Embed Size (px)
Citation preview

Is peak expiratory flow rate a predictor of complications in diabetes?
The Wisconsin Epidemiologic Study of Diabetic Retinopathy
Barbara E.K. Kleina,*, Scot E. Mossa, Ronald Kleina, Karen J. Cruickshanksa,b
aDepartment of Ophthalmology and Visual Sciences, University of Wisconsin-Madison, 610 North Walnut Street, 460 WARF, Madison, WI 53705-2397, USAbDepartment of Preventive Medicine, University of Wisconsin Medical School, Madison, WI 53705-2397, USA
Received 28 February 2001; received in revised form 11 June 2001; accepted 18 June 2001
Abstract
The objective of this study was to determine whether peak expiratory flow rate is a predictor of complications of diabetes. Peak expiratory
flow rate was measured at the 10-year follow-up (third examination) of a cohort of persons with younger-onset diabetes. The relationships of
progression of diabetic retinopathy by two steps, progression to proliferative retinopathy and of incidences of macular edema, sore or ulcers
on feet or ankles, lower extremity amputation, proteinuria, and cardiovascular disease 4 years after this examination with respect to peak
expiratory flow rate were evaluated. Study procedures including measurements of blood pressure, height and weight, grading of fundus
photographs, peak expiratory flow rate, urinalysis, and medical history were performed according to standard protocols. Peak expiratory flow
rate was not associated in univariate analyses with progression of retinopathy, incidences of proliferative retinopathy, macular edema or lower
extremity amputation, sores or ulcers on feet or ankles, gross proteinuria, or self-reported cardiovascular disease. However, when using
multivariable models to include the effects of other risk factors, peak expiratory flow rate was significantly associated with the combined
incidences of sores or ulcers on feet and ankles, or lower extremity amputations (OR= 0.61, 95% CI 0.42–0.88). These data suggest that
peak expiratory flow rate is a predictor of subsequent complications in the lower extremities in those with long duration of younger-onset
diabetes. Evaluating this association in an incipient cohort would illuminate whether the relationship we found is likely to be causal. D 2001
Elsevier Science Inc. All rights reserved.
Keywords: Complication of diabetes; Peak expiratory flow rate
1. Introduction
Pulmonary and respiratory functions have been found to
be compromised in persons with Type 1 diabetes. Bell et al.
(1988) found decreased lung volume in persons with Type 1
diabetes. Schuyler, Niewoehner, Inkley, and Kohn (1976)
found increased lung elastic recoil in male subjects with
juvenile onset diabetes. Thickening of basal laminae of the
alveoli (Vracko, Thoring, & Huang, 1979) and diabetic
microangiopathy in the capillaries of the alveolar septa have
been reported (Walton, Byrd, Fields, Ossorio, & Roy, 1994).
These may affect diffusion of carbon monoxide (Sandler,
Bunn, & Stewart, 1986; Walton et al., 1994). Moreover,
transcutaneous oxygen pressure has been found to be
diminished in patients with Type 1 diabetes (Breuer, Breuer,
& Berger, 1988; Walton et al., 1994). While a large and
varied battery of pulmonary and respiratory function tests
(Breuer et al., 1988; Primhak, Whincup, Tsanakas, &
Milner, 1987; Ramirez et al., 1991) have been commonly
used in clinic based studies of people with diabetes, peak
expiratory flow rate is easily measured and can be incorpo-
rated in field studies (Dahlquist, Eisen, Wegman, & Kriebel,
1993). Moreover, peak expiratory flow rate has been shown
to be associated with mortality (Cook et al., 1991).
The development and progression of complications of
diabetes have been thought to be due to relative hypoxia in
the affected organs and tissues (Cameron & Cotter, 1999;
Dyck & Giannini, 1996; Linsenmeier et al., 1998; Nakhos-
tine, Nadeau, & Lamontagne, 1997; Veves et al., 1996).
Population-based studies rarely collect information about
hypoxia on the tissue or cellular level. However, it is
possible that pulmonary and respiratory dysfunction influ-
ence oxygenation of tissues. Thus, it may be informative to
investigate the association of pulmonary function to vas-
1056-8727/01/$ – see front matter D 2001 Elsevier Science Inc. All rights reserved.
PII: S1056 -8727 (01 )00170 -2
* Corresponding author. Tel.: +1-608-263-0276; fax: +1-608-263-
0279.
Journal of Diabetes and Its Complications 15 (2001) 301–306

cular complications of diabetes. We present the experience
derived from the Wisconsin Epidemiologic Study of Dia-
betic Retinopathy (WESDR) of the association of peak
expiratory flow rate and the development of these endpoints.
