-
KAWASAKI DISEASE
NINFA JOSON-VILLANUEVA, MD, FPPS, FPCC Pediatric
Cardiologist
-
KAWASAKI DISEASE
Definition/Epidemiology/Etiology/ Pathology Clinical Criteria
typical manifestations/clinical phases associated
findings/laboratory Atypical KD Complications Treatment Natural
History/ Follow-up
-
KAWASAKI DISEASE
Mucocutaneous Lymph Node Syndrome
an acute, self-limited, multisystem vasculitis of infancy and
childhood
Infantile Polyarteritis Nodosa
-
KAWASAKI DISEASE
1967: Dr. Tomisaku Kawasaki
-
KAWASAKI DISEASE: Epidemiology
In Japan: incidence of 184.6
cases/100,000 children/year in
-
KAWASAKI DISEASE: Epidemiology
Peak onset: 6-11 months
80% are under 4y/o
Male/female ratio:1.35:1
Recurrence rate: 3%
-
KAWASAKI DISEASE
ETIOLOGY: still UNKNOWN
clinical & epidemiological features suggest infectious
cause
Probable immunologic response triggered by several different
microbial agents
-
Kawasaki Disease: Recent Researches
identification of cytoplasmic inclusion bodies (aggregates of
viral proteins & RNA) &
virus-like particles in KD tissues
Rowley & colleagues (IKI 2008)
-
KAWASAKI DISEASE
Possible role of genetic predisposition:
1% with positive family history
50% of 2nd cases develop within 10 days of the first case
13% occurrence in twins
Genomic studies: functional single nucleotide polymorphism of
ITPKC gene that confers susceptiblity to KD (Onouchi, 2008)
-
KAWASAKI DISEASE: Pathology
Generalized systemic vasculitis involving blood vessels
throughout the body
Active inflammation--- progressive fibrosis---scar formation
In coronary arteries: arterial remodelling or
revascularization
-
KAWASAKI DISEASE: Diagnostic Criteria
FEVER for at least 5 days
AND 4 of the following:
1. Conjunctival injection
2. Changes in the oral mucosa
(mouth & lips)
3. Changes in the peripheral extremities
4. Polymorphous rash
5. Cervical lymphadenopathy
AND illness not explained by other known disease process.
-
Atypical or Incomplete Kawasaki Disease
children with KD manifested with fever & fewer than 4 of the
diagnostic clinical features
also at risk for coronary aneurysm
-
KAWASAKI DISEASE: FEVER
High spiking and remittent
Average duration=
11 days (5-23 days)
May extend to 3-4 weeks without treatment
-
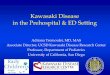
KAWASAKI DISEASE: EYE CHANGES
Bulbar conjunctivae are more affected
No exudates
No conjunctival edema
No corneal ulceration
No Pain Spares the limbus (avascular zone around the iris)
-
Eye Changes in Kawasaki Disease
-
KAWASAKI DISEASE: ORAL MUCOSA CHANGES
Appear within 1-3 days after onset of fever
a) diffuse erythema of the oropharyngeal mucosae
b) Lips: erythema, dryness, fissuring, peeling, cracking &
bleeding
-
KAWASAKI DISEASE:ORAL MUCOSA CHANGES
c) Strawberry tongue with prominent papillae
& erythema
*No oral ulcerations, pharyngeal exudates & Kopliks
spots
-
KAWASAKI DISEASE: CHANGES IN THE PERIPHERAL EXTREMITIES
Acute Phase:
a) induration (swelling) of hands & feet
(dorsal edema); sometimes painful
-
KAWASAKI DISEASE: Changes in the Peripheral Extremities
Acute phase:
b) Erythema of palms & soles; abrupt change to normal skin
at wrist & ankle (stocking & glove areas)
-
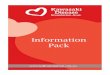
KAWASAKI DISEASE: Changes in the Peripheral Extremities
Subacute phase
(2 weeks after onset):
periungal desquamation of fingers & toes
Convalescent phase
(1 to 2 months after onset):
transverse grooves across nails (Beaus lines)
-
Desquamation of palms & fingers in the subacute phase of
KD
-
KAWASAKI DISEASE:
RASH
Polymorphous rash on trunk & extremities
most common: non-specific diffuse maculopapular erythematous
rash
No bullous & vesicular eruptions
-
KAWASAKI DISEASE: RASH
Quite common: groin erythema & desquamation
-
KAWASAKI DISEASE: CERVICAL LYMPHADENOPATHY
Least common feature (50-75%)
Usually unilateral & confined to the anterior cervical
triangle
Classic criterion:
1 lymph node
> 1.5 cm in size
Nonfluctuant, nonpurulent & nontender; no marked
erythema
-
KAWASAKI DISEASE:Other findings
Musculoskeletal Arthritis Arthralgia
Genitourinary
Urethritis meatitis
Gastrointestinal tract Diarrhea Vomiting abdominal pain hepatic
dysfunction gallbladder hydrops
Central Nervous System Extreme hyperirritability Aseptic
meningitis Sensorineural loss
