Embed Size (px)
Citation preview

Functional Neurolgical Disorder in PaediatricsJOSH KWANT
16/11/21

“Here is my body, speaking.”
Aims
• Understand the presentation of FND• Understand some of the mechanism
underlying• Discussion and questions• Role of physiotherapy and the MDT• Treatment of FND• Discussion and questions
“Many of the Truths that we cling to depend on our point of view”
YODA

Intro• Changing the culture of care for children and adolescents with
functional neurological disorder• https://www.sciencedirect.com/science/article/pii/S2589986421000605#b0385
• Often poorly managed in our healthcare system• FND presentation in children possibly 5-15% of paediatrician referrals, mostly
neurological, frequently misdiagnosed• Silo treatment- Can present with a wide range of physical and psychological
factors making it hard to fit into service• Poorly understood mechanism in the wider staff population• Many preconceptions and often excluding from service• Difficulty with language and stigma• Feigning in FND comparable with other neuro conditions 1-2%

Things to remember:
Everyone can help- easy to make a positive difference
Its treatable, can resolve completely
Timely education can make a huge difference to lifeling disability

Presentation
Often in age 10+ and particularly teens (periods of significant change physically and environmentally)
Female 3:1 Male
Variable symptoms, incongruence, adaptable
Alongside existing conditions (Mind, Brain, Body)
Variety of presentations: Can be due to trauma, but could also be a high functioning, perfectionisitic individual with healthy supportive family life.

Physical Presentation
Can involve multiple systems in the body
Paralysis, Movement, Sensory problems, Seizures, Consciousness, Tremor, Dystonia, Tics, dizziness
Also: voice, language, swallow, vision, bowel/bladder, cardiac, blood pressure, breathing, unusual behaviour, cognition
Can fluctuate or be constant, be present by itself or as an overlay to an existing condition

FND Mechanism
Link between stress systems and motor systems
Problems with attention and expectation related to their body functioning
May involve psychological factors, trauma or abuse, but may involve NONE of those
Not caused specifically by physical damage to the system, but could be triggered by physical symptoms or exist alongside other conditions
Symptoms can fluctuate due to the varying pathways utilized by the brain for function

Possible mechanism-THINK HOLISITIC!

Attention
• The brain senses changes in the body• It focusses on this change and there is a cascading effect
on the brain function• The hyperexcitability of the system contributes to this
effect• Abnormal processing of sensory information• Problems with conceptualising explicit movement (implicit
intact)
• The brain is unusally attentive to the body and when that attention is distracted the movement may return to normal
• It can be a key way of demonstrating the condition to the patient and explaining how it happens.
• It can also be used as part of treatment in retraining automated movements

Expectation
The brain starts to predict movement incorrectly- picking up on information that the body is sending and attributing unnecessary importance to it.
This can result in a drop in motor function- like confidence. What we expect to happen, happens in an unusual or unexpected way
The loop of expectation/attention and action is reinforced, resulting in poorer movement. It can often be in conjunction with dissociative behaviours
By demonstrating and practicing normalized movements we can retrain this confidence, altering the expectation of movement back to a more usual and expected form

Brain Studies• fMRI, CT, SPECT, tMS etc.• Abnormal Emotional processing affecting mvt intiation
• ↑ R Amygdala, Insula and bilateral cingulate cortices ↓ SMA/DLPF cortex• Abnormal sense of agency (cause of your actions)
• ↑ Tempero-parietal junction (perception) connect with SMA, ↓ TPJ connect with sensorimotor cortex and cerebellum
• Abnormal inhibitory function (in motor weakness)• ↓ activity in cortical area responding to area of weakness. No change in those feigning
symptoms• Abnormal subcortical changes
• ↑ activity in controlateral Thalamus and BG with sensorimotor stimulation of affected limb (in unilateral presentation)
• ↑ DLPF cortex in both organic and functional dystonia, ↑ in M1 for organic, ↑ in cerebellum and BG in functional dystonia
• Structural changes• ↑ stress-mediated neuroplasticity in Amygdala, insula and cingulate cortex (similar to PTSD)• ↑ Thickening of premotor cortex in functional hemiparesis• ↓ volume of left Thalamus in functional movement disorders, irrespective of presentation

Neurons that fire together, wire together.

