Embed Size (px)
Citation preview

January 28, 2005 Sean Tunis, M.D., MSc Chief Medical Officer Director, Office of Clinical Standards and Quality Centers for Medicare & Medicaid Services 7500 Security Blvd., Mail Stop S3-02-01 Baltimore, MD 21244 Dear Dr. Tunis: The purpose of this letter is to provide the Centers for Medicare and Medicaid Services (CMS) with a unified response from the nephrology community to the Draft Policy on Monitoring of Erythropoietin for Beneficiaries with End Stage Renal Disease (ESRD) that was released on July 8, 2004. In the interest of patient care, representatives of the broad nephrology community, including patient groups, providers, professional organizations, and industry have come together to present CMS with the following consensus position and recommendation. Consensus Position and Recommendation from The Nephrology Community The Draft Policy proposes new rules for review of dialysis patient claims. Specifically, the Draft Policy focuses on monitoring absolute erythropoietin (EPOGEN®, epoetin alfa, or EPO) doses at specific hemoglobin levels, rather than monitoring for appropriate EPO dose adjustments. Monitoring of EPO dose adjustments is necessary given the wide variability in both patient hemoglobin levels and individual response to EPO. Following the release of the Draft Policy, the implementation of the Medicare Modernization Act (MMA) has resulted in a fundamental change in the payment policy for dialysis services, including separately billable drugs, which was intended to address CMS’s stated concerns regarding perverse incentives related to drug utilization1. Any subsequent changes in payment or coverage could significantly impact the quality of care for this fragile and chronically ill patient group. In light of these changes, the broad nephrology community has come together to provide a consensus recommendation with the goal of preserving patient outcomes. The potential impact of an overly restrictive EPO monitoring policy is well known to the nephrology community, as seen in the decline of the dialysis population’s hemoglobin levels following implementation of the initial policy in 1997. As a result, the monitoring policy was modified in 1998 to its current form, which utilizes post-payment review. 1 CMS July 8, 2004 Draft Policy: Monitoring of Erythropoietin for Beneficiaries with End Stage Renal Disease.

Renal Community Consensus Letter Dr. Sean Tunis Page 2 of 12
In response to the July 2004 Draft Monitoring Policy, a broad representation of key stakeholders in the nephrology community provided CMS with detailed comments suggesting that the Draft Policy would result in unintended consequences and negatively impact the quality of care for dialysis patients. After a review of these stakeholder comments, the revised payment policy for ESRD-related medications, and published data suggesting that practitioners appropriately titrate EPO doses in response to observed hemoglobin levels2, the nephrology community believes that the impetus for the Draft EPO coverage policy has been reduced. The nephrology community recommends that CMS direct fiscal intermediaries (FIs) to refrain from implementing their own Local Medical Review Policies (LMRPs) regarding EPO use in dialysis due to the risk of further impairing quality of care and potentially increasing the number of patients with hemoglobin levels below 11g/dL. Should CMS decide that it is in the best interests of patients and that there is sufficient need to continue an EPO coverage policy, we strongly recommend that CMS implement a policy based on sound scientific and clinical rationale using the following core tenets:
• Full and timely reimbursement of EPO claims should be made when physicians appropriately adjust EPO doses in response to observed hemoglobin levels. Reimbursement should not be guided by an arbitrary dose edit that does not recognize individual patient requirements.
• CMS should maintain only a post-payment review framework. This is especially important due to the precarious financial status of small providers.
• A claims-based solution should utilize a single claim form. • When necessary, reduced reimbursement should be guided by recommended dose
adjustments rather than dose edits. Absolute dose edits fail to take into account inherent patient variability in response as well as differences in EPO requirements due to individual body habitus.
• Full payment should be made when medical justification for a hemoglobin level or a prescribing decision is provided.
In an effort to be constructive and to provide CMS with a consensus recommendation, the nephrology community stakeholders held a series of meetings, which culminated in the following consensus recommendation on a specific audit procedure for EPO3:
2 Collins, A., et al. (2004) Longitudinal Evaluation of Hemoglobin (Hb) Levels and Epoetin alfa Doses in US Hemodialysis Patients Reveals Important Trends in Anemia Management. Abstract presented at the American Society of Nephrology Meeting October 2004. In this analysis, Dr. Collins et al. looked at a total of 150,279 patients representing 5,806 dialysis facilities. The Hb values of those patient cohorts that had a starting mean Hb either above or below the 11.0 to 12.5 g/dL range migrated into the target range during the analysis period (P < 0.01). To achieve this, Epoetin alfa doses were titrated in response to Hb levels (P < 0.01 comparing April vs. May mean Epoetin alfa doses). Among patients with a starting mean monthly Hb value within the 11.0 to 12.5 g/dL range, mean Epoetin alfa doses were essentially unchanged over time (P > 0.05). 3 This recommended policy should not apply to the small number of ESRD beneficiaries receiving home dialysis.

