Embed Size (px)
Citation preview
Document number: GRNP1/CN/0012 Version: 1 Page 1 Paper copies of this document should be kept to a minimum and checks made with the electronic version to
ensure the version to hand is the most recent.
ISUE01 BCUHB FRAMEWORK UNDERTAKING PATIENT EXPERIENCE STORIES Date to be reviewed:
September 2013 No of pages: 30
Author(s): Christine Cowley Diane Henderson
Author(s) title: Lead Nurse Professional & Practice Development PPI Manager
Responsible dept / director:
Improving Service User Experience Team
Approved by: Improving Service User Experience sub-group Date approved: 16th September 2010 Endorsement by: Hilary Stevens, Non-Exec Date endorsed: 16th September 2010 Date activated (live):
April 2011
Documents to be read alongside this document: Complaints Policies and Procedures Consent to Share Information (Child Protection) Policy Data Protection Freedom of Information Act 2000 and Environmental Information Regulations Good Research Practice – Data Management Policy Maintaining Confidentiality Procedure Guidelines for obtaining consent in respect of Children and Young People Informed Consent to Treatment and Investigation Policy Single Equality Scheme 2010 Lone Working Policy Freedom of Information Act 2000 Caldicott Committee Report 1997 Review
Purpose of Issue/Description of current changes: New policy document for BCUHB
First operational: April 2011 Previously reviewed: Changes made yes/no:
PROPRIETARY INFORMATION
This document contains proprietary information belonging to the Betsi Cadwaladr University Health Board. Do not produce all or any part of this document without written
permission from the BCUHB.
Version: 1
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 2 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
CONTENTS
1. Introduction ............................................................................ 3
1.2. Benefits ....................................................................................... 3
2. Purpose of this Framework ................................................... 4
3. Scope ...................................................................................... 4
4. Finding patients, carers, service users who are willing to tell their stories.................................................................................... 4
4.1. Inviting people to come and tell their stories ............................... 5
5. The Interview Process ........................................................... 5 5.1. Summary of the Process ............................................................. 5 5.2. Conducting the Patient Story Interview ....................................... 6
6. Action following the Interview .............................................. 7 6.1. Immediate Action following the Interview .................................... 7 6.2. Summarising the interview and action planning .......................... 7
7. Maintaining a record of Patient’s Stories ............................. 8
8. Storage of Transcripts of Interviews .................................... 8 8.1. Storage of Information ................................................................. 8 8.2. Use of Information ....................................................................... 9
9. Training and Experience........................................................ 9 9.1. Who can undertake Patient Story interviews? ............................. 9 9.2. Responsibility .............................................................................. 9
10. Future Developments .......................................................... 10 Appendix 1: 1000 Lives One Story - Four Applications ....... 11
Appendix 2: Example Patient’s Stories Information Leaflet for Patients ........................................................................................ 12
Appendix 3: Guidance for Video or Digitally recorded Stories14
Appendix 4: Patient’s Stories Registration Form ..................... 18
Appendix 5: Patient’s Stories Consent Form – Section A ....... 19
Appendix 6: Equality Monitoring Information .......................... 21
Appendix 7: Patient Stories Transcript Form ........................... 22
Appendix 8: Conducting Patient Stories Flow Chart ............... 24
Appendix 8: Summary of the Caldicott Principles ................... 25
Appendix 9: Summary Reporting Incidents, Concerns and Complaints that may arise during the Patient Interview ......... 26
Appendix 10 – Contact Details for further advice .................... 28
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 3 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
1. Introduction Patients’ Stories are about learning and actively listening to patients’, relatives ‘or carers’ stories of their healthcare journey. It involves looking at the care and emotional journey that they experience when they come into contact with health services. It is a means of engaging with patients and carers in a different way by developing a genuine equal two-way conversation. The conversation is not looking for facts, or judgements, but values the story teller’s unique perspective of their experience. The same methodology can be used to listen to staff stories; therefore this framework can be used for both the recording of patients and staff stories. Staff may want to tell their stories as an advocate for patients, or to share their own experiences of a healthcare journey as a patient, carer, or as a member of staff. If this framework is being used to collect staff stories just transpose the word patient to staff. To aid a free flow of conversation a loose structure is applied to the story telling / taking interview. The focus of the inquiry is the experience of being a patient or relative, with the aim shifting from simply trying to measure patient satisfaction to actively improving our understanding of their experience and their needs. The use of patient stories in organisations has been described as using an old skill in a new context. The essence of the approach is storytellers being listened to, by observers who identify key elements coming out in the stories. Stories are memorable and self-propagating and a story that describes direct experience changes understanding, giving the listener an opportunity to learn from tacit knowledge. At its core is the use of knowledge to identify changes. Stories can be a powerful way of sharing problems and solutions and are a way of influencing and informing staff. The nature of this method of gaining service user feedback lies within the modernisation of the NHS and specifically the 1000 Lives Campaign and Nurse Leadership Programmes. It is emerging as a developing research methodology. The 1000 Lives Campaign promotes the use of patients’ stories as an effective and powerful way of making sure that patients’ voices are heard and improvement is centred on the needs of patients. They describe one story as having four potential applications, these being: learning, education, media relations and inspiring (see appendix 1). The emphasis is on discovering the experiences of patients and carers at a local level, and taking local actions as a consequence. 1.2. Benefits Embedding this approach into the culture of BCUHB will make patients’ stories an accepted method by which we: Identify areas of concern and areas of good practice. Ensure that patients / staff feel valued and listened to. Identify equality and human rights principles and links to service improvement. Reduce complaints.
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 4 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Improve listening and questioning skills of staff. Create a culture of openness. Increase our understanding of the effect of ill health and the clinical environment
on individuals. Increase reflection and feedback to staff, improving communication, teamwork
and relationships which will as a result improve the working environment and patient care.
Celebrate and share good practice. Model for improvement and an approach to service planning. 2. Purpose of this Framework The purpose of this framework is to ensure there is an agreed process and set of standards to support the recording of patient stories. It provides: A rationale for the process. Information and guidance to staff undertaking narrative interviews. A process by which interviews are conducted and feedback given. Standards to ensure the requirements of governance, data protection and
confidentiality are maintained. Protection to patients, public, staff and the organisation. 3. Scope
The document applies to all staff within BCUHB. 4. Finding patients, carers, service users who are willing to tell
their stories Some patients’ stories are so compelling that they may be recorded and acted on, on an individual basis. However, the majority of narratives should not be established as a stand alone activity. They should form part of local service improvement plans and quality improvement activities. The learning gained from them also has the potential to influence wider organisational strategies and plans. Patients’ narratives may occur at a number of different levels ranging from care, treatments, service developments and strategic policy making. An example in BCUHB is the recording of stories of patients who had undergone upper G.I. surgery. Their stories were recorded digitally with the intention of sharing the experiences of patients with healthcare professionals, other patients, and carers, and to inform service improvements. Once the context and service area has been agreed there are several routes that can be used to recruit people who are willing to share their stories. These may include:
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 5 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Poster/leaflet campaigns in GP surgeries, rehabilitation classes, Expert Patient Programme groups, outpatient’s clinics etc. Posters and leaflets will need to be adapted to fit context and service area. For an example patient information leaflet (see appendix 2).
Asking patients and carers before discharge if they would be interested in being involved at a later date.
Approaching local patients’ support groups or volunteer sector organisations. Placing information on BCUHB websites or partnership websites. Placing information in BCUHB newsletters or partnership organisations
newsletters. People who have made complaints to the Health Board may wish to tell their
story. This should be done after the complaints process has been completed. 4.1. Inviting people to come and tell their stories People who have agreed to tell their story should be contacted before the interview to ensure that:
The interview process is explained to them. A mutually convenient time and date is agreed for the interview. They have received a copy of a Patient’s Story information leaflet (appendix
2) They are advised that consent will be required and that their story may be
tape-recorded, videoed, digitally recorded or written notes taken. They are aware that their story will be anonymised and will be shared with the
team and other health care professional as appropriate, to bring about service improvements.
