplementation
– Vegetarians should have vitamin Vegetarians should have vitamin intakeintake
3. Lifetime monthly injection 3. Lifetime monthly injection of IM Vit B12of IM Vit B12

Megaloblastic AnemiasMegaloblastic Anemias
Nursing ManagementNursing Management 1. Monitor patient1. Monitor patient 2. Provide assistance in 2. Provide assistance in
ambulationambulation 3. Oral care for tongue sore3. Oral care for tongue sore 4. Explain the need for 4. Explain the need for
lifetime IM injection of vit B12lifetime IM injection of vit B12

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
A severe chronic A severe chronic incurable hemolytic incurable hemolytic anemia that results anemia that results from heritance of the from heritance of the sickle hemoglobin sickle hemoglobin gene.gene.

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Causative factorCausative factor–Genetic inheritance Genetic inheritance of the sickle gene- of the sickle gene- HbS geneHbS gene

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
PathophysiologyPathophysiologyDecreased O2, Cold, Decreased O2, Cold, Vasoconstriction can Vasoconstriction can precipitate sickling precipitate sickling processprocess

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCellPathophysiologyPathophysiology
FactorsFactors cause defective cause defective hemoglobin to acquire a hemoglobin to acquire a rigid, crystal-like C-shaped rigid, crystal-like C-shaped configurationconfiguration Sickled Sickled RBCs will adhere to RBCs will adhere to endotheliumendothelium pile up and pile up and plug the vesselsplug the vessels ischemia resultsischemia results pain, pain, swelling and feverswelling and fever

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Assessment FindingsAssessment Findings1. jaundice1. jaundice2. enlarged skull and 2. enlarged skull and facial bonesfacial bones
3. tachycardia, 3. tachycardia, murmurs and murmurs and cardiomegalycardiomegaly
Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Assessment FindingsAssessment FindingsPrimary sites of Primary sites of thrombotic occlusion: thrombotic occlusion: spleen, lungs and CNSspleen, lungs and CNS
Chest pain, dyspneaChest pain, dyspnea

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Assessment FindingsAssessment Findings1. Sickle cell crises1. Sickle cell crises
–Results from tissue hypoxia Results from tissue hypoxia and necrosisand necrosis
2. Acute chest syndrome2. Acute chest syndrome–Manifested by a rapidly Manifested by a rapidly falling hemoglobin level, falling hemoglobin level, tachycardia, fever and tachycardia, fever and chest infiltrates in the CXRchest infiltrates in the CXR

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Medical ManagementMedical Management1. Bone marrow 1. Bone marrow transplanttransplant
2. Hydroxyurea2. Hydroxyurea–Increases the HbFIncreases the HbF
3. Long term RBC 3. Long term RBC trnasfusiontrnasfusion

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Nursing ManagementNursing Management1. manage the pain1. manage the pain
–Support and elevate Support and elevate acutely inflamed jointacutely inflamed joint
–Relaxation techniquesRelaxation techniques–analgesicsanalgesics

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Nursing ManagementNursing Management2. Prevent and manage 2. Prevent and manage infectioninfection–Monitor status of Monitor status of patientpatient
–Initiate prompt Initiate prompt antibiotic therapyantibiotic therapy

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Nursing ManagementNursing Management3. Promote coping skills3. Promote coping skills
–Provide accurate Provide accurate informationinformation
–Allow patient to verbalize Allow patient to verbalize her concerns about her concerns about medication, prognosis medication, prognosis and future pregnancyand future pregnancy

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Nursing ManagementNursing Management4. Monitor and prevent 4. Monitor and prevent potential complicationspotential complications–Provide always adequate Provide always adequate hydrationhydration
–Avoid cold, temperature Avoid cold, temperature that may cause that may cause vasoconstrictionvasoconstriction
Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Nursing ManagementNursing Management4. Monitor and 4. Monitor and prevent potential prevent potential complicationscomplications–Leg ulcerLeg ulcer
Aseptic techniqueAseptic technique

Hemolytic Anemia: Sickle Hemolytic Anemia: Sickle CellCell
Nursing ManagementNursing Management4. Monitor and prevent 4. Monitor and prevent potential complicationspotential complications–PriapismPriapism
Sudden painful erectionSudden painful erectionInstruct patient to empty Instruct patient to empty bladder, then take a bladder, then take a warm bathwarm bath

