Embed Size (px)
Citation preview
Pathophysiology andCurrent Management ofBurn Injury
Leslie DeSanti, BS, RN & Burn Research Nurse & Burn Center & Brigham and Women_s Hospital & Boston, MA
The author has disclosed that she has no significant relationships or financial interests in any commercial companies that pertain to this education activity.
Wolters Kluwer Health has identified and resolved all faculty conflicts of interest regarding this educational activity.
PURPOSE
To provide the physician and registered professional nurse with an overview of the pathophysiology and current
management of burn injuries.
TARGET AUDIENCE
This continuing education activity is intended for physicians and nurses with an interest in learning about
evidence-based prevention and management of burn wounds.
OBJECTIVES
After reading the article and taking the test, the participant should be able to:
1. Explain the pathophysiology of skin function.
2. Describe the different types of burn injuries.
3. Identify the treatment strategies for burn injuries.
ADV SKIN WOUND CARE 2005;18:323-32; quiz 333-4.
Tremendous advances have been made in the manage-
ment of burn injury in the past decade. Mortality and
morbidity have been markedly reduced due to overall
major improvements in critical care, metabolic support, infec-
tion control, and wound management.1-8
As with any wound, many systemic factors impact burn
wound healing, including metabolic response to injury, nutri-
tional status, presence of systemic infection, and other systemic
insults such as pain and stress. Fortunately, the advances in
burn wound care have focused on addressing these factors.
Aggressive surgical management of deep burns, improvement
of the wound healing environment with use of silver release
dressings, better pain control in partial-thickness burns, im-
proved healing of partial-thickness burns with temporary skin
substitutes, improved functional and cosmetic outcomes of
massive burns with use of adjuvant therapies, and optimum
C M ECATEGORY 1
1 Credit
ceceANCC/AACN
3.5 Contact Hours
JULY/AUGUST 2005
extraC L I N I C A L M A N A G E M E N T
ADVANCES IN SKIN & WOUND CARE & JULY/AUGUST 2005323WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
management of major burns in burn centers are among the
advances in burn care.1-8
A burn is defined as damage to the skin caused by excessive
heat or caustic chemicals. The most common burn injuries
result from exposure to heat and chemicals. Full-thickness
burns usually develop, causing immediate cell death andmatrix
destruction, with the most severe damage on the wound
surface.8 -10 Additional heat and inflammation induce tissue
injury beneath the nonviable surface, which can either progress
over time to healing or can deteriorate to further necrosis,
depending on the approach to treatment.
Managing a burn wound is challenging because treatment
must be continuously adapted to the changing wound biology,
dictated by the burn injury process, the host_s response to
injury, and the wound environment.6-8 Flexibility in adapting
care to the changing wound is essential.
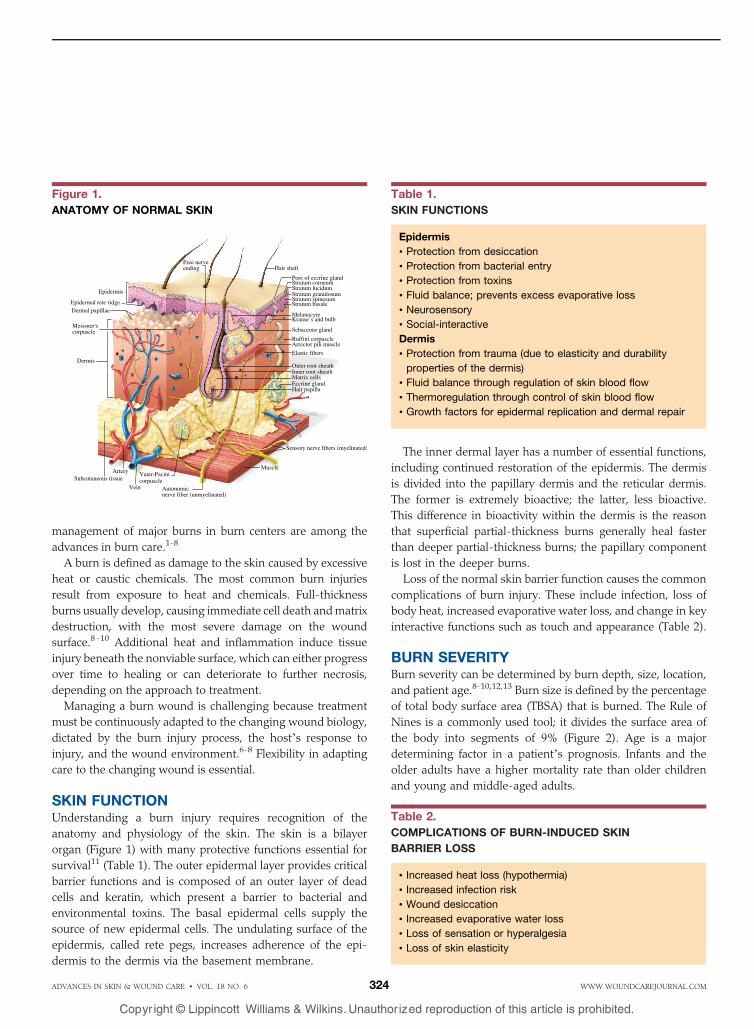
SKIN FUNCTIONUnderstanding a burn injury requires recognition of the
anatomy and physiology of the skin. The skin is a bilayer
organ (Figure 1) with many protective functions essential for
survival11 (Table 1). The outer epidermal layer provides critical
barrier functions and is composed of an outer layer of dead
cells and keratin, which present a barrier to bacterial and
environmental toxins. The basal epidermal cells supply the
source of new epidermal cells. The undulating surface of the
epidermis, called rete pegs, increases adherence of the epi-
dermis to the dermis via the basement membrane.
The inner dermal layer has a number of essential functions,
including continued restoration of the epidermis. The dermis
is divided into the papillary dermis and the reticular dermis.
The former is extremely bioactive; the latter, less bioactive.
This difference in bioactivity within the dermis is the reason
that superficial partial-thickness burns generally heal faster
than deeper partial-thickness burns; the papillary component
is lost in the deeper burns.
Loss of the normal skin barrier function causes the common
complications of burn injury. These include infection, loss of
body heat, increased evaporative water loss, and change in key
interactive functions such as touch and appearance (Table 2).
BURN SEVERITYBurn severity can be determined by burn depth, size, location,
and patient age.8-10,12,13 Burn size is defined by the percentage
of total body surface area (TBSA) that is burned. The Rule of
Nines is a commonly used tool; it divides the surface area of
the body into segments of 9% (Figure 2). Age is a major
determining factor in a patient_s prognosis. Infants and the
older adults have a higher mortality rate than older children
and young and middle-aged adults.
Table 1.
SKIN FUNCTIONS
Epidermis
& Protection from desiccation
& Protection from bacterial entry
& Protection from toxins
& Fluid balance; prevents excess evaporative loss
& Neurosensory
& Social-interactive
Dermis
& Protection from trauma (due to elasticity and durability
properties of the dermis)
& Fluid balance through regulation of skin blood flow
& Thermoregulation through control of skin blood flow
& Growth factors for epidermal replication and dermal repair
Figure 1.
