Embed Size (px)
Citation preview

Kawasaki disease:The Rheumatologist’s Perspective
By Angela Migowa, MBCHB-UON, MMed (Pediatrics and Child Health)-AKUHNPediatric Rheumatology Fellow
Montreal Children’s Hospital, McGill University

Mother Theresa of Calcutta
“……..Few of us can do bigthings; but we can dosmall things in a bigway………”

Objective
• To understand the pathophysiology ofKawasaki disease.
To correlate the pathophysiology to theclinical manifestations and managementKawasaki disease.
of•


Introduction
• Kawasaki disease (KD) is an acute, febrile, self-limiting vasculitis of unknown etiology whichleads to the formation of ectasia, dilatation, oraneurysm of the coronary arteries inapproximately 25% of untreated children.
Jamieson N et al. Int J Pediatr 2013;2013:645391.Furusho K et al. Lancet 1984;2:1055e8.
Nagashima M, et al. J Pediatr 1987;110:710e2.Terai M et al. J Pediatr 1997;131:888e93

Introduction

Historical perspective
First case….. an unusual illnesswith rash and fever in a 4-year-old child at the Red Cross Hospitalin Tokyo, Japan, in January, 1961.
“….I could make no diagnosis ofthis unusual sickness for which Icould find no reference in themedical literature….”
Kawasaki T, Kosaki F, Okawa S, Shigematsu I Yanagawa H. A newinfantile acute febrile mucocutaneous lymph node syndrome(MLNS) prevailing in Japan. Pediatrics 1974;54: 271e6.
•
•

Epidemiology
• Second commonest vasculitis of childhood after Henoch Schönleinpurpura.
The incidence in Japan is 138/100000 in children younger than 5 years,whereas in the USA, it is 17.1/100 000, and in the UK 8.1/100 000.
Approximately 85% of children with KD are younger than 5 years of age.Peak age incidence is 18–24 months.
Patients aged less than 3 months, or more than 8 years are encounteredless commonly, but are at increased risk for coronary artery aneurysms(CAA).
Eleftheriou D,Levin M, Shingadia D, et al. Arch Dis Child 2014;99:74–83.
•
•
•

JC Burns, MP Glode.Lancet 2004; 364: 533–44

EpidemiologyAuthor (Country, Year) Publication
Ikpatt N.W. et al ( Nigeria,1989) Case report
Elamin A et al (Sudan, 1993) Case series (2 patients)
Jalel C et al (Tunisia, 2000-2002) Case series (11 patients)
Badoe et al (Ghana, 2007) Case series ( 3 patients)
Rakotovao D.N. et al (Madagascar, 2008) Case series ( 5 patients)
Mabiala J.R. et al (Congo, 2015) Case series (11 patients)

Spectrum Of Musculoskeletal Inpatient DiagnosesPediatric Center In East Africa In 2011
At a
Angela Migowa1, Ines Colmegna2, Evelyne Ng'ang'a3, John Wachira4, Thomas Ngwiri5, Carol A. Hitchon6, Sasha Bernatsky7 and RosieScuccimarri8 1Pediatrics, Aga Khan University Hospital, Nairobi, Kenya, 2Rheumatology, McGill University Health Centre, Montreal, QC,Canada, 3Pediatrics, University of Nairobi, Nairobi, Kenya, 4Pediatrics, Gertrude's Children Hospital, Nairobi, Kenya, 5Pediatrics,Gertrude's Children's Hospital, Nairobi, Kenya, 6Rheumatology, University of Manitoba, Winnipeg, MB, Canada, 7Division of ClinicalEpidemiology, McGill University Health Center, Montreal, QC, Canada, 8McGill University, Montreal, QC, Canada.
• Results: The total number of admissions to Gertrude’s Hospital during 2011 was 8,011. Among those, 35patients were identified as having an ‘M-code’ diagnosis at discharge. When the records were reviewed,non-MSK conditions accounted for 20% (7 cases) of all ‘M-code’ admissions. Minor surgical proceduresmade up 14.3% (5 cases). When both of these were excluded, diseases of the MSK system and CTrepresented 0.28% of the total admissions in 2011. Validated diagnoses were classified as inflammatoryarthropathies (39.1% or 9 cases), septic arthritis (30.4% or 7 cases); soft tissue and muscle infections(17.4% or 4 cases) and Kawasaki disease (KD) (13.1 % or 3 cases).
•

Pathophysiology
• The aetiology of KD remains unknown.
• Various pathogens including retroviruses, Epstein–Barr virus,coronavirus, propionibacterium acnes, staphylococcal andstreptococcal superantigens have been implicated asinfectious triggers of KD.
Various genetic predispositions have been implicated.
Eleftheriou D et al. Arch Dis Child 2014;99:74–83
•