That they still have the option to opt out at any time during the interview, or to request their story is deleted at a later stage should they change their mind.
5. The Interview Process 5.1. Summary of the Process
Patient stories are gathered in a one-to-one (sometimes small group) setting where a two-way conversation takes place.
Ideally the person conducting the interview should not have been directly
involved in the story teller’s care. Patients and/or carers should be offered the opportunity to tell their stories to someone totally unconnected with their past or potentially future treatment. However, some patients may wish to tell their story to someone they have built a rapport with, this will need to be agreed with individual patients.
The purpose is not to investigate specific areas or issues but to listen to the
story teller. The interview style should be unobtrusive and non-directive, only asking direct
questions to seek clarification of an issue.
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 6 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Open and prompt questions should be used. These encourage a natural
discussion about experiences that may trigger significant memories and thoughts, producing a biography of care from their perspective.
The interview can be tape recorded, or written notes taken at the time of the
interview. If the interview is to be recorded by note taking it is advised that the interviewer is accompanied by a note taker, in order not to disturb the free flow of the conversation.
In some cases it may be decided to video or digitally record a patient’s story.
The style of recording should be agreed with the story teller before the interview. For further information about video or digitally recording stories see appendix 3.
All patients’ stories must be registered on the Health Board’s Patient Stories
Registration form (see appendix 4)
Consent must be obtained before the interview takes place (see appendix 5) 5.2. Conducting the Patient Story Interview Table 1: If you have not undertaken an interview before please speak to your line manager for further advice, or contact one of the contacts listed in Appendix 10.A. Prepare the environment and set the scene Interviews must take place in private, away from the area of care. If the story is to
be recorded away from BCUHB premises, please consider the Lone Working Policy.
The interview area must be accessible for people with physical or sensory impairments.
The patient’s language of choice must be taken into account. Ensure that the interview will not be disturbed. Offer refreshments and put the story teller at their ease. Explain the interview process and how long the interview is likely to take. B. Gain consent Consent is the patient’s/carer’s permission for the interview to take place, and to
agree in what context the story will be used once recorded. For the consent to be valid, the story teller must: be competent to make the particular decision; have received sufficient information to make an informed decision not be acting under duress. Advise the confidentiality will be maintained, however this can not be
guaranteed if potential POVA, child protection of criminal issues arise. Consent to undertake a Patient’s Story must be obtained using the Health
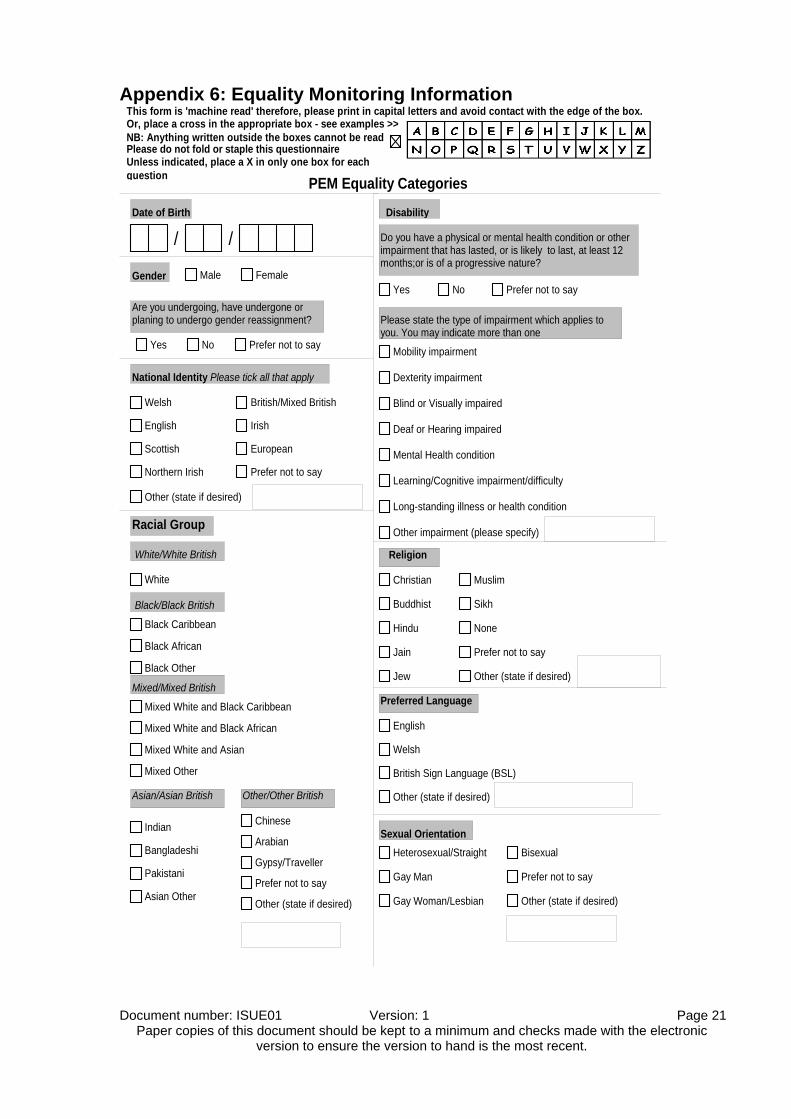
Board’s Patients’ Stories consent form (see appendix 5) C. Equality Monitoring Ask patient to complete Equality Monitoring (see appendix 6) and return to the
co-ordinator of the central database.
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 7 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
D. The interview Using open questions invite the storyteller to talk about their experiences. Questions listed below may be used but these are only a guide.
o What was it like to be a patient in, X? o What do you remember the most? o Is there a significant memory of care? o Was there anything that surprised/worried/pleased you? o How did that make you feel? o Were your needs met? o Tell me more about………… o Is there anything you would like to add?
Searching questions should be used to probe into areas of concern. For example, comments made about how they were spoken to may prompt the interviewer to probe more deeply on communication issues and/or staff attitude.E. Closing the Interview Thank the storyteller for their contribution and explain the interview will be analysed, anonymised and where appropriate shared with colleagues. Story telling can be an emotional experience; it may be necessary to spend some
time with the storyteller to offer support if needed. In some cases it may be appropriate to advise them to seek the support of their GP, Nurse Specialist or local voluntary organisations who may be able to arrange additional emotional support.