ANATOMY OF NORMAL SKIN
Table 2.
COMPLICATIONS OF BURN-INDUCED SKIN
BARRIER LOSS
& Increased heat loss (hypothermia)
& Increased infection risk
& Wound desiccation
& Increased evaporative water loss
& Loss of sensation or hyperalgesia
& Loss of skin elasticity
ADVANCES IN SKIN & WOUND CARE & VOL. 18 NO. 6 324 WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
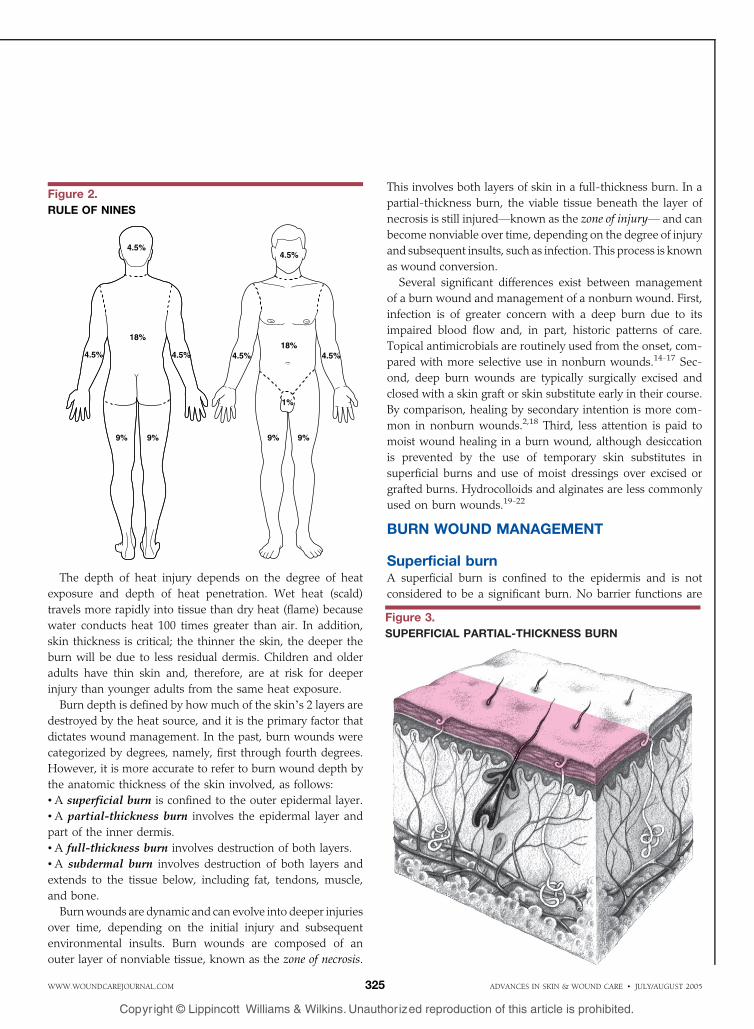
The depth of heat injury depends on the degree of heat
exposure and depth of heat penetration. Wet heat (scald)
travels more rapidly into tissue than dry heat (flame) because
water conducts heat 100 times greater than air. In addition,
skin thickness is critical; the thinner the skin, the deeper the
burn will be due to less residual dermis. Children and older
adults have thin skin and, therefore, are at risk for deeper
injury than younger adults from the same heat exposure.
Burn depth is defined by how much of the skin_s 2 layers are
destroyed by the heat source, and it is the primary factor that
dictates wound management. In the past, burn wounds were
categorized by degrees, namely, first through fourth degrees.
However, it is more accurate to refer to burn wound depth by
the anatomic thickness of the skin involved, as follows:
& A superficial burn is confined to the outer epidermal layer.
& A partial-thickness burn involves the epidermal layer and
part of the inner dermis.
& A full-thickness burn involves destruction of both layers.
& A subdermal burn involves destruction of both layers and
extends to the tissue below, including fat, tendons, muscle,
and bone.
Burnwounds are dynamic and can evolve into deeper injuries
over time, depending on the initial injury and subsequent
environmental insults. Burn wounds are composed of an
outer layer of nonviable tissue, known as the zone of necrosis.
This involves both layers of skin in a full-thickness burn. In a
partial-thickness burn, the viable tissue beneath the layer of
necrosis is still injuredVknown as the zone of injuryV and can
become nonviable over time, depending on the degree of injury
and subsequent insults, such as infection. This process is known
as wound conversion.
Several significant differences exist between management
of a burn wound and management of a nonburn wound. First,
infection is of greater concern with a deep burn due to its
impaired blood flow and, in part, historic patterns of care.
Topical antimicrobials are routinely used from the onset, com-
pared with more selective use in nonburn wounds.14-17 Sec-
ond, deep burn wounds are typically surgically excised and
closed with a skin graft or skin substitute early in their course.
By comparison, healing by secondary intention is more com-
mon in nonburn wounds.2,18 Third, less attention is paid to
moist wound healing in a burn wound, although desiccation
is prevented by the use of temporary skin substitutes in
superficial burns and use of moist dressings over excised or
grafted burns. Hydrocolloids and alginates are less commonly
used on burn wounds.19-22
BURN WOUND MANAGEMENT
Superficial burnA superficial burn is confined to the epidermis and is not
considered to be a significant burn. No barrier functions are
Figure 2.
RULE OF NINES
Figure 3.
SUPERFICIAL PARTIAL-THICKNESS BURN
ADVANCES IN SKIN & WOUND CARE & JULY/AUGUST 2005325WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
altered. The most common form of superficial burn is caused
by ultraviolet radiation from the sun (sunburn). It generally
heals by itself in less than a week without scarring. Skin
moisturizers can be used to treat a superficial burn.
Partial-thickness burnA partial-thickness burn involves the destruction of the
epidermal layer and portions of the dermis; it does not extend
through both layers. There are 2 depths of partial-thickness
burnsVsuperficial partial-thickness and deep partial-thick-
nessVand each corresponds with a predictable healing time,
treatment modality, and outcome.