Eleftheriou D et al. Arch Dis Child 2014;99:74–83Downloaded from httpJ/adc.bmj.com' on June 22, 2015 - Published
by group.bmj.comReview
Table 1 Genome-wideassociation
studies inKawa~
disease(KD)
Gene
LocusPopulalion
Biologicas91ifkance
References31FCGR1A (encndes low-
affnityimmurogloilllil gammaFe region rea!ptcr II-a)
1q23
E11q,ea11Asian
The irr;olmne11 of KGRZA in !UlCeptilility ID KDhighi!t!IS the i'npo1ance oflgG l!Cl!JICl'S in lhe padogenesis of lhis inflammatorydisease and provides a bi~09cal basis for lhe w ofin~Mnous immurogbb,fo for treatm!nt.ITPKC ilC1S as a negaliw regJlillDr of T·cell activationlhrou!tt lhe C;r' /NFAT signali19 palhv.ay. and lhe Callele may mrtribiie ID immune hyper-ieaaivity il KO. 11isfirdi19 proviles nl'W insights irto lhe mechanisms ofimmune activation in KO and ef!1>hasises the i~r!CI' ofactivated T cells in the pathogenesis of this vasruillsABCC4 is a muUunai:>nal cydic nudeotide traisporter lhatstimulates the migram,y capacity of dendritic cells and amediator of prosti~andil efflux from human eels 11hb1edbynon-Slefcidal antoinflammatcry med~ations such asasprn.Variilli0f'6 in the FM1167ABLK region have beenassociated with several aU1Dinmune diseases. lUmas rheumatoid arthritis, iysternic lupuse,ylhernillDlUS. and 5151ernic sd~~ BIX encndesB~ymphoid tyrosine kinase, a S1t !amt, tyrosine bnasecbwnstream of the B·cell receplDr. Mecharism in KOpadogeresis unknotm.
CD40 l is ecpressed on the sllface of CD4 T·cells and~atelets, and engages wtlh CD«> l!Jllressed on thesllface of antigen-11esenting eels er endothelial cells.Transduees si;nals related ID eel activation ordevelopment. Elevated
l6ITPKC(inositolHilase()
1,4,5·trisphosphate
19q23
J~ese.American
JIABCC4 (ATP-linilingC, member 4)
cassett!,lUbfanly
13q32
E11q,ea11America11AuSIJilian
3'lntergenicBLK
region
betweenFAM167A ard
~22·23
J~ese
3'(1)10
20q12-q132
Tai.'lanese,Japanese
CAA. allOna<y artel)' .w>N6~ IIFAT, rude.11 faao,of
mat!d Tulk.

mina t VCAM-1 \......,-
onocyte
B
Acne
..........
....,..
JC040L.... Chemokines
1~
C040
0/CD!>pos1t1ve
~
<»
MNeutrophil
Endothelium LFA
-P-selectin
MCP-1
VEGF
Internalelasticla
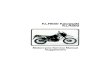
Figure 5: Proposed events in the evolutionofvasculitis
in KawasakisyndromeAn unknown inflammato,y stimulus sets in motion a cascade of events that in genetically predisposed individuals leads to inflammato,y-cell
infiltration, myointimal prolithinning of the media, and aneu,ysmal dilation of the vessel. A: Initially, activated circulating mononudear cells and platelets interact with endothelialcells that express s,intercellular adhesion molecule 1 (ICAM· 1), vascular-cell adhesion molecule 1 (VCAM·1), E-selectin, P-selectin, leading to margination of activatedmonocytes, platelets, ,endothelial cells also secrete monocyte chemoamactant protein 1 (MCP· 1), which further attracts monocyte/macrophages, and vascular endothelial-cell growth factor (\Ipenneability. B: Later, platelets adhere to thevascularwall elements. lnflammato,y cells cross the endothelium, accumulate in the intima, andliberate proinflammato,y nt(IL) 1, 6, and 8, tumour necrosis factor a (TNFa), and matrix metalloproteinases (MMPs). Neutrophils release neutrophil elastase, which damagesthe internal elastic larnu
. ..
. . ..
AVessel lumen
Macr.op.ha.ges ~~ positive T cell
~Platelet
~ Tcell.
1' C040L IL-6
.
Inti ma VLA-4 E-selectin /
I VEGF
It ,,
Media
Smooth mus.decells
lgA