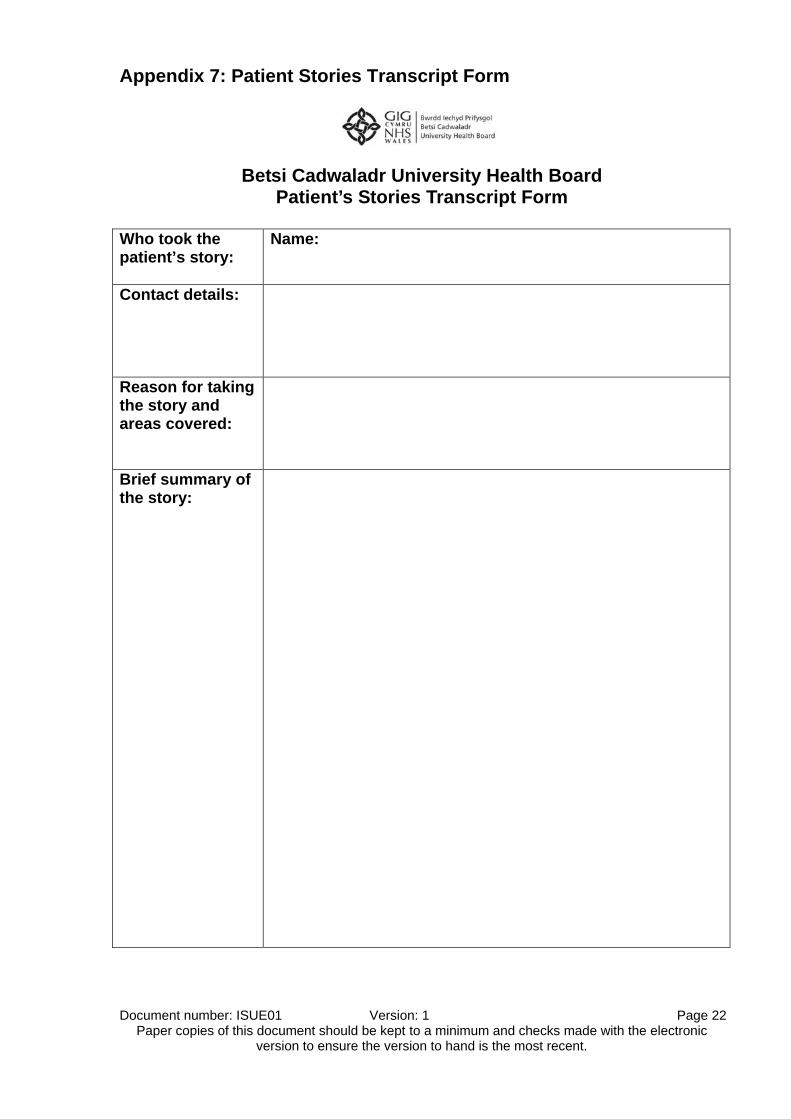
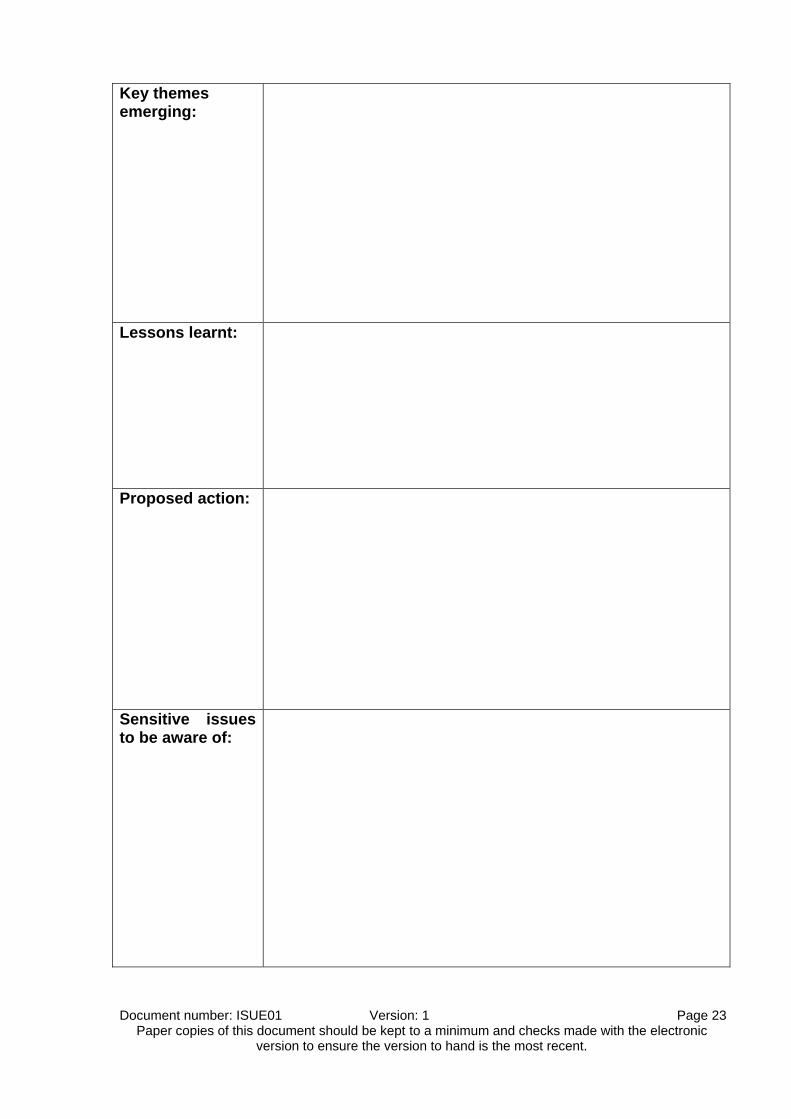
6. Action following the Interview 6.1. Immediate Action following the Interview The story taker should where possible initiate any changes that can be made immediately to improve care, or the environment. 6.2. Summarising the interview and action planning Table 2 A. Summarise the interview Ideally within 48-hours review the story and map its content. Prepare a summary of the story, using the transcript form (appendix 7) Record significant statements, incidents, themes and descriptions. Document themes under specific headings Include areas for quality improvement and indicators of good practice. Agree content with story teller
Notes must be anonymised and tapes coded. All information must be stored in a locked cupboard/desk with only the interviewer having access.B. Present and Share Findings It is suggested that the findings are shared with senior staff/managers who will discuss with the interviewer the most appropriate mechanism of sharing with colleagues. The interviewer may be required to attend meetings to relate the patient’s story to others, or to assist the participants in understanding outcomes from a patient’s
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 8 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
perspective. If this is the case the story should be reported from the patients’ point of view and not reinterpreted by staff. Stories that are short can be read verbatim. Rarely, should patients be asked to attend formal meetings to give their account in person. It may be more appropriate for the story taker to attend meeting to recount the story on behalf of the story teller.
C. Develop an action plan for improvement The interviewer, along with their line manager and colleagues must develop a plan of action to address the changes the interviews have highlighted. The responsibility for taking action should be shared equally amongst the team and may even be incorporated into individual performance plans. Involve patients and cares in considering how and what the improvements should be made and how they should be implemented.
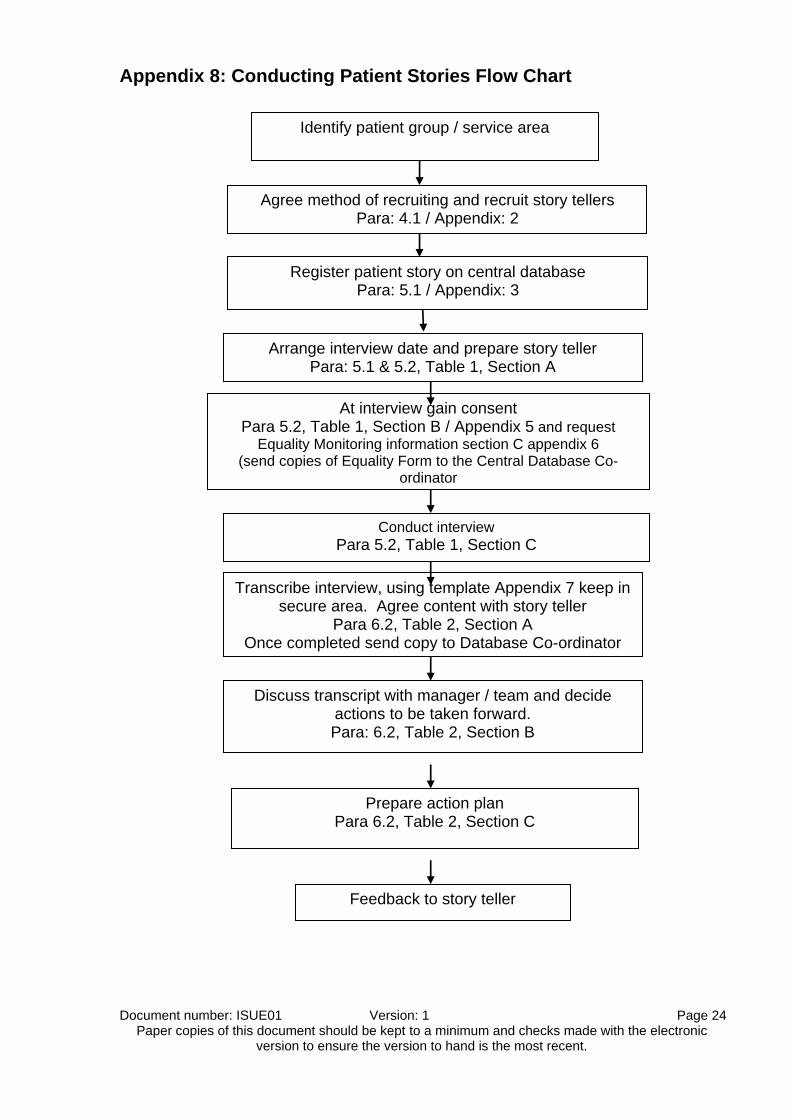
See appendix 6, which details a Flow Chart for conducting Patient Stories 7. Maintaining a record of Patient’s Stories A central register of Patients Stories will be maintained and all stories must be registered using the Patient Stories Registration form (see appendix 4). However, Clinical Programme Groups (CPGs) and other story takers are responsible for their own data; and are required to maintain records of:
Numbers of stories that have been recorded. Who took the stories and the area they covered. Details of key themes. Action plans and progress against them. Changes have been tested and records of improvements made.