2. Subjects and methods
2.1. Population
The population has been described in detail in previous
reports (Klein, Klein, Moss, et al., 1984; Klein, Klein, Moss,
& Cruickshanks, 1994; Klein, Klein, Moss, Davis, &
DeMets, 1984a, 1984b; Klein, Klein, Moss, Davis, &
DeMets, 1989a, 1989b). In brief, a sample of 2990 persons
was selected for the baseline examination from a total of
10,135 diabetic patients identified as receiving primary care
in an 11-county area in southern Wisconsin from July 1,
1979 through June 30, 1980. This sample was composed of
two groups. The first group consisted of all patients with a
diagnosis of diabetes before 30 years of age who took
insulin (1210 patients), the ‘‘younger-onset’’ group. The
second group consisted of a probability sample of the 5431
patients with a diagnosis of diabetes at 30 years of age or
older. Data from this ‘‘older-onset’’ group is omitted
because of the high mortality in this group in the later years
of follow-up.
Of the 1210 eligible younger-onset persons, 996 partici-
pated in the baseline examination in 1980–1986 (Examina-
tion 1) and 795 participated in the 10-year follow-up
(Examination 3). Of these, 651 were seen four years later
(Examination 4). Peak expiratory flow fate was first meas-
ured at the 10-year follow-up (examination 3). This serves
as the ‘‘baseline’’ for this paper and follow-up (incidence)
refers to Examination 4, an interval of 4 years.
2.2. Procedures
The examinations were performed in a mobile van in or
near the city where the participants resided. Pertinent parts
of the ocular and physical examinations included measuring
blood pressures (Hypertension Detection and Follow-up
Program Cooperative Group, 1976), dilating the pupils
and taking stereoscopic color fundus photographs of seven
standard fields (Diabetic Retinopathy Study Research
Group, 1981), determining random blood glucose and
glycosylated hemoglobin levels from a finger-prick capil-
lary blood sample (at baseline) and from venous blood (at
the follow-up examinations) (Quick-Step Fast Hemoglobin
Test System, Isolab, Akron, OH) (Moss, Klein, Klein,
Spennetta, & Shrago, 1988; Quick-Step Fast Hemoglobin
Test System, 1981), and obtaining a urine specimen for a
semiquantitative measurement of urine protein. Measure-
ment of peak expiratory flow was added at the 10-year
follow-up (Examination 3) (Wright, 1978) using the mini-
Wright peak flow meter (Clement Clarke, Columbus, OH
43219). The test was administered by the study examiners
who had been trained in the protocol, which is described by
the manufacturer (mini-Wright Peak Flow Meter, Clement
Clarke). Subjects were standing for all measurements. Three
measurements were made and the highest value was used in
these analyses. The meters were calibrated at eight flow
rates using a shop vacuum to generate flow (Cook, Evans,
Scherr, et al., 1989).
A standard structured interview was conducted, includ-
ing questions about age, age at diagnosis of diabetes,
cigarette smoking, cardiovascular disease, sores and ulcers
of the feet and ankles, and lower extremity amputations at
each study examination. At the 10-year examination, the
Respiratory Symptom Questionnaire recommended by the
American Thoracic Society was added (Ferris, 1978).
2.3. Grading protocol
To determine the incidence and progression of retinop-
athy in each eye, the fundus photographs were graded in a
masked fashion using the Early Treatment Diabetic Retin-
opathy Study (ETDRS) adaptation of the modified Airlie
House classification scheme (Early Treatment Diabetic
Retinopathy Study Research Group, 1991; Klein, Davis,
Segal, et al., 1984).
3. Definitions
At Level 10, no retinopathy was present; Levels 21, 31,
37, 43, 47, and 53 included nonproliferative diabetic retin-
opathy of increasing severity, and Levels 60, 61, 65, 71, 75,
and 85 included proliferative retinopathy of increasing
severity. In the analyses, eyes with proliferative retinopathy
at Levels 60–85 were grouped together as Level 60 + . This
included eyes that were treated with panretinal photocoagu-
lation during the follow-up interval. Eyes that could not be
graded for retinopathy levels because of opacities in the
media or enucleation not related to diabetic retinopathy were
classified as ‘‘cannot grade.’’
In determining retinopathy levels for a participant, the eye
with the higher level was given greater weight. Participants
in a given level were divided into two groups: those with this
level in each eye and those with a lesser level in one eye. For
example, the level for a participant with Level 37 retinopathy
in each eye is specified by the notation ‘‘Level 37/37.’’ This
scheme provided a 15-step scale (10/10, 21/ < 21, 21/21, 31/
< 31, 31/31, 37/ < 37, 37/37, 43/ < 43, 43/43, 43/ < 47, 47/47,
53/ < 53, 53/53, 60+/ < 60+, and 60+/60+) when all levels of
proliferative retinopathy were grouped as one level. For
purposes of classification, if retinopathy severity could not
be graded in an eye, this eye was considered to have the same
score as the participant’s other eye.
