Embed Size (px)
Citation preview
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2017
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1307
Intrasynovial flexor tendon injuriesand repair
SARA EDSFELDT
ISSN 1651-6206ISBN 978-91-554-9838-2urn:nbn:se:uu:diva-316559

Dissertation presented at Uppsala University to be publicly examined in Hedstrandsalen,Akademiska sjukhuset, Uppsala, Friday, 28 April 2017 at 13:00 for the degree of Doctor ofPhilosophy (Faculty of Medicine). The examination will be conducted in Swedish. Facultyexaminer: Lars Adolfsson (Linköping University, Department of Clinical and ExperimentalMedicine, Orthopedics).
AbstractEdsfeldt, S. 2017. Intrasynovial flexor tendon injuries and repair. Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty of Medicine 1307. 67 pp. Uppsala: ActaUniversitatis Upsaliensis. ISBN 978-91-554-9838-2.
Complications after surgical repair of intrasynovial flexor tendon injuries in the hand occurdespite advanced suture techniques and structured postoperative rehabilitation regimens. Earlycontrolled tendon mobilization prevents adhesion formations and improves tendon healing aswell as digit range of motion. To allow early postoperative rehabilitation, the strength of therepair must withstand forces created during the rehabilitation maneuvers. Improvements insuture biomechanics have increased repair strength, but up to 18 percent of repaired tendonsstill rupture. The overarching aim of this thesis was to investigate how to best treat intrasynovialflexor tendon injuries with limited risk of repair rupture, decreased adhesion formations, and toestimate the effect of individual patient and injury characteristics on functional outcome.
In two observational studies, we identified risk factors for rupture of repaired intrasynovialflexor digitorum profundus (FDP) tendons, and studied effects of these risk factors on thelong-term outcome. Age was associated with increased risk of repair rupture and impaireddigital mobility the first year after surgical repair. Concomitant flexor digitorum superficialis(FDS) transection was associated with increased risk of repair rupture without affecting digitalmobility. Concomitant nerve transection lowered the rupture risk without affecting digitalmobility.
To better understand forces generated in the flexor tendons during rehabilitation maneuvers,we measured in vivo forces in the index finger FDP and FDS tendons during rehabilitationexercises. Highest forces were measured during isolated FDP and FDS flexion for the FDP andFDS respectively. For the FDS tendon, higher forces were observed with the wrist at 30° flexioncompared to neutral position, and for the FDP tendon, forces were higher during active fingerflexion compared to place and hold.
PXL01 is a lactoferrin peptide with anti-adhesive effects previously demonstrated in animalstudies and a clinical trial to improve digital mobility when administrated around repairedtendons. We studied the mechanism of action of its corresponding rabbit peptide, rabPXL01 insodium hyaluronate (HA) in a rabbit model of flexor tendon transection and repair and used RT-qPCR to assess mRNA levels for different genes. Increased levels of PRG4 (encoding lubricin)were observed in rabPXL01 in HA treated tendons. The expression of Interleukin 1β, 6, and 8was repressed in tendon sheaths. RabPXL01 in HA might stimulate the release of lubricin anddiminish inflammation, which correspondingly reduces tendon-gliding resistance and adhesionformations during postoperative rehabilitation exercises.
The results of this thesis suggest individually adapted treatment plans, depending on repairstrength, patient and injury characteristics, as a possible way to improve outcome after flexortendon repair.
Sara Edsfeldt, Department of Surgical Sciences, Hand Surgery, Akademiska sjukhuset,Uppsala University, SE-75185 Uppsala, Sweden.
© Sara Edsfeldt 2017
ISSN 1651-6206ISBN 978-91-554-9838-2urn:nbn:se:uu:diva-316559 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-316559)

To Martin, Lea and Ellen

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Edsfeldt, S., Eklund, M., Wiig, M. Risk factors for rupture of re-paired flexor tendons in zone I and II. Submitted manuscript
II Edsfeldt, S., Eklund, M., Wiig, M. Prognostic factors for digital range of motion after intrasynovial flexor tendon injury and repair - Long-term follow-up on 311 patients treated with active extension-passive flexion with rubber bands. Submitted manuscript
III Edsfeldt, S., Rempel, D., Kursa, K., Diao, E., Lattanza, L. (2015) In vivo flexor tendon forces generated during different rehabilitation exercises. Journal of Hand Surgery European Volume, Sep;40(7):705-10
IV Edsfeldt, S., Holm, B., Mahlapuu, M., Reno, C., Hart, DA., Wiig, M. (2016) PXL01 in Sodium Hyaluronate results in increased PRG4 ex-pression: A potential mechanism for anti-adhesion. Upsala Journal of Medical Sciences, Sep 23:1-7
Reprints were made with permission from the respective publishers.

Contents
Introduction ................................................................................................... 11History of flexor tendon surgery .............................................................. 11Basic science of flexor tendons ................................................................ 12
Flexor tendon anatomy ........................................................................ 12Tendon nutrition ................................................................................... 14The healthy tendon ............................................................................... 14Tendon healing ..................................................................................... 15Molecular mechanisms during healing ................................................ 16
Treatment of flexor tendon injuries .......................................................... 19Flexor tendon repair ............................................................................. 19Flexor tendon rehabilitation ................................................................. 22Flexor tendon forces ............................................................................ 23PXL01 in HA ....................................................................................... 24
Adhesion formations and rupture of repairs ............................................. 24
Aims .............................................................................................................. 26
Material and Methods .................................................................................... 27Paper I and II: The retrospective studies .................................................. 27Paper III: Flexor tendon forces ................................................................. 30Paper IV: The rabbit model for evaluating the effect of rabPXL01 in HA on healing tendons and tendon sheaths ..................................................... 30
Surgical procedures and administration of rabPXL01 in HA .............. 30Sample collection ................................................................................. 32RNA extraction and reverse transcriptase-quantitative polymerase chain reaction (RT-qPCR) ................................................................... 32
Results ........................................................................................................... 35Paper I ....................................................................................................... 35Paper II ..................................................................................................... 36Paper III .................................................................................................... 38Paper IV .................................................................................................... 42
Discussion ..................................................................................................... 45Paper I and II ............................................................................................ 46Paper III .................................................................................................... 47Paper IV .................................................................................................... 48
Conclusion ..................................................................................................... 50
Visions to improve tendon healing ................................................................ 51Modifying the molecular mechanisms of tendon healing ........................ 51Identifying risk factors .............................................................................. 51
Sammanfattning på svenska .......................................................................... 52
Acknowledgements ....................................................................................... 55
References ..................................................................................................... 58
Abbreviations
AFF αSMA ANOVA bFGF cDNA COX-2 DNA FDP FDS FPL HA IFDP IFDS IGF-1 IL-1β IL-6 IL-8 iNOS mRNA PDGF PGE2 PH PRG4 RNA RT-qPCR TGF-β TNF-α
Active finger flexion α smooth muscle actin Analysis of variance Basic fibroblast growth factor Complementary deoxyribonucleic acid Cyclooxygenase 2 Deoxyribonucleic acid Flexor digitorum profundus Flexor digitorum superficialis Flexor pollicis longus Sodium hyaluronate Isolated flexor digitorum profundus flexion Isolated flexor digitorum superficialis flexion Insulin-like growth factor-1 Interleukin 1β Interleukin 6 Interleukin 8 Inducible nitric oxide synthase Messenger ribonucleic acid Platelet-derived growth factor Prostaglandin-E2 Place and hold Proteoglycan 4 Ribonucleic acid Reverse transcriptase-quantitative polymerase chain reaction Transforming growth factor β Tumor necrosis factor α
VEGF Vascular endothelial growth factor


11
Introduction
History of flexor tendon surgery When Sterling Bunnell wrote Surgery of the Hand, published 1944, he re-ferred to “no mans land” when describing intrasynovial primary flexor ten-don repairs by tendon grafting.1 These guidlines were challenged in 1960s by Verdan2 who advocated suture of the flexor digitorum profundus (FDP) tendon accurately with epitendinous sutures, excising the flexor digitorum superficialis (FDS) tendon, resecting the sheath and immobilizing the tendon ends to prevent tension on the suture line. This technique, primary repair by tendon-to-tendon suture was supported by Kleinert et al.,3 and Kessler and Nissim4 in the late sixties and it gained popularity. During the seventies, digit immobilization was abandoned in favor of early passive mobilization regimens, either by active extension-passive flexion protocol with rubber band to maintain the involved fingers in flexion described by Kleinert et al.,5 or by passive flexion and extension supplied by the patient, as described by Duran and Houser.6 Since then, the fields of flexor tendon surgery and treatment of intrasynovial flexor tendon injuries have produced enormous amounts of scientific research.7 Knowledge of tendon biology and the mo-lecular events during tendon healing,8-11 tendon biomechanics,12-16 mechani-cal characteristics of different repair techniques,17-22 suture materials or cali-ber has advanced tremendously.23,24 These scientific efforts have improved both surgical techniques of flexor tendon repairs and postoperative rehabili-tation exercises. However, reduced digit mobility and rupture of sutured flexor tendons still exist, and are complications that occur in 4-18% of su-tured tendons25,26 leading to social and economic consequences both for the patient and the society.25,27,28 Surprisingly, a recent report did not detect de-creasing frequency of reoperation after flexor tendon repair29 suggesting that the etiology of repair rupture is still not fully understood.
12
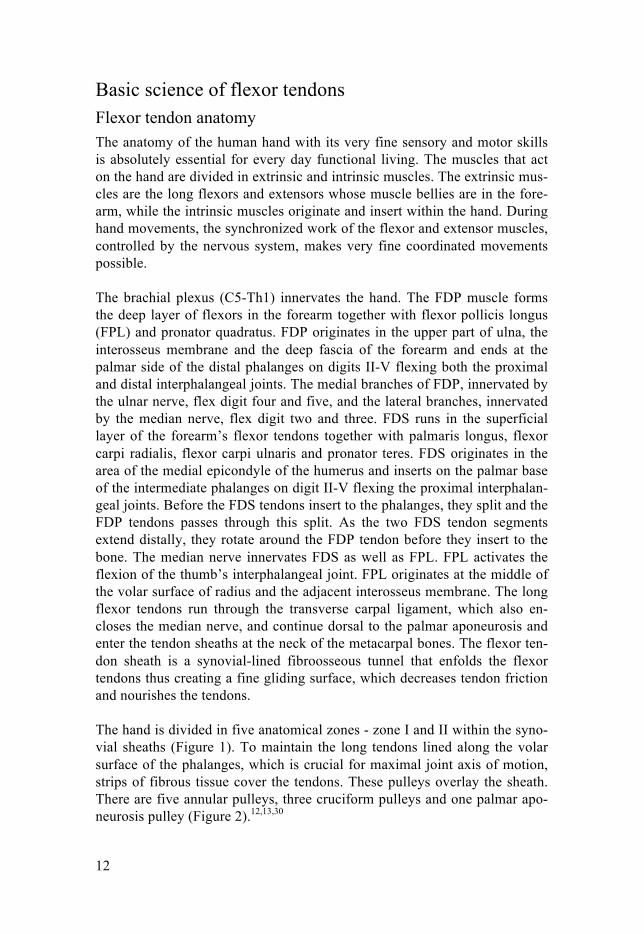
Basic science of flexor tendons Flexor tendon anatomy The anatomy of the human hand with its very fine sensory and motor skills is absolutely essential for every day functional living. The muscles that act on the hand are divided in extrinsic and intrinsic muscles. The extrinsic mus-cles are the long flexors and extensors whose muscle bellies are in the fore-arm, while the intrinsic muscles originate and insert within the hand. During hand movements, the synchronized work of the flexor and extensor muscles, controlled by the nervous system, makes very fine coordinated movements possible. The brachial plexus (C5-Th1) innervates the hand. The FDP muscle forms the deep layer of flexors in the forearm together with flexor pollicis longus (FPL) and pronator quadratus. FDP originates in the upper part of ulna, the interosseus membrane and the deep fascia of the forearm and ends at the palmar side of the distal phalanges on digits II-V flexing both the proximal and distal interphalangeal joints. The medial branches of FDP, innervated by the ulnar nerve, flex digit four and five, and the lateral branches, innervated by the median nerve, flex digit two and three. FDS runs in the superficial layer of the forearm’s flexor tendons together with palmaris longus, flexor carpi radialis, flexor carpi ulnaris and pronator teres. FDS originates in the area of the medial epicondyle of the humerus and inserts on the palmar base of the intermediate phalanges on digit II-V flexing the proximal interphalan-geal joints. Before the FDS tendons insert to the phalanges, they split and the FDP tendons passes through this split. As the two FDS tendon segments extend distally, they rotate around the FDP tendon before they insert to the bone. The median nerve innervates FDS as well as FPL. FPL activates the flexion of the thumb’s interphalangeal joint. FPL originates at the middle of the volar surface of radius and the adjacent interosseus membrane. The long flexor tendons run through the transverse carpal ligament, which also en-closes the median nerve, and continue dorsal to the palmar aponeurosis and enter the tendon sheaths at the neck of the metacarpal bones. The flexor ten-don sheath is a synovial-lined fibroosseous tunnel that enfolds the flexor tendons thus creating a fine gliding surface, which decreases tendon friction and nourishes the tendons. The hand is divided in five anatomical zones - zone I and II within the syno-vial sheaths (Figure 1). To maintain the long tendons lined along the volar surface of the phalanges, which is crucial for maximal joint axis of motion, strips of fibrous tissue cover the tendons. These pulleys overlay the sheath. There are five annular pulleys, three cruciform pulleys and one palmar apo-neurosis pulley (Figure 2).12,13,30
13
Figure 1. Hand zones (reprinted with permission from Plastic Surgery Key, plasticsurgerykey.com, access date 2017-03-01).
Figure 2. Pulleys and subdivisions of zone 1 and 2 (reprinted with permis-sion from Plastic Surgery Key, plasticsurgerykey.com, access date 2017-03-01)
14
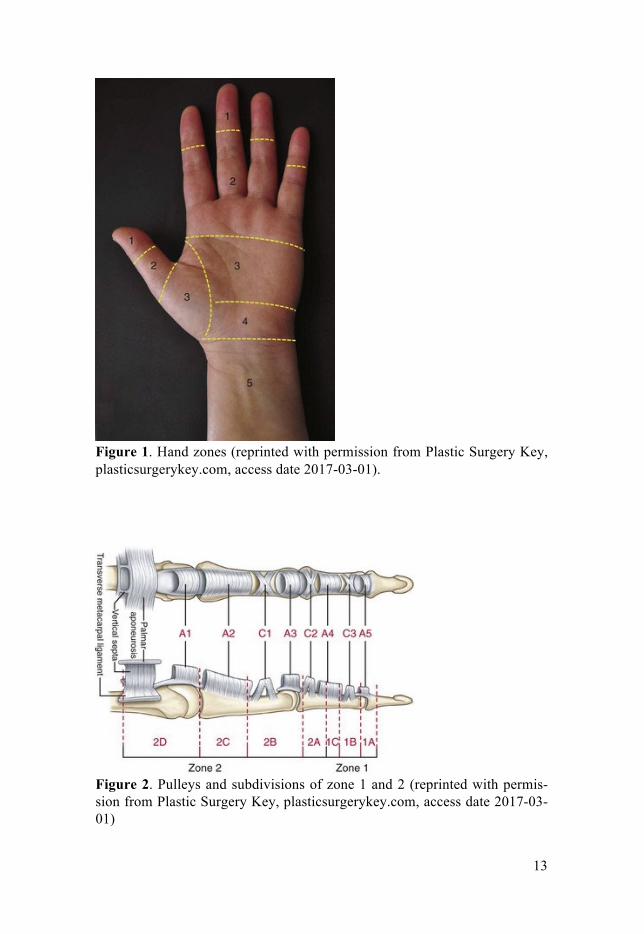
Tendon nutrition Intrasynovial flexor tendons are poorly vascularized and synovial fluid diffu-sion plays an important role in flexor tendon nutrition. Vascularity is particu-larly low on the palmar side, at the level of the proximal interphalangeal joints.31,32 Except from diffusion, the intasynovial flexor tendons depend on digital arteries, which supply vinculum brevis superficialis and vinculum longus superficialis thus nourishing the terminal portion of FDS, as well as vinculum longus profundus that supplies the dorsal side of FDP, and most distally, the vinculum brevis profundus (Figure 3).33 Figure 3. The vascular supply via vincular connections (Grey, Anatomy of the Human Body, Lea and Febiger, Philadelphia and New York)
The healthy tendon Tendon tissue contains few cells. The most predominant cell types are the tendon cells: the tenoblasts and tenocytes, representing 90-95% of the cellu-lar components. Additional cells are chondrocytes, synovial sheath cells on the tendon surface, and vascular cells in the endotenon and epitenon. The morphology and metabolic activity of the tendon cells change during aging. The tendon in the newborn has a high cell-matrix ratio and its tenoblasts have different shapes and sizes. The cell-matrix ratio decreases with aging. To compensate for decreasing cellularity, the tenoblasts transform to spider-shaped tenocytes with longer and thinner cellular processes to keep cell-to-
15
cell and cell-to-matrix contacts. Tenocytes are still metabolic active cells synthesizing matrix components, but not to the same extent as tenoblasts. Actin and myosin myofibrils activity are still preserved in the ageing teno-blasts.34,35 The tendon is predominately composed of collagen. Eighty-six percent of the dry weight is collagen, 1-5% proteoglycan, and 2% elastin. Less than 0.2% of the extracellular matrix contains inorganic components such as calcium. The extracellular matrix also contains other proteins such as glycosamino-glycans and glycoproteins, which, together with proteoglycans and elastin provide functional stability to the collagen fibers. Sixty to eighty percent of the tendon’s wet weight is water, which is believed to reduce friction. Nine-ty-five percent of the collagen in a healthy, uninjured tendon is type I. Ten-don collagen forms fibrils with intermolecular cross-links, which are essen-tial for tendon strength. A set of collagen fibrils forms a collagen fiber en-closed by the endotenon. Collagen fibers form a primary fiber bundle, and a set of primary fiber bundles forms a secondary fiber bundle, which in turn form a tertiary fiber bundle. The tertiary bundles compose the tendon en-folded by the epitenon. A synovial sheath covers the flexor tendons in the hand. The synovial sheath has a parietal and a visceral stratum, it produces synovial fluid for tendon lubrication and nutrition. Tendons outside the intra-synovial sheath zones have a peritendinous sheath called paratenon through which blood vessels enter and vascularize the endotedon and epitenon.8,34
Tendon healing A tendon injury and the following repair process cause disruptions of the fibril organization. The regions bordering both sides of the repair show thin-ner collagen fibers which, subsequently leads to a consistent loss of tensile strength.36,37 The tendon healing phases that follow injuries are: inflamma-tion, cell proliferation, and remodeling, which involve both intrinsic (prolif-eration of endotenon and epitenon tenocytes) and extrinsic (invasion of fi-broblasts and inflammatory cells from the periphery) healing mechanisms.9,38,39 During the inflammatory phase, approximately the first week after injury, the hematoma attracts aggregating platelets, which stimu-late the release of vasodilators and pro-inflammatory mediators. Erythro-cytes, platelets, macrophages and leucocytes attract and clot, engulf foreign body matter and produce cytokines. Vascular permeability increases, angio-genesis initiates, tenocytes proliferate and migrate to the wound site, and synthesis of collagen III initiates.9,40 The next phase, the proliferative phase, starts after a week. Tenocytes continue to be recruited; they proliferate and synthesize collagen III as well as proteoglycans and other extra cellular ma-trix components. The newly produced but randomly organized collagen III contributes to tissue strength. The highly cellular repair tissue, which con-

