Embed Size (px)
Citation preview
Technical note
Introducing standardized protocols for anthropological measurementof virtual subadult crania using computed tomography
Nicolene Lottering a,n, Donna M. MacGregor a, Mark D. Barry b, Mikaela S. Reynolds a,Laura S. Gregory a
a Skeletal Biology and Forensic Anthropology Research Laboratory, School of Biomedical Sciences, Faculty of Health, Queensland University of Technology,Brisbane, QLD 4001, Australiab High Performance Computing and Research Services, Queensland University of Technology, Brisbane, QLD 4001, Australia
a r t i c l e i n f o
Article history:Received 28 October 2013Received in revised form20 November 2013Accepted 20 November 2013Available online 28 November 2013
Keywords:Forensic anthropologyCraniometricsMulti-slice computed tomographyPediatricsCraniumAustralia
a b s t r a c t
Objectives: This study introduces and assesses the precision of a standardized protocol for anthropo-metric measurement of the juvenile cranium using three-dimensional surface rendered models, forimplementation in forensic investigation or paleodemographic research.Materials and methods: A subset of multi-slice computed tomography (MSCT) DICOM datasets (n¼10) ofmodern Australian subadults (birth—10 years) was accessed from the “Skeletal Biology and ForensicAnthropology Virtual Osteological Database” (n41200), obtained from retrospective clinical scans takenat Brisbane children hospitals (2009–2013). The capabilities of Geomagic Design X™ form the basis of thisstudy; introducing standardized protocols using triangle surface mesh models to (i) ascertain lineardimensions using reference plane networks and (ii) calculate the area of complex regions of interest onthe cranium.Results: The protocols described in this paper demonstrate high levels of repeatability between fiveobservers of varying anatomical expertise and software experience. Intra- and inter-observer error wasindiscernible with total technical error of measurement (TEM) values r0.56 mm, constituting o0.33%relative error (rTEM) for linear measurements; and a TEM value of r12.89 mm2, equating to o1.18%(rTEM) of the total area of the anterior fontanelle and contiguous sutures.Conclusions: Exploiting the advances of MSCT in routine clinical assessment, this paper assesses theapplication of this virtual approach to acquire highly reproducible morphometric data in a non-invasivemanner for human identification and population studies in growth and development. The protocols andprecision testing presented are imperative for the advancement of “virtual anthropology” into routineAustralian medico-legal death investigation.
& 2013 Elsevier Ltd. All rights reserved.
1. Introduction
Due to a lack of documented skeletal collections available forresearch, access to clinical and post-mortem multi-slice computedtomography (MSCT) welcomes an exciting era in Australian“virtual anthropology” in the formation of large, contemporaryosteological databases for the construction of population-specificstandards for human identification [1]. The integration of MSCT asa screening tool in the disaster victim identification protocolproposed by Interpol [2], advocates the benefits of MSCT in massdisaster and medico-legal application where maceration of bonesmay be contrary to religious practices or prohibited by nationalregulations; and permits observer-independent documentation.
Accordingly, in a number of Australian mortuaries, a full bodyMSCT post-mortem scan constitutes standard autopsy procedureto supplement or replace conventional autopsy.
In clinical practice, cranial MSCT scans are routinely used fortrauma, the assessment of growth and development, pathologicalanalysis and interpretation, and as a diagnostic tool for a range ofmedical conditions. Anthropometric analyses using MSCT modelsare typically used for pre- and post-operative controls [3,4];virtual cranio-maxillofacial surgical planning and reconstructions[5–9]; and clinical evaluation of craniosynostosis [3,9–12]. Arecent influx of studies utilizing MSCT assesses the accuracy oftraditional craniometric measurements with two-dimensional(2D) or three-dimensional rendered models [13–17]. However,many studies including Kragskov et al. [16] demonstrate difficultyin localizing landmarks using axial slices in a multi-planar recon-struction space, while interpolating measurements on 3D volumerendering reconstructions is limited by voxel size, range of
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jofri
Journal of Forensic Radiology and Imaging
2212-4780/$ - see front matter & 2013 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.jofri.2013.11.005
n Corresponding author. Tel.: þ61 7 3138 1281.E-mail address: [email protected] (N. Lottering).