The incidence of any retinopathy was estimated from all
persons who had no retinopathy at the 1990–1992 exam-
ination (Level 10/10) and who participated 4 years later.
B.E.K. Klein et al. / Journal of Diabetes and Its Complications 15 (2001) 301–306302
Any retinopathy was defined as a retinopathy severity Level
21/ < 21 or worse at follow-up. Progression to proliferative
retinopathy was estimated for all persons who were clas-
sified as having no or nonproliferative retinopathy severity
(Level 53/53 or better at the 1990–1992 examination) and
who participated 4 years later. Proliferative retinopathy was
defined as a retinopathy severity Level 60+/ < 60+ or worse
at follow-up.
For persons with nonproliferative or no retinopathy,
progression was defined as an increase in the retinopathy
severity by two or more steps (e.g., 10/10 to 21/21 or worse
or 37/ < 37 to 43/ < 43 or worse). Progression was not
examined in persons who had proliferative retinopathy at
the 10-year examination.
Macular edema was defined as thickening of the retina
with or without partial loss of transparency within one disc
diameter (DD) from the center of the macula (Early Treat-
ment Diabetic Retinopathy Study Research Group, 1985) or
the presence of focal photocoagulation scars in the macular
area (associated with a history of development of macular
edema) as documented by stereoscopic fundus photographs.
Clinically significant macular edema was based on the
detailed gradings and was defined as the presence of any
one of the following: thickening of the retina located 500 mmor less from the center of the macula (Early Treatment
Diabetic Retinopathy Study Research Group, 1985), hard
exudates with thickening of the adjacent retina 500 mm or less
from the center of the macular, or a zone of retinal thickening
one disc area or larger in size, located one disc diameter or
less from the center of the macula. If macular edema could not
be graded in an eye, the individual was assigned the score of
the other eye. The incidence of macular edema was estimated
from data for all persons who had no macular edema and had
not been previously treated with photocoagulation at the
10-year examination and who participated in the follow-up
examination 4 years later.
Cardiovascular disease status was determined as fol-
lows: a person was classified as having a history of
cardiovascular disease if he/she reported having been told
by a physician that he/she had angina, or had a heart
attack or stroke. The history of angina, heart attack, and
stroke was verified by a physician. Incidence of cardio-
vascular disease was presence at the 14-year examination
among participants without it at the 10-year examination.
Urine protein was considered present at a concentration of
0.3 g/l or greater. Incidence of urine protein and incidence
of lower extremity amputation were defined in a manner
similar to incidence of cardiovascular disease. We also
defined the incidence of sores or ulcers on the feet or
ankles or lower extremity amputation as the occurrence of
either event among participants without both at the
10-year examination.
Current age was defined as the age at the time of the
examination in 1990–1992. Age at diagnosis of diabetes
was defined as the age at the time the diagnosis was first
recorded by a physician on the patient’s chart or in a
hospital record. The duration of diabetes was that period
between the age at diagnosis and the age at the 1990–
1992 examination.
The means of both systolic and diastolic blood pressures
were the averages of the last two of three measurements
(Hypertension Detection and Follow-up Program Coopera-
tive Group, 1976).
Cigarette smoking status was determined as follows: a
person was classified as having never smoked if he/she had
smoked fewer than 100 cigarettes in his/her lifetime, as
being an ex-smoker if he/she smoked more than this number
of cigarettes in his/her lifetime but had stopped smoking
before the examination, or as currently smoking if he/she
had not stopped. For purposes of analysis, two dichotomous
variables were defined: one to compare persons who had
previously smoked with those who had never smoked and
one to compare persons who currently smoked with those
who had never smoked. Because lower extremity amputa-
tions were infrequent (N = 13) and, because they may be a
result of sores or ulcers on the feet or ankles, we combined
information for incidences of these two categories of out-
come in the analytic models.