16
tains large amounts of water and extracellular matrix components, bridges the tendon gap. After approximately 6 weeks, during the remodeling phase, the production of collagen type III decreases and type I collagen synthesis increases. Cellularity and production of matrix components falls. The colla-gen becomes highly organized again into cross-linked fibrillar structures of the extra cellular matrix and tendon strength returns.8,9,40 During the inflammatory phase, the repair is as strong as the strength of the suture. The inflammation causes tissue edema, which, together with joint stiffness, damages to the gliding surfaces of the tendon and tendon sheaths or pulley, potential roughness of the repair and gap formations, increases ten-don gliding resistance and thus the forces on the repair during rehabilitation exercises.41-44 During the remodeling phase, tendon callus contributes to repair strength but the randomly organized collagen III fibers do not match the strength of a normal tendon.36,45 During this early period after surgery, a softening of the tendon tissue occurs which reduces failure strength.41 The highest risk of rupture of repair is between 2-4 weeks after surgery.46 Chang-es in repair strength over time and factors affecting the forces on the repair during rehabilitation exercises should be recognized to avoid forces that potentially exceed the strength of the repair ultimately causing gap for-mations and rupture of the repair. Though tendon strength returns during the remodeling phase, it will never gain the strength of uninjured normal tendon tissue.9,36
Molecular mechanisms during healing Several growth factors, cytokines and matrix proteins are involved in the cellular responses of activation and regulation during tendon repair9,47 and modifying the biological environment might be a future target for improving flexor tendon healing and outcomes after flexor tendon repair.48 The molecu-lar mechanisms during tendon healing is complex, and this thesis is not an attempt to cover all biological events that occur during the three stages of tendon healing, but rather a survey of the role of some of the key mediators influencing the healing process.
TGF-β – a critical growth factor Transforming growth factor β (TGF-β) is a family of cytokines with many biologic activities related to wound healing such as stimulation of collagen production and recruiting fibroblasts and macrophages.49-51 TGF-β has been found to accelerate wound healing.52 This effect can however lead to pro-gressive extracellular matrix deposition and TGF-β has shown to have a key roll in fibrosis and scar formations53 and inhibition of TGF-β reduced adhe-sion formation after flexor tendon repair in animal models.54,55

17
PRG4 – a lubrication factor Lubricin, also called Proteoglycan 4 (PRG4), is a mucinous glycoprotein encoded by the PRG4 gene. It is secreted into synovial fluid by synovial fibroblasts56 and the superficial zone cells of articular cartilage57 and menis-ci.58 Lubricin has been found on the surface of the flexor tendons59 and stud-ies have shown that lubricin reduces tendon-gliding resistance.60,61 Lubricin has also demonstrated lubricating properties on articular cartilage,62 reduc-tion of synovial cell overgrowth and protective effects on the surface of the cartilage.63 Tumor necrosis factor α (TNF-α) and interleukin 1 (IL-1) inhibit the expression of PRG4 and TGF-β stimulates the expression.59 The effect of adjuvant treatment with lubricin has been evaluated in canine models of flexor tendon repair:61,64-66 Carbodiimide derivatized hyaluronic acid (HA) and lubricin-treatment after tendon injury and repair exhibited significantly lower gliding resistance than tendons treated with HA alone61 and the gliding resistance and work of flexion of immobilized tendons were significantly improved by adjuvant treatment.64 However, two of these studies that showed positive effects on digit function also reported adverse effects on tendon healing and decreased repair strength.65,66 In another set of studies, the gliding resistance of intrasynovial flexor tendons was compared in PRG4 knockout, heterozygous and wild type mice.60 These results showed signifi-cantly higher gliding resistance in PRG4 knockout mice compared to the other groups.
Important inflammatory mediators Prolonged inflammation in the wound-healing cascade can lead to excessive adhesion formations. Inhibiting the inflammatory response might limit pro-liferation and remodeling which is believed to reduce scar formation.67 Modulating the inflammatory response after tendon injury and repair is therefore a future approach for tendon treatment.68
IL-1β has an important role in the inflammatory response. It stimulates the expression of cyclooxygenase 2 (COX-2), type 2 phospholipas A, inducible nitric oxide synthase (iNOS) and prostaglandin-E2 (PGE2) as well as in-creases the expression of adhesion molecules on mesenchymal cells and endothelial cells.69,70 In human tendon fibroblast cell cultures, IL-1β induced the matrix-degrading enzymes matrix metalloproteinases (MMPs) thus con-tributing to tendon matrix degradation. Presence of IL-1β also showed down-regulation of mRNA levels for collagen I. Taken together, IL-1β is an im-portant factor in tendon inflammation by inducing the expression and pro-duction of inflammatory mediators and matrix degradation which, is a part of normal tendon healing but also the pathogenesis of tendinopathy.71,72

18
Interleukin 6 (IL-6) is a cytokine with multiple biological functions includ-ing regulation of the immune response, hematopoiesis, the acute phase re-sponse and inflammation. Overproduction of IL-6 has been associated with various autoimmune diseases as well as cancer.73 Up-regulation of IL-6 has also been detected in tissue samples from ruptured and painful Achilles ten-dons in humans. It is therefore likely that IL-6 plays a role in both tendinopa-thy and healing of injured tendons.74,75
IL-8 is a chemotactic factor likely responsible for accumulation of neutro-phils to the site of inflammation. It is released in response to inflammatory stimuli such as IL-1, TNF.76 Tumor necrosis factor α (TNF-α) has a principal pro-inflammatory role in connective tissue posttraumatic inflammation. In response to TNF-α treat-ment, human tenocyte cell cultures reduced the type I collagen deposition, up-regulated the expression of MMPs, TNF-α, IL-1β, IL-6, and IL-10. Ex-cept from having catabolic effects on tendon healing in vitro, TNF-α in-creased elastin gene expression showing some anabolic effects on healing tendons as well.77 Cyclooxygenase 1 and 2 (Cox-1 and Cox-2) stimulate the synthesis of pros-taglandin, an important mediator in the inflammatory process. The gene for Cox-1 is expressed in many normal tissues throughout the body whereas the expression of the gene for Cox-2 is induced by pro-inflammatory mediators at the site of inflammation. Non-selective prostaglandin inhibitors have been shown to reduce adhesion formations after flexor tendon lacerations in rab-bits,78 but possible adverse effects on tendon healing have also been reported after cyclooxygenase inhibition of cultured cells from human flexor- and patellar tendons.79 The effect of selective inhibition of Cox-2 has been com-pared to effects resulting from inhibition of both Cox-1 and Cox-2. In this rabbit model, inhibition of both enzymes significantly increased range of toe motion compared to Cox-1 treated groups and placebo groups.80 Taken to-gether, treatment with prostaglandin inhibitors after tendon lacerations have shown variable effects on mechanical strength and histology81 which may be explained by the use of different substances and diverse time and mode of delivery. Inducible nitric oxide synthase (iNOS), one isoform of nitric oxide synthase, generates nitric oxide (NO). NO is involved in tendon healing: In host de-fense and by increasing blood flow. The expression of the gene for iNOS is primarily stimulated by pro-inflammatory cytokines such as TNF-α and IL-1 as well as cell products from bacteria.82 In a rat model, NO showed positive effects on collagen organization,83 and in clinical trials on humans, NO de-livered by a glyceryl trinitrate patch reduced some pain associated with