8. Storage of Transcripts of Interviews 8.1. Storage of Information
Once themes have been identified, tapes and hand written notes must be destroyed by the interviewer. Until that time, to prevent unauthorised access or loss, the information must be stored carefully in locked filing cabinets, with controlled access. Information must be stored as per the following policies and procedures:
Data Protection Good Research Practice - Data Management Policy Maintaining Confidentiality
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 9 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
8.2. Use of Information The Caldicott principles (appendix 8) must be adhered to in terms of patient confidentiality. The following is a summary of these principles;
Justify the purpose of holding data. Only use the data when absolutely necessary. Only use the minimum data required. Access to data is strictly on a need to know basis All employees must understand their responsibilities Understand and comply with the law
9. Training and Experience 9.1. Who can undertake Patient Story interviews? Interviews can be undertaken by members of staff (with agreement of their manager) and who have: Previous interview or counselling experience or skills. Training or experience in undertaking patient narrative interviews, i.e., through
the RCN Clinical Leadership Programme, or other relevant forms of training such as training through the 1000 Lives Campaign or experience from approved research projects.
The ability to put interviewees at ease and make them feel safe. Ability through questioning / interview skill to keep the storyteller on track without
leading them down a particular path. Personal robustness to be able to listen to people who on occasions may
describe difficult and distressing stories. 9.2. Responsibility Each person undertaking patient narratives is responsible for: Registering the story
Gaining consent and requesting that the patient completes an Equality Monitoring form.
Being familiar with additional support available to the story teller should unresolved, distressful issues.
Recognising their limitations and acknowledging when they need advice and support from a more experienced member of staff.
Recognising when issues revealed need to be acted upon immediately or are able to be addressed in subsequent action plans.
Recognising the need for confidentiality and maintaining anonymity of the people involved while at the same time recognising the need to share relevant information.
To disclose information where there may be a potential POVA, Child Protection, or criminal allegations.
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 10 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Discontinuing the interview if the storyteller is distressed and indicates that they wish to terminate the interview.
Discontinuing the interview where it is evident that the individual wishes to initiate a formal complaint.
Being familiar with the complaints procedure (appendix 9) Feedback to the story teller about actions taken in response to their story.
Should an issue or concern be raised relating to another discipline or department it is the responsibility of the interviewer to provide feedback to that discipline or department. The immediate line manager will be required to act on information received as appropriate, maintaining the confidentiality and anonymity of the patient/carer. 10. Future Developments Each CPG will need to agree: The number of interviews to be undertaken during an agreed period of time. How information is to be fed back to their staff and members of other healthcare
teams. How staff are to be involved in sharing good practice and addressing weaker
practices. The best means of giving feedback to patients and carers as to how their
information has been influential in supporting changes. How information received via patient stories can be incorporated into service
improvements.
Bwrdd Iechyd Prifysgol Betsi Cadwaladr
University Health Board
Document number: ISUE01 Version: 1 Page 11 Paper copies of this document should be kept to a minimum and checks made with the electronic version to ensure the version to hand is the most recent.
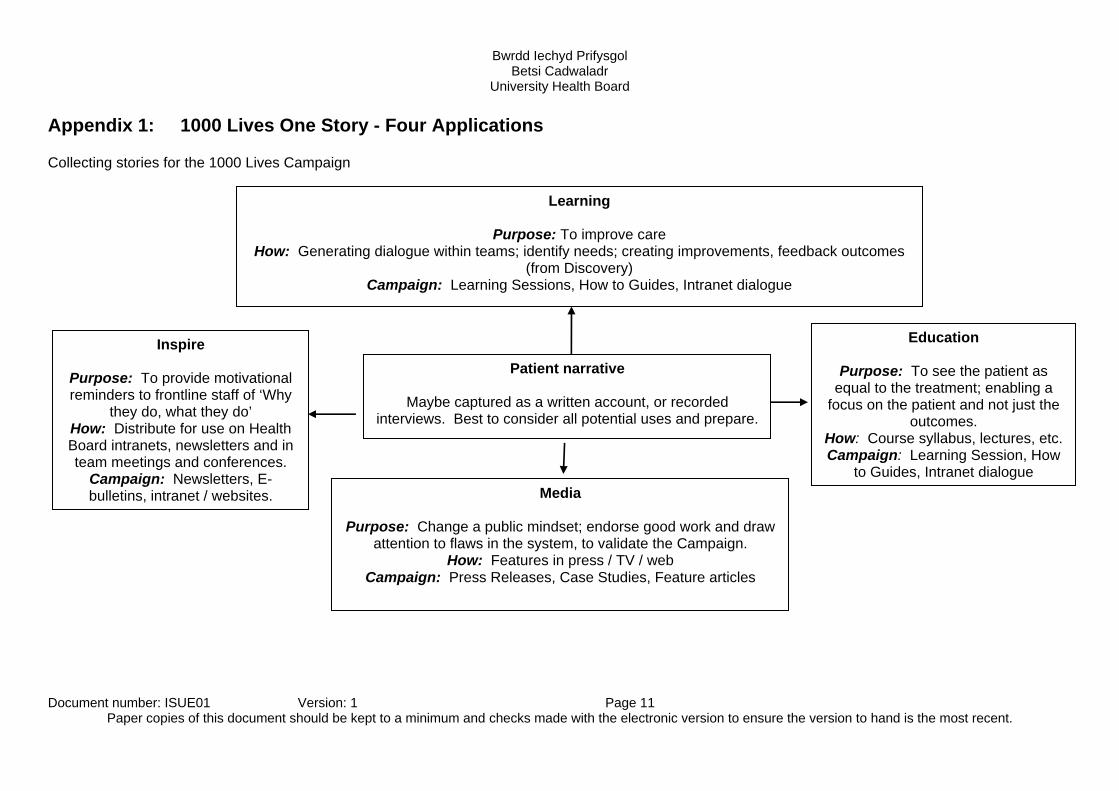
Appendix 1: 1000 Lives One Story - Four Applications Collecting stories for the 1000 Lives Campaign Learning
Purpose: To improve care
How: Generating dialogue within teams; identify needs; creating improvements, feedback outcomes (from Discovery)
Campaign: Learning Sessions, How to Guides, Intranet dialogue
Inspire
Purpose: To provide motivational reminders to frontline staff of ‘Why
they do, what they do’ How: Distribute for use on Health Board intranets, newsletters and in team meetings and conferences.
Campaign: Newsletters, E-bulletins, intranet / websites.
