Embed Size (px)
Citation preview
Is anyone listening tothe concerns of clinicalteachers?Mary Lawson, Department of Psychological Medicine, Monash University, Australia
There have been widespreaddeliberations about thequality of medical school
education in Australia, whichhave been voiced in both themedia and the academic environ-ment. Debate has been ferventand much of it has emanated fromdiscontented clinical teachers.
Some of the issues behind thediscontent include competitionbetween the specialty collegesand the medical schools in provi-sion of postgraduate training,concerns about the growth ofgraduate-entry medical education(GEM) and problem-based learn-ing (PBL), clinical workforce is-sues (particularly in ruralenvironments), selection issuesand an increased reliance on
international medical graduates.The ways in which these factorsimpact upon the milieu in whichclinical teaching is conducted arecomplex.
This paper outlines the factorsthat impact negatively on theexperience of the clinical teacherand how these have been ad-dressed at a national level.
WHAT IS IT REALLY LIKE TOBE A CLINICAL TEACHER?
The clinical teacher is widelyacknowledged as central to effec-tive clinical education.1 Recentwork has attempted to clarify ourunderstanding of what effectiveclinical teaching is using the
perceptions of physicians2 and allthose involved in the clinicalteaching episode.3 Some of thesefindings have not been antici-pated (such as the paradoxicalfinding that ‘humiliation andintimidation’ can be presented asqualities of both ‘good’ and ‘bad’clinical teachers). Less surpris-ingly, the impact of high qualityteaching is high and has beendemonstrated to influence thecareer choices of students posi-tively.4
We also know that clinicalteaching can be a solitary expe-rience and that some clinicalteachers oppose change, withexamples including resistance tothe introduction of peer observa-tion.5 This could be anticipated,
Clinicalteaching can be
a solitaryexperience
Ozzawapaper
218 � Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 218–223

given the customary isolation inwhich most clinical work takesplace. Much clinical teachingtakes place in a private spaceinvolving the patient and theclinician with the medical studentproviding an added dimension.So, in the clinical environment,one-to-one teaching is highlyvalued and medical schools oftenperceive low student:tutor ratiosto be key indicators of a qualityeducational system.
IN THE CONTEXT OF THEDOCTOR–PATIENTRELATIONSHIP, THREE ISA CROWD
When a patient is present, it is notdesirable to have a large number ofstudents there as well. One of thefew places where clinical teachingoccurs in a highly public arena isin the operating theatre. Otherclinical situations in which largegroups of students clamber aroundthe bedside to see clinical signs orask detailed or intimate questionsin the outpatient clinic have longbeen criticised. Patients shouldnot be treated as ‘clinical mate-rial’. The increasing trend toempower patients to participate inclinical decision-making is widelywelcomed and is attracting re-search efforts.6 Patients who areinvolved as equal partners in theclinical environment may, how-ever, decide that they do not wantto be examined or repeat theirclinical history to a succession ofeager but inexperienced students.Such drivers are challenging thestatus quo of patient-basedteaching.
Contemporary developmentsin clinical teaching have focusedon structured approaches toteaching and learning.7 Theseinclude the use of low and highfidelity simulation and greaterreliance on simulated patients.Although evaluated favourably,such approaches inevitablyremove students from authenticpatient contact. The resultingimpact on the clinical teacher
may be to isolate them furtherfrom mainstream educationalsystems.
HOW DO CLINICALTEACHERS GET SUPPORT?
Peer review systems are still rela-tively uncommon in clinicalteaching, and they are fraughtwith the same practical problemsas having multiple studentsaround – namely the clinicalenvironment is simply not con-ducive to large groups of people.The development of clinical auditand governance has forcedchange in a profession that hasnot been particularly open toscrutiny – especially not from
those outside the profession.8
There can even be a mistrust ofacademic colleagues who are per-ceived to be removed from the‘reality’ of clinical responsibili-ties. These misgivings are high-lighted by the ever-increasingclinical workload.