-
KAWASAKI DISEASE: Cardiovascular Findings
Congestive heart failure
Myocarditis, pericarditis, valvulitis Coronary artery findings:
arteritis
Aneurysms of medium-size noncoronary arteries
Raynauds phenomenon
Peripheral gangrene
-
KAWASAKI DISEASE
Erythema and
induration on BCG site
Rare findings: Testicular swelling, pulmonary nodules and
infiltrates, pleural effusions, and hemophagocyctic syndrome
-
KAWASAKI DISEASE
Gangrene of toes
-
KAWASAKI DISEASE: CLINICAL PHASES
1. Acute Febrile Phase
(1-10 days)
2. Subacute Phase
(11-20 days)
3. Convalescent Phase
(21-60 days) 4. Chronic Phase (7 years)
-
KAWASAKI DISEASE: ACUTE PHASE
Signs & symptoms:
fever
conjunctival injection
erythema of the oral mucosa
erythema & swelling of the hands & feet
cervical lymphadenopathy
rashes
aseptic meningitis
diarrhea
hepatic dysfunction
CARDIAC
myocarditis
pericardial effusion
coronary arteritis
-
KAWASAKI DISEASE: SUBACUTE PHASE
1-2 weeks which lasts up to 4 weeks after onset of fever
resolution of fever, rash & lympadenopathy
irritability, anorexia & conjunctival injection may
persists
Prominent features: Desquamation of fingers Thrombocytosis
CARDIAC: Coronary Artery Aneurysm - highest risk for death
-
KAWASAKI DISEASE: Convalescent Phase
usually 6-8 weeks after onset of illness
when all the clinical signs have disappeared
continues until the ESR returns to normal
-
KAWASAKI DISEASE: Common Pitfalls in Diagnosis
MISTAKEN FOR:
Fever + enlarged lymph node: presumed bacterial adenitis; given
antibiotics after which developed rash & mucosal changes
Allergy
Sterile pyuria Partially-treated UTI
Fever+ rash +CSF pleocytosis Viral meningitis
Fever + abdominal pain Acute abdomen
-
KAWASAKI DISEASE: Differential Diagnosis Viral infections
(measles, adenovirus,
enterovirus, Epstein-Barr virus) Scarlet fever Staphylococcal
scalded skin syndrome Toxic shock syndrome Bacterial cervical
lymphadenitis Drug hypersensitivity reactions Steven-Johnson
syndrome Juvenile Rheumatoid Arthritis Leptospirosis Mercury
hypersensitivity reaction
(acrodynia)
-
Kawasaki Disease: Cardiac Complications
Acute phase (30%)
Myocarditis
Pericarditis
Mitral insufficiency
CHF
Subacute phase
Mitral insufficiency
Coronary aneurysm
Coronary thrombosis with infarction
Convalescent
Coronary & peripheral aneurysms may persist
Chronic
Angina pectoris &/or myocardial insufficiency may
develop
-
KAWASAKI DISEASE: Cardiac Complications
Higher risk of coronary artery lesions in patients < 6 mons
old
20-25% of untreated cases develop coronary artery
abnormalities
Mortality rate drops from 1-2% to 0.08% with IVIG
Death usually due to myocardial infarction secondary to:
a) Thrombosis of a coronary aneurysm
b) Rupture of a large coronary artery
-
KAWASAKI DISEASE: Risk Factors for developing Coronary Artery
Aneurysms
1. Male gender 2. Very young infants, particularly < 6
months
where disease is atypical 3. Older age (> 5y/o), partly
because of the
delay in recognition and treatment 4. Prolonged fever (>16
days) & fever despite
IVIG therapy 5. Recurrence of fever after an afebrile period
of at least 48 hours
Koren G, et al , J Pediatr (1986) Beiser AS, et al, Am J Cardiol
(!998) Daniels SR, et al Am J Dis Child (1987)
-
KAWASAKI DISEASE: Risk Factors for developing Coronary Artery
Aneurysms
6. Anemia 7. Thrombocytopenia early in the disease &
thrombocytosis in a later stage 8. WBC >30,000/mm2 9. ESR >
101 mm/hr and high CRP 10. Elevated ESR and CRP > 30 days or
recurrent elevation 11. Low serum albumin & adjusted IgG
levels
Koren G, et al , J Pediatr (1986) Beiser AS, et al, Am J Cardiol
(!998) Daniels SR, et al Am J Dis Child (1987)
-
KAWASAKI DISEASE: 2D-echocardiography
Structural abnormalities in the coronary arteries
Valvular abnormalities
Pericardial effusion
Dilated left coronary artery
-
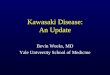
KAWASAKI DISEASE: Angiography
Left coronary angiogram (LAO):
huge aneurysm of left anterior descending artery
-
KAWASAKI DISEASE: Angiography
Multiple aneurysms in coronary arteries
-
Kawasaki Disease: Cardiac Imaging
CT scan coronary aneurysms, stenosis, intimal hypertrophy, wall
abnormalities
MRI myocardial ischemia
Multi-slice CT scan
-
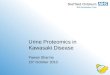
KAWASAKI DISEASE: Treatment