4. Statistical analysis
To determine the relative risks and 95% confidence
intervals for the endpoints, the peak expiratory flow rate
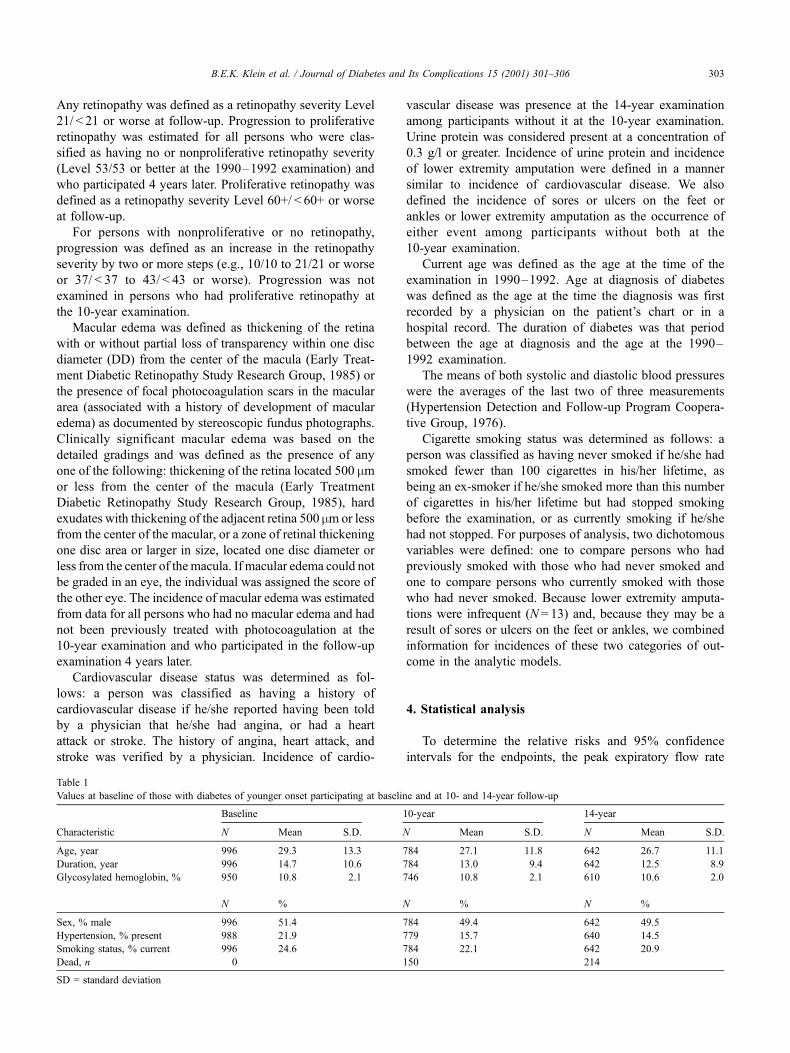
Table 1
Values at baseline of those with diabetes of younger onset participating at baseline and at 10- and 14-year follow-up
Baseline 10-year 14-year
Characteristic N Mean S.D. N Mean S.D. N Mean S.D.
Age, year 996 29.3 13.3 784 27.1 11.8 642 26.7 11.1
Duration, year 996 14.7 10.6 784 13.0 9.4 642 12.5 8.9
Glycosylated hemoglobin, % 950 10.8 2.1 746 10.8 2.1 610 10.6 2.0
N % N % N %
Sex, % male 996 51.4 784 49.4 642 49.5
Hypertension, % present 988 21.9 779 15.7 640 14.5
Smoking status, % current 996 24.6 784 22.1 642 20.9
Dead, n 0 150 214
SD = standard deviation
B.E.K. Klein et al. / Journal of Diabetes and Its Complications 15 (2001) 301–306 303
at the 10-year examination was divided into quartile ranges.
Tests for trends in rates were performed by the Mantel–
Haenszel procedure (Mantel, 1963). Multivariate analyses
for predicting the endpoints were performed by logistic
regression (Hosmer & Lemeshow, 1989). Power estimates
were obtained from nQuery Advisor and were based on the
c2 test of proportions (Elashoff, 1999).
5. Results
A comparison of persons who participated in the first
WESDR examination and in the third and fourth examina-
tions reveals that those participants who contributed data to
the current analyses were younger at baseline, more likely
to be nonsmokers and to have had lower blood pressure
(Table 1). Most who did not return for the later follow-up
examinations had died.
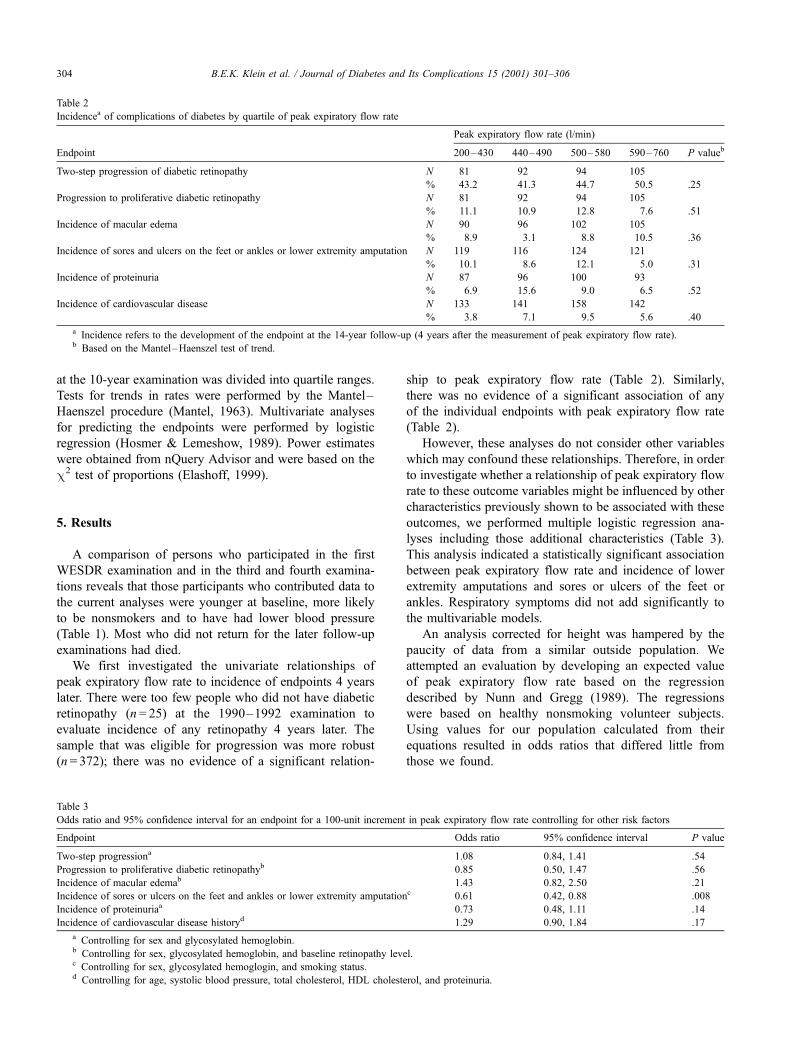
We first investigated the univariate relationships of
peak expiratory flow rate to incidence of endpoints 4 years
later. There were too few people who did not have diabetic
retinopathy (n = 25) at the 1990–1992 examination to
evaluate incidence of any retinopathy 4 years later. The
sample that was eligible for progression was more robust
(n = 372); there was no evidence of a significant relation-
ship to peak expiratory flow rate (Table 2). Similarly,
there was no evidence of a significant association of any
of the individual endpoints with peak expiratory flow rate
(Table 2).
However, these analyses do not consider other variables
which may confound these relationships. Therefore, in order
to investigate whether a relationship of peak expiratory flow
rate to these outcome variables might be influenced by other
characteristics previously shown to be associated with these