Introduction

AHA Scientific Statement
Diagnosis, Treatment,and Long-Term Management<Kawasaki Disease
on RheunA Statement for Health Professionals From the CommitteeCouncil on CardiovascuFever, Endocarditsi and Kawasaki Disease,
Disease in the Young, American Heart AssociationEndorsed by the American Academy of Pediatrics
Jane W. Newburger, MD, MPH; Masato Takahashi, MD; Michael A. Gerber,MD;Michael H. Gewitz, MD; Lloyd Y. Tani, MD; Jane C. Burns, MD; Stanford T. Shulman,
MAnn F. Bolger, MD; Patricia Ferrieri, MD; Robert S.Baltimore,
MD; Walter R. Wilson,MLarry M. Baddour, MD; Matthew E. Levison, MD; Thomas J. Pallasch,
DDS;Donald A. Palace, DMD; Kathryn A. Taubert, PhD
Background-Kawasakidisease is an acute self-limited vasculitis of childhood that is characterized by fever,nonexudative conjunctivitis,Iyrnphadenopathy,Coronaryto ischemic heart diseaseor
erythema of the lips andartery aneurysms or ectasiasudden death.
oral mucosa, changes in the extremities, rash,anddevelop in .., 15% to 25% of untreated children and
Methods and Results-A multidisciplinary committee of experts was convened to revise the American Heart Asreconunendations for diagnosis, treatment, and Jong-term management of Kawasaki disease. The writinggroupa new algorithm to aid clinicians in deciding which children with fever for >5 days and <4 classiccriteriundergo echocardiography, receive intravenous gamma globulin (IVIG) treatment, or both for Kawasaki
dist ~r• .• '1' I ; ' '· • 1' • • ,.; • •• ·I

Complete Kawasaki Disease

Incomplete Kawasaki Disease

Bilateral Bulbar Conjunctival Injectionwithout Exudate

Changes in Lips and Oral Cavity(Erythema, Stawberry Tongue)

Polymorphous Exanthema

Cervical Lymphadenopathy

Peeling, Erythema, Edema of Handsand Feet

SKIN PEELINGSEEN IN HEALINGKAWASAKI
Courtesy of Dr C. Hlela

Kawasaki Shock SyndromeARTICLE
Recognition of a I<avvasaki Disease Shock SyndromeJohn T. Kan"'9aye,MO--b, Matthtow S. Wilder, MD•, O.,laram Molkara, MO--•, J.,ffrey R. Frazer,MD--<,Joan Pancheri, RN, BSN, CCRCd, Adriana H.Tremoulet. MO---, Virginia E. Watson, MD•, Brook;e M. Befl, PharmD,MAS"". Jane C. Burns, MD""'o
"Oepamnentof Pediatrics,School of Medicine,and 'Oepanment of Pharmacy,Skaggs School of Pharmacyand Pharmaa!trtica Sciences. UniVe<sityof California, San D,ego, LlJolla, Ca ifomia; Ovis,ons of •EmergencyMedicine, <Cardology,<infectious Diseases, and sAI e<gy, Immunology, and Rheumatology,and "Center for Ped.atric OinlGllResearch,Rady Children's Hospital San Diego, San Diego,California
The au1hors haw indicated they hiN'r no fnand.11 rel•ionships relevant to t1lKl artide to d~.
What's Known on This Subject What This Study Adds
We haw obs<!M!Oshockand t,ypotension wtth inc:,e.,sangftequencyin newlYaiag nosed KO.Compared With hemodynam,cally normaj KO, KOSS IS assoc•neo\\1th ~ a easedaiflamm.auon.platelet mnsumpnon, IVKiresastance. mronarv arteryabnormal rues. mn:ral regurg auon. and myocara1a1dysfuncuon.
Althoughthe c.arCl9Ccomp41Cauons of l(J) are well knOHO.hemodynarrw:: lnst-blltty ISunusual u, the acute phase of mness. excepc as a compkauon a 1ntta'W!OOUSNXiclGJTllnJstrauon.
ABSTRACT
OBJECTIVE-We sought to define the characteristics that distinguish Kawasaki diseaseshock syndrome from hernodvnamtcaltv normal Kawasaki disease.
METHODSW. e collected data prospectively for all patients with Kawasaki disease who were treatedat a sing.le institution during a 4-year period. We defined Kawasaki disease shock syndromeon the basis of systolic hypotension for age, a sustained decrease in systolic blood pressure frombaseline of ~20%, or clinical signs of poor perfusion. We compared curucal and laboratoryfeatures, coronary artery measure•
WW\v.pediatrics.org/cgi/ooi/10.1542/peds.2008-1871
doi:10.1542/peds.2008-1871
Key WordsK.iwasala d,se.ase (Jnucocu1"000US tymphrode syndrome),shock.echoca•dJOQr.lpl,y,wntncut>r funcuooAbbrevaauonsJl([)_K;r11•ag,c1 dl5Gl5e"llG lntr.lYmOUS onmunog obulnIIDSS-K.rN.1Sakl d,,.,..., shocksyn~ome
ments. and responses to therapy and analyzed indices of ventricular diastolicfunction during acute and convalescent Kawasaki disease.
systolic and
RESULTS. Of 187 consecutive patients with Kawasaki disease. 13 (7o/o) met the defini• tion forKawasaki disease shock syrrd rorne, All received fluid resuscitation, and 7 (54%) requiredvasoactive infusions. Compared with patients without shock. pa• tients with Kawasaki disease shocksyndrome were more often Iernate and had larger proportions of bands. higher C-reactive proteinconcentrations, and lower hemoglo• bin concentrations and platelet counts. Evidence of corrsurnpttvecoagulopathy was corrarrrori in the Kawasaki disease shock syndrome group. Patients withKawasaki disease shock syrrdrorne more often had impaired left ventricular systolic function (ejectionfraction or <54%: 4 of 13 pa Lien ts [31 %] vs 2 of 86 patients [4%]). mitral regurgitation (5 of 13patterns [39%] vs 2 ol 83 patterns [2%]), coronary anery abnormalities (8 of 13 patterns [62%1vs 20 of 86 patients [23%]), and Im raverious
Adc:lre» correspondcnae: to Joh, T. ~•VD, [),vi.wf1 ot lmergcncy ViedOIIC. ~yOlildren·.s Hos.piul San Diego. 3:>20ChilchrfsW.y. '-'C 50/S, San Oiegc>. CA 92123--41112.l m;,utJ~dndag.
PEDAT*3 OS5N ~l#'TCXYs; Pr-n.. (ll] l--4005,: Ohn,. l098-'l2/Sl UlP)"91IO 2009by tho ""°""'n-,.,,df'lo<Wnc>
Imrnunogtobuttn resistance (6of 13 pallents [46°/oj vs 32 of 174 patients [ 18%1). Impairment of ventricular relaxation and compliance persisted

