Embed Size (px)
DESCRIPTION
Issue 1 - 2011 (Jan-Feb)
Citation preview
Organe de la sOciete rOyale belge de radiOlOgie (srbr)Orgaan van de kOninklijke belgische vereniging vOOr radiOlOgie (kbvr)
diagnOstic and interventiOnal imaging, related imaging sciences,and cOntinuing educatiOn
Wetteren 1
1 volume 94 Page 1-58
January-February
Bimonthly – 2011
P 702083
Project couv-2011.indd 1 16/02/11 10:41
JBR-BTR � 94/1 � 2011
Journal Belge de � Belgisch Tijdschrift voor � RADIOLOGIE
Founded in 1907
A bimonthly journal devoted to diagnostic and interventional imaging,related imaging sciences, and continuing education
Contents
The value of proton MR-spectroscopy in the differentiation of brain tumours from non-neoplastic brain lesions.H. Aydın, S. Sipahioglu, N. Aydın Oktay, E. Altın, V. Kızılgöz, B. Hekimoglu . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Pleuropulmonary blastoma presenting as a complicated pleural effusion.J. O’Brien, D. Rea, R. Hayes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Primary pelvic hydatid cyst with sciatic compression.F. Nouira, T. Chouikh, A. Charieg, S. Ghorbel, S. Jlidi, B. Chaouachi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Uterus didelphys with obstructed hemivagina and renal agenesis: MRI findings.A. Talebian Yazdi, K. De Smet, C. Ernst, B. Desprechins, J. de Mey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Acute adrenal insufficiency due to bilateral adrenal hemorrhage.X. Zhu, I.C. van der Schaaf, J.A. van der Valk, A.K. Bartelink, M. Nix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Hepatic alveolar echinococcosis: a diagnostic challenge.O. Yapici, S.M. Erturk, M. Ulusay, A. Ozel, A. Halefoglu, Z. Karpat, M. Basak . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Wernicke’s encephalopathy: a case report and MRI findings.S. Yucebilgin, T. Cirpan, C.Y. Sanhal, E. Ozan, T. Acar, S. Ozsener . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Diffuse “vertebra-within-vertebra” appearance at the adult age due to biphosphonate (pamidronate)administration during early adolescence.B. Coulier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Incidental radiological finding of a renal tumour leading to the diagnosis of Birt-Hogg-Dube syndrome.M. Schreuer, M. Lemmerling, W. Pauwels, D. Dewilde, C. Heyse, K.L. Verstraete . . . . . . . . . . . . . . . . . . . . . . . . 31
LETTER TO THE EDITOR
R. D’Hauwe, E. Lerut, L. De Wever, R. Oyen, F. Claus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
IMAGES IN CLINICAL RADIOLOGY
Pedunculated pleural lipoma.L. Cardinale, F. Avogliero, F. Solitro, C. Fava . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Denim Sandblasters’ Pneumoconiosis.M. Apaydin, M. Varer, S. Ayik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Dilated cisterna chyli.F.M. Vanhoenacker, M. Eyselbergs, C. Petre . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Iatrogenic facial subcutaneous emphysema after endodontic treatment.J. Coulier, F.C. Deprez . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
The ‘torus palatinus’: a common but relatively unknown entity.C. Boulet, M. De Maeseneer, T. Buisseret, M. Shahabpour, J. De Mey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
An unusual pelvic mass: bladder lymphoma.M. Alsinnawi, M. Quinlan, A. Brady, N. Khan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
The European day of Radiology (EDOR): an initiative of the ESR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43News from the Universities: Wetenschappelijke Prijs em Prof. Dr A.L. Baert . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Book presentation: De eerste wereldoorlog in Belgïe – Radiologie in “Trench coat” / La grande guerre de
1914-1918 – La radiologie belge monte au front. R. Van Tiggelen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Forthcoming courses and meetings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54Classified services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55Grants of the RBRS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56Instructions to Authors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iiSubscribers information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ciiAdvertising index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ciii
� The terms used for indexation of subjects were developed by the Radiological Society of North America (RSNA)over a period of years. Their use here is by permission of the RSNA. The terms may not be used in any otherindex, print or electronic, except by specific permission of RSNA.
�� Indexed in Index Medicus and in Zentralblatt Radiologie. Evaluated for Medline User, EMBASE and CANCERNET.Abstracted in Excerpta Medica Journals.
01-JBR-contents-11-1(dr)_Opmaak 1 16/02/11 11:19 Pagina 1

Imaging is an indispensable toolin modern medicine, yet very fewpatients know just how important itis. From cancer detection and thera-py to diagnosing stroke or serioustrauma in time, radiologists con-tribute to saving lives by coveringevery field of medicine. To raise pub-lic awareness, the European Societyof Radiology will launch theEuropean Day of Radiology onFebruary 10, marking the anniver-sary of x-ray discoverer WilhelmConrad Röntgen's death. MostEuropean national societies havejoined this initiative, including theRoyal Belgian Radiological Society,which has chosen to address thesensitive topic of radiation exposure.
Over the last decade, technicaladvances in computed tomography(CT) have been considerable. CTexaminations, which use x-rays anda computer to provide 3-dimension-al and slice images of the inside ofthe body, are now very fast andaccurate. For instance, CT can nowacquire excellent images of theentire body in less than 20 seconds.In patients suffering polytrauma, thisenables the quick overview of possi-bly life-threatening pathologies andincreases chances of survival. CT hasalso improved the detection of manycancers, significantly extending sur-vival time. Moreover, many abdomi-nal diseases are now easily diag-nosed and assessed with CT, pre-venting unnecessary surgery inmany cases. Finally, CT has becomethe standard imaging modality indiagnosing pulmonary embolismand is also gradually replacing car-diac catheterisation for some heartdiseases.
All these benefits have translatedinto a massive rise in CT examina-tions worldwide over the past twen-ty years. As a result, the population’scumulative exposure to ionisingradiation, a substance suspected ofcausing cancer in humans, hasgrown – and it may continue to growin the future. Ionising radiation is anintegral part of all imaging methods
pressure and frequencies, is widelyused in prenatal and paediatricimaging.
Over recent years, numerous successful efforts have been made toreduce the CT radiation dose. CTmanufacturers have developed CTscanners which are more dose- efficient and many radiologists haveoptimised their CT protocols in orderto reduce the radiation dose. “Theapproach is to act on the number ofperformed CT examinations and onthe dose per examination”, Tack said.
The high number of examinationshas been addressed by introducingprescription criteria to the entireBelgian medical community inNovember 2011. “The effects of suchguidelines are however not knownand almost impossible to predict asthere is no clear publication report-ing the potential benefit of such anapproach applied to an entire coun-try yet”, Tack explained.
Radiologists follow directives toensure patient safety. The ALARAprinciple (As Low As ReasonablyAchievable), which guarantees thatthe best examination is carried outusing the lowest possible dose ofradiation, is practised by every radi-ologist all around the world.
Regarding the dose per CT exam-ination, one can potentially reducethe collective dose by 30% if all scan-ners are correctly optimised.Surveys are being performed in theEU to measure inadequate practiceat least once every five years.Surveys show that there are signifi-cant differences between the lowestand the highest doses per acquisi-tion. It is suspected that the propor-tion of radiologists able to optimisetheir CT machines is low. In order tostimulate optimisation (reduction ofthe dose per examination), the fre-quency of surveys of CT examina-tions, conducted by the FANC(Federal Agency on Nuclear Control),will be increased to once a year inBelgium. Results from surveys couldserve as an objective of optimisationfor those who have not optimised
that use x-rays, such as CT or radio -graphy.
The dose provided by a CT exam-ination depends on the region onwhich it focuses. A chest CT gener-ates on average 7 mSv (millisievert –a derived unit of dose equivalentthat attempts to reflect the biologicaleffects of radiation), head CT, 2 mSv,and abdomen/ pelvic CT, 10 mSv.
The annual exposure for an aver-age person is about 3.6 mSv, 50 per-cent of which comes from naturalsources of radiation contained inwater, food, some materials and theatmosphere. The remaining 50 per-cent results from exposure to artifi-cial radiation sources, such as indus-trial sources like smoke detectors, asmall fraction from nuclear weaponstests, and medical sources – 60% ofwhich are induced by CT examina-tions.
However, it remains very difficultto assess the cancer risk induced bya CT examination, as the majority ofestimates so far are based on scien-tific studies of atomic bomb sur-vivors in Japan.
Every patient has a different sen-sitivity to radiation exposure, butsome factors are particularly signifi-cant. Children and young patientsare more sensitive than adults, forexample. “Fortunately, the numberof CT examinations performed inchildren is very low, especially whenscanning the body. Belgian radiolo-gists always consider all alternativesto CT prior to performing such exam-inations on children”, said DoctorDenis Tack, radiologist at the CliniqueLouis Caty, Baudour Hospital.
Females are also at slightly higherrisk, depending of the type of CTscan (e.g. CT of the thorax). Finally,the type of CT scan has a direct influ-ence on the exposure level.
Whenever possible, one performsexaminations with non-ionisingmodalities such as magnetic reso-nance imaging (MRI), which usesmagnetic fields to produce imagesof the inside of the body, and ultra-sound (US). US, which uses sound
JBR–BTR, 2011, 94: 1-2.
Radiation exposure in medicine: what you need to know
CELEBRATE THE POWDER OF IMAGING:THE EUROPEAN DAY OF RADIOLOGY
EDOR (Radiation)_Opmaak 1 9/02/11 09:52 Pagina 1

their CT acquisition parameters yet,with a system of awards for thosewho optimise and penalties forthose who don't.
The benefits of CT are undeniable,but nevertheless every examinationhas to be justified by a clinical indi-cation. In principle, the radiologisthas to weigh the potential benefitsagainst the risks and then decide ifthe ordered examination is appropri-ate or if a non-ionising modalitywould be more appropriate toanswer the clinical question. “Inadults, talking only about risks is notsatisfactory. One has to take intoaccount the benefit. For example,the risk of dying of pulmonaryembolism without adequate treat-ment is at least 50 to 500 times high-er than the radiation burden”, saidTack.
Educating referring doctors andradiologists could help reduce the
Patients should bear in mind thatCT examinations are not to berepeated at a different radiologicalinstitution, as the ordering physicianmight not know about CT studiesconducted shortly before the consul-tation.
Finally, frequent follow-up studiesusing CT could be avoided. In addi-tion, if CT is the only diagnosticmethod to answer the question ofthe follow-up study, a low dose pro-tocol with a reduced scan rangeshould be used. Depending on themedical question, diagnostic studieswithout ionising radiation such asMRI or US can be frequently used.
Contact:
Royal Belgian Radiological SocietyDr. B. DesprechinsPresident RBRS
number of examinations and thedose from CT even further. Doctorsshould be taught to take guidelinesinto account and be allowed to workwithin a reasonable timeframe.
One could also reduce CT dosesby enabling radiologists to change aprescription to a more appropriatetest or into a no-test strategy. Inaddition, one should help the med-ical community not to fear malprac-tice lawsuits, Tack believes.“Defensive medicine, to avoid anypossible malpractice lawsuit, plays avery important role in prescriptionwhen it comes to radiology”, he said.
Patients throughout the worldremain poorly informed about radia-tion exposure, so contact with theradiologist is key. They should firstbe informed that imaging tests maynot solve their problems. “They usu-ally believe CT and MR will seealmost everything”, added Tack.
2 JBR–BTR, 2011, 94 (1)
EDOR (Radiation)_Opmaak 1 9/02/11 09:52 Pagina 2

Non-invasive and accurate differ-entiation between neoplastic andnon-neoplastic brain lesions isimportant for determining the correct treatment plan and in somecases, may avoid the necessity ofbiopsy (1-3). Conventional MR imag-ing is a useful tool in the evaluationof tumoral and non-tumoral brainlesions but not really sufficient fordiagnosing all conditions (2-4).Proton magnetic resonance spec-troscopy [H-MRS]; A non-invasivetechnique, has been helpful inunderstanding the pathophysiologyof different pathologic processes (1-6). It has been used to observemetabolite changes for differentintracranial abnormalities such astumours, stroke, tuberculomas, multiple sclerosis (MS) and meta -bolic-inherited brain disorders,epilepsy and traumatic injuries (1-3,6). H-MRS provides biochemicalinformation from tissues by reflect-ing the alterations of metabolites inthe spectra, has proved to be usefulfor evaluating brain lesions espe -cially the differentiation of tumoursand non-neoplastic lesions (1, 2, 4).Several types of non-neoplasticbrain disorders (infectious- de my -elinating lesions etc.) can bepotentially misdiagnosed as braintumours, MR- Spectroscopy mayimprove the diagnosis of unknownbrain lesions (2-4, 7). H-MRS pro-vides information related to the
included in this retrospective study.Informed consent was obtained fromall the patients before the study.
The stratification of patients intotumoral or non-neoplastic groupdepends upon the following brainMRI items; For neoplastic group,Centrally or peripherally strongenhancing mass lesions with sur-rounding discrete vasogenic edemain cerebral or cerebellar hemi-spheres. For the non-neoplasticgroup; Plaque or nodular lesionsmostly situated at pericallosal-periventricular white matter- thalamus and basal ganglia, non-enhanced lesions without obviousmass effect with restricted diffusion,extra-axial non-enhancing cysticmasses with or without restriction inthe Diffusion Weighted MRI and focalnodular or conglomerated whitematter lesions. We have variety ofnon-neoplastic brain disorders thatinclude ischemic-demyelinating-metabolic (Wilson’s disease) andbenign mass lesions. Ischemic groupconsisted of acute and subacuteenfarcts , chronic ischemic areas orencephalomalasic regions wereexcluded. The demyelinating lesionswere; MS and Acute disseminatedensephalomyelitis (ADEM), all theactive or inactive plaques whethernew or old, were included in thisresearch. Diagnosis of all non-neoplastic brain disorders were confirmed by brain MRI, clinical andlaboratoy findings. We had intra -cranial tumours that include highgrade glial tumours (multiformglioblastoma-anaplastic astrocy-tomas), low-grade glial tumours(gliomatosis serebri-serebelli,ganglio gliomas), meningiomas andmetastasis. Except for a metastasiscase and two menengiomas, diagnosis of all brain neoplasms
neuronal integrity, cell proliferationor degradation, energy metabolismand necrotic transformation of brainor neoplastic tissues (5, 6, 8, 9).Particularly H-MRS is added to theroutine brain MRI in order to solvediagnostic problems such as differ-entiation of neoplastic and non-neo-plastic lesions, low and high gradetumours, ischemia from low gradegliomas or discriminating the metas-tases from primary brain tumoursand abcesses (3, 5, 6, 9). Variousspectroscopic methods have beenused to study tumour biology, gradegliomas, plan treatment and etc (3,5, 6, 8).
In this study, we aimed to test thestrength of H-MRS in the discrimina-tion of tumoral masses from non-neoplastic brain lesions. Further -more, we also wanted to check ifMRS can distinguish among thetypes of cerebral neoplasms.
Material and method
33 patients with intracranial masslesions confirmed by cranial MRIwere selected for proton-MR-Spectroscopy; 17 males-16 females,age range from 9 to 85, mean age 49± 2, patients for non-neoplastic brainlesions suggested by cranial MRIwere selected for H-MRS; 13 males-16 females with age range 17-80,mean age 48 ± 2. Totally 62 patients;30 males and 32 females were
JBR–BTR, 2010, 94: 3-12.
THE VALUE OF PROTON MR-SPECTROSCOPY IN THE DIFFERENTIATION OFBRAIN TUMOURS FROM NON-NEOPLASTIC BRAIN LESIONSH. Aydın, S. Sipahioglu, N. Aydın Oktay, E. Altın, V. Kızılgöz, B. Hekimoglu1
Purpose: Our aim was to evaluate the efficacy of Proton-MR Spectroscopy for the differentiation of cranial massesfrom non-neoplastic brain disorders.Material and method: 33 patients with intracranial mass lesions, 29 patients with non-neoplastic brain lesions:Ischemic-demyelinating-metabolic-benign cystic mass group; As a whole 62 patients: 30 males and 32 females wereincluded in this study.Results: In brain tumours, average Cho/NAA ratio 2.84-NAA/Cr ratio was 0.97, Cho/Cr ratio 2.42 and Cho/MI ratio was3.51. In non-neoplastic group; NAA/Cr ratio was extremely higher than tumour group, the other ratios were far lowerthan cranial mass lesions. Average Cho/NAA ratio: 0.50 ± 0.15, Cho/Cr ratio: 1.05 ± 0.14, Cho/MI ratio: 1.07 ± 0.73.Conclusion: Higher Cho/NAA and Cho/MI ratios with lower NAA/Cr ratio were most likely to be malignant.Additional lipid and lactate peaks were generally seen in malignant group.
Key-words: Brain, diseases – Brain neoplasms, MR – Magnetic resonance (MR), spectroscopy.
From: 1. Dıskapı Yıldırım Beyazıt Research Hospital, Radiology Department, Ankara,Turkey.Address for correspondence: Dr H. Aydin, Dıskapı Yıldırım Beyazıt Research Hospital,Radiology Department, Ankara, Turkey. E-mail: [email protected],[email protected]
aydin-hekimoglu-_Opmaak 1 9/02/11 10:10 Pagina 3