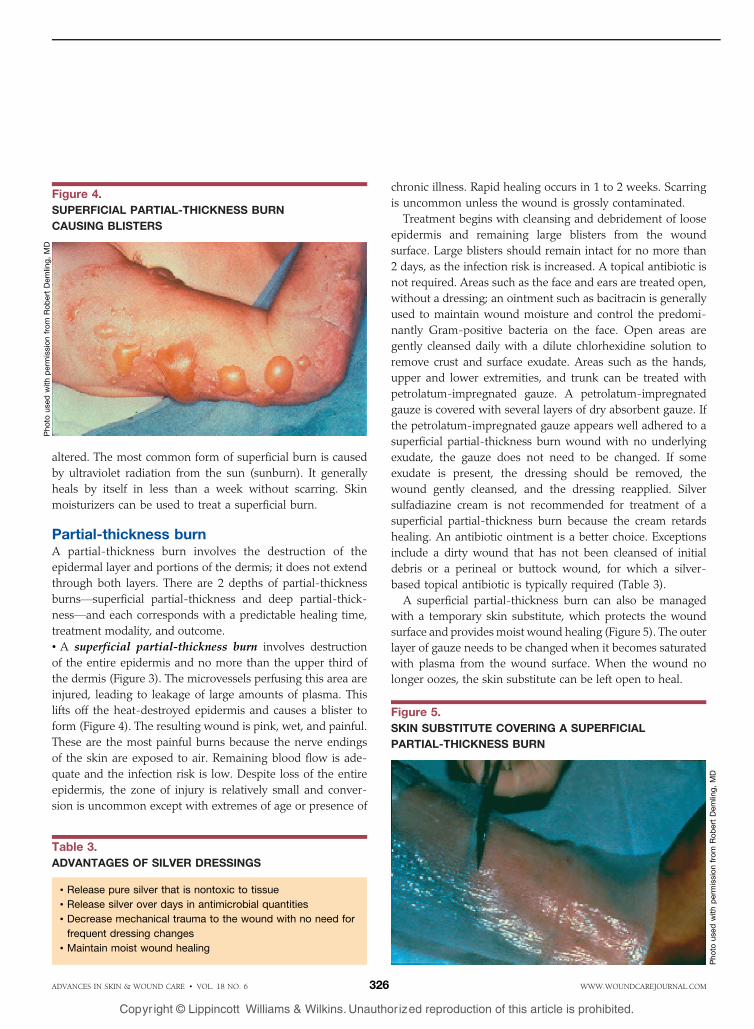
& A superficial partial-thickness burn involves destruction
of the entire epidermis and no more than the upper third of
the dermis (Figure 3). The microvessels perfusing this area are
injured, leading to leakage of large amounts of plasma. This
lifts off the heat-destroyed epidermis and causes a blister to
form (Figure 4). The resulting wound is pink, wet, and painful.
These are the most painful burns because the nerve endings
of the skin are exposed to air. Remaining blood flow is ade-
quate and the infection risk is low. Despite loss of the entire
epidermis, the zone of injury is relatively small and conver-
sion is uncommon except with extremes of age or presence of
chronic illness. Rapid healing occurs in 1 to 2 weeks. Scarring
is uncommon unless the wound is grossly contaminated.
Treatment begins with cleansing and debridement of loose
epidermis and remaining large blisters from the wound
surface. Large blisters should remain intact for no more than
2 days, as the infection risk is increased. A topical antibiotic is
not required. Areas such as the face and ears are treated open,
without a dressing; an ointment such as bacitracin is generally
used to maintain wound moisture and control the predomi-
nantly Gram-positive bacteria on the face. Open areas are
gently cleansed daily with a dilute chlorhexidine solution to
remove crust and surface exudate. Areas such as the hands,
upper and lower extremities, and trunk can be treated with
petrolatum-impregnated gauze. A petrolatum-impregnated
gauze is covered with several layers of dry absorbent gauze. If
the petrolatum-impregnated gauze appears well adhered to a
superficial partial-thickness burn wound with no underlying
exudate, the gauze does not need to be changed. If some
exudate is present, the dressing should be removed, the
wound gently cleansed, and the dressing reapplied. Silver
sulfadiazine cream is not recommended for treatment of a
superficial partial-thickness burn because the cream retards
healing. An antibiotic ointment is a better choice. Exceptions
include a dirty wound that has not been cleansed of initial
debris or a perineal or buttock wound, for which a silver-
based topical antibiotic is typically required (Table 3).
A superficial partial-thickness burn can also be managed
with a temporary skin substitute, which protects the wound
surface and provides moist wound healing (Figure 5). The outer
layer of gauze needs to be changed when it becomes saturated
with plasma from the wound surface. When the wound no
longer oozes, the skin substitute can be left open to heal.
Figure 4.
SUPERFICIAL PARTIAL-THICKNESS BURN
CAUSING BLISTERS
Photo
usedwithperm
issionfrom
RobertDemling,MD
Table 3.
ADVANTAGES OF SILVER DRESSINGS
& Release pure silver that is nontoxic to tissue
& Release silver over days in antimicrobial quantities
& Decrease mechanical trauma to the wound with no need for
frequent dressing changes
& Maintain moist wound healing
Figure 5.
SKIN SUBSTITUTE COVERING A SUPERFICIAL
PARTIAL-THICKNESS BURN
Photo
usedwithperm
issionfrom
RobertDemling,MD
ADVANCES IN SKIN & WOUND CARE & VOL. 18 NO. 6 326 WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
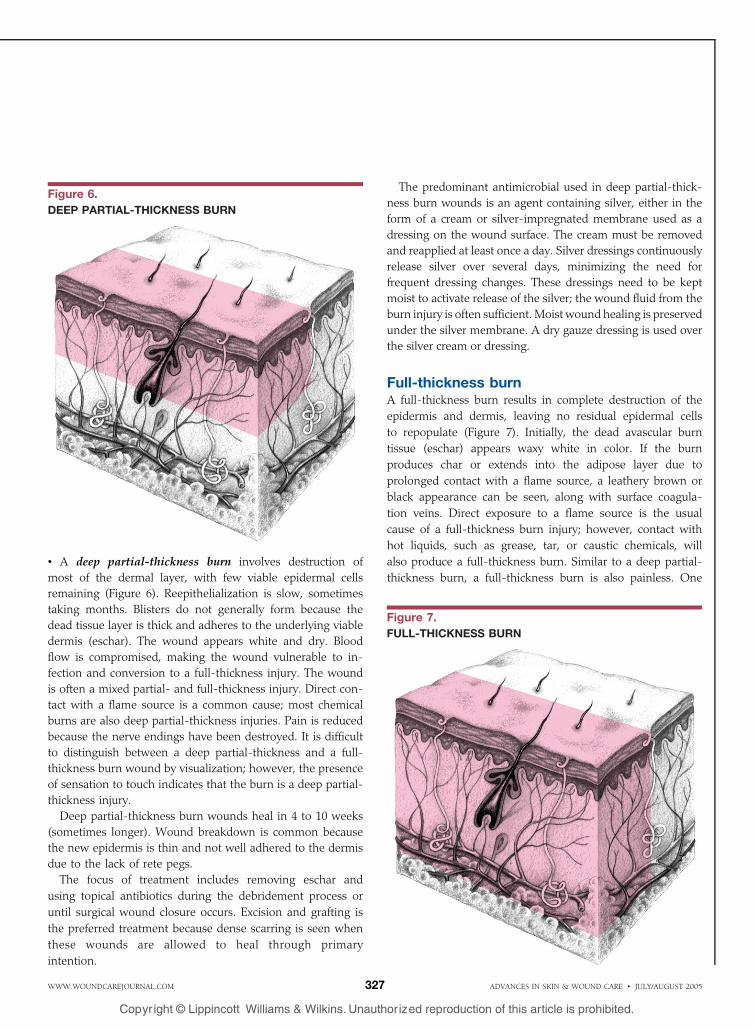
& A deep partial-thickness burn involves destruction of
most of the dermal layer, with few viable epidermal cells
remaining (Figure 6). Reepithelialization is slow, sometimes
taking months. Blisters do not generally form because the
dead tissue layer is thick and adheres to the underlying viable
dermis (eschar). The wound appears white and dry. Blood
flow is compromised, making the wound vulnerable to in-
fection and conversion to a full-thickness injury. The wound
is often a mixed partial- and full-thickness injury. Direct con-
tact with a flame source is a common cause; most chemical
burns are also deep partial-thickness injuries. Pain is reduced
because the nerve endings have been destroyed. It is difficult
to distinguish between a deep partial-thickness and a full-
thickness burn wound by visualization; however, the presence
of sensation to touch indicates that the burn is a deep partial-
thickness injury.