PolycythemiaPolycythemia
Refers to an INCREASE Refers to an INCREASE volume of RBCsvolume of RBCs
The hematocrit is The hematocrit is ELEVATED to more than ELEVATED to more than 55%55%
Clasified as Primary or Clasified as Primary or SecondarySecondary

PolycythemiaPolycythemia
POLYCYTHEMIA VERAPOLYCYTHEMIA VERA–Primary PolycythemiaPrimary Polycythemia–A proliferative disorder A proliferative disorder in which the myeloid in which the myeloid stem cells become stem cells become uncontrolled uncontrolled
PolycythemiaPolycythemia
POLYCYTHEMIA VERAPOLYCYTHEMIA VERACausative factorCausative factor
–unknownunknown

PolycythemiaPolycythemiaPOLYCYTHEMIA VERAPOLYCYTHEMIA VERAPathophysiologyPathophysiology
–The stem cells grow The stem cells grow uncontrollablyuncontrollably
–The bone marrow becomes The bone marrow becomes HYPERcellular and all the blood HYPERcellular and all the blood cells are increased in numbercells are increased in number

PolycythemiaPolycythemiaPOLYCYTHEMIA VERAPOLYCYTHEMIA VERAPathophysiologyPathophysiology
–The spleen resumes its function The spleen resumes its function of hematopoiesis and enlargesof hematopoiesis and enlarges
–Blood becomes thick and Blood becomes thick and viscous causing sluggish viscous causing sluggish circulationcirculation

PolycythemiaPolycythemiaPOLYCYTHEMIA VERAPOLYCYTHEMIA VERAPathophysiologyPathophysiology
–Overtime, the bone Overtime, the bone marrow becomes fibroticmarrow becomes fibrotic

PolycythemiaPolycythemiaPOLYCYTHEMIA VERAPOLYCYTHEMIA VERAAssessment findingsAssessment findings
–1. Skin is ruddy1. Skin is ruddy–2. Splenomegaly2. Splenomegaly–3. headache3. headache–4. dizziness, blurred vision4. dizziness, blurred vision–5. Angina, dyspnea and 5. Angina, dyspnea and thrombophlebitisthrombophlebitis

PolycythemiaPolycythemiaPOLYCYTHEMIA VERAPOLYCYTHEMIA VERALaboratory findingsLaboratory findings
–1. CBC- shows elevated RBC 1. CBC- shows elevated RBC massmass
–2. Normal oxygen saturation2. Normal oxygen saturation–3 Elevated WBC and 3 Elevated WBC and PlateletsPlatelets

PolycythemiaPolycythemiaPOLYCYTHEMIA VERAPOLYCYTHEMIA VERAComplicationsComplications
–1. Increased risk for 1. Increased risk for thrombophlebitis, CVA and thrombophlebitis, CVA and MIMI
–2. Bleeding due to 2. Bleeding due to dysfunctional blood cellsdysfunctional blood cells

PolycythemiaPolycythemiaPOLYCYTHEMIA VERAPOLYCYTHEMIA VERAMedical ManagementMedical Management
–1. To reduce the high blood cell 1. To reduce the high blood cell mass- PHLEBOTOMYmass- PHLEBOTOMY
–2. Allopurinol2. Allopurinol–3. Dipyridamole3. Dipyridamole–4. Chemotherapy to suppress 4. Chemotherapy to suppress bone marrowbone marrow

PolycythemiaPolycythemia Nursing ManagementNursing Management
– 1. Primary role of the nurse is 1. Primary role of the nurse is EDUCATOREDUCATOR
– 2. Regularly asses for the 2. Regularly asses for the development of complicationsdevelopment of complications
– 3. Assist in weekly phlebotomy3. Assist in weekly phlebotomy– 4. Advise to avoid alcohol and aspirin4. Advise to avoid alcohol and aspirin– 5. Advise tepid sponge bath or cool 5. Advise tepid sponge bath or cool
water to manage prurituswater to manage pruritus

LeukemiaLeukemiaMalignant disorders of blood Malignant disorders of blood
forming cells characterized by forming cells characterized by UNCONTROLLED proliferation UNCONTROLLED proliferation of WHITE BLOOD CELLS in the of WHITE BLOOD CELLS in the bone marrow- replacing bone marrow- replacing marrow elements . The WBC marrow elements . The WBC can also proliferate in the can also proliferate in the liver, spleen and lymph nodes.liver, spleen and lymph nodes.