Patient narrative
Maybe captured as a written account, or recorded interviews. Best to consider all potential uses and prepare.
Education
Purpose: To see the patient as equal to the treatment; enabling a
focus on the patient and not just the outcomes.
How: Course syllabus, lectures, etc. Campaign: Learning Session, How
to Guides, Intranet dialogue
Media
Purpose: Change a public mindset; endorse good work and draw attention to flaws in the system, to validate the Campaign.
How: Features in press / TV / web Campaign: Press Releases, Case Studies, Feature articles
Document number: ISUE01 Version: 1 Page 12 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Appendix 2: Example Patient’s Stories Information Leaflet for Patients
Patient Stories - Information for Patients What are Patient Stories? A patient’s story is simply you telling us your experience in your own words. We would really like to hear your story about your experience and the health care that you received. We are interested in listening to what it was like for you being a patient, or what it was like for your relatives or carers. Why do you want to listen to Patient’s Stories? We know that if changes are made in the NHS we can improve healthcare. We have some ideas about how we can do this from our own experience. Often, the smallest changes can make the biggest difference. By listening to and recording your story as a patient can we really hear and take on board what you have to say and learn how you feel about your experience. This will help us to take a good look at the service we provide and see how we might improve it. What will be expected of me? We will agree with you a time and place to meet, for you to tell one person from Betsi Cadwaladr University Health Board (BCUHB) your story. They may be accompanied by another person who will take notes, or you may prefer to have the conversation recorded on audio, some people like to have their story recorded by video camera. Staff who listen to patient’s stories have had the necessary training to do so and have good people skills. We are interested in hearing about the things that went well and things that did not go so well, and what you feel needs to change. Occasionally, we may ask a group of patients, carers to share their stories in a group setting. We will then listen to your story, together with other colleagues from the team, to draw out themes and issues of concern. This will help us to think about our services and how to improve them.
Document number: ISUE01 Version: 1 Page 13 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
What if I would prefer someone to speak on my behalf? Ideally we would like to talk with you; however we know that sometimes this may be difficult. In these circumstances we would still like to hear your story through a relative or someone you would like to speak on your behalf. We would want you as the patient to be present so that you can give as much input as possible. Who is involved in the team taking stories? The team is made up of different people who all work for the Health Board, some of whom are nurses, therapists or managers. You will probably not know the person who will listen to your story but they will explain fully who they are. However, some patients prefer to tell their story to staff who they know and trust. Do I have to take part? You do not have to tell your story. If you do agree to tell your story, you can still change your mind at any time without needing to give a reason. If at any stage after you have told your story you no longer wish us to use it, we will delete it from our records. Will taking part affect my health care? No, definitely not. Any future treatment or care you may need will not be affected by telling your story. What will you do with the information? The information that is collected will be treated in confidence. Any feedback will be kept anonymous, unless of course you gave your story as part of a video recording. Your details will not appear in any report or video footage. Your anonymised story will be shared with others so that the benefits of your story can be used to improve services. With your permission your story may be shared with staff in health and other related industries both within and outside the UK. It may also be used for educational purposes. Consent We will ask you to sign a consent form to make sure that you are fully aware of what is involved and so we can be confident that you have been given enough information about telling your story. Further Information If you wish to ask any more questions about telling your story, or if you want to discuss anything further, please do not hesitate to contact [insert name of local contact].
Document number: ISUE01 Version: 1 Page 14 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Appendix 3: Guidance for Video or Digitally recorded Stories Recording stories using digital media with the intention of producing an audio-visual (AV) product 1.1 Selecting this method This method of recording stories should be chosen when the desired finished product is a video or audio recording of the service user talking about their experiences. These stories may be presented as a video of the patient (video story), or as a photographic slideshow overlaid with an audio recording of the patient (audio story). Many stories will be suitable to be taken in this way; however there are additional issues to be considered by both the story taker and story teller.
Technical issues -use of recording equipment and editing software The interviewing space Interviewing techniques suitable for audio-visual recording The arenas in which the finished product will be presented Confidentiality, anonymity and consent Translation and bilingual issues Timescales Formats, storage and archiving
1.2 Technical issues In order to record AV material, the interviewer will need to operate the AV equipment, or co-operate with another member of staff who is able to operate the AV equipment for them. Equipment to produce the recording may include a video camera with in-built microphone, an external microphone, an audio field recorder, and where necessary, an audio mixing desk if there are several audio inputs, in addition to the tripods and cables required. Equipment to capture and edit the material may include a PC or Mac and a software editing package suitable for the format of files created, and possibly specialist audio software to improve the quality of the sound recording or dubbing different audio tracks onto the video. As the set-up and use of AV equipment is a specialism in its own right, it is recommended that interviewers work with staff familiar with the equipment and able to undertake that aspect of the work on their behalf, unless they are satisfied that their understanding of AV equipment is sufficient to ensure a successful recording. 1.3 The interviewing space As the equipment will record the sound as it is heard within the interviewing space, a number of issues become significant. The identified space should be:
Quiet and unlikely to be disturbed. Away from sources of noise, such as photocopiers or busy roads outside the
window. Consideration should also be given to the weather, as rain on the roof or a howling wind will also affect the sound recording.
Document number: ISUE01 Version: 1 Page 15 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Cleared of sources of background noise, such as ticking clocks and loud computers. Sounds which are common background noise within offices become very loud when heard on a recording.
Acoustically suitable, in that the space does not echo. Spaces with soft furnishings have fewer echoes than spaces with hard surfaces and windows.
All of the above apply to audio recordings. If the story is to be video recorded, the space should also:
Have a plain wall or suitable backdrop for the video. Be well and softly lit, so that harsh shadows are not cast.
1.4 Interviewing techniques suitable for audio-visual recording As a good digital story will not give any indication of the interviewer, the importance of asking open questions is paramount. The interview will also need to ensure that the storyteller understands that they will need to phrase their story in whole sentences. This makes the editing work easier. In addition to these issues, whatever is said by the interviewer will be recorded, and so the interviewer must avoid habits such as giving verbal encouragement to the patient while they tell the story, as these will also be picked up on the recording. 1.5 The arenas in which the finished product can be presented These will depend upon the nature of the story and the purpose for which it was given. Ways in which video or audio stories can be used include:
Presentation to conferences, committees or meetings to raise awareness or put a human face on the discussion.
In support of reports or bids. As part of in-house staff training. In public information, for example, to explain what to expect when attending
hospital for surgery. To promote or publicise the organisation, for example, in the media, on radio
or online. Each of these arenas has its own benefits and drawbacks which will make it more suitable for some types of story than others. The story taker should consider how the story will be used before embarking on a video or audio story, to ensure that the best use is made of the story. The story teller needs to understand the ways in which their story may be used and to give specific consent, particularly if the story will be made available outside the organisation. 1.6 Confidentiality, anonymity and consent The patient can be assured that their wishes with regard to the story and where it is used will be respected, however, before they consent to having their story recorded, they must understand that a video recording will not be anonymous, as their face will be visible. Likewise, their voice will be heard in the audio recording, and so it is possible that people who know them and who hear the story may be able to identify them. Their name and any other personal identifiable details can be kept from the
Document number: ISUE01 Version: 1 Page 16 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
public domain, however. Patients who are unwilling to be publically associated with their story may still be prepared to be audio recorded, or may be reassured knowing that they can limit the ways in which the story can be used. Patients who are very concerned about the possibility of being identified, those with highly personal stories or very controversial messages, may be happiest having their stories written down rather than recorded using an AV method. This should be discussed with the patient before the recording is begun, and the interviewer must be satisfied that the patient understands. To cover these issues and the issues in 1.5 above, a separate digital stories consent form has been developed. 1.7 Translation and bilingual issues Patients will give their stories in their language of choice, and should be matched with an interviewer who is able to communicate with them in their language of choice. Stories which are recorded for the purpose of using in a specific environment (i.e. at an internal meeting which is to be run through a single language) will not need to be translated if they are already in a language appropriate to that environment. Stories which will be made available to a wider audience may require translation. The options for translation are:
Working with the patient to produce two or more different versions of the story in different languages. Patients who are fluently bilingual may be happy to record their experiences in different languages, which will ensure that the patient’s own words and emphasis are retained.