Deep partial-thickness burn wounds heal in 4 to 10 weeks
(sometimes longer). Wound breakdown is common because
the new epidermis is thin and not well adhered to the dermis
due to the lack of rete pegs.
The focus of treatment includes removing eschar and
using topical antibiotics during the debridement process or
until surgical wound closure occurs. Excision and grafting is
the preferred treatment because dense scarring is seen when
these wounds are allowed to heal through primary
intention.
The predominant antimicrobial used in deep partial-thick-
ness burn wounds is an agent containing silver, either in the
form of a cream or silver-impregnated membrane used as a
dressing on the wound surface. The cream must be removed
and reapplied at least once a day. Silver dressings continuously
release silver over several days, minimizing the need for
frequent dressing changes. These dressings need to be kept
moist to activate release of the silver; the wound fluid from the
burn injury is often sufficient. Moist wound healing is preserved
under the silver membrane. A dry gauze dressing is used over
the silver cream or dressing.
Full-thickness burnA full-thickness burn results in complete destruction of the
epidermis and dermis, leaving no residual epidermal cells
to repopulate (Figure 7). Initially, the dead avascular burn
tissue (eschar) appears waxy white in color. If the burn
produces char or extends into the adipose layer due to
prolonged contact with a flame source, a leathery brown or
black appearance can be seen, along with surface coagula-
tion veins. Direct exposure to a flame source is the usual
cause of a full-thickness burn injury; however, contact with
hot liquids, such as grease, tar, or caustic chemicals, will
also produce a full-thickness burn. Similar to a deep partial-
thickness burn, a full-thickness burn is also painless. One
Figure 6.
DEEP PARTIAL-THICKNESS BURN
Figure 7.
FULL-THICKNESS BURN
ADVANCES IN SKIN & WOUND CARE & JULY/AUGUST 2005327WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
major difficulty is distinguishing a deep partial-thickness
burn from a full-thickness burn; however, treatment is sim-
ilar for both.
Treatment of a full-thickness burn wound includes early
surgical debridement and wound closure with a skin graft or
permanent skin substitute. Before the planned surgery, the
wound is treated with a silver-based antibiotic cream or
dressing, using a closed dressing technique.
Subdermal burnA subdermal burn entails complete destruction of the epi-
dermis and dermis, with extension into underlying tissue, such
as connective tissue, muscle, and bone. The wound appears
charred, dry, and brown or white without sensation; typi-
cally,the affected digit or extremity has limited or no move-
ment. Treatment often requires amputation of the involved
area.
BURNS REQUIRING SPECIAL CAREBurns to the face, eyes, ears, hands, feet, and perineum have a
greater risk of complications and potential functional and
cosmetic disabilities. These burns should be managed in a
burn care facility.23,24
FaceBurns to the face are at high risk for cosmetic and functional
disability. For superficial burns, gentle and frequent cleansing
to remove all devitalized tissue is followed by application of an
antibiotic ointment such as bacitracin 2 to 3 times a day to pre-
vent desiccation and control residual Gram-positive organisms.
The face is treated open. Temporary skin substitutes can be
useful because they help protect the wound and eliminate
pain.25
Deeper facial burns require a more aggressive approach to
help prevent infection, including the use of silver products and
frequent debridement of loose necrotic tissue. Surgical
management is typically needed.
EarsSuperficial ear burns are managed similarly to facial burn
injuries; however, external pressure should not be applied to
the injured helix. The cartilage in this area is already poorly
vascularized and any compressionwill potentiate further injury.
Pressure control includes removing pillows or pressure while
sleeping. Deeper burns need more potent topical therapy,
usually with a silver or mafenide cream. Chondritis, or cartilage
infection, is a major complication and leads to loss of cartilage
and permanent deformity. Systemic antibiotics are required.
Hands and feetBurns to the hands and feet can cause functional disability.
Superficial burns are managed with a petrolatum-impreg-
nated gauze or skin substitute. Skin substitutes help provide
wound protection and pain control, especially in wounds on
the feet. Deeper burns require therapy with silver-based
products. When the hands and feet are injured, each digit
should be individually wrapped to minimize functional
disability, such as web space contractures, and to allow for
continued movement and aggressive physical therapy.
PerineumA perineal burn is at high risk for developing infection and
requires thorough cleansing and reapplication of topical
agents after urination or defecation.
Major burnsMajor burns can lead to significant morbidity or mortality;
treating them requires expertise in burn care. They are defined
as follows:
& partial-thickness burns greater than 10% of TBSA
& burns that involve the face, hands, feet, genitalia, perineum,
or major joints
& full-thickness burns in any age group, over 1% of body
surface
& electrical burns, including lightning injury
& chemical burns
& inhalation injury
& a child with any of the above burn injuries
& burn injury in patients with preexisting medical disorders
that could complicate management
& any burned child, if the hospital initially receiving the patient
does not have qualified personnel or equipment for children.
Patients with major burns are usually admitted to the
hospital and should be treated in a burn center.23,24
BURN WOUND INFECTIONMost burns are at risk for infection. Burn wound infection is
defined as bacterial invasion into viable tissue beneath the
burn eschar.16,17,26,27 Because all burns are colonized with
bacteria, a positive swab culture does not mean infection is
Table 4.
LOCAL SIGNS OF BURN WOUND INFECTION
& Black or brown focal areas of discoloration
& Enhanced sloughing of burned tissue
& Partial-thickness wound converting to full-thickness wound
& Increasing edema around the wound edges
& Softening of focal subeschar
ADVANCES IN SKIN & WOUND CARE & VOL. 18 NO. 6 328 WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
present. Infection is diagnosed by quantitative culturing of a
small full-thickness biopsy of the burn wound, including some
viable tissue. A bacterial count exceeding 105 organisms per
gram of tissue indicates infection because this amount of
bacteria typically overwhelms local immune defenses. Infec-
tion can also be diagnosed clinically, although this method is
less reliable.