19
chronic lateral epicondylitis of the elbow84 and chronic Achilles tendinopa-thy.85
αSMA – a myofibroblast marker The myofibroblast is a type of fibroblast with specific contractile abilities necessary for wound healing. The differentiation of myofibroblasts is stimu-lated by inflammatory mediators such as TGF-β, and by mechanical stress.86 The myofibroblast’s microfilamentous apparatus contains actin and myosin, and it has been suggested that especially α smooth muscle actin (αSMA) is responsible for the contractile activity.87 Cells expressing αSMA are numer-ous in hypertrophic scars that develop after burns, and reducing αSMA lev-els might be one way to diminish scar formation.88
Treatment of flexor tendon injuries Flexor tendon repair Improving outcomes after flexor tendon repair by increasing the strength of the repair without negatively interfering with healing mechanisms and ten-don gliding is a goal for hand surgeons and basic researchers within the field. The repair must be strong enough to withstand forces during early rehabilitation exercises thus preventing gap formation and rupture, while causing minimal tissue damage.
Number of strands and suture configuration The strength of the repair depends on a number of factors such as number of strands,18,19,22,89 suture caliber,24 suture material and technique.17,20,21,23 Tre-mendous amounts of work has been performed to investigate these variables’ effect on the biomechanical characteristics of the tendon suture, thus giving surgeons many different sutures and suture techniques to choose between. The individual effect of these variables on suture strength has been studied and number of core suture strands and peripheral suture purchase were found to significantly increase repair strength compared to the other variables.90 4-strand repairs typically withstand ultimate forces of 49-85 N,18-22 and 6-strand repairs 51-76 N17,19 before repair failure, but forces up to 124 N18,21 have been observed. Increasing the number of strands to 8 or more will cre-ate a stronger repair22,89 but perhaps to the cost of impaired healing or in-creased tendon friction. Today, the recommendation is to use 4- or 6-strands for the core suture with a 3-0 or 4-0 suture.91,92 The optimal length of the suture purchase is 7-10 mm which has shown both good repair strength and low tendon gliding resistance.93,94

20
Except from number of strands and suture purchase, the holding capacity of the suture technique depends on its strength and number of anchor points in the tendon ends, as well as the knot.92 Therefore, increasing number of strands by using a double-threaded needle does not necessarily increase re-pair strength since number of anchor points does not match number of strands. Even though some studies have showed promising results using this technique,22,89 it might cause repair failure by suture pullout.17 Similarly, increasing the number of anchor points from 1 locked to 2 locked without increasing the number of strands did not increase the tensile strength of the suture configuration. For the grasping sutures however, there was a signifi-cant increase in strength when using 2 grasping anchor points.95 Pennington first described the locking suture concept; a suture configuration that tighten around the tendon fibers with tension unlike the grasping suture technique which pulls trough the fibers and distract with tension.96 Additional locking core suture concepts such as the cross- or circle locks are also in use to-day.21,97 The locking repair technique might withstand higher forces before failure, with suture rupture as the most common mode of failure,21,97 but opposite opinions have been stated believing that the locking configuration does not add much to repair strength.98 A locking suture is probably the pref-erable technique, although different locking techniques withstand different amounts of forces making choice of locking technique important.97,99
Gliding resistance versus repair strength The gliding resistance of the repair is an important factor to consider. A strong multi-strand locking core suture may cause increased friction and thereby impede tendon gliding, and though the repair is strong enough to withstand high forces during rehabilitation, its increased friction may result in adhesion formations and impaired outcomes.42,100-102 A suture configura-tion with minimal exposure of suture material on the surface of the tendon as well as placing the knot between the repaired tendon ends might minimize tendon gliding friction.42,99-101,103 The locking loop itself does not seem to interfere with gliding resistance.99,100 Placing the knot outside the repair has shown some increase in repair strength initially, but 6 weeks after surgical repair, the repairs with knots inside demonstrated significantly increased strength compared repairs with knots outside the repair site although the knot-inside suture occupied 23% of the cross-sectional area.104 Knots outside the repair is preferably placed on the lateral side since one lateral knot demonstrated lower gliding resistance than one volar knot or two knots on both sides of the tendon.105 Similar to placement of the knot, the core suture placement effects gliding resistance. Savage sutures placed volar significant-ly increased work of flexion compared to dorsal sutures, and for tendons with dorsally placed sutures, work of flexion was similar despite using dif-ferent core suture caliber whereas tendons with volar sutures increased work of flexion when suture caliber increased from 5-0 to 4-0.106

21
Choice of core suture material effects repair strength21,23 and gliding re-sistance.105,107 Braided polyester/monofilament polyethylene composite (Fi-berWire) has good mechanical properties23 and outperformed braided poly-ester coated with polybutilate (Ethibond) and nylon sutures in strength when using a locked suture configuration (Becker/Massachusetts General Hospital (MGH) repair) but not when using a grasping suture technique (Strickland repair).21 FiberWire is a low friction suture material but when this suture was used for tendon repair with a different locking core suture technique (modi-fied Pennington repair) it did not significantly affect gliding resistance or repair strength compared to the same suture technique using Ethibond.107 These differences indicate that the variability in friction between suture ma-terials is of less importance compared to the effect of suture configuration on gliding resistance.107 The poor knot-holding characteristics of FiberWire with a likely need of more than four throws might be a disadvantage in flex-or tendon surgery.100 Depending on suture technique, increasing suture caliber may increase repair strength as well as gliding resistance.24,101,105,108 However, like the great ef-fect of suture configuration on gliding resistance,107 the effect of suture con-figuration also overtook that of suture caliber especially for the grasping modified Kessler suture technique meaning that larger caliber sutures do not necessarily increase repair strength though it may increase gliding re-sistance.101
The peripheral suture The peripheral suture improves gap strength and ultimate force of the repair.109 It has been shown that the repair strength is significantly improved by increasing depth and purchase of the peripheral suture to 2 mm.90,110 The simple running peripheral suture is widely used because of its strength and simplicity91 although more complicated techniques have been developed and have demonstrated improved gap resistance and ultimate strength of the re-pair, as well as decreased gliding resistance compared to the simple running suture.111 Placing the knot inside the repair significantly reduces the gliding resistance of the simple running peripheral suture, but also some of its strength.111 To conclude, the ideal repair is a 4- or 6-strand suture configuration with locking tendon anchor points and 7-10 mm length in suture purchase but minimal exposure of suture material on tendon surface in combination with a strong suture material completed with a simple peripheral running suture with deep, wide stitches.

22
Flexor tendon rehabilitation Numerous clinical investigations and experimental studies on animals have shown that early controlled tendon mobilization after surgical repair prevent adhesion formations, improves tendon healing and digit range of motion.112,113 Many mobilization protocols are practiced today. They can be divided in three main groups: Early passive mobilization regimens with ei-ther active extension-passive flexion with rubber band to maintain the in-volved fingers in flexion described by Kleinert et al.,5 or passive flexion and extension supplied by the patient,6 place hold where the patient passively flexes the fingers and maintains them actively in flexed position114,115 and early active range of motion with the patient actively flexing the fingers.116,117 Passive mobilization protocols may have a higher risk of ten-don adhesion and loss of digit range of motion while active mobilization protocols may have a higher risk of repair rupture, but no consensus exists about the best type of motion or hand posture to use for applying force to tendons during rehabilitation.118 It might be hypothesized that a low profile suture technique with low break-ing strength and low gliding resistance, e.g. the modified Kessler repair100, may be suitable for passive mobilization regimens. Repair rupture is unlikely since low force is applied on the repair, while its low gliding resistance will assure tendon excursion during passive mobilization. In contrast, a high pro-file suture technique with high breaking strength and high gliding resistance, such as the augmented Becker/Massachusetts General Hospital (MGH)100 repair, may not allow smooth tendon excursion and are perhaps better suited for active motion protocols where higher loads are applied on the tendon. The increased strength of the repair will still hold tendon ends during reha-bilitation exercises. Methods of evaluating outcome There are many different systems of evaluating outcomes after flexor tendon repair, of which three have gained popularity: Strickland and Glogovac crite-ria,112 the TAM method, advised by the American Society for Surgery of the Hand, and the Buck-Gramcko method.119 Only fingers with the same total range of active motion (MCP, PIP and DIP joints) as the contralateral hand are rated as excellent in the TAM method, whereas in the Strickland and Glogovac criteria, an excellent score requires sufficient range of motion (PIP and DIP joints) for functionally excellent results but not necessarily the same as the contralateral finger. Tendon healing and restoration of collagen fibers continues for months8,9,40 and the final outcome after flexor tendon repairs should not be evaluated earlier than 3 months after surgery,25 however full activity might be allowed earlier.120
23
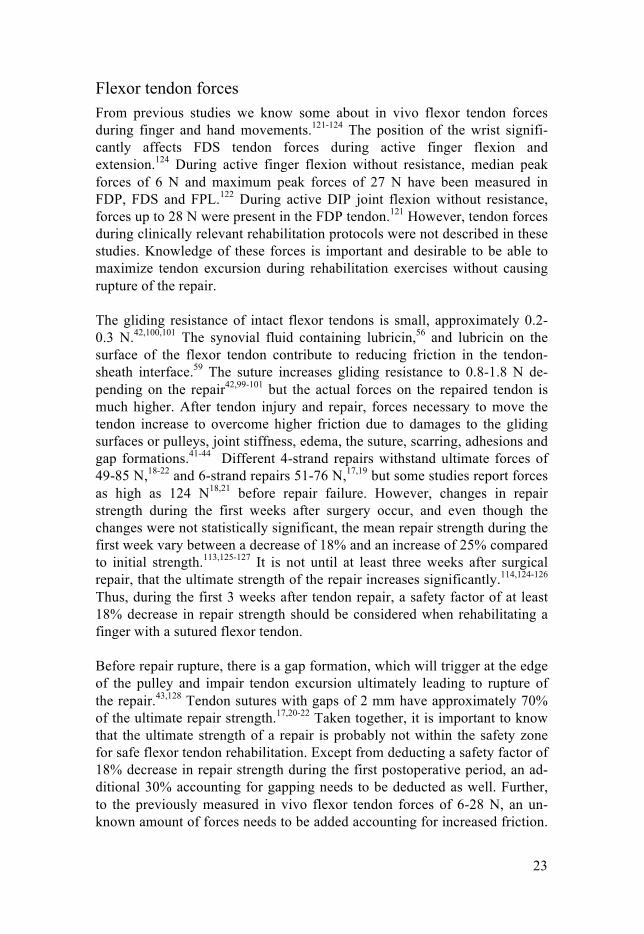
Flexor tendon forces From previous studies we know some about in vivo flexor tendon forces during finger and hand movements.121-124 The position of the wrist signifi-cantly affects FDS tendon forces during active finger flexion and extension.124 During active finger flexion without resistance, median peak forces of 6 N and maximum peak forces of 27 N have been measured in FDP, FDS and FPL.122 During active DIP joint flexion without resistance, forces up to 28 N were present in the FDP tendon.121 However, tendon forces during clinically relevant rehabilitation protocols were not described in these studies. Knowledge of these forces is important and desirable to be able to maximize tendon excursion during rehabilitation exercises without causing rupture of the repair. The gliding resistance of intact flexor tendons is small, approximately 0.2-0.3 N.42,100,101 The synovial fluid containing lubricin,56 and lubricin on the surface of the flexor tendon contribute to reducing friction in the tendon-sheath interface.59 The suture increases gliding resistance to 0.8-1.8 N de-pending on the repair42,99-101 but the actual forces on the repaired tendon is much higher. After tendon injury and repair, forces necessary to move the tendon increase to overcome higher friction due to damages to the gliding surfaces or pulleys, joint stiffness, edema, the suture, scarring, adhesions and gap formations.41-44 Different 4-strand repairs withstand ultimate forces of 49-85 N,18-22 and 6-strand repairs 51-76 N,17,19 but some studies report forces as high as 124 N18,21 before repair failure. However, changes in repair strength during the first weeks after surgery occur, and even though the changes were not statistically significant, the mean repair strength during the first week vary between a decrease of 18% and an increase of 25% compared to initial strength.113,125-127 It is not until at least three weeks after surgical repair, that the ultimate strength of the repair increases significantly.114,124-126
Thus, during the first 3 weeks after tendon repair, a safety factor of at least 18% decrease in repair strength should be considered when rehabilitating a finger with a sutured flexor tendon. Before repair rupture, there is a gap formation, which will trigger at the edge of the pulley and impair tendon excursion ultimately leading to rupture of the repair.43,128 Tendon sutures with gaps of 2 mm have approximately 70% of the ultimate repair strength.17,20-22 Taken together, it is important to know that the ultimate strength of a repair is probably not within the safety zone for safe flexor tendon rehabilitation. Except from deducting a safety factor of 18% decrease in repair strength during the first postoperative period, an ad-ditional 30% accounting for gapping needs to be deducted as well. Further, to the previously measured in vivo flexor tendon forces of 6-28 N, an un-known amount of forces needs to be added accounting for increased friction.
24
Considering this, a repair withstanding forces of 49-85 N does not seem excessively strong.
PXL01 in HA PXL01 is a synthetic peptide derived from human lactoferrin. Previous in vitro studies with human cell lines showed PXL01 to exhibit an inhibitory effect on some important hallmarks of adhesion formation by reducing se-cretion of inflammatory cytokines, promoting fibrinolysis and reducing in-fections.129 Adjuvant treatment with PXL01 with HA as a carrier exhibited reduced adhesion formations in experimental models of abdominal surgery in rats129 and flexor tendon repair surgery in rabbits.130,131 A recent clinical trial investigating the value of adjuvant treatment with PXL01 in HA after flexor tendon injury and repair in the hand, showed significantly increased digit mobility in PXL01 in HA treated fingers compared to placebo.132 We used the corresponding peptide derived from the rabbit lactoferrin, rabPXL01 in HA, in a rabbit model of tendon injury and repair. By using the homologous peptide, we aimed for a more appropriate evaluation of the po-tential mechanisms of action of the PXL01 peptide.
Adhesion formations and rupture of repairs Peritendinous adhesions and repair rupture are troublesome complications. The formation of peritendinous adhesions, when surrounding tissue attach to the tendon surface during healing, is a complication of the intrinsic and ex-trinsic healing mechanisms that occur during tendon healing.11 The extent of adhesion formations depends on a number of factors. One important factor is the amount of trauma the tendon and tendon sheath suffer from during the initial injury or surgery.133 In addition, factors such as suture technique42,100-
102 and suture material105,107,111 effect gliding resistance and subsequently the formation of peritendinous adhesions.102 Early controlled tendon mobiliza-tion will prevent adhesion formation and improve digit range of motion112,113 but on the other hand, excessive stress on the suture can cause gap for-mations. Tendon gap of more than 3 mm is associated with increased rupture risk and adhesion formations, which ultimately leads to impaired outcomes after flexor tendon repair.43,128 By adding a slight tension to the core suture, proximately 10%, gap formations might be prevented.134 Limiting the forces on the tendon during postoperative rehabilitation exercises enough to induce tendon excursion but without causing gap formation will further reduce the risk of repair rupture. The aetiology of repair ruptures is not fully understood. A rupture rate of 4-18%25,26 world wide and a trend where the incidence of complications (re-

