Embed Size (px)
Citation preview

Pediatrics
Kawasaki Disease Reconsidered
New Insights and Expert Advice for a Challenging Disease
John Darby, MD
Stanford Shulman, MD
Nisha Tamaskar, MD
Brian Shirley, DO
Page 1
xxx00.#####.ppt 7/19/2016 7:33:46 AMPediatrics Pediatrics
Introductions
•Who are we? • John Darby, MD
• Texas Children’s Hospital / Baylor College of Medicine
• Hospitalist
• Nisha Tamaskar, MD
• Texas Children’s Hospital / Baylor College of Medicine
• Hospitalist Fellow
• Stanford Shulman, MD
• Lurie Children’s Hospital / Northwestern University School of Medicine
• Infectious Disease Physician
• KD Guru
• Brian Shirley, DO
• Texas Children’s Hospital / Baylor College of Medicine
• Rheumatology Fellow

Page 2
xxx00.#####.ppt 7/19/2016 7:33:46 AMPediatrics Pediatrics
Introductions
•Who are we? • John Darby, MD
• Texas Children’s Hospital / Baylor College of Medicine
• Hospitalist
• Nisha Tamaskar, MD
• Texas Children’s Hospital / Baylor College of Medicine
• Hospitalist Fellow
• Stanford Shulman, MD
• Lurie Children’s Hospital / Northwestern University School of Medicine
• Infectious Disease Physician
• KD Guru
• Brian Shirley, DO
• Texas Children’s Hospital / Baylor College of Medicine
• Rheumatology Fellow
Page 3
xxx00.#####.ppt 7/19/2016 7:33:47 AMPediatrics Pediatrics
Introductions
•Who are we? • John Darby, MD
• Texas Children’s Hospital / Baylor College of Medicine
• Hospitalist
• Nisha Tamaskar, MD
• Texas Children’s Hospital / Baylor College of Medicine
• Hospitalist Fellow
• Stanford Shulman, MD
• Lurie Children’s Hospital / Northwestern University School of Medicine
• Infectious Disease Physician
• KD Guru
• Brian Shirley, DO
• Texas Children’s Hospital / Baylor College of Medicine
• Rheumatology Fellow

Page 4
xxx00.#####.ppt 7/19/2016 7:33:47 AMPediatrics Pediatrics
Introductions
•Who are we? • John Darby, MD
• Texas Children’s Hospital / Baylor College of Medicine
• Hospitalist
• Nisha Tamaskar, MD
• Texas Children’s Hospital / Baylor College of Medicine
• Hospitalist Fellow
• Stanford Shulman, MD
• Lurie Children’s Hospital / Northwestern University School of Medicine
• Infectious Disease Physician
• KD Guru
• Brian Shirley, DO
• Texas Children’s Hospital / Baylor College of Medicine
• Rheumatology Fellow
Page 5
xxx00.#####.ppt 7/19/2016 7:33:48 AMPediatrics Pediatrics
Disclosures
•None of the presenters have any relevant financial relations to disclose
•We do not intend to discuss an unapproved/investigative use of a commercial product/device in our presentation

Page 6
xxx00.#####.ppt 7/19/2016 7:33:48 AMPediatrics Pediatrics
Introductions
•Who are you?
Page 7
xxx00.#####.ppt 7/19/2016 7:33:48 AMPediatrics Pediatrics
Objectives
•At the conclusion of this activity, participants will be able to…
•Compare Kawasaki Disease practice patterns
•Recognize features of classic and incomplete presentations of Kawasaki Disease and formulate a robust differential diagnosis
•Identify potential complications of Kawasaki Disease and prepare management plans

Page 8
xxx00.#####.ppt 7/19/2016 7:33:49 AMPediatrics Pediatrics
•Section 1 (PHM):
•Classic Presentations of KD
•Pathophysiology and Epidemiology
•Section 2 (ID):
• Incomplete Presentations of KD and KD syndromes
•Differential Diagnosis of KD
•Section 3 (Rheumatology):
•Treatment of KD
•Complications of KD
Structure of the workshop
Page 9
xxx00.#####.ppt 7/19/2016 7:33:49 AMPediatrics Pediatrics
Themes
•Recognize practice variation
•Cases and audience questions
•Polleverywhere login:
•Time for questions
•Who’s missing? Cardiology