were confirmed pathologically eitherby biopsy or open-surgery. Patientwith cranial metastases was still suf-fering from a known primary neo-plasm and has also metastatic infil-trations in his lungs and liver sobiopsy was not needed. The diagno-sis of extra-axial menengiomas wasbased upon the MRI and clinical find-ings as the patients refused the biop-sy. All the MRI and Multi-voxel spec-troscopic analysis were carried outwith an 8-channel 1.5 T MR scanner(Philips Achieva, Philips Medical sys-tems-Netherlands) by using a stan-dart head and neck array coil.Multivoxel spectroscopic technique(MVS) was taken into account for alllesions in the study; in contrary wedidn’t perform single-voxel spec-troscopy in this research.
The MRS was performed by usingpoint-resolved spectroscopy (PRESS)with a volume of interest (VOI),1*1*0.5 cm3 standard voxel sizes forthe MVS and presaturation bandsplaced around the VOI. Dependingupon the tumour and the lesion size,approximately 5-10 cm3 tumor areaon the multivoxel imaging was har-bored with the volume made up ofsuch Standard voxels. We have posi-tioned the possible voxel within thesolid tumoural or lesional areaavoiding areas of cysts, normalappearing brain parenchyma, scalpor skull base contamination (6-8).Automatic shimming of the linearx,y,z channels was used to optimizefield homogeneity, water resonanceand water suppression pulses wereoptimized for the consistent watersaturation.
Data analysis
Proton spectrum was recorded inaxial plane with TR; 1500 ms,TE; 26and 144 ms, FOV; 24 x 24 cm, 0.5 cmslice thickness, 256 x 256 matrix and24 x 24 phase encoding. Duration ofscan for both TE acquisitions wasabout 5 min. Time domain data weremultiplied with a Gaussian functionof 90 (Centre 0, halfwidth 256 ms),2D Fourier transformed phase andbase-line corrected, quantified bymeans of frequency domain curvefitting with the assumption of aGaussian line shape, spectral analy-sis and all post-processing were car-ried out by using a software ofPhilips Achieva Netherland work-shop. 0-4.35 ppm is analysed andmetabolite signals and the data wereprocessed as follows; N-Acetylaspartate (NAA) at 2 ppm, creatine(Cr) at 3-3.1 ppm, Phosphocreatine(Cr2) at 3.8-3.9 ppm, Choline (Cho) at
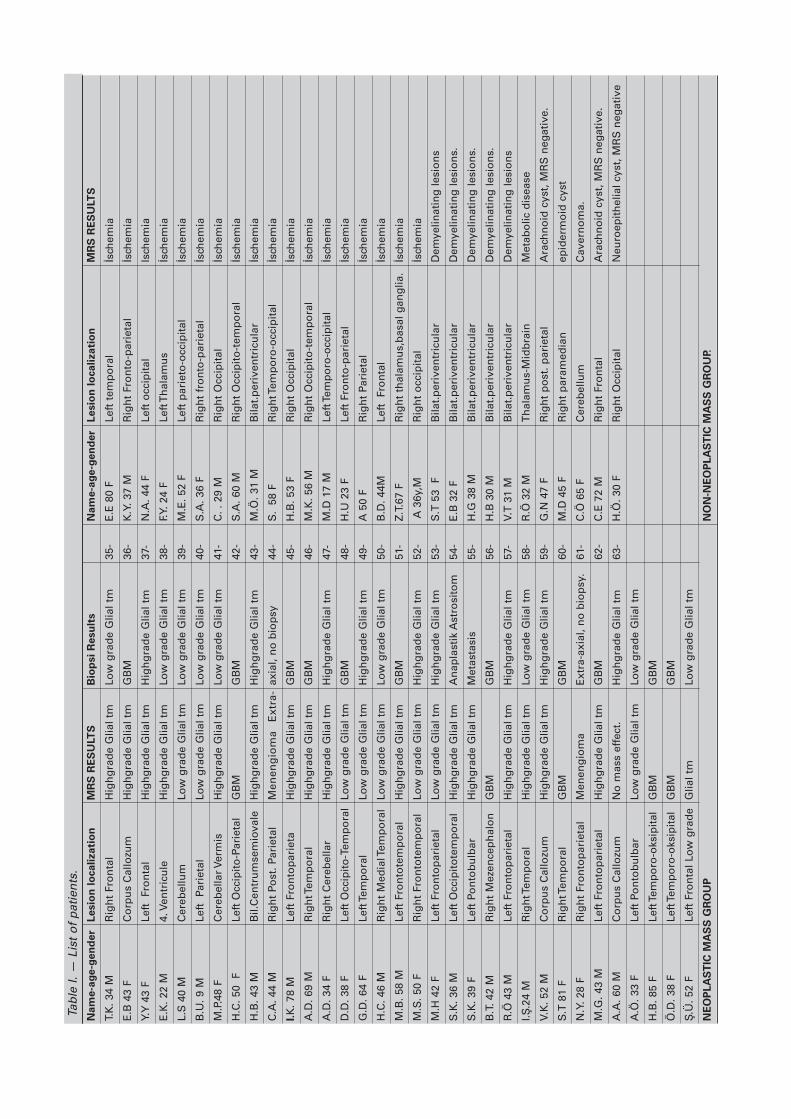
demyelinating (MS-ADEM)-metabol-ic (Wilson syndrome), benign cysticmass group (arachnoid-epidermoidcysts-cavernoma); we have the ageand the gender of patients, lesionlocalizations, NAA/Cr, Cho/NAA,Cho/Cr, Cho/MI ratios, biopsy resultsand other increased metabolitepeaks (Table I). 30 patients withspace-occupying brain massesunderwent biopsy or open surgery,only the metastasis and menin-giomas had no histopathologic con-firmation. In one patient, there wasno mass profile in MRSI but thehistopathology was anaplastic astro-cytoma, except for this case H-MRSproved all the mass lesions (32/33).The statistical analysis and measure-ment of metabolite peaks were per-formed in 32 patients. The diagnosisof other non-neoplastic lesions wereproved by MRI, by clinical routes andby biochemical laboratory results.The spectra from the contralateralbrain or from the healthy volunteersrevealed a consistent pattern of thefour major peaks of NAA, Cr, Choand MI, no lactate or lipid reso-nances were visible in these cases.The average NAA/Cr, Cho/NAA,Cho/Cr, Cho/MI ratios were 1.46 ±0.13, 0.56 ± -0.22, 0.80 ± -0.07, 0.41 ±0.09. These ratios were assumed tobe the cut-off values for the differen-tiation between malignant and non-neoplastic brain lesions. We per-formed two acquisitions in thisresearch, TE: 26 msec and 144 msec.Cho/MI ratio was obtained at shortTE acquisition, all the other ratioswere calculated at long TE applica-tion. The metabolites or the ratios ofthem were assumed to be increasedor decreased in a voxel, only if themeasurements in the mentionedpixel had been normalized with ref-erence to the contralateral normalappearing pixel, this was calculatedfor each metabolite with regard tothe healthy opposite side referencepoint.
According to H-MRS; We had 9low-grade (Grade 1-2) gliomas, alllow grade gliomas showedincreased Cho and reduced NAA res-onances, as an average Cho/NAAratio; 1.66 ± 0.35, all low-gradegliomas in this study showedincreased Cho and moderatelydecreased Cr, as an average Cho/Crratio; 2.25 ± 0.63. Low-grade glialtumours also showed moderatelyincreased MI, with an averageCho/MI ratio; 2.55 ± 0.86 which wasprecisely elevated (Table II, Fig. 1).According to Cho/Cr ratio by usingone-tailed parametrical varianceanalysis test, there was a significant
3.2 ppm, lipids (Lip) at 0.9-1.3 ppm,lactate (Lac) at 1.3-1.4 ppm , gluta-mate and glutamine (Glx) at2.45 ppm, glycine and or myo-inosi-tol (Gly-MI) at 3.6-3.75 ppm (3, 4, 6,7). Standard, optimum and sufficientbase-line correction for metaboliteswere also performed. Two doubletsinverted owing to phase modulationdue to J coupling were defined, Lacat 1.4 ppm and alanine (Ala) at1.5 ppm. At TE 144 ms, Lac can bedifferentiated from lipids with a nar-row bandwidth comparable with thepeaks of other metabolites andshows an inverted J-coupled doublepeak at 1.4 ppm (3, 4, 6). Tumour andlesion metabolite signal intensitieswere quantified, normalized byexpressing the peak area intensitiesof the metabolites especially NAA-Cho-Cr as ratios of normal brainparenchymal values to intratumoralmetabolites (NAA\Cr, NAA \ Cho), Lipand Lac which were not detectable innormal brain, were normalized usingthe contralateral reference spectrumas an internal standart (1, 3, 8). Forinstance, we compared the lesionalNAA to the lesional Cr, had thelesional NAA\Cr ratio and this wasidentical for all metabolites andratios. Contralateral reference voxelwas placed just symmetric to thecenter of the original brain lesion,however for the midline lesions;The normal reference spectra andmetabolite ratios were obtainedfrom the healthy volunteers who hadno cerebral or cerebellar abnormali-ties. 3 healthy volunteers wereincluded in this study.
All analyses were performed byusing a software program (SPSS forWindows, SPSS, Chicago-Illinois).Significance of differences betweenvarious cranial masses and non-neo-plastic lesion groups (Ischemic-demyelinating-metabolic and benigncystic mass lesions) for brainmetabolites and metabolite ratioswere tested with one-tailed paramet-ric variance analysis test, Pearsonchi-square test and difference testamong mass groups, the sensitivityand the specificity of H-MRS for allneoplastic and non-neoplasticgroup, were tested by chi-squarecross table test, p < 0.05 were con-sidered to be statistically significantdifferences.
Results
In both cranial neoplastic masslesions (Glial tumours-metastasis-menengiomas) and non neoplasticbrain disorders, including ischemic-
4 JBR–BTR, 2011, 94 (1)
aydin-hekimoglu-_Opmaak 1 9/02/11 10:10 Pagina 4
Name-age-gender
Lesion localization
MRS RESULTS
Biopsi Results
Name-age-gender Lesion localization
MRS RESULTS
T.K. 3
4 M
Right Frontal
Highgrade Glial tm
Low grade Glial tm
35-
E.E 80 F
Left tem
poral
İschem
ia
E.B 43 F
Corpus Callozum
Highgrade Glial tm
GBM
36-
K.Y. 3
7 M
Right Fronto-parietal
İschem
ia
Y.Y 43 F
Left Frontal
Highgrade Glial tm
Highgrade Glial tm
37-
N.A. 4
4 F
Left occipital
Ischem
ia
E.K. 2
2 M
4. Ven
tricule
Highgrade Glial tm
Low grade Glial tm
38-
F.Y. 24 F
Left Thalam
us
İschem
ia
L.S 40 M
Cereb
ellum
Low grade Glial tm
Low grade Glial tm
39-
M.E. 5
2 F
Left parieto-occipital
İschem
ia
B.U. 9
MLeft Pa
rietal
Low grade Glial tm
Low grade Glial tm
40-
S.A. 3
6 F
Right fronto-parietal
İschem
ia
M.P.48 F
Cereb
ellar V
ermis
Highgrade Glial tm
Low grade Glial tm
41-
C.�. 29 M
Right Occipital
İschem
ia
H.C. 5
0 F
Left Occipito-Parietal
GBM
GBM
42-
S.A. 6
0 M
Right Occipito-tem
poral
İschem
ia
H.B. 4
3 M
Bil.Cen
trumsemiovale
Highgrade Glial tm
Highgrade Glial tm
43-
M.Ö. 3
1 M
Bilat.periven
tricular
İschem
ia
C.A. 4
4 M
Right Po
st. P
arietal
Men
engioma
Extra-axial, no biopsy
44-
S.� 58 F
Right Tem
poro-occipital
İschem
ia
I.K. 7
8 M
Left Frontoparieta
Highgrade Glial tm
GBM
45-
H.B. 5
3 F
Right Occipital
İschem
ia
A.D. 6
9 M
Right Tem
poral
Highgrade Glial tm
GBM
46-
M.K. 5
6 M
Right Occipito-tem
poral
İschem
ia
A.D. 3
4 F
Right Cereb
ellar
Highgrade Glial tm
Highgrade Glial tm
47-
M.D 17 M
Left Tem
poro-occipital
İschem
ia
D.D. 3
8 F
Left Occipito-Tem
poralLo
w grade Glial tm
GBM
48-
H.U 23 F
Left Fronto-parietal
İschem
ia
G.D. 6
4 F
Left Tem
poral
Low grade Glial tm
Highgrade Glial tm
49-
A 50 F
Right Pa
rietal
İschem
ia
H.C. 4
6 M
Right Med
ial Tem
poral
Low grade Glial tm
Low grade Glial tm
50-
B.D. 4
4MLeft Frontal
İschem
ia
M.B. 5
8 M
Left Frontotemporal
Highgrade Glial tm
GBM
51-
Z.T.67 F
Right thalam
us,basal gan
glia.İschem
ia
M.S. 5
0 F
Right Frontotemporal
Low grade Glial tm
Highgrade Glial tm
52-
�A 36y,M
Right occipital
İschem
ia
M.H 42 F
Left Frontoparietal
Low grade Glial tm
Highgrade Glial tm
53-
S.T 53 F
Bilat.periven
tricular
Dem
yelin
ating le
sions
S.K. 3
6 M
Left Occipitotemporal
Highgrade Glial tm
Anap
lastik Astrositom
54-
E.B 32 F
Bilat.periven
tricular
Dem
yelin
ating le
sions.
S.K. 3
9 F
Left Pontobulbar
Highgrade Glial tm
Metastasis
55-
H.G 38 M
Bilat.periven
tricular
Dem
yelin
ating le
sions.
B.T. 4
2 M
Right Mezen
cephalon
GBM
GBM
56-
H.B 30 M
Bilat.periven
tricular
Dem
yelin
ating le
sions.
R.Ö 43 M
Left Frontoparietal
Highgrade Glial tm
Highgrade Glial tm
57-
V.T 31 M
Bilat.periven
tricular
Dem
yelin
ating le
sions
I.S.24 M
Right Tem
poral
Highgrade Glial tm
Low grade Glial tm
58-
R.Ö 32 M
Thalam
us-Midbrain
Metab
olic disease
V.K. 5
2 M
Corpus Callozum
Highgrade Glial tm
Highgrade Glial tm
59-
G.N 47 F
Right post. p
arietal
Arachnoid cyst, M
RS neg
ative.
S.T 81 F
Right Tem
poral
GBM
GBM
60-
M.D 45 F
Right param
edian
epidermoid cyst
N.Y. 2
8 F
Right Frontoparietal
Men
engioma
Extra-axial, n
o biopsy.
61-
C.Ö 65 F
Cereb
ellum
Cavernoma.
M.G. 4
3 M
Left Frontoparietal
Highgrade Glial tm
GBM
62-
C.E 72 M
Right Frontal
Arachnoid cyst, M
RS neg
ative.
A.A. 6
0 M
Corpus Callozum
No m
ass effect.
Highgrade Glial tm
63-
H.Ö. 3
0 F
Right Occipital
Neu
roep
ithelial cyst, M
RS neg
ative
A.Ö. 3
3 F
Left Pontobulbar
Low grade Glial tm
Low grade Glial tm
H.B. 8
5 F
Left Tem
poro-oksipital
GBM
GBM
Ö.D. 3
8 F
Left Tem
poro-oksipital
GBM
GBM
S.Ü. 5
2 F
Left Frontal L
ow grade
Glial tm
Low grade Glial tm
NEOPLASTIC MASS GROUP
NON-NEOPLASTIC MASS GROUP.
Table I. —
List of patients.
aydin-hekimoglu-_Opmaak 1 9/02/11 10:10 Pagina 5
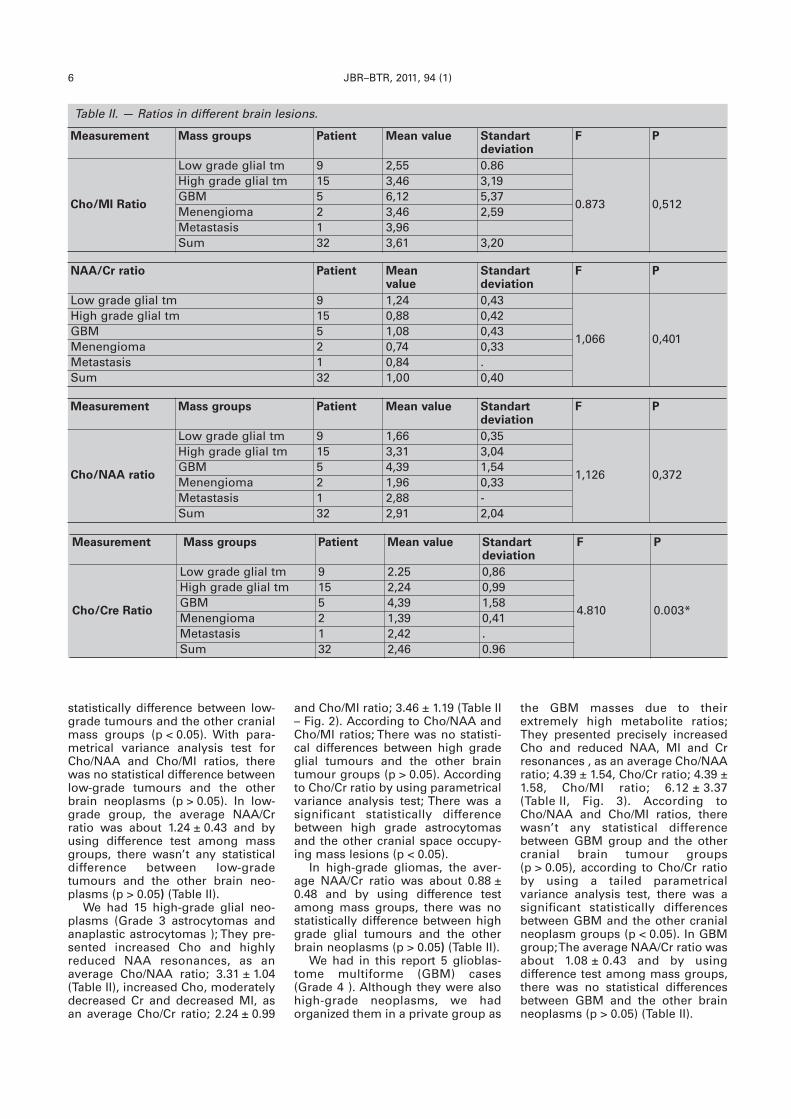
statistically difference between low-grade tumours and the other cranialmass groups (p < 0.05). With para-metrical variance analysis test forCho/NAA and Cho/MI ratios, therewas no statistical difference betweenlow-grade tumours and the otherbrain neoplasms (p > 0.05). In low-grade group, the average NAA/Crratio was about 1.24 ± 0.43 and byusing difference test among massgroups, there wasn’t any statisticaldifference between low-gradetumours and the other brain neo-plasms (p > 0.05) (Table II).
We had 15 high-grade glial neo-plasms (Grade 3 astrocytomas andanaplastic astrocytomas ); They pre-sented increased Cho and highlyreduced NAA resonances, as anaverage Cho/NAA ratio; 3.31 ± 1.04(Table II), increased Cho, moderatelydecreased Cr and decreased MI, asan average Cho/Cr ratio; 2.24 ± 0.99
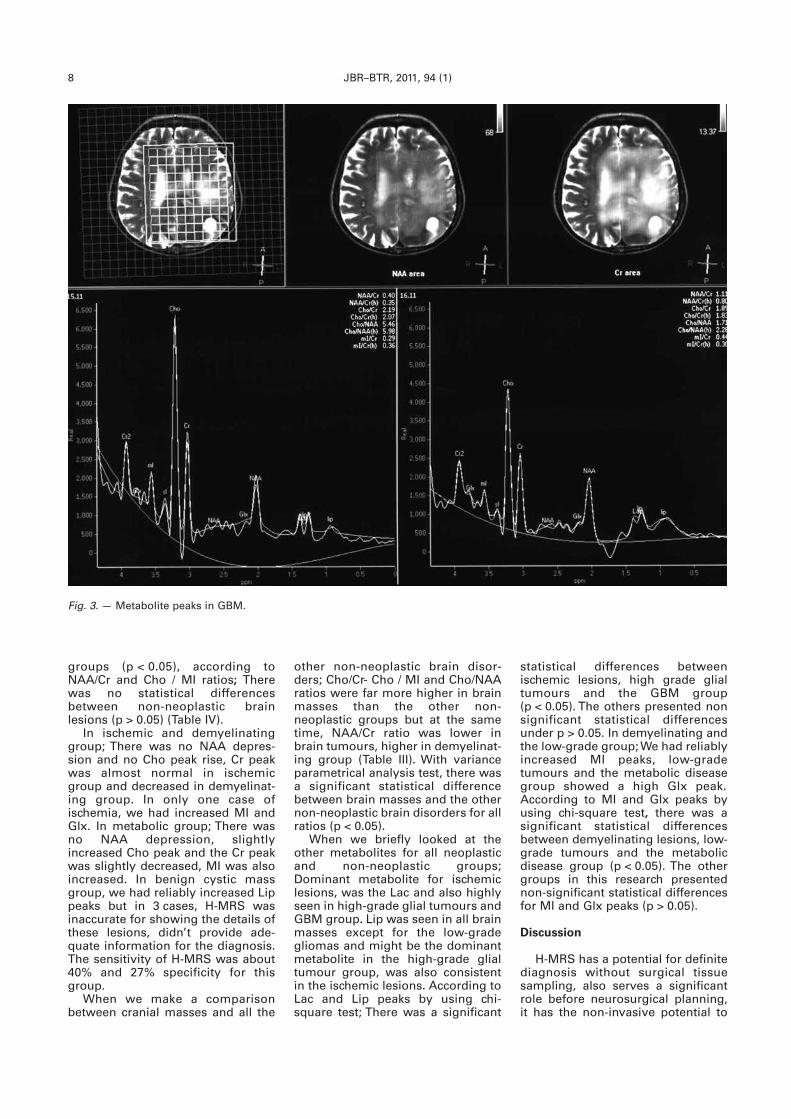
the GBM masses due to theirextremely high metabolite ratios;They presented precisely increasedCho and reduced NAA, MI and Crresonances , as an average Cho/NAAratio; 4.39 ± 1.54, Cho/Cr ratio; 4.39 ±1.58, Cho/MI ratio; 6.12 ± 3.37(Table II, Fig. 3). According toCho/NAA and Cho/MI ratios, therewasn’t any statistical differencebetween GBM group and the othercranial brain tumour groups(p > 0.05), according to Cho/Cr ratioby using a tailed parametrical variance analysis test, there was asignificant statistically differencesbetween GBM and the other cranialneoplasm groups (p < 0.05). In GBMgroup; The average NAA/Cr ratio wasabout 1.08 ± 0.43 and by using difference test among mass groups,there was no statistical differencesbetween GBM and the other brainneoplasms (p > 0.05) (Table II).
and Cho/MI ratio; 3.46 ± 1.19 (Table II– Fig. 2). According to Cho/NAA andCho/MI ratios; There was no statisti-cal differences between high gradeglial tumours and the other braintumour groups (p > 0.05). Accordingto Cho/Cr ratio by using parametricalvariance analysis test; There was asignificant statistically differencebetween high grade astrocytomasand the other cranial space occupy-ing mass lesions (p < 0.05).
In high-grade gliomas, the aver-age NAA/Cr ratio was about 0.88 ±0.48 and by using difference testamong mass groups, there was nostatistically difference between highgrade glial tumours and the otherbrain neoplasms (p > 0.05) (Table II).
We had in this report 5 glioblas-tome multiforme (GBM) cases(Grade 4 ). Although they were alsohigh-grade neoplasms, we hadorganized them in a private group as
6 JBR–BTR, 2011, 94 (1)
Table II. — Ratios in different brain lesions.
Measurement Mass groups Patient Mean value Standartdeviation
F P
Cho/MI Ratio
Low grade glial tm 9 2,55 0.86
0.873 0,512
High grade glial tm 15 3,46 3,19GBM 5 6,12 5,37Menengioma 2 3,46 2,59Metastasis 1 3,96Sum 32 3,61 3,20
Measurement Mass groups Patient Mean value Standartdeviation
F P
Cho/NAA ratio
Low grade glial tm 9 1,66 0,35
1,126 0,372
High grade glial tm 15 3,31 3,04GBM 5 4,39 1,54Menengioma 2 1,96 0,33Metastasis 1 2,88 -Sum 32 2,91 2,04
Measurement Mass groups Patient Mean value Standartdeviation
F P
Cho/Cre Ratio
Low grade glial tm 9 2.25 0,86
4.810 0.003*
High grade glial tm 15 2,24 0,99GBM 5 4,39 1,58Menengioma 2 1,39 0,41Metastasis 1 2,42 .Sum 32 2,46 0.96
NAA/Cr ratio Patient Meanvalue
Standartdeviation
F P
Low grade glial tm 9 1,24 0,43
1,066 0,401
High grade glial tm 15 0,88 0,42GBM 5 1,08 0,43Menengioma 2 0,74 0,33Metastasis 1 0,84 .Sum 32 1,00 0,40
aydin-hekimoglu-_Opmaak 1 9/02/11 10:10 Pagina 6
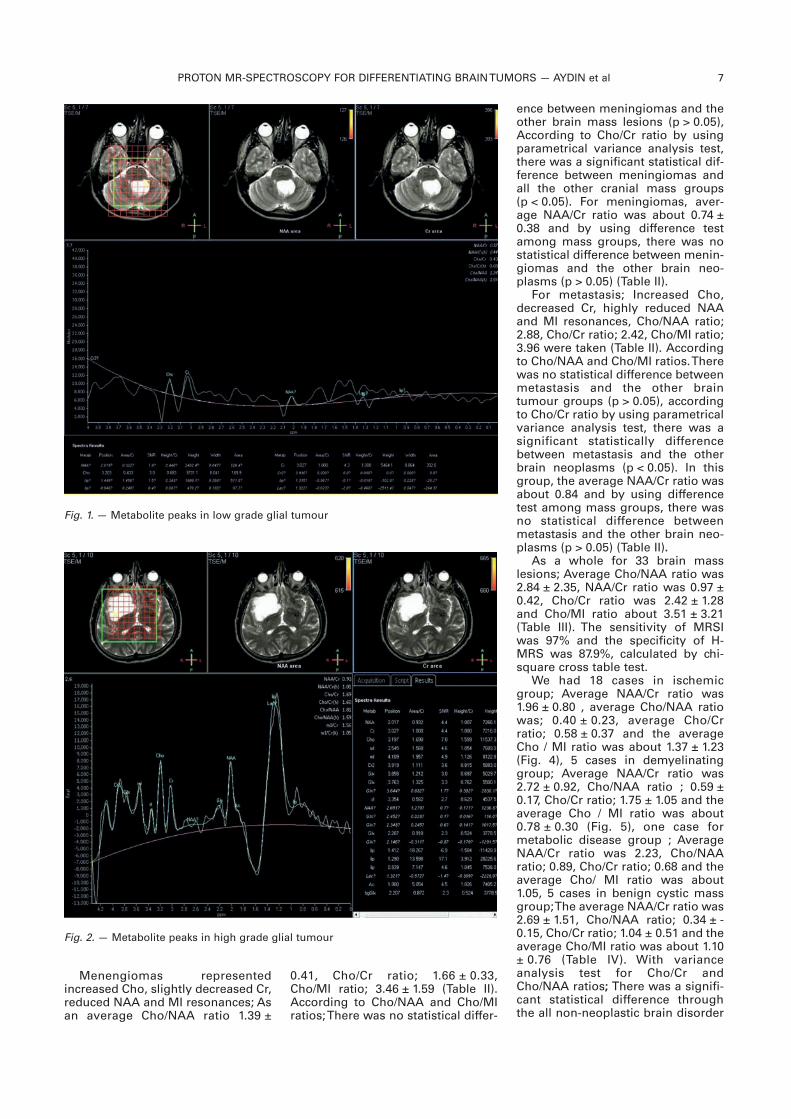
Menengiomas representedincreased Cho, slightly decreased Cr,reduced NAA and MI resonances; Asan average Cho/NAA ratio 1.39 ±
ence between meningiomas and theother brain mass lesions (p > 0.05),According to Cho/Cr ratio by usingparametrical variance analysis test,there was a significant statistical dif-ference between meningiomas andall the other cranial mass groups(p < 0.05). For meningiomas, aver-age NAA/Cr ratio was about 0.74 ±0.38 and by using difference testamong mass groups, there was nostatistical difference between menin-giomas and the other brain neo-plasms (p > 0.05) (Table II).For metastasis; Increased Cho,
decreased Cr, highly reduced NAAand MI resonances, Cho/NAA ratio;2.88, Cho/Cr ratio; 2.42, Cho/MI ratio;3.96 were taken (Table II). Accordingto Cho/NAA and Cho/MI ratios. Therewas no statistical difference betweenmetastasis and the other braintumour groups (p > 0.05), accordingto Cho/Cr ratio by using parametricalvariance analysis test, there was asignificant statistically differencebetween metastasis and the otherbrain neoplasms (p < 0.05). In thisgroup, the average NAA/Cr ratio wasabout 0.84 and by using differencetest among mass groups, there wasno statistical difference betweenmetastasis and the other brain neo-plasms (p > 0.05) (Table II).As a whole for 33 brain mass
lesions; Average Cho/NAA ratio was2.84 ± 2.35, NAA/Cr ratio was 0.97 ±0.42, Cho/Cr ratio was 2.42 ± 1.28and Cho/MI ratio about 3.51 ± 3.21(Table III). The sensitivity of MRSIwas 97% and the specificity of H-MRS was 87.9%, calculated by chi-square cross table test. We had 18 cases in ischemic
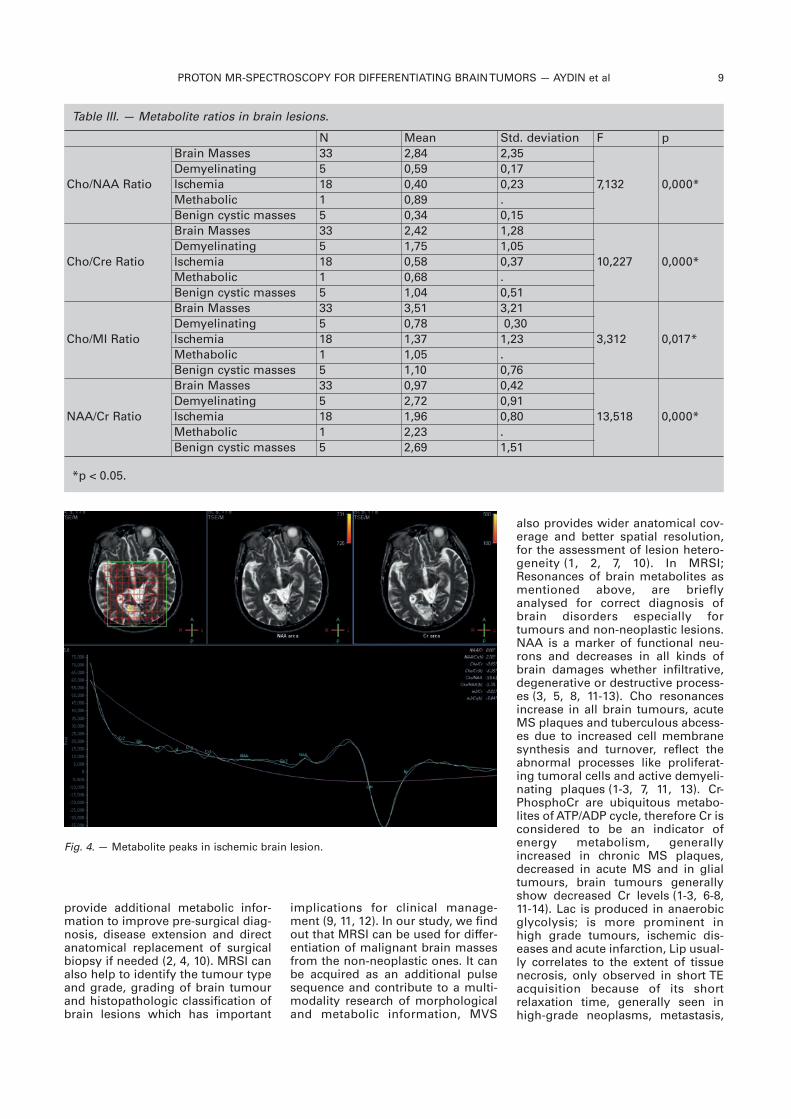
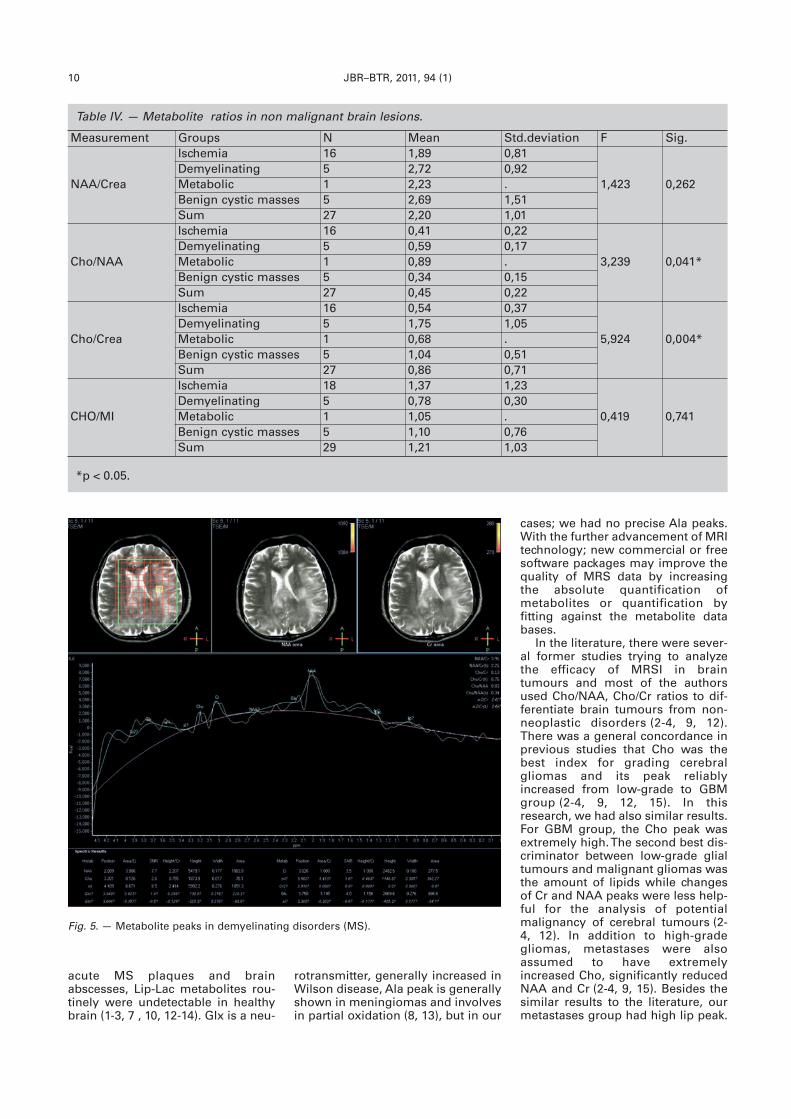
group; Average NAA/Cr ratio was1.96 ± 0.80 , average Cho/NAA ratiowas; 0.40 ± 0.23, average Cho/Crratio; 0.58 ± 0.37 and the averageCho / MI ratio was about 1.37 ± 1.23(Fig. 4), 5 cases in demyelinatinggroup; Average NAA/Cr ratio was2.72 ± 0.92, Cho/NAA ratio ; 0.59 ±0.17, Cho/Cr ratio; 1.75 ± 1.05 and theaverage Cho / MI ratio was about0.78 ± 0.30 (Fig. 5), one case formetabolic disease group ; AverageNAA/Cr ratio was 2.23, Cho/NAAratio; 0.89, Cho/Cr ratio; 0.68 and theaverage Cho/ MI ratio was about1.05, 5 cases in benign cystic massgroup; The average NAA/Cr ratio was2.69 ± 1.51, Cho/NAA ratio; 0.34 ± -0.15, Cho/Cr ratio; 1.04 ± 0.51 and theaverage Cho/MI ratio was about 1.10± 0.76 (Table IV). With varianceanalysis test for Cho/Cr andCho/NAA ratios; There was a signifi-cant statistical difference throughthe all non-neoplastic brain disorder
0.41, Cho/Cr ratio; 1.66 ± 0.33,Cho/MI ratio; 3.46 ± 1.59 (Table II).According to Cho/NAA and Cho/MIratios; There was no statistical differ-
PROTON MR-SPECTROSCOPY FOR DIFFERENTIATING BRAIN TUMORS — AYDIN et al 7
Fig. 1. — Metabolite peaks in low grade glial tumour
Fig. 2. — Metabolite peaks in high grade glial tumour
aydin-hekimoglu-_Opmaak 1 16/02/11 08:44 Pagina 7
groups (p < 0.05), according toNAA/Cr and Cho / MI ratios; Therewas no statistical differencesbetween non-neoplastic brainlesions (p > 0.05) (Table IV).
In ischemic and demyelinatinggroup; There was no NAA depres-sion and no Cho peak rise, Cr peakwas almost normal in ischemicgroup and decreased in demyelinat-ing group. In only one case ofischemia, we had increased MI andGlx. In metabolic group; There wasno NAA depression, slightlyincreased Cho peak and the Cr peakwas slightly decreased, MI was alsoincreased. In benign cystic massgroup, we had reliably increased Lippeaks but in 3 cases, H-MRS wasinaccurate for showing the details ofthese lesions, didn’t provide ade-quate information for the diagnosis.The sensitivity of H-MRS was about40% and 27% specificity for thisgroup.
When we make a comparisonbetween cranial masses and all the
statistical differences betweenischemic lesions, high grade glialtumours and the GBM group(p < 0.05). The others presented nonsignificant statistical differencesunder p > 0.05. In demyelinating andthe low-grade group; We had reliablyincreased MI peaks, low-gradetumours and the metabolic diseasegroup showed a high Glx peak.According to MI and Glx peaks byusing chi-square test, there was asignificant statistical differencesbetween demyelinating lesions, low-grade tumours and the metabolicdisease group (p < 0.05). The othergroups in this research presentednon-significant statistical differencesfor MI and Glx peaks (p > 0.05).
Discussion
H-MRS has a potential for definitediagnosis without surgical tissuesampling, also serves a significantrole before neurosurgical planning,it has the non-invasive potential to
other non-neoplastic brain disor-ders; Cho/Cr- Cho / MI and Cho/NAAratios were far more higher in brainmasses than the other non- neoplastic groups but at the sametime, NAA/Cr ratio was lower inbrain tumours, higher in demyelinat-ing group (Table III). With varianceparametrical analysis test, there wasa significant statistical differencebetween brain masses and the othernon-neoplastic brain disorders for allratios (p < 0.05).
When we briefly looked at theother metabolites for all neoplasticand non-neoplastic groups;Dominant metabolite for ischemiclesions, was the Lac and also highlyseen in high-grade glial tumours andGBM group. Lip was seen in all brainmasses except for the low-gradegliomas and might be the dominantmetabolite in the high-grade glialtumour group, was also consistentin the ischemic lesions. According toLac and Lip peaks by using chi-square test; There was a significant
8 JBR–BTR, 2011, 94 (1)
Fig. 3. — Metabolite peaks in GBM.
aydin-hekimoglu-_Opmaak 1 9/02/11 10:10 Pagina 8
provide additional metabolic infor-mation to improve pre-surgical diag-nosis, disease extension and directanatomical replacement of surgicalbiopsy if needed (2, 4, 10). MRSI canalso help to identify the tumour typeand grade, grading of brain tumourand histopathologic classification ofbrain lesions which has important
also provides wider anatomical cov-erage and better spatial resolution,for the assessment of lesion hetero-geneity (1, 2, 7, 10). In MRSI;Resonances of brain metabolites asmentioned above, are brieflyanalysed for correct diagnosis ofbrain disorders especially fortumours and non-neoplastic lesions.NAA is a marker of functional neu-rons and decreases in all kinds ofbrain damages whether infiltrative,degenerative or destructive process-es (3, 5, 8, 11-13). Cho resonancesincrease in all brain tumours, acuteMS plaques and tuberculous abcess-es due to increased cell membranesynthesis and turnover, reflect theabnormal processes like proliferat-ing tumoral cells and active demyeli-nating plaques (1-3, 7, 11, 13). Cr-PhosphoCr are ubiquitous metabo-lites of ATP/ADP cycle, therefore Cr isconsidered to be an indicator ofenergy metabolism, generallyincreased in chronic MS plaques,decreased in acute MS and in glialtumours, brain tumours generallyshow decreased Cr levels (1-3, 6-8,11-14). Lac is produced in anaerobicglycolysis; is more prominent inhigh grade tumours, ischemic dis-eases and acute infarction, Lip usual-ly correlates to the extent of tissuenecrosis, only observed in short TEacquisition because of its shortrelaxation time, generally seen inhigh-grade neoplasms, metastasis,
implications for clinical manage-ment (9, 11, 12). In our study, we findout that MRSI can be used for differ-entiation of malignant brain massesfrom the non-neoplastic ones. It canbe acquired as an additional pulsesequence and contribute to a multi-modality research of morphologicaland metabolic information, MVS
PROTON MR-SPECTROSCOPY FOR DIFFERENTIATING BRAIN TUMORS — AYDIN et al 9
Table III. — Metabolite ratios in brain lesions.
*p < 0.05.
N Mean Std. deviation F p
Cho/NAA Ratio
Brain Masses 33 2,84 2,35
7,132 0,000*Demyelinating 5 0,59 0,17Ischemia 18 0,40 0,23Methabolic 1 0,89 .Benign cystic masses 5 0,34 0,15
Cho/Cre Ratio
Brain Masses 33 2,42 1,28
10,227 0,000* Demyelinating 5 1,75 1,05 Ischemia 18 0,58 0,37Methabolic 1 0,68 .Benign cystic masses 5 1,04 0,51
Cho/MI Ratio
Brain Masses 33 3,51 3,21
3,312 0,017* Demyelinating 5 0,78 0,30 Ischemia 18 1,37 1,23Methabolic 1 1,05 .Benign cystic masses 5 1,10 0,76
NAA/Cr Ratio
Brain Masses 33 0,97 0,42
13,518 0,000* Demyelinating 5 2,72 0,91 Ischemia 18 1,96 0,80Methabolic 1 2,23 .Benign cystic masses 5 2,69 1,51
Fig. 4. — Metabolite peaks in ischemic brain lesion.
aydin-hekimoglu-_Opmaak 1 9/02/11 10:10 Pagina 9
acute MS plaques and brainabscesses, Lip-Lac metabolites rou-tinely were undetectable in healthybrain (1-3, 7 , 10, 12-14). Glx is a neu-
cases; we had no precise Ala peaks.With the further advancement of MRItechnology; new commercial or freesoftware packages may improve thequality of MRS data by increasingthe absolute quantification ofmetabolites or quantification by fitting against the metabolite databases.
In the literature, there were sever-al former studies trying to analyzethe efficacy of MRSI in braintumours and most of the authorsused Cho/NAA, Cho/Cr ratios to dif-ferentiate brain tumours from non-neoplastic disorders (2-4, 9, 12).There was a general concordance inprevious studies that Cho was thebest index for grading cerebralgliomas and its peak reliablyincreased from low-grade to GBMgroup (2-4, 9, 12, 15). In thisresearch, we had also similar results.For GBM group, the Cho peak wasextremely high. The second best dis-criminator between low-grade glialtumours and malignant gliomas wasthe amount of lipids while changesof Cr and NAA peaks were less help-ful for the analysis of potentialmalignancy of cerebral tumours (2-4, 12). In addition to high-gradegliomas, metastases were alsoassumed to have extremelyincreased Cho, significantly reducedNAA and Cr (2-4, 9, 15). Besides thesimilar results to the literature, ourmetastases group had high lip peak.
rotransmitter, generally increased inWilson disease, Ala peak is generallyshown in meningiomas and involvesin partial oxidation (8, 13), but in our
10 JBR–BTR, 2011, 94 (1)
Table IV. — Metabolite ratios in non malignant brain lesions.
*p < 0.05.
Measurement Groups N Mean Std.deviation F Sig.
NAA/Crea
Ischemia 16 1,89 0,81
1,423 0,262Demyelinating 5 2,72 0,92Metabolic 1 2,23 .Benign cystic masses 5 2,69 1,51Sum 27 2,20 1,01
Cho/NAA
Ischemia 16 0,41 0,22
3,239 0,041*Demyelinating 5 0,59 0,17Metabolic 1 0,89 .Benign cystic masses 5 0,34 0,15Sum 27 0,45 0,22
Cho/Crea
Ischemia 16 0,54 0,37
5,924 0,004*Demyelinating 5 1,75 1,05Metabolic 1 0,68 .Benign cystic masses 5 1,04 0,51Sum 27 0,86 0,71
CHO/MI
Ischemia 18 1,37 1,23
0,419 0,741Demyelinating 5 0,78 0,30Metabolic 1 1,05 .Benign cystic masses 5 1,10 0,76Sum 29 1,21 1,03
Fig. 5. — Metabolite peaks in demyelinating disorders (MS).
aydin-hekimoglu-_Opmaak 1 9/02/11 10:10 Pagina 10

In the benign cystic cranial massesof non-neoplastic group, we hadalso strong lipid resonances.
MR-Spectroscopy has also animportant diagnostic role, especiallywhen it reveals reduced NAA with-out increased Cho, in theseinstances MRS findings may sparethe patient from biopsy (4, 16, 17).Cho/NAA, Cho/Cr ratios were thevaluable tools for determining themalignancy of cranial neoplasms,used by most of the authors (3-5, 9-12, 15). In most of the former stud-ies, both ratios increased from low-grade to high-grade gliomas, alsoextremely higher in metastases andPrimitive neuroectodermal tumours(PNET) (3, 5, 8, 9, 11, 15). In thisresearch, Cho/Cr ratio more than 2.5was presented as malignant (p <0.05) . We had no PNET type tumourbut both ratios were similarlyincreased in low-high grade glialtumours and in metastases. In ourstudy, the lowest Cho/Cr ratio amongthe other brain masses was present-ed in meningiomas. In this group, wehad strong elevation of Cho reso-nance but contrary to literature, therewas no precise Cr decrease andCho/Cr ratio was the lowest in menin-giomas, we didn’t see any Ala reso-nance for both meningiomas.
We tried to make another varia-tion by using Cho/MI ratio in order tocategorize tumours according totheir potential malignancy and triedto differentiate malignant cranialmasses from non-neoplastic disor-ders which were not frequently seenin the past former studies. Amongthese masses; Cho/MI ratio was thehighest in GBM and lowest in Low-grade glial tumours. It was alsoextremely high in higher-gradegliomas and metastasis groups. Incranial mass groups; We had anaverage Cho/MI ratio about 3.51,therefore we could easily concludethat increased ratio was stronglyrelated with malignancy of thetumours. In non-neoplastic group;The highest Cho/MI ratio was inischemic group, about 1.37. Withthese datas, one could easily con-clude that Cho/MI ratio more than 3was most likely to be malignantrather than benign (p < 0.05). In ourresearch, Cho/MI ratio was really adiagnostic tool for grading gliomas,categorizing the tumours accordingto their malignancy rates and differ-entiation from non-neoplasticlesions.
The primary results of our studypresented that MR-Spectroscopyhad a good sensitivity and specifici-ty among the non-neoplastic brain
ders and differentiation of themfrom the brain tumours based on theNAA/Cr, Cho/ NAA ratios (1, 2, 4, 7,10). NAA/Cr ratio more than 2 waspresented as non-malignant (p <0.05) and elevated NAA/Cr ratio washighly specific for the demyelinatingdiseases (2, 4, 7, 17). In our experi-ence; NAA/Cr ratio was the highestin demyelinating group and the low-est in brain masses. Cho/NAA ratioabove 1.5 was assumed to be malig-nant in the previous former stud-ies (2-6, 13, 15). In our paper, thenon-neoplastic group had preciselylower Cho/NAA ratio than the cranialmass groups. To our belief, Cho/NAAratio above 2 mostly focused tomalignancy (p < 0.05). Some casesof demyelinating lesions were pre-sented as mimicking high-gradegliomas because of histopathologicsimilarities which include hypercel-lularity-reactive astrocytes-mitoticand necrotic areas (1, 4, 17), we didn’t have such misclassified casesin our report. As a whole; This studyprovided that increased Cho/NAA,Cho/MI and Cho/Cr ratios withdecreased NAA/Cr ratio should easi-ly be used in the differentiation ofmalignant ones from the non- neoplastic brain lesions and couldaid to the relevant literature with thisaspect.
Conclusion
As a summary, a brain lesion withhigher Cho/NAA, Cho/Cr and Cho/MIratio plus lower NAA/Cr ratio wasmost likely to be malignant.Additionally, lip and lac peaks werealso frequently seen in more malig-nant lesions. A higher MI peak generally presented low-grade malig-nancy or a non-neoplastic disorderespecially demyelinating lesions.
Acknowledgements
We thank Mr.Egemen Alper andErdeniz Yurdakul for their brief assis-tance in handling of those all MRSIprocedures and also we are so grate-ful to the Schering-Germany for theirfinancial supports.
References
1. Mader I., Rauer S., Gall P., Klose U.:H-MR spectroscopy of inflammation,infection and ischemia of te brain. EurJ Radiol 2008, 67: 250-257.
2. Majos C., Aguilera C., Alonso J.,Sape J.M., Castaner S., Sanchez J.J.,et al.: Proton-MR spectroscopyimproves Discrimination betweentumour and pseudo-tumoral lesion in
disorders except for the cystic cra-nial masses, Perfusion MR andDiffusion Weighted MR imagingcould also be added to MRS findingsin order to get more beneficialresults (2, 4, 7, 10, 16). When we lookat the literature; Elevated Cho levelsand reduced NAA levels had beenreported in acute MS plaques andhad been explained by reactiveastrogliosis, inflammation and earlyaxonal degeneration, MI at short TEwas also a discriminating metabolitefor the acute MS and also increasedin cases of glial activation or gliosis,represented dominancy in low-gradeastrocytomas related to abnormalastrocyte proliferation, neverthelessmight also be seen in Encephalitis,Dementia, Epilepsy and SSPE-PMLlike brain disorders (1, 7, 10, 13, 14),but in high grade gliomas, metas-tases and more malignant tumours,its peak sharply declined (1, 2, 4, 15,17). In our study, we had also elevat-ed MI peaks in non-neoplasticdemyelinating group. According toprevious studies, there was no sig-nificant difference in the level of Cramong the non-neoplastic brainlesions (1, 4, 17). In our series, Crpeak was strongly decreased indemyelinating group. Infarctions asmentioned in the literature showincreased Lac, progressive Choreduction in the chronic phase andalso increased NAA peak especiallyin acute and subacute phases (1, 7,10). In our ischemic group, Lac wasalso the dominant metabolite. Glxpeak was the highest in the metabol-ic group. In the non-neoplasticgroup, Cho peak was highest inmetabolic group and Cr was strong-ly decreased at the demyelinatinggroup. NAA/Cr ratio was also higherin demyelinating group. In the differ-entiation of low-grade group fromthe non-neoplastic disorders; Mostof the authors considered the Chopeak and Cho/NAA, Cho/Cr ratios asthe reference standards, they mostlymade the discrimination by the elevated Cho/NAA, Cho/Cr ratios andhigh Cho peak in the selected vox-els (2-4, 9, 12, 13). In our paper withcorrespondence to these ratios, low-grade group had significantly higherresults than the non-neoplastic brainlesions as seen in the former studies,at the same time we also used theCho/MI ratio for the differentiation ofboth groups and although this ratiowas lowest in low-grade groupthrough the other neoplastic massgroups, was certainly higher thanthe non-neoplastic group.
In the previous researches, evalu-ation of non-neoplastic brain disor-
PROTON MR-SPECTROSCOPY FOR DIFFERENTIATING BRAIN TUMORS — AYDIN et al 11
aydin-hekimoglu-_Opmaak 1 9/02/11 10:10 Pagina 11

solid brain masses. AJNR, 2009, 30:544-551.
3. Hartmann W., Herminghaus S.,Krings T., Marquardt G.,Lanfermann H., Pilatus U., et al.:Clinical application of proton magnet-ic resonance spectroscopy in thediagnosis of intracranial masslesions. Neuroradiology 2002, 44:371-381.
4. Hourani R., Brant L.J., Rizk T.,Weingart J.D., Barker P.B., Horska A.,et al.: Can Proton MR Spectroscopicand Perfusion imaging differentiatebetween neoplastic and non-neoplas-tic brain lesions in adults? AJNR2008, 29: 366-372.
5. Poptani H., Gupta R., Roy R.,Pandey R., Jain V.K., Chhabra D.K.:Characterization of Intracranial masslesions with in vivo Proton MRSpectroscopy. AJNR 1995, 16: 1593-1603.
6. Sibtain N.A., Howe F.A.,Saunders D.E.: The clinical value ofproton magnetic resonance spec-troscopy in adult brain tumours. ClinRadiol, 2007, 62: 109-119.
7. Papanagiotou P., Grunwald I.Q.,Farmakis G., Hartmann K.M.,Politi M., Roth C., et al.: MR-
brain: Utility in clinic al setting-initialresults. Eur J Radiol, 2005, 55: 401-408.
13. Papanagiotou P., Backens M.,Grunwald I.Q., Farmakis G., Politi M.,Roth C., et al.: MR-Spektroskopie beiHirntumoren. Radiologe, 2007, 47:520-529.
14. Faria A.V., Reis F., Zanardi V.,Menezes J.R., Cendes F.: The patternof Proton-Magnetic resonanceSpectro scopy in non-neoplasticEncephalic lesions. Arq Neuro -psiquiatr, 2004, 62(2b): 429-436.
15. Venkatesh S.K., Gupta R.K., Pal L.,Husain N., Husain M.: Spectroscopicincrease in choline signal, is a non-specific marker for differentiation ofinfective-inflammatory from neoplas-tic lesions of the brain. J Magn ResonImaging, 2001, 14: 8-15.
16. Lai P.H., Hsu S.S., Ding S.W., Ko C.W.,Fu J.H., Weng M.J., et al.: Proton mag-netic resonance spectroscopy anddiffusion-weighted imaging inintracranial cystic mass lesions. SurgNeurol, 2007, 68: 25-36.
17. Narayana P.A.: Magnetic resonanceSpectroscopy in the monitoring ofMultipl Sclerosis. J Neuroimaging,2005, 15: 46-57.
Spektroskopie bei entzündlichenHirnerkrankungen. Radiologe, 2008,48: 582-587.
8. Callot V., Galanaud D., Le Fur Y.,Gouny S.C., Ranjeva J.P., Cozzone P.J.:H-MR spectroscopy of human braintumours , A practical approach. Eur JRadiol, 2008, 67: 268-274.
9. Majos C., Alonso J., Aguilera C.,Serrallonga M., Martin J.P.,Acebes J.J., et al.: Proton magneticresonance of human brain tumours,Assessment of differences betweentumour types and its applicability inbrain tumour categorization. EurRadiol, 2003, 13: 582-591.
10. Nagar V.A., Ye J., Xu M., Ng W.H.,Yeo T.T., Ong P.L., et al.: Multi-voxelMR Spectroscopic Imaging-Distinguishing Intracranial Tumoursfrom Non-neoplastic Diseases. AnnAcad Med Singapore, 2007, 36: 309-313.
11. Magalhaes A., Godfrey W., Shen Y.,Hu J., Smith W.: Proton magnetic res-onance Spectroscopy of brainTumours correlated with pathology.Acad Radiol, 2005, 12: 51-57.
12. Parmar H., Lim T.C., Yin H., Chua V.,Khin LW., Raidy T., et al.: Multi-voxelMR Spectroscopic imaging of the
12 JBR–BTR, 2011, 94 (1)
Our selection of new radiology titles!
Clinical Ultrasound 3/e Two-Volume SetWeston, Baxter, Allan Elsevier – 1672 pp – February 2011 € 277,20
Diagnostic Ultrasound 4/e Two Volume SetRumack Mosby – 2192 pp – January 2011 € 298,30
Diagnostic Imaging: Spine 2/eRoss J.S., Crim J. LWW/Amirsys – 1000 pp – November 2010 € 294,40
Critical Care RadiologySchaefer-Prokop C.M. Thieme Verlag – 236 pp – February 2011 € 119,95
Cardiovascular Imaging 2-Volume SetHo V., Reddy G.P. WB Saunders – 2160 pp – December 2010 € 254,90
ACCO Leuven ACCO Adrénaline ACCO GentM-Theresiastraat 2 43, Rue Martin V St-Pietersnieuwstr. 1053000 Leuven 1200 Bruxelles 9000 GentTel 016/29.11.00 Tel 02/763.16.86 Tel 09/235.73.00Fax 016/20.73.89 Fax 02/772.10.04 Fax 09/235.73.01
aydin-hekimoglu-_Opmaak 1 16/02/11 09:07 Pagina 12