outcomes, we performed multiple logistic regression ana-
lyses including those additional characteristics (Table 3).
This analysis indicated a statistically significant association
between peak expiratory flow rate and incidence of lower
extremity amputations and sores or ulcers of the feet or
ankles. Respiratory symptoms did not add significantly to
the multivariable models.
An analysis corrected for height was hampered by the
paucity of data from a similar outside population. We
attempted an evaluation by developing an expected value
of peak expiratory flow rate based on the regression
described by Nunn and Gregg (1989). The regressions
were based on healthy nonsmoking volunteer subjects.
Using values for our population calculated from their
equations resulted in odds ratios that differed little from
those we found.
Table 2
Incidencea of complications of diabetes by quartile of peak expiratory flow rate
Peak expiratory flow rate (l/min)
Endpoint 200–430 440–490 500–580 590–760 P valueb
Two-step progression of diabetic retinopathy N 81 92 94 105
% 43.2 41.3 44.7 50.5 .25
Progression to proliferative diabetic retinopathy N 81 92 94 105
% 11.1 10.9 12.8 7.6 .51
Incidence of macular edema N 90 96 102 105
% 8.9 3.1 8.8 10.5 .36
Incidence of sores and ulcers on the feet or ankles or lower extremity amputation N 119 116 124 121
% 10.1 8.6 12.1 5.0 .31
Incidence of proteinuria N 87 96 100 93
% 6.9 15.6 9.0 6.5 .52
Incidence of cardiovascular disease N 133 141 158 142
% 3.8 7.1 9.5 5.6 .40
a Incidence refers to the development of the endpoint at the 14-year follow-up (4 years after the measurement of peak expiratory flow rate).b Based on the Mantel–Haenszel test of trend.
Table 3
Odds ratio and 95% confidence interval for an endpoint for a 100-unit increment in peak expiratory flow rate controlling for other risk factors
Endpoint Odds ratio 95% confidence interval P value
Two-step progressiona 1.08 0.84, 1.41 .54
Progression to proliferative diabetic retinopathyb 0.85 0.50, 1.47 .56
Incidence of macular edemab 1.43 0.82, 2.50 .21
Incidence of sores or ulcers on the feet and ankles or lower extremity amputationc 0.61 0.42, 0.88 .008
Incidence of proteinuriaa 0.73 0.48, 1.11 .14
Incidence of cardiovascular disease historyd 1.29 0.90, 1.84 .17
a Controlling for sex and glycosylated hemoglobin.b Controlling for sex, glycosylated hemoglobin, and baseline retinopathy level.c Controlling for sex, glycosylated hemoglogin, and smoking status.d Controlling for age, systolic blood pressure, total cholesterol, HDL cholesterol, and proteinuria.