Dubbing another language over the video or photographic slideshow. This will require the original story to be transcribed verbatim, translated and then recorded in another language by a fluent speaker. This new audio track will then need to be edited with the video to create a new version of the patient story. It may be necessary to use an actor to record the new audio, to ensure that the match between original and new version is as close as possible.
Subtitling the original story. As above, the original story will need to be transcribed and translated and then edited into the video using the video editing software.
Transcribed and provided as a bilingual written version. These options should be discussed with the story teller at the time of taking the story. 1.8 Timescales Producing a video or audio story requires that the original recording is edited into a finished product, which can be a time consuming process. An hour-long interview may be cut down to two or three minutes of the most powerful material. The additional time taken to edit the recording, using an appropriate software package, and perhaps working with a colleague who has the required level of expertise to work with the software, needs to be considered so that sufficient time is allowed within the project.
Document number: ISUE01 Version: 1 Page 17 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
1.9 Formats, storage and archiving To make digital patient stories as accessible as possible across the organisation, each finished story should be saved both as an .AVI file at high resolution, and as a .mpg lower resolution file. .mpg video files can be played by Windows Media Player, which is installed on most computers within the organisation as the default software. Stories which have been produced purely on audio, with no accompanying video or graphic images, can be saved in mp3 format. Both the finished product and the original recording should be saved, either to a designated section of the server if space is available, or to DVD. Consideration should be given to the confidentiality and sensitivity of the information on both the original and finished story when arranging how to save and store the files, as well as any specific instructions the story teller has given as to the handling of their story. A copy of the finished product on DVD should also be sent to the Patient Stories Register for reference.
Document number: ISUE01 Version: 1 Page 18 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
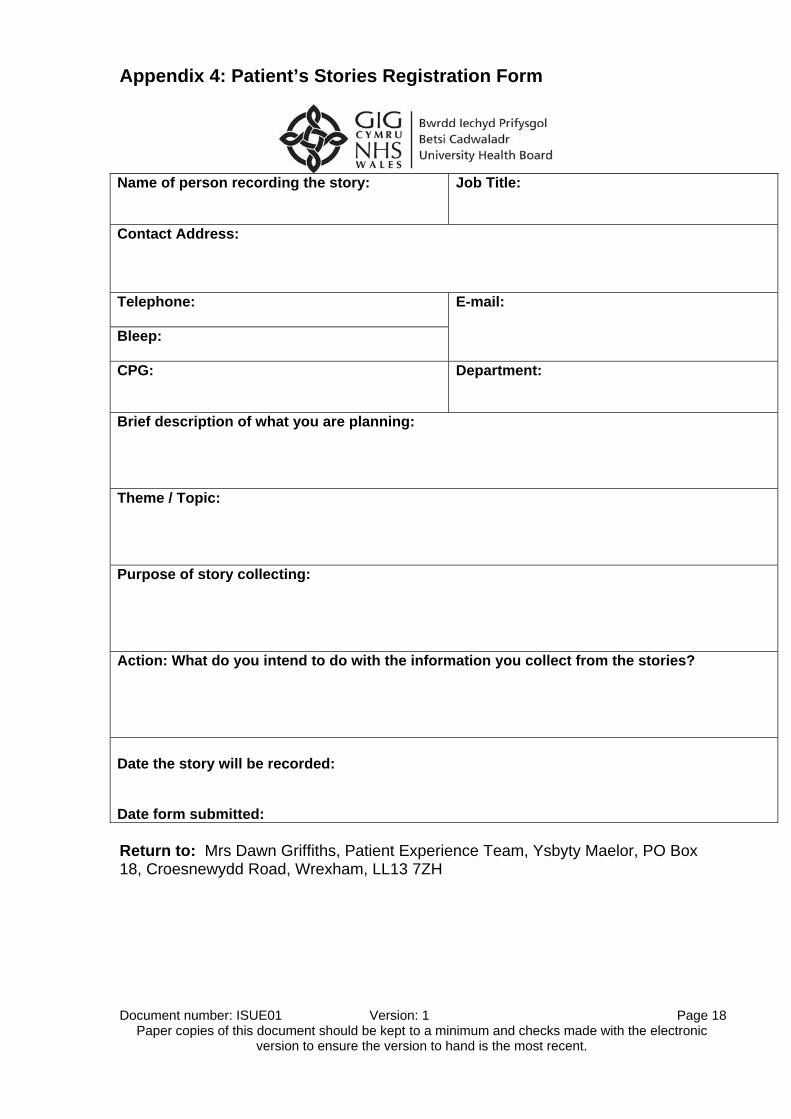
Appendix 4: Patient’s Stories Registration Form
Name of person recording the story:
Job Title:
Contact Address: Telephone:
E-mail:
Bleep: CPG:
Department:
Brief description of what you are planning:
Theme / Topic:
Purpose of story collecting: Action: What do you intend to do with the information you collect from the stories? Date the story will be recorded: Date form submitted: Return to: Mrs Dawn Griffiths, Patient Experience Team, Ysbyty Maelor, PO Box 18, Croesnewydd Road, Wrexham, LL13 7ZH
Document number: ISUE01 Version: 1 Page 19 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
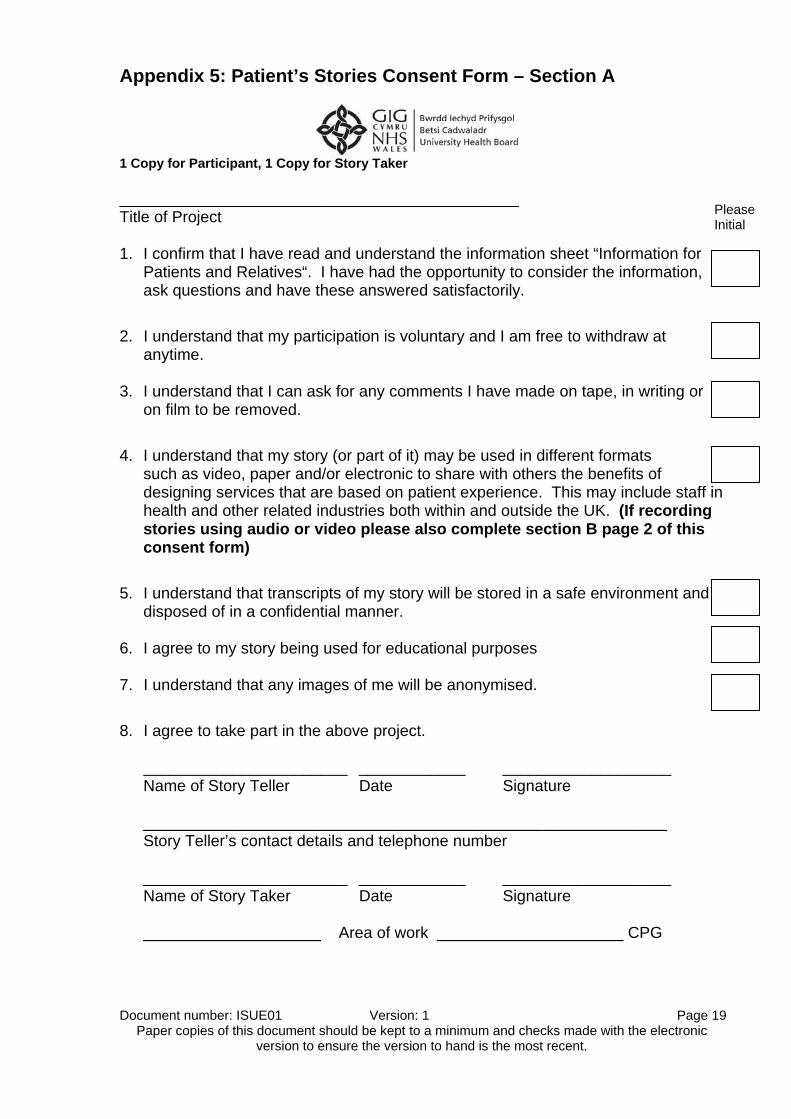
Appendix 5: Patient’s Stories Consent Form – Section A
1 Copy for Participant, 1 Copy for Story Taker _____________________________________________ Title of Project 1. I confirm that I have read and understand the information sheet “Information for
Patients and Relatives“. I have had the opportunity to consider the information, ask questions and have these answered satisfactorily.