Case report
A 3year-old previously healthy girlwas referred to the emergencydepartment with a 2-day history ofincreasing dyspnoea and drowsi-ness. Laboratory investigationsrevealed an elevated white cell countof 20cells/mm3, with normal haemo-globin and platelet levels. ESR waselevated at 110 mm/hour. A chest x-ray revealed extensive opacificationof the right hemithorax with minimalaerated lung in the right apex. Therewas marked mediastinal shift to theleft and patchy left lower lobe con-solidation. There was also a small airpocket projected to the right of themidline which was suggested to be apnuematocoele (Fig. 1). An ultra-sound of her chest revealed that theright lung was abnormally echogenicwith multiple fluid-filled cysticspaces and was surrounded by alarge collection of septated fluidwhich suggesting empyema (Fig. 2).The diagnosis of underlying lungabscess was proposed. A subse-quent Computed Tomography (CT)thorax was performed (Fig. 3) whichconfirmed mediastinal shift to theleft, with a thick rind of peripul-monary fluid. Furthermore, the rightlower lobe parenchyma appearedabnormal with a mixed solid andcystic appearance. The patient wasreferred for thoracotomy, with ahistopathological diagnosis ofpleuro pulmonary blastoma.
Discussion
Pulmonary blastoma is a rareaggressive neoplasm which usuallypresents as a well-defined lunglesion or pleural effusion and
WDFA usually affects adults witha history of smoking and may bemistaken for bronchogenic carcino-ma. Pleuropulmonary blastoma is adistinct tumour of childhood and canbe classified into three subtypesdepending on the histologicalappearance. Type I is a purely cystictumour, type II has mixed solid andcystic components and type III is asolid tumour (2). There have beenreports of a better prognosis associ-ated with type I disease in compari-son with Types II and III, however thishas not proven to be statistically sig-nificant and may be due to the lackof data and the rarity of this tumour.
On CT, PPB appears as a mixedsolid and cystic lesion with a necrot-ic centre and variable contrastenhancement, or a persistent pleuraleffusion and can cause completeopacification of a hemithorax, withco-existing mediastinal shift.Differential diagnosis depends onthe presentation, however, condi-tions such as congenital cystic ade-nomatoid malformation (CCAM)
accounts for 0.25-0.5% of lungmalignancies. These tumours arecomposed of malignant immatureepithelial or mesenchymal cellswhich may bear a resemblance toearly embryological lung tissue.They can be classified into three sub-groups: Classic pulmonary blastoma(PB), well-differentiated fetal adeno-carcinoma (WDFA) and pleuropul-monary blastoma (PPB) (1).
Classic pulmonary blastoma is themost common subtype and oftenpresents with non-specific respirato-ry symptoms with two peak age inci-dences in the first and fourthdecades of life. Chest x-rays reveal asolitary lung mass or nodule, how-ever 40% may be diagnosed coinci-dentally.
JBR–BTR, 2011, 94: 13-14.
PLEUROPULMONARY BLASTOMA PRESENTING AS A COMPLICATEDPLEURAL EFFUSIONJ. O’Brien, D. Rea, R. Hayes1
Pleuropulmonary blastoma (PPB) is a rare tumour of mesenchymal cells. We present a case of PPB in a child, whichpresented to the emergency department with an extensive pleural effusion. We discuss the radiological features,pathology, classification and treatment of this condition. This case reiterates the importance of considering this diagnosis prior to surgical intervention, to improve the long term prognosis of this aggressive disease.
Key-word: Blastoma.
From: 1. Dept. of Radiology, Our Lady’s Hospital for Sick Children, Crumlin, Dublin,Ireland.Address for correspondence: Dr J. O’Brien, M.D., Dept. of Radiology, Our Lady’sHospital for Sick Children, Dublin, Ireland. E-mail: [email protected]
Fig. 1. — Chest X-ray demonstrating extensive opacification ofthe right hemithorax with marked mediastinal shift to the leftand patchy left lower lobe consolidation. There was an area ofaerated lung at the right apex and also a small air pocket projected to the right of the midline.
o'brien-_Opmaak 1 9/02/11 10:18 Pagina 13

should also be considered and it canbe difficult to distinguish this fromPPB type I (3). It is also important tonote that, these lesions can oftenarise in association with congenitallung lesions such as the previouslymentioned CCAM (4). In the case ofan opaque hemi-thorax with an asso-ciated rib lesion, considerationshould also be given to lymphoma orEwing’s sarcoma. There are no specif-ic genetic markers yet identifieddespite extensive investigation (5),however 25% cases are associatedwith familial malignancies includingsarcomas, medulloblastomas, lym-phoma, leukaemia and PPB.
Patients are often commenced ontreatment for an empyema with apoor response.
Surgery is the mainstay of treat-ment, with a combination of
two atypical cases and review of theliterature. BJR, 2005, 78: 437-440.
2. Priest J.R., McDermott M.B.,Bhatia S., Watterson J., Mannivel J.C.,Dehner L.P.: Pleuropulmonary blastoma: a clinicopathologic studyof 50 cases. Cancer, 1997, 80 (1): 147-161.
3. Orazi C., Inserra A., Schingo PM., DeSio L., Cutrera R., Boldrini R.,Malena S.: Pleuropulmonary blas-toma, a distinctive neoplasm of child-hood: report of three cases. PediatrRadiol, 2007, 37: 337-344.
4. Naffaa L., Donnelly L.: Imaging findings in pleuropulmonary blastoma. Pediatr Radiol, 2005, 35:387-391.
5. Taube J.M., Griffin C.A., Yonescu R.,Morsberger L., Argani P., Askin F.B.,Batista D.A.: Pleuropulmonary blastoma: cytogenetic and spectralkaryotype analysis. Pediatr DevPathol, 2006, 9: 453-461.
chemotherapy and radiotherapy,however it is an aggressive tumourwith a relatively poor prognosis,which increases with tumour masseslarger than 5 cm at diagnosis.
Unfortunately, a pre-operativediagnosis is rarely made, and thediagnosis is usually seen retro -spectively on histopathologicalanalysis of the surgical specimenwhich has often not achieved defini-tive surgical margins. Since an ade-quate resection is required to preventtumour seeding, a pre-operative con-sideration should be given to thisdiagnosis the presence of these fea-tures to ensure a better prognosis.
References
1. Walker R., Suvarna K., Matthews S.:Pulmonary blastoma: presentation of
14 JBR–BTR, 2011, 94 (1)
Fig. 2. — Longitudinal ultrasound scan over right lung demon-strating echogenic parenchyma with septated fluid.
Fig. 3. — Axial post-contrast CT scan of the thorax confirms amixed solid/cystic mass in the right hemithorax with surround-ing peripulmonary fluid. There is also significant shift of themediastinum to the left.
o'brien-_Opmaak 1 9/02/11 10:18 Pagina 14
Hydatid disease caused byechinococcus granulosus is endemicin Tunisia where the incidence is241cases/year (1). It is thereforeamong common surgical and diag-nosis problems in Tunisia. Hydatiddisease has a predilection to locatein the liver and lung (90%). It canalso be encountered in almost everypart of the body from the crown ofthe head (1) to the big toe (2).Pelvic localizations represent 1-
2% of all locations in the Tunisianpublications and 1% in the Europeanones (3).We report on one case of pelvic
hydatic cyst and expose the clinicaland radiological characteristics ofthe disease and the therapeutic management particular of this rarelocation.
Case report
An 8- year-old boy with no specif-ic illness was admitted for explo-ration of sciatica pain and limpinglasting for 2 months in a context ofweight loss and asthenia.Abdominal examination showed
a painless pelvic non mobile masswithout hepatomegaly or spleno -megaly. At digital rectal examinationregular para-rectal mass withoutsphincter troubles was detected. Theneurological examination showedleft sciatica pain, limping and negative Achilles’s reflex.The electromyography pointed to
a lesion at the L5-S1 level.Biological explorations demon-
strated normal blood concentrationof αfoetoprotein and βHCG werenormal. Chest X ray was normal.
Abdominal Ultrasound revealed a10 x 9 cm cystic pelvic mass without
colon and compression of the homo-lateral sciatica.At surgical exploration (Fig. 2) a
retroperitoneal mass pushing therectum to the right and the iliac ves-sels to the left was found. The aspectof prominent dome evocated hydaticcyst.The surrounding structures were
protected with gauzes soaked in nor-mal saline solution as a filter againstmacroscopic spillage. The cyst wasthen punctured and aspirated, takingextreme care to prevent inadvertentspillage of intracystic fluid. Thehypertonic saline (20% NaCl)
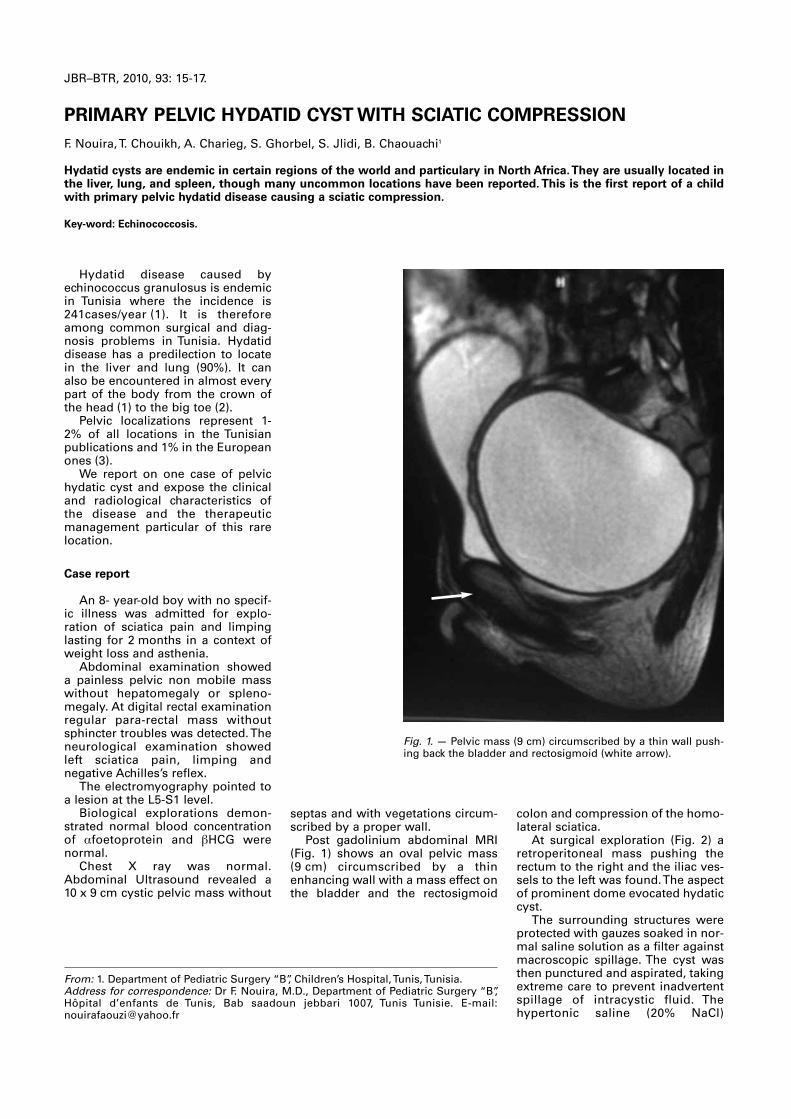
septas and with vegetations circum-scribed by a proper wall.Post gadolinium abdominal MRI
(Fig. 1) shows an oval pelvic mass(9 cm) circumscribed by a thinenhancing wall with a mass effect onthe bladder and the rectosigmoid
JBR–BTR, 2010, 93: 15-17.
PRIMARY PELVIC HYDATID CYST WITH SCIATIC COMPRESSIONF. Nouira, T. Chouikh, A. Charieg, S. Ghorbel, S. Jlidi, B. Chaouachi1
Hydatid cysts are endemic in certain regions of the world and particulary in North Africa. They are usually located inthe liver, lung, and spleen, though many uncommon locations have been reported. This is the first report of a childwith primary pelvic hydatid disease causing a sciatic compression.
Key-word: Echinococcosis.
From: 1. Department of Pediatric Surgery “B”, Children’s Hospital, Tunis, Tunisia.Address for correspondence: Dr F. Nouira, M.D., Department of Pediatric Surgery “B”,Hôpital d’enfants de Tunis, Bab saadoun jebbari 1007, Tunis Tunisie. E-mail:[email protected]
Fig. 1. — Pelvic mass (9 cm) circumscribed by a thin wall push-ing back the bladder and rectosigmoid (white arrow).
nouira-_Opmaak 1 16/02/11 09:44 Pagina 15

solution was injected into the cyst asa scolicidal agent. After 5 minutes, asuction device with side holes wasinserted into the cyst and the fluidwas evacuated. The germinal mem-brane was then pulled out. Theremaining protuberant pericysticwall was widely excised with inser-tion of an omental flap into theremaining cystic cavity.
Postoperative recovery wasprompt and uneventful withdecrease of pain and limping. Thepatient received albendazole treat-ment for one year. Follow up after2 years showed a regression of theneurological symptomatology.
Discussion
Retroperitoneal and retrovesicallocations of a hydatid cyst are rareeven in endemic areas. According tothe theory of Deve, fissuring or rup-ture of a primary hepatic, splenic ormesenteric cyst would seed its con-tents in the abdominal cavity (4). Thisprimary cyst might then heal andeven disappear, leaving a scar thatcould be overlooked. The pouch ofDouglas would then be the preferredsite for the development of a sec-ondary cyst in the pelvis, initiallyintraperitoneal and later sub -peritoneal (5).
In the absence of a primary visceral lesion and of peritonealseeding, hematogenous dissemina-
many processes, including embry-onal cyst, lymphangioma, and diges-tive duplicity.
Serological tests are undeniabletools for diagnosis and followup ofhydatitose. Enzyme-linkedimmunosorbent assay (ELISA) andimmunoelectrophoresis are avail-able. Indirect hemagglutination andELISA are the most sensitiveimmunological methods to diagnosehuman hydatidosis but a false-posi-tive reaction secondary to cross-reactivity with other parasitic infec-tions is possible. In the United Statesthe Centers for Disease Control cur-rently recommends a combinationof specific ELISA and Western blotserology (9).
According to the World HealthOrganization study group onechinococcosis, surgery is still thetreatment of choice to provide com-plete cure.
The optimal treatment of primaryretroperitoneal hydatic cyst is com-plete removal of the cyst withoutcontamination of the field and with-out sacrificing the organs involvedthrough the appropriate abdominalincision (10).
Removal of germinal epitheliumand fluid with scoleces may causehydatid dissemination and allergicmanifestations, even anaphylacticshock. Ideally then, total cyst exci-sion or pericystectomy should beperformed (3, 11).
If the localization of the cyst andinvasion to vital structures preventthe total excision, partial pericystec-tomy is the treatment of choice afterinjection of scolocidal agent fol-lowed by removal of germinativemembrane (12-14).
Prophylactic measures, such asirrigation with a scolicidal solutionare strongly recommended.Hypertonic 30% saline solution forlocal irrigation, evacuation of thecyst content may be necessary whenthe hydatid fluid is under high ten-sion. Aspiration of the cyst has beenconsidered an option to standardsurgical therapy for elderly patientsand an alternative to partial cystexcision or pericystectomy inpatients with unresectable disease inthe liver. Aspiration of a third of thecyst volume is followed by instilla-tion of the same volume of 95%ethanol within the cyst.
Chowbey et al reported a patientwhose RHC was removed endoscop-ically, but this procedure wasapplied to only few cases andrequires further study (12).
Preoperative treatment with benzimidazoles (albendazole,
tion could explain the pathogenesisof a solitary retroperitoneal lesion.Oncospheres hatch and penetratethe intestinal wall disseminating pri-marily to the liver, secondarily to thelung and finally anywhere to formunilocular cysts. They also can passthrough the liver and lung barriers,without seeding these structures,and develop an implant any-where (6, 7). Other pathogenichypotheses for an isolated retroperi-toneal or retrovesical cyst have alsobeen proposed (8, 6): migration ofthe larvae from the intestinal lymphvessels to the thoracic channel andthen anywhere in the body throughthe hemorrhoidal vessels to achievea prerectal or retrovesical location orfrom the rectal ampulla.
Retroperitoneal cysts generallypresents as a palpable mass or withflank pain as in our case. A mass waspalpable on digital rectal examina-tion. Digestive symptoms, such asconstipation, abdominal pain due tothe compression effect of the massare reported. Neurological compres-sion is in theory possible but exceptionally reported. Our patientpresented limping and sciatica painand neurological defect negativeAchilles’s reflex of the left foot.
The imaging findings frequentlysuggest hydatid disease but are usu-ally inconclusive and a differentialdiagnosis may not be made beforesurgery. A retrovesical cyst mimics
16 JBR–BTR, 2011, 94 (1)
Fig. 2. — The cyst was opened and a discus proligerus wasextracted.
nouira-_Opmaak 1 10/02/11 08:35 Pagina 16

mebendazole) has been reported tosoften the cyst and to reduce intra-cystic pressure, enabling the sur-geons to remove the endocyst moreeasily (10). Postoperative treatmentwith benzimidazoles of patients canreduce the rate of recurrence (10,13). It is particularly recommended ifthere is cyst spillage during surgeryor partial cyst removal (12). Theprevalence of long-term recurrenceranges between 2 and 25%.Recurrence can be due to incompletecyst removal or previously undetect-ed cysts (10).
Conclusion
In endemic regions, HC should beconsidered in the differential diagno-sis of retroperitoneal cystic lesions.Clinical symptoms are no specific,and appear long time at a late stageof the development of the parasit.Abdomino-pelvic US is the mostuseful diagnostic tool, and MRI isefficient in the differential diagnosis.
Total cyst excision should be triedin all cases. When this is not possi-ble, removal of all germinative mem-branes and partial pericystectomy
Hidatidosis retrovesical. Actas UrolEsp, 1983, 7: 165.
9. King C.H.: Cestodes. In: Principles andPractice of Infectious Diseases, 4thed. Edited by Mandell G.L.,Bennett J. E. and Dolin R. New York:Churchill Livingstone, 1995, pp 2544-2553.
10. Pawlowski Z.S., Eckert J., Vuitton D.,et al.: Echinococcosis inhumans: clinical aspects, diagnosis and treat-ment. A Public HealthProblem ofGlobal Concern. Paris, France: WorldOrganisation for Animal Health andWorld Health Organisation, 2001, 20:71.
11. Njeh M., Hajri M., Chebil M., et al.: Lekyste hydatique rétro-vésical. A -propos de deux cas. Ann Urol, 1993b,27: 97.
12. Chowbey P.K., Wadhwa A., Shah S.,et al.: Endoscopic managementof a retroperitoneal hydatid cyst.J Laparo endosc, 2004, 14: 236-240.
13. Buttenschoen K., Buttenschoen D.:Echinococcus granulosus infection:the challenge of surgical treatment.Arch Surg, 2003, 388: 218-230.
14. Durakbasa C.U., Tireli G.A.,Sehiralti V., et al.: An audit on pediatric hydatid disease of uncommon localization: incidence,diagnosis, surgical approach, andoutcome. J Pediatr Surg, 2006, 41:1457-1463.
with the use of scolocidal agents arethe treatments of choice. Additionaladjuvant medical therapy is essen-tial to avoid recurrence.
References
1. Beggs I.: The radiological appear-ances of hydatic disease of the liver.Clin Radiol, 1983, 34: 555-563.
2. Gharbi H., Cheikh M., Hamza R.: Leslocations rares de l'hydatidose chezl'enfant. Ann Radiol, 1977, 20: 151-157.
3. Bennani S., El Mrini M., Raji A., et al.:Les kystes hydatiques rétro-vésicauxet rétro-péritonéaux isolés: à proposde cinq cas. Ann Urol, 1992, 26: 244-349.
4. Deve F.: L'échinococcose secondaire.Société d'Editions Scientifiques.Paris, 190.
5. Kotoulas, G., Gouliamos, A.,Kalovidouris, et al. Computed tomo-graphic localization of pelvic hydatiddisease. Eur J Rad, 1990, 11: 38.
6. Ouadfel, J., Assem, A., Errougani, A.,et al: Le kyste hydatique rétropéri-tonéal isolé. Ann Chir, 1990, 44: 243.
7. Haddad, S. I. and Khairallah, A.:Surgical consideration of hydatid disease: report of some unusualcases. Ann Surg, 1940, 111: 597.
8. Fernandez A., Silmi-Moyano A.,Rodriguez-Vallejo J.M., et al:
PRIMARY PELVIC HYDATID CYST — NOUIRA et al 17
nouira-_Opmaak 1 10/02/11 08:35 Pagina 17
Müllerian duct abnormalities(MDA) are developmental disordersleading to dysmorphism of thefemale genital tract. The disruptionof the normal embryologic fusion ofthe paramesonephric (Müllerian)ducts or the non-resorption of theuterine septum is believed to be thecrucial element in this entity (1, 2).Buttram and Gibbons have created awidely used classification of MDA (3)
MDA are rare syndromes andscarcely reported on in English liter-ature. But the introduction of themodern MRI equipment has led toimproved recognition and familiaritywith these complex malformations.
Clinically the patients presentwith nonspecific symptoms aroundthe time of menarche. Imaging canbe helpful in the correct diagnosis,preventing delayed surgical inter-vention and possible infertility.
In this report we present a case ofuterus didelphys with an obstructedhemivagina and ipsilateral renalagenesis (Buttram and Gibbonsclass III) and a brief review of litera-ture.
Case report
A 12-year-old female patient pre-sented at our emergency depart-ment with intermittent abdominalpain and heavy vaginal blood loss.The menstrual cycle had started6 months before and was incon -spicuous until the last 2 months. Atthat time menstruation was accom-panied by intense pains and heavyblood loss.
Initial clinical workup did not leadto a specific diagnosis. Pelvic ultra-sound was performed and showedhematometra with suspicion of uter-
Ipsilaterally to the affected side ofthe internal genitalia, absence of theleft kidney was noted (Fig. 5).
The MRI results were consistentwith uterus didelphys with anobstructed hemivagina and ipsilater-al renal agenesis.
The patient underwent gynaeco-logic intervention, the obstructedhemivagina was opened and theseptum between the two vaginas wasexcised. There were no major com-plications and the next day the patientleft our hospital in good condition.
Discussion
MDA are developmental disordersthat can lead to a variety of abnor-malities in the female urogenital tract.The reported incidence in Englishliterature is 0.5-5% (1, 2). Buttramand Gibbons have classified thevarious MDA into 6 categories (3).
The presented case illustrates theimaging findings of uterus didelphyswith an imperforate hemivagina and
ine dysmorphism. The patient wasscheduled for a MRI of the pelvis.
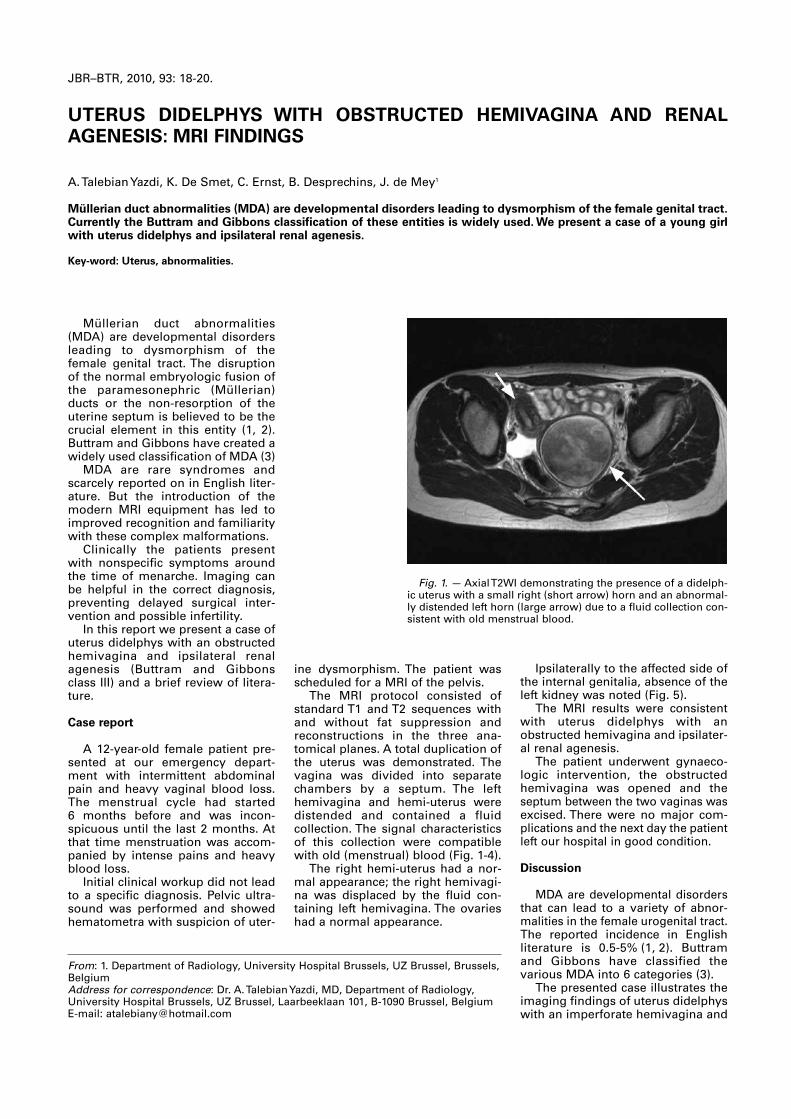
The MRI protocol consisted ofstandard T1 and T2 sequences withand without fat suppression andreconstructions in the three ana -tomical planes. A total duplication ofthe uterus was demonstrated. Thevagina was divided into separatechambers by a septum. The lefthemivagina and hemi-uterus weredistended and contained a fluidcollection . The signal characteristicsof this collection were compatiblewith old (menstrual) blood (Fig. 1-4).
The right hemi-uterus had a nor-mal appearance; the right hemivagi-na was displaced by the fluid con-taining left hemivagina. The ovarieshad a normal appearance.
JBR–BTR, 2010, 93: 18-20.
UTERUS DIDELPHYS WITH OBSTRUCTED HEMIVAGINA AND RENALAGENESIS : MRI FINDINGS
A. Talebian Yazdi, K. De Smet, C. Ernst, B. Desprechins, J. de Mey1
Müllerian duct abnormalities (MDA) are developmental disorders leading to dysmorphism of the female genital tract.Currently the Buttram and Gibbons classification of these entities is widely used. We present a case of a young girlwith uterus didelphys and ipsilateral renal agenesis.
Key-word: Uterus, abnormalities.
From: 1. Department of Radiology, University Hospital Brussels, UZ Brussel, Brussels,BelgiumAddress for correspondence: Dr. A. Talebian Yazdi, MD, Department of Radiology,University Hospital Brussels, UZ Brussel, Laarbeeklaan 101, B-1090 Brussel, BelgiumE-mail: [email protected]
Fig. 1. — Axial T2WI demonstrating the presence of a didelph-ic uterus with a small right (short arrow) horn and an abnormal-ly distended left horn (large arrow) due to a fluid collection con-sistent with old menstrual blood.
Talebian Yaszi et al_Opmaak 1 16/02/11 09:40 Pagina 18
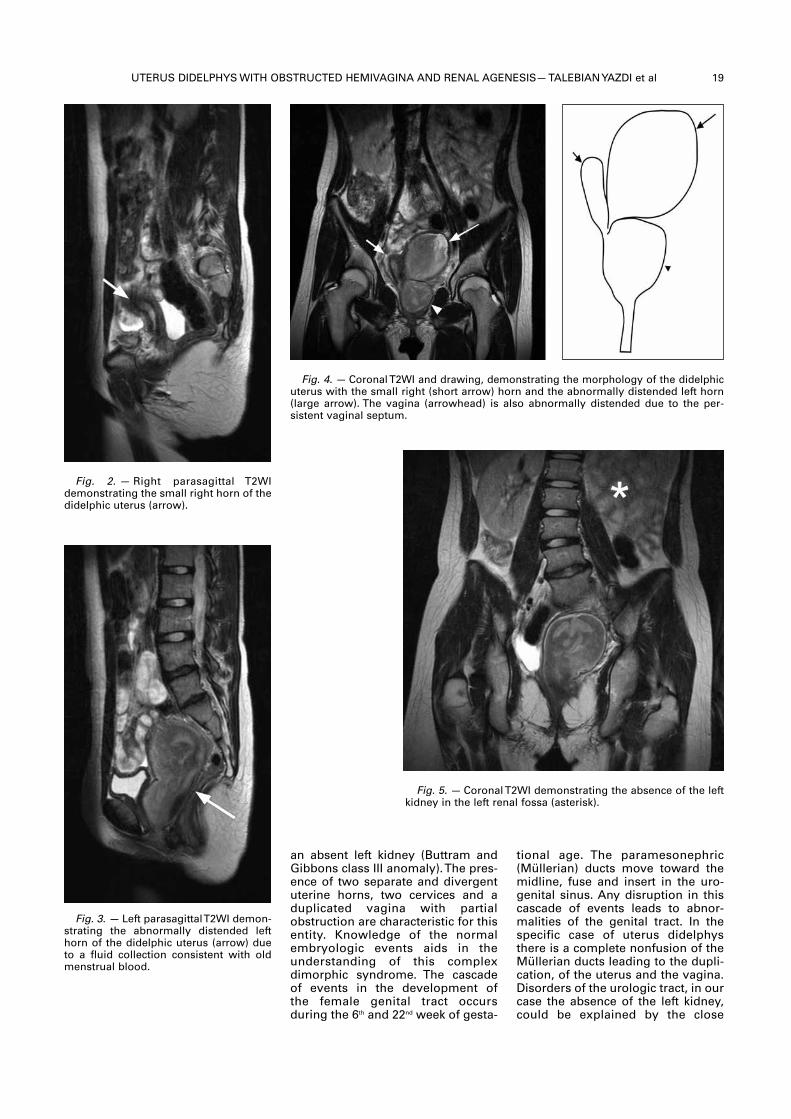
UTERUS DIDELPHYS WITH OBSTRUCTED HEMIVAGINA AND RENAL AGENESIS— TALEBIAN YAZDI et al 19
tional age. The paramesonephric(Müllerian) ducts move toward themidline, fuse and insert in the uro-genital sinus. Any disruption in thiscascade of events leads to abnor-malities of the genital tract. In thespecific case of uterus didelphysthere is a complete nonfusion of theMüllerian ducts leading to the dupli-cation, of the uterus and the vagina.Disorders of the urologic tract, in ourcase the absence of the left kidney,could be explained by the close
an absent left kidney (Buttram andGibbons class III anomaly). The pres-ence of two separate and divergentuterine horns, two cervices and aduplicated vagina with partialobstruction are characteristic for thisentity. Knowledge of the normalembryologic events aids in theunderstanding of this complexdimorphic syndrome. The cascadeof events in the development ofthe female genital tract occursduring the 6th and 22nd week of gesta-
Fig. 2. — Right parasagittal T2WIdemon strating the small right horn of thedidelphic uterus (arrow).
Fig. 3. — Left parasagittal T2WI demon-strating the abnormally distended lefthorn of the didelphic uterus (arrow) dueto a fluid collection consistent with oldmenstrual blood.
Fig. 4. — Coronal T2WI and drawing, demonstrating the morphology of the didelphicuterus with the small right (short arrow) horn and the abnormally distended left horn(large arrow). The vagina (arrowhead) is also abnormally distended due to the per -sistent vaginal septum.
Fig. 5. — Coronal T2WI demonstrating the absence of the leftkidney in the left renal fossa (asterisk).
Talebian Yaszi et al_Opmaak 1 16/02/11 09:40 Pagina 19