Consequently, it is difficult forclinical teachers to feel part of abroader educational system. Tu-tors report feeling removed fromuniversity decision-making sys-tems and can feel that theirendeavour goes unrecognised andunrewarded.9 Medical schoolshave been criticised for failing togive, and potentially receive,feedback.10
Patientsshould not betreated as‘clinicalmaterial’
� Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 218–223 219
The debate regarding the needfor more tangible rewards andrecognition for clinical teachinghas been extensive. Formal pro-vision of teacher training isincreasing but this is still at arelatively adolescent stage ofdevelopment. In the UK, theLabour government had a visionof compulsory teacher training forall teachers involved in highereducation by 2006. This remainssome way off and is far from thecase in the Australian context.11
No wonder clinical teachersmay be feeling discontented.
THE IMPLICATIONS OFWORKING AND TEACHINGIN ISOLATION
Working in such isolated circum-stances, it is hard for teachers toassess the competence of stu-dents and junior doctors ‘objec-tively’. It is difficult to calibratestandards across students. Newermethods of teaching and learningthat differ from teachers’ ownexperiences may seem strange andunfathomable. Moreover undesir-able teaching practices, such asthe use of ridicule and humilia-tion, can go unchallenged.12
HOW TO HEAR ANDRESPOND TO CONCERNS
Failing to canvass, listen andrespond to the concerns of
teachers can escalate them.In Australia the media haveaired multiple reports of ardentdissatisfaction with variouscomponents of the medical edu-
cation system expressed publiclyby a number of senior or formeracademics and clinical special-ists.13–18 The questions ‘Is medi-cal education in crisis?’ and ‘Arewe downgrading basic medicalsciences?’ have been asked bymembers of the Australian medi-cal community, such as the Aus-tralian Doctors’ Fund. Headlinecomments such as ‘Dr Deaths fromour own medical schools’ havefuelled the debate on the qualityof both medical students andmedical schools. The implicationhas been that Australia is under-going a ‘dumbing down’ of med-ical education.
To prevent an upward spiral ofconcerns, there are a number ofmeans by which clinical teachers’views could be garnered:
The media haveaired multiple
reports ofardent
dissatisfaction
220 � Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 218–223
• Participation in staff trainingand professional developmenton education: this can work attwo levels – to enhance skillsacquisition and reduce thefeelings of isolation via aca-demic networking.
• Routine and robust systems forevaluating clinical teaching:there are many systems toevaluate clinical teaching.However, it is difficult toprovide this consistently andcomprehensively across clini-cal sites, whilst ensuring thatfeedback is timely and reachesthe correct individuals is ahard task.
• Involvement in medical educa-tion research and development:such initiatives can addresslocal concerns and providecontextualised solutions toproblems in practice.
Such strategies work withvarying degrees of success inpractice. In Australia, where thereare few medical schools, massivegeographical distances and a rel-ative scarcity of academic net-works and associations formedical education, such endeav-our can be thwarted.
THE RESPONSE TOCONCERNS ABOUT THEQUALITY OF MEDICALEDUCATION IN AUSTRALIA
The debate about the educationof medical students in Australia,both in the medical communityand in the media, could not beignored. It centred on percep-tions of poor knowledge of anat-omy, concerns associated with theuse of PBL, GEM and studentselection.
The former Minister of Educa-tion, the Hon Dr Brendan Nelson,announced in February 2005 thata major empirical review of med-ical education would take place.The Australian Medical EducationStudy (AMES), which is beingmanaged by the Department of
Education, Science and Training(DEST), is intended to answer thequestion: ‘What makes for successin medical education?’