25
operation, repair rupture and adhesions) is not clearly improving135 might raise the question if further investigations on suture technique, suture materi-al and rehabilitation regimens will reduce the incidence of reoperation and impaired digit motion. It is well known that flexor tendons must be treated delicately during surgery, sutured with a fine surgical technique, and mobi-lized postoperatively using an adequate regimen. However, it is also interest-ing to speculate in what effects population and patient based factors may have on the outcome after intrasynovial flexor tendon repairs. These ques-tions have been raised before. In retrospective case series, Dy et al.29 showed that increasing age and worker’s compensation health care were associated with a higher risk of reoperation. Moriya et al., 2014136 and Rigo et al., 2016137 identified negative correlations between digital mobility and patient age. Rigo et al., 2016137 also found smoking and delayed surgery to be nega-tive predictors of digital mobility. Population and patient based research could deepen the understanding of the etiology of repair rupture and im-paired digit range of motion.135 This knowledge might make it possible to identify patients with high risks of repair rupture and impaired digit range of motion, ultimately individualizing treatment and rehabilitation and thereby improving the outcome of flexor tendon injuries. Depending on risk factors, the initial injury and the repair, surgical technique and postoperative reha-bilitation protocols may be individualized. Possibilities to modify and reinforce the surgical technique are well docu-mented,91,92 but the actual tendon forces that are created during different rehabilitation exercises are less investigated making scientifically verified rehabilitation modifications difficult and speculative. Knowledge of in vivo forces in FDP and FDS during commonly used rehabilitation exercises, and by comparing these forces to the strength of a standard repair, rehabilitation exercises can be individually adapted to ensure that the forces on the repair stay within the safety zone. For some patients, for example patients with high risks of repair rupture and adhesion formations or patients unable to participate in early motion therapy due to multiple injuries or other medical conditions, adjuvant treatment of the gliding surfaces of the tendon might be a future possibility to reduce friction in the tendon-sheath interface.61 Lubri-cation of the tendon surface might allow for a delayed rehabilitation after flexor tendon surgery,64 or reduce the risk of repair rupture and adhesion formations in high-risk individuals. By tailoring the treatment individually, the risk of repair rupture and adhesion formations might be minimized thus reducing the need of reoperation and improving digit range of motion.
26
Aims
The general aims of this thesis were to: Investigate patient factors that possi-bly interfere with tendon healing and the outcome after flexor tendon repair; To find a basis for creating recommendations for safe rehabilitation with limited risk of repair rupture by measuring FDP and FDS tendons forces during commonly used rehabilitation maneuvers and compare them to the reported strength of a flexor tendon repair; To investigate the anti-adhesive mechanisms of the lactoferrin peptide PXL01 in HA by using its correspond-ing rabbit lactoferrin peptide, rabPXL01 in HA, in a rabbit model of healing tendons and tendon sheaths.
The specific aims were to: • Identify patient based factors and concomitant injuries affecting
the risk of rupture of repair after FDP tendon injury and repair inzone I and II
• Describe digital range of motion after FDP tendon injury and re-pair in zone I and II
• Estimate the effect of the previously identified risk factors for re-pair rupture: a concomitant nerve transection, the combination ofFDP and FDS tendon transection, and increasing age, on the long-term outcome after FDP tendon transection and repair in zone Iand II
• Measure in vivo forces generated in the FDP and FDS tendonsduring commonly used rehabilitation maneuvers
• Describe the relationship between forces during commonly usedmaneuvers at varying wrist positions and to compare them to thereported strength of a flexor tendon repair
• Find possible mechanisms behind the anti-adhesive effects of therabbit lactoferrin peptide rabPXL01 in HA on healing tendons andtendon sheaths by assessing mRNA levels for lubricin and a sub-set of relevant molecules involved in the outcome after rabbitflexor tendon repair

27
Material and Methods
Paper I and II: The retrospective studies The two patient and population based studies are the result of observational analyses of 404 patients with 443 acute FDP or FPL tendon injuries in zone I and II (digits I-V). All patients were treated at the Department of Hand Sur-gery, Uppsala University Hospital between 2000-2006. In both studies, we excluded thumb injuries, patients with partial FDP tendon injuries, patients treated with tendon reinsertion to distal phalangeal bone and patients who could not attend physician or physiotherapist appointments due to illness or death. In the first paper, we also excluded patients younger than 18 years old. In the second paper, we also excluded patients immobilized in plaster splint or mobilized using any other protocol than the Kleinert’s rehabilitation protocol5 modified by Silfverskiöld and May114 (hereafter referred to simply as Kleinert). Follow-up time was at least 1 year. Finger mobility was controlled 2, 3, 6, 12 and 24 months postoperatively by physiotherapists trained in hand physio-therapy. Patient based data (e.g. age, sex etc.), suture technique and number of strands, rehabilitation regime (Kleinert, place and hold or orthosis (immo-bilized 4 weeks from below the elbow to fingertips, with the wrist in neutral position, the metacarpophalangeal joint in 90 degrees of flexion, and the interphalangeal joints straight)) as well as pre- and postoperative complica-tions (concomitant nerve transection and combined FDP and FDS tendon transection) were collected from each patient’s medical record (Table 1). The Central Ethical Review Board in Uppsala approved the studies.
28
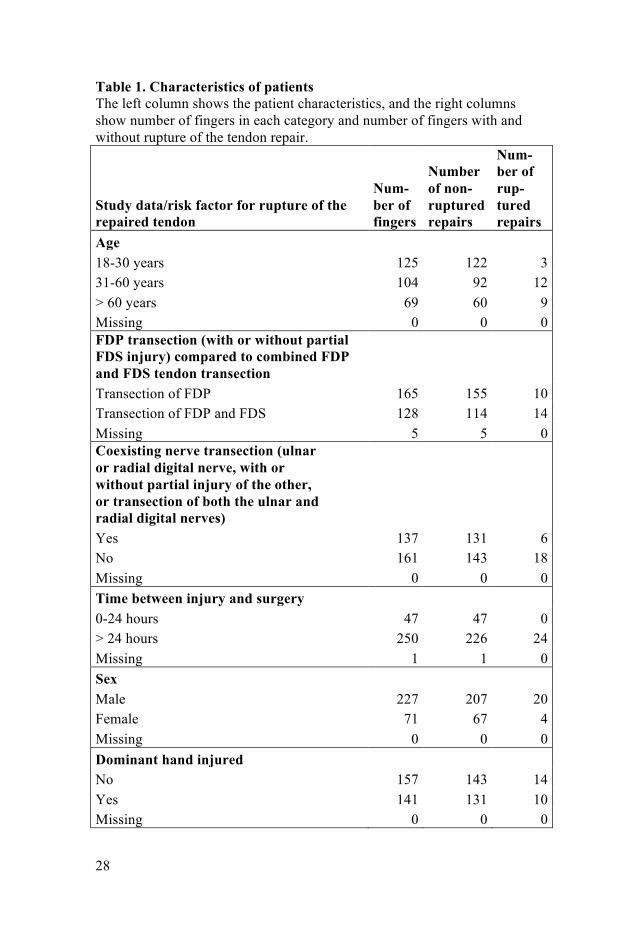
Table 1. Characteristics of patients The left column shows the patient characteristics, and the right columns show number of fingers in each category and number of fingers with and without rupture of the tendon repair.
Study data/risk factor for rupture of the repaired tendon
Num-ber of fingers
Number of non-ruptured repairs
Num-ber of rup-tured repairs
Age 18-30 years 125 122 3
31-60 years 104 92 12 > 60 years 69 60 9 Missing 0 0 0 FDP transection (with or without partial FDS injury) compared to combined FDP and FDS tendon transection
Transection of FDP 165 155 10 Transection of FDP and FDS 128 114 14 Missing 5 5 0 Coexisting nerve transection (ulnar or radial digital nerve, with or without partial injury of the other, or transection of both the ulnar and radial digital nerves)
Yes 137 131 6 No 161 143 18 Missing 0 0 0 Time between injury and surgery
0-24 hours 47 47 0 > 24 hours 250 226 24 Missing 1 1 0 Sex
Male 227 207 20 Female 71 67 4 Missing 0 0 0 Dominant hand injured
No 157 143 14 Yes 141 131 10 Missing 0 0 0
29
Core suture technique Modified Kessler 207 187 20
Tsuge 70 68 2 Mattress 21 19 2 Missing 0 0 0 Postoperative rehabilitation regime
Kleinert 255 238 17 Orthosis (immobilized 4 weeks) 29 22 7 Place and hold 13 13 0 Missing 1 1 0 Number of core suture strands
Two 210 190 20 Four 88 84 4 Missing 0 0 0 In the first paper, we included 267 patients with 298 injured fingers (age >18 years, mean 37 years, 24% women, 76% men). All tendons were sutured tendon-to-tendon using core and epitendinous sutures. We analyzed data using multivariable conditional logistic regression with FDP tendon repair rupture confirmed by clinical observation as a binary study endpoint, and computed odds ratio for each risk factor. In order to control for possibly correlated outcomes within the same patient, fingers belonging to the same patient were regarded as strata in the conditional logistic model. All p-values were two-sided. P < 0.05 was considered significant. In the second paper, we evaluated digital range of motion on 273 patients with a total of 311 treated fingers using Strickland’s evaluation system. Hy-perextension was equal to 0 degrees. All patients were postoperatively treat-ed with active extension-passive flexion with rubber bands to maintain the involved fingers in flexion (Kleinert).5 We described digital range of motion for the patient cohort. To evaluate the long-term effects of the identified risk factors in Paper I on digital mobility, we categorized patients into 3 groups: 0-25 years, 26-50 years, and more than 50 years old. We also identified pa-tients with coexisting nerve transection and patients with transection of both the FDP and the FDS tendons and their digital range of motion were com-pared to patients with intact or partially injured nerves or FDS tendon. In this study we used chi square tests to test for differences in outcomes in different groups (age groups, coexisting nerve transection, and patients with transec-tion of both the FDP and the FDS tendons). Missing data was handled using a missing completely at random (MCAR) assumption. To investigate if this assumption was reasonable (we did not know if there was a pattern in at-

30
tendance of physiotherapist appointments), we used logistic regression to test whether Strickland score at previous appointment were associated with attending a given physiotherapy appointment. P < 0.05 was considered sig-nificant.
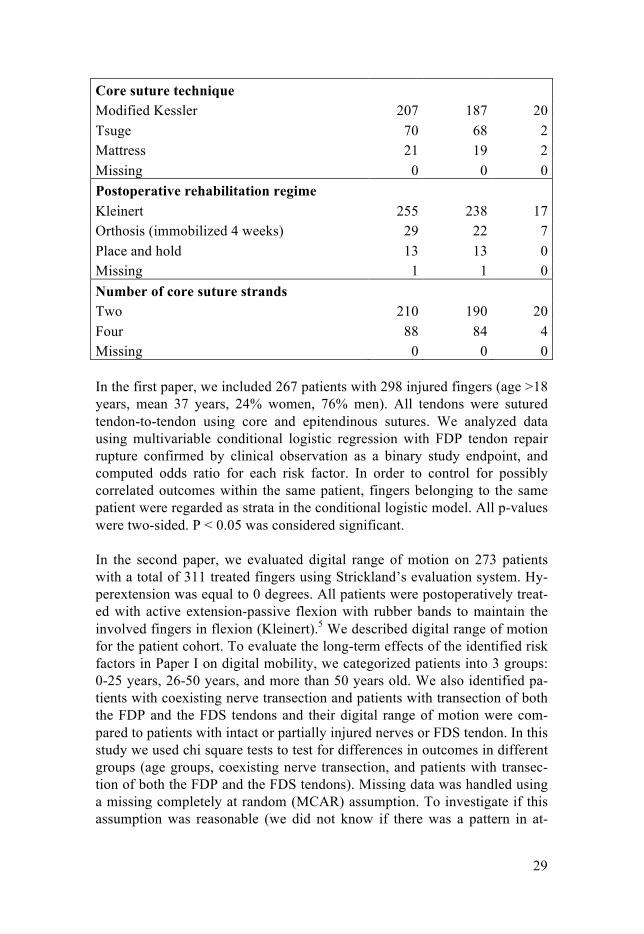
Paper III: Flexor tendon forces We used a buckle force transducer (Figure 4) to measure in vivo flexor ten-don forces during commonly used rehabilitation maneuvers. We placed the transducer on the FDP and FDS tendons of the index finger in the carpal canal during open carpal tunnel release of 12 patients. Each patient per-formed four different rehabilitation maneuvers (place and hold, active com-posite finger flexion, isolated FDP flexion, isolated FDS flexion) with the wrist in neutral position (0° flexion) and in 30° flexion, as well as tenodesis. Force data was collected via 4 silicon strain gauges connected to a computer. We obtained peak tendon forces for each maneuver by recording the maneu-vers on video and synchronizing the force data with the video. Peak tendon forces for the different maneuvers were compared and significant differences identified by a two factor repeated measures analysis of variance (ANOVA). To test for differences of individual factor levels, we used Tukey’s follow-up test. Tenodesis was not included in the statistical analysis because it could not be assigned a wrist posture. We compared peak tendon forces with the reported strength of a 4-and 6-strand standard flexor tendon repair. In order to select appropriate studies to compare with, we searched in PubMed and selected appropriate studies based on relevance, publication date, and study design. P < 0.05 was considered significant.
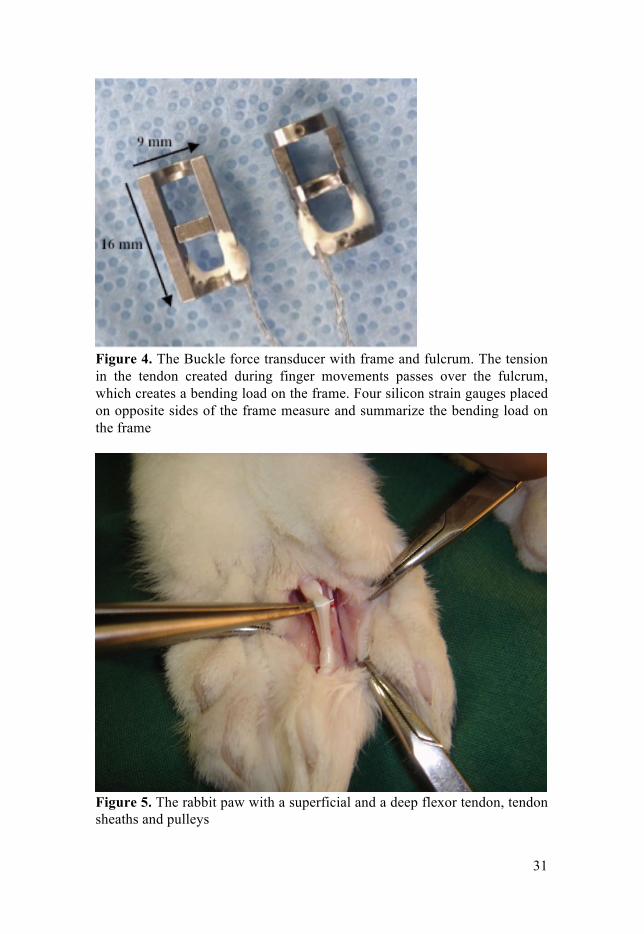
Paper IV: The rabbit model for evaluating the effect of rabPXL01 in HA on healing tendons and tendon sheaths Surgical procedures and administration of rabPXL01 in HA The rabbit model is a well-proven model that is designed to mimic deep flexor tendon injury and repair in humans. The rabbit paw is similar to the human hand: it has a superficial and a deep flexor tendon, tendon sheaths and pulleys (Figure 5). To imitate rehabilitation regime used in clinical prac-tice, the rabbit flexor tendons were partially divided at the muscle-tendon transition to decrease the tensile load on the flexor tendon’s phalangeal sec-tion. This allowed for partially unloaded flexion of the rabbit digits, which imitate unloaded active rehabilitation used in clinical practice today.
31
Figure 4. The Buckle force transducer with frame and fulcrum. The tension in the tendon created during finger movements passes over the fulcrum, which creates a bending load on the frame. Four silicon strain gauges placed on opposite sides of the frame measure and summarize the bending load on the frame
Figure 5. The rabbit paw with a superficial and a deep flexor tendon, tendon sheaths and pulleys