20 JBR–BTR, 2011, 94 (1)
embryologic relationship betweenthe mesonephric (Wolffian) ductsand the paramesonephric ducts.Various teratologic influences arebelieved to cause concomitant uro-logic and gynaecologic malforma-tions (4-6)
MRI, with its superior soft tissueresolution, often leads to a straight-forward diagnosis of complexMüllerian duct abnormalities. There -fore it is considered the best non-invasive tool in the work-up of mal-formations of the urogenital tract.
Knowledge of the main imagingfindings of uterus didelphys andother MDA will aid in the timely andcorrect diagnosis. Complications ofdelayed diagnosis are infection withsubsequent abscess formation andhysterectomy with or withoutoophorectomy leading to infertility.
their distribution among subtypes?J Reprod Med, 1998, 43: 877–887.
2. Stampe Sorensen S. Estimatedprevalence of müllerian anomalies.Acta Obstet Gynecol Scand, 1988, 67:441-445.
3. Buttram V.C. Jr, Gibbons W.E.Müllerian anomalies: a proposedclassification (an analysis of 144cases). Fertil Steril, 1979, 32: 40-46.
4. Anderson K.A., McAninch J.W.Uterus didelphia with left hemato -colpos and ipsilateral renal agenesis.J Urol, 1982, 127: 550-553.
5. Yoder I.C., Pfister R.C. Unilateralhematocolpos and ipsilateral renalagenesis: report of two cases andreview of the literature. AJR, 1976,127: 303-308.
6. Eisenberg E., Farber M., Mitchell Jr, G.W.Complete duplication of the uterusand cervix with a unilaterally imper-forate vagina. Obstet Gynecol 1982,60: 259-262.
Conclusion
Müllerian duct abnormalitiesencompass a variety of dimorphicchanges in the female genital tract,often with associated urologicanomalies. In this paper the MRcharacteristics of uterus didelphyswith an imperforate hemivagina andan absent left kidney were dis-cussed. Familiarity of the radiologistwith the imaging findings of this raresyndrome is important, becausedelayed diagnosis increases thechance of complication and possibleinfertility.
References
1. Nahum G.G. Uterine anomalies:how common are they and what is
Talebian Yaszi et al_Opmaak 1 16/02/11 09:40 Pagina 20
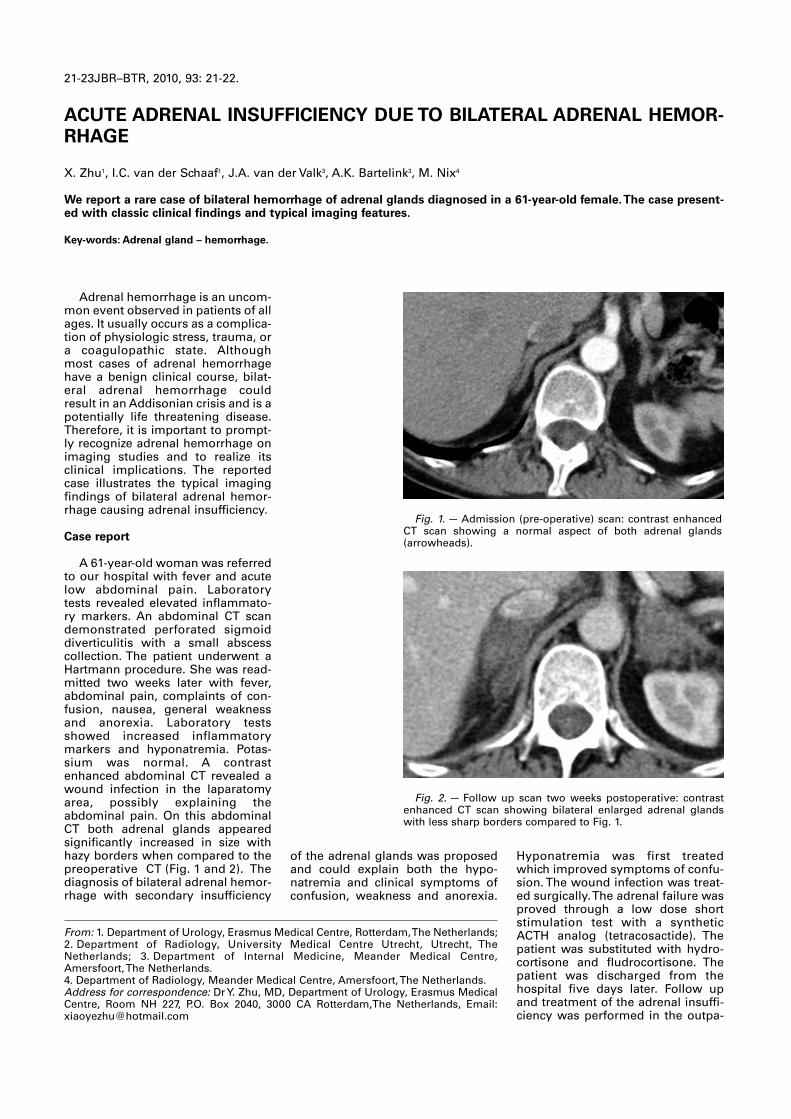
Adrenal hemorrhage is an uncom-mon event observed in patients of allages. It usually occurs as a complica-tion of physiologic stress, trauma, ora coagulopathic state. Althoughmost cases of adrenal hemorrhagehave a benign clinical course, bilat-eral adrenal hemorrhage couldresult in an Addisonian crisis and is apotentially life threatening disease.Therefore, it is important to prompt-ly recognize adrenal hemorrhage onimaging studies and to realize itsclinical implications. The reportedcase illustrates the typical imagingfindings of bilateral adrenal hemor-rhage causing adrenal insufficiency.
Case report
A 61-year-old woman was referredto our hospital with fever and acutelow abdominal pain. Laboratorytests revealed elevated inflammato-ry markers. An abdominal CT scandemonstrated perforated sigmoiddiverticulitis with a small abscesscollection. The patient underwent aHartmann procedure. She was read-mitted two weeks later with fever,abdominal pain, complaints of con-fusion, nausea, general weaknessand anorexia. Laboratory testsshowed increased inflammatorymarkers and hyponatremia. Potas -sium was normal. A contrastenhanced abdominal CT revealed awound infection in the laparatomyarea, possibly explaining theabdominal pain. On this abdominalCT both adrenal glands appearedsignificantly increased in size withhazy borders when compared to thepreoperative CT (Fig. 1 and 2). Thediagnosis of bilateral adrenal hemor-rhage with secondary insufficiency
Hyponatremia was first treatedwhich improved symptoms of confu-sion. The wound infection was treat-ed surgically. The adrenal failure wasproved through a low dose shortstimulation test with a syntheticACTH analog (tetracosactide). Thepatient was substituted with hydro-cortisone and fludrocortisone. Thepatient was discharged from thehospital five days later. Follow upand treatment of the adrenal insuffi-ciency was performed in the outpa-
of the adrenal glands was proposedand could explain both the hypo -natremia and clinical symptoms ofconfusion , weakness and anorexia.
21-23JBR–BTR, 2010, 93: 21-22.
ACUTE ADRENAL INSUFFICIENCY DUE TO BILATERAL ADRENAL HEMOR-RHAGE
X. Zhu1, I.C. van der Schaaf1, J.A. van der Valk3, A.K. Bartelink3, M. Nix4
We report a rare case of bilateral hemorrhage of adrenal glands diagnosed in a 61-year-old female. The case present-ed with classic clinical findings and typical imaging features.
Key-words: Adrenal gland – hemorrhage.
From: 1. Department of Urology, Erasmus Medical Centre, Rotterdam, The Netherlands;2. Department of Radiology, University Medical Centre Utrecht, Utrecht, TheNetherlands; 3. Department of Internal Medicine, Meander Medical Centre,Amersfoort, The Netherlands. 4. Department of Radiology, Meander Medical Centre, Amersfoort, The Netherlands.Address for correspondence: Dr Y. Zhu, MD, Department of Urology, Erasmus MedicalCentre, Room NH 227, P.O. Box 2040, 3000 CA Rotterdam,The Netherlands, Email:[email protected]
Fig. 1.— Admission (pre-operative) scan: contrast enhancedCT scan showing a normal aspect of both adrenal glands(arrowheads).
Fig. 2.— Follow up scan two weeks postoperative: contrastenhanced CT scan showing bilateral enlarged adrenal glandswith less sharp borders compared to Fig. 1.
Zhu et al_Opmaak 1 16/02/11 09:38 Pagina 21
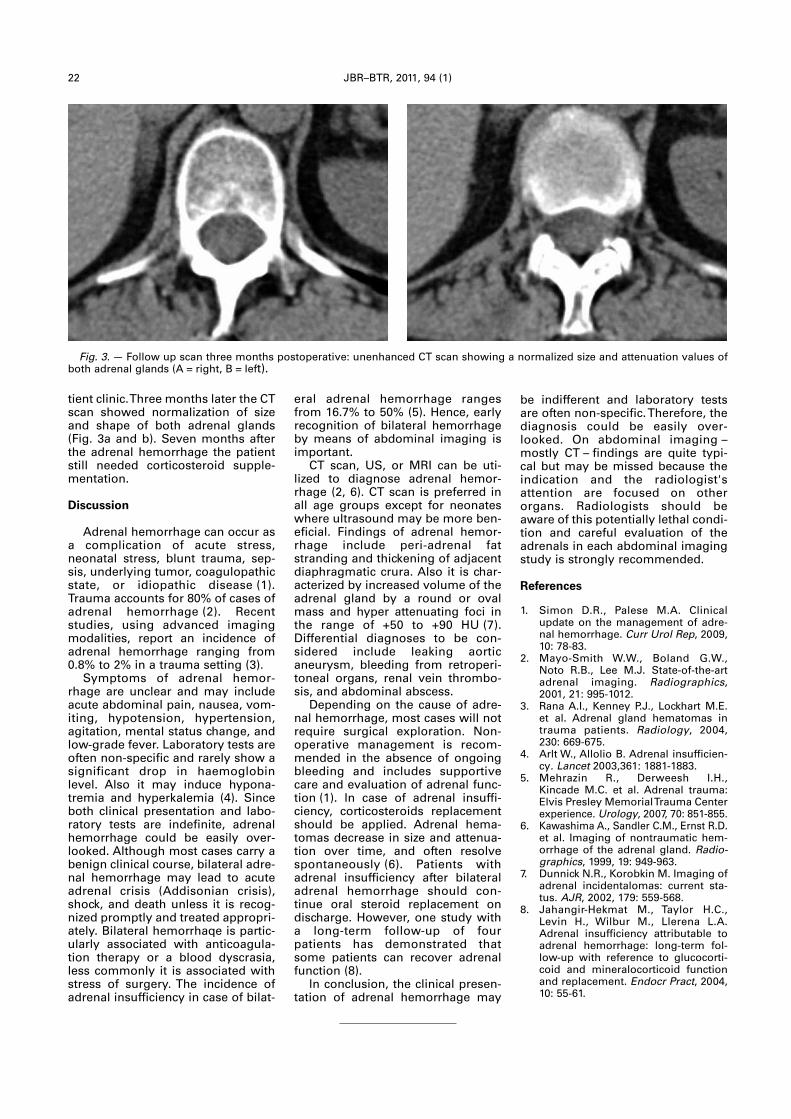
tient clinic. Three months later the CTscan showed normalization of sizeand shape of both adrenal glands(Fig. 3a and b). Seven months afterthe adrenal hemorrhage the patientstill needed corticosteroid supple-mentation.
Discussion
Adrenal hemorrhage can occur asa complication of acute stress,neonatal stress, blunt trauma, sep-sis, underlying tumor, coagulopathicstate, or idiopathic disease (1).Trauma accounts for 80% of cases ofadrenal hemorrhage (2). Recentstudies, using advanced imagingmodalities, report an incidence ofadrenal hemorrhage ranging from0.8% to 2% in a trauma setting (3). Symptoms of adrenal hemor-
rhage are unclear and may includeacute abdominal pain, nausea, vom-iting, hypotension, hypertension,agitation, mental status change, andlow-grade fever. Laboratory tests areoften non-specific and rarely show asignificant drop in haemoglobinlevel. Also it may induce hypona-tremia and hyperkalemia (4). Sinceboth clinical presentation and labo-ratory tests are indefinite, adrenalhemorrhage could be easily over-looked. Although most cases carry abenign clinical course, bilateral adre-nal hemorrhage may lead to acuteadrenal crisis (Addisonian crisis),shock, and death unless it is recog-nized promptly and treated appropri-ately. Bilateral hemorrhaqe is partic-ularly associated with anticoagula-tion therapy or a blood dyscrasia,less commonly it is associated withstress of surgery. The incidence ofadrenal insufficiency in case of bilat-
be indifferent and laboratory testsare often non-specific. Therefore, thediagnosis could be easily over-looked. On abdominal imaging –mostly CT – findings are quite typi-cal but may be missed because theindication and the radiologist'sattention are focused on otherorgans. Radiologists should beaware of this potentially lethal condi-tion and careful evaluation of theadrenals in each abdominal imagingstudy is strongly recommended.
References
1. Simon D.R., Palese M.A. Clinicalupdate on the management of adre-nal hemorrhage. Curr Urol Rep, 2009,10: 78-83.
2. Mayo-Smith W.W., Boland G.W.,Noto R.B., Lee M.J. State-of-the-artadrenal imaging. Radio graphics,2001, 21: 995-1012.
3. Rana A.I., Kenney P.J., Lockhart M.E.et al. Adrenal gland hema tomas intrauma patients. Radi ology, 2004,230: 669-675.
4. Arlt W., Allolio B. Adrenal insufficien-cy. Lancet 2003,361: 1881-1883.
5. Mehrazin R., Derweesh I.H.,Kincade M.C. et al. Adrenal trauma:Elvis Presley Memorial Trauma Centerexperience. Urology, 2007, 70: 851-855.
6. Kawashima A., Sandler C.M., Ernst R.D.et al. Imaging of nontraumatic hem-orrhage of the adrenal gland. Radio -graphics, 1999, 19: 949-963.
7. Dunnick N.R., Korobkin M. Imaging ofadrenal incidentalomas: current sta-tus. AJR, 2002, 179: 559-568.
8. Jahangir-Hekmat M., Taylor H.C.,Levin H., Wilbur M., Llerena L.A.Adrenal insufficiency attributable toadrenal hemorrhage: long-term fol-low-up with reference to glucocorti-coid and mineralocorticoid functionand replacement. Endocr Pract, 2004,10: 55-61.
eral adrenal hemorrhage rangesfrom 16.7% to 50% (5). Hence, earlyrecognition of bilateral hemorrhageby means of abdominal imaging isimportant. CT scan, US, or MRI can be uti-
lized to diagnose adrenal hemor-rhage (2, 6). CT scan is preferred inall age groups except for neonateswhere ultrasound may be more ben-eficial. Findings of adrenal hemor-rhage include peri-adrenal fatstranding and thickening of adjacentdiaphragmatic crura. Also it is char-acterized by increased volume of theadrenal gland by a round or ovalmass and hyper attenuating foci inthe range of +50 to +90 HU (7).Differential diagnoses to be con -sidered include leaking aorticaneurysm, bleeding from retroperi-toneal organs, renal vein thrombo-sis, and abdominal abscess. Depending on the cause of adre-
nal hemorrhage, most cases will notrequire surgical exploration. Non -operative management is recom-mended in the absence of ongoingbleeding and includes supportivecare and evaluation of adrenal func-tion (1). ln case of adrenal insuffi-ciency, corticosteroids replacementshould be applied. Adrenal hema -tomas decrease in size and attenua-tion over time, and often resolvespontaneously (6). Patients withadrenal insufficiency after bilateraladrenal hemorrhage should con -tinue oral steroid replacement ondischarge. However, one study witha long-term follow-up of fourpatients has demonstrated thatsome patients can recover adrenalfunction (8). ln conclusion, the clinical presen-
tation of adrenal hemorrhage may
22 JBR–BTR, 2011, 94 (1)
Fig. 3.— Follow up scan three months postoperative: unenhanced CT scan showing a normalized size and attenuation values ofboth adrenal glands (A = right, B = left).
Zhu et al_Opmaak 1 16/02/11 09:38 Pagina 22

Case report
Alveolar echinococcosis is a rare,but potentially fatal, chronic and pro-gressive disease, caused by infesta-tion of the liver by Echinococcusmultilocularis. Humans are the inter-mediate host that become infectedby ingestion of the wild berries,plants or water which is contaminat-ed with eggs of the parasites or bydirect contact with the definitivehost, which is the wild canine (foxes,wolves). The disease is usually seenin central and northern Europe,North America, Canada, China andJapan (1). It is endemic in easternTurkey (2). An invasive tumor-likemulti-vesiculated lesion developsduring a long, asymptomatic periodwhich is characteristic for the dis-ease. In this study we present a caseof Echinococcus multilocularis infes-tation, forming a tumor-like lesion inthe liver.A 61- year-old man was referred to
our clinic with right-upper quadrantpain, weight loss and fatigue ofalmost 1 year duration. Physicalexamination revealed no significantfinding. Abnormal laboratory find-ings were as follows: erythrocytesedimentation rate 52 mm/h (5-25 mm/h), gamma-glutamyl trans-ferase 122 IU/L (8-61 IU/L), lactatedehydrogenase 500 IU/L (240-480 IU/L), serum aspartate transami-nase 52 IU/L (0-37 IU/L), white bloodcell count 10.75 x10^3/Ul (3.8-10.0 x 10^3/Ul), neutrophil percent-age 32.8 (45-78%), eosinophil per-centage 34.8 (0.8- 7.0%), haemoglo-bin 11.6 g/dL (13.0-17.5 g/dL), CA 125level 48.2 U/ml (0-30.2 U/ml), CA 19-9 level 71.4 U/ml (0-37 U/ml).Hepatitis B surface antigen level was287.8 mIU/ml in the serum (positive:> 10 mIU/ml).Ultrasonography (Aplio XV,
Toshiba, Tokyo, Japan) revealed a
Following the radiological work-up, the patient was referred to theliver biopsy. The biopsy was com-pleted without any complication. Thehistopathologic work-up, as themost reliable method to have thedefinitive diagnosis, showed hepaticalveolar echinococcosis.
Discussion
Hepatic infestation of echino -coccus multilocularis appears as anill-defined infiltrative disease usuallyconsisting of cystic and solid compo-nents. Microcalcifications are commonly seen (3). Necrotic areasfrequently develop due to ischemiaas the lesion size increase. The surrounding vascular structures andbiliary system may be infiltrated bythe disease or they may even be displaced due to the mass effect ofthe lesion, which imitates a slow- growing tumor (3).In most cases, lesions are
hyperechoic with heterogeneousechopattern and indistinct marginson ultrasonography (USG) (1).Cavitary or cystic to vesicularappearance can be seen within themasses. Color Doppler USG showsthe absence of vascular flow in thesolid components of the lesions (4). CT imaging of the liver infestation
shows heterogeneous, ill-defined,hypodense areas which have poor orno enhancement after intravenouscontrast administration (1). In 90%of the infected cases, calcificationsare found (1). Pseudocystic necroticareas and dilatation of the intra -hepatic bile ducts can also be identi-fied (3). The fibrotic changes of the
disease process and extension of thelesion within the liver parenchymacan be demonstrated by MRI (3).Fibrosis and parasitic tissue havelow signal intensity on T1-weightedimages (3). On T2-weighted images,lesions may be hypointense,hyperintense or isointense (1).Central necrotic zones and cysticperipheral extensions are betteridentified on T2-weighted images (3).
large heterogeneous liver massalmost completely filling the rightlobe with isoechoic and hyperechoicareas relative to the normal liverparenchyma. There was a smallhypoechoic cystic space with irregu-lar margins on the right upperperipheral region (Fig. 1A). The masshad irregular, indistinct borders. Itdemonstrated no significant findingby colored Doppler ultrasonography.Because the use of sonographic con-trast agents were not allowed by theministry of health in Turkey, contrastenhanced ultrasonography could notbe performed. Unenhanced abdominal comput-
ed tomography (Siemens SomatomSensation 16-detector row CT,Erlangen, Germany) revealed anarea of heterogeneous density in theright lobe of the liver with some mil-limetric calcifications located cen-trally (Fig. 1B). The margins wereindistinct and ill-defined. There wasno prominent contrast enhancementafter the iodinated contrast mediuminjection (Fig. 1C). MagneticResonance imaging (Signa Excite HD1.5T; GE Healthcare, Milwaukee, WI,USA) of the liver revealed a hetero-geneous hypointense mass withirregular margins on both unen-hanced T1 and T2- weighted images(Fig. 2A-B). The lesion measured16 cm x 12 cm; it was almost totallyfilling the right upper lobe andextending into the left lobe. It hada right peripheral cystic necroticarea. After the administration ofhepatocyte-specific contrast agent(Primovist 0.25 mmol/ml - BayerSchering, Berlin,Germany), thelesion revealed no contrast enhance-ment in arterial (Fig. 2C) and portalvenous phases. There was no con-trast enhancement in the late hepa-tobiliary phase (Fig. 2D), indicatingthat the mass does not contain anyhepatocytes.
JBR–BTR, 2011, 94: 23-25.
HEPATIC ALVEOLAR ECHINOCOCCOSIS: A DIAGNOSTIC CHALLENGEO. Yapici, S.M. Erturk, M. Ulusay, A. Ozel, A. Halefoglu, Z. Karpat, M. Basak1
We report a case of alveolar echinococcosis involving the liver in a 61-year-old male. Alveolar echinococcosis is a rarechronic and progressive disease, which can involve mostly liver and in rare cases lung and brain. It is caused byEchinococcus multilocularis. In this report we describe the imaging findings of hepatic involvement of alveolarechinococcosis by ultrasonography, computed tomography and magnetic resonance imaging.
Key-word: Echinococcosis.
From: Department of Radiology, Sisli Etfal Training and Research Hospital, Istanbul,Turkey.Address for correspondence: Dr O. Yapici, Department of Radiology, Sisli Etfal Trainingand Research Hospital, Istanbul, Turkey. E-mail: [email protected]
yapici-_Opmaak 1 16/02/11 09:37 Pagina 23
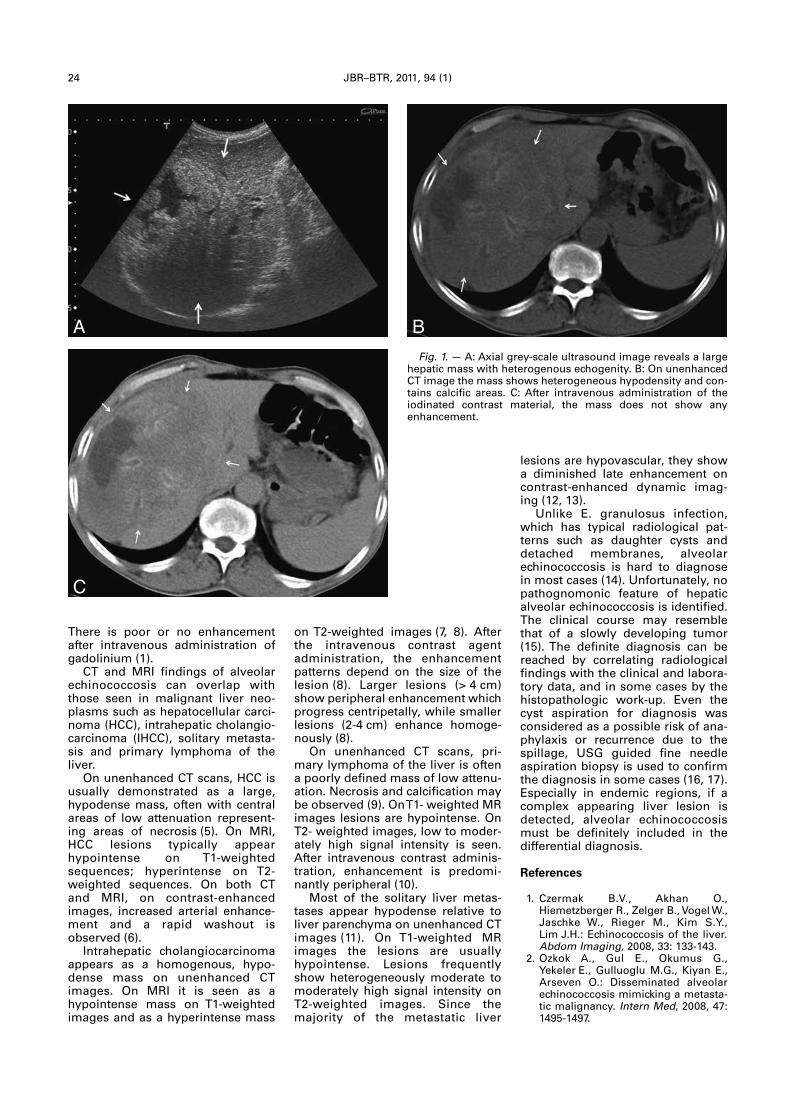
24 JBR–BTR, 2011, 94 (1)
There is poor or no enhancementafter intravenous administration ofgadolinium (1).CT and MRI findings of alveolar
echinococcosis can overlap withthose seen in malignant liver neo-plasms such as hepatocellular carci-noma (HCC), intrahepatic cholangio-carcinoma (IHCC), solitary metasta-sis and primary lymphoma of theliver. On unenhanced CT scans, HCC is
usually demonstrated as a large,hypodense mass, often with centralareas of low attenuation represent-ing areas of necrosis (5). On MRI,HCC lesions typically appearhypointense on T1-weightedsequences; hyperintense on T2-weighted sequences. On both CTand MRI, on contrast-enhancedimages, increased arterial enhance-ment and a rapid washout isobserved (6). Intrahepatic cholangiocarcinoma
appears as a homogenous, hypo-dense mass on unenhanced CTimages. On MRI it is seen as ahypointense mass on T1-weightedimages and as a hyperintense mass
lesions are hypovascular, they showa diminished late enhancement oncontrast-enhanced dynamic imag-ing (12, 13).Unlike E. granulosus infection,
which has typical radiological pat-terns such as daughter cysts anddetached membranes, alveolarechinococcosis is hard to diagnosein most cases (14). Unfortunately, nopathognomonic feature of hepaticalveolar echinococcosis is identified.The clinical course may resemblethat of a slowly developing tumor(15). The definite diagnosis can bereached by correlating radiologicalfindings with the clinical and labora-tory data, and in some cases by thehistopathologic work-up. Even thecyst aspiration for diagnosis wasconsidered as a possible risk of ana-phylaxis or recurrence due to thespillage, USG guided fine needleaspiration biopsy is used to confirmthe diagnosis in some cases (16, 17).Especially in endemic regions, if acomplex appearing liver lesion isdetected, alveolar echinococcosismust be definitely included in thedifferential diagnosis.
References
1. Czermak B.V., Akhan O.,Hiemetzberger R., Zelger B., Vogel W.,Jaschke W., Rieger M., Kim S.Y.,Lim J.H.: Echinococcosis of the liver.Abdom Imaging, 2008, 33: 133-143.
2. Ozkok A., Gul E., Okumus G.,Yekeler E., Gulluoglu M.G., Kiyan E.,Arseven O.: Disseminated alveolarechinococcosis mimicking a metasta-tic malignancy. Intern Med, 2008, 47:1495-1497.
on T2-weighted images (7, 8). Afterthe intravenous contrast agentadministration, the enhancementpatterns depend on the size of thelesion (8). Larger lesions (> 4 cm)show peripheral enhancement whichprogress centripetally, while smallerlesions (2-4 cm) enhance homoge-nously (8).On unenhanced CT scans, pri-
mary lymphoma of the liver is oftena poorly defined mass of low attenu-ation. Necrosis and calcification maybe observed (9). On T1- weighted MRimages lesions are hypointense. OnT2- weighted images, low to moder-ately high signal intensity is seen.After intravenous contrast adminis-tration, enhancement is predomi-nantly peripheral (10). Most of the solitary liver metas-
tases appear hypodense relative toliver parenchyma on unenhanced CTimages (11). On T1-weighted MRimages the lesions are usuallyhypointense. Lesions frequentlyshow heterogeneously moderate tomoderately high signal intensity onT2-weighted images. Since themajority of the metastatic liver
Fig. 1. — A: Axial grey-scale ultrasound image reveals a largehepatic mass with heterogenous echogenity. B: On unenhancedCT image the mass shows heterogeneous hypodensity and con-tains calcific areas. C: After intravenous administration of theiodinated contrast material, the mass does not show anyenhancement.
A B
C
yapici-_Opmaak 1 16/02/11 09:37 Pagina 24
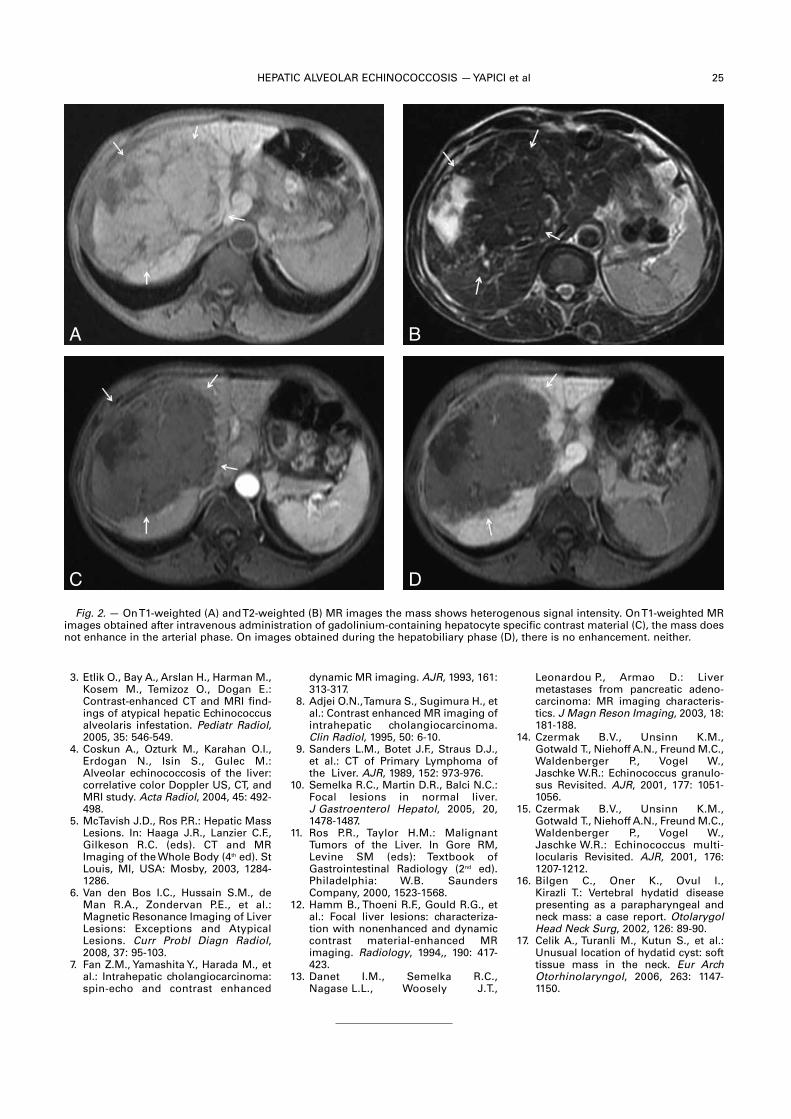
HEPATIC ALVEOLAR ECHINOCOCCOSIS — YAPICI et al 25
3. Etlik O., Bay A., Arslan H., Harman M.,Kosem M., Temizoz O., Dogan E.:Contrast-enhanced CT and MRI find-ings of atypical hepatic Echinococcusalveolaris infestation. Pediatr Radiol,2005, 35: 546-549.
4. Coskun A., Ozturk M., Karahan O.I.,Erdogan N., Isin S., Gulec M.:Alveolar echinococcosis of the liver:correlative color Doppler US, CT, andMRI study. Acta Radiol, 2004, 45: 492-498.
5. McTavish J.D., Ros P.R.: Hepatic MassLesions. In: Haaga J.R., Lanzier C.F.,Gilkeson R.C. (eds). CT and MRImaging of the Whole Body (4th ed). StLouis, MI, USA: Mosby, 2003, 1284-1286.
6. Van den Bos I.C., Hussain S.M., deMan R.A., Zondervan P.E., et al.:Magnetic Resonance Imaging of LiverLesions: Exceptions and AtypicalLesions. Curr Probl Diagn Radiol,2008, 37: 95-103.
7. Fan Z.M., Yamashita Y., Harada M., etal.: Intrahepatic cholangiocarcinoma:spin-echo and contrast enhanced
Leonardou P., Armao D.: Liver metastases from pancreatic adeno-carcinoma: MR imaging characteris-tics. J Magn Reson Imaging, 2003, 18:181-188.
14. Czermak B.V., Unsinn K.M.,Gotwald T., Niehoff A.N., Freund M.C.,Waldenberger P., Vogel W.,Jaschke W.R.: Echinococcus granulo-sus Revisited. AJR, 2001, 177: 1051-1056.
15. Czermak B.V., Unsinn K.M.,Gotwald T., Niehoff A.N., Freund M.C.,Waldenberger P., Vogel W.,Jaschke W.R.: Echinococcus multi -locularis Revisited. AJR, 2001, 176:1207-1212.
16. Bilgen C., Oner K., Ovul I.,Kirazli T.: Vertebral hydatid diseasepresenting as a parapharyngeal andneck mass: a case report. OtolarygolHead Neck Surg, 2002, 126: 89-90.
17. Celik A., Turanli M., Kutun S., et al.:Unusual location of hydatid cyst: softtissue mass in the neck. Eur ArchOtorhinolaryngol, 2006, 263: 1147-1150.
dynamic MR imaging. AJR, 1993, 161:313-317.
8. Adjei O.N., Tamura S., Sugimura H., etal.: Contrast enhanced MR imaging ofintrahepatic cholangiocarcinoma.Clin Radiol, 1995, 50: 6-10.
9. Sanders L.M., Botet J.F., Straus D.J.,et al.: CT of Primary Lymphoma ofthe Liver. AJR, 1989, 152: 973-976.
10. Semelka R.C., Martin D.R., Balci N.C.:Focal lesions in normal liver.J Gastroenterol Hepatol, 2005, 20,1478-1487.
11. Ros P.R., Taylor H.M.: MalignantTumors of the Liver. In Gore RM,Levine SM (eds): Textbook ofGastrointestinal Radiology (2nd ed).Philadelphia: W.B. SaundersCompany, 2000, 1523-1568.
12. Hamm B., Thoeni R.F., Gould R.G., etal.: Focal liver lesions: characteriza-tion with nonenhanced and dynamiccontrast material-enhanced MR imaging. Radiology, 1994,, 190: 417-423.
13. Danet I.M., Semelka R.C.,Nagase L.L., Woosely J.T.,
Fig. 2.— On T1-weighted (A) and T2-weighted (B) MR images the mass shows heterogenous signal intensity. On T1-weighted MRimages obtained after intravenous administration of gadolinium-containing hepatocyte specific contrast material (C), the mass doesnot enhance in the arterial phase. On images obtained during the hepatobiliary phase (D), there is no enhancement. neither.
A B
C D
yapici-_Opmaak 1 16/02/11 09:37 Pagina 25
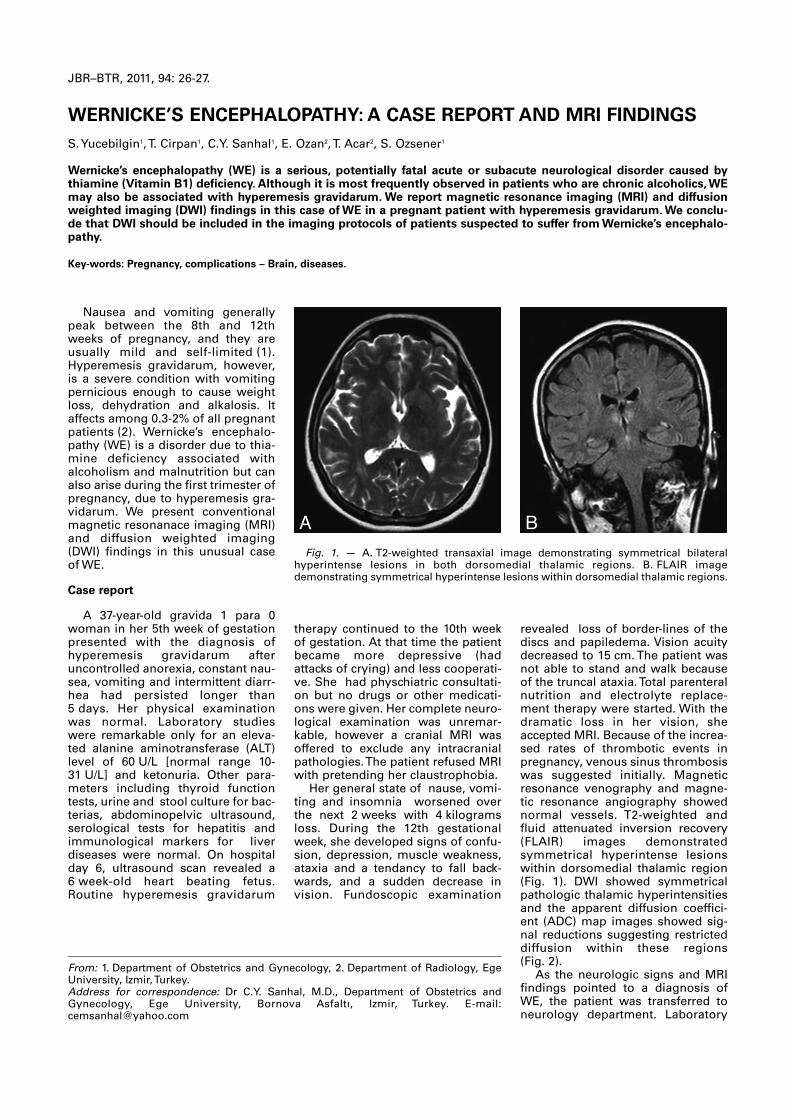
Nausea and vomiting generallypeak between the 8th and 12thweeks of pregnancy, and they areusually mild and self-limited (1).Hyperemesis gravidarum, however,is a severe condition with vomitingpernicious enough to cause weightloss, dehydration and alkalosis. Itaffects among 0.3-2% of all pregnantpatients (2). Wernicke’s encephalo-pathy (WE) is a disorder due to thia-mine deficiency associated withalcoholism and malnutrition but canalso arise during the first trimester ofpregnancy, due to hyperemesis gra-vidarum. We present conventionalmagnetic resonanace imaging (MRI)and diffusion weighted imaging(DWI) findings in this unusual caseof WE.
Case report
A 37-year-old gravida 1 para 0woman in her 5th week of gestationpresented with the diagnosis ofhyperemesis gravidarum afteruncontrolled anorexia, constant nau-sea, vomiting and intermittent diarr-hea had persisted longer than5 days. Her physical examinationwas normal. Laboratory studieswere remarkable only for an eleva-ted alanine aminotransferase (ALT)level of 60 U/L [normal range 10-31 U/L] and ketonuria. Other para-meters including thyroid functiontests, urine and stool culture for bac-terias, abdominopelvic ultrasound,serological tests for hepatitis andimmunological markers for liverdiseases were normal. On hospitalday 6, ultrasound scan revealed a6 week-old heart beating fetus.Routine hyperemesis gravidarum
revealed loss of border-lines of thediscs and papiledema. Vision acuitydecreased to 15 cm. The patient wasnot able to stand and walk becauseof the truncal ataxia. Total parenteralnutrition and electrolyte replace-ment therapy were started. With thedramatic loss in her vision, sheaccepted MRI. Because of the increa-sed rates of thrombotic events inpregnancy, venous sinus thrombosiswas suggested initially. Magneticresonance venography and magne-tic resonance angiography showednormal vessels. T2-weighted andfluid attenuated inversion recovery(FLAIR) images demonstratedsymmetrical hyperintense lesionswithin dorsomedial thalamic region(Fig. 1). DWI showed symmetricalpathologic thalamic hyperintensitiesand the apparent diffusion coeffici-ent (ADC) map images showed sig-nal reductions suggesting restricteddiffusion within these regions(Fig. 2).As the neurologic signs and MRI
findings pointed to a diagnosis ofWE, the patient was transferred toneurology department. Laboratory
therapy continued to the 10th weekof gestation. At that time the patientbecame more depressive (hadattacks of crying) and less cooperati-ve. She had physchiatric consultati-on but no drugs or other medicati-ons were given. Her complete neuro-logical examination was unremar-kable, however a cranial MRI wasoffered to exclude any intracranialpathologies. The patient refused MRIwith pretending her claustrophobia.Her general state of nause, vomi-
ting and insomnia worsened overthe next 2 weeks with 4 kilogramsloss. During the 12th gestationalweek, she developed signs of confu-sion, depression, muscle weakness,ataxia and a tendancy to fall back-wards, and a sudden decrease invision. Fundoscopic examination
JBR–BTR, 2011, 94: 26-27.
WERNICKE’S ENCEPHALOPATHY: A CASE REPORT AND MRI FINDINGSS. Yucebilgin1, T. Cirpan1, C.Y. Sanhal1, E. Ozan2, T. Acar2, S. Ozsener1
Wernicke’s encephalopathy (WE) is a serious, potentially fatal acute or subacute neurological disorder caused by thiamine (Vitamin B1) deficiency. Although it is most frequently observed in patients who are chronic alcoholics, WEmay also be associated with hyperemesis gravidarum. We report magnetic resonance imaging (MRI) and diffusionweighted imaging (DWI) findings in this case of WE in a pregnant patient with hyperemesis gravidarum. We conclu-de that DWI should be included in the imaging protocols of patients suspected to suffer from Wernicke’s encephalo-pathy.
Key-words: Pregnancy, complications – Brain, diseases.
From: 1. Department of Obstetrics and Gynecology, 2. Department of Radiology, EgeUniversity, Izmir, Turkey.Address for correspondence: Dr C.Y. Sanhal, M.D., Department of Obstetrics andGynecology, Ege University, Bornova Asfaltı, Izmir, Turkey. E-mail:[email protected]
Fig. 1. — A. T2-weighted transaxial image demonstrating symmetrical bilateralhyper intense lesions in both dorsomedial thalamic regions. B. FLAIR image demonstrating symmetrical hyperintense lesions within dorsomedial thalamic regions.
A B
yucebilgin-_Opmaak 1 16/02/11 09:36 Pagina 26
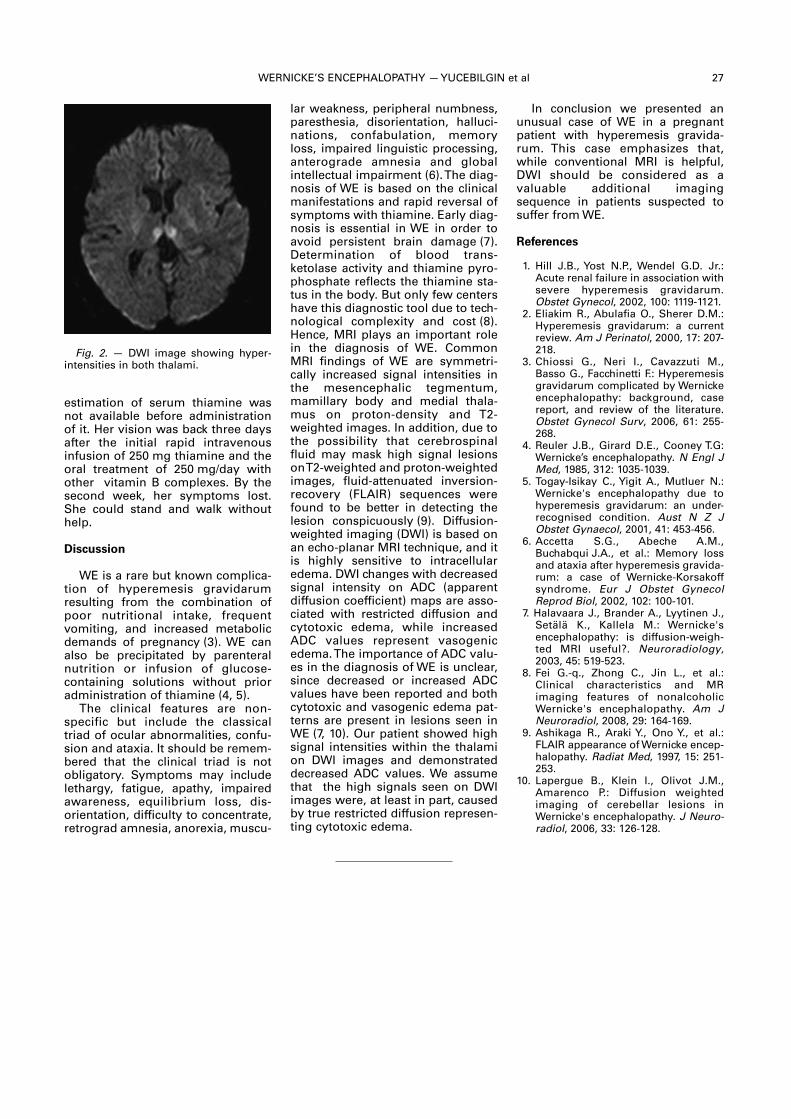
WERNICKE’S ENCEPHALOPATHY — YUCEBILGIN et al 27
estimation of serum thiamine wasnot available before administrationof it. Her vision was back three daysafter the initial rapid intravenousinfusion of 250 mg thiamine and theoral treatment of 250 mg/day withother vitamin B complexes. By thesecond week, her symptoms lost.She could stand and walk withouthelp.
Discussion
WE is a rare but known complica-tion of hyperemesis gravidarumresulting from the combination ofpoor nutritional intake, frequentvomiting, and increased metabolicdemands of pregnancy (3). WE canalso be precipitated by parenteralnutrition or infusion of glucose- containing solutions without prioradministration of thiamine (4, 5).The clinical features are non-
specific but include the classicaltriad of ocular abnormalities, confu-sion and ataxia. It should be remem-bered that the clinical triad is notobligatory. Symptoms may includelethargy, fatigue, apathy, impairedawareness, equilibrium loss, dis -orientation, difficulty to concentrate,retrograd amnesia, anorexia, muscu-
In conclusion we presented anunusual case of WE in a pregnantpatient with hyperemesis gravida-rum. This case emphasizes that,while conventional MRI is helpful,DWI should be considered as a valuable additional imaging sequence in patients suspected tosuffer from WE.
References
1. Hill J.B., Yost N.P., Wendel G.D. Jr.:Acute renal failure in association withsevere hyperemesis gravidarum.Obstet Gynecol, 2002, 100: 1119-1121.
2. Eliakim R., Abulafia O., Sherer D.M.:Hyperemesis gravidarum: a currentreview. Am J Perinatol, 2000, 17: 207-218.
3. Chiossi G., Neri I., Cavazzuti M.,Basso G., Facchinetti F.: Hyperemesisgravidarum complicated by Wernickeencephalopathy: background, casereport, and review of the literature.Obstet Gynecol Surv, 2006, 61: 255-268.
4. Reuler J.B., Girard D.E., Cooney T.G:Wernicke’s encephalopathy. N Engl JMed, 1985, 312: 1035-1039.
5. Togay-Isikay C., Yigit A., Mutluer N.:Wernicke's encephalopathy due tohyperemesis gravidarum: an under-recognised condition. Aust N Z JObstet Gynaecol, 2001, 41: 453-456.
6. Accetta S.G., Abeche A.M.,Buchabqui J.A., et al.: Memory lossand ataxia after hyperemesis gravida-rum: a case of Wernicke-Korsakoffsyndrome. Eur J Obstet GynecolReprod Biol, 2002, 102: 100-101.
7. Halavaara J., Brander A., Lyytinen J.,Setälä K., Kallela M.: Wernicke'sencephalopathy: is diffusion-weigh-ted MRI useful?. Neuroradiology,2003, 45: 519-523.
8. Fei G.-q., Zhong C., Jin L., et al.:Clinical characteristics and MR imaging features of nonalcoholicWernicke's encephalopathy. Am JNeuroradiol, 2008, 29: 164-169.
9. Ashikaga R., Araki Y., Ono Y., et al.:FLAIR appearance of Wernicke encep-halopathy. Radiat Med, 1997, 15: 251-253.
10. Lapergue B., Klein I., Olivot J.M.,Amarenco P.: Diffusion weighted imaging of cerebellar lesions inWernicke's encephalopathy. J Neuro -radiol, 2006, 33: 126-128.
lar weakness, peripheral numbness,paresthesia, disorien tation, halluci-nations, confabulation, memoryloss, impaired linguistic processing,anterograde amnesia and globalintellectual impairment (6). The diag-nosis of WE is based on the clinicalmanifestations and rapid reversal ofsymptoms with thiamine. Early diag-nosis is essential in WE in order toavoid persistent brain damage (7).Determination of blood trans -ketolase activity and thiamine pyro -phosphate reflects the thiamine sta-tus in the body. But only few centershave this diagnostic tool due to tech-nological complexity and cost (8).Hence, MRI plays an important rolein the diagnosis of WE. CommonMRI findings of WE are symmetri-cally increased signal intensities inthe mesencephalic tegmentum,mamillary body and medial thala-mus on proton-density and T2-weighted images. In addition, due tothe possibility that cerebrospinalfluid may mask high signal lesionson T2-weighted and proton-weightedimages, fluid-attenuated inversion-recovery (FLAIR) sequences werefound to be better in detecting thelesion conspicuously (9). Diffusion-weighted imaging (DWI) is based onan echo-planar MRI technique, and itis highly sensitive to intracellularedema. DWI changes with decreasedsignal intensity on ADC (apparentdiffusion coefficient) maps are asso-ciated with restricted diffusion andcytotoxic edema, while increasedADC values represent vasogenicedema. The importance of ADC valu-es in the diagnosis of WE is unclear,since decreased or increased ADCvalues have been reported and bothcytotoxic and vasogenic edema pat-terns are present in lesions seen inWE (7, 10). Our patient showed highsignal intensities within the thalamion DWI images and demonstrateddecreased ADC values. We assumethat the high signals seen on DWIimages were, at least in part, causedby true restricted diffusion represen-ting cytotoxic edema.
Fig. 2. — DWI image showing hyper -intensities in both thalami.
yucebilgin-_Opmaak 1 16/02/11 09:36 Pagina 27