CASE STUDY-16 y.oFemale
• Assessed in March• High performing in school, good group of
friends• Very close relationship with parents,
younger sister (at home) and brother, older sister (away from home)
• Due to do GCSEs in summer• Dance, Scouts, active• Had heart repair for TOF in infancy- no
issues since• Diagnosed with FND 1.5 years prior (Age
14) No other PMH• Mum and Dad both present for
assessment• Initially mum helped give info, but by the
end conversation was only with her

Subjective
• Describes happy, healthy relationships and family life, enjoys school.
• No specifics on bullying but had a couple of episodes where a photo was circulated and also a video.
• Fainting episode for 1.5 years, started when left out of a group chat of her close friends
• Non-epileptic absence seizures since that at regular intervals (monthly)
• Reduced during lockdown, but started developing:• tremors- large and small amplitude in legs• Stuttering talking
• 2-3 week history of movement issues- unable to walk (legs collapse), but can move legs on the ground, can crawl around home and manage all ADL.
• Has issues with panic and anxiety and is seeing psychologist
• Admits she puts a lot of pressure on herself
• Guilty about effect it has on family• Low self-esteem- feels she should be a better person• Perfectionistic

Objective
• Has had investigations prior to this and all have come back clear
• Initially poor eye contact, but improved during session
• Moving normally in sitting, gesturing with both hands
• Jerking of legs noted initially, but settled once conversing
• Moving normally on the ground for all activities
• On trying to stand, tries to use arms to pull herself up, but legs won’t hold her and she collapses
• No reported sensory change

Discussion
• Any Questions?

Role of MDT
• MDT WORKING VITAL• Very important- particularly Consultant
(diagnosis) and School engagement (long term management)
• Joined up, scope for very close working as lots of overlap
• Importance of psychology where needed• Importance of psychologically informed
treatment for physio and OT


Role of Physio
• Restoration of Motor function (affect movement dysfunction, distraction, retrain normal patterns)
• Physical Conditioning (enjoying activity and being fit)
• Education• Autonomic system regulation
(breathing control, Bp resilience, Exercise tolerance)
• Stress resistance (relaxation, breathing with movement)
• Managing pain• Pick up on symptoms for potential
investigation• Aspects of Compassion Focused
Therapy
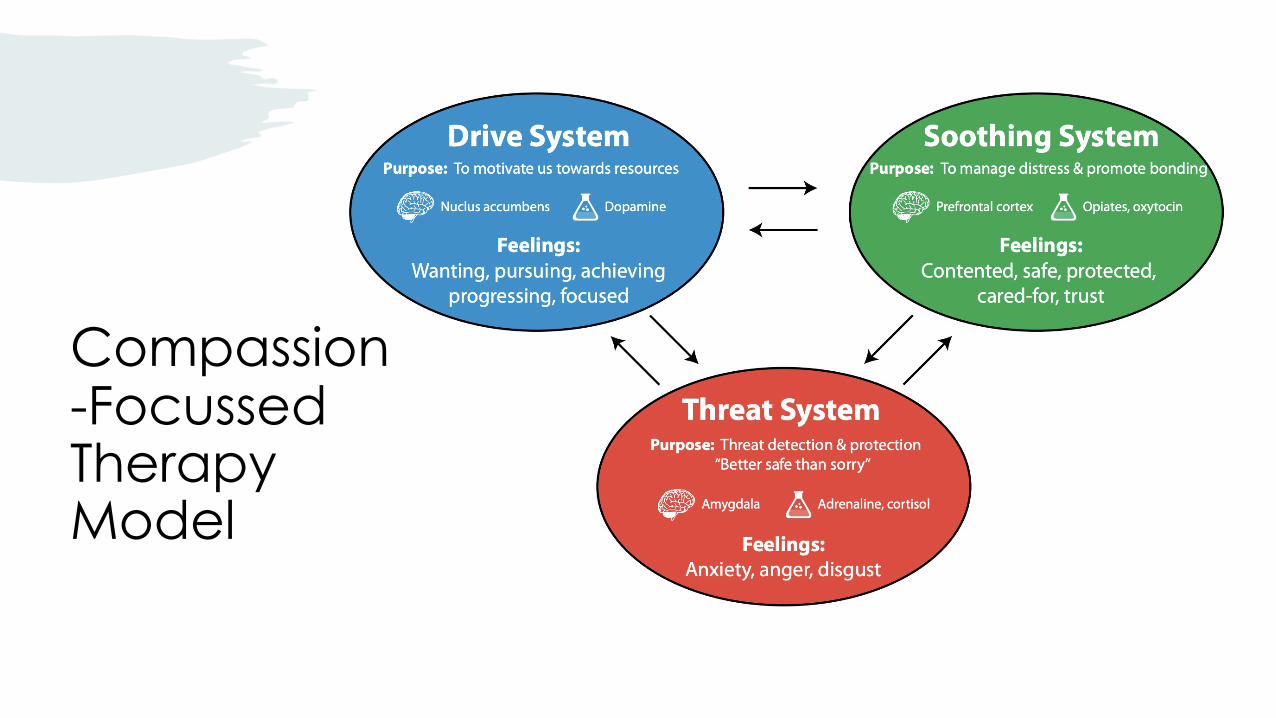
Compassion-FocussedTherapy Model