32
We performed the surgical procedures on 24 female young adult New Zea-land White rabbits weighing 3 kg (±0.3 kg) under sterile conditions during anesthesia with fentanyl-fluanisone (0.3 ml/kg body weight; Hypnorm, Janssen, Beerse, Belgium) and midazolam (2mg/kg body weight; Dormicum, Roche, Basel, Switzerland). The rabbits were given a prophylactic dose of cefuroxime (100 mg; Zinacef, GlaxoSmithKline, London, United Kingdom) intravenously before surgery. We incised the third digit longitudinally and opened the flexor tendon sheath approximately 10 mm between the first and second annular pulley before resecting the superficial flexor tendon and transversely dividing the intermediate segment of the deep flexor tendon. We sutured the tendon ends with Kessler core sutures (5-0 Prolene, Ethicon, Sollentuna, Sweden) and simple running sutures in the epitenon (6-0, PDS, Ethicon). The paws of the rabbits were randomized to either receive rabPXL01 in HA treatment (20 mg/ml rabPXL01 in 1.5% HA) or to be left untreated (paired control). We administrated rabPXL01 in HA locally around the repaired tendons randomized to receive adjuvant treatment by inserting a 24GA catheter into the opening of the tendon sheath, and left it within the tendon sheath as the tendon sheath was closed with a running 6-0 PDS suture (Ethicon). We injected the rabPXL01 in HA formula (0.3 ml) when performing the final sutures. The same procedure was done in the un-treated paw but without injecting rabPXL01 in HA formula. We closed the skin with a running suture (5-0 Ethilon, Ethicon).
Sample collection We harvested equally sized segments of tendons and tendon sheaths (4 mm proximal and 4 mm distal of the repair site) 1, 3 and 6 days after surgery. The rabbits were sedated with midazolam (Dormicum, Roche) and eu-thanized by a lethal dose of Pentobarbitalnatrium (Apoteket, Uppsala, Swe-den). We rinsed the samples in physiological saline and cleaned them from sutures, put them into tared cryovials which we immediately placed in liquid nitrogen and stored at -80°C until further analysis.
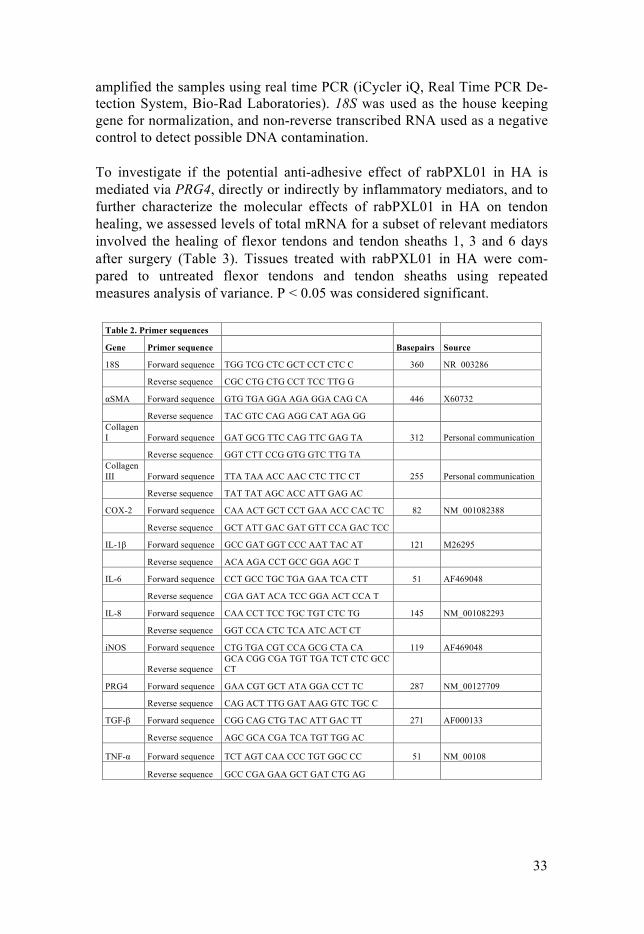
RNA extraction and reverse transcriptase-quantitative polymerase chain reaction (RT-qPCR) We extracted RNA from the tissue samples using the TRIspin method.138 We eluted the RNA using an RNeasy Total RNA Kit (Qiagen, Chatsworth, Cali-fornia, USA) and quantified the RNA fluorometrically with Sybrgreen (Mandel, Guelph, Ontario, Canada). We processed the RNA for reverse tran-scription to cDNA using a Qiagen Omniscript kit (Omniscript RT Kit, Qi-agen, Mississauga, Ontario, Canada). The cDNA was prepared for qPCR using IQ SYBR Green Supermix (Bio-Rad Laboratories Mississauga, Cana-da). We added primers previously utilized for rabbit tissues (Table 2) and
33
amplified the samples using real time PCR (iCycler iQ, Real Time PCR De-tection System, Bio-Rad Laboratories). 18S was used as the house keeping gene for normalization, and non-reverse transcribed RNA used as a negative control to detect possible DNA contamination.
To investigate if the potential anti-adhesive effect of rabPXL01 in HA is mediated via PRG4, directly or indirectly by inflammatory mediators, and to further characterize the molecular effects of rabPXL01 in HA on tendon healing, we assessed levels of total mRNA for a subset of relevant mediators involved the healing of flexor tendons and tendon sheaths 1, 3 and 6 days after surgery (Table 3). Tissues treated with rabPXL01 in HA were com-pared to untreated flexor tendons and tendon sheaths using repeated measures analysis of variance. P < 0.05 was considered significant.
Table 2. Primer sequences
Gene Primer sequence Basepairs Source
18S Forward sequence TGG TCG CTC GCT CCT CTC C 360 NR_003286
Reverse sequence CGC CTG CTG CCT TCC TTG G
!SMA Forward sequence GTG TGA GGA AGA GGA CAG CA 446 X60732
Reverse sequence TAC GTC CAG AGG CAT AGA GG Collagen I Forward sequence GAT GCG TTC CAG TTC GAG TA 312 Personal communication
Reverse sequence GGT CTT CCG GTG GTC TTG TA Collagen III Forward sequence TTA TAA ACC AAC CTC TTC CT 255 Personal communication
Reverse sequence TAT TAT AGC ACC ATT GAG AC
COX-2 Forward sequence CAA ACT GCT CCT GAA ACC CAC TC 82 NM_001082388
Reverse sequence GCT ATT GAC GAT GTT CCA GAC TCC
IL-1" Forward sequence GCC GAT GGT CCC AAT TAC AT 121 M26295
Reverse sequence ACA AGA CCT GCC GGA AGC T
IL-6 Forward sequence CCT GCC TGC TGA GAA TCA CTT 51 AF469048
Reverse sequence CGA GAT ACA TCC GGA ACT CCA T
IL-8 Forward sequence CAA CCT TCC TGC TGT CTC TG 145 NM_001082293
Reverse sequence GGT CCA CTC TCA ATC ACT CT
iNOS Forward sequence CTG TGA CGT CCA GCG CTA CA 119 AF469048
Reverse sequence GCA CGG CGA TGT TGA TCT CTC GCC CT
PRG4 Forward sequence GAA CGT GCT ATA GGA CCT TC 287 NM_00127709
Reverse sequence CAG ACT TTG GAT AAG GTC TGC C
TGF-" Forward sequence CGG CAG CTG TAC ATT GAC TT 271 AF000133
Reverse sequence AGC GCA CGA TCA TGT TGG AC
TNF-! Forward sequence TCT AGT CAA CCC TGT GGC CC 51 NM_00108
Reverse sequence GCC CGA GAA GCT GAT CTG AG
34
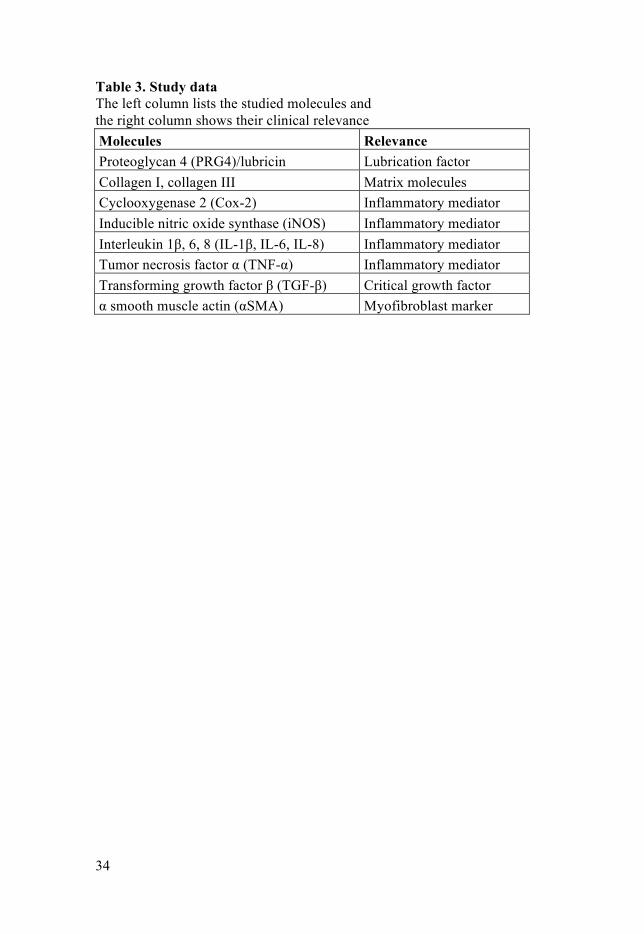
Table 3. Study data The left column lists the studied molecules and the right column shows their clinical relevance Molecules Relevance Proteoglycan 4 (PRG4)/lubricin Lubrication factor Collagen I, collagen III Matrix molecules Cyclooxygenase 2 (Cox-2) Inflammatory mediator Inducible nitric oxide synthase (iNOS) Inflammatory mediator Interleukin 1β, 6, 8 (IL-1β, IL-6, IL-8) Inflammatory mediator Tumor necrosis factor α (TNF-α) Inflammatory mediator Transforming growth factor β (TGF-β) Critical growth factor α smooth muscle actin (αSMA) Myofibroblast marker
35
Results
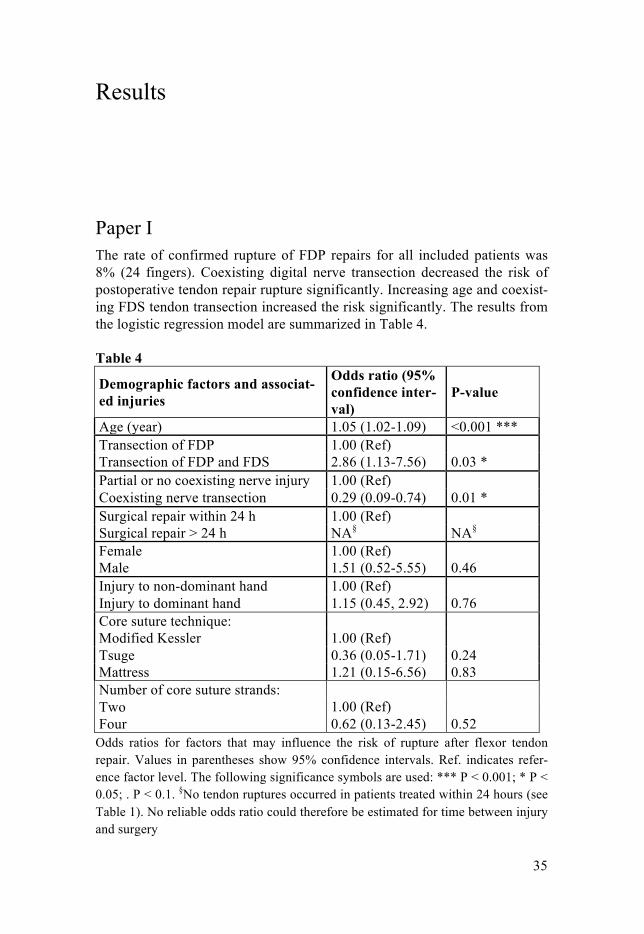
Paper I The rate of confirmed rupture of FDP repairs for all included patients was 8% (24 fingers). Coexisting digital nerve transection decreased the risk of postoperative tendon repair rupture significantly. Increasing age and coexist-ing FDS tendon transection increased the risk significantly. The results from the logistic regression model are summarized in Table 4. Table 4
Demographic factors and associat-ed injuries
Odds ratio (95% confidence inter-val)
P-value
Age (year) 1.05 (1.02-1.09) <0.001 *** Transection of FDP 1.00 (Ref) Transection of FDP and FDS 2.86 (1.13-7.56) 0.03 * Partial or no coexisting nerve injury 1.00 (Ref) Coexisting nerve transection 0.29 (0.09-0.74) 0.01 * Surgical repair within 24 h 1.00 (Ref) Surgical repair > 24 h NA§ NA§ Female 1.00 (Ref) Male 1.51 (0.52-5.55) 0.46 Injury to non-dominant hand 1.00 (Ref) Injury to dominant hand 1.15 (0.45, 2.92) 0.76 Core suture technique: Modified Kessler 1.00 (Ref) Tsuge 0.36 (0.05-1.71) 0.24 Mattress 1.21 (0.15-6.56) 0.83 Number of core suture strands: Two 1.00 (Ref) Four 0.62 (0.13-2.45) 0.52
Odds ratios for factors that may influence the risk of rupture after flexor tendon repair. Values in parentheses show 95% confidence intervals. Ref. indicates refer-ence factor level. The following significance symbols are used: *** P < 0.001; * P < 0.05; . P < 0.1. §No tendon ruptures occurred in patients treated within 24 hours (see Table 1). No reliable odds ratio could therefore be estimated for time between injury and surgery
36
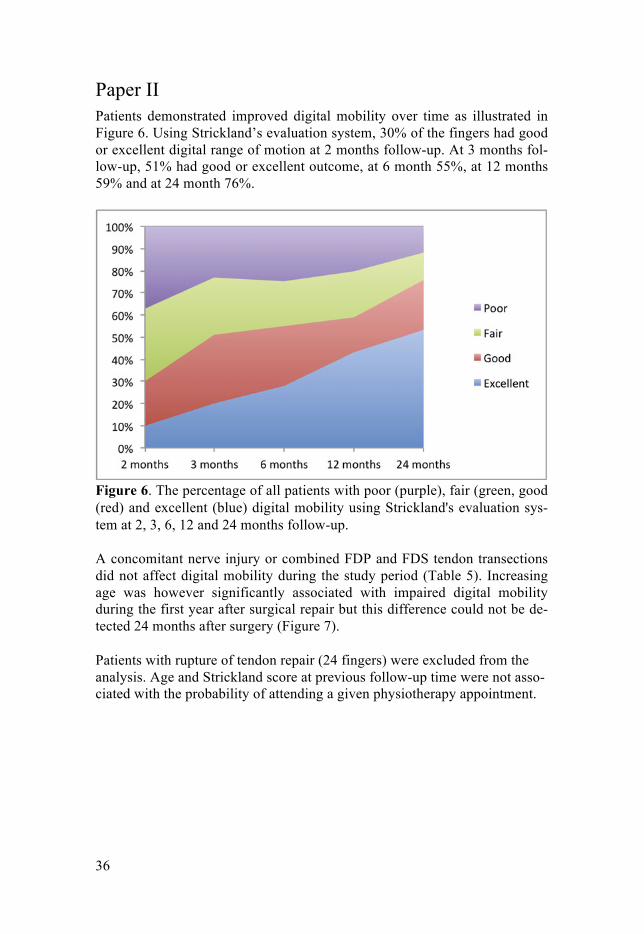
Paper II Patients demonstrated improved digital mobility over time as illustrated in Figure 6. Using Strickland’s evaluation system, 30% of the fingers had good or excellent digital range of motion at 2 months follow-up. At 3 months fol-low-up, 51% had good or excellent outcome, at 6 month 55%, at 12 months 59% and at 24 month 76%.
Figure 6. The percentage of all patients with poor (purple), fair (green, good (red) and excellent (blue) digital mobility using Strickland's evaluation sys-tem at 2, 3, 6, 12 and 24 months follow-up.
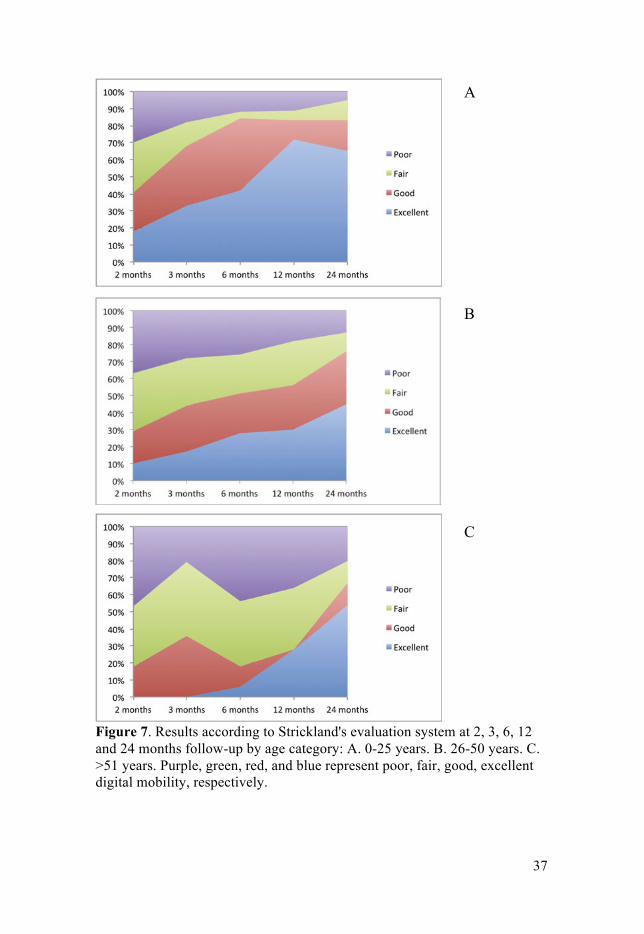
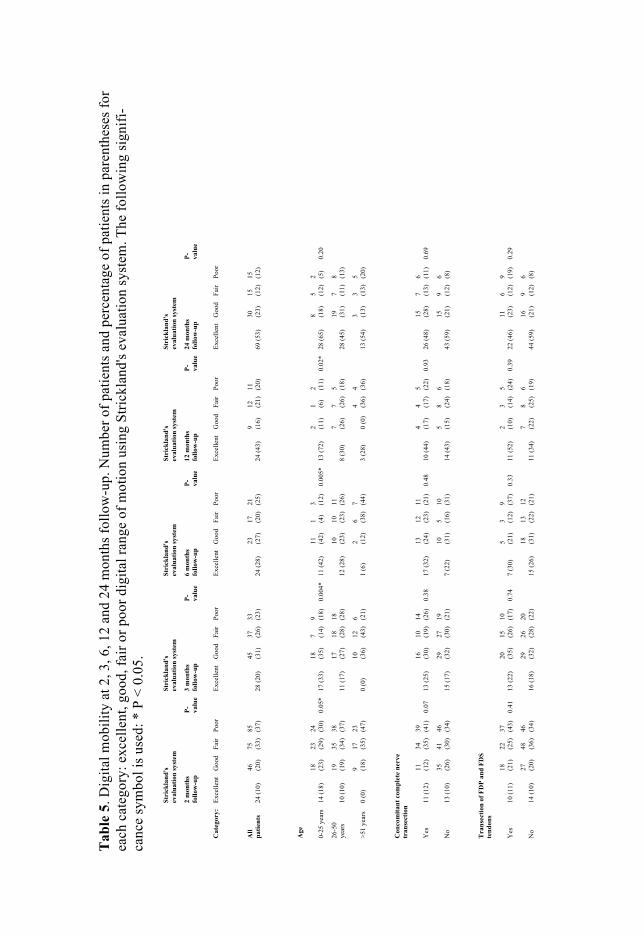
A concomitant nerve injury or combined FDP and FDS tendon transections did not affect digital mobility during the study period (Table 5). Increasing age was however significantly associated with impaired digital mobility during the first year after surgical repair but this difference could not be de-tected 24 months after surgery (Figure 7).
Patients with rupture of tendon repair (24 fingers) were excluded from the analysis. Age and Strickland score at previous follow-up time were not asso-ciated with the probability of attending a given physiotherapy appointment.
37
Figure 7. Results according to Strickland's evaluation system at 2, 3, 6, 12 and 24 months follow-up by age category: A. 0-25 years. B. 26-50 years. C. >51 years. Purple, green, red, and blue represent poor, fair, good, excellentdigital mobility, respectively.
A
B
C
Tab
le 5
. Dig
ital m
obili
ty a
t 2, 3
, 6, 1
2 an
d 24
mon
ths f
ollo
w-u
p. N
umbe
r of p
atie
nts a
nd p
erce
ntag
e of
pat
ient
s in
pare
nthe
ses f
or
each
cat
egor
y: e
xcel
lent
, goo
d, fa
ir or
poo
r dig
ital r
ange
of m
otio
n us
ing
Stric
klan
d's e
valu
atio
n sy
stem
. The
follo
win
g si
gnifi
-ca
nce
sym
bol i
s use
d: *
P <
0.0
5.
Stri
ckla
nd's
ev
alua
tion
syst
em
Stri
ckla
nd's
ev
alua
tion
syst
em
Stri
ckla
nd's
ev
alua
tion
syst
em
Stri
ckla
nd's
ev
alua
tion
syst
em
Stri
ckla
nd's
ev
alua
tion
syst
em
2 m
onth
s fo
llow
-up
P- valu
e 3
mon
ths
follo
w-u
p P- va
lue
6 m
onth
s fo
llow
-up
P- valu
e 12
mon
ths
follo
w-u
p P- va
lue
24 m
onth
s fo
llow
-up
P- valu
e
Cat
egor
y:
Exce
llent
G
ood
Fair
Poor
Ex
celle
nt
Goo
d Fa
ir Po
or
Exce
llent
G
ood
Fair
Poor
Ex
celle
nt
Goo
d Fa
ir Po
or
Exce
llent
G
ood
Fair
Poor
All
patie
nts
24 (1
0)
46
(20)
75
(3
3)
85
(37)
28 (2
0)45
(3
1)
37
(26)
33
(2
3)24
(28)
23
(27)
17
(2
0)
21
(25)
24 (4
3)9 (1
6)
12
(21)
11
(2
0)69
(53)
30
(23)
15
(1
2)
15
(12)
Age
0-25
yea
rs
14 (1
8)18
(2
3)
23
(29)
24
(3
0)0.
05*
17 (3
3)18
(3
5)
7 (14)
9 (1
8)0.
004*
11
(42)
11
(42)
1 (4
) 3 (1
2)0.
005*
13
(72)
2 (11)
1 (6
) 2 (1
1)0.
02*
28 (6
5)8 (1
8)
5 (12)
2 (5
)0.
20
26-5
0 ye
ars
10 (1
0)
19
(19)
35
(3
4)
38
(37)
11 (1
7)17
(2
7)
18
(28)
18
(2
8)12
(28)
10
(23)
10
(2
3)
11
(26)
8 (3
0)7 (2
6)
7 (26)
5 (1
8)28
(45)
19
(31)
7 (1
1)
8 (13)
>51
year
s 0
(0)
9 (18)
17
(3
5)
23
(47)
0 (0
)10
(3
6)
12
(43)
6 (2
1)1
(6)
2 (12)
6 (3
8)
7 (44)
3 (2
8)0
(0)
4 (36)
4 (3
6)13
(54)
3 (13)
3 (1
3)
5 (20)
Con
com
itant
com
plet
e ne
rve
tran
sect
ion
Yes
11
(12)
11
(1
2)
34
(35)
39
(4
1)0.
07
13 (2
5)16
(3
0)
10
(19)
14
(2
6)0.
3817
(32)
13
(2
4)
12
(23)
11
(2
1)0.
4810
(44)
4 (1
7)
4 (17)
5 (2
2)0.
93
26 (4
8)15
(2
8)
7 (13)
6 (1
1)0.
69
No
13 (1
0)
35
(26)
41
(3
0)
46
(34)
15 (1
7)29
(3
2)
27
(30)
19
(2
1)7
(22)
10
(31)
5 (1
6)
10
(31)
14 (4
3)5 (1
5)
8 (24)
6 (1
8)43
(59)
15
(21)
9 (1
2)
6 (8)
Tra
nsec
tion
of F
DP
and
FDS
tend
ons
Yes
10
(11)
18
(2
1)
22
(25)
37
(4
3)0.
41
13 (2
2)20
(3
5)
15
(26)
10
(1
7)0.
747
(30)
5 (2
1)
3 (12)
9 (3
7)0.
3311
(52)
2 (1
0)
3 (14)
5 (2
4)0.
39
22 (4
6)11
(2
3)
6 (12)
9 (1
9)0.
29
No
14 (1
0)
27
(20)
48
(3
6)
46
(34)
16 (1
8)29
(3
2)
26
(28)
20
(2
2)15
(26)
18
(31)
13
(2
2)
12
(21)
11 (3
4)7 (2
2)
8 (25)
6 (1
9)44
(59)
16
(21)
9 (1
2)
6 (8)
39
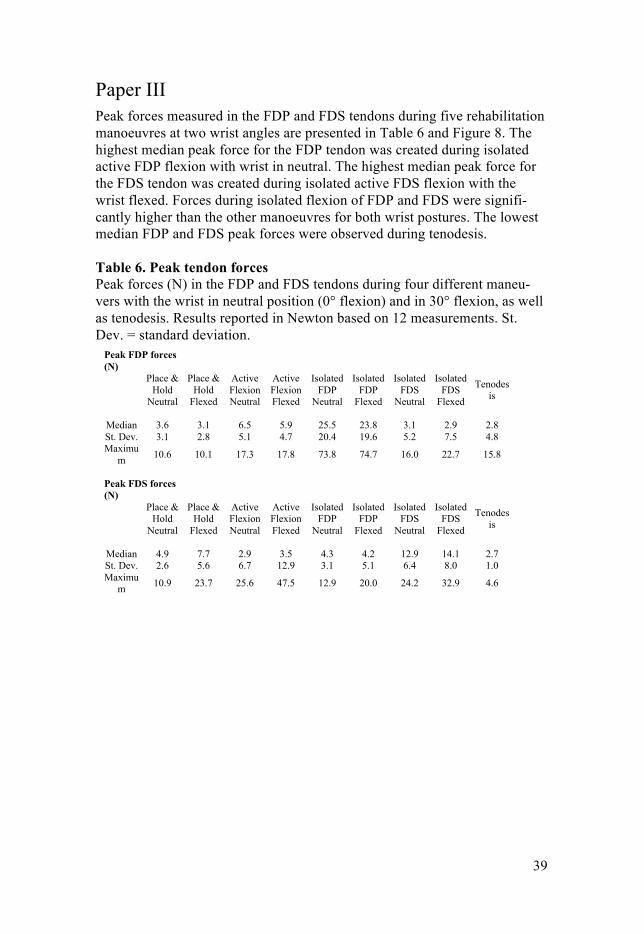
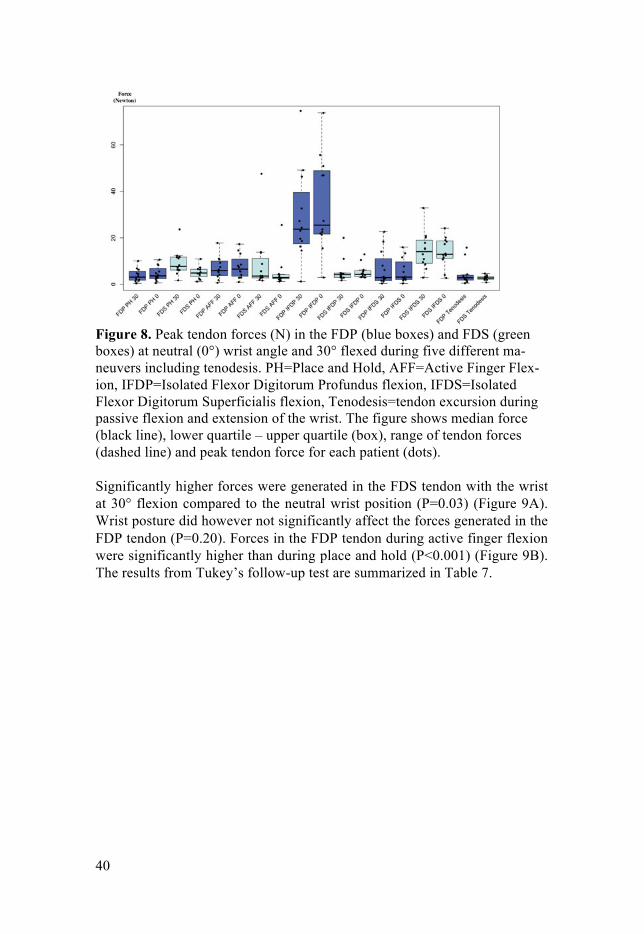
Paper III Peak forces measured in the FDP and FDS tendons during five rehabilitation manoeuvres at two wrist angles are presented in Table 6 and Figure 8. The highest median peak force for the FDP tendon was created during isolated active FDP flexion with wrist in neutral. The highest median peak force for the FDS tendon was created during isolated active FDS flexion with the wrist flexed. Forces during isolated flexion of FDP and FDS were signifi-cantly higher than the other manoeuvres for both wrist postures. The lowest median FDP and FDS peak forces were observed during tenodesis.
Table 6. Peak tendon forces Peak forces (N) in the FDP and FDS tendons during four different maneu-vers with the wrist in neutral position (0° flexion) and in 30° flexion, as well as tenodesis. Results reported in Newton based on 12 measurements. St. Dev. = standard deviation.
Peak FDP forces (N)
Place & Hold
Neutral
Place & Hold
Flexed
Active Flexion Neutral
Active Flexion Flexed
Isolated FDP
Neutral
Isolated FDP
Flexed
Isolated FDS
Neutral
Isolated FDS
Flexed
Tenodesis
Median 3.6 3.1 6.5 5.9 25.5 23.8 3.1 2.9 2.8 St. Dev. 3.1 2.8 5.1 4.7 20.4 19.6 5.2 7.5 4.8 Maximu
m 10.6 10.1 17.3 17.8 73.8 74.7 16.0 22.7 15.8
Peak FDS forces (N)
Place & Hold
Neutral
Place & Hold
Flexed
Active Flexion Neutral
Active Flexion Flexed
Isolated FDP
Neutral
Isolated FDP
Flexed
Isolated FDS
Neutral
Isolated FDS
Flexed
Tenodesis
Median 4.9 7.7 2.9 3.5 4.3 4.2 12.9 14.1 2.7 St. Dev. 2.6 5.6 6.7 12.9 3.1 5.1 6.4 8.0 1.0 Maximu
m 10.9 23.7 25.6 47.5 12.9 20.0 24.2 32.9 4.6
40
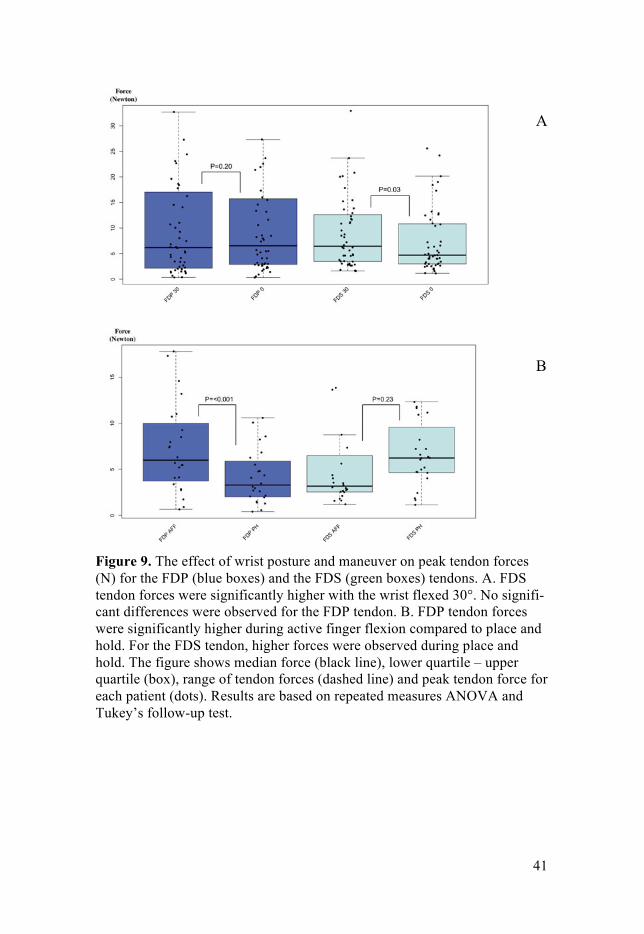
Figure 8. Peak tendon forces (N) in the FDP (blue boxes) and FDS (green boxes) at neutral (0°) wrist angle and 30° flexed during five different ma-neuvers including tenodesis. PH=Place and Hold, AFF=Active Finger Flex-ion, IFDP=Isolated Flexor Digitorum Profundus flexion, IFDS=Isolated Flexor Digitorum Superficialis flexion, Tenodesis=tendon excursion during passive flexion and extension of the wrist. The figure shows median force (black line), lower quartile – upper quartile (box), range of tendon forces (dashed line) and peak tendon force for each patient (dots). Significantly higher forces were generated in the FDS tendon with the wrist at 30° flexion compared to the neutral wrist position (P=0.03) (Figure 9A). Wrist posture did however not significantly affect the forces generated in the FDP tendon (P=0.20). Forces in the FDP tendon during active finger flexion were significantly higher than during place and hold (P<0.001) (Figure 9B). The results from Tukey’s follow-up test are summarized in Table 7.
41
Figure 9. The effect of wrist posture and maneuver on peak tendon forces (N) for the FDP (blue boxes) and the FDS (green boxes) tendons. A. FDS tendon forces were significantly higher with the wrist flexed 30°. No signifi-cant differences were observed for the FDP tendon. B. FDP tendon forces were significantly higher during active finger flexion compared to place and hold. For the FDS tendon, higher forces were observed during place and hold. The figure shows median force (black line), lower quartile – upper quartile (box), range of tendon forces (dashed line) and peak tendon force for each patient (dots). Results are based on repeated measures ANOVA and Tukey’s follow-up test.
A
B
42
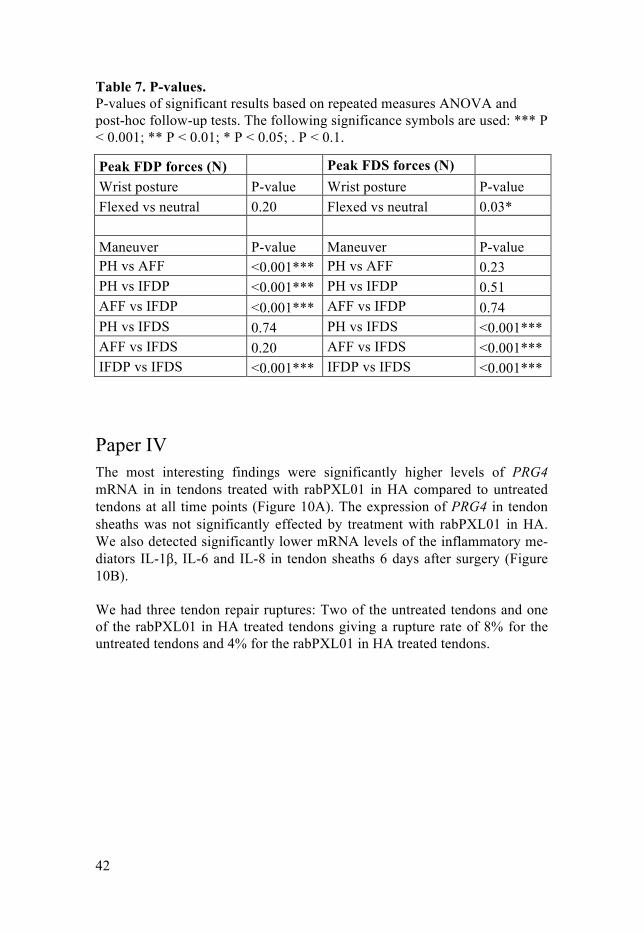
Table 7. P-values. P-values of significant results based on repeated measures ANOVA and post-hoc follow-up tests. The following significance symbols are used: *** P < 0.001; ** P < 0.01; * P < 0.05; . P < 0.1.
Peak FDP forces (N)
Peak FDS forces (N) Wrist posture P-value Wrist posture P-value
Flexed vs neutral 0.20 Flexed vs neutral 0.03*
Maneuver P-value Maneuver P-value PH vs AFF <0.001*** PH vs AFF 0.23 PH vs IFDP <0.001*** PH vs IFDP 0.51 AFF vs IFDP <0.001*** AFF vs IFDP 0.74 PH vs IFDS 0.74 PH vs IFDS <0.001*** AFF vs IFDS 0.20 AFF vs IFDS <0.001*** IFDP vs IFDS <0.001*** IFDP vs IFDS <0.001***
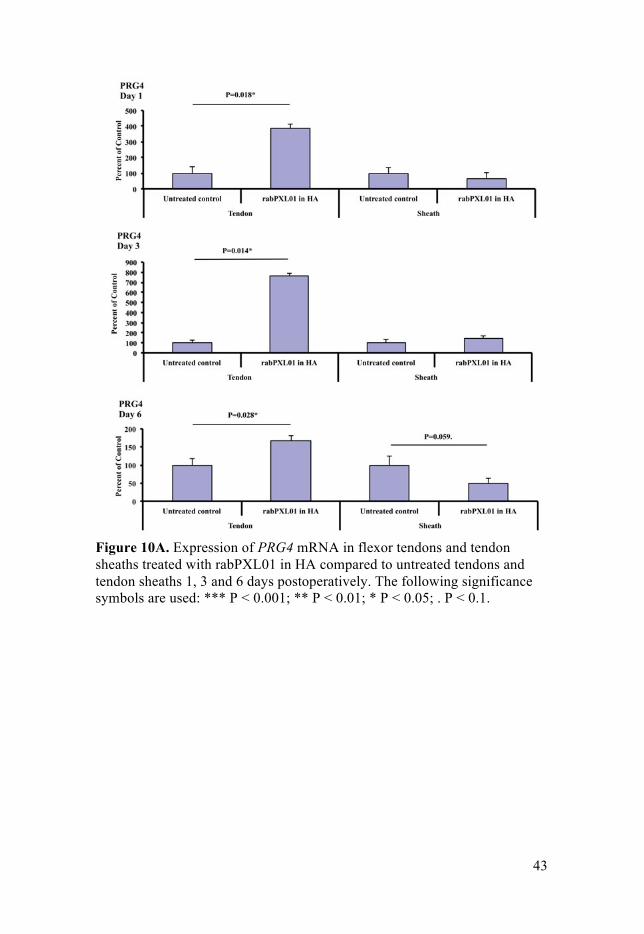
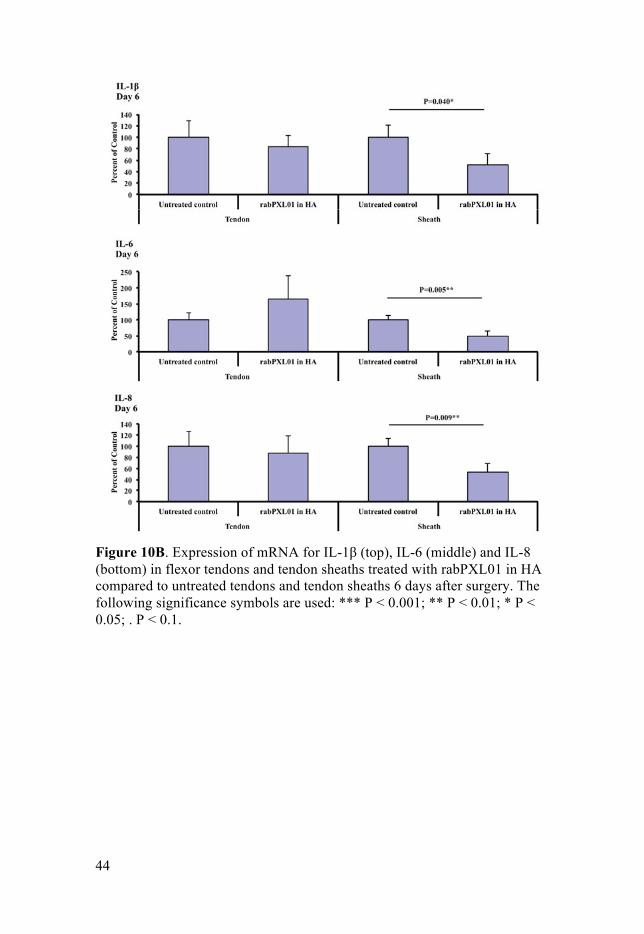
Paper IV The most interesting findings were significantly higher levels of PRG4 mRNA in in tendons treated with rabPXL01 in HA compared to untreated tendons at all time points (Figure 10A). The expression of PRG4 in tendon sheaths was not significantly effected by treatment with rabPXL01 in HA. We also detected significantly lower mRNA levels of the inflammatory me-diators IL-1β, IL-6 and IL-8 in tendon sheaths 6 days after surgery (Figure 10B). We had three tendon repair ruptures: Two of the untreated tendons and one of the rabPXL01 in HA treated tendons giving a rupture rate of 8% for the untreated tendons and 4% for the rabPXL01 in HA treated tendons.
43
Figure 10A. Expression of PRG4 mRNA in flexor tendons and tendon sheaths treated with rabPXL01 in HA compared to untreated tendons and tendon sheaths 1, 3 and 6 days postoperatively. The following significance symbols are used: *** P < 0.001; ** P < 0.01; * P < 0.05; . P < 0.1.
44
Figure 10B. Expression of mRNA for IL-1β (top), IL-6 (middle) and IL-8 (bottom) in flexor tendons and tendon sheaths treated with rabPXL01 in HA compared to untreated tendons and tendon sheaths 6 days after surgery. The following significance symbols are used: *** P < 0.001; ** P < 0.01; * P < 0.05; . P < 0.1.