B.E.K. Klein et al. / Journal of Diabetes and Its Complications 15 (2001) 301–306304

6. Discussion
Our analyses suggest that peak expiratory flow rate was
inversely associated with progression to proliferative retin-
opathy, incidence of lower extremity amputation or of sores
or ulcers on the feet or ankles, and incidence of proteinuria,
although only the relationship to the lower extremity lesions
was significant.
Diminished pulmonary and respiratory functions may be
associated with tissue oxygenation and other metabolic
functions at the cellular level. These could be causally
related to the complications that we have evaluated. Dia-
betes is associated with hyalinization of alveolar basement
membranes, microvascular changes (Vracko et al., 1979),
and abnormal lung elasticity (Schuyler et al., 1976). There
are various measures of pulmonary and respiratory function
that are used to detect which mechanism is more likely to be
compromised. Peak expiratory flow rate is only one such
measure and it is thought to best reflect large airway
functions, while our subjects may be experiencing pulmon-
ary/respiratory dysfunction on many levels. Because it is not
feasible to perform more extensive testing, we are limited in
our ability to determine the presence and severity of other
pulmonary/respiratory functions that may have been influ-
enced by diabetes in our population.
The prevalence and incidence of sores and ulcers on the
feet or ankles and lower extremity amputations (Moss,
Klein, & Klein, 1992) in this cohort have been shown to
be related to many characteristics, some of which are
related directly to diabetes, others not. The findings from
the current investigation add another factor. Peak expir-
atory flow rate is at least a risk indicator, if not a cause of
these problems.
A possible explanation for the lack of significant asso-
ciations between poorer peak expiratory flow rate and other
vascular complications, aside from the possibility that no
causal relationship exists, is that these complications are
more strongly associated with the other risk factors and with
local factors than is true for the lower extremity lesions.
While peak expiratory flow rate has been linked to mortality
from cardiovascular disease (Cook et al., 1991), there are
little published data describing its association to measures
of tissue oxygenation which may be a direct result of
diabetic microangiopathy.
The underlying approach we have taken is the longit-
udinal one which is appropriate when searching for poten-
tially causal associations. However, it is likely that
diminished peak expiratory flow rate is another ‘‘complica-
tion’’ of diabetes and one which may precede the other
complications. It may or may not be causally related to the
development or progression of the other lesions. We are
unable to sort these questions out in our observational
epidemiologic investigation.
Another consideration in evaluating our findings is that
the average duration of diabetes of our cohort when we did
our initial measurement of peak expiratory flow rate was 23
years. The group had already experienced significant incid-
ence and progression of diabetic retinopathy (Klein et al.,
1989a, 1989b), macular edema (Klein, Moss, Klein, Davis,
& DeMets, 1989), proteinuria (Klein, Klein, & Moss, 1991),
amputations (Moss et al., 1992), end stage renal disease
(Klein, Klein, & Moss, 1996), and death (Moss, Klein, &
Klein, 1991). Thus, those at highest risk for many of the
endpoints of interest, even if they were related to pulmonary
function, were excluded from the analyses by virtue of
having experienced the event at or before we measured
peak expiratory flow rate and therefore were not eligible to
be incident cases.
We note that peak expiratory flow rate is dependent upon
subject effort (Clement & Van de Woestijne, 1971; Sobel &
Emergil, 1964). Effort may be a function of physical fitness
and therefore peak expiratory flow rate may, in a sense, be a
psycho-physical test. However, it is associated with age,
smoking, and respiratory symptoms suggesting that it is
reflecting pathologic or possibly degenerative states (Cook
et al, 1989).
Lastly, we have limited power to detect some of these
relationships. For example, the power to find a halving of
the incidence of proteinuria between the lowest and highest
quartiles of peak expiratory flow rate is 10–15%.
In light of research findings of others showing a
relationship of peak expiratory flow rate to cardiovascular
disease death (Cook et al., 1991) and to findings in this
cohort indicating the relationship of glycosylated hemo-
globin to peak expiratory flow rate, studies of the
relationship of microvascular endpoints to pulmonary
function early in the course of disease are of interest
and may be best addressed by studying an incipient
cohort. They may suggest that the importance of glyce-
mia in complications may, in part, be mediated by
pulmonary function.
Acknowledgments
This research is supported by National Institute of Health
grant EY12198 (R. Klein, BEK Klein).
References
Bell, D., Collier, A., Matthews, D. M., Cooksey, E. J., McHardy, G. J., &
Clarke, B. F. (1988). Are reduced lung volumes in IDDM due to defect
in connective tissue? Diabetes, 37, 829–831.
Breuer, H. W., Breuer, J., & Berger, M. (1988). Transcutaneous oxygen
pressure measurements in Type I diabetic patients for early detection of
functional diabetic microangiopathy. European Journal of Clinical In-
vestigation, 18, 454–459.
Cameron, N. E., & Cotter, M. A. (1999). Effects of antioxidants on nerve
and vascular dysfunction in experimental diabetes. Diabetes Research
and Clinical Practice, 45, 137–146.