Pediatrics
Epidemiology and Pathophysiology
Nisha Tamaskar, MD
Page 11
xxx00.#####.ppt 7/19/2016 7:33:50 AMPediatrics Pediatrics
Audience Question 1To whom are patients with KD primarily admitted in your hospital?
A) Hospital Medicine (General Medicine)
B) Infectious Disease
C) Rheumatology
D) Cardiology
E) Other

Page 12
xxx00.#####.ppt 7/19/2016 7:33:50 AMPediatrics Pediatrics
Audience Question 2Is any subspecialty/department automatically consulted when a patient is diagnosed with KD?
A) No, unless things get complicated, most patients are managed only by the general service
B) Yes, ID
C) Yes, Rheumatology
D) Yes, Cardiology
E) Yes, other
Page 13
xxx00.#####.ppt 7/19/2016 7:33:51 AMPediatrics Pediatrics
Audience Question 3In patients with classic KD with no complications, in addition to the PCP, who follows patients with KD after discharge?
A) PCP only
B) ID
C) Rheumatology
D) Cardiology
E) Multiple services

Page 14
xxx00.#####.ppt 7/19/2016 7:33:51 AMPediatrics Pediatrics
•Annual US incidence ~20 per 100,000 children <5yrs old
•80-90% of cases occur in children 6mo-5yrs old
•Peak 18-24 mo
•Rare beyond late childhood
•Older children may experience delays in diagnosis
•Boys > Girls
Epidemiology
Page 15
xxx00.#####.ppt 7/19/2016 7:33:51 AMPediatrics Pediatrics
•Japan:
•10x increased risk of KD for children with an affected sibling
•2x increased risk of KD for children with a previously affected parent
•North America: case reports of families with multiple affected members
Epidemiology

Page 16
xxx00.#####.ppt 7/19/2016 7:33:52 AMPediatrics Pediatrics
Pathophysiology
Page 17
xxx00.#####.ppt 7/19/2016 7:33:52 AMPediatrics Pediatrics
• Pathophysiology: Vasculitis Rheumatology?
•Definite immune perturbations: cytokine cascade stimulation and endothelial cell activation
•Advanced treatments are immunomodulators
Who Owns KD?

Page 18
xxx00.#####.ppt 7/19/2016 7:33:53 AMPediatrics Pediatrics
• Etiology: Infection? Infectious Disease?
•Age distribution
•Winter–spring seasonality
•Community outbreaks with wave-like geographic spread
•Laboratory features
•However…no identifiable infectious cause yet
Who Owns KD?
Page 19
xxx00.#####.ppt 7/19/2016 7:33:53 AMPediatrics Pediatrics
• Consequences: Coronary Aneurysms Cardiology?
Who Owns KD?

Pediatrics
Classic Presentations
John Darby, MD
Page 21
xxx00.#####.ppt 7/19/2016 7:33:54 AMPediatrics Pediatrics
Audience question 4
• How many patients with KD do you see a month?
A) <1
B) 1
C) 2 – 4
D) >4

Page 22
xxx00.#####.ppt 7/19/2016 7:33:54 AMPediatrics Pediatrics
Audience question 5
• Which of the following is NOT a feature associated with typical KD?
A) Erythematous, peeling groin rash
B) Refusal to bear weight
C) Erythema multiforme rash
D) Bulbar conjunctival injection
E) Posterior pharyngitis
Page 23
xxx00.#####.ppt 7/19/2016 7:33:55 AMPediatrics Pediatrics
Audience question 6
• All of the following are laboratory findings of typical KD EXCEPT:
•A) Normal peripheral white count with left shift
•B) Leukocytosis > 15K
•C) Hypernatremia
•D) CSF pleocytosis
•E) Albumin < 3.0 mg/dL
•F) Elevated serum transaminases