Table 4 describes some of the local signs of burn wound
infection. Although systemic signs of increased fever and other
signs of sepsis provide valuable information when evaluating
for infection, fever and elevated white count are commonly
seen in burn patients without infection because of the
inflammatory response to burn tissue.
Systemic antibiotics plus topical antibiotics specific to the
cultured organisms are used to treat burn wound infection.
Eschar is also debrided to help remove the source of infection
while providing better access to the remaining infected viable
tissue for topical antibiotics. The topical antibiotic mafenide
(Sulfamylon) is often used either as a solution or cream to
treat burn wound infections because it has better tissue
penetration than available silver products. Silver-based agents
can be used after debridement has removed most of the in-
fected tissue.
ADVANCED PRODUCTS FOR BURN CARE
Silver-release productsSilver has been used for centuries to prevent and treat a variety
of diseases, most notably infections. Silver has extremely potent
antimicrobial properties, with levels in solutions exceeding 10
parts per million. Silver ions appear to kill microorganisms
instantly by blocking their respiratory enzyme system (energy
production) and altering microbe deoxyribonucleic acid (DNA)
and the cell wall; they have no toxic effect on human cells in
vivo. However, the available delivery systemsVoften in the
form of a saltVhave been limiting factors to successful biologic
use of this noble metal in burn wound care.
Silver nitrate and silver sulfadiazine have been used to
deliver antimicrobial silver for the past 40 years. However,
they impair fibroblast and epithelial proliferation, which
impairs healing.28-30
Silver itself is considered to be nontoxic to human cells
in vivo. The only reported complication is the cosmetic
abnormality argyria, which is caused by precipitation of silver
salts in the skin and results in a bluish gray discoloration.
Clinical evaluations have found no tissue toxicity. The major
complications attributed to silver compounds are due to the
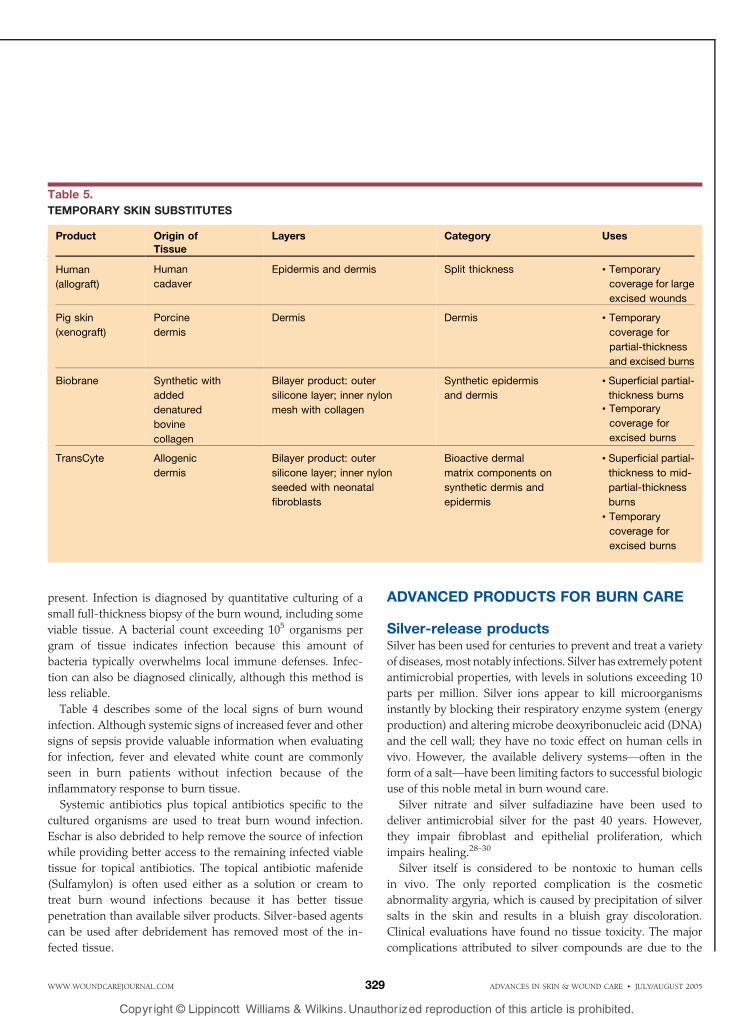
Table 5.
TEMPORARY SKIN SUBSTITUTES
Product Origin ofTissue
Layers Category Uses
Human
(allograft)
Human
cadaver
Epidermis and dermis Split thickness & Temporary
coverage for large
excised wounds
Pig skin
(xenograft)
Porcine
dermis
Dermis Dermis & Temporary
coverage for
partial-thickness
and excised burns
Biobrane Synthetic with
added
denatured
bovine
collagen
Bilayer product: outer
silicone layer; inner nylon
mesh with collagen
Synthetic epidermis
and dermis
& Superficial partial-
thickness burns
& Temporary
coverage for
excised burns
TransCyte Allogenic
dermis
Bilayer product: outer
silicone layer; inner nylon
seeded with neonatal
fibroblasts
Bioactive dermal
matrix components on
synthetic dermis and
epidermis
& Superficial partial-
thickness to mid-
partial-thickness
burns
& Temporary
coverage for
excised burns
ADVANCES IN SKIN & WOUND CARE & JULY/AUGUST 2005329WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
complex, or anionVnamely, nitrate and sulfadiazineVand not
the silver itself.
Pure silver present in current silver dressings has been shown
not only to have potent antimicrobial activity, but also to lack
toxicity to wound cells. Some data also indicate prohealing and
anti-inflammatory properties of pure silver, including blocking
excess matrix metalloproteinase (MMP) activity.31-34
Current silver dressings release pure silver ions in anti-
microbial concentrations from a membrane surface over a
period of days. Sustained release of silver is important in
reducing bacterial burden. Silver nitratemust be applied every 2
hours to be effective, and the cream base in silver sulfadiazine
reacts with serous exudate to form a pseudo-eschar that must
be removed before the cream can be reapplied. Current silver
dressings can be left in place for up to 7 days. The wound does
not have to bemanipulated during this period, which decreases
trauma to new epithelial growth and reduces the wound_s
bacterial burden. A thin moisture layer beneath the silver
dressing also maintains a moist healing environment. The
available hyperosmolar creams, which have a short period of
silver activity, can also cause surface desiccation.
Skin substitutesMajor advances in patient care have resulted in a marked
decrease in morbidity and mortality, especially with massive
burns. In addition to survival, the current focus of burn wound
care is on improving long-term function and appearance of
the healed or replaced skin cover and the quality of life.35-50
The issue of quality of life has generated a significant interest
in the use of skin substitutes to improve wound healing,
control pain, create more rapid closure, improve functional
and cosmetic outcome, and, in the case of massive burns, in-
crease survival.
To more effectively address these issues, the new genera-
tion of skin substitutes is typically biologically active. The
bioactivity can modulate the burn wound instead of only
providing coverage. The new products have not displaced the
more inert standard burn wound dressings. Instead, they are
used in conjunction with these products and have specific
indications. Skin substitutes can be classified as temporary
wound coverings used to decrease pain and augment healing
or permanent skin substitutes used to add or replace the
remaining skin components.