OtherIrritabilityArthritisPneumonitisUveitis
Clinical Features••••• Gastroenteritis,
gallbladdergastrointestinal ischaemia, hydrops of
•••
Dysuria from sterile urethritis or meatitisErythema and induration at BCG vaccination siteMacrophage Activating Syndrome

Laboratory Investigations
Elevated ESR, CRPModerate to high WBC count with left shiftAnemiaThrombocytosis (usually occurs later)Mild-moderate elevation in transaminasesLow albuminLow sodiumSterile pyuria
••••••••

Differential Diagnosis

I-+I
I Red
eyes
I-+
I Extremity
changes
I-+
Cervicalcat scratch. tularaemiaBilateral -+? Epstein-Barr virus,cytomegalovirus,
.
.
.
fingers and toes toxic shocksyndrome. drug
lesions coxsackie virus, measles
Mucositis with -+ ? Stevens-Johnsonsyndrome
Mucousmembrane
rheumatoid arthritis
conjunctivitis,adenovirus.
Respiratory symptoms -+? Adenovirus, measles
acute rheumaticfiNer
orjust fever, chronic course
Ill contacts -+ ?Viral exanthem
Rash accentuated
I Fever
+-I Rash
Medications -+? Drug reaction Restingtachycardia/gallop -+ ? Kawasaki syndrome, RecentMMR .,. ? Vaccine reactionviral myocarditis,
Travel, pets -+? Measles, leptospirosis Generalised lymphadenopathy,-+ ? Juvenilerheumatoid arthritisEiythroderma -+? Toxic shock syndrome splenomegaly, arthritis,
in groin with peeling-+? Kawasaki syndrome. scarlet fever Arthritis and abdominal pain.-+ ? PolyarteritisnodosaPruritic rash -+? Scarlet fever,drug reaction,
chronic course atopic dermatitis
Uveitis -+? Kawasaki syndrome,
leptospirosis, Discrete intraoral -+ ? Herpes simplex virussarcoidosis, pauciarticular juvenile
with Koplik spots Exudative conjunctivitis -+? St!Nens-Johnsonsyndrome, bacterial
plaques +- changes enterovirus,
measles
Itchy eyes with tearing -+? Allergic conjunctivitis
Oedema and peeling -+ ? Kawasaki syndrome,scarlet fever,
reactions, enterovirus
Unilateral -+? Group A ~-hae~ic
lymphadenopathy
toxoplasmosis, Kikuchi'snecrotising lymphadenitis

Cardiac Monitoring
• All patients with KD should undergo echocardiography at diagnosis at 10-14 daysand at 6–8 weeks after the onset of the disease.
Echocardiography should be performed at least weekly in those with aneurysmsdetected on initial echocardiography (ECHO) and those with ongoing activeinflammation to monitor aneurysm size progression, or the development ofthrombus formation.
A negative echocardiogram does not exclude the diagnosis of KD.
JW Newburger et al. Circulation 2004;110:2747–71.PA Brogan PA et al. Arch Dis Child2002;86:286–90.Eleftheriou D et al. Arch Dis Child 2014;99:74–83
•
•