Page 24
xxx00.#####.ppt 7/19/2016 7:33:55 AMPediatrics Pediatrics
•Diagnostic Criteria
•Fever
•Conjunctival injection
•Rash
•Mucositis
•Extremity changes
•Lymphadenopathy
Classic Presentations
Page 25
xxx00.#####.ppt 7/19/2016 7:33:55 AMPediatrics Pediatrics
•Supporting Findings
•Cardiovascular findings
•Tachycardia, coronary artery changes, etc
•GI Complaints
•Irritability
•Anorexia
•Arthritis
Classic Presentations

Page 26
xxx00.#####.ppt 7/19/2016 7:33:56 AMPediatrics Pediatrics
• Most consistent manifestation of KD
• High spiking and with peak typically >39 C (102 F)1
•Minimally responsive to anitpyretics
•Present daily for >5 days
•Can last for 3 – 4 weeks if untreated
Fever
Page 27
xxx00.#####.ppt 7/19/2016 7:33:56 AMPediatrics Pediatrics
• Bilateral
• Typically begins shortly after onset of the fever
• Involves the bulbar conjunctivae (sparing the limbus)
• Non-exudative, painless
Conjunctival injection

Page 29
xxx00.#####.ppt 7/19/2016 7:33:57 AMPediatrics Pediatrics
•“Non-specific, diffuse maculopapular eruption.”
•Scarlatiniform rash, erythroderma, erythema-multiforme-like rash
•Rash is typically extensive
•Accentuated in the perineal region and early desquamation may occur
•(Urticarial exanthema)
•(Fine micropustular eruption)
Rash

Page 31
xxx00.#####.ppt 7/19/2016 7:33:57 AMPediatrics Pediatrics
• Strawberry tongue
• Redness and/or swelling of the lips
• Dryness, fissuring, peeling, cracking and bleeding of the lips
• Absence of oral ulcerations and pharyngeal exudates
Mucositis

Page 33
xxx00.#####.ppt 7/19/2016 7:33:58 AMPediatrics Pediatrics
• Erythema of the palms and soles
• Painful induration of the hands or feet
• Periungal desquamation of the fingers and toes
•Begins within 2 – 3 weeks after onset of fever
• Deep transverse grooves across the nails (Beau’s lines)
•1 to 2 months after onset of fever
Extremity Changes


Page 36
xxx00.#####.ppt 7/19/2016 7:33:58 AMPediatrics Pediatrics
• Least common of the clinical features
• Typically unilateral and anterior cervical triangle
• ≥1 lymph node that is >1.5 cm in diameter
• Firm and nonfluctuant
• Not associated with marked erythema of the overlying skin
• Non tender or slightly tender
Lymphadenopathy

Page 38
xxx00.#####.ppt 7/19/2016 7:33:59 AMPediatrics Pediatrics
•Leading cause of long term morbidity and mortality in KD
•Coronary arteries
•Arteritis, aneurysm, giant aneurysm
•Pericardium
•Pericardial effusion
•Myocardium
•Tachycardia, myocarditis, depressed cardiac output1, 2
•Valves
•Mitral regurgitation
Cardiac Findings
Fujiwara. Pediatrics 1978; 100-101.Yutani. Br Heart J. 1980 589-592
Page 39
xxx00.#####.ppt 7/19/2016 7:33:59 AMPediatrics Pediatrics
•Arthritis and arthralgia
•Small interphalangeal joints, large weight-bearing joints
•Gastrointestinal complaints
•Diarrhea, vomiting, and abdominal pain
•Acute acalculous distention of the gallbladder (hydrops)
•Irritability
•Rhinorrhea and Cough
Non-cardiac findings

Page 40
xxx00.#####.ppt 7/19/2016 7:33:59 AMPediatrics Pediatrics
•Leukocytosis with neutrophils and bands
•Elevated ESR and CRP (ESR ≥ 40 mm/h, CRP ≥ 3.0 mg/dL)
•Anemia for age
•Hypoalbuminemia (Albumin < 3.0 mg/dL)
•Hyponatremia
•Thrombocytosis
•Elevated serum transaminases
•Elevated GGT
•Sterile pyuria (≥ 10 WBC/high-powered field)
Laboratory Findings
Page 41
xxx00.#####.ppt 7/19/2016 7:34:00 AMPediatrics Pediatrics
Audience question 4
• All of the following are laboratory findings of typical KD EXCEPT:
•A) Normal peripheral white count with left shift
•B) Leukocytosis > 15K
•C) Hypernatremia
•D) CSF pleocytosis
•E) Albumin < 3.0 mg/dL
•F) Elevated serum transaminases