2. I understand that my participation is voluntary and I am free to withdraw at anytime.
3. I understand that I can ask for any comments I have made on tape, in writing or
on film to be removed.
4. I understand that my story (or part of it) may be used in different formats such as video, paper and/or electronic to share with others the benefits of designing services that are based on patient experience. This may include staff in health and other related industries both within and outside the UK. (If recording stories using audio or video please also complete section B page 2 of this consent form)
5. I understand that transcripts of my story will be stored in a safe environment and disposed of in a confidential manner.
6. I agree to my story being used for educational purposes 7. I understand that any images of me will be anonymised.
8. I agree to take part in the above project.
_______________________ ____________ ___________________ Name of Story Teller Date Signature ___________________________________________________________ Story Teller’s contact details and telephone number _______________________ ____________ ___________________ Name of Story Taker Date Signature ____________________ Area of work _____________________ CPG
Please Initial
Document number: ISUE01 Version: 1 Page 20 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
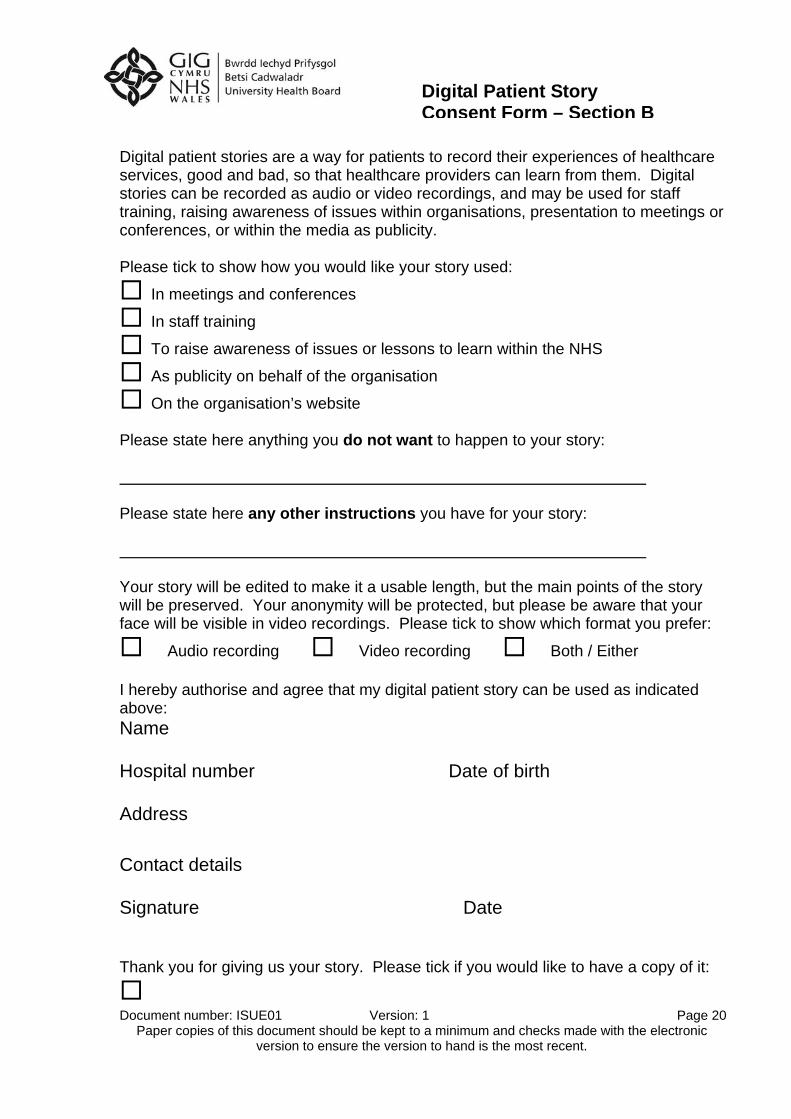
Digital patient stories are a way for patients to record their experiences of healthcare services, good and bad, so that healthcare providers can learn from them. Digital stories can be recorded as audio or video recordings, and may be used for staff training, raising awareness of issues within organisations, presentation to meetings or conferences, or within the media as publicity. Please tick to show how you would like your story used:
In meetings and conferences
In staff training
To raise awareness of issues or lessons to learn within the NHS
As publicity on behalf of the organisation
On the organisation’s website Please state here anything you do not want to happen to your story: Please state here any other instructions you have for your story: Your story will be edited to make it a usable length, but the main points of the story will be preserved. Your anonymity will be protected, but please be aware that your face will be visible in video recordings. Please tick to show which format you prefer:
Audio recording Video recording Both / Either I hereby authorise and agree that my digital patient story can be used as indicated above: Name
Hospital number
Date of birth
Address
Contact details
Signature
Date
Thank you for giving us your story. Please tick if you would like to have a copy of it:
Digital Patient Story Consent Form – Section B
Document number: ISUE01 Version: 1 Page 21 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Appendix 6: Equality Monitoring Information
PEM Equality Categories
Date of Birth
/ /
Gender Male Female
Are you undergoing, have undergone orplaning to undergo gender reassignment?
Yes No Prefer not to say
National Identity Please tick all that apply
Welsh
English
Scottish
Northern Irish
British/Mixed British
Irish
European
Prefer not to say
Other (state if desired)
Racial Group
White
Black Caribbean
Black African
Black Other
Asian/Asian British
Indian
Bangladeshi
Pakistani
Asian Other
Mixed White and Black Caribbean
Mixed White and Black African
Mixed White and Asian
Mixed Other
Mixed/Mixed British
Other/Other British
Chinese
Arabian
Gypsy/Traveller
Prefer not to say
Other (state if desired)
White/White British
Black/Black British
Disability
Do you have a physical or mental health condition or otherimpairment that has lasted, or is likely to last, at least 12months;or is of a progressive nature?