& Temporary skin substitutes are used to help heal partial-
thickness burns or donor sites and close clean excised wounds
until skin is available for grafting (Table 5). There are typically
no living cells present in temporary skin substitutes.
Temporary skin substitutes typically feature a bilayer
structure consisting of an outer epidermal analog and a more
biologically active inner dermal analog. The purpose of a
temporary skin substitute is twofold. The first objective is to
close the wound, thereby protecting it from environmental
insults. The second objective is to provide an optimal wound
healing environment by adding dermal factors that activate
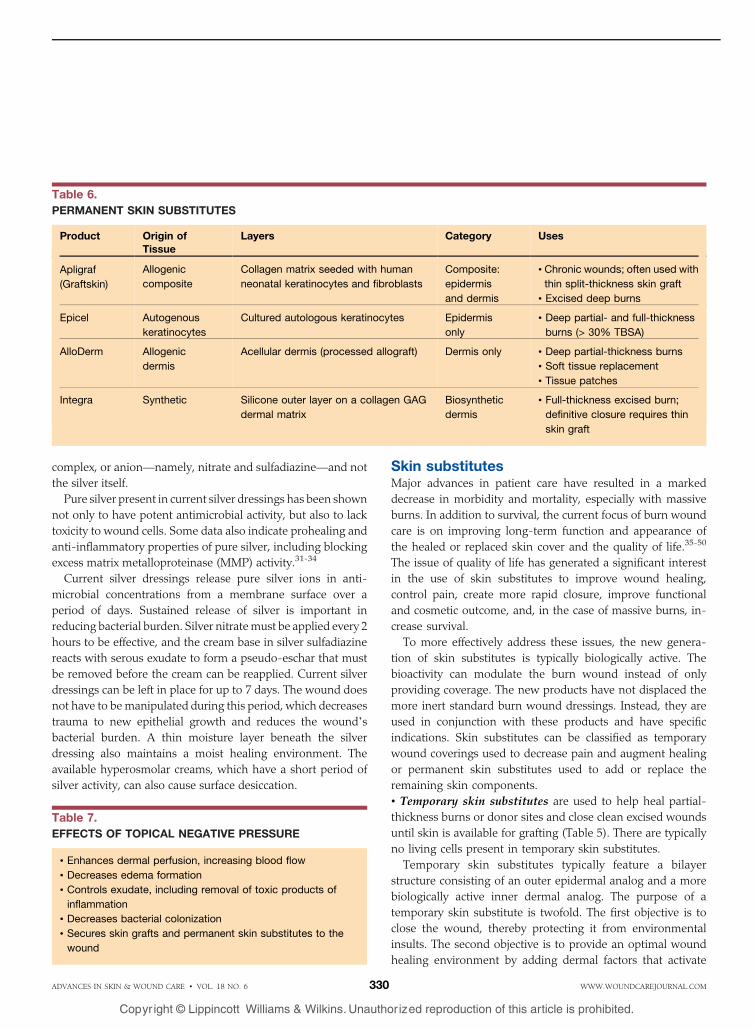
Table 6.
PERMANENT SKIN SUBSTITUTES
Product Origin ofTissue
Layers Category Uses
Apligraf
(Graftskin)
Allogenic
composite
Collagen matrix seeded with human
neonatal keratinocytes and fibroblasts
Composite:
epidermis
and dermis
& Chronic wounds; often used with
thin split-thickness skin graft
& Excised deep burns
Epicel Autogenous
keratinocytes
Cultured autologous keratinocytes Epidermis
only
& Deep partial- and full-thickness
burns (> 30% TBSA)
AlloDerm Allogenic
dermis
Acellular dermis (processed allograft) Dermis only & Deep partial-thickness burns
& Soft tissue replacement
& Tissue patches
Integra Synthetic Silicone outer layer on a collagen GAG
dermal matrix
Biosynthetic
dermis
& Full-thickness excised burn;
definitive closure requires thin
skin graft
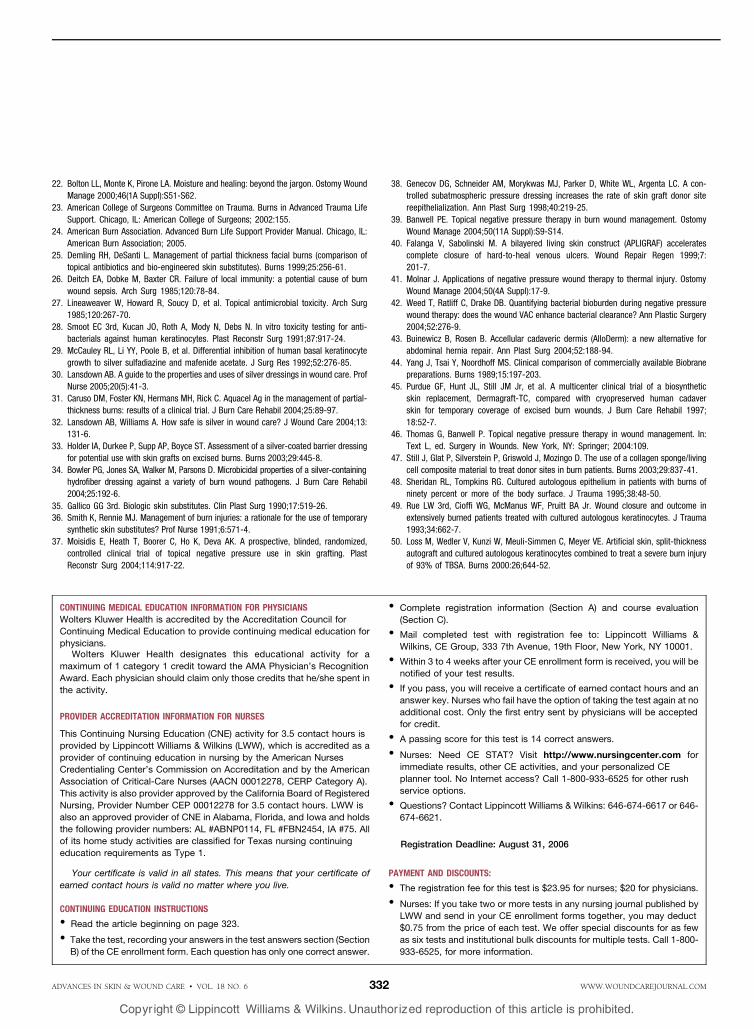
Table 7.
EFFECTS OF TOPICAL NEGATIVE PRESSURE
& Enhances dermal perfusion, increasing blood flow
& Decreases edema formation
& Controls exudate, including removal of toxic products of
inflammation
& Decreases bacterial colonization
& Secures skin grafts and permanent skin substitutes to the
wound
ADVANCES IN SKIN & WOUND CARE & VOL. 18 NO. 6 330 WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

and stimulate wound healing. Biologically active dermal
components are typically naturally provided to the inner
layer, which is then applied to the remaining dermis in a
partial-thickness burn or an excised wound.