Page 42
xxx00.#####.ppt 7/19/2016 7:34:00 AMPediatrics Pediatrics
Incomplete Presentations and Additional Kawasaki
SyndromesStanford T. Shulman, M.D.
Virginia H. Rogers Professor of Pediatric Infectious Diseases

Case 3
• 8 month old male presents with 6 days of fever, bilateral non-exudative conjunctival injection and history of a fleeting macular truncal rash.• Labs: WBC 16, 73% Neutrophils, Hgb 9.8 g/dL, platelets 350K, ESR
47 mm/hr, CRP 13 mg/dL, albumin 2.8 g/dL, ALT 80
• Diagnosis? • A) Complete KD• B) Incomplete KD• C) Rubeola• D) JIA
Incomplete (Atypical) KD• Children (often infants) with fever plus fewer than four other
diagnostic criteria• Does not refer to unusual clinical features• Extremely difficult diagnostic dilemmas• Patients appear to have same laboratory profile as classic
cases• Overdiagnosis and underdiagnosis
45

Incomplete (Atypical) KD• At least 5 days of fever plus <4 classic KD features• Risk for coronary disease = classic KD• Especially seen in <1 year olds• Inflammatory markers (ESR > 40, CRP > 3.0 mg/dL) are
most useful for screening• Maintain “high index of suspicion”
46
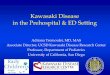
Evaluation of Suspected Incomplete Kawasaki Disease1
Newburger. Pediatrics 2004; 114:1709.

AHA Algorithm: Supplemental Criteria• Albumin 3.0 gm/dl• Anemia for age• Elevated ALT• Platelets 450,000/mm3 after day 7• WBC 15,000/mm3 • Pyuria (10 WBC/HPF)• (Hyponatremia)
48
KD Syndromes• Lymph Node predominant • Kawasaki Shock Syndrome• KD in infants <1 year of age• KD in children >8 years of age• How about adenovirus?
49


Kawasaki (“Kawashocki”) Shock Syndrome• Hypotension plus more typical KD symptoms, which may
develop during course• Older girls often affected• Compared to usual KD patients, higher CRP levels, lower
initial albumin, sodium, and platelets, more IVIG resistance, possibly higher rates of CA abnormalities
52
Dominguez: Pediatr 2008:122: e786Kanagaye: Pediatr 2009:123:e783
Schuster, Shulman
KD in infants < 1 year of age• Particularly high risk for CA abnormalities
• Boys <6 months are highest risk• Manifestations often subtle
• Often lack full diagnostic criteria (incomplete)• Standard treatment effective (IVIG, ASA)
53

Kawasaki Disease in Children >Eight Years• About 5% of all Kawasaki Disease patients• Predominance of white males• Frequently delayed diagnosis and therapy
• GI and joint manifestations common• Meningismus observed• These features serve as distractions from diagnosis
• Coronary abnormalities more common
54
Stockheim. J Ped 2000; 137:250.
Differential Diagnosis• Drug Reactions• JIA• Viral infections
55

Differential Diagnosis• Drug Reactions
• History of drug use• Much lower inflammatory markers than KD• Hives not in KD• Target lesions (E. multiforme) in KD
56
Differential Diagnosis• JIA
• Fever, Rash, Joints (±), high ESR/CRP• Often apparent in follow-up, little or transient response to IVIG/ASA
57