Renal Community Consensus Letter Dr. Sean Tunis Page 3 of 12
• Physicians and providers should be instructed to include two hemoglobin values on each claim form: both the last hemoglobin value from the previous claim period and the last hemoglobin value from the current claim period.
• CMS should allow for a value code on the claim form to indicate that the EPO dose was appropriately reduced by at least 25%4 in response to reported hemoglobin above the audit threshold of 13g/dL (when medical justification is not included).
• When there is a hemoglobin value above the audit threshold of 13g/dL, the individual EPO dose immediately preceding and following that dose reduction should be included on the claim form, thereby providing additional documentation of appropriate dose reduction.
• Claims that contain two hemoglobin values above the audit threshold of 13g/dL without a value code indicating that the EPO dose was appropriately reduced by 25%, or without medical justification, should be subject to post-payment review. In the absence of medical justification or documentation of an EPO dose reduction of 25% (utilizing the two EPO doses provided), the EPO component of the claim should be subject to a 25% payment penalty for that claim period.
Summary of Consensus Recommendation
Hb Value #1 (g/dL)
Hb Value #2 (g/dL)
Action in Response to Hb Value #1 ≥ 13 g/dL FI Action
>13 <13 Any No post-payment review
Value code indicating >25% EPO dose reduction
No post-payment review
>13 >13 In the absence of a value code, documentation of doses showing a >25% EPO dose reduction
Or Medical justification only
Post-payment review resulting in full
payment
>13 >13 No evidence of a >25% EPO dose reduction nor medical justification
Payment reduction of EPO portion of claim
by 25% We have used a hemoglobin administrative threshold of 13g/dL as included in the CMS Draft Policy The complexity of monitoring EPO utilization cannot be overstated. In comments submitted to CMS, the nephrology community has emphasized that a limited cross-
4 The 25% dose adjustment was selected based on recommendations included in the EPO package insert and the NKF- K/DOQI™ Clinical Practice Guidelines for Anemia of Chronic Kidney Disease, 2000 (Am J Kidney Dis. 2001; 37 (supplement 1):S182-S238).

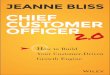
Renal Community Consensus Letter Dr. Sean Tunis Page 4 of 12 sectional evaluation of EPO dose and hemoglobin is incapable of discriminating appropriate from inappropriate EPO prescribing. Thus, changes to the Medicare EPO coverage policy should be considered with extreme care, as the adverse unintended impact on patient outcomes following a coverage and payment policy change in the ESRD setting could be substantial. Finally, as CMS seeks to further improve the quality of care for ESRD patients, we urge that CMS focus attention on preventive strategies to reduce the incidence of ESRD among Medicare beneficiaries, which represents an important potential opportunity for cost savings to CMS in the ESRD system.5 We would look forward to meeting with CMS to discuss this specific consensus recommendation. Sincerely,
Lesley Dinwiddie President American Nephrology Nurses’ Association
John Newmann Chair, Public Policy Committee American Kidney Fund
5See Figure 1.

Renal Community Consensus Letter Dr. Sean Tunis Page 5 of 12
Mary Jane Helenek President & CEO American Regent
Helen Torley Vice President & General Manager Nephrology Business Unit Amgen
Randall W. Maxey President AMMA
Tomas Berl, M.D. President American Society of Nephrology
C. Basil Mundy Vice President, Government Affairs and Corporate Relations Bone Care International

Renal Community Consensus Letter Dr. Sean Tunis Page 6 of 12 Susan Vogel President California Dialysis Council
Diane Wish President & CEO Centers for Dialysis Care
Kent J. Thiry Chairman & CEO DaVita, Inc.
President DaVita Patients Citizens

Renal Community Consensus Letter Dr. Sean Tunis Page 7 of 12
Mats Wahlstrom President Fresenius Medical Care North America
Larry Buckelew Gambro Healthcare
Kathleen E. Means President Kidney Care Partners
Dori Schatell Executive Director Medical Education Institute
David Warnock, M.D. President National Kidney Foundation

Renal Community Consensus Letter Dr. Sean Tunis Page 8 of 12
Maureen Michael President National Renal Administrators Association
Joyce Jackson President and Chief Executive Officer Northwest Kidney Centers
Raymond M. Hakim, M.D. Executive Vice President and Chief Medical Officer Renal Care Group, Inc.
RPA Jim Weiss Renal Physicians Association