1. ASPIRIN Anti-inflammatory dose in acute
phase= 80-100 mg/kg/day given every 6 hours
Antiplatelet / anti-thrombotic dose: 3-5 mg/kg/day single dose
2-3 days after the fever lyzes; given for 6 weeks & continued
indefinitely if coronary abnormalities are observed
-
KAWASAKI DISEASE: Treatment
2. IV Immunoglobulin
Acute phase:
2 g/kg given single infusion for 12 hours OR
400 mg/kg/day for 4 days
leads to rapid defervescence of fever & more rapid
normalization of acute phase reactants compared to treatment with
ASA alone
improves myocardial function
-
KAWASAKI DISEASE
Mechanism of action of IVIG: UNKNOWN
With generalized anti-inflammatory effect
Possible: 1. Modulation of cytokine production
2. Neutralization of bacterial superantigens or other etiologic
agents
3. Augmentation of T-cell suppressor activity
4. Suppression of antibody synthesis
5. Provision of anti-idiotypic antibodies
Circulation, 2004; 110
-
Kawasaki Disease:Treatment
3. Heparin/ Warfarin Indicated in large coronary
aneurysms with or without thrombus
IV heparin or subcutaneous low molecular weight (LMWH)
heparin
Warfarin dose titrated to target INR of 2 2.5; should be given
with low dose aspirin
Disadvantage: interactions with Vit K rich food and many
drugs
-
Kawasaki Disease: Treatment
4. Corticosteroids- ONLY indicated for IVIG resistant
patients
(15% of patients have resistance to 1st IVIG)
Varying responses to addition of steroids to IVIG
IKI 2008:T. Suzuki et al: as prime therapy, beneficial in those
who have high risk of being IVIG non-responders
H. Suzuki et al: worse coronary outcomes
-
KAWASAKI DISEASE
TREATMENT of Patients Who Failed to Respond to Initial
Therapy:
Retreatment with IVIG 2g/kg Steroids: should be restricted
to
children in whom 2 infusions of IVIG have been given
IV Methylprednisolone: 30 mg/kg for 2-3 hours once daily for 1
to 3 days
Circulation 2004;110
-
KAWASAKI DISEASE
TREATMENT of Patients Who Failed to Respond to Initial
Therapy:
Infliximab (anti-TNF-alpha agent)- given with 2nd dose of IVIG
in IVIG resistant patients
Others: Plasma exchange
Ulinastatin
Abciximab
Monoclonal antibodies
Cytototoxic agents: cyclophosphamide
Circulation, 2004:110
-
KAWASAKI DISEASE: Treatment
4. Anti-CHF regimen when necessary
inotropes
diuretics
vasodilators
-
KAWASAKI DISEASE: Treatment Failure
persistent or recrudescent fever 36 hours after completion of
initial IVIG infusion
-
KAWASAKI DISEASE:Prevention of Thrombosis in Patients with
Coronary Disease
1. Antiplatelet therapy: Aspirin, dipyridamole, clopidogrel
2. Anticoagulant therapy: Warfarin, heparin
-
KAWASAKI DISEASE: Surgical & Catheter Coronary
Interventions
Cardiac Catheterization: Balloon angioplasty Rotational Ablation
Stent Placement Coronary artery bypass grafts for obstructive
lesions Indications for Cardiac Transplantation: Severe
myocardial dysfunction Severe ventricular arrhythmia Severe
coronary lesions
-
KAWASAKI DISEASE: Long-Term Follow-up
Spontaneous regression of aneurysms (50-70%) in 1-2 years
Factors which favor regression:
< 1 year age of onset of KD
Aneurysm: small size, fusiform morphology, location in distal
coronary segment
-
Kawasaki Disease: Long-Term Follow-up
Atherosclerosis, lipid abnormalities, late coronary artery
lesions
Need for counselling for healthy life-style (proper diet &
exercise)
B. McCrindle (IKS, 2008)
-
KAWASAKI DISEASE: Important Parameters for Follow-up
1. After baseline 2D-echo, repeat study:
2-4 weeks after onset of illness
4-6 months after illness
9-12 months after illness
OR as deemed clinically indicated
-
KAWASAKI DISEASE: Important Parameters for Follow-up
2. After baseline ESR & Platelet Count
REPEAT
2-3 weeks after onset of illness
6-8 weeks following onset
guide in discontinuation of salicylates
3. ECG as necessary
-
Summary
Kawasaki Disease is an acute multisystem
vasculitis of infancy and childhood.
The standard criteria for diagnosis
includes: fever for 5days or more plus the
presence of 4/5 of the ff: nonpurulent
conjunctivitis, oral mucosal changes,
unilateral cervical lymphadenopathy,
polymorphous rashes and swelling of
hands/feet.
-
Summary
Treatment is intravenous immunoglobulin
and aspirin.
Long-term follow-up of children with
Kawasaki Disease is advisable.
-
Thank you.