-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
1/21
26/4/2013
(c) Simon Lam 2013 1
Keratoconus UpdatesDiagnosis and Specialty Lenses Fitting
ByMr Simon Lam
PD in Opt (HKPU),BSc in Opt (USA), MBA (Hull), DACE (WDA)
Head Optometrist, Optic Point Pte Ltd
Visiting Lecturer, Republic Polytechnic, Singapore
Keratoconus
What have we learnt from the past?
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
2/21
26/4/2013
(c) Simon Lam 2013 2
Keratoconus Characteristics
Non-inflammatory.
Central or para-central corneal thinning.
Corneal steepening or protrusion.
Increased astigmatism and possibly myopia.
Loss of best spectacle corrected visual acuity.
Corneal striae and scarring.Corneal hydrops (inflammatory).
Pathology of Keratoconus
Loss of Bowmans Layer.
Stromal Thinning.
Apoptosis.
Increased Enzyme Activity.
Enlarged Prominent Corneal Nerves.
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
3/21
26/4/2013
(c) Simon Lam 2013 3
Causes of Keratoconus
Heredity vs. Mechanical
Cellular
Tissue
Genetic
Heredity vs. Mechanical
Does eye rubbing cause Keratoconus?
2 out of 250 doctors feel that rubbing is a
cause.
KC patients do rub their eyes more often
than those without KC.
What is it that makes KC patients rub their
eyes?
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
4/21
26/4/2013
(c) Simon Lam 2013 4
Cellular Changes
Keratoconus cells are hypersensitive.
Increased enzyme activity, lack of enzyme
inhibitors.
Matrix substrate instability in response to
environmental stress factors.
mtDNA damage and exaggerated oxidativeresponse causing cellular
damage.
Tissue Changes
Loss of Bowmans layer.
Lamellar slippage.
Lack anchoring lamellar fibrils.
Apoptosis of the stroma causing anterior
thinning.
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
5/21
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
6/21
26/4/2013
(c) Simon Lam 2013 6
Progression and PrognosisAge is a big factor.
The younger the diagnosis, the poorer theprognosis.
Less likely to progress to the point of atransplant if diagnosed
in the 30s.
20% of Keratoconus patients result in corneal
transplants.35 to 45% of all transplants are due to
Keratoconus.
Possible Aggravating Factors
UV exposure.
Allergies.
Vigorous eye rubbing.
Poorly fitting contact lenses.
Inflammation.
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
7/21
26/4/2013
(c) Simon Lam 2013 7
Hallmarks of Keratoconus A decline in visual acuity (6/9 or
below).
A distorted retinoscopy reflex.
Distortion of the keratometry mire.
Frequent changes in spectacle cylinder power and
axis.
Increased myopia.
Squeezing of the eyelids to create a pinhole effect. The
appearance of halos or starbursts around light
during night-time viewing.
Associated atopic disease
Keratoconus Clinical Signs
External Signs
Munson Sign
Rizzuti PhenomenonRizzuti's sign is appreciated
when a slit lamp beam is
focused on the nasal aspect
of the limbus. When viewed
temporally, the apex of the
cone will be illuminated.
Corneal Protrusion may
cause angulations on the
lower lid when down gaze
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
8/21
26/4/2013
(c) Simon Lam 2013 8
Keratoconus Clinical Signs
Refractive Signs
Retinoscopic scissors reflex
Increased myopia
Increase in and irregularity of astigmatism
Keratoconus Clinical Signs
Keratometry signs
Lack of mire parallelism
Mire distortion
Increase in and irregularity of astigmatism
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
9/21
26/4/2013
(c) Simon Lam 2013 9
Keratoconus Clinical Signs
Slit-lamp Biomicroscopic Signs
Vogt striae
Fleischer ring
Scarring
Increased visibility of nerve fibers
Corneal thinning
Hydrops
Keratoconus Clinical Signs
Corneal Topography Signs
Compression of mires in affected region
Colour map shows power increased in
isolated area of cone
Inferior superior dioptric asymmetry
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
10/21
26/4/2013
(c) Simon Lam 2013 10
Keratoconus Clinical Signs
Optical Coherence Tomography Signs
Uneven thickness of the cornea
Increase in the Anterior Chamber Depth
Decentered apex
Types of Keratoconus
Nipple/Oval cone - central or mildly para-
central localized thinning and steepening.