Biphosphonates are not com -monly used in childhood and adoles-cence youth except for very specificentities like osteogenesis imperfec-ta, recurrent multifocal osteomyelitisand juvenile osteoporosis. We reporta very rare case of diffuse alterationof the vertebral bony structure fortu-itously found in a 20-year-old patientand essentially characterized by animpressive “vertebra-within-verte-bra” appearance. This aspect wasfound being the result of an unusualuse of intravenous perfusions ofbiphosphonate (Pamidronate) duringearly adolescence (at the age ofeleven) for – probably overestimat-ed – reflex sympathetic dystrophyafter tibial fracture. The clinical appli-cations of biphosphonates arebriefly remembered and the phys-iopathology of the induced bonechanges is explained.
Case report
A 20-year-old patient was referredfor X-ray evaluation of spine after acar accident. He presented with complaints of moderate low backpain. Plain films failed to reveal anyvertebral fracture but demonstratedatypical uniform diffuse alterationsof the vertebral structure. All verte-bral bodies were delineated by adouble bony cortex creating animpressing "bone-within-bone" or"vertebra-within-vertebra" appear-ance. Duplication of the bony cortexwas also found at the level of theiliac crests, acetabular roofs, sacroil-iac joints and vertebral spinousprocesses (Fig. 1, 2). The patient wasunsuccessfully questioned about theoccurrence of serious medical
illustrated) at the age of eleven. Twomonths after trauma a diagnosis of– probably overestimated – reflexsympathetic dystrophy (RSD) wasevocated on the basis of clinicalsigns, plain films and bone scintigra-phy (not illustrated). The patientreceived intravenous perfusionsof biphosphonate (pamidronate).
events during childhood or earlyadolescence. Fortunately a revue ofhis medical records revealed a history of tibiofibular fracture (not
JBR–BTR, 2011, 94: 28-30.
DIFFUSE “VERTEBRA-WITHIN-VERTEBRA” APPEARANCE AT THE ADULTAGE DUE TO BIPHOSPHONATE (PAMIDRONATE) ADMINISTRATION DURING EARLY ADOLESCENCEB. Coulier1
We report a rare case of diffuse alteration of the vertebral bony structure fortuitously found in a 20-year-old patientand essentially characterized by an impressive “vertebra-within-vertebra” appearance. This aspect was found beingthe result of an unusual use of intravenous perfusions of biphosphonate (Pamidronate) during early adolescence forreflex sympathetic dystrophy after tibial fracture. The clinical applications of biphosphonates are briefly reminded andthe physiopathology of the induced bone changes is explained.
Key-words: Biphosphonates – Bones, growth and development – Children, skeletal system.
From: 1. Department of Diagnostic Radiology , Clinique St Luc, Bouge (Namur), Belgium.Address for correspondence: Dr B. Coulier, M.D., Department of Diagnostic Radiology,Clinique St Luc, Rue St Luc 8, 5004 Bouge (Namur). Belgium. E-mail: [email protected]
Fig. 1. — Lateral plains films of the thoracic (A) and lumbar (B) spine. Vertebral bod-ies are all delineated by a double bony cortex creating an impressing "bone-within-bone" or "vertebra-within-vertebra" configuration (black arrows). Duplication of thebony cortex is also visible at the level the vertebral spinous processes (white arrows).
A B
coulier(vertebra)_Opmaak 1 16/02/11 09:46 Pagina 28
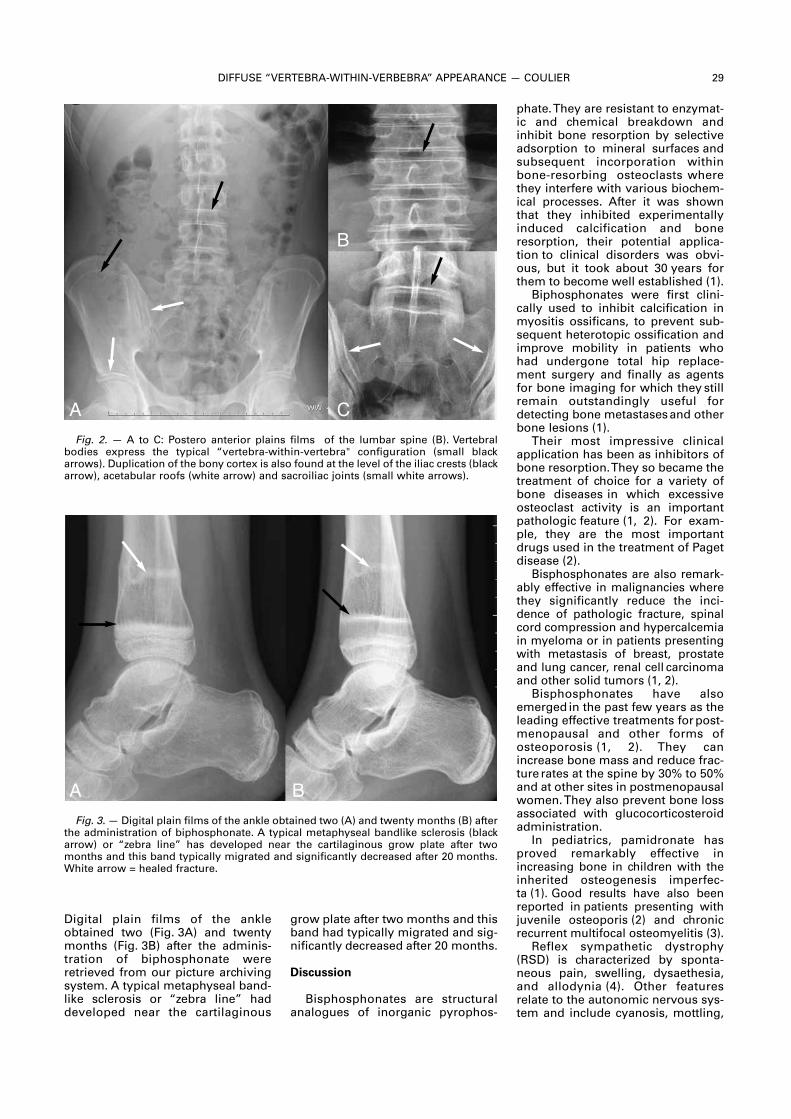
DIFFUSE “VERTEBRA-WITHIN-VERBEBRA” APPEARANCE — COULIER 29
Digital plain films of the ankleobtained two (Fig. 3A) and twentymonths (Fig. 3B) after the adminis-tration of biphosphonate wereretrieved from our picture archivingsystem. A typical metaphyseal band-like sclerosis or “zebra line” haddeveloped near the cartilaginous
phate. They are resistant to enzymat-ic and chemical breakdown andinhibit bone resorption by selectiveadsorption to mineral surfaces andsubsequent incorporation withinbone-resorbing osteoclasts wherethey interfere with various biochem-ical processes. After it was shownthat they inhibited experimentallyinduced calcification and boneresorption, their potential applica-tion to clinical disorders was obvi-ous, but it took about 30 years forthem to become well established (1).
Biphosphonates were first clini-cally used to inhibit calcification inmyositis ossificans, to prevent sub-sequent heterotopic ossification andimprove mobility in patients whohad undergone total hip replace-ment surgery and finally as agentsfor bone imaging for which they stillremain outstandingly useful fordetecting bone metastasesand otherbone lesions (1).
Their most impressive clinicalapplication has been as inhibitors ofbone resorption. They so became thetreatment of choice for a variety ofbone diseases in which excessiveosteoclast activity is an importantpathologic feature (1, 2). For exam-ple, they are the most importantdrugs used in the treatment of Pagetdisease (2).
Bisphosphonates are also remark-ably effective in malignancies wherethey significantly reduce the inci-dence of pathologic fracture, spinalcord compression and hypercalcemiain myeloma or in patients presentingwith metastasis of breast, prostateand lung cancer, renal cell carcinomaand other solid tumors (1, 2).
Bisphosphonates have alsoemerged in the past few years as theleading effective treatments forpost-menopausal and other forms ofosteoporosis (1, 2). They canincrease bone mass and reduce frac-ture rates at the spine by 30% to 50%and at other sites in postmenopausalwomen. They also prevent bone lossassociated with glucocorticosteroidadministration.
In pediatrics, pamidronate hasproved remarkably effective inincreasing bone in children with theinherited osteogenesis imperfec-ta (1). Good results have also beenreported in patients presenting withjuvenile osteoporis (2) and chronicrecurrent multifocal osteo myelitis (3).
Reflex sympathetic dystrophy(RSD) is characterized by sponta-neous pain, swelling, dysaethesia,and allodynia (4). Other featuresrelate to the autonomic nervous sys-tem and include cyanosis, mottling,
grow plate after two months and thisband had typically migrated and sig-nificantly decreased after 20 months.
Discussion
Bisphosphonates are structuralanalogues of inorganic pyrophos-
Fig. 2. — A to C: Postero anterior plains films of the lumbar spine (B). Vertebral bodies express the typical “vertebra-within-vertebra" configuration (small blackarrows). Duplication of the bony cortex is also found at the level of the iliac crests (blackarrow), acetabular roofs (white arrow) and sacroiliac joints (small white arrows).
Fig. 3.— Digital plain films of the ankle obtained two (A) and twenty months (B) afterthe administration of biphosphonate. A typical metaphyseal bandlike sclerosis (blackarrow) or “zebra line” has developed near the cartilaginous grow plate after twomonths and this band typically migrated and significantly decreased after 20 months.White arrow = healed fracture.
A
B
C
A B
coulier(vertebra)_Opmaak 1 16/02/11 09:46 Pagina 29

30 JBR–BTR, 2011, 94 (1)
sweating and reduction in tempera-ture. In some cases more permanentand serious features may developincluding muscle atrophy, deminer-alization of bone, and contracturesof soft tissue around the affectedjoint. There is currently great contro-versy over the pathogenesis ofRSD (5). Some authors believe thatthe disease is the result of a post-traumatic reflexive neuronal mecha-nism which leads to abnormal painperception and exacerbated efferentsympathetic activity (5).
Innumerable conditions are asso-ciated with the development of RSDbut in more than 60% of casesdescribed in adults there is a historyof trauma.
Among pediatrics RSD is consid-ered as being a rare and under-diag-nosed event. The history of trauma isless common and, when present,usually of lesser intensity. RSD usually involves children in latechildhood or early adolescence, witha mean age of onset of 12-13 yearsand a higher frequency in girls thanboys (5).
Bisphosphonates were proposedin the treatment of RSD due to theiraction as potent osteoclast-blockingagents (6). Pamidronate appeared tobe effective and well tolerated in thetreatment of refractory RSD (6-8).Use of pamidronate as the first-intention treatment for RSD can alsobe proposed (2). However, there aretwo limiting factors: the cost ofamidronate and the need for intra-venous administration. Osteo -necrosis of the jaw (ONJ) has beendescribed as a complication of bisphosphonate therapy in adultsbut not among paediatric patients upto now (9).
The occurrence of metaphysealbandlike sclerosis (and in minder pro-portion of metaphyseal undertubula-tion) induced by biphosphonates isprobably the result of the establish-ment of a new equilibrium betweenosteoblastic and osteoclastic activitywithin the bone after an initial phaseof inhibition of osteoclastic activitywithout equal decrease in theosteoblastic activity (10). The relativeresultant increase in bone formationin addition to the already high level ofosteoblastic activity near the growthplates result in the development ofsclerosis in the growing child.Multiple linear bands of increasedbone density have also beendescribed at the metaphysic of longbones in children receiving cyclicalpamidronate infusions. The same
2. Devogelaer J.P.: Treatment of bonediseases with bisphosphonates,excluding osteoporosis. Curr OpinRheumatol, 2000, 12: 331-335.
3. Gleeson H., Wiltshire E., Briody J., etal.: Childhood chronic recurrent mul-tifocal osteomyelitis: pamidronatetherapy decreases pain and improvesvertebral shape. J Rheumatol, 2008,35: 707-712.
4. Maillefert J.F., Chatard C., Owen S., etal.: Treatment of refractory reflexsympathetic dystrophy withpamidronate. Ann Rheum Dis, 1995,54: 687.
5. Lotito A.P., Campos L.M., Dias M.H.,Silva C.A.: Reflex sympathetic dystro-phy. J Pediatr (Rio J), 2004, 80: 159-162.
6. Kubalek I., Fain O., Paries J.,Kettaneh A., Thomas M.: Treatment ofreflex sympathetic dystrophy withpamidronate: 29 cases. Rheuma -tology (Oxford), 2001, 40: 1394-1397.
7. Simm P.J., Briody J., McQuade M.,Munns C.F.: The successful use ofpamidronate in an 11-year-old girlwith complex regional pain syn-drome: response to treatmentdemonstrated by serial peripheralquantitative computerised tomo-graphic scans. Bone, 2010,46: 885-888.
8. Adami S., Fossaluzza V., Gatti D.,Fracassi E., Braga V.: Bisphosphonatetherapy of reflex sympathetic dystro-phy syndrome. Ann Rheum Dis, 1997,56: 201-204.
9. Chahine C., Cheung M.S., Head T.W.,et al.: Tooth extraction socket healingin pediatric patients treated withintravenous pamidronate. J Pediatr,2008, 153: 719-720.
10. van Persijn van Meerten E.L.,Kroon H.M., Papapoulos S.E.: Epi-and metaphyseal changes in childrencaused by administration of bisphos-phonates. Radiology, 1992 ,184: 249-254.
11. Davies J.H., Gregory J.W.:Radiographic long bone appearancein a child administered cyclicalpamidronate. Arch Dis Child, 2003,88: 854.
12. Srinivasan R.: Pamidronate lines.Indian Pediatr, 2005, 42: 959-960.
13. Grissom L.E., Harcke H.T.:Radiographic features of bisphospho-nate therapy in pediatric patients.Pediatr Radiol, 2003,33: 226-229.
14. Devogelaer J.P., Malghem J.,Maldague B., Nagant deDeuxchaisnes C.: Radiological mani-festations of bisphosphonate treat-ment with APD in a child sufferingfrom osteogenesis imperfecta.Skeletal Radiol, 1987, 16: 360-363.
15. Vanhoenacker F.M., DeBeuckeleer L.H., Van Hul W., et al.:Sclerosing bone dysplasias: Geneticand radioclinical features. Eur Radiol,2000;10: 1423-1433.
phenomenon in areas of concentricbone growth (epi- and apophysesand vertebral bodies) causes ringlikesclerosis resulting in bone-within-bone or vertebra-within-vertebraappearance (11-14).
A gradual decrease in the degreeof sclerosis has been observed afterdiscontinuation of medication beforethe closure of the growth plates andin patients receiving medication afterclosure. This observation is probablydue to a return to a normal level ofbone turnover with a gradual replace-ment of the sclerotic bone by bonewith normal density. The disappear-ance of metaphyseal sclerosis in fol-low-up studies in individual subjectshas suggested that sclerosis was acompletely reversible phenomenon.
A bone-within-bone appearanceis a rare finding. In children, thisappearance can occur after boneinfarction in sickle cell anemia andGaucher disease. In these disorders,however, this abnormality is mostcommonly seen in the diaphyses ofthe long tubular bones and is rarelygeneralized. It can also accompanyheavy metal intoxication and can bea normal finding in the spine ofneonates (10).
Sclerosing bone dysplasias mustalso be mentioned. These diseasesare classified into three groups: dys-plasias of endochondral bone forma-tion (essentially affecting the spon-giosa), dysplasias of intramembra-nous bone formation (essentiallyaffecting the diaphysis) and mixedsclerosing dysplasia. Among dys-plasias of endochondral bone forma-tion type II autosomal-dominant(adult type) osteopetrosis andosteopathia striata can commonlyshow the bone-within-bone appear-ance and/or dense striations (15).
The persistence of bone-within-bone in the axial skeleton of thereported case appears ratherremarkable and has, to our knowl-edge only exceptionally been report-ed (10, 14). The reason probablyresides in the fact that biphospho-nates are not currently used as firstline treatment of reflex sympatheticdystrophy during early adolescence.Moreover the opportunity to fortu-itously obtain plain films of the spinein a young adult who has receivedthis atypical treatment during growis extremely uncommon.
Bibliography
1. Russell R.G.: Bisphosphonates: modeof action and pharmacology.Pediatrics, 2007,119: 150-162.
coulier(vertebra)_Opmaak 1 16/02/11 09:46 Pagina 30

Case report
A 24-year-old man was admittedto the hospital for investigation ofretrosternal pain suggestive of peri-carditis. Initial investigationsrevealed a CRP level of 3.4 mg/dl anddiscrete ECG changes confirming thesuspicion of pericarditis. A contrastenhanced computed tomography(CT) examination of the chest andthe upper abdomen was performedto rule out conditions such as pul-monary embolism and aortic dissec-tion, but the examination showed noabnormalities. However, it was inci-dentally noted that a solid contrastcaptating nodule of 2 cm was pres-ent posteriorly in the interpolarregion of the left kidney (Fig. 1A). Thekidney otherwise appeared normaland no other abdominal abnormali-ties were seen. The patient subse-quently underwent a gadoliniumenhanced magnetic resonance imag-ing (MRI) study of the kidneys onwhich the presence of the nodulewas confirmed. The mass was hypo-intense on the T1- and T2-weightedimages (Fig. 1B), and showed slightenhancement after intravenousinjection of gadolinium (Fig. 1C). Apartial nephrectomy was performed.The anatomopathological analysis ofthe nodule showed an oncocytoma.Postoperatively our young patientsurprisingly showed a left-sidedpneumothorax. The pneumothoraxresolved within 5 days after chestdrain insertion.
The history of our patientrevealed that one month prior to thisadmission, our patient was treated
nose and cheeks. About 25% of theFLCN-mutation carriers do not mani-fest skin lesions (1).
The most threatening complica-tion of BHD syndrome is renal cancer. In a series of 124 individualswith BHD, 27% of the patients hadrenal tumours at a mean age of50.4 years (range 31-74 years) (2).The earliest reported age at diagno-sis of renal cancer in a patient withBHD syndrome is 20 years (3). Aunique characteristic of this condi-tion is the mixture of histologicaltypes of renal tumours seen in a single kidney or patient, with chromophobe renal cell carcinoma(RCC), clear cell RCC and oncocy-toma respectively accounting for upto 34%, 9% and 8% of the cases (4).In addition to this, the presence ofdifferent cell populations within anindividual tumour, the so-calledhybrid oncocytic tumour (50%), isfrequently observed in BHD patients.Furthermore, kidney tumours in BHDsyndrome usually occur earlier thansporadic tumours and are generallymultiple and bilateral (5). This is notthe case in our patient. Therefore afamilial history of renal cancer, thediagnosis of early-onset renal cancer(< 50 years), or the presence of multiple bilateral kidney tumoursshould raise suspicion of BHD syndrome, particularly if the pre-dominant histological type is chromophobe renal cell carcinomaor hybrid oncocytic tumour. CT andMRI usually show multiple, bilateral,heterogeneous, solid renal massesthat demonstrate heterogeneousenhancement after contrast adminis-tration. In our patient the family history of a malignant renal tumourand the discovery of a benign onco-cytoma at the age of 24, were cluesto the diagnosis of BHD syndrome.
On CT examination of the thorax,more than 80% of adult patients withBHD have multiple lung cysts. It isknown that pulmonary cysts mayrupture under the pressure of
for a primary left-sided pneumotho-rax with thoracoscopic pleurectomyand basal bullectomy after chestdrainage had failed (Fig. 1D). Thepatient also had a known history ofulcerative colitis, for which he hadbeen under treatment for severalyears. Furthermore, family historyrevealed that our patients father diedat a young age due to renal cancer.Because of the wide variety of clini-cal problems present in a youngpatient and because of his familyhistory of renal cancer, our patientwas referred for genetic counselling.Molecular genetic research con-firmed the diagnosis of Birt-Hogg-Dubé (BHD) syndrome, a rare auto-somal dominant disorder.
Discussion
Birt-Hogg-Dubé syndrome is arare autosomal dominant conditioncharacterised by benign tumours ofthe hair follicle, renal tumours of dif-ferent histological types, pulmonarycysts, and spontaneous pneumotho-races. The condition is caused bygermline mutations in the FLCNgene, which encodes folliculin. Atpresent about 200 families with BHDsyndrome with pathogenic FLCNmutations have been reportedworldwide. BHD syndrome is proba-bly under-diagnosed because of thewide variability in its clinical expres-sion. Patients might present withrenal cancer or pneumothorax, con-ditions that generally occur sporadi-cally. The skin lesions usually appearafter the age of 20 years, as multipledome-shaped, whitish papules on
JBR–BTR, 2011, 94: 31-33.
INCIDENTAL RADIOLOGICAL FINDING OF A RENAL TUMOUR LEADING TOTHE DIAGNOSIS OF BIRT-HOGG-DUBE SYNDROMEM. Schreuer1,2, M. Lemmerling2, W. Pauwels3, D. Dewilde2, C. Heyse1,2, K.L. Verstraete1
Birt-Hogg-Dubé (BHD) syndrome is a rare autosomal dominant condition characterised by benign tumours of the hairfollicle, renal cancer, pulmonary cysts and spontaneous pneumothorax. We report the diagnosis of a BHD syndromeachieved after incidental radiological finding of a renal tumour in a 24-year old man. The patient also displayed recurrent pneumothoraces and showed to have cysts in the basis of both lungs. The association of recurrent pneumo -thoraces and renal neoplastic disease should alert for the possible presence of this syndrome.
Key-word: Oncocytoma.
From: 1. Department of Radiology UZ Gent, 2. Department of Radiology AZ Sint-LucasHospital Gent, 3. Department of Gastroenterology AZ Sint-Lucas Hospital Gent,Belgium.Address for correspondence: Dr M. Lemmerling, Department of Radiology, AZ Sint-Lucas Hospital Gent, Groenebriel 1, B-9000 Gent, Belgium.E-mail: [email protected]
schreuer-_Opmaak 1 16/02/11 09:48 Pagina 31
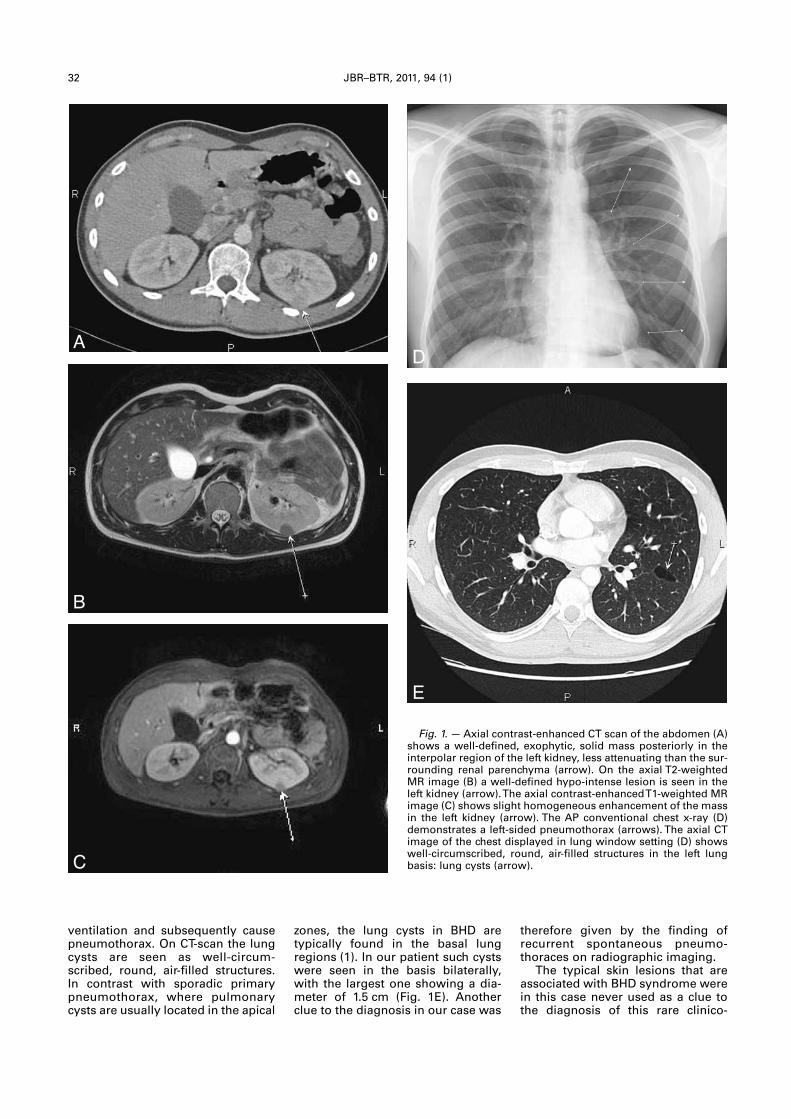
32 JBR–BTR, 2011, 94 (1)
ventilation and subsequently causepneumothorax. On CT-scan the lungcysts are seen as well-circum-scribed, round, air-filled structures.In contrast with sporadic primarypneumothorax, where pulmonarycysts are usually located in the apical
therefore given by the finding ofrecurrent spontaneous pneumo -thoraces on radiographic imaging.
The typical skin lesions that areassociated with BHD syndrome werein this case never used as a clue tothe diagnosis of this rare clinico-
zones, the lung cysts in BHD are typically found in the basal lungregions (1). In our patient such cystswere seen in the basis bilaterally,with the largest one showing a dia -meter of 1.5 cm (Fig. 1E). Anotherclue to the diagnosis in our case was
Fig. 1.— Axial contrast-enhanced CT scan of the abdomen (A)shows a well-defined, exophytic, solid mass posteriorly in theinterpolar region of the left kidney, less attenuating than the sur-rounding renal parenchyma (arrow). On the axial T2-weightedMR image (B) a well-defined hypo-intense lesion is seen in theleft kidney (arrow). The axial contrast-enhanced T1-weighted MRimage (C) shows slight homogeneous enhancement of the massin the left kidney (arrow). The AP conventional chest x-ray (D)demonstrates a left-sided pneumothorax (arrows). The axial CTimage of the chest displayed in lung window setting (D) showswell-circumscribed, round, air-filled structures in the left lungbasis: lung cysts (arrow).
A
B
C
E
D
schreuer-_Opmaak 1 16/02/11 09:48 Pagina 32