Journal of Forensic Radiology and Imaging 2 (2014) 34–38
intensity values and software capabilities. Recently for forensicanthropological application, Robinson et al. [17] and Brough et al.[18] introduced standardized protocols for measurement of thebones of the lower limb and the clavicle using 2D measurementsobtained from creating “virtual osteometric boards”; howevertransposition into the third dimension using CT surface renderingshas yet to be conducted for anthropological analysis.
This study proposes a methodology for attaining linear anthro-pometric measurements and novel areal calculations of thecranium using surface rendered models, for implementation inforensic investigation at the time of autopsy or for paleodemo-graphic research. Further, this study aims to determine whetherthe aforementioned protocols are highly repeatable betweenobservers of varying expertise, for application in clinical andforensic practice.
2. Materials and methods
The “Skeletal Biology and Forensic Anthropology Virtual Osteo-logical Database” housed at the Queensland University of Technol-ogy, consists of multi-slice computed tomography (MSCT) datasetsobtained from modern Australian male and female individualsaged birth to 75 years (n¼1272, November 2013). At the time ofpublication, the database included cranial/cervical CT scansacquired from 670 infants and juveniles obtained from theDepartments of Medical Imaging, Royal Brisbane Children's Hos-pital (Toshiba Aquilion LB™ CT (Toshiba Medical Systems, Tochigi,Japan); voxel size: 0.391 mm�0.391 mm�0.30 mm; slice thick-ness: 0.5 mm, slice overlap: 0.3 mm) and The Mater HealthServices (Philips Brilliance 64 CT (Philips Medical Systems, Cleve-land, USA); voxel size: 0.363 mm�0.363 mm�0.45 mm; slicethickness: 0.5 mm, slice overlap: 0.3 mm), Brisbane, Queensland(2009–2013). Biological parameters including age, sex, ancestryand weight are embedded into the meta-data of each dataset anddisclosed to investigators. Ten subadult cranial MSCT scanswere sampled from this database for validation of the followingmorphometric protocols.
2.1. Morphometric (absolute cranial size) assessment
The thin-slice stacked DICOM sets were uploaded into Amiras
(VSG, FEI Company, United States) for automated image segmenta-tion and isosurface model generation at a threshold of 150 HU.Consistent with standardized medical imaging protocols, a GantryTilt Correction (730 degrees) was applied to datasets obtainedfrom RCH, to normalize slice angle. Each cranial surface model wasextracted as a stereolithography (stl) file native to CAD software3D systems including Geomagic Design X™ (3D Systems, Inc.,United States). In Geomagic Design X™ each model was decimatedand cleaned by filling holes and applying a smoothing algorithm tocorrect any minor anomalies introduced in the isosurfacing pro-cess prior to optimization to produce a high-quality 3D recon-struction. In order to determine the maximum length and breadthof the cranium, a series of anatomical planes were constructed toprovide a reference coordinate system. The premise of this proto-col is that once the anatomical “reference” planes were identified,“offset” planes were defined to correspond to the most extremepositions or contours of the surface model (Fig. 1). Automatedplane-to-plane measurements were then calculated between theoffset planes. Maximum cranial length (GOL [19]) was measuredbetween the anterior and posterior extreme position planesparallel to the coronal plane (Fig. 1F), while maximum cranialbreadth (XCB) was measured between the bilateral extremeposition planes parallel to the mid-sagittal plane.
2.2. Connective tissue area (fontanelle) quantification
To quantify the connective tissue area corresponding to theanterior fontanelle and contiguous sutures (sagittal, coronal andmetopic sutures), the cranial isosurface mesh was anatomicallyaligned from a superior perspective. A virtual rescan (Fig. 2A) witha 0.1 mm�0.1 mm grid was conducted to isolate the superiorentity of the cranial vault. For individuals exhibiting delimitedsutures, a series of bridges were designed to enclose the perimeterof the model. The area of the isolated mesh was automaticallycalculated where the area of the connective tissue fontanelle isabsent from the surface model (bone threshold algorithm applied).With reference to the surrounding curvature network of the regionof interest, Geomagic Design X™ applies an algorithm in its fillholes function to interpolate missing surface triangles with refer-ence to an inner boundary curve (Fig. 2C). A secondary arealmeasurement with the filled fontanelle and contiguous sutureswas then calculated. Subtraction of the original mesh from thefilled mesh gave a surface area measurement corresponding to theregion of interest.