45
Discussion
An active population using their hands contributes to a never-ending source of intrasynovial flexor tendon injuries in the hand. Scientific progresses within this area have improved the outcome after intrasynovial flexor tendon injury and repair, but we can still wish for more. Paper I and II investigated risk factors for rupture of repair and impaired digital range of motion after flexor tendon jury and repair. These studies are observational and evaluated standard care. After identifying risk factors for rupture of repair and im-paired digital mobility, the next step was to find possible ways to modulate the treatment for high-risk patients. This possibility was investigated in Pa-per III. Knowledge of forces transmitted over the repair during rehabilitation and comparing these forces to the strength of a standard repair may make it possible to design a rehabilitation protocol that is individually customized depending on identified risk factors, the patient, and the repair. This study was conducted in the Outpatient Surgery Center at University of California, San Francisco (UCSF), during open carpal tunnel release of 12 patients. I spent a year of my doctorial studies at UCSF and this work was completed during this year. Patients at high risk of adhesions and impaired digital range of motion might gain from adjuvant treatment after surgery. PXL01 in HA seems to have this potential and Paper IV investigates the mechanism of action of this lubricat-ing formula by analyzing its effect on gene expression in a rabbit model of tendon injury and repair. This work was done in collaboration with McCaig Institute for Bone and Joint Health, University of Calgary, Calgary, Canada. I learn the methods used in Paper IV during studies at Dr Hart’s laboratory at McCaig Institute for Bone and Joint Health. Taken together, this thesis includes work to identify some of the problems associated with intrasynovial flexor tendon injury and repair, and work that investigate possible solutions for these problems. To achieve this I have used a wide range of research methods, including two epidemiological studies, one clinical study on humans, and one basic research study.
46
Paper I and II Why do some patients suffer from rupture of their flexor tendon repair? We investigated the impact of demography and associated injuries on post-surgical results and found age, concomitant nerve and combined FDP and FDS tendon injuries to be significantly associated with rupture of repair. I have read a large number of papers investigating the biomechanics of the suture. Those studies have obviously helped improving the results after in-trasynovial flexor tendon repair. However, the rupture rate worldwide is still 4-18%25,26 and the rate of reoperation after flexor tendon repair did not show a decreasing trend between 1998-2005.29 From previous studies by Dy et al., 2012,29 Moriya et al., 2015136 and Rigo et al., 2016137 we know some about the negative effect of age on the risk for repair rupture and impaired digital mobility. They have previously reported on predictors of poor outcome after flexor tendon injury and repair. Dy et al., 2012,29 studied risk factors for reoperation after flexor tendon injury and repair, whereas Moriya et al., 2015136 and Rigo et al., 2016137 published co-hort studies analyzing factors affecting digital range of motion. Consistent with those studies, we found age to correlate negatively with the risk of re-pair rupture and impaired outcome. Our studies showed 5% increased risk of rupture per patient life-year and increasing age was significantly associated with impaired digital range of motion but only during the first year after surgical repair. Interestingly, the difference in digital range of motion could not be detected 24 months after surgery meaning that follow-up studies of digital mobility after finger trauma might benefit from continuing over a 2 years time-span. We found a more pronounced age effect than Dy et al., 201229 who report roughly 1% increased risk of reoperation per patient life-year. The difference in age effect is likely due to the fact that we study pa-tients with rupture of repairs whereas Dy et al., 201229 does not distinguish between patients with rupture of repairs and tenolysis. In our studies there were no restrictions in rehabilitation exercise with re-spect to whether the tendon transection was combined with a nerve transec-tion or not. However, a patient with a combined tendon and nerve repair might be more careful during rehabilitation exercises to reduce tension on the sutured nerve and tendon, which in theory could result in reduced range of motion. We found nerve transections to significantly decrease the risk of repair rupture without affecting digital mobility. Our findings are compara-ble to those reported by Dy et al., 201229 who showed patient with combined tendon and nerve repair to less likely undergo reoperation. Our results are also in line with those by Rosberg et al. 200327 and Rigo et al., 2016.137 They found no significant effects on digit range of motion after flexor ten-don repair in patients with an accompanying digital nerve injury. However,