BIRTH-HOGG-DUBE SYNDROME — SCHREUER et al 33
pathologic condition. Concerningthe initial complaints, the retro -sternal pain was most likely theresult of a viral pericarditis of whichour patient steadily recovered. Thispericarditis episode was probablyunrelated to the syndrome.
Finally, since our patient is knownwith ulcerative colitis, we alsosearched for a possible link betweenulcerative colitis and BHD syndrome,but as far as we know no other casesof BHD syndrome have been report-ed in combination with inflammato-ry bowel disease. Throughout theyears, a number of pathological conditions have been linked to BHDsyndrome. Intestinal polyps havebeen described more than once incombination with BHD syndrome,but no association was demonstrat-ed so far. The general consensusnow is that patients with BHD syndrome are not at risk for colonpolyps or colonic adenocarcino-ma (6, 7). Due to the risk of renalcancers for individuals who have afamily history of BHD syndrome, different surveillance programs havebeen suggested aimed at earlyrecognition and treatment of cancer.A yearly MRI scan of the kidneysstarting at the age of 20 years isprobably best, but the exact role of
Hammel P., Bergerheim U.,Hedblad M.A., Bradley M., Teh B.T.,Nordenskjöld M., Richard S.: Clinicaland genetic studies of Birt-Hogg-Dubé syndrome. J Med Genet, 2002,39: 906-912.
4. Pavlovich C.P., Walther M.M.,Eyler R.A., Hewitt S.M., Zbar B.,Linehan W.M., Merino M.J.: Renaltumors in the Birt-Hogg-dubé syn-drome. Am J Surg Pathol, 2002, 26:1542-1552.
5. Weirich G., Junker K., Salles P.G.O.,Lim S.D., de Peralta-Venturina M.N.,Alvarado-Cabrero I., Jimenez R.E.,Cabras A.D., Höfler H., Schubert J.,Amin M.B.: Comparative genomichybridization analysis of renal onco-cytomas (RO), chromophobe renalcell carcinomas (CHRCC) and tumorswith hybrid histology – HybridOncocytic Tumors (HOT). ModernPathology, 2002, 15: 186.
6. Adley B.P., Smith N.D., Nayar R.,Yang X.J.: Birt-Hogg-Dubé syndrome:clinicopathologic findings and genet-ic alterations. Arch Pathol Lab Med,2006, 130: 1865-1870.
7. Zbar B., Alvord W.G., Glenn G.,Turner M., Pavlovich C.P., Schmidt L.,Walther M., Choyke P., Weirich G.,Hewitt S.M., Duray P., Gabril F.,Greenberg C., Merino M.J., Toro J.,Linehan W.M.: Risk of renal andcolonic neoplasm and spontaneouspneumothorax in the Birt-Hogg-Dubésyndrome. Cancer EpidemiolBiomarkers Prev, 2002, 11: 393-400.
CT and ultrasonography has notbeen fully investigated (1).
In conclusion, we describe thecase of a patient with the rare Birt-Hogg-Dubé syndrome, a probablyunderdiagnosed syndrome that ispassed on to following generationsin an autosomal dominant fashion.Recurrent pneumothoraces withcysts in the basis of the lungs ratherthan in the apical regions in associa-tion with renal neoplastic diseaseshould alert for the possible pres-ence of this syndrome.
References
1. Menko F.H., van Steensel M.A.,Giraud S., Friis-Hansen L., Richard S.,Ungari S., Nordenskjöld M.,Hansen T.V., Solly J., Maher ER.: Birt-Hogg-Dubé syndrome: diagnosis andmanagement. Lancet Oncol, 2009, 10:1199-1206.
2. Pavlovich C.P., Grubb R.L., Hurley K.,Glenn G.M., Toro J., Schmidt L.S.,Torres-Cabala C., Merino M.J.,Zbar B., Choyke P., Walther M.M.,Linehan W.M.: Evaluation and man-agement of renal tumors in the Birt-Hogg-Dubé syndrome. J Urol, 2005,173: 1482-1486.
3. Khoo S.K., Giraud S., Kahnoski K.,Chen J., Motorna O., Nickolov R.,Binet O., Lambert D., Friedel J.,Lévy R., Ferlicot S., Wolkenstein P.,
schreuer-_Opmaak 1 16/02/11 09:48 Pagina 33
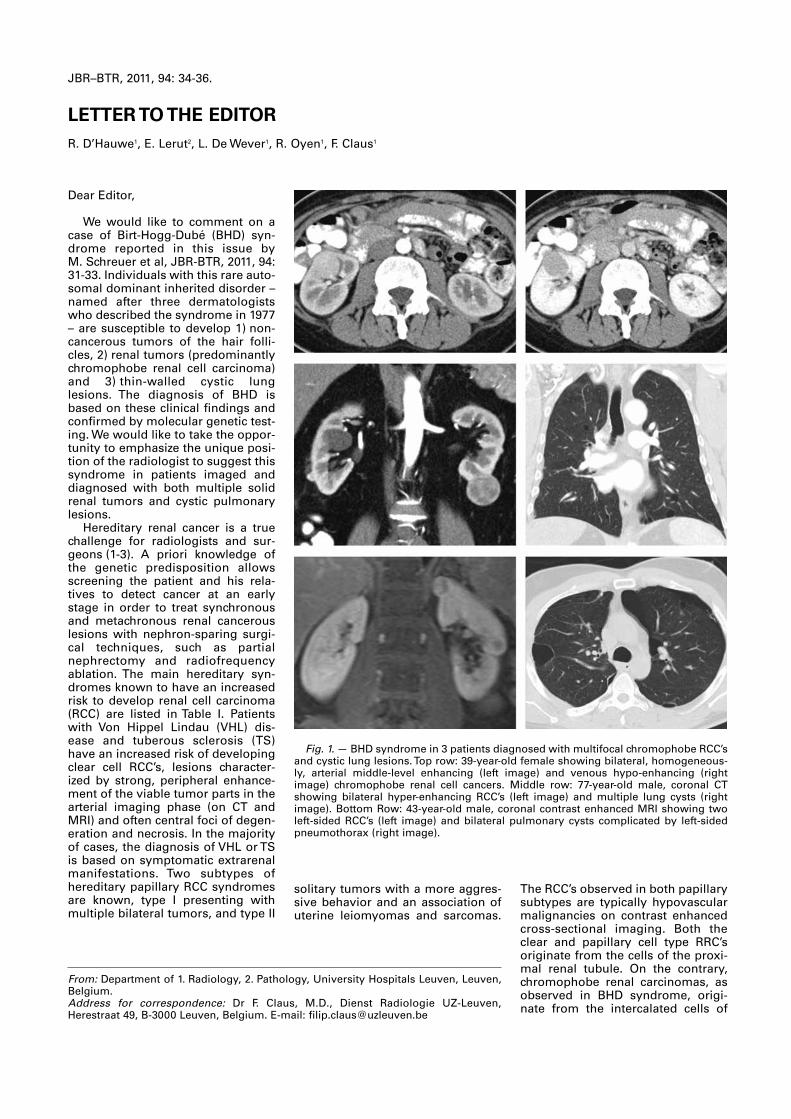
Dear Editor,
We would like to comment on acase of Birt-Hogg-Dubé (BHD) syn-drome reported in this issue byM. Schreuer et al, JBR-BTR, 2011, 94:31-33. Individuals with this rare auto-somal dominant inherited disorder –named after three dermatologistswho described the syndrome in 1977– are susceptible to develop 1) non-cancerous tumors of the hair folli-cles, 2) renal tumors (predominantlychromophobe renal cell carcinoma)and 3) thin-walled cystic lunglesions. The diagnosis of BHD isbased on these clinical findings andconfirmed by molecular genetic test-ing. We would like to take the oppor-tunity to emphasize the unique posi-tion of the radiologist to suggest thissyndrome in patients imaged anddiagnosed with both multiple solidrenal tumors and cystic pulmonarylesions.
Hereditary renal cancer is a truechallenge for radiologists and sur-geons (1-3). A priori knowledge ofthe genetic predisposition allowsscreening the patient and his rela-tives to detect cancer at an earlystage in order to treat synchronousand metachronous renal cancerouslesions with nephron-sparing surgi-cal techniques, such as partialnephrectomy and radiofrequencyablation. The main hereditary syn-dromes known to have an increasedrisk to develop renal cell carcinoma(RCC) are listed in Table I. Patientswith Von Hippel Lindau (VHL) dis-ease and tuberous sclerosis (TS)have an increased risk of developingclear cell RCC’s, lesions character-ized by strong, peripheral enhance-ment of the viable tumor parts in thearterial imaging phase (on CT andMRI) and often central foci of degen-eration and necrosis. In the majorityof cases, the diagnosis of VHL or TSis based on symptomatic extrarenalmanifestations. Two subtypes ofhereditary papillary RCC syndromesare known, type I presenting withmultiple bilateral tumors, and type II
The RCC’s observed in both papillarysubtypes are typically hypovascularmalignancies on contrast enhancedcross-sectional imaging. Both theclear and papillary cell type RRC’soriginate from the cells of the proxi-mal renal tubule. On the contrary,chromophobe renal carcinomas, asobserved in BHD syndrome, origi-nate from the intercalated cells of
solitary tumors with a more aggres-sive behavior and an association ofuterine leiomyomas and sarcomas.
JBR–BTR, 2011, 94: 34-36.
LETTER TO THE EDITORR. D’Hauwe1, E. Lerut2, L. De Wever1, R. Oyen1, F. Claus1
From: Department of 1. Radiology, 2. Pathology, University Hospitals Leuven, Leuven,Belgium.Address for correspondence: Dr F. Claus, M.D., Dienst Radiologie UZ-Leuven,Herestraat 49, B-3000 Leuven, Belgium. E-mail: [email protected]
Fig. 1. — BHD syndrome in 3 patients diagnosed with multifocal chromophobe RCC’sand cystic lung lesions. Top row: 39-year-old female showing bilateral, homogeneous-ly, arterial middle-level enhancing (left image) and venous hypo-enhancing (rightimage) chromophobe renal cell cancers. Middle row: 77-year-old male, coronal CTshowing bilateral hyper-enhancing RCC’s (left image) and multiple lung cysts (rightimage). Bottom Row: 43-year-old male, coronal contrast enhanced MRI showing twoleft-sided RCC’s (left image) and bilateral pulmonary cysts complicated by left-sidedpneumothorax (right image).
d'hauwe-_Opmaak 1 16/02/11 09:50 Pagina 34
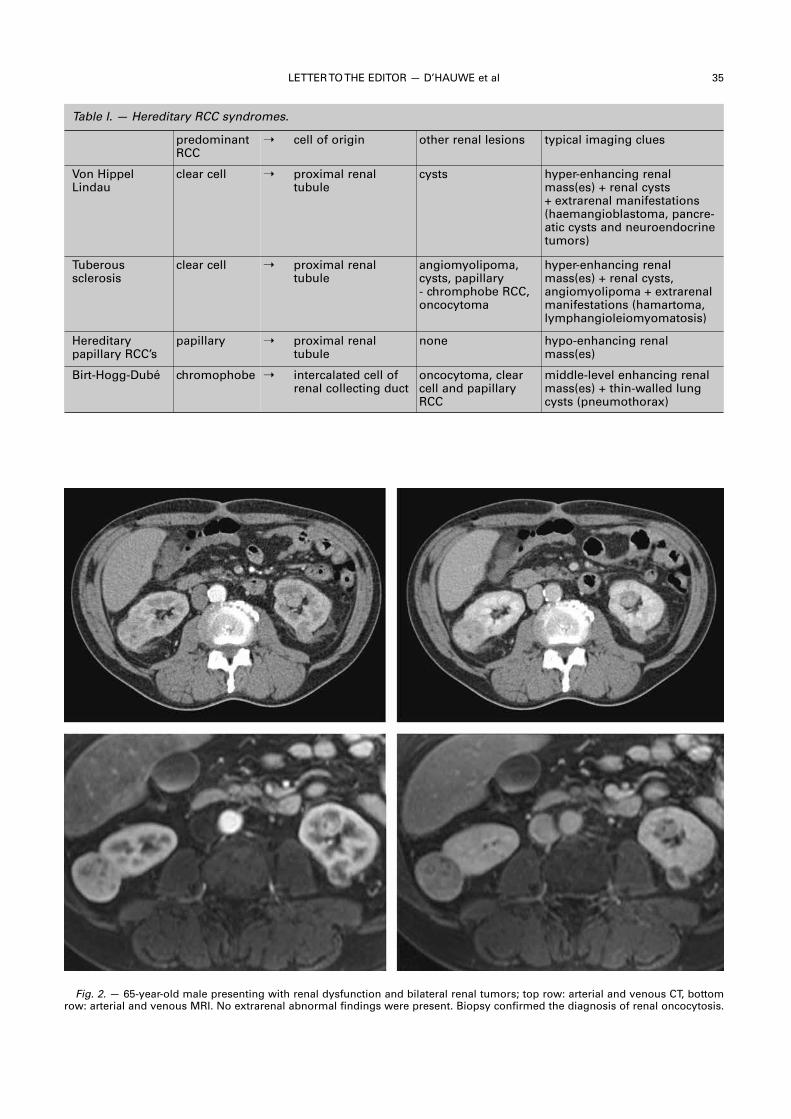
LETTER TO THE EDITOR — D’HAUWE et al 35
Fig. 2. — 65-year-old male presenting with renal dysfunction and bilateral renal tumors; top row: arterial and venous CT, bottomrow: arterial and venous MRI. No extrarenal abnormal findings were present. Biopsy confirmed the diagnosis of renal oncocytosis.
Table I. — Hereditary RCC syndromes.
predominantRCC
� cell of origin other renal lesions typical imaging clues
Von HippelLindau
clear cell � proximal renal tubule
cysts hyper-enhancing renalmass(es) + renal cysts+ extrarenal manifestations(haemangioblastoma, pancre-atic cysts and neuroendocrinetumors)
Tuberous sclerosis
clear cell � proximal renal tubule
angiomyolipoma,cysts, papillary- chromphobe RCC,oncocytoma
hyper-enhancing renalmass(es) + renal cysts,angiomyolipoma + extrarenalmanifestations (hamartoma,lymphangioleiomyomatosis)
Hereditary papillary RCC’s
papillary � proximal renal tubule
none hypo-enhancing renalmass(es)
Birt-Hogg-Dubé chromophobe � intercalated cell ofrenal collecting duct
oncocytoma, clearcell and papillaryRCC
middle-level enhancing renalmass(es) + thin-walled lungcysts (pneumothorax)
d'hauwe-_Opmaak 1 16/02/11 09:50 Pagina 35
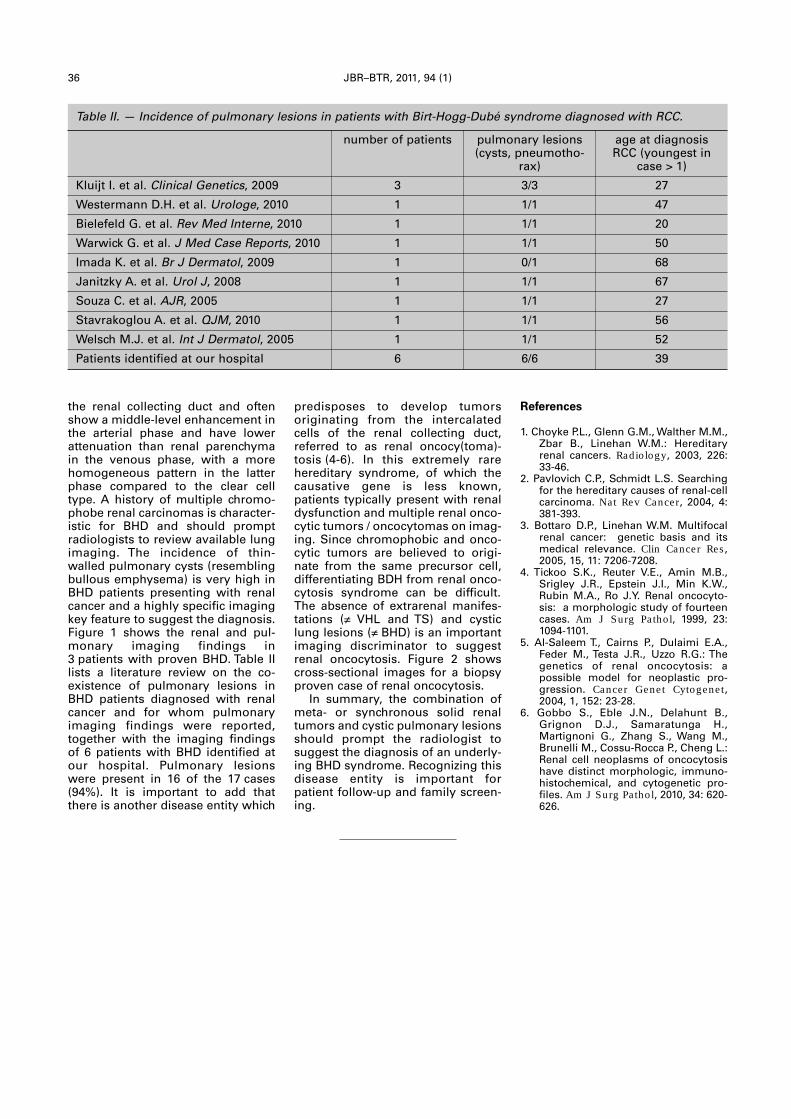
36 JBR–BTR, 2011, 94 (1)
the renal collecting duct and oftenshow a middle-level enhancement inthe arterial phase and have lowerattenuation than renal parenchymain the venous phase, with a morehomogeneous pattern in the latterphase compared to the clear celltype. A history of multiple chromo-phobe renal carcinomas is character-istic for BHD and should promptradiologists to review available lungimaging. The incidence of thin-walled pulmonary cysts (resemblingbullous emphysema) is very high inBHD patients presenting with renalcancer and a highly specific imagingkey feature to suggest the diagnosis.Figure 1 shows the renal and pul-monary imaging findings in3 patients with proven BHD. Table IIlists a literature review on the co-existence of pulmonary lesions inBHD patients diagnosed with renalcancer and for whom pulmonaryimaging findings were reported,together with the imaging findingsof 6 patients with BHD identified atour hospital. Pulmonary lesionswere present in 16 of the 17 cases(94%). It is important to add thatthere is another disease entity which
References
1. Choyke P.L., Glenn G.M., Walther M.M.,Zbar B., Linehan W.M.: Hereditaryrenal cancers. Radiology, 2003, 226:33-46.
2. Pavlovich C.P., Schmidt L.S. Searchingfor the hereditary causes of renal-cellcarcinoma. Nat Rev Cancer, 2004, 4:381-393.
3. Bottaro D.P., Linehan W.M. Multifocalrenal cancer: genetic basis and itsmedical relevance. Clin Cancer Res,2005, 15, 11: 7206-7208.
4. Tickoo S.K., Reuter V.E., Amin M.B.,Srigley J.R., Epstein J.I., Min K.W.,Rubin M.A., Ro J.Y. Renal oncocyto-sis: a morphologic study of fourteencases. Am J Surg Pathol, 1999, 23:1094-1101.
5. Al-Saleem T., Cairns P., Dulaimi E.A.,Feder M., Testa J.R., Uzzo R.G.: Thegenetics of renal oncocytosis: a possible model for neoplastic pro-gression. Cancer G enet Cytogenet,2004, 1, 152: 23-28.
6. Gobbo S., Eble J.N., Delahunt B.,Grignon D.J., Samaratunga H.,Martignoni G., Zhang S., Wang M.,Brunelli M., Cossu-Rocca P., Cheng L.:Renal cell neoplasms of oncocytosishave distinct morphologic, immuno-histochemical, and cytogenetic pro-files. Am J Surg Pathol, 2010, 34: 620-626.
predisposes to develop tumors originating from the intercalatedcells of the renal collecting duct,referred to as renal oncocy(toma) -tosis (4-6). In this extremely rarehereditary syndrome, of which thecausative gene is less known,patients typically present with renaldysfunction and multiple renal onco-cytic tumors / oncocytomas on imag-ing. Since chromophobic and onco-cytic tumors are believed to origi-nate from the same precursor cell,differentiating BDH from renal onco-cytosis syndrome can be difficult .The absence of extrarenal manifes-tations (� VHL and TS) and cysticlung lesions (� BHD) is an importantimaging discriminator to suggestrenal oncocytosis. Figure 2 showscross-sectional images for a biopsyproven case of renal onco cytosis.
In summary, the combination ofmeta- or synchronous solid renaltumors and cystic pulmonary lesionsshould prompt the radiologist tosuggest the diagnosis of an underly-ing BHD syndrome. Recognizing thisdisease entity is important forpatient follow-up and family screen-ing.
Table II. — Incidence of pulmonary lesions in patients with Birt-Hogg-Dubé syndrome diagnosed with RCC.
number of patients pulmonary lesions(cysts, pneumotho-
rax)
age at diagnosisRCC (youngest in
case > 1)
Kluijt I. et al. Clinical Genetics, 2009 3 3/3 27
Westermann D.H. et al. Urologe, 2010 1 1/1 47
Bielefeld G. et al. Rev Med Interne, 2010 1 1/1 20
Warwick G. et al. J Med Case Reports, 2010 1 1/1 50
Imada K. et al. Br J Dermatol, 2009 1 0/1 68
Janitzky A. et al. Urol J, 2008 1 1/1 67
Souza C. et al. AJR, 2005 1 1/1 27
Stavrakoglou A. et al. QJM, 2010 1 1/1 56
Welsch M.J. et al. Int J Dermatol, 2005 1 1/1 52
Patients identified at our hospital 6 6/6 39
d'hauwe-_Opmaak 1 16/02/11 09:51 Pagina 36

Pedunculated pleural lipoma
L. Cardinale, F. Avogliero, F. Solitro, C. Fava1
A 70-year-old woman was hospitalized for dyspnea and chestpain. After radiological examinations and bronchoscopy, she wasdiagnosed with a stage IVsmall-cell carcinoma of the lung. Collaterally, chest CT showed an hypodense pleural sessile
mass, with smooth, well defined borders and homogeneous fatattenuation of approximately –100 HU; it showed no enhancementafter intravenous contrast material administration (Fig. A).The lesion was suggestive for pleural lipoma.At the next CT examination pleural effusion, due to a primary
disease progression, was detected. The mass, floating into pleuraleffusion, had now a polypoid appearance and was inserted into theparietal pleura with a small pedicle (Fig. B,C).
Comment
Most patients with pleural lipoma are asymptomatic until incidental detection at radiological examinations; the rare caseswith symptoms in bulky masses may include nonproductivecough, back pain, dyspnea. Definitive diagnosis is made at CTwhen the lesion in question shows an homogeneous fat attenua-tion of approximately −100 HU, smooth borders abutting on thelungs, tapering or obtuse margins with the pleural surface and contact with the pleura with at least one quarter of the mass’s circumference. A pedicle is rarely visible. Biopsy is recommendedfor those lesions with an non-homogeneous density (for the risk ofatypical lipomatous tumors and liposarcomas). Another peduncu-lated neoplasm which enters into the differential diagnosis withlipoma is the localized fibrous tumor of the pleura. However, thefibrous tumor has not the peculiar fat attenuation.
JBR–BTR, 2011, 94: 37.
IMAGES IN CLINICAL RADIOLOGY
1. University of Turin, Department of Clinical & Biological Sciences,Radiology Unit, San Luigi Hospital, Orbassano (Torino), Italy.
A
C
B
images-cardinale-_Opmaak 1 16/02/11 09:53 Pagina 1

Denim sandblasters’ pneumoconiosis
M. Apaydin1, M. Varer1, S. Ayik
A 28-year-old man with long standing dyspnea for 4 years and ahistory of dry cough, sweating and loss of weight was admitted tothe hospital. Physical examination showed fine crackles at the endof inspiration. The laboratory tests revealed increased low densitylipoprotein level with slight increase in erytrocyte sedimentationrate. Sputum smears for blood culture and tuberculosis were negative. He was referred to the radiology department for imagingstudies. Chest radiography revealed bilateral reticulonodular infiltrates in upper and middle zones. High resolution computedtomography showed bilateral diffuse intralobular micronodules inupper and mid lung zones with interlobular septal lines also bilate-ral pleural thickening was seen (A). Right middle lung zone showedhyperaeration (B). Also he had bilateral hilar, right paratracheal,prevascular and subcarinal lymphadenopathies (C). He had beenworking in producing sandblasted denims for 10 years. The diagno-sis was based on clinical history, occupational exposure to silicadust, and chest x-ray findings after other possible diagnoses wereruled out.
Comment
Denim sandblasting changes the color of the denim and givesworn appearance. Quartz is used for denim sandblasting and causethe most common form of pneumoconiosis called silicosis byinhaled dust containing crystalline silica. It easily develops in smalland unventilated unhealthy working place conditions with exten-ded exposure to tiny sand particles. Silicosis is untreatable andcauses death by impairing general health status. It can be seen inunderdeveloped as well as developed countries. Mining, drilling,construction, pottery making are the most known etiologic factors.Also, it can be accombined with autoimmune disease. Tuberculosisis a frequent complication of this disease and there is a strong linkbetween lung cancer and silicosis. Three main clinical presenta -tition was described; acute/silicoproteinosis, classic, acceleratedtypes. Radiologic findings depends the stage and type of the disease.The most common presentation is classic chronic silicosislike our case. These patients are usually become clinically andradiologically symptommatic after 10-20 years of chronic silicaexposure.Smooth nodular infiltrations, interlobular and intralobular septal
thickening, axial interstitium thickening, ground glass consolidation,honeycombing, pleural thickening, low-attenuated areas, mediastinal lymphadenopathies are the most detected abnorma -lities on CT.Denim sandblasters’ silicosis is a rare cause of pneumoconiosis.
There is no cure for this preventable enviromental disease. So it isvery important to be aware of clinical and radiological findings ofdenim sandblasters’ silicosis.
JBR–BTR, 2011, 94: 38.
IMAGES IN CLINICAL RADIOLOGY
1. Department of Radiology, 2. Sleep and Chest Disorders Unit, IzmirAtaturk Education and Reseach Hospital, Izmir, Turkey.
A
B
C
images-apaydin-_Opmaak 1 16/02/11 09:55 Pagina 1
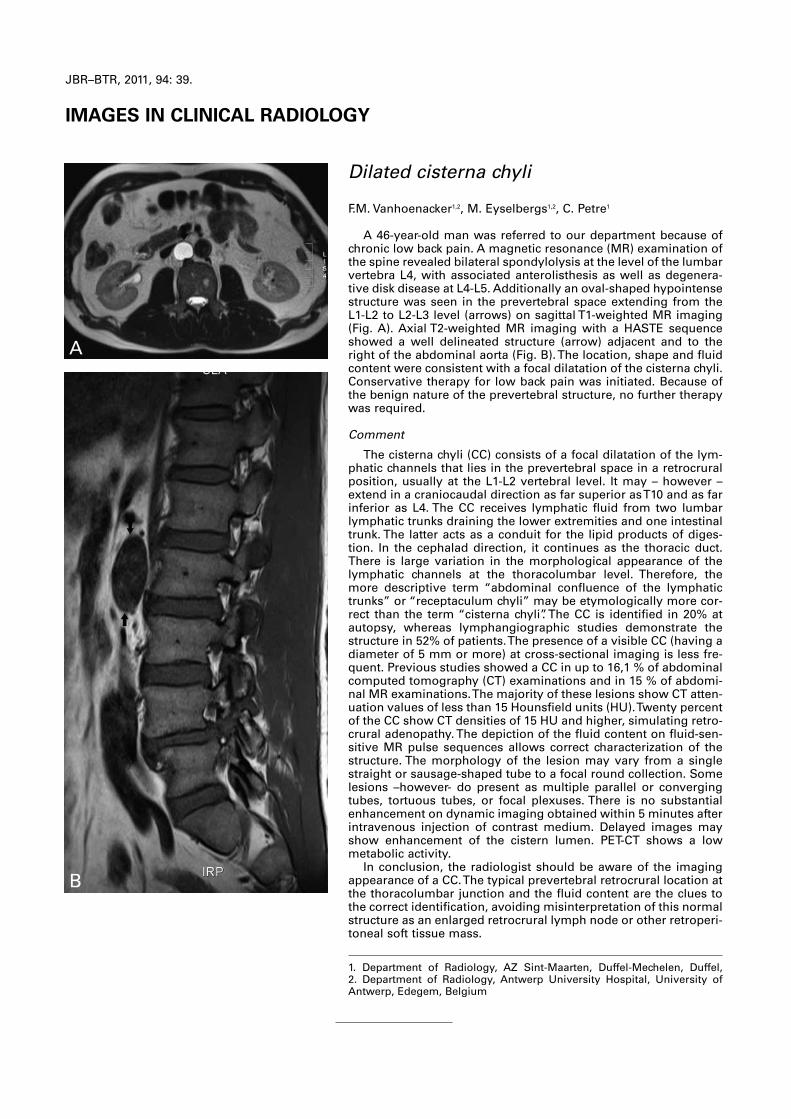
JBR–BTR, 2011, 94: 39.
IMAGES IN CLINICAL RADIOLOGY
Dilated cisterna chyli
F.M. Vanhoenacker1,2, M. Eyselbergs1,2, C. Petre1
A 46-year-old man was referred to our department because ofchronic low back pain. A magnetic resonance (MR) examination ofthe spine revealed bilateral spondylolysis at the level of the lumbarvertebra L4, with associated anterolisthesis as well as degenera-tive disk disease at L4-L5. Additionally an oval-shaped hypointensestructure was seen in the prevertebral space extending from theL1-L2 to L2-L3 level (arrows) on sagittal T1-weighted MR imaging(Fig. A). Axial T2-weighted MR imaging with a HASTE sequenceshowed a well delineated structure (arrow) adjacent and to theright of the abdominal aorta (Fig. B). The location, shape and fluidcontent were consistent with a focal dilatation of the cisterna chyli.Conservative therapy for low back pain was initiated. Because ofthe benign nature of the prevertebral structure, no further therapywas required.
Comment
The cisterna chyli (CC) consists of a focal dilatation of the lym-phatic channels that lies in the prevertebral space in a retrocruralposition, usually at the L1-L2 vertebral level. It may – however –extend in a craniocaudal direction as far superior as T10 and as farinferior as L4. The CC receives lymphatic fluid from two lumbarlymphatic trunks draining the lower extremities and one intestinaltrunk. The latter acts as a conduit for the lipid products of diges-tion. In the cephalad direction, it continues as the thoracic duct.There is large variation in the morphological appearance of thelymphatic channels at the thoracolumbar level. Therefore, themore descriptive term “abdominal confluence of the lymphatictrunks” or “receptaculum chyli” may be etymologically more cor-rect than the term “cisterna chyli”. The CC is identified in 20% atautopsy, whereas lymphangiographic studies demonstrate thestructure in 52% of patients. The presence of a visible CC (having adiameter of 5 mm or more) at cross-sectional imaging is less fre-quent. Previous studies showed a CC in up to 16,1 % of abdominalcomputed tomography (CT) examinations and in 15 % of abdomi-nal MR examinations. The majority of these lesions show CT atten-uation values of less than 15 Hounsfield units (HU). Twenty percentof the CC show CT densities of 15 HU and higher, simulating retro-crural adenopathy. The depiction of the fluid content on fluid-sen-sitive MR pulse sequences allows correct characterization of thestructure. The morphology of the lesion may vary from a singlestraight or sausage-shaped tube to a focal round collection. Somelesions –however- do present as multiple parallel or convergingtubes, tortuous tubes, or focal plexuses. There is no substantialenhancement on dynamic imaging obtained within 5 minutes afterintravenous injection of contrast medium. Delayed images mayshow enhancement of the cistern lumen. PET-CT shows a lowmetabolic activity.In conclusion, the radiologist should be aware of the imaging
appearance of a CC. The typical prevertebral retrocrural location atthe thoracolumbar junction and the fluid content are the clues tothe correct identification, avoiding misinterpretation of this normalstructure as an enlarged retrocrural lymph node or other retroperi-toneal soft tissue mass.
A
B
1. Department of Radiology, AZ Sint-Maarten, Duffel-Mechelen, Duffel, 2. Department of Radiology, Antwerp University Hospital, University ofAntwerp, Edegem, Belgium
images-vanhoenacker_images-coulier 16/02/11 09:56 Pagina 1

