Embed Size (px)
Citation preview

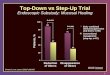
IST-3 – an imaging substudy
Dr Ingrid Kane
Clinical research fellow

Background
• Currently IST-3 specifies CT scan prior to randomisation into trial
• Growing interest in MRI, with some centres in Europe, preferring this method of imaging
• Can MRI help us select patients who will benefit from thrombolysis?

MRI• Diffusion weighted imaging – DWI –
sensitive to early ischaemic change• Perfusion imaging – PWI –
demonstrates blood flow in and around infarct
• The difference between these 2 may represent the salvageable brain
• Can be time consuming, not all patients tolerate.

Current trials
• DIAS/DEDAS – using mismatch to select patients for desmotoplase therapy
• EPITHET – recording MR PWI/DWI in patients randomised to rt-PA or placebo up to 6hrs (selected on CT criteria)
• None looking at role of microhaemorrhages or white matter lesions and risks with rt-PA

Practical,streamlined and optimal use of
imaging in acute stroke
Supported by small project grant from the Chief Scientist Office, UK

Ultimate aims• Can routine MR be made more rapid, practical and
safe in acute stroke• Does the ischaemic lesion appearance on DWI
predict the amount of non-salvageable tissue?• Is the benefit of rt-PA confined to those with a
PWI>DWI lesion?• Are patients with white matter hyperintensities or
microhaemorrhages at greater risk of haemorrhage after rt-PA
• How do CT ‘early infarct signs’ relate to MR ‘early infarct signs’?

Pilot study
• In the context of IST-3 is it feasible to run an MR imaging substudy to improve the safety of thrombolysis?
• Study will run 9am-5pm Mon – Fri.
• Patients suitable for IST-3 who have no contraindications to MR will be recruited

Patient with signs and symptoms of acute stroke presenting < 5 hours after symptom onset
Assessed by acute stroke team and suitability for IST-3 ascertained.
Admit for standard stroke care
Arrange urgent CT scan to exclude any evidence of bleed
Evidence of intracerebral bleed – not entered for trial. Usual stroke care
No evidence of bleed, but contraindications to MR – randomise to IST-3
No evidence of bleed and no contraindications to MR. Randomise to IST-3, whilst transferring to MR scanner.Draw up bolus of treatment and prepare infusion. After MR complete transfer to stroke ward for treatment
Follow-up scan at 24-48 hours. Mode of scan depends on arm of trial entered into
Not eligibleEligible
NO INTRACEREBRAL BLEED
Note: if, at anytime, the MR scanner is unavailable for any reason the patient will undergo CT scanning and, if there is no evidence of intracerebral haemorrhage, they will be randomised to IST-3 as per the usual protocol. If any patients are eligible to receive thrombolysis under the strict current licence they can still be entered into the MR arm of the study prior to receiving treatment.
BLEED

Survey of UK stroke centres
• Is MR available on-site?
• Is MR available to acute stroke patients?
• If so, are services available 24hrs/day
• Estimate of number of acute stroke patients who could potentially undergo DWI and PWI imaging