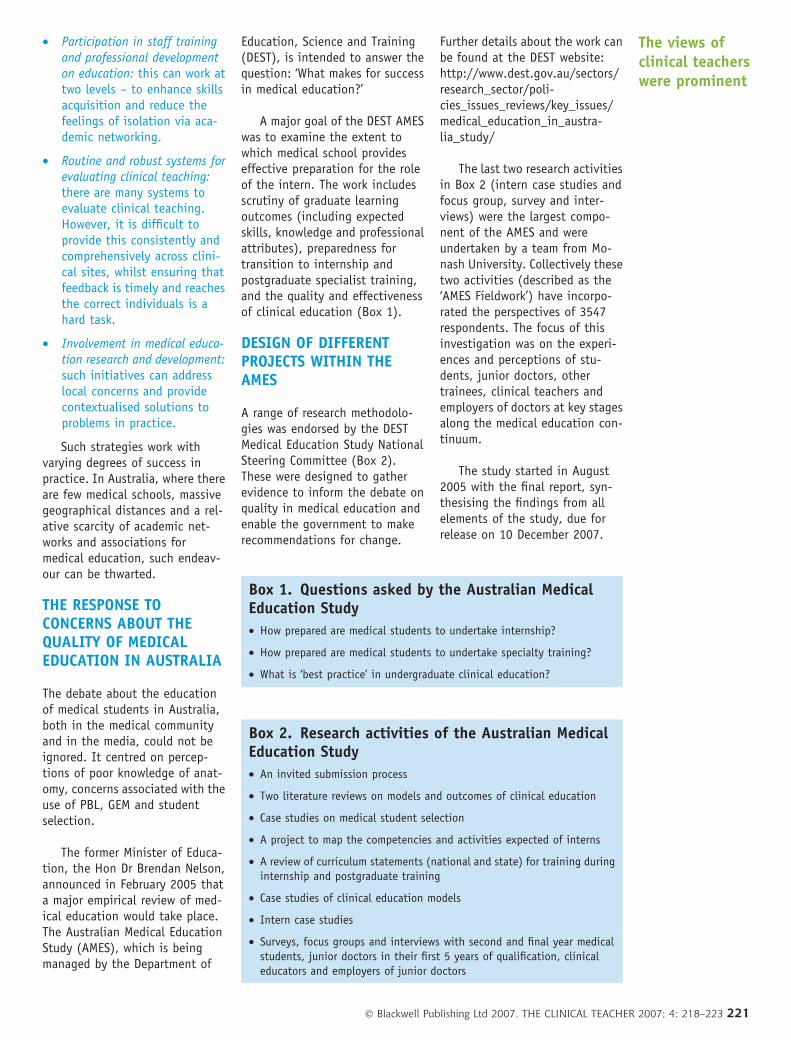
A major goal of the DEST AMESwas to examine the extent towhich medical school provideseffective preparation for the roleof the intern. The work includesscrutiny of graduate learningoutcomes (including expectedskills, knowledge and professionalattributes), preparedness fortransition to internship andpostgraduate specialist training,and the quality and effectivenessof clinical education (Box 1).
DESIGN OF DIFFERENTPROJECTS WITHIN THEAMES
A range of research methodolo-gies was endorsed by the DESTMedical Education Study NationalSteering Committee (Box 2).These were designed to gatherevidence to inform the debate onquality in medical education andenable the government to makerecommendations for change.
Further details about the work canbe found at the DEST website:http://www.dest.gov.au/sectors/research_sector/poli-cies_issues_reviews/key_issues/medical_education_in_austra-lia_study/
The last two research activitiesin Box 2 (intern case studies andfocus group, survey and inter-views) were the largest compo-nent of the AMES and wereundertaken by a team from Mo-nash University. Collectively thesetwo activities (described as the‘AMES Fieldwork’) have incorpo-rated the perspectives of 3547respondents. The focus of thisinvestigation was on the experi-ences and perceptions of stu-dents, junior doctors, othertrainees, clinical teachers andemployers of doctors at key stagesalong the medical education con-tinuum.
The study started in August2005 with the final report, syn-thesising the findings from allelements of the study, due forrelease on 10 December 2007.
Box 1. Questions asked by the Australian MedicalEducation Study
• How prepared are medical students to undertake internship?
• How prepared are medical students to undertake specialty training?
• What is ‘best practice’ in undergraduate clinical education?
