Embed Size (px)
Citation preview

ISOPOL XVII, Porto, 5-8 May 2010
Andrew Wadge
Chief Scientist
Food Standards Agency, UK
How can the social sciences help us understand the prevalence of listeriosis
in the UK?

Outline of talk
•Foodborne disease – the burden and priorities
•Our strategic plan 2010-15 – safe food
•FSA messaging
•Trends in listeriosis in England and Wales
•Advisory Committee on the Microbiological Safety of Food (ACMSF)
•Consumption patterns in over 60s
•Contribution of the social sciences

Estimated number of cases and deaths associated with indigenous foodborne disease: England and
Wales 2007
Cases (%) Deaths (%)Campylobacter 333,652 (36.0) 80 (18.1) Cl. perfringens 18,540 ( 2.0) 20 (4.5)Salmonella 32,155 (4.3) 92 (20.8)E. coli O157 920 (<0.1) 21 (4.7)L.monocytogenes 455 (<0.1) 162 (36.6)
Norovirus 175,250 (18.9) 29 (6.5)All agents 925,767 443
Source: HPA data
FSA Strategic plan 2005-2010 – “Reduce foodborne disease further”

Estimated annual foodborne disease cases England & Wales 2000-2007
Sources: HPA and FSA data
No. cases
Total cost of illness includes the direct costs to NHS and individuals in loss of earnings as well as indirect costs

FSA’s strategy 2010-2015- Outcomes
Food produced or sold in the UK is safe to eat • Reduce foodborne disease using a targeted approach - tackling Campylobacter in chicken as a priority - Listeria in ready to eat chilled foods• Intelligence on, global food chains to identify and reduce the impact of potential new and re-emerging risks- particularly chemical contamination
Consumers understand about safe food and healthy eating, and have the information they need to make informed choices • Improve public awareness and use of messages about healthy eating and good food hygiene practice at home
Full strategy at www.food.gov.uk/strategy
0
50
100
150
200
250
'83 '84 '85 '86 '87 '88 '89 '90 '91 '92 '93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03 '04 '05 '06 '07 '08
Cas
es
Year
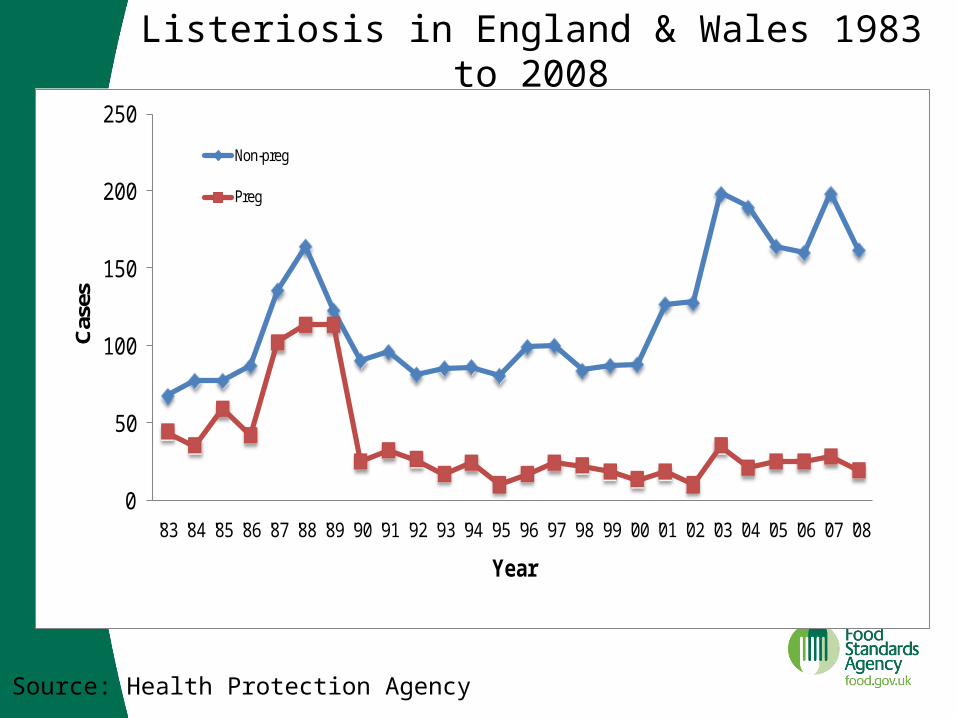
Non-preg
Preg
Listeriosis in England & Wales 1983 to 2008
Source: Health Protection Agency