LeukemiaLeukemia
The leukemias are named The leukemias are named after the specific lines of after the specific lines of blood cells afffected blood cells afffected primarilyprimarily– MyeloidMyeloid– LymphoidLymphoid– MonocyticMonocytic

LeukemiaLeukemia
The leukemias are named also The leukemias are named also according to the maturation of according to the maturation of cellscells
ACUTEACUTE– The cells are primarily immatureThe cells are primarily immature
CHRONICCHRONIC– The cells are primarily mature The cells are primarily mature or diferentiatedor diferentiated

LeukemiaLeukemia
ACUTE myelocytic leukemiaACUTE myelocytic leukemiaACUTE lymphocytic leukemiaACUTE lymphocytic leukemia
CHRONIC myelocytic leukemiaCHRONIC myelocytic leukemiaCHRONIC lymphocytic leukemiaCHRONIC lymphocytic leukemia
LeukemiaLeukemia
ETIOLOGIC FACTORSETIOLOGIC FACTORS– UNKNOWMUNKNOWM– Probably exposure to Probably exposure to radiationradiation
– Chemical agentsChemical agents– Infectious agentsInfectious agents– GeneticGenetic

LeukemiaLeukemia
– PATHOPHYSIOLOGY of PATHOPHYSIOLOGY of ACUTE LeukemiaACUTE Leukemia
Uncontrolled proliferation of Uncontrolled proliferation of immature cellsimmature cells suppresses bone marrow suppresses bone marrow functionfunction severe anemia, severe anemia, thrombocytopenia and thrombocytopenia and granulocytopeniagranulocytopenia

LeukemiaLeukemia
– PATHOPHYSIOLOGY of PATHOPHYSIOLOGY of CHRONIC LeukemiaCHRONIC Leukemia
Uncontrolled proliferation of Uncontrolled proliferation of DIFFERENTIATED cellsDIFFERENTIATED cells slow suppression of bone slow suppression of bone marrow functionmarrow function milder milder symptomssymptoms

LeukemiaLeukemia
ASSESSMENT FINDINGSASSESSMENT FINDINGS ACUTE LEUKEMIAACUTE LEUKEMIA
– PallorPallor– FatigueFatigue– DyspneaDyspnea– HemorrhagesHemorrhages– OrganomegalyOrganomegaly– HeadacheHeadache– vomitingvomiting

LeukemiaLeukemia
ASSESSMENT FINDINGSASSESSMENT FINDINGS CHRONIC LEUKEMIACHRONIC LEUKEMIA
– Less severe symptomsLess severe symptoms– organomegalyorganomegaly

LeukemiaLeukemia
LABORATORY FINDINGSLABORATORY FINDINGS Peripheral WBC count varies Peripheral WBC count varies
widely widely Bone marrow aspiration biopsy Bone marrow aspiration biopsy
reveals a large percentage of reveals a large percentage of immature cells- BLASTSimmature cells- BLASTS
Erythrocytes and platelets are Erythrocytes and platelets are decreaseddecreased

LeukemiaLeukemia
Medical ManagementMedical Management
1.1. ChemotherapyChemotherapy
2.2. Bone marrow transplantationBone marrow transplantation

LeukemiaLeukemia
Nursing ManagementNursing Management 1. Manage AND prevent 1. Manage AND prevent
infectioninfection– Monitor temperatureMonitor temperature– Assess for signs of infectionAssess for signs of infection– Be alert if the neutrophil count Be alert if the neutrophil count
drops below 1,000 cells/mm3drops below 1,000 cells/mm3

LeukemiaLeukemia
Nursing ManagementNursing Management 2. Maintain skin integrity2. Maintain skin integrity
3. Provide pain relief3. Provide pain relief
4. Provide information as to 4. Provide information as to therapy- chemo and bone therapy- chemo and bone marrow transplantationmarrow transplantation




























![Cardio Nursing- Course Audit 2[1]](https://img.pdfslide.us/doc/110x75/5466384cb4af9f80038b4721/cardio-nursing-course-audit-21.jpg)