JBR–BTR, 2011, 94: 40.
IMAGES IN CLINICAL RADIOLOGY
Iatrogenic facial subcutaneous emphyse-ma after endodontic treatment
J. Coulier1, F.C. Deprez2
A 74-year-old woman was referred to the ophthalmologicdepartment by her dentist, for an acute left facial swelling afterextraction of the left higher canine (tooth n° 23).
Patient presented left superior and inferior palpebral oedemaextending to left periorbital subcutaneous tissues (Fig. A – CT sur-face rendering). The skin appeared normal without any erythemaand palpation revealed typical subcutaneous gaseous crepitations.Dysphagia and dyspnea were absent. Complete extensive oph-thalmologic examination was also normal.
Unenhanced facial CT was performed and revealed diffuse leftfacial subcutaneous emphysema involving both left eyelids, theleft malar Bichat fat and left peribuccal subcutaneous fat but alsothe left infratemporal, pterygomandibular and parapharyngealspaces (Fig. B – coronal views and Fig. C – axial views). No facialsinuses anomaly or bone interruption was observed on CT series,even in the left superior alveolar bones. These findings associatedwith recent dental extraction history allowed to diagnose iatro-genic left facial subcutaneous emphysema, caused by a high-speed dental hand-piece use.
Treatment consisted on short oral corticotherapy and antibio-therapy (amoxycillin/clavulanic acid).
Comment
Iatrogenic subcutaneous emphysema in the head and neckregion may arise after various interventions, including anesthesia,maxillofacial procedures, head–neck surgery and, less commonly,dental surgery involving extraction, implants or other procedures.During dental treatment, the use of compressed air to dry the rootcanal (with air-cooled high-speed dental hand-pieces) occasionallylet the air penetrate soft tissues, dissecting periodontal ligamentand gingival tissue, leading to subcutaneous emphysema.Pneumothorax, pneumomediastinum or even pneumoperitoneumcan be observed because of the relationship between the cervicalprevertebral space and the mediastinum. Life-threatening or evenfatal complications can exceptionally occur due to venous (pul-monary) air embolism or paradoxal arterial systemic air embolism.
After complicated dental surgery, air spreading occurs rapidly,within seconds to minutes. Patient senses immediate discomfortor pain in the affected area. Subcutaneous emphysema usuallyresorbs spontaneously within few days. Main complication is sub-cutaneous tissues infection due to oral flora.
Main differential diagnosis of facial swelling after medical procedures is hematoma, allergic reaction or angioedema, butsubcutaneous crepitations palpation leads to correct diagnose. CT-scan is recommended to confirm and determine the extent of sub-cutaneous emphysema.
A
B
C 1. Department of Ophtalmology, Cliniques Universitaires St-Luc, Brussels,2. Department of Radiology, Clinique St-Pierre, Ottignies-LLN, Belgium.
images-coulier_latrogenic_images-coulier 16/02/11 09:57 Pagina 1

The ‘torus palatinus’: a common but relativelyunknown entity
C. Boulet, M. De Maeseneer, T. Buisseret, M. Shahabpour, J. de Mey1
A 60-year-old woman was referred for imaging evaluation of a lump at themidline of the hard palate. The lump was painless but felt hard and lobulatedon palpation.Ulcerations were not apparent. It had appeared gradually overtime. An open mouth spiral head CT study before and after intravenous contrast injection was performed, with bone reconstructions of the facialskeleton. It revealed a flat based bony thickening at the cleft of the hard palatewith a width of 11 mm and a length of 15 mm (Fig. A,B,C). The bony protru-sion was covered by a thin layer of mucosa (Fig. D). Contrast enhancementwas absent. No other lesions were evident in the oral cavity. The nasal cavityand nasal septum were normal.
Comment
A torus (Latin for “lump”) is an exostosis consisting of a dense cortex anda limited amount of bone marrow, usually covered by a thin layer of mucosa.The ’torus palatinus’ presents clinically in three shapes: spindle-shaped,nodular or lobular. They are located at the juncture of the palatine apophysisof the maxillae. A mandibular counterpart can be found (torus mandibularis)on the internal side of the horizontal branch of the mandibula, above themylohyoid line, in the premolar region. Some authors define it as a congen-ital anomaly, due to “overactivity” of the osteoblasts with bone beingdeposited along the line of fusion of the palate. A hereditary autosomal dominant form has been described in the literature, but in up to 70% of thecases, the torus was attributed to environmental factors, mainly related toocclusal stress. The growth of the tori is gradual, being greater in the secondor third decade of life. The prevalence is higher in women, which could indicate a linkage to the X-chromosome. In addition the tori seem more common in some ethnic groups (eg. Eskimos, Japanese and AfricanAmericans). The diagnosis is usually made during clinical examination by adentist. It is mostly asymptomatic, but could lead to phonatory disturbances,limitation of mastication, ulceration of the mucosa (mimicking cancer), fooddeposition and instability of dental prosthetics. Radiographs (perapical,occlusal or panoramic) are not very useful. Clinical examination is sufficientin most of the cases, but in case of doubt CT of the facial skeleton is the bestoption. MRI does not contribute to the diagnosis. Differential diagnosis withsarcoma or squamous cell carcinoma is not difficult because there is no boneremoddeling, osteolysis, or mucosal ulceration. Removal of the torus is usu-ally not necessary. Surgical treatment is ony indicated with disturbances ofphonation, limitation of mastication, sensitivity or ulceration of the overlyingmucosa, and instabilty or conflict with dental prosthetics. Removal of theaccessory cortical bone of the tori can also be performed in case of need ofautogenous bone grafts in periodontal implant surgery.
JBR–BTR, 2011, 94: 41.
IMAGES IN CLINICAL RADIOLOGY
1. Department of Radiology, UZ Brussel, Jette, Belgium.
A
B
C
D
images-boulet-_Opmaak 1 16/02/11 09:59 Pagina 1

An unusual pelvic mass: bladder lymphoma
M. Alsinnawi1, M. Quinlan1, A. Brady2, N. Khan1
A 58-year-old woman presented to the emergency department after aminor fall, complaining of lower abdominal pain. A large, tender massarising from the pelvis was palpable, in association with abdominal wallbruising. The patient believed that she may have had a “lump” there forseveral years. She had had a total abdominal hysterectomy and bilateralsalpingo-oopherectomy for benign fibroids three years previously. Shedenied any gastrointestinal (GI) or genitourinary symptoms. She had nonight sweats or weight loss. Routine blood investigations were normal.A CT scan of her abdomen and pelvis with oral and IV contrast contrast
was performed to investigate what was thought to be a rectus sheathhaematoma. This has revealed abnormal retroperitoneal lymphadenopa-thy in the mid and lower Abdomen (Fig. A). Most of her bladder wasreplaced by a 16 x 12 x 10 cm soft-tissue density mass (Fig. B). There wasmild dilatation of both ureters with mild left hydronephrosis. Appearancessuggested a malignant process, given the retroperitoneal adenopathy.Ultrasound-guided biopsy of a right-sided 13 x 8 mm solid inguinal lymphnode was performed; histology of this was inconclusive. Following this, a rigid cystoscopy confirmed a grossly abnormal blad-
der with a diffuse, thick mass and a non-friable, pale-looking mucosawhich was intact. Multiple resection biopsies were taken. MRI of pelvis thenext day showed almost complete absence of a bladder lumen. The blad-der wall was diffusely thickened, measuring 10 cms in places (Fig. C).Pathologically-enlarged iliac and retroperitoneal nodes were seen.Abnormal stranding of perivesical fat suggested transmural malignantinfiltration. The histology of her bladder biopsies showed dense, diffuseinfiltration by small lymphocytes, covered in part by intact urothelium.Microscopy and immunohistochemistry supported the diagnosis of lowgrade, diffuse, B-cell Non Hodgkin’s Lymphoma (NHL). A diagnosis of pri-mary malignant lymphoma arising in the urinary bladder was made. Shewas referred on to the Haematology service for further investigation andtreatment. Given that her International Prognostic Index is 2-3/5, six cyclesof RCHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine andPrednisolone) chemotherapy were planned. After completing her treat-ment, she will be re-staged with appropriate scans.
Comment
About 40% of NHL present in extra-nodal sites, with the skin and the GItract being the most frequent sites. Primary bladder lymphoma is a raredisease, responsible for only 0.2% of extra-nodal lymphomas. The diseaseis typically seen in middle-aged and elderly females. The frequency ofNHL in the urinary bladder is higher than Hodgkin’s lymphoma.
Presentation can be variable with symptoms including haematuria, pain, dysuria, nocturia, frequency or recurrentUTIs. Bladder lymphomas tend to occur at the base and the trigone of the bladder and usually form a sessile masswith normal urothelium. Cystoscopy commonly shows a solid tumour without surface changes. The surroundingmucosa is typically intact but in a very large tumour the mucosa can be ulcerated. Upper tract dilatation can occursecondary to mass effect and ureteric obstruction. Histopathological studies are essential for the diagnosis. It is oftendifficult to differentiate lymphoma from sarcoma or carcinoma on frozen section biopsy. Histologically, primary blad-der lymphoma is most commonly low-grade NHL of the B-cell type. About 20% of B-cell bladder lymphoma is high-grade. Reported management of primary bladder low-grade NHL is varied. Partial or total cystectomy, radiotherapy,chemotherapy, or combined therapies have all been described. Surgery may be inappropriate in these patients, giventhe high success rate with either radiotherapy or chemotherapy. Repeat cystoscopy is recommended for follow-up ofall patients.In summary, this case highlights the difficulties in diagnostic differentiation relating to large pelvic masses in
middle age females. In the differential diagnosis of bladder tumours, malignant lymphoma of the bladder should beconsidered. Despite the fact that primary bladder lymphoma is a rare condition, we should be aware of the excellentcomplete remission rates and good prognosis.
JBR–BTR, 2011, 94: 42.
IMAGES IN CLINICAL RADIOLOGY
Department of 1. Urology and 2. Radiology, Mercy University Hospital, Cork,Ireland.
A
B
C
images-alsinnawi-_Opmaak 1 16/02/11 10:00 Pagina 1

Imaging is an indispensable toolin modern medicine, yet very fewpatients know just how important itis. From cancer detection and thera-py to diagnosing stroke or serioustrauma in time, radiologists con-tribute to saving lives by coveringevery field of medicine. To raise pub-lic awareness, the European Societyof Radiology has launched the1st European Day of Radiology onFebruary 10, in memory of x-ray discoverer Wilhelm Conrad Röntgen.
Vienna, December 2010 – Radiolo -gists, radiographers, nurses or any-one else who has witnessed the dif-ference that can be made by medicalimaging cannot fail to appreciate thevalue of its role in modern health-care, but the world of radiology isoften something of an unsung heroamong the general public. Althoughmany procedures are well known byname, and the impact that a singleroutine examination can have on apatient’s life can be life-altering, theperception of radiology held by mostof us is often far less clear than thehigh-resolution images interpretedby its practitioners. Most people are familiar with the
concept of the diagnostic x-ray asthe traditional role of radiology, butnumerous advances in research andtechnology have led radiology toplay an increasingly prominent partin healthcare, not just in terms ofspotting problems, but also as amajor contributor to treatment andrecovery. Working in tandem withother disciplines, radiology has hada major impact on achievements insuch significant areas as early cancerdetection, speedy trauma analysis,and precise stroke localisation,among many others.In order to raise awareness
among the general public and drawattention to the broad contributionimaging makes to general health-care, the European Society ofRadiology (ESR) decided to launchthe 1st European Day of Radiology onFebruary 10th, the anniversary of the
in radiology are universal. Althoughseveral radiological societies will beparticipating in the European Day ofRadiology, the initiative was con-ceived and coordinated centrally bythe ESR, a non-profit organisationbased in Vienna, Austria. Formed in2005 through the merging of twoother organisations – the EuropeanAssociation of Radiology and theEuropean Congress of Radiology –,the ESR has spent the last five yearspromoting and coordinating all man-ner of radiological activities, bring-ing together more than 50,000 mem-bers worldwide in the process. The date of February 10 was cho-
sen for the European Day ofRadiology to draw a link between thebeginnings of radiology and its cur-rent status, so as to highlight theprogress made, as much as to hon-our the life of the man who made thevery first steps in founding the disci-pline. Wilhelm Conrad Röntgenreceived the Nobel Prize in Physics in1901 “in recognition of the extraordi-nary services he has rendered by thediscovery of the remarkable rayssubsequently named after him”.Significantly, he refused to take outpatents, intending the practicalapplications of x-rays to benefitmankind to the greatest possibleextent, and did not even want hisdiscovery to bear his name. Longafter his passing he is still undoubt-edly the most important personalityin the history of radiology, havinglaid the foundations for the manyand varied advances made in hiswake.Through the European Day of
Radiology, the ESR and all participat-ing societies will be hoping to con-tribute to making those advancesbetter known and to bringing theimage of radiology into a sharperfocus.
ESR Press OfficeNeutorgasse 91010 Vienna, [email protected]
death of Wilhelm Conrad Röntgen,who first discovered x-rays in 1895.The European Day of Radiology will,for the first time, see coordinatedpress activities undertaken bynational radiological societies acrossEurope to highlight the role and sig-nificance of medical imaging.Societies from seventeen coun-
tries have accepted the ESR’s invita-tion to take part in this endeavour, allof whom will launch press releaseson key topics, focusing on the recentchallenges and achievements in theirrespective countries. The topicsreflect some of the most importantissues in radiology, which are just asrelevant to potential patients as theyare to those working in the field.Cancer detection and therapy, emer-gency radiology, patient safety andradiation dose reduction, and strokeimaging are all areas of majorimportance in radiology, and eachparticipating country will take atleast one of these subjects as thefocus of its press activities, withsome societies also deciding to sup-port them with various events heldon and around February 10. The national radiological societies
of Austria, Belgium, the CzechRepublic, Croatia, France, Georgia,Hungary, Ireland, Italy, Lithuania,Poland, Romania, Spain, Sweden,Switzerland, Turkey and the UK allagreed to take part in the initiative,and a total of 23 representatives ofthese societies have been inter-viewed by ESR staff to create pressreleases that will be distributed tothe media in their home countries.In many cases the topics will be the
same and the general essence willbe similar, but the close involvementof the radiological societies meanseach press release bears a particularnational relevance. It is hoped thatthis will increase the specificity ofthe campaign’s wider message andhelp to enhance radiology’s imageas an essential and progressive ele-ment of modern medical care. Healthcare systems vary from
country to country, but the big issues
JBR–BTR, 2011, 94: 43.
CELEBRATE THE POWER OF IMAGING:THE EUROPEAN DAY OF RADIOLOGY1
1 Responding to the invitation of the European Society of Radiology President Desprechins with the board of the Royal BelgianRadiological Society have organized a press conference in the Museum of Radiology in Brussels on the 10th of February. Consideringtheir appeal to the general public, two topics were chosen for this conference, namely acute stroke and safety image (dose reduc-tion). The summaries of the presentations by three radiologists will appear in the next issue of JBR-BTR.
EDOR (Celebrate)_Opmaak 1 16/02/11 10:02 Pagina 1
JBR–BTR, 2011, 94: 44.
NEWS FROM THE UNIVERSITIES
A
Wetenschappelijke Prijs em Prof Dr A.L. BaertDinsdag 7 december 2010 kreeg Dr. Chantal Van Ongeval de 7de “Wetenschappelijke Prijs Em Professor DoctorA.L. Baert” ter waarde van 2.500 euro.
De jury heeft haar de titel toegekend “Laureaat Wetenschappelijke Prijs Em Professor Doctor A.L. Baert”, voor haaronderzoekswerk “Performance and optimization of clinical digital mammography”.
Dr Van Ongeval is staflid van de dienst Radiologie.
Deze tweejaarlijkse prijs bekroont het werk van een radioloog, opgeleid aan één van de vier Nederlandstalige universiteiten in België, op basis van een met goed gevolg verdedigde doctoraatsthesis.
De prijs werd voor de 1ste keer uitgereikt in 1998, ex aequo aan Prof Dr Robert Hermans, Dr Marc Lemmerling enDr Lieven Van Hoe.De volgende laureaten waren:Prof Dr J. Van Goethem (2000)Prof Dr M. De Maeseneer (2002)Prof Dr S. Dymarkowski (2004)Prof Dr M. Van Goethem (2006)Prof Dr G. Maleux (2008)
De 8ste “Wetenschappelijke Prijs Em Professor Doctor A.L. Baert” Periode 2011-2012 zal uitgereikt worden in december 2012. Het Algemeen Reglement zal in het najaar 2011 in het Belgisch tijdschrift voor radiologie gepubliceerd worden.
From left to right: Prof. E. Ponette, Prof. R.F. Dondelinger, Dr Ch. Van Ongeval, Prof. A.L. Baert, Dr P. Cleeren.
news (Wet. Prijs Baert)_Opmaak 1 16/02/11 10:03 Pagina 1
Inhoudstafel
Lijst van medewerkers . . . . . . . . . . . . . . . . . . . . . . . IToelichting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . IIIIllustratie . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . VVoorwoord . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . VIIHoofdstuk 1 Aanvang van de radiologie in
het leger . . . . . . . . . . . . . . . . . . . . . . . 1Hoofdstuk 2 Belgische legerradiologen bij de
pioniers . . . . . . . . . . . . . . . . . . . . . . . 5Hoofdstuk 3 Opvattingen van de Medische Dienst
bij de aanvang van de oorlog . . . . . 11Hoofdstuk 4 De radiologie trekt naar het
IJzerfront . . . . . . . . . . . . . . . . . . . . . . 15Hoofdstuk 5 Hoe werkt de röntgenapparatuur in
deze tijd nu eigenlijk? . . . . . . . . . . . . 25Hoofdstuk 6 Voertuigen voor radiologie . . . . . . . 35Hoofdstuk 7 Plaatsbepaling en verwijdering
van projectielen . . . . . . . . . . . . . . . . 51Hoofdstuk 8 De gevaren van de X-Stralen . . . . . . 67Hoofdstuk 9 Moeilijkheden en oplossingen
in de radiologie . . . . . . . . . . . . . . . . . 75Hoofdstuk 10 Ongelukkige tussenkomst van
Röntgen . . . . . . . . . . . . . . . . . . . . . . . 81Hoofdstuk 11 Dr. Etienne Henrard: de radioloog
die generaal wordt . . . . . . . . . . . . . . 87Hoofdstuk 12 Van laborant tot technoloog . . . . . . 97
Hoofdstuk 13 De radiologie beschreven doorhen die haar hebben ondergaan . . . 103
Hoofdstuk 14 Positieve gevolgen van het conflictvoor de radiologie . . . . . . . . . . . . . . 107
Nawoord . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121Klein lexicon ter uitleg . . . . . . . . . . . . . . . . . . . . . . . 125Bronnenvermelding . . . . . . . . . . . . . . . . . . . . . . . . . . 129Index van eigennamen . . . . . . . . . . . . . . . . . . . . . . . 137Dankbetuigingen . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141Inhoudstafel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143
JBR–BTR, 2011, 94: 46-53.
De eerste Wereldoorlog in BelgiëRadiologie in "Trench Coat"René Van Tiggelen
Met de medewerking vanLuc De Broe, Walter Esch, Françoise Goetghebuer,Georges Mazy, Lieven Mortelmans, François Olier,Laurent Provost, Robert Smets, Ronny Van Loon, LucViaene
Vertaling Jan DirckxVormgeving Jacques LouagieBrussel 2011
La Grande Guerre de 1914-1918La radiologie belge monte au frontRené Van Tiggelen
Avec la collaboration deLuc De Broe, Jan Dirckx, Walter Esch, F. Goetghebuer,Georges Mazy, Lieven Mortelmans, François Olier,Laurent Provost, Robert Smets, Ronny Van Loon, LucViaene
Mise en pages par Jacques LouagieBruxelles 2011
A
Table des matières
Liste des collaborateurs . . . . . . . . . . . . . . . . . . . . . . IAvant-propos . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . IIIIllustration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . VPréface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . VIIChap. 1 Les débuts de la radiologie
militaire . . . . . . . . . . . . . . . . . . . . . . . . . 1Chap. 2 Les radiologues militaires belges
parmi les pionniers . . . . . . . . . . . . . . . 5Chap. 3 Doctrine du service médical
jusqu'au début des hostilités . . . . . . . 11Chap. 4 La radiologie monte au front
de l'Yser . . . . . . . . . . . . . . . . . . . . . . . . 15Chap. 5 En fait, comment l'appareillage
fonctionne-t-il à l'époque ? . . . . . . . . . 25Chap. 6 Voitures de radiologie . . . . . . . . . . . . . 35Chap. 7 La localisation des projectiles et
leur extraction . . . . . . . . . . . . . . . . . . . 51Chap. 8 Les dangers des rayons X . . . . . . . . . . 67Chap. 9 Difficultés radiologiques et
solutions . . . . . . . . . . . . . . . . . . . . . . . . 75Chap. 10 Intervention malheureuse de
Röntgen . . . . . . . . . . . . . . . . . . . . . . . . . 81Chap. 11 Le Dr Etienne Henrard: le radiologue
qui devint général . . . . . . . . . . . . . . . . 87Chap. 12 Du garçon de laboratoire au
manipulateur . . . . . . . . . . . . . . . . . . . . 97Chap. 13 La radiologie décrite par ceux
qui l’ont subie . . . . . . . . . . . . . . . . . . . . 103Chap. 14 Conséquences radiologiques
positives du conflit . . . . . . . . . . . . . . . . 107Postface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121Petit lexique explicatif . . . . . . . . . . . . . . . . . . . . . . . . 125Sources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 129Index des noms propres . . . . . . . . . . . . . . . . . . . . . . 137Remerciements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141Table des matières . . . . . . . . . . . . . . . . . . . . . . . . . . . 143
Inschrijving:
Militair Hospitaal Koningin AstridBruynstraat 2, 1120 [email protected].: +32 (0)2 264.40.97Fax: +32 (0)2 264.40.98
Souscription:
Hôpital Militaire Reine Astridrue Bruyn 2, 1120 [email protected]él.: +32 (0)2 264.40.97Fax: +32 (0)2 264.40.98
Musée (tekst ned.+fr)_Opmaak 1 16/02/11 11:29 Pagina 46
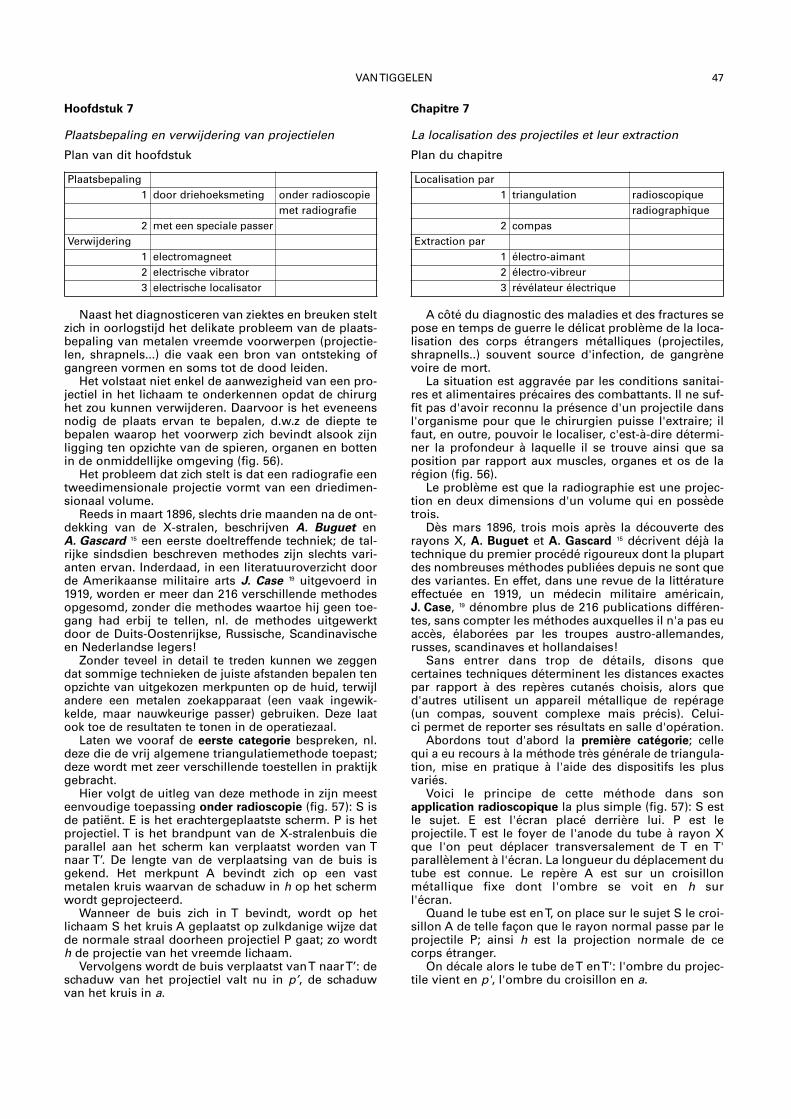
VAN TIGGELEN 47
Hoofdstuk 7
Plaatsbepaling en verwijdering van projectielen
Plan van dit hoofdstuk
Naast het diagnosticeren van ziektes en breuken steltzich in oorlogstijd het delikate probleem van de plaats-bepaling van metalen vreemde voorwerpen (projectie-len, shrapnels...) die vaak een bron van ontsteking ofgangreen vormen en soms tot de dood leiden.
Het volstaat niet enkel de aanwezigheid van een pro-jectiel in het lichaam te onderkennen opdat de chirurghet zou kunnen verwijderen. Daarvoor is het eveneensnodig de plaats ervan te bepalen, d.w.z de diepte tebepalen waarop het voorwerp zich bevindt alsook zijnligging ten opzichte van de spieren, organen en bottenin de onmiddellijke omgeving (fig. 56).
Het probleem dat zich stelt is dat een radiografie eentweedimensionale projectie vormt van een driedimen-sionaal volume.
Reeds in maart 1896, slechts drie maanden na de ont-dekking van de X-stralen, beschrijven A. Buguet enA. Gascard 15 een eerste doeltreffende techniek; de tal-rijke sindsdien beschreven methodes zijn slechts vari-anten ervan. Inderdaad, in een literatuuroverzicht doorde Amerikaanse militaire arts J. Case 19 uitgevoerd in1919, worden er meer dan 216 verschillende methodesopgesomd, zonder die methodes waartoe hij geen toe-gang had erbij te tellen, nl. de methodes uitgewerktdoor de Duits-Oostenrijkse, Russische, Scandinavischeen Nederlandse legers!
Zonder teveel in detail te treden kunnen we zeggendat sommige technieken de juiste afstanden bepalen tenopzichte van uitgekozen merkpunten op de huid, terwijlandere een metalen zoekapparaat (een vaak ingewik -kelde, maar nauwkeurige passer) gebruiken. Deze laatook toe de resultaten te tonen in de operatie zaal.
Laten we vooraf de eerste categorie bespreken, nl.deze die de vrij algemene triangulatiemethode toepast;deze wordt met zeer verschillende toestellen in praktijkgebracht.
Hier volgt de uitleg van deze methode in zijn meesteenvoudige toepassing onder radioscopie (fig. 57): S isde patiënt. E is het erachtergeplaatste scherm. P is hetprojectiel. T is het brandpunt van de X-stralenbuis dieparallel aan het scherm kan verplaatst worden van Tnaar T’. De lengte van de verplaatsing van de buis isgekend. Het merkpunt A bevindt zich op een vast metalen kruis waarvan de schaduw in h op het schermwordt geprojecteerd.
Wanneer de buis zich in T bevindt, wordt op hetlichaam S het kruis A geplaatst op zulkdanige wijze datde normale straal doorheen projectiel P gaat; zo wordth de projectie van het vreemde lichaam.
Vervolgens wordt de buis verplaatst van T naar T’: deschaduw van het projectiel valt nu in p’, de schaduwvan het kruis in a.
Chapitre 7
La localisation des projectiles et leur extraction
Plan du chapitre
A côté du diagnostic des maladies et des fractures sepose en temps de guerre le délicat problème de la loca-lisation des corps étrangers métalliques (projectiles,shrapnells..) souvent source d'infection, de gangrènevoire de mort.
La situation est aggravée par les conditions sanitai-res et alimentaires précaires des combattants. Il ne suf-fit pas d'avoir reconnu la présence d'un projectile dansl'organisme pour que le chirurgien puisse l'extraire; ilfaut, en outre, pouvoir le localiser, c'est-à-dire détermi-ner la profondeur à laquelle il se trouve ainsi que saposition par rapport aux muscles, organes et os de larégion (fig. 56).
Le problème est que la radiographie est une projec-tion en deux dimensions d'un volume qui en possèdetrois.
Dès mars 1896, trois mois après la découverte desrayons X, A. Buguet et A. Gascard 15 décrivent déjà latechnique du premier procédé rigoureux dont la plupartdes nombreuses méthodes publiées depuis ne sont quedes variantes. En effet, dans une revue de la littératureeffectuée en 1919, un médecin militaire américain,J. Case, 19 dénombre plus de 216 publications différen-tes, sans compter les méthodes auxquelles il n'a pas euaccès, élaborées par les troupes austro-allemandes,russes, scandinaves et hollandaises!
Sans entrer dans trop de détails, disons que certaines techniques déterminent les distances exactespar rapport à des repères cutanés choisis, alors qued'autres utilisent un appareil métallique de repérage(un compas, souvent complexe mais précis). Celui-ci permet de reporter ses résultats en salle d'opération.
Abordons tout d'abord la première catégorie; cellequi a eu recours à la méthode très générale de triangula-tion, mise en pratique à l'aide des dispositifs les plusvariés.
Voici le principe de cette méthode dans son application radioscopique la plus simple (fig. 57): S estle sujet. E est l'écran placé derrière lui. P est le projectile. T est le foyer de l'anode du tube à rayon Xque l'on peut déplacer transversalement de T en T'parallèlement à l'écran. La longueur du déplacement dutube est connue. Le repère A est sur un croisillon métallique fixe dont l'ombre se voit en h surl'écran.
Quand le tube est en T, on place sur le sujet S le croi-sillon A de telle façon que le rayon normal passe par leprojectile P; ainsi h est la projection normale de cecorps étranger.
On décale alors le tube de T en T': l'ombre du projec-tile vient en p', l'ombre du croisillon en a.
Localisation par1 triangulation radioscopique
radiographique2 compas
Extraction par1 électro-aimant2 électro-vibreur3 révélateur électrique
Plaatsbepaling1 door driehoeksmeting onder radioscopie
met radiografie2 met een speciale passer
Verwijdering1 electromagneet2 electrische vibrator3 electrische localisator
Musée (tekst ned.+fr)_Opmaak 1 16/02/11 11:29 Pagina 47
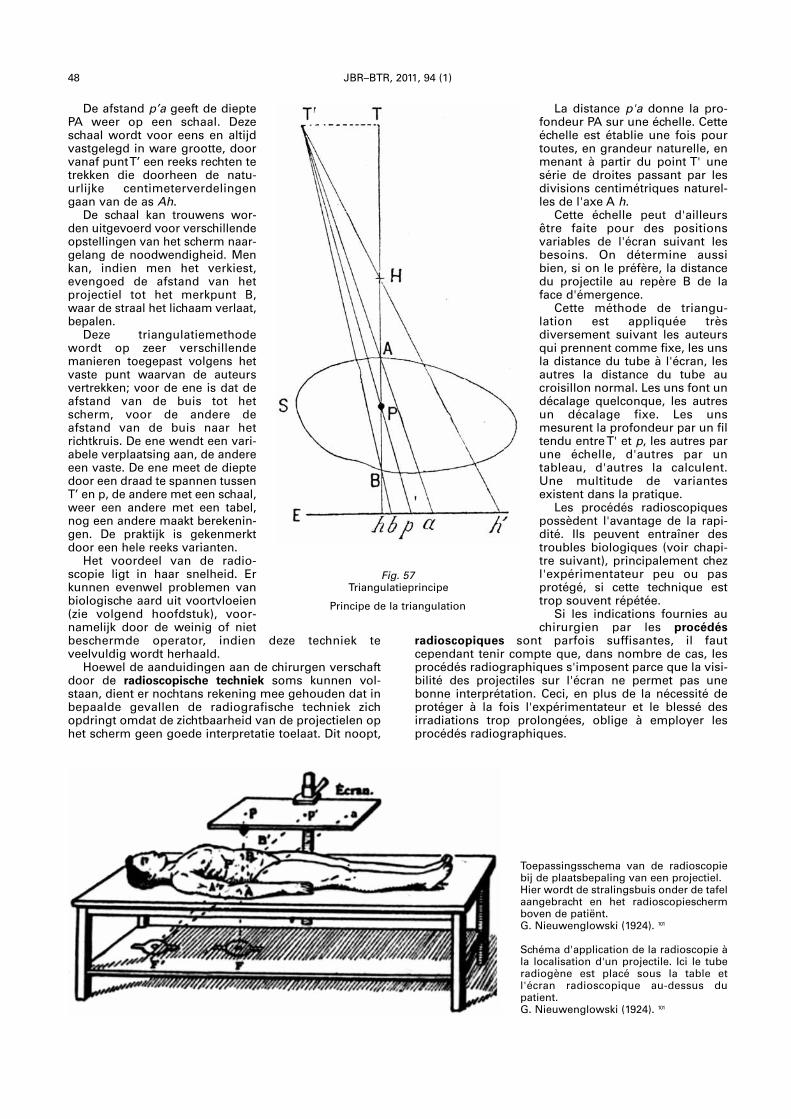
48 JBR–BTR, 2011, 94 (1)
De afstand p’a geeft de dieptePA weer op een schaal. Dezeschaal wordt voor eens en altijdvastgelegd in ware grootte, doorvanaf punt T’ een reeks rechten tetrekken die doorheen de natu-urlijke centimeterverdelingengaan van de as Ah.
De schaal kan trouwens wor-den uitgevoerd voor verschillendeopstellingen van het scherm naar -gelang de noodwendigheid. Menkan, indien men het verkiest,evengoed de afstand van hetprojec tiel tot het merkpunt B,waar de straal het lichaam verlaat,bepalen.
Deze triangulatiemethodewordt op zeer verschillendemanieren toegepast volgens hetvaste punt waarvan de auteursvertrekken; voor de ene is dat deafstand van de buis tot hetscherm, voor de andere de afstand van de buis naar hetrichtkruis. De ene wendt een vari-abele verplaatsing aan, de andereeen vaste. De ene meet de dieptedoor een draad te spannen tussenT’ en p, de andere met een schaal,weer een andere met een tabel,nog een andere maakt berekenin-gen. De praktijk is gekenmerktdoor een hele reeks varianten.
Het voordeel van de radio-scopie ligt in haar snelheid. Erkunnen evenwel problemen vanbiologische aard uit voortvloeien(zie volgend hoofdstuk), voor-namelijk door de weinig of nietbeschermde operator, indien deze techniek teveelvuldig wordt herhaald.
Hoewel de aanduidingen aan de chirurgen verschaftdoor de radioscopische techniek soms kunnen vol-staan, dient er nochtans rekening mee gehouden dat inbepaalde gevallen de radiografische techniek zichopdringt omdat de zichtbaarheid van de projectielen ophet scherm geen goede interpretatie toelaat. Dit noopt,
La distance p'a donne la pro-fondeur PA sur une échelle. Cetteéchelle est établie une fois pourtoutes, en grandeur naturelle, enmenant à partir du point T' unesérie de droites passant par lesdivisions centimétriques naturel-les de l'axe A h.
Cette échelle peut d'ailleursêtre faite pour des positions variables de l'écran suivant lesbesoins. On détermine aussibien, si on le préfère, la distancedu projectile au repère B de laface d'émergence.
Cette méthode de triangu -lation est appliquée très diversement suivant les auteursqui prennent comme fixe, les unsla distance du tube à l'écran, lesautres la distance du tube aucroisillon normal. Les uns font undécalage quelconque, les autresun décalage fixe. Les uns mesurent la profondeur par un filtendu entre T' et p, les autres parune échelle, d'autres par untableau, d'autres la calculent.Une multitude de variantes existent dans la pratique.
Les procédés radioscopiquespossèdent l'avantage de la rapi-dité. Ils peuvent entraîner destroubles biologiques (voir chapi-tre suivant), principalement chezl'expérimentateur peu ou pasprotégé, si cette technique esttrop souvent répétée.
Si les indications fournies auchirurgien par les procédés
radioscopiques sont parfois suffisantes, il faut cependant tenir compte que, dans nombre de cas, lesprocédés radiographiques s'imposent parce que la visi-bilité des projectiles sur l'écran ne permet pas unebonne interprétation. Ceci, en plus de la nécessité deprotéger à la fois l'expérimentateur et le blessé des irradiations trop prolongées, oblige à employer les procédés radiographiques.
Fig. 57Triangulatieprincipe
Principe de la triangulation
Toepassingsschema van de radioscopiebij de plaatsbepaling van een projectiel.Hier wordt de stralingsbuis onder de tafelaangebracht en het radioscopieschermboven de patiënt.G. Nieuwenglowski (1924). 101
Schéma d'application de la radioscopie àla localisation d'un projectile. Ici le tuberadiogène est placé sous la table etl'écran radioscopique au-dessus dupatient.G. Nieuwenglowski (1924). 101
Musée (tekst ned.+fr)_Opmaak 1 16/02/11 11:29 Pagina 48