Clement, J., & Van de Woestijne, K. P. (1971). Variability of maximum
expiratory flow-volume curves and effort independency. Journal of
Applied Physiology, 31, 55–62.
B.E.K. Klein et al. / Journal of Diabetes and Its Complications 15 (2001) 301–306 305
Cook, N. R., Evans, D. A., Scherr, P. A., Speizer, F. E., Vedal, S., Branch,
L. G., Huntley, J. C., Hennekens, C. H., & Taylor, J. O. (1989). Peak
expiratory rate in an elderly population. American Journal of Epidemi-
ology, 130, 66–78.
Cook, N. R., Evans, D. A., Scherr, P. A., Speizer, F. E., Taylor, J. O., &
Hennekens, C. H. (1991). Peak expiratory flow rate and 5-year mortal-
ity in an elderly population. American Journal of Epidemiology, 133,
784–794.
Dahlquist, M., Eisen, E. A., Wegman, D. H., & Kriebel, D. (1993). Re-
productivity of peak flow measurements. Occupational Medicine, State
of the Art Reviews, Vol. 8, No. 2, Philadelphia, Hanley and Belfus,
April – June.
Diabetic Retinopathy Study Research Group. (1981). Report 7: a modifi-
cation of the Airlie House classification of diabetic retinopathy. Inves-
tigative Ophthalmology and Visual Science, 21, 210–226.
Dyck, P. J., & Giannini, C. (1996). Pathologic alterations in the diabetic
neuropathies of humans: a review. Journal of Neuropathology and Ex-
perimental Neurology, 55, 1181–1193.
Early Treatment Diabetic Retinopathy Study Research Group. (1985).
Photocoagulation for diabetic macular edema. Early treatment dia-
betic retinopathy study report 1. Archives of Ophthalmology, 103,
1796–1806.
Early Treatment Diabetic Retinopathy Study Research Group. (1991).
Grading diabeti retinopathy from stereoscopic color fundus photo-
graphs—an extension of the modified Airlie House classification.
ETDRS Report No. 10. Ophthalmology, 98, 786–806.
Elashoff, J. D. (1999). nQuery Advisor, Version 3.0 User’s Guide. Los
Angeles, CA.
Ferris, B. G. (1978). Epidemiology standardization project (American Thora-
cic Society). American Review of Respiratory Disease, 118, 1–120.
Hosmer, D. W., & Lemeshow, S. (1989). Applied logistic regression. New
York: Wiley.
Hypertension Detection and Follow-up Program Cooperative Group.
(1976). The hypertensive detection and follow-up program. Preventive
Medicine, 5, 207–215.
Klein, B. E. K., Davis, M. D., Segal, P., Long, J. A., Harris, W. A., Haug,
G., Magli, Y., & Syrjala, S. (1984). Diabetic retinopathy. Assessment of
severity and progression. Ophthalmology, 91, 10–17.
Klein, R., Klein, B. E. K., Moss, S. E., et al (1984). Prevalence of diabetes
mellitus in southern Wisconsin. American Journal of Epidemiology,
119, 54–61.
Klein, R., Klein, B. E. K., & Moss, S. E. (1991). The incidence of gross
proteinuria in people with insulin-dependent diabetes mellitus. Archives
of Internal Medicine, 151, 1344–1348.
Klein, R., Klein, B. E. K., & Moss, S. E. (1996). Relation of glycemic
control to diabetic microvascular complications in diabetes mellitus.
Annals of Internal Medicine, 124, 90–96.
Klein, R., Klein, B. E. K., Moss, S. E., & Cruickshanks, K. J. (1994). The
Wisconsin epidemiologic study of diabetic retinopathy: XIV. Ten-year
incidence and progression of diabetic retinopathy. Archives of Ophthal-
mology, 112, 1217–1228.
Klein, R., Klein, B. E. K., Moss, S. E., Davis, M. D., & DeMets, D. L.
(1984a). The Wisconsin epidemiologic study of diabetic retinopathy: II.
Prevalence and risk of diabetic retinopathy when age at diagnosis is less
than 30 years. Archives of Ophthalmology, 102, 520–526.
Klein, R., Klein, B. E. K., Moss, S. E., Davis, M. D., & DeMets, D. L.
(1984b). The Wisconsin epidemiologic study of diabetic retinopathy:
III. Prevalence and risk of diabetic retinopathy when age at diagnosis is
30 or more years. Archives of Ophthalmology, 102, 527–532.
Klein, R., Klein, B. E. K., Moss, S. E., Davis, M. D., & DeMets, D. L.
(1989a). The Wisconsin epidemiologic study of diabetic retinopathy:
IX. Four-year incidence and progression of diabetic retinopathy when
age at diagnosis is less than 30 years. Archives of Ophthalmology, 107,
237–243.
