Embed Size (px)
Citation preview

Hypertensive retinopathy:A Review For PG preparation
Dr. Prithwiraj Maiti
Intern, R.G.Kar Medical College, Kolkata
Founder of Pgblaster India
Author of the following titles (Both published by Jaypee Brothers):
A Practical Handbook of Pathology Specimens and Slides &
An Ultimate Guide to Community Medicine

Contents
• Introduction
• Pathogenesis
• Grading
• Clinical types
• Clinical features
• Diagnosis
• Management

Introduction
• Hypertensive retinopathy refers to the changes in the fundus occurring in a patient of systemic hypertension.

Pathogenesis
3 factors are responsible for pathogenesis of hypertensive retinopathy:
1. Vasoconstriction: It is the primary response of retinal arterioles to raised blood pressure. It reflects the severity of hypertension.
2. Atherosclerosis: It mainly occurs in older patients. It reflects the duration of hypertension.
3. Increased vascular permeability: It results from hypoxia and may result in retinal edema, exudates and hemorrhages.

Keith and Wegner Grading (1939)
GRADE 1 : Tortuosity (twisting) of retinal arteries with increased reflectiveness (silver wiring)
GRADE 2 : Grade 1 + Arteriovenous napping (thickened retinal arteries pass over retinal veins)
GRADE 3 : Grade 2 + flamed shape haemorrhage and cotton wool exudates (due to small infarct)
GRADE 4 : Grade 3 + papilloedema (blurry margin of the optic disc due to swelling).

NORMAL RETINAL IMAGE

GRADE 1: Tortuosity of retinal arteries and silver wiring
GRADE 2 : G1 + AV nipping (arrow – artery cross over onto vein)
GRADE 3 : G2 + flame-shaped haemorrhage and cotton wool exudate (whitish)
GRADE 4 : G3 + papilloedema

Clinical types
4 clinical types are seen:
Hypertension with involutionary (senile) sclerosis: In old age patients
Hypertension without sclerosis: In young patients exposed to raised BP for a short duration
Hypertension with compensatory arteriolar sclerosis: In young patients exposed to benign hypertension for a long duration (usually associated with benign nephrosclerosis; thus called renal retinopathy)
Malignant hypertension: Rapidly progressive and severe changes in fundus (marked vasoconstriction, papilloedema, flame shaped hemorrhage, cotton wool spots…. everything is seen; but papilloedema is an essential feature).

Clinical features
• Acute malignant hypertension will cause patients to complain of eye pain, headaches or reduced visual acuity.
• Chronic arteriosclerotic changes from hypertension will not cause any symptoms alone.

Diagnosis
Diagnosis is by history (duration and severity of hypertension) and fundoscopy. Sometimes, fluorescein angiography may be required.
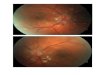
Fluorescein angiography showing capillary nonperfusion in the area corresponding to the cotton-wool patch; note the hypofluorescence of the intraretinal hemorrhage, caused by blockage

Management
• By itself, chronic hypertensive retinopathy rarely, if ever, results in significant loss of vision. Treatment of the underlying systemic condition can halt the progress of the retinal changes, but arteriolar narrowing and arteriovenous nicking usually are permanent.
• Treatment of malignant hypertensive retinopathy consists of lowering blood pressure in a slow, deliberate, controlled fashion to prevent end-organ damage.
• Too rapid a decline can lead to ischemia of the optic nerve head, brain and other vital organs, resulting in permanent damage.

• Drugs that are commonly used in the outpatient setting to reduce blood pressure include:
Angiotensin converting enzyme inhibitors,
Calcium channel blockers,
Diuretics, and
β-adrenergic blockers.
• Very rarely, If vision loss occurs, treatment of the retinal edema with laser or with intravitreal injection of corticosteroids or antivascularendothelial growth factor drugs (eg, ranibizumab, pegaptanib, bevacizumab) may be useful.

Thank you….


![Review Article ...or 4 hypertensive retinopathy [1]. In one study, 16.7% of ... taneously hypertensive rat (SHR) [24–27]. Furthermore, bilateral dorsal rhizotomy at the level T-10](https://img.pdfslide.us/doc/110x75/60e109cdafe2e515524457bd/review-article-or-4-hypertensive-retinopathy-1-in-one-study-167-of-.jpg)








![The Guide - Diabetic Retinopathy - Vision Lossvisionloss.org.au/wp-content/uploads/2016/05/The... · the guide [diabetic retinopathy] What is Diabetic Retinopathy? Diabetic Retinopathy](https://img.pdfslide.us/doc/110x75/5e3ed00bf9c32e41ea6578a8/the-guide-diabetic-retinopathy-vision-the-guide-diabetic-retinopathy-what.jpg)