2.3. Observer error assessment
Morphometric variables including GOL, XCB and fontanelle areawere measured once on each subadult cranium (n¼10) by fiveindependent observers to assess inter-observer error in dataacquisition; intra-observer error (NL) was measured on threedifferent evaluation days with a minimum of one day betweenre-measurement. To verify the accuracy of the anthropometricmeasurements attained by MSCT, inter-instrument validity wasconducted on three dry juvenile skulls for GOL and XCB usingdigital spreading calipers. Equivalent virtual measurements weretaken on the 3D surface rendering models of the same skulls andcompared to analogue measurements. Error was quantified usingtechnical error of measurement (TEM), relative TEM (rTEM) andcoefficient of reliability (R); acceptable levels for measurementdata were rTEM o5% and R40.95 [20].
3. Results
Intra-observer and inter-observer TEM and rTEM for maximumcranial length are provided in Table 1 and Table 2, respectively, foreach of the 10 subjects. Mean rTEM did not exceed 1.01% and 1.7%for intra- and inter-observer error testing, respectively; with acoefficient of variation 40.99 for all measurement protocols(Table 3). Mann–Whitney U-Tests demonstrated no significantdifferences (PZ0.05) between observers despite varying profes-sional experience in anatomy and Geomagic Design X™. Inter-instrument error between analogue and MSCT measurementswere minimal (rTEM:r0.49%; R: 0.999) (Table 3).
4. Discussion
Consistent with the frequent recovery of the skull in forensiccasework [21], the primary purpose of this paper was to introducestandardized protocols for CT surface rendered models of thecranium using sophisticated reverse engineering capabilities toattain traditional craniometric variables and areal measurements.Further, utilizing the morphologically complex subadult cranium,this study demonstrates that the Geomagic Design X™ protocolscan be reliably replicated by investigators of varying anatomicaland/or technical experience when comprehensive instructions areavailable.
N. Lottering et al. / Journal of Forensic Radiology and Imaging 2 (2014) 34–38 35
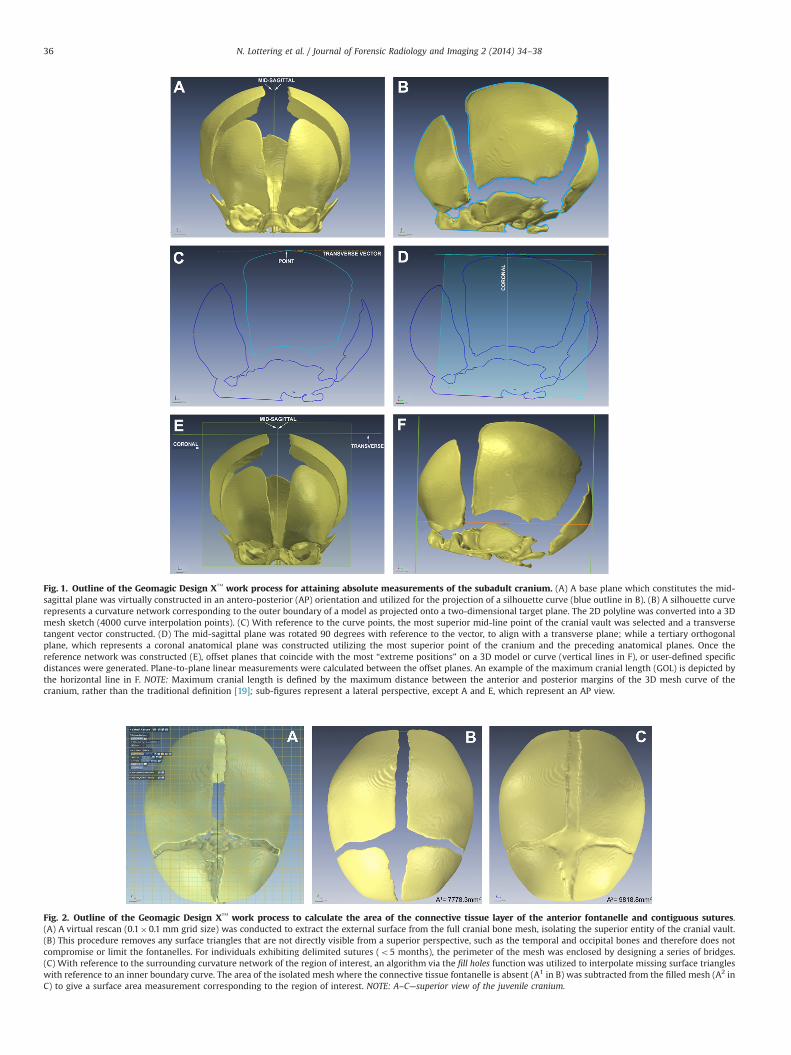
Fig. 1. Outline of the Geomagic Design X™ work process for attaining absolute measurements of the subadult cranium. (A) A base plane which constitutes the mid-sagittal plane was virtually constructed in an antero-posterior (AP) orientation and utilized for the projection of a silhouette curve (blue outline in B). (B) A silhouette curverepresents a curvature network corresponding to the outer boundary of a model as projected onto a two-dimensional target plane. The 2D polyline was converted into a 3Dmesh sketch (4000 curve interpolation points). (C) With reference to the curve points, the most superior mid-line point of the cranial vault was selected and a transversetangent vector constructed. (D) The mid-sagittal plane was rotated 90 degrees with reference to the vector, to align with a transverse plane; while a tertiary orthogonalplane, which represents a coronal anatomical plane was constructed utilizing the most superior point of the cranium and the preceding anatomical planes. Once thereference network was constructed (E), offset planes that coincide with the most “extreme positions” on a 3D model or curve (vertical lines in F), or user-defined specificdistances were generated. Plane-to-plane linear measurements were calculated between the offset planes. An example of the maximum cranial length (GOL) is depicted bythe horizontal line in F. NOTE: Maximum cranial length is defined by the maximum distance between the anterior and posterior margins of the 3D mesh curve of thecranium, rather than the traditional definition [19]; sub-figures represent a lateral perspective, except A and E, which represent an AP view.