IV
T<ell actNation and p,o11e<o11on J.
T-Qlll ;opopl0$is t
..:::;::::;::-,..
Pro-inllammelOty cytol<ine prOdudoon J.
DC ddferen1111tlon 1 n-Exp,eulonolC01dt DC •- - -~----
?NK-ffled18llld A0CC f I
"1
E,cp,eulon ol •cliVllling FC)As J.
' lg
NK-<:e-ll Allon t
-~IUfflOUt a<:1Mly tExponslon ofSuppress,.,e luncliOn ol Trvg ce11S •
lnhlb<toty Fc,flllB t
&cell p,oflefallon !
YNeutrophil dealll - Te,gtec
Neutrophl ectillatlOn by lgG <llme.s bonding FC)As 0t by ANCA 1
lgG IVlg P'GP"tallOns • Cytotoxic granules F~ • Ant,gen
Innate Immunity Adaptlw ImmunityOC-ffl8diat..i T-eel actMulon •Endocytosls ..
AnC~lnllammllto,y cylOklno p,cduct,on t IL·2 p,cduction J.
Expression ol MHC class II and coabmulalD<ymoieaJloS J. Y T <ell c:t,lferentiauon J.
e.·.. ::.·
:·:~'-·(~
lnc:tuce Cflange$ In NK-cel tralflcldng lrom blood IO -
Cytcldne pro<luebOn 8l>d degrenulall!Cn i
Trvg cell• i
8-cel &1,op&c,$S T
Nou1reJizatJOttof 8-cell lUMVd ta<*WSBlockade ol ec!iVlltlng Fc,A
Neutrophl 8C11vetionby lgG mo,,c,,., • ~ FC)Aa J
N<lutrophl lldhesoon to endotheliumJ.
Key: Y ,n Actl\laling
lkell recepc0t$on B celS • Unrc:tentiflec:t sia-._lic .,. lnhbto,y F~receptor
TRaYD$"'• L