Keratoglobus - Large generalized thinning
and steepening.
PMD (pellucid marginal degeneration)
peripheral thinning and steepening.
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
11/21
26/4/2013
(c) Simon Lam 2013 11
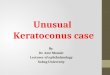
Cone Types and Prevalence
Nipple (28.7%) Oval (44.3%) Globus (6.7%)
Source: McMahon TT. Collaborative Longitudinal evaluation of
Keratoconus
Update ,AAAO meeting Dec 2006.
Nipple Cone
Central Steepening
Steepest form (Less than 5 mm in Diameter)
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
12/21
26/4/2013
(c) Simon Lam 2013 12
Oval Cone
Displace inferior Steepening
More than 5 mm in Diameter
Keratoglobus
Wider 75 to 90% of cornea (more than 5
mm in Diameter)
Not as steep.
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
13/21
26/4/2013
(c) Simon Lam 2013 13
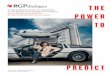
Pellucid Marginal Degeneration
Inferior Peripheral Thinning
Types of the Keratoconus- Summary
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
14/21
26/4/2013
(c) Simon Lam 2013 14
How to Treat Keratoconus Spectacles
Contacts Soft Standard
Soft Custom
RGP Standard
RGP Custom
Hybrid
Surgery Intacs
Penetrating Keratoplasty
Riboflavin/UV treatment (Cross-Linking) preventprogression of
Keratoconus
When to Intervene?
Best Spectacle/Soft CL Acuity 20/30 or
better?
Good tolerance of acuity.
Corneal health is not compromised.
If it isnt broke, dont fix it.
Best Spectacle/Soft CL Acuity worse than
20/30?
Specialized contact lenses.
My opinion, use RGP lenses.
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
15/21
26/4/2013
(c) Simon Lam 2013 15
Corneal Shape affect RGP fitting
Which RGP Design?
Early Keratoconus
Standard RGP
KC RGP
Mid-stage Keratoconus KC RGP
Custom KC RGP
Advanced Keratoconus
Custom KC RGP
Intra-limbal or Scleral RGP
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
16/21
26/4/2013
(c) Simon Lam 2013 16
Golden Rules of Fitting Corneal topography: just a starting
point.
Fluorescein patterns
No single method
A successful contact lens fit :
Allows the patient to wear the lens for many
hoursMaximizes vision
Keeps the corneal integrity intact.
Fitting Philosophies
Three point touch design: (ideal fit)
Steep fitting: (apical clearance )
Flat fitting:
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
17/21
26/4/2013
(c) Simon Lam 2013 17
Nipple/Oval Cone Fitting
Most common form of KC.
Early stages - simple RGP or KC RGP
Later stages KC RGP usually small and
steep.
The steeper the cone, the smaller the lensdiameter.
Igel EE-conus Lens
72% of patients notice an increase in acuity
with aspheric, aberration control. Lens to be centered on the
cone.
Reduce excessive movement (1 to 2mm).
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
18/21
26/4/2013
(c) Simon Lam 2013 18
Fitting Igel EE-conus Lens
Too high tighten edge lift
reduce OAD
steepen base curve
Too low increase edge liftincrease OAD
flatten base curve
Fitting Igel EE-conus Lens
Centrally fitting the
lens on a nipple
cone better insures
optimal acuity and
comfort.
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
19/21
26/4/2013
(c) Simon Lam 2013 19
Advance Keratoconus K-reading >56D
Normal KC RGP cannot improve Vision
Aware of KC lens
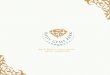
Mini-Scleral Design - MSD
Large RGP (14mm 18mm) very stable lens.
Vaults the cornea, rests on the sclera
improve comfort.
Creates a fluid filled environment. Improve VA with new
spherical surface
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
20/21
26/4/2013
(c) Simon Lam 2013 20
Mini-Scleral Design
Fitting Pearls
Tendency to tighten after initial fitting.
Light central touch will increase acuity.
Avoid central staining.
Movement is necessary but slight movement isusually
sufficient.
Pay attention to tear flow beneath lens.
The steeper the lens, the smaller OAD and lessmovement.
Dont change too many parameters at once.
-
8/12/2019 Keratoconus Update and RGP Fitting 2013 KL
21/21
26/4/2013
Thank You
Any Question?