47
Trumble et al.28 demonstrated poorer outcomes within this patient group. The effect of a concomitant nerve injury is therefore an interesting target on which to focus future investigations on. A combined transection of the FDP and FDS tendons was found to increase the risk of rupture of the repair without affecting digital mobility. These results match those of Strickland et al 1980112 and of Baktir et al., 1996139 who studied digital mobility and reported similar results following repair of both the FDS and FDP tendon. Increased risk of rupture of repair is under-standable since the forces during rehabilitation exercises rely on two sutured tendons (or one if only the FDP is sutured). Absence of effect on digital range of motion following a combined FDP and FDS tendon injury was however surprising since two repairs are likely to give greater contact sur-face between the suture and the sheath leading to more adhesion formations.
Paper III Isolated flexion of the FDP and FDS tendons generated the highest forces. These maneuvers are implemented to allow tendon gliding of only the ten-don that is activated, but unexpectedly forces up to 23 N were observed in the other tendon during the isolated tendon maneuver. The forces in the FDP tendon during isolated flexion of the FDS tendon are similar to the forces generated in the FDP during active finger flexion. Those peak forces could exceed repair strength in some patients. Isolated FDP and FDS flexion create high forces on the tendons but low excursions between the tendons140 and should be avoided during rehabilitation. Active finger flexion generated significantly higher forces in the FDP tendon compared to place and hold. The place and hold maneuver, when the fingers are passively flexed to touch the palm and then actively maintained in that position, is believed to minimize the force on the tendon compared to active finger flexion. Surprisingly, the forces in the FDS tendon tended to be higher during place and hold. With respect to the FDP tendon, passive finger flex-ion may be used for patients who need to limit the force on the tendon during early postoperative rehabilitation. Flexed wrist position seems not to protect the repair but rather increase the risk of rupture of the repair. Significantly higher FDS tendon forces were measured with the wrist at 30° flexion com-pared to neutral wrist position. Though wrist position did not affect FDP tendon forces, nothing suggests that flexed wrist position is preferable. A standard 4-strand repair withstands ultimate forces of 49-85 N,18-22 and a 6-strand repair 51-76 N17,19 before repair failure. This is far more than the median peak forces that we have measured. However, the repair must with-