Differential Diagnosis• Viral infections
• Fever rarely persists > 6 days• Much lower inflammatory markers than KD
58
Case 4• 8 month old male presents with 6 days of fever, bilateral non-
exudative conjunctival injection and history of a fleeting macular truncal rash.• Labs: WBC 16, 73% Neutrophils, Hgb 9.8 g/dL, platelets 350K, ESR 47
mm/hr, CRP 13 mg/dL, albumin 2.8 g/dL, ALT 80, • Respiratory viral panel is positive for adenovirus.
• Diagnosis? • A) Acute Adenovirus infection• B) Incomplete KD• C) Rubeola• D) Typical KD
59

Differential Diagnosis•Adenovirus can mimic KD
• Exudative conjunctivitis, rash, elevated LFT• Adeno often reactivates with intercurrent febrile illnesses (+ PCR)• Less impressive ESR/CRP levels than KD
60
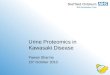
KD vs Adenovirus infection
KD – Like ADENOVIRAL infection
KD with Adenovirus detection
Tongue / Lip involvement 63% 93%
Rash 47% 93%
Hands / Feet 27% 85%
Unilateral Cervical LN 6% 40%
<4 KD Criteria 96% 15%
Adapted from Song, et al. J Peds. 2016; 170:325‐30

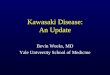
KD vs Adenovirus infectionKD – Like ADENOVIRAL infection
KD with Adenovirus detection
ESR > 40 57% 80%
CRP > 7.0 14% 50%
WBC > 15K 16% 50%
Plt > 450 (after 7 d of fever) 4% 35%
Pyuria (> 10/HPF) 2% 50%
Adenovirus Cycle Threshold 25 35
Adapted from Song, et al. J Peds. 2016; 170:325‐30
Pediatrics
Treatment and ComplicationsJoel Brian Shirley, DO

Page 64
xxx00.#####.ppt 7/19/2016 7:34:04 AMPediatrics Pediatrics
KD – Management ReviewPEDIATRICS Vol. 114 No. 6 December 2004
Page 65
xxx00.#####.ppt 7/19/2016 7:34:05 AMPediatrics Pediatrics
•Intravenous Immune Globulin (IVIG)
•2 grams/kg administered as a single infusion over 8 to 12 hours
•Administer within 10 days of fever onset (within 7 days where possible)
•Administer after 10th day if: persistent fever or aneurysms and ↑CRP and/or ESR
•Aspirin
•80 – 100 mg/kg per day divided in 4 doses
•Administer along with IVIG
•Decrease to 3 – 5 mg/kg per day at 48 – 72 hours after fever cessation
• Continue this dose for 6 – 8 weeks from illness onset in children with no coronary changes
KD – Initial Therapy

Page 66
xxx00.#####.ppt 7/19/2016 7:34:05 AMPediatrics Pediatrics
•10 month old Hispanic male with Kawasaki Disease
•Received IVIG and aspirin
•Febrile to 101.0 degrees 38 hours after completion of IVIG
Case 5
Page 67
xxx00.#####.ppt 7/19/2016 7:34:06 AMPediatrics Pediatrics
Audience Poll
Which of the following options would you choose as next course of action?
a. Retreat with IVIG alone
b. Retreat with IVIG + steroid (IV methylprednisolone, PO prednisone)
c. Administer steroid alone (IV methylprednisolone, PO prednisone)
d. Administer TNFa inhibitor alone (infliximab, etanercept)
e. Observe

Page 68
xxx00.#####.ppt 7/19/2016 7:34:06 AMPediatrics Pediatrics
KD – Initial Therapy Nonresponder
•Failure to respond generally defined as persistent or recrudescent fever ≥36 hours after completion of initial IVIG
•~15% of patients with KD initially treated with IVIG & aspirin fail to respond
•Persistent or recrudescent fever is single strongest risk factor for development of coronary artery aneurysms
Page 69
xxx00.#####.ppt 7/19/2016 7:34:06 AMPediatrics Pediatrics
KD – Initial Therapy Nonresponder
•Various retrospective studies demonstrate risk factors for nonresponsiveness to initial therapy:
• ↑ CRP (≥10mg/dL)
• ↑ AST and ALT
• ↑ % bands
• Early diagnosis (on or before day 4 suggesting more aggressive disease)
• < 1 year of age
• Sodium ≤ 133 mmol/L
• Platelet count ≤ 300,000/mm3
•Note: scoring systems have high sensitivity in Japanese population, but they have NOT been reliable predictors in multiethnic populations