Klein, R., Klein, B. E. K., Moss, S. E., Davis, M. D., & DeMets, D. L.
(1989b). The Wisconsin epidemiologic study of diabetic retinopathy:
X. Four-year incidence and progression of diabetic retinopathy when
age at diagnosis is 30 years or more. Archives of Ophthalmology, 107,
244–249.
Klein, R., Moss, S. E., Klein, B. E. K., Davis, M. D., & DeMets, D.
L. (1989). The Wisconsin epidemiologic study of diabetic retino-
pathy: XI. The incidence of macular edema. Ophthalmology, 96,
1501–1510.
Linsenmeier, R. A., Braun, R. D., McRipley, M. A., Padnick, L. B., Ahmed,
D. L., Hatchell, D. L., McLeod, D. S., & Lutty, G. A. (1998). Retinal
hypoxia in long-term diabetic cats. Investigative Ophthalmology and
Visual Science, 39, 1647–1657.
Mantel, N. (1963). Chi-square tests with one degree of freedom: extensions
of the Mantel–Haenszel procedure. Journal of the American Statisti-
cian Association, 58, 690–700.
Moss, S. E., Klein, R., & Klein, B. E. K. (1991). Cause-specific mortality in
a population-based study of diabetes. American Journal of Public
Health, 81, 1158–1162.
Moss, S. E., Klein, R., & Klein, B. E. K. (1992). The prevalence and
incidence of lower extremity amputation in a diabetic population. Ar-
chives of Internal Medicine, 152, 610–616.
Moss, S. E., Klein, R., Klein, B. E. K., Spennetta, T. L., & Shrago, E. S.
(1988). Methodologic considerations in measuring glycosylated hemo-
globin in epidemiologic studies. Journal of Clinical Epidemiology, 41,
645–649.
Nakhostine, N., Nadeau, R., & Lamontagne, D. (1997). Altered hypoxia-
induced coronary vasodilatation in diabetic rabbit heart. Canadian Jour-
nal of Physiology and Pharmacology, 75, 1267–1272.
Nunn, A. J., & Gregg, J. (1989). New regression equation for predict-
ing peak expiratory flow in adults. British Medical Journal, 298,
1068–1070.
Primhak, R. A., Whincup, G., Tsanakas, J. N., & Milner, R. D. (1987).
Reduced vital capacity in insulin-dependent diabetes. Diabetes, 36,
324–326.
Quick-Step Fast Hemoglobin Test System (1981). Akron, OH: Isolab.
Ramirez, L. C., Dal Nogare, A., Hsia, C., Arauz, C., Butt, I., Strowig, S. M.,
Schnurr-Breen, L., & Raskin, P. (1991). Relationship between diabetes
control and pulmonary function in insulin-dependent diabetes mellitus.
American Journal of Medicine, 91, 371–376.
Sandler, M., Bunn, A. E., & Stewart, R. I. (1986). Pulmonary function in
young insulin-dependent diabetic subjects. Chest, 90, 670–675.
Schuyler, M. R., Niewoehner, D. E., Inkley, S. R., & Kohn, R. (1976).
Abnormal lung elasticity in juvenile diabetes mellitus. American Review
of Respiratory Disease, 113 (1), 37–41.
Sobel, B. J., & Emergil, C. (1964). Subject effort and the expiratory flow
rate. American Review of Respiratory Disease, 89, 402–408.
Veves, A., Donaghue, V. M., Sarnow, M. R., Giurini, J. M., Campbell, D.
W., & LoGerfo, F. W. (1996). The impact of reversal of hypoxia by
revascularization on the peripheral nerve function of diabetic patients.
Diabetologia, 39, 344–348.
Vracko, R., Thorning, D., & Huang, T. W. (1979). Basal lamina of alveo-
lar epithelium and capillaries: quantitative changes with aging and in
diabetes mellitus. American Review of Respiratory Disease, 120 (5),
973–983.
Walton, S., Byrd, R. R. Jr., Fields, C. L., Ossorio, M. A., & Roy, T. M.
(1994). Abnormal pulmonary function and juvenile onset diabetes mel-
litus. Journal of the Kent Medical Association, 92, 101–104.
Wright, B. M. (1978). A miniature Wright peak flow meter. British Medical
Journal, 2, 1627–1628.
B.E.K. Klein et al. / Journal of Diabetes and Its Complications 15 (2001) 301–306306

![The Guide - Diabetic Retinopathy - Vision Lossvisionloss.org.au/wp-content/uploads/2016/05/The... · the guide [diabetic retinopathy] What is Diabetic Retinopathy? Diabetic Retinopathy](https://img.pdfslide.us/doc/110x75/5e3ed00bf9c32e41ea6578a8/the-guide-diabetic-retinopathy-vision-the-guide-diabetic-retinopathy-what.jpg)