Fig. 2. Outline of the Geomagic Design X™ work process to calculate the area of the connective tissue layer of the anterior fontanelle and contiguous sutures.(A) A virtual rescan (0.1�0.1 mm grid size) was conducted to extract the external surface from the full cranial bone mesh, isolating the superior entity of the cranial vault.(B) This procedure removes any surface triangles that are not directly visible from a superior perspective, such as the temporal and occipital bones and therefore does notcompromise or limit the fontanelles. For individuals exhibiting delimited sutures (o5 months), the perimeter of the mesh was enclosed by designing a series of bridges.(C) With reference to the surrounding curvature network of the region of interest, an algorithm via the fill holes function was utilized to interpolate missing surface triangleswith reference to an inner boundary curve. The area of the isolated mesh where the connective tissue fontanelle is absent (A1 in B) was subtracted from the filled mesh (A2 inC) to give a surface area measurement corresponding to the region of interest. NOTE: A–C—superior view of the juvenile cranium.
N. Lottering et al. / Journal of Forensic Radiology and Imaging 2 (2014) 34–3836

This study exploits the advantages offered by visualizationtechnology and the capabilities of Geomagic Design X™ andsimilar software. Although validation studies comparing MSCTmeasurement to those obtained on dry skeletal material havebeen exhaustive [18,20,22,23]; our protocols demonstrated negli-gible inter-instrument error (TEM:r0.19 mm) on three subadultteaching skulls using the same resolution specifications and linearmeasurements on both dry and virtual models, corroborating thatdigitally measured variables deviate in a range of 1–2 mm fromanalogue measurements [20,22].
This paper proposes a standardized protocol for anthropo-metric measurement for implementation in post-mortem autopsyprocedure, pediatric clinical examination or surgical planning.Precision testing demonstrated low intra- and inter-observer errorwith R-values Z0.99. Quantification of the fontanelle area demon-strated a small increase in relative error (r1.17% rTEM) comparedto the linear measurements GOL and XCB (r0.33% rTEM). Theaforementioned coefficients of reliability and rTEM figures areabove the R¼0.95 and below the 5% rTEM standards for anthro-pometric studies [20]. Franklin et al. [20] reports large discrepan-cies in craniometric measurements such as inter-orbital breadthand attributes this to observer variation in the interpretationand location of landmarks. In contrast, the offset plane protocolproposed in this study, may be utilized to conduct routinecraniometric measurements utilizing Geomagic Design X™ in anautomated manner, potentially reducing the subjective errorassociated with such analyses.