Page 70
xxx00.#####.ppt 7/19/2016 7:34:07 AMPediatrics Pediatrics
KD – Initial Therapy Nonresponder
•Children who fail initial therapy for KD:
•No prospective randomized trials have evaluated optimal therapy
•Several retrospective studies indicate retreating with IVIG is effective
•Recommendation: retreat IVIG as a single infusion of 2 grams/kg for a total cumulative IVIG of 4 grams/kg
Page 71
xxx00.#####.ppt 7/19/2016 7:34:07 AMPediatrics Pediatrics
Case 6
•10 month old Hispanic male with Kawasaki Disease
•Received IVIG and high dose aspirin
•Fever and irritability persist
•Retreated with IVIG
•Fever persists, CRP rises higher
•Now What?

Page 72
xxx00.#####.ppt 7/19/2016 7:34:08 AMPediatrics Pediatrics
Audience Poll
Which of the following options would you choose?
a. Retreat with IVIG
b. Administer steroid (IV methylprednisolone, PO prednisone)
c. Administer TNFa inhibitor (infliximab, etanercept)
d. Ask for help
Page 73
xxx00.#####.ppt 7/19/2016 7:34:08 AMPediatrics Pediatrics
•10 month old Hispanic male with Kawasaki Disease
•Initial echocardiogram demonstrates early coronary artery dilatation in the LAD and RCA
•What now?
Case 7

Page 74
xxx00.#####.ppt 7/19/2016 7:34:08 AMPediatrics Pediatrics
Audience Poll
Which of the following options would you choose?
a. Administer IVIG alone
b. Administer IVIG + steroid (IV methylprednisolone, PO prednisone)
c. Administer IVIG + TNFa inhibitor (infliximab, etanercept)
d. Ask for help
Page 75
xxx00.#####.ppt 7/19/2016 7:34:09 AMPediatrics Pediatrics
Salvage Therapy
•Despite multiple doses of IVIG, about 5% of patients remain febrile
•As fever continues, coronary artery aneurysm risk increases
•Various salvage agents have been used in small studies, yet proven benefit has not been firmly established
•Disclaimer: Therapy when IVIG refractory is case dependent and there is considerable variability among institutions for which is used. The following are more common agents

Page 76
xxx00.#####.ppt 7/19/2016 7:34:09 AMPediatrics Pediatrics
Steroid Pulse Therapy
Page 77
xxx00.#####.ppt 7/19/2016 7:34:10 AMPediatrics Pediatrics
Steroid Pulse Therapy

Page 78
xxx00.#####.ppt 7/19/2016 7:34:10 AMPediatrics Pediatrics
Infliximab Therapy
Page 79
xxx00.#####.ppt 7/19/2016 7:34:11 AMPediatrics Pediatrics
Infliximab Therapy
J Rheumatol, 2012

Page 80
xxx00.#####.ppt 7/19/2016 7:34:11 AMPediatrics Pediatrics
•Anakinra in Infants and Children With Coronary Artery Abnormalities in Acute Kawasaki Disease
•Completion December 2020
•A Randomized, Double Blind, Placebo Controlled Study of the Effects of Etanercept in Children Presenting With Kawasaki Disease
•Completion July 2016
•Others: cyclosporine and plasma exchange
Clinical Trials Ongoing
Page 81
xxx00.#####.ppt 7/19/2016 7:34:12 AMPediatrics Pediatrics
•3 yo African American Female with fever for 6 days and clinical stigmata for KD
•Initial Labs:
•CRP 4 mg/dL, ESR 45 mm/hr
•WBC 16,000/mm3, Hgb 10.3 g/dL, Platelets 325,000/mm3
•Albumin 2.3mg/dL
•Received IVIG and aspirin but high fever persists ‐ retreatment with IVIG
•Fever continues…
Case 8