0
20
40
60
80
100
120
140
'90 '91 '92 '93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03 '04 '05 '06 '07 '08
Cases
Year
Pregnant
<60 CNS
<60 Bact
60+ CNS
60+ Bact
Listeriosis in England & Wales 1990 to 2008.
Source: Health Protection Agency
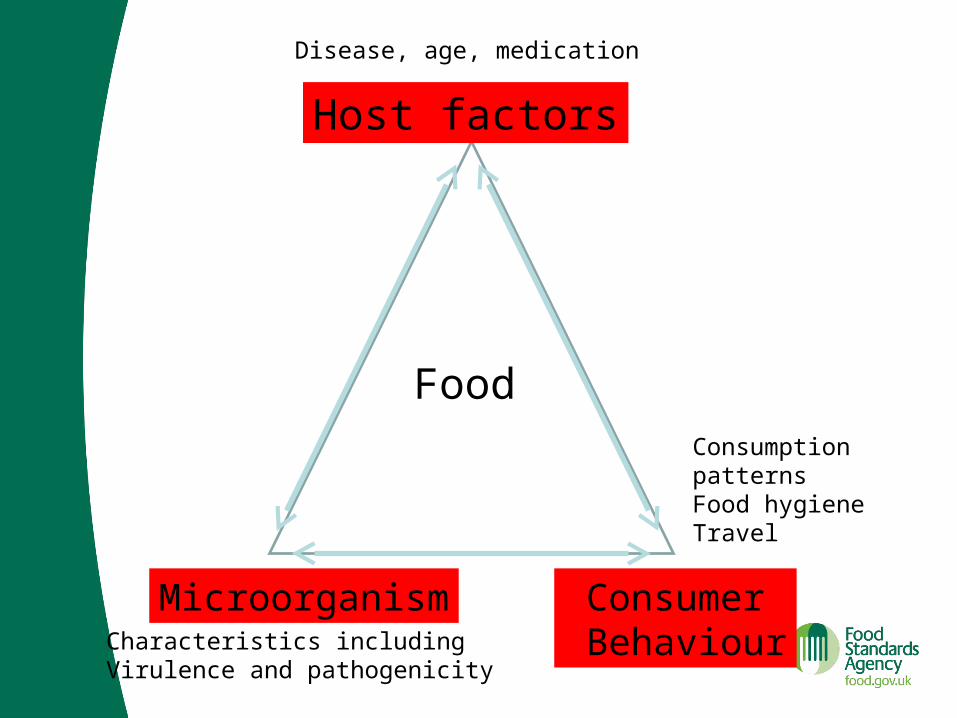
Host factors
Microorganism Consumer Behaviour
FoodConsumptionpatternsFood hygieneTravel
Disease, age, medication
Characteristics includingVirulence and pathogenicity
0
2
4
6
8
10
12
Year
Ca
se
s p
er
mill
ion
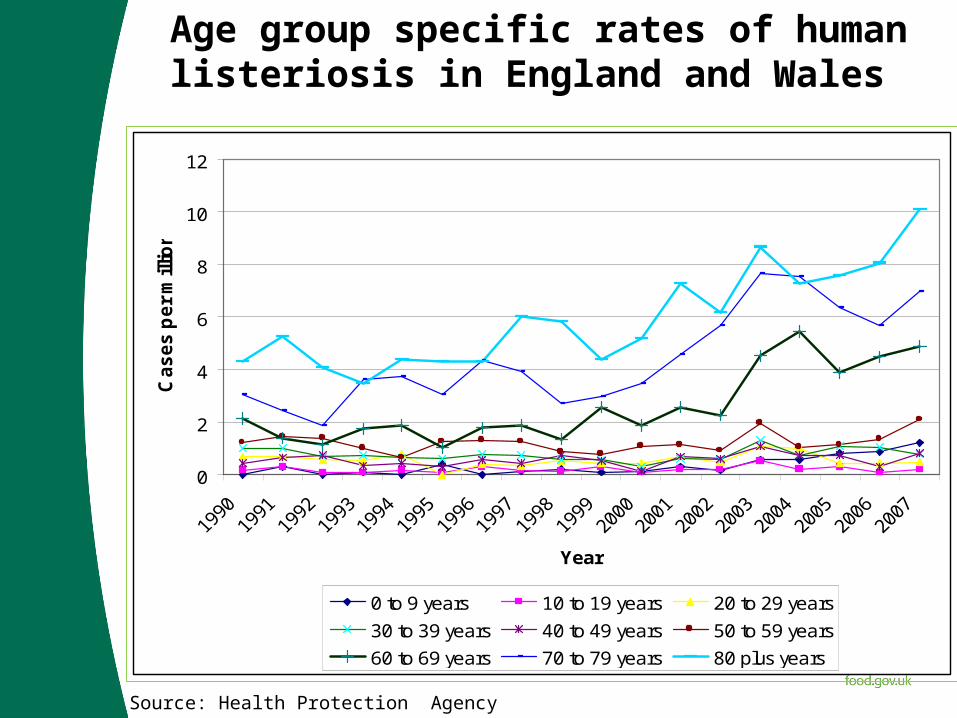
0 to 9 years 10 to 19 years 20 to 29 years
30 to 39 years 40 to 49 years 50 to 59 years
60 to 69 years 70 to 79 years 80 plus years
Age group specific rates of human listeriosis in England and Wales
Source: Health Protection Agency
Conclusions of the ACMSF ad hoc group on vulnerable groups
• Increase in UK and some European counties mostly in patients aged over 60 years with bacteraemia – no evidence of a common source relationship
• The increase and shift in presentation of listeriosis cannot be attributed to improved diagnostics
• Elderly individuals are more likely to have underlying conditions which predispose to listeriosis than younger age groups.
• Evidence suggests that the incidence and levels of L.monocytogenes at the points of production and sale are not higher than those detected in the late 1980s
• Maintaining active surveillance for Listeria spp. in foods is important to inform control of this organism
• More information is needed on food consumption and food handling and storage behaviours in the home of the over 60s, including those who are vulnerable