Treatment

Vol. 324 No. 23 SINGLE-DOSE GAMMA GLOBULIN FOR KAWASAKI SYNDROME - NEWBURGER ET AL. 1633
A SINGLE INTRAVENOUSINFUSIONS
INFUSION OF GAMMA GLOBULIN AS COMPARED WITH FOURIN THE TREATMENT OF ACUTE KAWASAKI SYNDROME
MASATO TAKAHASHI, M.D., ALEXA s. BEISER, PH.D., JANE c. BURNS,M.D.,JANE w. NEWBURGER, M.D.,JOHN BASTIAN, M.D., KYUNGJA CHUNG, M.D., STEVEND. COLAN, M.D., c. ELISEDUFFY, M.D.,
DAVID R. FuLTON, M.D., MARV P. GLODE, M.D., WILBERT H. MASON, M.D., H. CoDv MEISSNER, M.D., ANNE H. RowLEV, M.D.,STANFORD T. SHULMAN, M.D., VENUDHAR REDDY, M.D., ROBERT P. SuNDEL, M.D., JAMES W. WIGGINS,M.D., THEODORE CoLTON,
Sc.D., MARIAN E. MELISH, M.D.,AND FRED S. ROSEN, M.D.
Abstract Background. Treatment of acute Kawasaki ment and 1 .84 (95 percent confidence limits, 0.89 and3.82) seven weeks after enrollment. Children treated withthe single-infusion regimen had lower mean temperatureswhile hospitalized (day 2, P<0.001; day 3, P = 0.004), aswell as a shorter mean duration of fever (P = 0.028). Fur•thermore, in the single-infusion group the laboratory in•dexes of acute inflammation moved more rapidly towardnormal, including the adjusted serum albumin level(P = 0.004), alpha,-antitrypsin level (P = 0.007), andC-reactive protein level (P = 0.017). Lower lgG levels onday 4 were associated with a higher prevalence of coro•nary lesions {P = 0.005) and with a greater degree of sys•temic inflammatio·n. The two groups had a similar inci•dence of adverse effects (including new or worsening
syndrome with a four-day course of intravenous gammaglobulin, together with aspirin, has been demonstratedto be safe and effective in preventing coronary-artery le•sions and reducing systemic inflammation. We hypoth• esizedthat therapy with a single, very high dose of gamma globulinwould be at least as effective as the standard regimen.
Methods. We conducted a multicenter, randomized, controlledtrial involving 549 children with acute Kawasaki syndrome. Thechildren were assigned to receive gamma globulin either as a singleinfusion of 2 g per kilogram of body weight over 1 O hours or asdaily infusions of 400 mgper kilogram for four consecutive days. Both treatment
through the 14th day of illness, then 3 to 5 mg per kilogram perday).
Results. The relative prevalence of coronary abnor•malities, adjusted for age and sex, among patients treatedwith the four-day regimen, as compared with those treated withthe single-infusion regimen, was 1.94 (95 percent
groups received aspirin (100 mg per kilogram per day congestive heart failure in nine children), which occurred in 2. 7percent of the children overall. All the adverse ef• fects weretransient.
Conclusions. In children with acute Kawasaki disease,a single large dose of intravenous gamma globulin is moreeffective than the conventional regimen of four smaller daily dosesand is equally safe. (N Engl J Med 1991; 324:1633-9.)confidence limits, 1.01 and 3.71) two weeks after enroll-
KAWASAKI syndrome is an acute illness of child• prevalence of coronary-artery lesions. 7 On the basis of theseobservations, we conducted a multicenter, ran• domized trial in theUnited States. Gamma globulin administered in four consecutivedaily doses, together with aspirin, resulted in a marked reductionin the prevalence of coronary-artery abnormalities as com• paredwith aspirin alone.8 Furthermore, this treat• ment had a rapidand dramatic antiinflammatory ef• fect. Motivated by the potentialeconomic and social benefits of shortening the hospital stay forpatients with Kawasaki syndrome, we organized a second mul•ticenter, randomized trial to ascertain whether the ad• ministrationof intravenous gamma globulin in a sin• gle large dose would havesimilar or better efficacy and safety than the standard regimen offour daily doses.
hood characterized by fever, rash, conjunctivitis,inflammation of the mucous membranes, swollen ery•thematous hands and feet, and cervical adenopathy.1•2The histopathological features of vasculitis involvingarterioles, capillaries, and venules appear in the earli• est phaseof the disease." Subsequently, the walls of the coronary arteries andother medium-sized muscu• lar arteries may show evidence offocal segmental de• struction, with coronary-artery aneurysms orectasia developing in approximately 15 to 25 percent of affect• edchildren.4·6 Studies in Japan suggested that the in• travenousadministration of gamma globulin during the acute phase ofKawasaki syndrome decreased the
From 1he Departments of Cardiology and Medicine. Children's Hospital, and the Department ofPediatrics. Harvard Medical School. Boston (J.W.N., S.D.C .• R.P .S., F.S.R. ); the Department ofPediatrics, Children's Memorial Hospital and Northwestern Univen;ity School of Medicine.Chicago (C.E.D., A.H.R.,S. T. S. ); Children "s Hospital. the University of Colorado Health Sciences Center, and theUniversity of Colorado School of Medicine, Denver (M.P.G., J. W.W.); Children's Hospital ofLos Angeles and the University of Southern California School of Medicine, Los Angeles(W.H.M., M.T.); Children's Hospital, the University of California Medical Center, and theUniversity of California School of Medicine, San Diego (J.C.B., J.B., K.J.C.); Tufts-NewEngland Medical Center and Tufts University School of Medicine, Boston (D.R.F., H.C.M.);Kapiolani-Children's Medical Center and John A. Bums School of Medicine, Honolulu (M.E.M.• V.R.); and the Department of Epidemiology and Biostatis• tics. Boston University School ofPublic Heahh, Boston (A.S.B .. T.C.). Address reprint requests to Dr. Newburgcr at the Depanmentof Cardiology. Children's Hospital, 300 Longwood Ave., Boston, MA 02115.
Supponed by grants (HL 34545, RR 02172, and RR 69) from the NationalInstitutes of Health.
METHODS
Enrollment of Patients
We enrolled patients from May 1986 through November 1989 at seven centers inthe United States. We defined cases of Kawasaki syndrome according to thefollowing criteria: fever; nonexudative conjunctival injection; changes in the oralpharynx, including mucosa) erythema, dry, fissured lips, and "urre wber-r-y tongue'';changes in the extremities, characteristically erythema of the palms and soles, edemaof the hands and feet, or periungual dcsquamationin the subacutc phase of the disease; rash; and ces-vjca! adenopathy (one or morenodes at least 1.5 cm in diameter). The criteria for entry into the study requiredthat patients have fever plus four of the other five signs and have no clinical orlaboratory evidence of any other disease known to mimic Kawasaki syndrome. Wealso
IVIG dose:2 g/kggiven over10 hours

IVIGIf persistence of fever ≥ 36 h after completion of the first infusion, retreatwith IVIG (2g/kg).
•
Hemolytic anemia is a complication of IVIG (more often seen with IVIGretreatment). Therefore monitor hemoglobin.
The presumed mechanism of hemolysis is that of direct antibodymediated attack.
There is a greater risk for hemolysis in patients with non-O blood groups.
R. Berard, B. Whittemore and R. Scuccimarri. Pediatric Rheumatology 2012, 10:10DJ Gordon et al. Am J Hematol 2009, 84(11):771-772.
J. Kahwaji et al. Clin J Am Soc Nephrol 2009, 4:1993-1997.
•
•
•

Steroids

Steroids
Intravenous methylprednisone therapy seems to benefit IVIG-resistant KD2ndpatients. If persistence of fever occurs after
methylprednisolone.IVIG, consider pulse
JC Burns et al. Genes Immun 2005;6:438 e44.Miura M et al.Eur J Pediatr 2008;167:1119 e23.
Furukawa T et al. Arch Dis Child 2008;93:142 e6.
•