Box 2. Research activities of the Australian MedicalEducation Study
• An invited submission process
• Two literature reviews on models and outcomes of clinical education
• Case studies on medical student selection
• A project to map the competencies and activities expected of interns
• A review of curriculum statements (national and state) for training duringinternship and postgraduate training
• Case studies of clinical education models
• Intern case studies
• Surveys, focus groups and interviews with second and final year medicalstudents, junior doctors in their first 5 years of qualification, clinicaleducators and employers of junior doctors
The views ofclinical teacherswere prominent
� Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 218–223 221

STRENGTHS OF THE AMESFIELDWORK
The AMES Fieldwork was con-ducted effectively with the guid-ance of a steering committeeable to provide a national andinternational perspective to thelocal situation. It was successfulin involving a large number ofindividuals with interest andinvestment in the education ofmedical students. This work hasachieved high levels of visibilityand profile within the medicaleducation community, by evalu-ating the perceptions of quality,effectiveness and preparednessfor clinical practice from a rangeof different stakeholder perspec-tives. The range of complemen-tary research methodologiesemployed has enabled a deeperunderstanding of issues to bedeveloped.
The views of clinical teacherswere prominent in the invitedsubmission process of the study.Within the fieldwork component,over 800 responses were obtainedfrom this group. The junior doctorcohort also contained individualswith a clinical teaching role,which included over 1000 furtherparticipants. It would certainly befair to say that the perspective ofthe clinical teacher has beencanvassed.
WHAT WILL HAPPEN NEXTAND WHAT WILL BE THEIMPACT?
The research process for theAMES is not yet complete. Theresults from the different re-search findings need to be fullysynthesised and interpreted. It iscritical that this synthesis con-siders the unique context andcircumstances of medical educa-tion in general and clinicalteaching in particular. It mustalso draw from the results ofearlier work in this context andenvironment, and use these as abaseline for comparisons to bemade.19
The implications for policy andpractice need to be distilled inconsultation with those whounderstand the system (not onlythe educational context but alsothe rapidly changing health carecontext) and those who have apractical understanding of all theconstraints under which medicaleducation operates. The partner-ship and collaboration betweengovernment departments will becritical to its effective achieve-ment.
The findings must be dissem-inated widely to those on whomthey impact. Recommendationsneed to be made and thenimplemented, and the changesevaluated for their impact onpractice.
All this will take time. Asalways, there is a tension be-tween the ability to conductresearch and the ability toimplement associated recommen-dations in a timely fashion,before the situation and circum-stances measured in the firstplace change.
Previous experience showsthat reviews and studies take along time to work through thesystem in medical education.An example of this is providedby the ‘Holsgrove report’ onGeneral Practice Education andTraining.20 Initial work startedon this review in 1994 and thereport was published in 1996.A whole series of activitiesoccurred subsequent to this,including further investigationand review. The ultimatechanges to general practicetraining went much further thanthe recommendations of theoriginal report, but the entireprocess extended over a periodof almost a decade.21 It isunlikely that the barriers anddrivers shaping medical educa-tion in 2007 will be the same in2017. The AMES needs to bereported in a timely and exten-sive way.
WILL THE AMES MAKE ANYDIFFERENCE TO CLINICALTEACHERS?
The impact of the AMES on clin-ical teachers remains to be seen.The invited submission processharnessed the views of a largenumber of individuals and organ-isations. Similarly, the fieldworkhas involved an extensive numberof key stakeholders in the educa-tional process, but the clinicalteachers need to view the inves-tigative process as a credibleresponse to the concerns thatthey originally raised. Medicaleducation research has not beencredited with the capacity toachieve this reliably in the past.21
So, one of the unanswered ques-tions is whether the experience ofclinical teachers will be shaped bythese research results. At themoment this is impossible topredict. A bigger question iswhether Australian clinicalteachers are very different in theirconcerns to clinical teachers any-where else in the world. There islittle reason to believe that thisshould be the case. The release ofthe study outcomes and theresulting debate in the nationaland international medical com-munity is something that is ea-gerly anticipated. Clinicalteachers in this neck of the woodshave certainly had their say.We must wait and see whethertheir message was accurate, wellreceived and will result in any-thing being changed for them.