11
19
60
40
66
15 15
69
43
62
0
10
20
30
40
50
60
70
80
Homemade Frozen Fresh Chilled Ambient
Total Consumers
Adults 65+
Adults 65+ are more likely to eat homemade foods, fresh foods and chilled foods. They are less likely to consume frozen and ambient
foods. % of individual meal occasions
Total In Home, 52 w/e end Aug 2007
Source: ACMSF report on the increased incidence of listeriosis in the elderly 2009
acmsf.food.gov.uk/acmsfreps/

Contribution of the social sciences to the problem
• Are behaviours contributing to the risk of listeriosis in the over 60’s?
• In particular: consumption patterns, food storage and food preparation practices
• What underpins these behaviours? – Socio-demographics, lifestyle, accommodation, health
status, beliefs and attitudes. • Can’t explain the increase – lack of historical data• But, can explore what is happening now and create a
baseline for future comparisons

Defining the group at risk
• Diverse age group• Wide variety of socio-demographic characteristics: age,
income, household composition, marital and employment status, health, ethnicity etc.
• Different generations and cohorts• Significant life changes• All have effects on health status and wellbeing, in turn
contribute to daily living and food habits• Lack of differentiation characteristic of the current
literature

What have we done so far?
• Advice paper produced by the Social Science Research Committee:
“Liseria monocytogenes and the food storage and food handling practices of the over 60s at home”
• Conducted preliminary literature search and interviews with experts
• Found existing literature to be somewhat fragmented with topics explored in isolation
• Recommended thorough review of literature• Developed recommendations for primary research

Challenges
• How to measure behaviours that are often latent
• Actual behaviours versus stated behaviours
• Who to research– Who is at risk? Need to consider the diversity of
older households within the UK– Particular methodological considerations for this
age group
• Lack of existing data in general

What will we do next?
• “Food and You” survey, including a module of questions on food safety and hygiene
• Evidence review• Considering observational research and household
study with those who have had listeriosis• Refrigerator survey• Robust cross disciplinary approach• Exploring the international response

Contact us with suggestions
• Dr Andrew Wadge:
• Social Science Research Committee:

AcknowledgementsAdvisory CommitteesACMSFSSRCFood Standards AgencyRobyn AckermanJane BarrettJoyce BrownPaul CookBob MartinHealth Protection AgencyIan Gillespie





