Aspirin

AspirinASA 80-100 mg/kg/day ÷ 4 doses until day 14 or until afebrile;then switch to 3 – 5 mg/kg/day until 6 – 8 weeks.
•
If echo at 6 – 8 weeks is normal, then can stop ASA;continue.
if not
Some centers use 3 – 5 mg/kg/day throughout.
Meta-analysis comparing anti-inflammatory doses of aspirinwith high-dose aspirin combined with IVIG found no significantdifference in the incidence of CAA between the groups.
Newburger et al. Circulation 1993;87(5):1776-80.
Scuccimarri R. Pediatr Clin North Am. 2012 Apr;59(2):425-45.Terai M, Shulman ST. J Pediatr 1997;131:888–93.
•
•
•

Aspirin
• In the convalescent phase of the condition, if aneurysms persist,antiplatelet therapy in the form of low-dose aspirin (2–5 mg/kg) should becontinued long-term until the aneurysms resolve.
Clopidogrel is an alternative antiplatelet agent that could be considered.
In the presence of giant aneurysms (>8 mm) warfarin is recommended in
addition to aspirin.
Eleftheriou D et al. Arch Dis Child 2014;99:74–83.Newburger JW et al. Circulation 2004;110:2747–71.
Sugahara Y et al. Ped Cardiol 2008;29:398–401.
•
•

Other Treatment Options
• Infliximab (monoclonaltumor necrosis factor)CyclophosphamideCyclosporine AMethotrexateAbciximab
antibody against
••••


Prognosis
• Consequential myocardial ischemia and/orinfarction have been recorded not only shortly
inafter KD, but also duringaffected children.
later adult life
MH Wu et al. Circ Cardiovasc Qual Outcomes 2012;5:566e70.JC Burns et al. J Am Coll Cardiol 1996;28:253e7.
S Kitamura . Coron Artery Dis 2002;13:437e47.