Yes No Prefer not to say
Please state the type of impairment which applies toyou. You may indicate more than one
Mobility impairment
Dexterity impairment
Blind or Visually impaired
Deaf or Hearing impaired
Mental Health condition
Learning/Cognitive impairment/difficulty
Long-standing illness or health condition
Other impairment (please specify)
Religion
Christian
Buddhist
Hindu
Jain
Jew
Muslim
Sikh
None
Prefer not to say
Other (state if desired)
Preferred Language
English
Welsh
British Sign Language (BSL)
Other (state if desired)
Sexual Orientation
Heterosexual/Straight
Gay Man
Gay Woman/Lesbian
Bisexual
Prefer not to say
Other (state if desired)
This form is 'machine read' therefore, please print in capital letters and avoid contact with the edge of the box.Or, place a cross in the appropriate box - see examples >>NB: Anything written outside the boxes cannot be readPlease do not fold or staple this questionnaireUnless indicated, place a X in only one box for eachquestion
Document number: ISUE01 Version: 1 Page 22 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Appendix 7: Patient Stories Transcript Form
Betsi Cadwaladr University Health Board Patient’s Stories Transcript Form
Who took the patient’s story:
Name:
Contact details:
Reason for taking the story and areas covered:
Brief summary of the story:
Document number: ISUE01 Version: 1 Page 23 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Key themes emerging:
Lessons learnt:
Proposed action:
Sensitive issues to be aware of:
Document number: ISUE01 Version: 1 Page 24 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Appendix 8: Conducting Patient Stories Flow Chart
Identify patient group / service area
Agree method of recruiting and recruit story tellers Para: 4.1 / Appendix: 2
Register patient story on central database Para: 5.1 / Appendix: 3
Arrange interview date and prepare story teller Para: 5.1 & 5.2, Table 1, Section A
At interview gain consent Para 5.2, Table 1, Section B / Appendix 5 and request
Equality Monitoring information section C appendix 6 (send copies of Equality Form to the Central Database Co-
ordinator
Conduct interview Para 5.2, Table 1, Section C
Transcribe interview, using template Appendix 7 keep in secure area. Agree content with story teller
Para 6.2, Table 2, Section A Once completed send copy to Database Co-ordinator
Discuss transcript with manager / team and decide actions to be taken forward. Para: 6.2, Table 2, Section B
Prepare action plan Para 6.2, Table 2, Section C
Feedback to story teller
Document number: ISUE01 Version: 1 Page 25 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Appendix 8: Summary of the Caldicott Principles
Principle 1 - Justify the purpose(s) Every proposed use or transfer of patient-identifiable information within or from an organisation should be clearly defined and scrutinised, with continuing uses regularly reviewed by an appropriate Guardian.
Principle 2 - Don't use patient-identifiable information unless it is absolutely necessary Patient-identifiable information items should not be used unless there is no alternative.
Principle 3 - Use the minimum necessary patient identifiable information Where use of patient-identifiable information is considered to be essential, each individual item of information should be justified with the aim of reducing identifiability.
Principle 4 - Access to patient-identifiable information should be on a strict need to know basis Only those individuals who need access to patient-identifiable information should have access to it, and they should only have access to the information items that they need to see.
Principle 5 - Everyone should be aware of their responsibilities Action should be taken to ensure that those handling patient-identifiable information - both clinical and non-clinical staff - are aware of their responsibilities and obligations to respect patient confidentiality.
Principle 6 - Understand and comply with the law Every use of patient-identifiable information must be lawful. Someone in each organisation should be responsible for ensuring that the organisation complies with legal requirements.
Document number: ISUE01 Version: 1 Page 26 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Appendix 9: Summary Reporting Incidents, Concerns and Complaints that may arise during the Patient Interview Should the patient reveal something during the interview that may necessitate further discussion, investigation or action, the Health Board's Complaints and Incident Reporting policies should be followed. Any incident that may give rise to an adverse or clinical incident as defined in the Risk Management Policy 'Any occurrence which is not consistent with the routine treatment or care of the patient, or the routine operation of the Health Board’. An untoward Incident is defined as ‘Any event that has given or may give rise to actual or possible personal injury, to patient dissatisfaction, or to property or damage’. A near miss is ‘An occurrence which, but for luck or skilful management, would in all probability have become an adverse incident’.
During the patient interview the interviewer will not react at the time. Once the interview is completed the interviewer can raise the issue again. If it is thought that immediate action is required the patient / carer will be asked
whether they have spoken to the person responsible for that department / ward. They should be asked whether they are aware of the complaints procedure. If the patient gives permission to act on their behalf, the matter can be taken
forward as per the Complaints Policy and Incident Reporting system. The information obtained at the interview is confidential and it may not be
appropriate to take matters forward without specific permission Wherever possible the member of staff receiving the complaint should resolve
those within her own competencies as soon as possible, by liaising with the department Sister / Charge Nurse.
Any complaints outside the remit of the Sister / Charge Nurse will be referred to the Department / Service Manager.
Reporting Procedure Complaints / Issues Raised The interviewer should inform the Sister / Charge Nurse immediately of the nature
and potential consequence of the complaint. Local action should be undertaken as appropriate. Informal complaints whether resolved or not at local level, will be recorded by the
interviewer or the Sister / Charge Nurse and forwarded to the relevant Complaints Department (as per Complaints Policy).
Should the patient/carer not be satisfied with the proposed resolution, the complaint should be passed to the relevant BCUHB Complaints Department to be dealt with formally.
If an incident is raised and the patient/carer wishes it to be dealt with formally they will be advised to contact the relevant BCUHB Complaints Department who will then contact the person directly.
Serious complaints/incidents that may give rise to wider issues affecting the Health Board should be reported immediately to a Directorate Manager, Health Board Director or Risk Manager.
Document number: ISUE01 Version: 1 Page 27 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Where reported incidents are likely to have a significant impact upon the Health Board, or indicate systematic failures in procedure, an incident summary report will be prepared.
An incident reporting form (IR1) should be completed. Details of the person informed should be recorded on the form. All remedial action should be recorded on the incident report form. Feedback will be given to the person who reported the incident, as appropriate. Should there be clinical elements of any complaint a copy of the complaint must
be sent to the individual Consultant and Directorate Manager / Head of Nursing as appropriate.
Children have the right to complain on their own behalf. The information leaflet 'How to make complaints, comments or compliments’, will
be available and accessible to all staff in the ward / department. Contact Numbers BCUHB Complaints Departments:
o Complaints Department
Glan Clwyd Hospital 01745 534140
o Complaints Department Wrexham Maelor Hospital 01978-725543
o Complaints Department
Ysbyty Bangor 01248 384194
Contacting Numbers Community Health Council for Complaints Advocates
Conwy Locality Office: Telephone: 01492 878840 Denbighshire Locality Office: Telephone: 01492 878840
Flintshire Locality Office: Telephone 01978 356178
Gwynedd Locality Office: Telephone: 01286 674961
Dolgellau Office: Telephone: 01341 422236
Wrexham Locality Office: Telephone: 01978 356178
Ynys Môn Locality Office: Telephone: 01248 723283

Document number: ISUE01 Version: 1 Page 28 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Appendix 10 – Contact Details for further advice Diane Henderson, PPI Manager Email: [email protected] Telephone: 01978-727125 / 1814-7125 Julie Jones, Research & Clinical Audit Manager Email: [email protected] Telephone: 01978-727502 / 1814-7502 Rhiannon Graham-Garnett (for stories being recorded through audio and visual means) Email: [email protected] Telephone: 01286-674272 Christine Cowley, Lead Nurse Professional and Practice Development Email: [email protected] Telephone: 01978 727020 / 1814-7020 Jenny Welstand, Nurse Specialist, Cardiology Email: [email protected] Telephone: 01978 727299 / 1814-7299
Document number: ISUE01 Version: 1 Page 29 Paper copies of this document should be kept to a minimum and checks made with the electronic
version to ensure the version to hand is the most recent.
Members of the Working Group: Name Title Heather Piggott Assistant Director of Nursing Kathy Collins Hospital Manager (E&C) Sylvia Hughes PPI Manager (W) Rhiannon Graham Garnett Patient Support (W) Julie Jones Clinical Audit Manager Yvonne Lush Head of Nursing, Cancer CPG Beryl McLoughlin Practice Development Lead Nurse Julie Smith Assoc Chief of Staff, Nursing & Medicines Management Wynne Roberts Pastoral Care & Partnership Manager (W) Jenny Welstand Nurse Specialist, Cardiology Ken Williams Quality Coordinator (E&C)
Engagement has taken place with: Name Title Date Consulted Improving Service User Experience sub-group
September 2010
Patient Stories Working Group
May 2010
Inpatient Satisfaction Working Group
June 2010
Complaints Leads June 2010 ACOS’s June 2010 PPI Leads June 2010 CPGs June 2010





