REFERENCES
1. Jolly B. Clinical education: teachers
and Stritter’s student. Med Educ
2006;40:604–606.
2. Knight LV, Bligh J. Physicians’ per-
ceptions of clinical teaching: a
qualitative analysis in the context of
change. Adv Health Sci Ed 2006;11:
221–234.
3. Chitsabesan P, Corbett S, Walker L,
Spencer J, Barton JR. Describing
clinical teachers’ characteristics and
behaviours using critical incidents
and repertory grids. Med Educ
2006;40:645–653.
Reviews andstudies take a
long time towork through
the system
222 � Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 218–223
4. Musunuru S, Lewis B, Rikkers LF,
Chen H. Effective surgical residents
strongly influence medical students
to pursue surgical careers. J Am Coll
Surg 2007;204:164–167.
5. Adshead L, White PW, Stephenson A.
Introducing peer observation of
teaching to GP teachers: a ques-
tionnaire study. Med Teacher
2006;28:68–73.
6. Garfield S, Smith F, Francis SA,
Chalmers C. Can patients’ preferences
for involvement in decision-making
regarding the use of medicines be
predicted? Patient Educ Counsel
2007;66:361–367.
7. Bagot K, Lawson M, Jolly B et al.
International approaches to under-
graduate clinical training, Report
commissioned by Policy and Strategic
Projects Divisions, Department of
Human Services, Victoria, 2005
Available at: http://www.dhs.vic.-
gov.au/pdpd/workforce/downloads/
dhs_project_report_19july2005.pdf
(accessed 13 August 2007).
8. Irvine D. Patients, professionalism,
and revalidation. BMJ 2005;330:
1265–1268.
9. Seabrook MA. Medical teachers’
concerns about the clinical teaching
context. Med Educ 2003;37:213–
222.
10. Hendry RG, Kawai GW, Moody WE
et al. Consultant attitudes to
undertaking undergraduate teaching
duties: perspectives from hospitals
serving a large medical school. Med
Educ 2005;39:1129–1139.
11. Cook M. High aims for teaching:
Universities dispense higher learn-
ing: moves are afoot to bring their
teaching up to the same level. The
Age Newspaper April 30, 2003:
http://www.theage.com.au/
articles/2003/04/30/
1051381990622.html
(accessed 13 August 2007).
12. Stark P. Teaching and learning in the
clinical setting: a qualitative study
of the perceptions of students and
teachers. Med Educ 2003;37:975–
982.
13. Howe M. Anatomy of a crisis.
Weekend Australian 6 May 2006:
p 30. News Limited.
14. Cresswell A. Doctors fail basic anat-
omy. Weekend Australian 6 May
2006: p 1. News Limited.
15. Australian Associated Press, 2006.
New South Wales: Med schools will
be turning out Dr Deaths, Prof warns.
AAP Newswire 6 May 2005.
16. Cresswell A. Junior MDs to catch up
on anatomy. The Australian 8
May2006: p 5. General News.
17. Stevenson R, Burns J. Interview with
Julian Smith, Professor of Surgery,
Monash University. a3AW (Mel-
bourne) Breakfast. Media Report
2006.
18. Bryant S. Medical training may be
moving away from its intentions.
(Opinion). The Australian 27 May
2006.
19. Pearson S-A, Rolfe I, Ringland C,
Kay-Lambkin F. A comparison of
practice outcomes of graduates from
traditional and non-traditional
medical schools in Australia.
Med Educ 2002;36:985–991.
20. Trumble S. Changes to training for
general practice in Australia. Asia
Pacific Family Med 2003;2:171–174.
21. Skelton J. Two and a bit cheers for
academic medicine. BMJ
2006;333:716.
� Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 218–223 223