Recently, a protocol published by Brough et al. [18] forconducting virtual measurements on the juvenile clavicle usinga multi-planar view in Osirixs exhibits many similarities to theprotocols discussed in this paper, with the primary differencebeing assessment using 2D axial and lateral views rather than 3Disosurface mesh models. Two-dimensional images have distinctlimitations, including image distortion, constrained slice angleand are dependent on the patient's head position and orientation.For pediatric datasets, head alignment and slice angles vary due todifficulties with keeping children immobilized in the CT scanner;potentially resulting in significant differences in landmark locationand 2D measurements. This protocol demonstrates the benefit ofusing a reference plane-network to delineate extremities of sur-face rendered models; the protocol is not dependent on theoriginal co-ordinate system of the DICOM dataset which isdetermined by the voxel size. Furthermore depending on theinstitution scanning protocol, such was the case by the RoyalChildren's Hospital, a Gantry Tilt of 730 degrees is applied toreduce radiation exposure; therefore failure to apply post-processing techniques such as correction factors, has the potentialto influence measurement accuracy. Utilizing 3D high-qualitysurface models this study provides a superior visualization med-ium to understand spatial structures and morphological features,as well as the ability to re-slice the DICOM data according tostandardized anatomically defined planes to perform complexshape analyses. Furthermore, since inter-instrument error is neg-ligible, CT examination welcomes complex measurement capabil-ities beyond traditional linear measurements employed incraniometric and cephalometric analyses, such as areal measure-ments as demonstrated by the measurement of the anteriorfontanelle connective tissue area in this paper. Although thispaper demonstrates the utility of Geomagic Design X™ for mor-phometric analysis, the principles of the methodological processcan readily be adapted for use in similar programs, such asMimicss (Leuven, Belgium) independent of the imaging modality(MRI versus CT) used. The applications of these protocols are wide-ranging, with particular interest in morphometric analysis of
Table 1Intra-observer technical error of measurement (TEM) and relative TEM (rTEM)values from repeat measurements of maximum cranial length (mm) on ten subjectsperformed by a single observer (NL) on three evaluation days.
Subject Maximum length (mm) TEM (mm) rTEM (%)
1 2 3
1 127.17 127.18 127.13 0.02 0.022 118.92 118.28 118.54 0.32 0.273 133.01 132.81 133.00 0.11 0.084 115.03 115.28 115.42 0.16 0.145 137.41 137.56 137.48 0.06 0.046 150.68 150.02 150.15 0.35 0.237 155.47 155.74 156.05 0.24 0.158 156.19 156.21 156.21 0.01 0.019 139.64 139.84 139.65 0.09 0.07
10 166.04 166.20 166.18 0.07 0.04
Table 2Inter-observer technical error of measurement (TEM) and relative TEM (rTEM)values from measurements of maximum cranial length (mm) performed by fiveobserversa on 10 subjects.
Subject Maximum length (mm) TEM (mm) rTEM (%)
1(UG)c 2(UG)c 3(PG)d 4(PG)d 5(NA)b
1 127.37 127.16 127.13 127.25 127.03 0.13 0.102 117.71 117.92 117.35 118.19 117.63 0.31 0.273 133.37 132.94 134.15 133.23 132.86 0.51 0.394 115.01 115.25 115.25 115.21 115.10 0.10 0.095 137.24 137.41 136.08 137.91 137.23 0.67 0.496 139.85 139.64 138.75 138.97 139.37 0.45 0.337 150.85 150.27 150.97 148.13 150.32 1.15 0.778 154.33 155.75 154.31 155.31 155.63 0.69 0.459 155.97 156.2 156.17 156.31 155.87 0.17 0.11
10 166.22 166.11 165.27 165.12 166.17 0.53 0.33
a Observer experience: PG—postgraduate level of anatomy experience (410years); UG—undergraduate level of anatomy (43 years); NA—no anatomy experi-ence.
b Advanced Geomagic Designs experience (45 years).c Moderate Geomagic Designs experience (2–3 years).d No prior Geomagic Design X™ experience.
Table 3Intra/inter-observer error and inter-instrumental error. Total technical error ofmeasurement (TEM), mean relative technical error of measurement (rTEM) andcoefficient of variation (R) calculated using MSCT measurements from the precisionstudy for observer and instrumental error analysis. NOTE: For TEM values, maximumlength and breadth reported in millimeters; fontanelle area reported in millimeters2.