IMPORTANT
• Tone of voice• Safe place• Their story not yours• Patience• Easy to understand
language, but not patronizing

Subjective Assessment
• See video-https://www.youtube.com/watch?v=w4obwKD8JLU
• FNDS website- Jon Stone 11/06/20- delivering a diagnosis
• List of all historic symptoms and timeline• Current symptoms and presentation
• Previous medical history• Investigations to date and pending• Ask about family, school life, or other stressors/safety
mechanisms• Any particular triggers to condition and any to
symptoms• Consider and check any secondary gains (changes
to schooling, one-to-one teaching)

Things to consider when questioning
Predisposing Factors (Unique to each of us) •Your genetic make-up, your beliefs, how you think the body works, experience of ill-health (direct and indirect), culture, trauma/abuse/grief/illness
1Precipitating Factors (Triggers, stuff that helps the FND to establish)•Physical, Psychological, Social, bits of all of them.
•Things like injury, hormone changes, new sensations, pain, physical illness, medication, experiences, trauma, stress, grief, emotional event, challenging ideas to health behaviours, group effect.
2Perpetuating Factors (Things that keep it hanging around) •Reduced recognition of the condition or hampering treatment.
•Physical, Psychological, Social and bits of all of them.
•Things like pain, frustration, expectation, awareness, previous treatment, secondary gains, health professional intervention, social effects, self-worth, ongoing trauma/abuse.
3
Objective Assessment
• Observe them moving• Try in different postural positions and in
different tasks• Engaging and Fun• Observe in task when distracted• Look for inconsistencies in movement• Observe and note the impairment with the
patient and family but don’t give it a lot of attention
• Look for normalised movement• Special tests

Observations and Special tests (see tables at end)• Give way weakness• Incongruity• Tip toe standing possible despite poor ankle strength on local testing• Hoovers sign
• Hip flexion of strong limb in supine with contralateral extension felt in weak limb
• Hip abductor sign• Hip abduction of strong limb with contralateral abduction felt in weak limb
• Tremor entrainment• Whack a mole sign• Dragging of foot• Inconsistent limp• Change of movement patterns when engaged in task

Treatment
• Listen compassionately• Explain condition origin (Simple explanation
of FND using brain stress image )• Retrain movements with distraction-
demonstrate to patient• Avoid repetition of difficult movement-
reduce fear associated with it• Focus on fun movement, things that enhance
and engage• Enhance movement patterns in available
range• Engage with movement in different positions

Brain-Stress model
When the red dot gets bigger it eventually impacts on movement or other aspects of your condition

CASE STUDY-16 y.oFemale
Treatment
• Discussed FND and her understanding of it• Reviewed when her symptoms arose and what affected
them• Practiced floor based exercise such as Yoga, and exercise
in kneeling (indoor basketball with her sister)• Has fun doing yoga with her dad (because he’s so bad at it)
so encouraged.• Focus on floor and interpretive dance (which she likes)
rather than worrying about her ballet• Mental imagery around how her legs feel and truth about
her condition (might feel weak, but its properly strong!)• Affirmation of her value and importance outside of being
unwell (not a victim and not a burden)• Acceptance of her perception of failure• Focus on being kind to herself and realistic in her
expectations• Discussed pacing and rest.• Gave challenges for progressively more challenging
exercise with distraction• Suggested ideas for her to take to her psychologist to discuss
further (dissociation about her friendships and the impact it had, feelings of self-worthlessness)
• 90 min session - 70 mins on subjective and discussion, 20 mins on physical practice and exercise

Outcome
• No further physio sessions
• Mum spoke to school about recommendations and graded return to face-to-face
• Worked on her activity independently (with family) and gradually regained function in legs
• Back to dancing and sport
• Passed GCSE’s and onto A-Levels
• Less anxious about her symptoms and potential recurrence
• Ongoing work with psychologist
• Aware of potential for relapse when stressors start to rise again

Conclusion• FND happens when the stress management parts of the brain start to
impact on the other areas of the brain, disrupting function.• Its not due to damage to the structures of the brain, but is very disabling
and is due to misfiring of otherwise healthy areas of the brain• Can be fully treatable, but longer onset prior to diagnosis can be linked
with poorer outcome• Importance of treating the individual, as unique, and as part of an MDT• Language is vital, as well as reducing stigma, with the most important
aspect being the understanding and acceptance of the condition rather than just focusing on symptoms resolution
• Consider their journey through the healthcare system till the point you see them, be patient and try and give them time wherever possible.