VAN TIGGELEN 49
benevens de noodzakelijkheid om de uitvoerder van hetexperiment en de gewonde te beschermen tegen telangdurige bestraling, tot toepassing van de radio -grafie techniek.
Daar ook zijn veelvuldige technieken voorgesteld, ennog ingewikkelder dan deze die gebruik maken van deradioscopie! We bespreken hier de methodevoorgesteld door G. Massiot (fig. 58). De lamp wordt inM geplaatst, men glijdt in de gleuven onder de sokkelvan de koepel het kartonnen - of vezelplaatje dat hetschietlood draagt.
Terwijl de lampdrager verplaatst wordt, wordt eenschietlood aangebracht, dat de richtstraal voorstelt, ophet punt dat gekozen wordt als spoor van deze straal.
Deze plaatsing dient gemerkt te worden door de staafT, zodanig te verplaatsen dat zijn uiteinde samenvalt methet schietlood en dat zijn richting waarlijk vertikaal is.
Een eerste belichting wordt verricht (fig. 58-A) en indie voorwaarden geeft het uiteinde van de staaf hetspoor van de richtstraal weer in N, en een schaduw vanhet projectiel P projecteert zich in O. Een tweede belicht-ing wordt in dezelfde omstandigheden uitgevoerd, na deverplaatsing van de lamp over een willekeurige afstand.
Deze tweede belichting maakt een nieuwe afdruk opdezelfde plaat van het spoor van de richtstraal, uitgaandevan M’ naar N’ en van een schaduw O’ van hetzelfde pro-jectiel P. Vervolgens wordt de radiografische plaat (R) dieeerst onder de patiënt is geplaatst, weggenomen.
Zo zijn de betrekkelijke plaatsen van NN’, OO’bekomen: het komt er nu op aan deze schaduwen tegebruiken om de betrekkelijk hoogte van het projectielte vinden ten opzichte van het vlak van de plaat. Op eenwillekeurige tafel wordt het buisstatief geplaatst, nadatmen de lamp en de koepel niet meer nodig heeft, voorde volgende handelingen (fig. 58 B).
Là encore, de multiples moyens ont été proposés etle plus souvent encore plus compliqués que ceuxempruntant la radioscopie! Nous retiendrons ici laméthode proposée par G. Massiot (fig. 58). L'ampouleétant placée en M, on introduit dans les rainures prati-quées sous le socle de la cupule, la plaquette de cartonou de fibre qui supporte le fil à plomb.
En déplaçant le porte-ampoule on amène un fil àplomb, représentant le rayon normal, au point qu'on achoisi comme trace de ce rayon.
Il faut repérer cet emplacement en disposant unetige T coulissant horizontalement le long du support etverticalement dans un écrou fendu, de façon que sonextrémité se confonde avec le plomb du fil, et que sadirection soit bien verticale.
On fait une première exposition (fig. 58-A) et dansces conditions l'extrémité de la tige donne la trace durayon normal en N, et une ombre du projectile P se faiten O. Une seconde pose est réalisée dans les mêmesconditions après avoir déplacé l'ampoule d'une quanti-té arbitraire.
Cette seconde exposition donne lieu à l'impressionnouvelle sur la même plaque de la trace du rayon nor-mal, émanant de M' en N' et une ombre O' du mêmeprojectile P. La plaque radiographique (R) qu'on avaitpréalablement posée sous le malade est ensuite retirée.
Ayant obtenu les positions relatives des points NN',OO': il s'agit maintenant d'utiliser ces ombres à larecherche de la hauteur relative du projectile par rap-port au plan de la plaque.
On porte sur une table quelconque ce porte-ampou-le, après avoir retiré l'ampoule et la cupule dont on n'aplus besoin, pour les manipulations qui vont suivre (fig.58-B).
Radioscopische tafel “Ledoux-Lebard” van het militair hospitaal Beveren-aan-de-IJzer (Privé verzameling).
Table radioscopique "Ledoux-Lebard" de l'hôpital militaire de Beveren-sur-Yser (Collection privée).
Musée (tekst ned.+fr)_Opmaak 1 16/02/11 11:29 Pagina 49
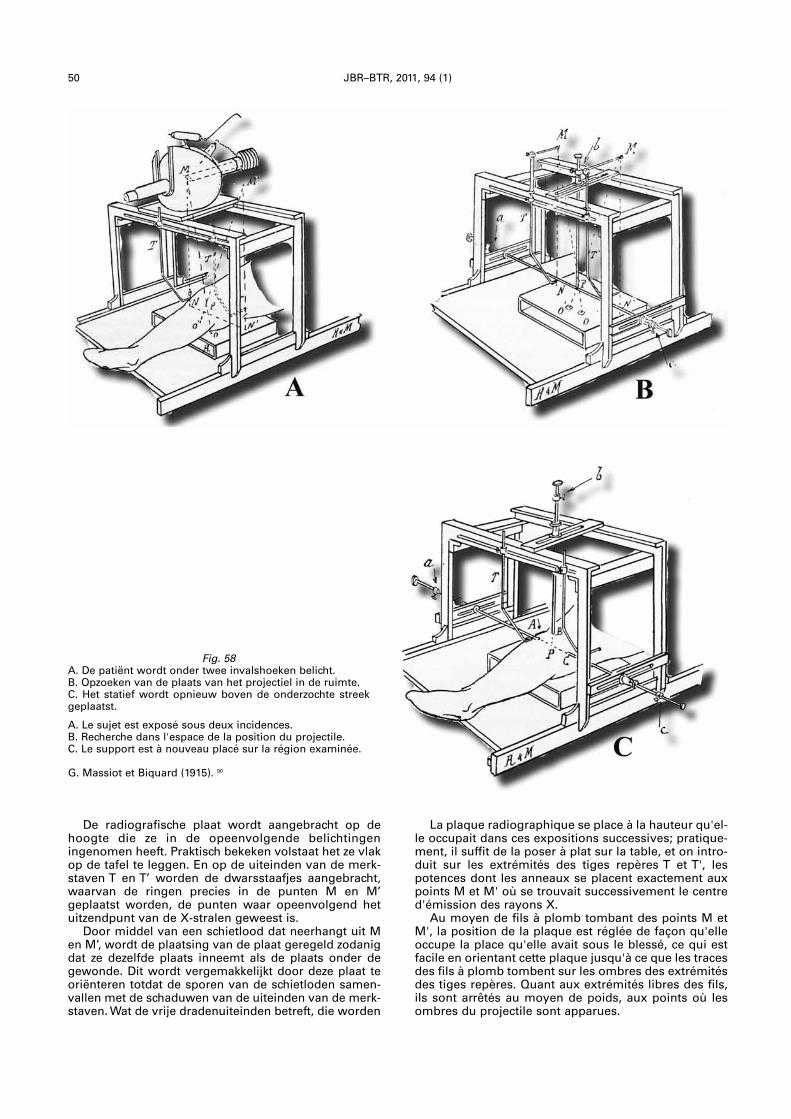
50 JBR–BTR, 2011, 94 (1)
De radiografische plaat wordt aangebracht op dehoogte die ze in de opeenvolgende belichtingeningenomen heeft. Praktisch bekeken volstaat het ze vlakop de tafel te leggen. En op de uiteinden van de merk-staven T en T’ worden de dwarsstaafjes aangebracht,waarvan de ringen precies in de punten M en M’geplaatst worden, de punten waar opeenvolgend hetuitzendpunt van de X-stralen geweest is.
Door middel van een schietlood dat neerhangt uit Men M’, wordt de plaatsing van de plaat geregeld zodanigdat ze dezelfde plaats inneemt als de plaats onder degewonde. Dit wordt vergemakkelijkt door deze plaat teoriënteren totdat de sporen van de schietloden samen-vallen met de schaduwen van de uiteinden van de merk-staven. Wat de vrije dradenuiteinden betreft, die worden
La plaque radiographique se place à la hauteur qu'el-le occupait dans ces expositions successives; pratique-ment, il suffit de la poser à plat sur la table, et on intro-duit sur les extrémités des tiges repères T et T', lespotences dont les anneaux se placent exactement auxpoints M et M' où se trouvait successivement le centred'émission des rayons X.
Au moyen de fils à plomb tombant des points M etM', la position de la plaque est réglée de façon qu'elleoccupe la place qu'elle avait sous le blessé, ce qui estfacile en orientant cette plaque jusqu'à ce que les tracesdes fils à plomb tombent sur les ombres des extrémitésdes tiges repères. Quant aux extrémités libres des fils,ils sont arrêtés au moyen de poids, aux points où lesombres du projectile sont apparues.
Fig. 58A. De patiënt wordt onder twee invalshoeken belicht.B. Opzoeken van de plaats van het projectiel in de ruimte.C. Het statief wordt opnieuw boven de onderzochte streekgeplaatst.
A. Le sujet est exposé sous deux incidences.B. Recherche dans l'espace de la position du projectile.C. Le support est à nouveau placé sur la région examinée.
G. Massiot et Biquard (1915). 90
Musée (tekst ned.+fr)_Opmaak 1 16/02/11 11:29 Pagina 50

VAN TIGGELEN 51
tegengehouden door een gewicht op die plaatsen waarde schaduwen van het projectiel verschenen zijn.
Het kruisingspunt van deze draden stelt de plaats vanhet projectiel voor.
Om de plaats ervan in de ruimte vast te leggen, tenoverstaan van welbepaalde coördinaten, worden deuiteinden van de drie staven a,b en c loodrecht aange-bracht aan de drie zijden van het buisstatief in het con-tact met punt P.
Met zorg wordt eveneens de aanwijzer C glijdendaangebracht op elke staaf, tegen hun respectievelijkehuls. Deze drie staven vormen samen het vlak waarin hetprojectiel zich bevindt. De draden die geen dienst meerdoen worden teruggetrokken. De drie staven worden vanmekaar verwijderd zonder de aanwijzer te verplaatsen,om toe te staan het lampenstatief opnieuw over debestraalde oppervlakte te plaatsen en dat op de plaatsdie het eerst ingenomen heeft, zoals getoond in fig. 58 C.
De drie staven a,b, en c worden naar mekaar toege-bracht en zodoende worden drie merkpunten bepaalddie met een dermatografisch potlood worden aange-bracht. Deze drie punten bepalen een vlak waarin hetprojectiel zich bevindt en de drie betrekkelijke afstandenvan elke aanwijzer aan de stavenhulzen, komenovereen met de diepte van het projectiel met betrekkingtot die drie punten.
De aanduidingen, gegeven door de betrekkelijkeplaatsen van de drie staven, kunnen volstaan maarimmobiliseren het radiografiematerieel tot op het ogen-blik waarop de chirurg wordt geroepen voor de ingreep.
Le point de croisement de ces fils représente la placedu projectile.
Pour en fixer la position dans l'espace, par rapport àdes coordonnées bien définies, les extrémités de troistiges a,b,c, sont amenées perpendiculairement auxtrois faces du porte-ampoule au contact avec le pointP.
On a soin également d'amener les index C coulissantsur chaque tige, contre leur douille respective. Ces troistiges constituent un plan dans lequel se trouve le pro-jectile. Les fils qui n'ont plus d'utilité sont retirés, lestrois tiges sont écartées sans déplacer les index, pourpermettre de poser à nouveau le support d'ampoule au-dessus de la région radiographiée et à l'endroit qu'iloccupait primitivement, comme le montre la figure 58-C.
Les trois tiges a, b, c, sont rapprochées au contactavec la peau, et l'on détermine ainsi trois points derepère qu'on trace avec un crayon dermographique.Ces trois points définissent un plan dans lequel se trouve le projectile, et les trois distances relatives dechaque index aux douilles des tiges, correspondentaux profondeurs du projectile par rapport à ces troispoints.
Les indications fournies par les positions relativesdes trois tiges peuvent être suffisantes, mais immobili-sent le matériel radiographique jusqu'au moment où lechirurgien sera appelé à intervenir.
Fig. 59Plaatsbepalingspasser voor de opsporing van projectielen, van Geneesheer Majoor E. Hirtz.
Compas-localisateur pour recherche de projectiles du médecin-major E. Hirtz.
Belgian Museum of Radiology
Musée (tekst ned.+fr)_Opmaak 1 16/02/11 11:29 Pagina 51
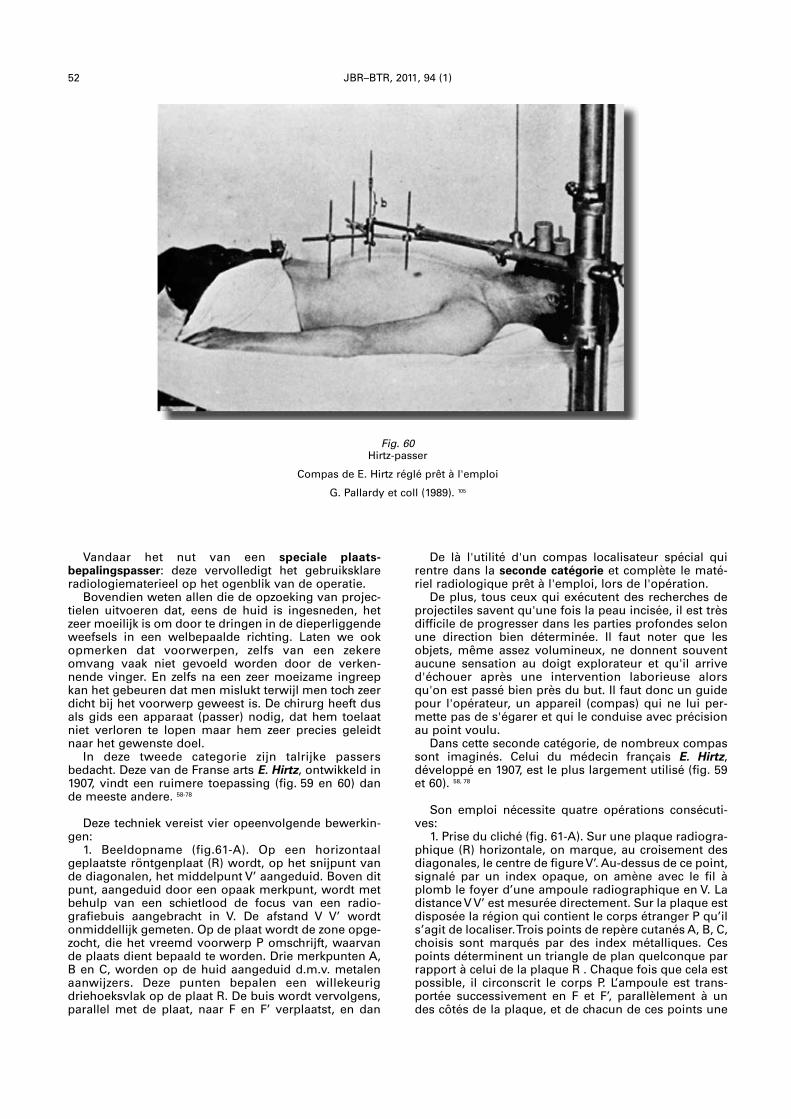
52 JBR–BTR, 2011, 94 (1)
Vandaar het nut van een speciale plaats -bepalingspasser: deze vervolledigt het gebruiksklareradiologiematerieel op het ogenblik van de operatie.
Bovendien weten allen die de opzoeking van projec-tielen uitvoeren dat, eens de huid is ingesneden, hetzeer moeilijk is om door te dringen in de dieperliggendeweefsels in een welbepaalde richting. Laten we ookopmerken dat voorwerpen, zelfs van een zekereomvang vaak niet gevoeld worden door de verken-nende vinger. En zelfs na een zeer moeizame ingreepkan het gebeuren dat men mislukt terwijl men toch zeerdicht bij het voorwerp geweest is. De chirurg heeft dusals gids een apparaat (passer) nodig, dat hem toelaatniet verloren te lopen maar hem zeer precies geleidtnaar het gewenste doel.
In deze tweede categorie zijn talrijke passersbedacht. Deze van de Franse arts E. Hirtz, ontwikkeld in1907, vindt een ruimere toepassing (fig. 59 en 60) dande meeste andere. 58-78
Deze techniek vereist vier opeenvolgende bewerkin-gen:
1. Beeldopname (fig.61-A). Op een horizontaalgeplaatste röntgenplaat (R) wordt, op het snijpunt vande diagonalen, het middelpunt V’ aangeduid. Boven ditpunt, aangeduid door een opaak merkpunt, wordt metbehulp van een schietlood de focus van een radio -grafiebuis aangebracht in V. De afstand V V’ wordtonmiddellijk gemeten. Op de plaat wordt de zone opge-zocht, die het vreemd voorwerp P omschrijft, waarvande plaats dient bepaald te worden. Drie merkpunten A,B en C, worden op de huid aangeduid d.m.v. metalenaanwijzers. Deze punten bepalen een willekeurigdriehoeksvlak op de plaat R. De buis wordt vervolgens,parallel met de plaat, naar F en F’ verplaatst, en dan
De là l'utilité d'un compas localisateur spécial quirentre dans la seconde catégorie et complète le maté-riel radiologique prêt à l'emploi, lors de l'opération.
De plus, tous ceux qui exécutent des recherches deprojectiles savent qu'une fois la peau incisée, il est trèsdifficile de progresser dans les parties profondes selonune direction bien déterminée. Il faut noter que lesobjets, même assez volumineux, ne donnent souventaucune sensation au doigt explorateur et qu'il arrived'échouer après une intervention laborieuse alorsqu'on est passé bien près du but. Il faut donc un guidepour l'opérateur, un appareil (compas) qui ne lui per-mette pas de s'égarer et qui le conduise avec précisionau point voulu.
Dans cette seconde catégorie, de nombreux compassont imaginés. Celui du médecin français E. Hirtz, développé en 1907, est le plus largement utilisé (fig. 59et 60). 58, 78
Son emploi nécessite quatre opérations consécuti-ves:
1. Prise du cliché (fig. 61-A). Sur une plaque radiogra-phique (R) horizontale, on marque, au croisement desdiagonales, le centre de figure V’. Au-dessus de ce point,signalé par un index opaque, on amène avec le fil àplomb le foyer d’une ampoule radiographique en V. Ladistance V V’ est mesurée directement. Sur la plaque estdisposée la région qui contient le corps étranger P qu’ils’agit de localiser. Trois points de repère cutanés A, B, C,choisis sont marqués par des index métalliques. Cespoints déterminent un triangle de plan quelconque parrapport à celui de la plaque R . Chaque fois que cela estpossible, il circonscrit le corps P. L’ampoule est trans-portée successivement en F et F’, parallèlement à undes côtés de la plaque, et de chacun de ces points une
Fig. 60Hirtz-passer
Compas de E. Hirtz réglé prêt à l'emploi
G. Pallardy et coll (1989). 105
Musée (tekst ned.+fr)_Opmaak 1 16/02/11 11:29 Pagina 52
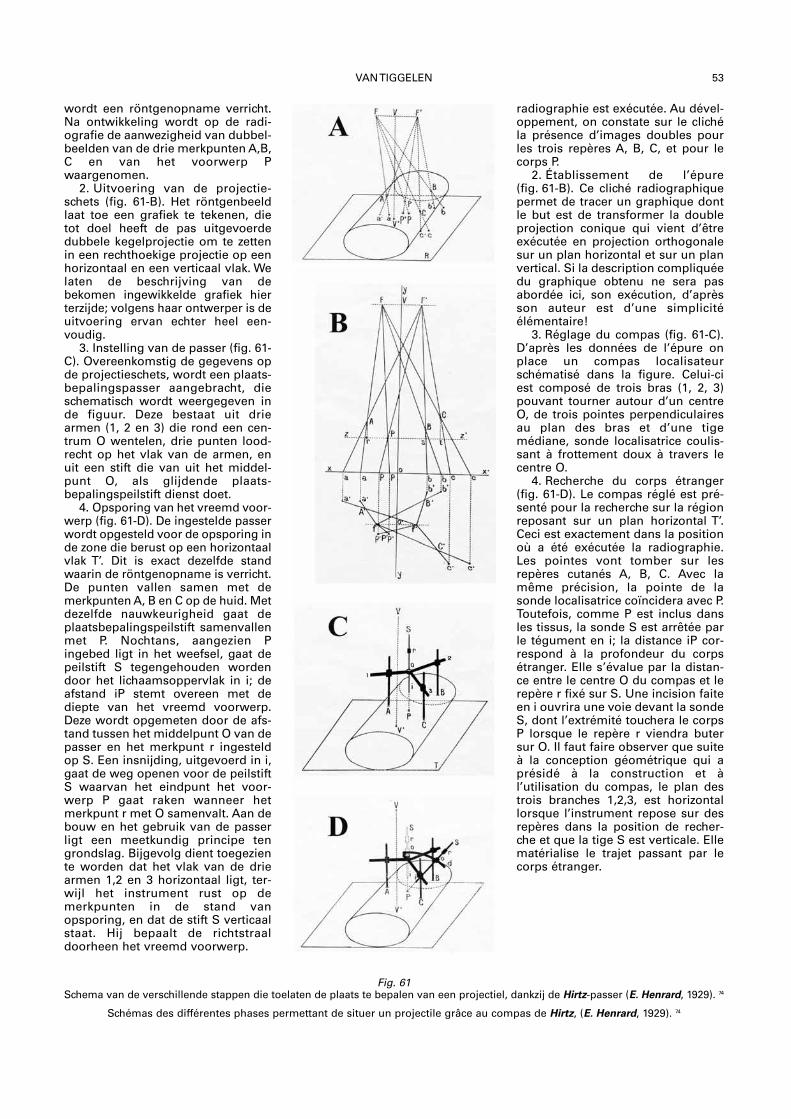
VAN TIGGELEN 53
wordt een röntgenopname verricht.Na ontwikkeling wordt op de radi-ografie de aanwezigheid van dubbel-beelden van de drie merkpunten A,B,C en van het voorwerp Pwaargenomen.
2. Uitvoering van de projectie -schets (fig. 61-B). Het röntgenbeeldlaat toe een grafiek te tekenen, dietot doel heeft de pas uitgevoerdedubbele kegelprojectie om te zettenin een rechthoekige projectie op eenhorizontaal en een verticaal vlak. Welaten de beschrijving van debekomen ingewikkelde grafiek hierterzijde; volgens haar ontwerper is deuitvoering ervan echter heel een-voudig.
3. Instelling van de passer (fig. 61-C). Overeenkomstig de gegevens opde projectieschets, wordt een plaats-bepalingspasser aangebracht, dieschematisch wordt weergegeven inde figuur. Deze bestaat uit driearmen (1, 2 en 3) die rond een cen-trum O wentelen, drie punten lood-recht op het vlak van de armen, enuit een stift die van uit het middel -punt O, als glijdende plaats -bepalingspeilstift dienst doet.
4. Opsporing van het vreemd voor-werp (fig. 61-D). De ingestelde passerwordt opgesteld voor de opsporing inde zone die berust op een horizontaalvlak T’. Dit is exact dezelfde standwaarin de röntgenopname is verricht.De punten vallen samen met demerkpunten A, B en C op de huid. Metdezelfde nauwkeurig heid gaat deplaatsbepalingspeilstift samenvallenmet P. Nochtans, aangezien Pingebed ligt in het weefsel, gaat depeilstift S tegengehouden wordendoor het lichaamsoppervlak in i; deafstand iP stemt overeen met dediepte van het vreemd voorwerp.Deze wordt opgemeten door de afs-tand tussen het middelpunt O van depasser en het merkpunt r ingesteldop S. Een insnijding, uitgevoerd in i,gaat de weg openen voor de peilstiftS waarvan het eindpunt het voor -werp P gaat raken wanneer hetmerkpunt r met O samenvalt. Aan debouw en het gebruik van de passerligt een meetkundig principe tengrondslag. Bijgevolg dient toegeziente worden dat het vlak van de driearmen 1,2 en 3 horizontaal ligt, ter-wijl het instrument rust op demerkpunten in de stand vanopsporing, en dat de stift S verticaalstaat. Hij bepaalt de richtstraaldoorheen het vreemd voorwerp.
radiographie est exécutée. Au dével-oppement, on constate sur le clichéla présence d’images doubles pourles trois repères A, B, C, et pour lecorps P.
2. Établissement de l’épure(fig. 61-B). Ce cliché radiographiquepermet de tracer un graphique dontle but est de transformer la doubleprojection conique qui vient d’êtreexécutée en projection orthogonalesur un plan horizontal et sur un planvertical. Si la description compliquéedu graphique obtenu ne sera pasabordée ici, son exécution, d’aprèsson auteur est d’une simplicité élémentaire!
3. Réglage du compas (fig. 61-C).D’après les données de l’épure onplace un compas localisateur schématisé dans la figure. Celui-ciest composé de trois bras (1, 2, 3)pouvant tourner autour d’un centreO, de trois pointes perpendiculairesau plan des bras et d’une tige médiane, sonde localisatrice coulis-sant à frottement doux à travers lecentre O.
4. Recherche du corps étranger(fig. 61-D). Le compas réglé est pré-senté pour la recherche sur la région reposant sur un plan horizontal T’.Ceci est exactement dans la positionoù a été exécutée la radiographie.Les pointes vont tomber sur lesrepères cutanés A, B, C. Avec lamême précision, la pointe de lasonde localisatrice coïncidera avec P.Toutefois, comme P est inclus dansles tissus, la sonde S est arrêtée parle tégument en i; la distance iP cor-respond à la profondeur du corpsétranger. Elle s’évalue par la distan-ce entre le centre O du compas et lerepère r fixé sur S. Une incision faiteen i ouvrira une voie devant la sondeS, dont l’extrémité touchera le corpsP lorsque le repère r viendra butersur O. Il faut faire observer que suiteà la conception géométrique qui aprésidé à la construction et à l’utilisation du compas, le plan destrois branches 1,2,3, est horizontallorsque l’instrument repose sur des repères dans la position de recher-che et que la tige S est verticale. Ellematérialise le trajet passant par lecorps étranger.
Fig. 61Schema van de verschillende stappen die toelaten de plaats te bepalen van een projectiel, dankzij de Hirtz-passer (E. Henrard, 1929). 74
Schémas des différentes phases permettant de situer un projectile grâce au compas de Hirtz, (E. Henrard, 1929). 74
Musée (tekst ned.+fr)_Opmaak 1 16/02/11 11:29 Pagina 53
19.11.11Annual RBRS symposium 2011Imaging of the spine and the spinalcord: state-of-the-artOrganization: Dr B. Desprechins
02.02.11RBRS – Cardiac imagingInformation: [email protected]
18.03.11RBRS – Cardiovascular and inter -ventional radiologyAntwerp, UZAInformation: Dr O. d’Archambeau,[email protected]
24-25.03.11ATELIERS DE COLONOSCOPIE VIRTUELLELiège, Clinique Saint-JosephInformation: www.chc.be
25.03.11RBRS – Bone and jointsInformation: [email protected]
21.04.11RBRS – Pediatric radiologyAntwerp, UZAInformation: [email protected]
21.05.11RBRS – Bone and jointsInformation: [email protected]
08-10.09.1124THANNUAL MEETING AND REFRESHERCOURSE OF THE ESHNRBruggeInformation: [email protected]
30.09.11RBRS – Cardiovascular and inter -ventional radiologyLeuven, KULInformation: Dr G. Maleux,[email protected]
11.10.11RBRS – Pediatric radiologyBrussels, UZInformation: [email protected]
18.10.11RBRS – Chest radiologyBrussels, UCL St LucInformation: [email protected]
21.11.11RBRS – NeuroradiologyInformation: [email protected]
16.12.11RBRS – Cardiovascular and inter -ventional radiologyInformation: Dr M. Laureys,[email protected]
03-05.06.111st ESUR TEACHING COURSE ONPROSTATE MRIGhentInformation:www.prostatemricourse.com
10.06.11RBRS – Head and neck radiologyInformation:[email protected]
14.06.11RBRS – Chest radiologyBrussels, UCL St LucInformation: [email protected]
20.06.11RBRS – NeuroradiologyInformation: [email protected]
21.06.11RBRS – Pediatric radiologyLiège, CHInformation: [email protected]
24.06.11RBRS – Cardiovascular and inter -ventional radiologyMont-Godinne, UCLInformation: Dr J.F. De Wispelaere,[email protected]
JBR–BTR, 2011, 94: 54-55.
FORTHCOMING COURSES AND MEETINGS
NATIONAL CALENDER
Detailed and real time information is available on RBRS website at www.rbrs.org
03.03.2011ECR 2011Information: www.myesr.org
14.03.2011Neonatal Ultrasound Course. Why, howand when an ultrasound image?Florence, ItalyInformation: www.aimgroup.eu
26.03.2011SIR 2011 Society of InterventionalRadiology Annual Scientific Meeting2011Chicago, USAInformation: http://www.sirmeeting.org/
03.04.2011SRES 11 Surgical and RadiologicalEndovascular SymposiumMartiniqueInformation: www.rbrs.org
03.04.201143rd International Diagnostic CourseDavosInformation: www.idkd.org
13.04.201114th European Society of Gastrointestinaland Abdominal Radiology Hands-onWorkshop on CT- Colonography 2011Gothenburg, SwedenInformation: http://www.esgar.org/index.php?pid=285&lang=1
18.04.2011Short Course on Abdominal Ultrasoundin Infectious Diseases and TropicalMedicine 2011Pavia, ItalyInformation: http://www.tropicalultrasound.org/
18.04.2011ERASMUS COURSE CardiovascularBologna, ItalyInformation: www.emricourse.org
27.04.2011GEST 2011 Europe – Global Emboliza tionSymposium and TechnologiesParis, FranceInformation: www.gest2011.eu
Annual Symposium 2011: 19.11.11
RBRS – Cardiovascular and interventio-nal radiology18.03.11, 24.06.11, 30.09.11, 16.12.11
RBRS – Bone and joints25.03.11, 21.05.11
RBRS – Pediatric radiology21.04.11, 21.06.11, 11.10.11
RBRS – Chest radiology14.06.11, 18.10.11
RBRS – Cardiac imaging02.02.11
RBRS – Neuroradiology20.06.11, 21.11.11
RBRS – Head and neck radiology10.06.11
Miscellaneous:24-25.03.11, 03-05.06.11, 08-10.09.11
INTERNATIONAL CALENDER
forthc. courses-94(1)_Opmaak 1 16/02/11 10:26 Pagina 54
FORTHCOMING COURSES AND MEETINGS 55
28.04.11ESOR GALEN ADVANCED COURSE:Urogenital Cross-Sectional ImagingBarcelona, SpainInformation: www.myESR.org/esor
04-07.05.11ADVANCED MRI 2011-02-01Graz, AustriaInformation:www.diagnosticzentrum.com
15.05.11INTERNATIONAL CONFERENCE OFNON-INVASIVE CARDIOVASCULARIMAGING 2011Amsterdam, The NetherlandsInformation: http://www.escardio.org/congresses/ICNC10/Pages/welcome.aspx
21.05.11ESGAR 2011 European Society ofGastrointestinal and AbdominalRadiologyVenice, ItalyInformation: www.esgar.org
08.06.11CONGRÈS 2011 MEETING CIRA-SFICV10e réunion annuelle de CIRA conjointement avec la SFICVMontreal, CanadaInformation & RegistrationFor Canadian and International participants:
22.06.11COMPUTER ASSISTED RADIOLOGY ANDSURGERY – 25th International Congressand Exhibition 2011Berlin, GermanyInformation: http://www.cars-int.org/
21-24.09.11USA, San DiegoISS MUSCULOSKELETAL IMAGINGCOURSEFUNDAMENTALS TO ADVANCED CONCEPTInformation:www.internationalskeletalsociety.com
21-25.10.11JFR – JOURNÉES FRANÇAISES DERADIOLOGYParis, FranceInformation: www.sfrnet.org
27.11-02.12.11RSNA ANNUAL MEETINGChicago, USAInformation: www.rsna.org
08.11.1111TH WORLD FEDERATION OF INTERVENTIONAL AND THERAPEUTICNEURORADIOLOGY CONGRESSSouth Africa, Cape TownInformation: www.wfitn2011.org
Registration (starting January 2011):www.ciraweb.orgE-mail: [email protected].: 514-282-2744For participants fromFrance:Registration (starting January 2011):[email protected]: [email protected].: 04 67 79 24 95
09-11.06.1118TH EUROPEAN SOCIETY OFMUSCULO SKELETAL RADIOLOGYMEETING (ESSR)Crete, GreeceMain theme refresher course:Bone marrow.Additional refresher courses on differentMSK topics.Scientific papers on all aspects of MSKRadiologyInformation: http://www.essr.org/cms/website.php?id=/en/essr_home.htm
18.06.11Paris, France8EME JOURNEE DE RADIOLOGIE HEPATO-BILIAIRE DU GROUPE HOSPITALIERBICETRE-PAUL BROUSSETheme: Les nouveautés technologiques– Le carcinome hépato-cellulaire revisitéen 2011 – L’exploration moderne desvoies biliairesInformation: Secrétariat du Pr M.F. Bellin,[email protected]
CLASSIFIED SERVICES
Experienced, native English teacher in Brussels offers:
1) Proofreading of oral presentations;2) Business English lessons.
References available upon request from commercial firms, civil servants within the EU institutions, and onefrom the Belgian Thoracic Society.
If interested please contact Iain Campbell on: [email protected] or on: mobile 0493-212244.
CLASSIFIED SERVICES
Région Lilloise, groupe radiologique, 5 sites dont scanner.Cherche plusieurs associés en vue de l’ouverture d’une IRM.Conditions financières très intéressantes.Revenus très importants.Pas de garde.Tél.: 00.33.6.13.23.84.69.
forthc. courses-94(1)_Opmaak 1 16/02/11 10:26 Pagina 55





![BP520 JBR 517 JBR - Universal Airlinesuvairlines.com/admin/resources/LHBP.pdfABONY 1L [ABO1L], JBR 1L Licensed to BRITISH AIRWAYS PLC, . Printed from JeppView disc 23-06. Notice: After](https://img.pdfslide.us/doc/110x75/603a9ab8acfc0749f75c4eb7/bp520-jbr-517-jbr-universal-abony-1l-abo1l-jbr-1l-licensed-to-british-airways.jpg)