Total TEM TEM (Range) Mean rTEM (%) SDa R
Intra-observer:Max. length 0.19 0.01–0.35 0.11 0.15 0.992Max. breadth 0.10 0.00–0.05 0.02 0.02 0.999Fontanelle area 12.89 1.61–17.75 1.01 10.01 0.999
Inter-observer:Max. length 0.56 0.10–1.14 0.33 0.47 0.999Max. breadth 0.21 0.01–0.44 0.14 0.17 0.999Fontanelle area 12.45 0.00–22.32 1.17 13.11 0.995
Inter-instrument:Max. length 0.19 0.33–0.75 0.49 0.59 0.999Max. breadth 0.14 0.33–0.50 0.48 0.45 0.999
a SD¼mean within-subject standard deviation.
N. Lottering et al. / Journal of Forensic Radiology and Imaging 2 (2014) 34–38 37

skeletal elements for forensic investigation; clinical researchassessing temporal skeletal changes and surgical planning anddesign processes such as personalized orthopedic implants.
The Skeletal Biology and Forensic Anthropology ResearchLaboratory aims to develop contemporary population-standardsfor anthropological investigation of Australian individuals residingin Queensland. This paper introduces an objective approach formorphometric assessment of the skeleton of Australian individualsusing high-quality 3D isosurface mesh models that circumventssignificant observer error. Whilst this paper focuses on theassessment of the cranium, our research laboratory is currentlyundertaking metric anthropological analysis of MSCT 3D models ofthe post-cranial skeleton to provide standardized guidelines forimplementation in post-mortem examination in Australian mor-tuaries and pediatric clinical examination.
Ethical approval disclosure statement
Ethical approval for this research was granted by The ChildrensHealth Service District Ethics Committee (HREC/12/QRCH/208),with site-specific approval granted by The Mater Health Servicesand Royal Childrens Hospital Research Governance offices. Ethicalapproval was ratified by QUT Research Ethics Unit (Approval No.1200000716) and approved by The Queensland Governmentunder the Public Health Act (Section 284) 2005 (RD004657).
Acknowledgements
The investigators would like to acknowledge the radiographersMs. Debbie Watson and Mr. Michael Saide of the Departments ofMedical Imaging at the Royal Children's Hospital Brisbane and TheMater Health Services, Brisbane for provision of data and trainingin CT interpretation. We extend our gratitude to Dr. Lance Wilson,Biomedical Engineer of the Institute of Health Biomedical Innova-tion for his technical input.
References
[1] N. Lottering, D.M. MacGregor, M. Meredith, C.L. Alston, L.S. Gregory, Evaluationof the Suchey-Brooks method of age estimation in an Australian subpopulationusing computed tomography of the pubic symphyseal surface, Am J. Phys.Anthropol. 150 (2013) 386–399.
[2] M. Sidler, C. Jackowski, R. Dirnhofer, P. Vock, M. Thali, Use of multislicecomputed tomography in disaster victim identification—advantages and limita-tions, Forensic Sci. Int. 169 (2007) 118–128.
[3] T.H. Junger, M. Reicherts, D. Steinberger, H. Collmann, B. Kotrikova, J. Zoller,H. Howaldt, Standardized evaluation and documentation of findings in patientswith craniosynostosis, J. Cranio. Maxill. Surg. 29 (2001) 25–32.
[4] J.F. Wilbrand, M. Wilbrand, J. Pons-Kuehnemann, J.C. Blecher, P. Christophis,H.P. Howaldt, Value and reliability of anthropometric measurements of cranialdeformity in early childhood, J. Craniomaxillofac. Surg. 39 (2011) 24–29.
[5] D.E. Altobeli, R. Kikinis, J.B. Mulliken, H. Cline, W. Lorensen, F. Jolesz, et al.,Computer-assisted three-dimensional planning in craniofacial surgery, PlastReconstr. Surg. 92 (1993) 576.
[6] M.G.P. Cavalcanti, J.W. Haller, M.W. Vannier, Three-dimensional computedtomography landmark measurement in craniofacial surgical planning: experi-mental validation in vitro, J. Oral. Maxillofac. Surg. 57 (1999) 690–694.
[7] S. Aboul-Hosn Centenero, E. Hernandez-Alfaro, 3D planning in orthognathicsurgery: CAD/CAM surgical splints and prediction of the soft and hard tissuesresults—our experience in 16 cases, J. Craniomaxillofac. Surg. 40 (2012)162–168.