Appendix- Resource list
• FNDS: the FND society. Worth a year’s subscription to have access to a significant webinar back catalogue
• FND Hope: Charity with excellent resource and support network for parents and children with FND; https://www.fndhope.org.uk/
• Website: www.neurosymptoms.org. Improve knowledge of the condition and recommend to patients JUDISCIOUSLY (when they’re ready) as it is full on with info.
• Twitter: FND Portal: @FndPortal. A person with FND and with extensive knowledge of the latest published research as well as connecting personal stories.
• Video of simple diagnosis (Patient Friendly): https://www.youtube.com/watch?v=DYtE8h2swnM
• Adult patient experience (dutch with subtitles): https://www.youtube.com/watch?v=w4lqr4Mo32M

References• Kasia Kozlowska, Tyson Sawchuk, Jeff L. Waugh, Helene Helgeland, Janet Baker, Stephen Scher, Aaron D. Fobian. Changing the culture of care for children and adolescents with
functional neurological disorder. Epilepsy & Behavior Reports, Volume 16, 2021
• Espay AJ, Aybek S, Carson A, et al. Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders. JAMA Neurol. 2018;75(9):1132-1141.
• Roelofs, J.J., Teodoro, T. & Edwards, M.J. Neuroimaging in Functional Movement Disorders. Curr Neurol Neurosci Rep 19, 12 (2019)
• Nielsen G, Stone J, Matthews A, et al Physiotherapy for functional motor disorders: a consensus recommendation. Journal of Neurology, Neurosurgery & Psychiatry 2015;86:1113-1119
• Valerie Voon, Andrea E. Cavanna, Kerry Coburn, Shirlene Sampson, Alya Reeve, W. Curt LaFrance, Jr. Functional Neuroanatomy and Neurophysiology of Functional Neurological Disorders (Conversion Disorder). The Journal of Neuropsychiatry and Clinical Neurosciences 2016 28:3, 168-190
• Edwards MJ, Adams RA, Brown H, et al.: A Bayesian account of ‘hysteria’. Brain, 2012; 135:3495–3512
• Stone J, LaFrance WC Jr, Brown R, et al.: Conversion disorder: current problems and potential solutions for DSM-5. J Psychosom Res 2011; 71:369–376
• V. Voon, C. Brezing, C. Gallea, R. Ameli, K. Roelofs, W.C.LaFrance, et al. Emotional stimuli and motor conversion disorder. Brain, 133 (5) (2010), pp. 1526-1536
• D.L. Perez, M.J. Edwards, G. Nielsen, K. Kozlowska, M. Hallett, W.C. LaFrance, Jr. Decade of progress in motor functional neurological disorder: Continuing the momentum. J NeurolNeurosurg Psychiatry, 92 (6) (2021), pp. 668-677
• Stone J, Carson A, Duncan R, et al. Who is referred to neurology clinics?—the diagnoses made in 3781 new patients. Clin Neurol Neurosurg 2010; 112(9):747–751.
• Espay AJ, Lang AE. Phenotype-specific diagnosis of functional (psychogenic) movement disorders. Curr Neurol Neurosci Rep 2015;15(6):32
• Kaski D, Bronstein AM, Edwards MJ, Stone J. Cranial functional (psychogenic) movement disorders. Lancet Neurol 2015;14(12):1196–1205
• Baik JS, Lang AE. Gait abnormalities in psychogenic movement disorders. Mov Disord2007;22(3):395–399
• Reuber M, Howlett S, Khan A, Grünewald RA. Non-epileptic seizures and other functional neurological symptoms: predisposing, precipitating, and perpetuating factors. Psychosomatics2007;48(3):230–238
• Kozlowska, K; Scher, S; Helgeland, H. Functional somatic symptoms in children and adolescentshttps://library.oapen.org/bitstream/handle/20.500.12657/42568/2020_Book_FunctionalSomaticSymptomsInChi.pdf?sequence=1
• Gilli, Peter. Patient Perspective. Connections, Fall 2021.https://www.canva.com/design/DAEkw1Ey7e8/uFM0wsL5przDbB3fklvbbg/view?utm_content=DAEkw1Ey7e8&utm_campaign=designshare&utm_medium=link&utm_source=sharebutton#14

Appendix:
Observation signs








![Josh.6:21 · Josh.6:21 They utterly destroyed everything in the city [of Jericho], both man and woman, young and old, and ox and sheep and donkey, with the edge of the sword. Josh.8:25](https://img.pdfslide.us/doc/110x75/5f08b0d77e708231d4234063/josh621-josh621-they-utterly-destroyed-everything-in-the-city-of-jericho.jpg)