& Permanent skin substitutes are used to replace lost skin by
providing an epidermis, dermis, or both. They offer a higher
quality of skin than a thin skin graft (Table 6). Most perma-
nent skin substitutes contain viable skin cells as well as
components of the dermal matrix.
The purpose of a permanent skin substitute is to restore
full-thickness skin loss and improve the quality of the skin
that has been replaced after a severe burn. Permanent skin
replacement is a more complex process than the use of a
temporary skin replacement product.35-50
Two approaches are available to develop a permanent skin
substitute. The first is the use of a bilayer skin substitute, with
the inner layer being incorporated into the wound as a neo-
dermis, rather than removed like a temporary product. The
outer layer is either a synthetic to be replaced by autograft
(epidermis) or actual human epithelial cells. The epithelial
cells, which will form the epidermal barrier, are often not
sufficiently developed at placement to immediately act in this
capacity.
The second approach is to provide either an epidermal or
dermal analog or a 1-layer tissue. These products are technically
not permanent skin substitutes on initial placement because
there is no bilayer structure, although they are often described
as such.
One disadvantage of skin substitutes is the absence of active
antimicrobial activity; however, early effective wound closure
decreases the risk of bacterial growth.
Topical negative pressure therapyThe use of topical negative pressure (TNP) in the form of
vacuum-assisted closure (VAC) is a recognized treatment for
wounds.36-45 Some of the effects of TNP therapy using VAC
are listed in Table 7.
Because of its beneficial effects, TNP therapy has been
introduced to various aspects of burn wound management
with positive results. For example, TNP therapy has been
used for the initial management of high-risk burns, such as
moderately deep hand burns, to decrease edema and
improve outcomes. Wound conversion appears less likely
when TNP is used in these cases because it removes edema
and improves dermal blood flow. TNP therapy has also
been found to improve management of difficult burns,
especially those on the perineum and buttocks. Increased
healing of donor sites and improved skin graft take have
also been reported.
SUMMARYMultiple factors affect burn severity and outcome. Burn depth,
percentage of TBSA, age, chronic illness, overall heath status,
part of the body burned, and presence of smoke inhalation
injury contribute to the rate of burn survival.
Management of a burn wound has made remarkable
progress over the last 10 years. Statistics indicate that burn
survival has markedly improved in recent years, provided
that optimum care is available from the injury scene to
discharge. These outcomes, in part, parallel the advances made
in wound healing and general wound management. Improve-
ments in technology, infection control, and skin substitutes
have also contributed to the improvements made in burn
wound care.
Although significant differences remain in the pathophy-
siology and treatment of burn wounds compared with
nonburn wounds, the focus of wound care remains the same:
rapid wound closure and universal infection control.&REFERENCES1. Artz C. Historical aspects of burn management. Surg Clin North Am 1970;50:1193-200.
2. Munster AM, Smith-Meek M, Sharkey P. The effect of early surgical intervention on
mortality and cost-effectiveness in burn care, 1978-91. Burns 1994;20:61-4.
3. Moncrief JA. Topical therapy of the burn wound: present status. Clin Pharmacol Ther
1969;10:439-48.
4. Spies M, Muller M, Herdon D. Modulation of the hypermetabolic response after burns.
In: Herndon D, ed. Total Burn Care. Philadelphia, PA: WB Saunders; 2001:363.
5. Sheridan R. Burn care: results of technical and organizational progress. JAMA 2003;
290:719-22.
6. Monafo WW. Initial management of burns. N Engl J Med 1996:335;1581-6.
7. Demling RH, Seigne P. Metabolic management of patients with severe burns. World
J Surg 2000;24:673-80.
8. Monafo W, Bessy P. Wound care in total burn care. In: Herndon D, ed. Total Burn Care.
Philadelphia, PA: WB Saunders; 2001:109.
9. Monafo WW, West MA. Current treatment recommendations for topical burn therapy.
Drugs 1990;40:364-73.
10. Williams W. Pathophysiology of the burn wound. In: Herndon D, ed. Total Burn Care.
Philadelphia, PA: WB Saunders; 2001:514.
11. Mast B. The skin. In: Cohen K, Diegelmann L, eds. Wound Healing. Philadelphia, PA: WB
Saunders; 1992:344-55.
12. Zawacki B. Reversal of capillary stasis and prevention of necrosis in burns. Ann Surg
1974;180:98-102.
13. Constable JD. The state of burn care: past, present and future. Burns 1994;20:
316-24.
14. Moncrief JA. The development of topical therapy. J Trauma 1971;11:906-10.
15. Aldrich R. The role of infection in burns, therapy and treatment. N Eng J Med 1933;
208:249.
16. Heggers J, Hawkins H, Edgar P, Villarreal C, Herndon D. Treatment of infections in burns.
In: Herndon D, ed. Total Burn Care. Philadelphia, PA: WB Saunders; 2001:120-69.
17. Robson MC. Bacterial control in the burn wound. Clin Plast Surg 1979;6:515-22.
18. Engrav LH, Heimbach DM, Reus JL, Harnar TJ, Marvin JA. Early excision and grafting
vs. monoperative treatment of burns of indeterminant depth: a randomized prospective
study. J Trauma 1983;23:1001-4.
19. Boswick J. The role of dressings in treating burn wounds. In: The Art and Science of
Burn Care. Gaithersburg, MD: Aspen; 1987:53.
20. Park GB. Burn wound coverings–a review. Biomater Med Dev Artif Organs 1978;6:1-35.
21. Krasner D, Kennedy KL, Rolstad BS, Roma AW. The ABCs of wound care dressings.
Ostomy Wound Manage 1993;39(8):66, 68-9,72.
ADVANCES IN SKIN & WOUND CARE & JULY/AUGUST 2005331WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
22. Bolton LL, Monte K, Pirone LA. Moisture and healing: beyond the jargon. Ostomy Wound
Manage 2000;46(1A Suppl):S51-S62.
23. American College of Surgeons Committee on Trauma. Burns in Advanced Trauma Life
Support. Chicago, IL: American College of Surgeons; 2002:155.
24. American Burn Association. Advanced Burn Life Support Provider Manual. Chicago, IL:
American Burn Association; 2005.
25. Demling RH, DeSanti L. Management of partial thickness facial burns (comparison of
topical antibiotics and bio-engineered skin substitutes). Burns 1999;25:256-61.
26. Deitch EA, Dobke M, Baxter CR. Failure of local immunity: a potential cause of burn
wound sepsis. Arch Surg 1985;120:78-84.
27. Lineaweaver W, Howard R, Soucy D, et al. Topical antimicrobial toxicity. Arch Surg
1985;120:267-70.
28. Smoot EC 3rd, Kucan JO, Roth A, Mody N, Debs N. In vitro toxicity testing for anti-
bacterials against human keratinocytes. Plast Reconstr Surg 1991;87:917-24.