Renal Community Consensus Letter Dr. Sean Tunis Page 9 of 12
Lori Hartwell Renal Support Network
Mark Burke Chief Executive Officer Satellite Healthcare cc: Dr. Mark McClellan

Renal Community Consensus Letter Dr. Sean Tunis Page 10 of 12
APPENDIX The Scientific and Clinical Rationale Supporting the Consensus Position and Recommendations In the comment letters provided to CMS, the nephrology community has consistently emphasized the following key points in support of their position:
• Patients with hemoglobin levels within the NKF-K/DOQI™ recommended target
range (11 – 12 g/dL) have better outcomes than those below the target level. • There is considerable natural variability in individual patient hemoglobin levels,
making it difficult to consistently maintain hemoglobin within a narrow range. This variability means that intermittent excursions above the administrative threshold level of 13 g/dL occur despite the appropriate utilization of EPO.
• In general, there is greater than 20-fold variability in EPO doses required to achieve target hemoglobin levels6.
• Stopping and starting EPO therapy can lead to dramatic dips in hemoglobin levels that may require high doses of EPO to regain the target level.
• Analyses demonstrate that when patient care is observed over time (i.e., longitudinally), EPO doses are appropriately adjusted as necessary to maintain target hemoglobin levels7.
The Draft Policy Proposed by CMS Will Have Serious Unintended Consequences CMS issued the Draft Policy to address, in part, the agency’s perception of over-utilization of EPO, as stated in the October 2003 Solicitation for Comment. Based on the many comments submitted to CMS in October 2004, the vast majority of patients are managed with appropriate EPO utilization8. Importantly, the nephrology community is particularly concerned that the potential negative impact on the quality of care of patients following implementation of the Draft Policy may be magnified if this is done concurrently with the reimbursement changes for EPO, as stated in the 2005 Physician Fee Schedule Final Rule. The Draft Policy focuses on monitoring absolute EPO doses, instead of examining appropriate dose adjustments. Editing of EPO doses without consideration of the change in EPO dose is inconsistent with both the FDA-approved EPOGEN® package insert and the recognition that individual sensitivity to EPO is highly variable. The Draft Policy as written will identify a great number of false positive claims for review ⎯ a costly inefficiency that potentially penalizes appropriate patient care. Identification of a high
6 Eschbach et al. Annals of Internal Medicine. 1989; 111:992-1000 7 Collins, A., et al. (2004) Longitudinal Evaluation of Hemoglobin (Hb) Levels and Epoetin alfa Doses in US Hemodialysis Patients Reveals Important Trends in Anemia Management. Abstract presented at the American Society of Nephrology Meeting October 2004. 8 ibid

Renal Community Consensus Letter Dr. Sean Tunis Page 11 of 12
proportion of false positive claims may result in changes in physician behavior and compromise the quality of care, as evidenced by an increase in the percentage of patients with hemoglobin levels below 11 g/dL9. The Draft Policy is also designed to monitor care using a single claim form, containing the last hemoglobin of the claim period and the total monthly EPO dose. Because physicians adjust EPO doses as necessary to maintain target hemoglobin levels, monitoring care through an evaluation of EPO doses that precede observed hemoglobin levels is suboptimal. Hemoglobin values often remain above the recommended target range during the time period of a single claim, despite appropriate EPO dose reductions. Thus, implementation of the Draft Policy would result in the flagging of a substantial number of claims (9% per claim period and 50% of patients with at least one flagged claim per year); over two-thirds of these flagged claims would ultimately result in full payment because they reflect appropriate EPO dosing in response to previous hemoglobin levels (i.e., false positive claims). Furthermore, Analyses of the Draft Policy’s impact predict a possible increase in the percentage of patients with hemoglobin levels below 11 g/dL, the extent of which will depend on physicians’ and providers’ tolerance for the percentage of reviewed claims10.
9 Reference: Amgen’s August 25, 2004 Comment Letter (Appendix I) on the Draft Policy on Monitoring of Erythropoietin for Beneficiaries with End Stage Renal Disease (ESRD). 10 Reference: Amgen’s August 25, 2004 Comment Letter (Appendix I, page 9) on the Draft Policy on Monitoring of Erythropoietin for Beneficiaries with End Stage Renal Disease (ESRD).

Renal Community Consensus Letter Dr. Sean Tunis Page 12 of 12
Figure 1
Jan 2005CDRGChronic Disease Research group
Patients: 2002 Period prevalent FFS
Expenditures: 2002Period prevalent costs
All Medicare
DM
CHF ESRD
CKD
Chronic Kidney Disease in the Medicare Population: CKD, DM, CHF; Size and Cost*
Size Cost
5.8%
1.1%
20.7%25.1% 41.3% 48.1%
19%
7.8%
*USRDS special study for CMS
3836826v3