[8] L. Zhao, P.K. Patel, M. Cohen, Application of virtual surgical planning withcomputer assisted design and manufacturing technology to cranio-maxillofacial surgery, Arch. Plast. Surg. 39 (2012) 309–316.
[9] B.D. Foley, W.P. Thayer, A. Honeybrook, S. McKenna, S. Press, Mandibularreconstruction using computer-aided design and computer-aided manufactur-ing: an analysis of surgical results, J. Oral. Maxillofac. Surg. 71 (2013) e111–e119.
[10] N.R. Saber, J. Phillips, T. Looi, Z. Usmani, J. Burge, J. Drake, et al., Generation ofnormative pediatric skull models for use in cranial vault remodeling proce-dures, Childs. Nerv. Syst. 28 (2012) 405–410.
[11] S. Ruiz-Correa, R.W. Sze, J.R. Starr, H.J. Lin, M.L. Speltz, M.L. Cunningham, et al.,New Scaphocephaly severity indices of sagittal craniosynostosis: a compara-tive study with cranial index quantifications, Cleft Palate Craniofac. J. 43(2006) 211–221.
[12] E.J. Van Lindert, F.J. Siepel, H. Delye, A.M. Ettema, S.J. Berge, T.J.J. Maal, et al.,Validation of cephalic index measurements in scaphocephaly, Childs Nerv.Syst. 29 (2013) 1007–1014.
[13] M.G.P. Cavalcanti, M.W. Vannier, Quantitative analysis of spiral computedtomography for craniofacial clinical applications, Dentomaxillofac. Radiol. 27(1998) 344–350.
[14] M.G.P. Cavalcanti, S.S. Rocha, M.W. Vannier, Craniofacial measurements basedon 3D-CT volume rendering: implications for clinical applications, Dentomax-illofac. Rad. 33 (2004) 170–176.
[15] D.O. Kim, H.J. Kim, H. Jung, H.K. Jeong, S.I. Hong, K.D. Kim, Quantitativeevaluation of acquisition parameters in three-dimensional imaging withmultidetector computed tomography using human skull phantom, J. Digit.Imaging 15 (Suppl. 1) (2002) 254–257.
[16] J. Kragskov, C. Bosch, C. Gyldensted, S. Sindet-Pedersen, Comparison of thereliability of craniofacial anatomical landmarks based on cephalometric radio-graphs and three-dimensional CT scans, Cleft Palate Craniofac. J. 34 (1997)111–116.
[17] C. Robinson, R. Eisma, B. Morgan, A. Jeffery, E.A.M. Graham, S. Black, et al.,Anthropological measurement of lower limb and foot bones using multi-detector computed tomography, J. Forensic Sci. 53 (2008) 1289–1295.
[18] A.L. Brough, J. Bennett, B. Morgan, S. Black, G.N. Rutty, Anthropologicalmeasurement of the juvenile clavicle using multi-detector computed tomo-graphy—affirming reliability, J. Forensic Sci. 58 (2013) 946–951.
[19] Howells W.W. Cranial variation in man: a study by multi- variate analysis ofpatterns of difference among recent human populations. Peabody Museum ofArchaeology and Ethnology: Massachusetts, 1973.
[20] D. Franklin, A. Cardini, A. Flavel, A. Kuliukas, M.K. Marks, R. Hart, et al.,Concordance of traditional osteometric and volume-rendered MSCT interland-mark cranial measurements, Int. J. Legal. Med. 127 (2013) 505–520.
[21] R.L. Jantz, M. Mahfouz, N.R. Shirley, E. Abdel-Fatah, Technical Report: Improv-ing Sex Estimation from Crania using 3-Dimensional CT scans. NationalInstitute of Justice: Award No: 2008-DN-BX-K182; 2013.
[22] M.A. Verhoff, F. Ramsthaler, J. Krahahn, U. Deml, R.J. Gille, S. Grabherr, et al.,Digital forensic osteology—possibilities in cooperation with the Virtopsys
project, Forensic Sci. Int. 174 (2008) 152–156.[23] O. Ferrant, C. Rouge-Maillart, L. Guittet, F. Papin, B. Clin, G. Fau, et al., Age at
death estimation of adult males using coxal bone and CT scan: a preliminarystudy, Forensic Sci. Int. 186 (2009) 14–21.
N. Lottering et al. / Journal of Forensic Radiology and Imaging 2 (2014) 34–3838