29. McCauley RL, Li YY, Poole B, et al. Differential inhibition of human basal keratinocyte
growth to silver sulfadiazine and mafenide acetate. J Surg Res 1992;52:276-85.
30. Lansdown AB. A guide to the properties and uses of silver dressings in wound care. Prof
Nurse 2005;20(5):41-3.
31. Caruso DM, Foster KN, Hermans MH, Rick C. Aquacel Ag in the management of partial-
thickness burns: results of a clinical trial. J Burn Care Rehabil 2004;25:89-97.
32. Lansdown AB, Williams A. How safe is silver in wound care? J Wound Care 2004;13:
131-6.
33. Holder IA, Durkee P, Supp AP, Boyce ST. Assessment of a silver-coated barrier dressing
for potential use with skin grafts on excised burns. Burns 2003;29:445-8.
34. Bowler PG, Jones SA, Walker M, Parsons D. Microbicidal properties of a silver-containing
hydrofiber dressing against a variety of burn wound pathogens. J Burn Care Rehabil
2004;25:192-6.
35. Gallico GG 3rd. Biologic skin substitutes. Clin Plast Surg 1990;17:519-26.
36. Smith K, Rennie MJ. Management of burn injuries: a rationale for the use of temporary
synthetic skin substitutes? Prof Nurse 1991;6:571-4.
37. Moisidis E, Heath T, Boorer C, Ho K, Deva AK. A prospective, blinded, randomized,
controlled clinical trial of topical negative pressure use in skin grafting. Plast
Reconstr Surg 2004;114:917-22.
38. Genecov DG, Schneider AM, Morykwas MJ, Parker D, White WL, Argenta LC. A con-
trolled subatmospheric pressure dressing increases the rate of skin graft donor site
reepithelialization. Ann Plast Surg 1998;40:219-25.
39. Banwell PE. Topical negative pressure therapy in burn wound management. Ostomy
Wound Manage 2004;50(11A Suppl):S9-S14.
40. Falanga V, Sabolinski M. A bilayered living skin construct (APLIGRAF) accelerates
complete closure of hard-to-heal venous ulcers. Wound Repair Regen 1999;7:
201-7.
41. Molnar J. Applications of negative pressure wound therapy to thermal injury. Ostomy
Wound Manage 2004;50(4A Suppl):17-9.
42. Weed T, Ratliff C, Drake DB. Quantifying bacterial bioburden during negative pressure
wound therapy: does the wound VAC enhance bacterial clearance? Ann Plastic Surgery
2004;52:276-9.
43. Buinewicz B, Rosen B. Accellular cadaveric dermis (AlloDerm): a new alternative for
abdominal hernia repair. Ann Plast Surg 2004;52:188-94.
44. Yang J, Tsai Y, Noordhoff MS. Clinical comparison of commercially available Biobrane
preparations. Burns 1989;15:197-203.
45. Purdue GF, Hunt JL, Still JM Jr, et al. A multicenter clinical trial of a biosynthetic
skin replacement, Dermagraft-TC, compared with cryopreserved human cadaver
skin for temporary coverage of excised burn wounds. J Burn Care Rehabil 1997;
18:52-7.
46. Thomas G, Banwell P. Topical negative pressure therapy in wound management. In:
Text L, ed. Surgery in Wounds. New York, NY: Springer; 2004:109.
47. Still J, Glat P, Silverstein P, Griswold J, Mozingo D. The use of a collagen sponge/living
cell composite material to treat donor sites in burn patients. Burns 2003;29:837-41.
48. Sheridan RL, Tompkins RG. Cultured autologous epithelium in patients with burns of
ninety percent or more of the body surface. J Trauma 1995;38:48-50.
49. Rue LW 3rd, Cioffi WG, McManus WF, Pruitt BA Jr. Wound closure and outcome in
extensively burned patients treated with cultured autologous keratinocytes. J Trauma
1993;34:662-7.
50. Loss M, Wedler V, Kunzi W, Meuli-Simmen C, Meyer VE. Artificial skin, split-thickness
autograft and cultured autologous keratinocytes combined to treat a severe burn injury
of 93% of TBSA. Burns 2000:26;644-52.
CONTINUING MEDICAL EDUCATION INFORMATION FOR PHYSICIANSWolters Kluwer Health is accredited by the Accreditation Council for
Continuing Medical Education to provide continuing medical education for
physicians.Wolters Kluwer Health designates this educational activity for a
maximum of 1 category 1 credit toward the AMA Physician’s Recognition
Award. Each physician should claim only those credits that he/she spent in
the activity.
PROVIDER ACCREDITATION INFORMATION FOR NURSES
This Continuing Nursing Education (CNE) activity for 3.5 contact hours is
provided by Lippincott Williams & Wilkins (LWW), which is accredited as a
provider of continuing education in nursing by the American Nurses
Credentialing Center’s Commission on Accreditation and by the American
Association of Critical-Care Nurses (AACN 00012278, CERP Category A).
This activity is also provider approved by the California Board of Registered
Nursing, Provider Number CEP 00012278 for 3.5 contact hours. LWW is
also an approved provider of CNE in Alabama, Florida, and Iowa and holds
the following provider numbers: AL #ABNP0114, FL #FBN2454, IA #75. All
of its home study activities are classified for Texas nursing continuing
education requirements as Type 1.
Your certificate is valid in all states. This means that your certificate of
earned contact hours is valid no matter where you live.
CONTINUING EDUCATION INSTRUCTIONS
& Read the article beginning on page 323.
& Take the test, recording your answers in the test answers section (Section
B) of the CE enrollment form. Each question has only one correct answer.
& Complete registration information (Section A) and course evaluation
(Section C).
& Mail completed test with registration fee to: Lippincott Williams &
Wilkins, CE Group, 333 7th Avenue, 19th Floor, New York, NY 10001.
& Within 3 to 4 weeks after your CE enrollment form is received, you will be
notified of your test results.
& If you pass, you will receive a certificate of earned contact hours and an
answer key. Nurses who fail have the option of taking the test again at no
additional cost. Only the first entry sent by physicians will be accepted
for credit.
& A passing score for this test is 14 correct answers.
& Nurses: Need CE STAT? Visit http://www.nursingcenter.com for
immediate results, other CE activities, and your personalized CE
planner tool. No Internet access? Call 1-800-933-6525 for other rush
service options.
& Questions? Contact Lippincott Williams & Wilkins: 646-674-6617 or 646-
674-6621.
Registration Deadline: August 31, 2006
PAYMENT AND DISCOUNTS:
& The registration fee for this test is $23.95 for nurses; $20 for physicians.
& Nurses: If you take two or more tests in any nursing journal published by
LWW and send in your CE enrollment forms together, you may deduct
$0.75 from the price of each test. We offer special discounts for as few
as six tests and institutional bulk discounts for multiple tests. Call 1-800-
933-6525, for more information.
ADVANCES IN SKIN & WOUND CARE & VOL. 18 NO. 6 332 WWW.WOUNDCAREJOURNAL.COM
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.