Page 82
xxx00.#####.ppt 7/19/2016 7:34:12 AMPediatrics Pediatrics
•Clinical status evolves:
•Prominent abdomen
•Seizure x 2
•Petechiae on palate and trunk
•Abdomain US: hepatosplenomegaly
•CBC: WBC 2.5, Hgb 7.2, Plts 20
•↑ PT/PTT/Ddimer
•↑ ferritin
•↑ AST/ALT
•↓ Fibrinogen
Case 8 continued
Page 83
xxx00.#####.ppt 7/19/2016 7:34:13 AMPediatrics Pediatrics
•Macrophage Activation Syndrome (1-2% of patients)
• Severe, potentially fatal condition caused by excessive activation of macrophages
and T cells overwhelming inflammatory reaction.
•Characterized by:
• Persistent fever
• Hepatosplenomegaly and liver disease
• Lymphadenopathy
• Severe cytopenias
• Coagulopathy consistent with DIC
• Hyperferritinemia and hypofibrinogenemia
• Hemophagocytosis in bone marrow, liver, spleen or lymph glands
KD Complications

Page 84
xxx00.#####.ppt 7/19/2016 7:34:13 AMPediatrics Pediatrics
• 9 month old AA male, presented to ED for fever of 11 days and features of Kawasaki Disease
• ECHO: LAD and RCA ectasia
•Diagnosis: Kawasaki disease
•Appropriate therapy initiated
•Persisting fever and inflammation
•LAD and RCA aneurysm (D14)
•Pulsatile nodes bilateral axilla (Day 15)…
Case 9
Page 85
xxx00.#####.ppt 7/19/2016 7:34:13 AMPediatrics Pediatrics
KD Complications
•Peripheral Artery Aneurysms•Occurs in approximately 2% of untreated patients
•Most commonly involves axillary, iliac, brachial, and mesenteric vessels
•As can be seen with coronary circulation, peripheral vessels may develop stenotic/thrombotic complication
•Distal ischemia >> gangrene in most severe cases

Page 86
xxx00.#####.ppt 7/19/2016 7:34:14 AMPediatrics Pediatrics
Questions?
Page 87
xxx00.#####.ppt 7/19/2016 7:34:14 AMPediatrics Pediatrics
• Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004; 110:2747.
• Kim T, Choi W, Woo CW, et al. Predictive risk factors for coronary artery abnormalities in Kawasaki disease. Eur J Pediatr 2007; 166:421.
• Newburger, J.W., et al., Randomized trial of pulsed corticosteroid therapy for primary treatment of Kawasaki disease. N Engl J Med, 2007. 356(7): p. 663-75.
• Sundel RP, Burns JC, Baker A, et al. Gamma globulin retreatment in Kawasaki disease. J Pediatr 1993;123:657-659.
• Burns JC, Capparelli EV, Brown JA, et al. Intravenous gamma-globulin treatment and retreatment in Kawasaki disease. Pediatr Infect Dis J 1998;17:1144-1148.
• Wright DA, Newburger JW, Baker A, Sundel RP. Treatment of immune globulin-resistant Kawasaki disease with pulsed doses of corticosteroids. J Pediatr 1996; 128:146.
• Hashino K, Ishnii M, Iemura M, et al. Re-treatment for immune globulin-resistant Kawasaki disease: a comparative study of additional immune globulin and steroid pulse therapy. Pediatr Int, 2001;43:211–217.
• Wright DA, Newburger JW, Baker A, et al. Treatment of immune globulin resistant Kawasaki disease with pulsed doses of corticosteroids. J Pediatr, 1996;128:146–149.
• Mori, M., et al., Efficacy and limitation of infliximab treatment for children with Kawasaki disease intractable to intravenous immunoglobulin therapy: report of an open-label case series. J Rheumatol, 2012. 39(4): p. 864-7.
• Son MB, Gauvreau K, Burns JC, et al. Infliximab for intravenous immunoglobulin resistance in Kawasaki disease: a retrospective study. J Pediatr, 2011;158:644–649.
• R Petty, R Laxer, C Lindsley, L Wedderburn. Textbook of Pediatric Rheumatology, 7th Ed. 2015.
References