1246 THE NEW ENGLAND JOURNAL OF MEDICINE May 7, 1992
MORTALITY AMONG CHILDREN WITH KAWASAKI DISEASE IN JAPAN
Yosrxxz u NAKAMURA, M.D., H1RosH1 YANAGAWA, M.D., AND ToMJSAKu KAWASAKI, M.D.
Abstract Background and Methods. It is not certainwhether patients with Kawasaki disease have a higher deathrate than the age-matched healthy population. We thereforeundertook a study to investigate this question. Between July1982 and December 1988, 53 collaborating treatment centerscollected data on all patients who had an unequivocal newdiagnosis of Kawasaki disease; pa• tients who had recurrentdisease or whose first visit to the treatment center occurred morethan 14 days after the onset of symptoms were excluded. Patientswere followed from the time of the first visit to the treatmentcenter until December 31, 1989, or until death, whicheveroccurred first. The expected number of deaths was calculatedfrom Japanese vital-statistics data and compared with the num• berobserved.
Results. Of 4676 patients who met the eligibility crite•ria, 4608 (98.5 percent) were followed through either the end ofthe study or the date of death. Thirteen patients (1 O boys and 3girls) died during the study period. The number of deathsexpected was 7.61 (ratio of observed to expect-
ed deaths, 1. 71 ; 95 percent confidence interval, 0.91 to2.92). The ratio was 2.04 (95 percent confidence interval,0.98 to 3.76) for boys and 1.11 (95 percent confidenceinterval, 0.23 to 3.23) for girls. During the acute phase of thedisease (the first two months after onset), the ratios of observedto expected deaths were higher: 9.86 overall (95 percent confidenceinterval, 3.95 to 20.31 ), 13.33 for boys (95 percent confidenceinterval, 4.89 to 29.07), and 3.85 for girls (95 percentconfidence interval, 0.1 O to 21 .42). After the acute phase,however, both sexes had ratios of observed to expected deathsthat were lower than 1 , and the difference from the controlpopulation was not statisti• cally significant.
Conclusions. The mortality rate among boys with Ka• wasakidisease in Japan is twice that among healthy boys of the same age,and most deaths occur within two months of diagnosis. Themortality rate among girls with the dis• ease appears similar tothat among healthy girls, although the numbers are very small.(N Engl J Med 1992;326:1246-9.)
SINCE the first description of Kawasaki disease by METHODS
one of us in 196 7, 1 case reports from more than 50 Entrance Criteria
To date. t t nationwide surveys of Kawasaki disease have been conductedby the Japanese Kawasaki Disease Research Committee. All patients in whomKawasaki disease was diagnosed during a 2'1.i· year period from July 1982through December 1984 were included in the eighth survey.1~ Patientsincluded in the 9th survey were given the diagnosis during a two-yearperiod from January 1985 through December 1986,:' and those includedin the 10th survey during a rwo-vear period from January .. 1987 throughDecember1988.'
In 1990, a collaborative research group was formed to conduct a follow-upstudy of patients with Kawasaki disease. The research group includedmembers of the Japanese Kawasaki Disease Re· search Committee andpediatricians from 53 treatment centers (see the Appendix). All patients inwhom Kawasaki disease was diag· nosed who were seen at the 53 treatmentcenters were included in the 8th, 9th, and I 0th nationwide surveys andserved as the patient population for this study. We included only patientswho met the following criteria: the diagnosis of Kawasaki disease hadto be unequivocal according to diagnostic guidelines developed by thecomrnirtee.!" the disease had to be in its initial episode, and the patienthad to have presented at the treatment center less than 15 days after theonset of symptoms. Thus, patients were excluded from the study if thediagnosis was only probable, if they had recurrent disease, or if theywere first seen after the 14th day of symptoms. These limitations wereimposed to avoid bias due to the large numbers of patients with late cardiacsequelae seen at large referral hospitals.
countries have appeared. This febrile disease, thecause of which is unknown, primarily affects infants andtoddlers, in whom it causes widespread vasculitis. Cardiacsequelae, notably coronary aneurysms and carditis, occur in10 to 20 percent of patients? Duringa two-year period ( 1985 through 1986), 28 deaths fromKawasaki disease (a case fatality rate of 0.1 percent)were reported in Japan.3
Many Invesrigators'"!" have conducted long-termfollow-up studies that have focused on survival and cardiacsequelae among patients with Kawasaki dis• ease. Thesestudies, however, included only patients with cardiaclesions, and follow-up was conducted only to assess theefficacy of treatment. Although such studies yield valuableinformation about the outcomesof severely afTected patients, the results may withregard to the prognosis for the total patientswith Kawasaki disease.
be biasedgroup of
To clarify the overall prognosis, we conducted alarge multicenter study in which virtually all patients whoreceived a diagnosis of Kawasaki disease were followed,including those who did not return to the treatment center.Our goal was to determine whether patients with Kawasakidisease were more likely to die than age-matched healthychildren. Protocol
The patients were followed from the time they first came to the treatmentcenter until December 31, 1989, or the time of death, if it occurred beforethat date. The status of the patients on January 1,1990, was confirmed by review of records of patient visits co the treatmentcenter after January I, 1990; by requests for information from the patients'parents if there was no visit between January and September 1990; and bychecks of resident registration records in municipal offices when no replywas received. Deaths were con· firmed by leuers from the parents or byresidential registration
From Department of Public Health. Jichi Medical School, Tochigi, Japan (Y.N .•H.Y.), and the Kawasaki Disease Research Information Center, Tok.yo (T.K.).Address reprint requests to Dr. Nakamura at the Depanmcnt of Public Hcallh. JichiMedical School. Yakushiji 3311-1, Minamikawachi-machi, To• chigi-ken, 329-04Japan.
Conducted as a research project by 1hc Japanese Kawasaki Disease ResearchCommiuee, of which Dr. Kawasaki is the chairperson. and supported by 1heMinistry of Heahh and Welfare of the Japanese Government.
Treatment centers participating in this study arc listed in the Appendix.

Long Term Follow UpMI caused by thrombosis occlusion of abnormal coronary artery isprinciple cause of death.
•
Usually occurs within first year.
Small solitary aneurysms require long term aspirin therapy.
Giant aneurysms or multiple complex aneurysms require longterm anti-platelet therapy and anticoagulation.
Primary surgical management is coronary artery bypass graft.•
•
•
•

Miriam Makeba
“Age is…wisdom, if onehas lived one's lifeproperly.”

SummaryKawasaki disease (KD) is an acute, febrile, self-limitingvasculitis that leads to aneurysms of the coronaries inapproximately 25% of untreated children.
•
Early recognition and treatment is imperative to decreaseof coronary aneurysms.
risk
IVIG and aspirin form the cornerstone of treatment in KD.
Cardiac monitoring is keycoronary aneurysms.
in detection and management of•
•
•

Asante
Thanks to our patients who inspire us toimprove and be better healthcare providers.Thanks to all my mentors and teachers in myprofessional journey.Thanks to Dr. R. Scuccimarri for her guidanceand support in preparation for the scientifictalks and lectures.Thanks to Dr. C Hlela for providing pictures inthis presentation.
•
•
•
•

Asante! Thank you! Merci!




![Kawasaki Robot K series · Kawasaki Robot K series] ... Kawasaki Robotics (USA), Inc. Kawasaki Robot Corporate Headquarters for Americas ... Japan & Asia ] 3 Combination of](https://img.pdfslide.us/doc/110x75/5b52f2687f8b9a056a8df79c/kawasaki-robot-k-series-kawasaki-robot-k-series-kawasaki-robotics-usa.jpg)