48
stand forces generated during early mobilization both initially and following early tendon softening. The mean repair strengths during the first postopera-tive 10 days vary between a decrease of 18% to an increase of 25% com-pared to initial strength.113,125-127 Before repair rupture, a tendon gap form, which impairs tendon excursion and may lead to rupture.43,128 Tendon suture gaps of 2 mm have approximately 70% of the ultimate repair strength.17,20-22 After deducting a safety factor of 18% decreased repair strength and 30 % for gapping, we estimated that peak forces on the flexor tendon during reha-bilitation should be less than 28 and 29 N for 4-strand and 6-strand sutures respectively. Based on our data, we recommend active finger flexion and place and hold with the wrist in neutral, as well as tenodesis during the first 3 weeks after a 4- or 6-strand surgical repair of the FDP or FDS tendons. Isolated flexion of the FDP and FDS should be avoided. The individual differences in forces between patients are large. This could be explained by individual differences between hands e.g. joint stiffness and differences in the motor control of the tendons. The FDP tendon to the index finger is separated whereas the tendons to the middle, ring and little fingers are conjoined. This anatomical difference might also affect forces generated by the tendons to ulnar fingers. We also have some evidence for age and concomitant injuries to affect the risk of rupture of repair. These individual differences and possible concomitant injuries need also to be considered when planning a patient’s rehabilitation protocol.
Paper IV Studies of PXL01 in HA administrated around repaired tendons have shown statistically significant increase in digit range of motion in both humans132 and rabbits.130,131 We have tried to clarify the mechanisms underlying these effects. We found significantly increased expression of PRG4 in tendons treated with rabPXL01 in HA 1, 3 and 6 days after surgery, and a significant and coordinated suppression of mRNA levels for IL-1β, L-6 and IL-8 in tendon sheaths 6 days after surgery. Increased expression of PRG4 in ten-dons suggests that rabPXL01 in HA leads to an increase in lubricin produc-tion, and subsequently reduces the gliding resistance and inhibits adhesion formations after flexor tendon repair. Our results are consistent with previ-ous studies on the effect of lubricin on the gliding resistance of intrasynovial tendons60,61,64-66 except that adjuvant treatment with rabPXL01 did not in-crease the rupture rate which was seen in two of the previous studies.65,66 We believe suppression of mRNA levels for IL-1β, IL-6 and IL-8 in tendon sheaths gives a down-regulation of the inflammatory response postoperative-ly. Prolonged inflammation in the wound-healing cascade can lead to exces-

49
sive adhesion formation, whereas down-regulation is believed to restrict proliferation and remodeling leading to prevention of scarring.67 Suppression of inflammation and increased lubricin levels might be some of the mecha-nisms behind the improvement in digit range of motion that has been shown after adjuvant treatment with PXL01 in HA.130-132 Treatment with PXL01 in HA could be beneficial especially for patients at risk of impaired digital range of motion after intrasynovial flexor tendon injury and repair by re-duced on site inflammation and increased levels of lubricin.

50
Conclusion
The results of this thesis suggest that the successful way to optimize the out-come after intarsynovial flexor tendon injury and repair is to see to the whole patient, try not to focus only on her or his injury, and to create individually adapted treatment plans depending on the patient, the injury and the repair. To reduce the risk of rupture of repair and impaired digital mobility after intrasynovial FDP tendon injuries, our two observational studies indicate that patient based factors are as important as suture biomechanics. Increasing age and concomitant FDS tendon transection increase the risk of rupture postoperatively, whereas a concomitant nerve transection seems to have a protective effect. To predict the long-term outcome, the single most im-portant factor is the age of the patient. Our clinical study of forces generated in the FDP and FDS during flexor tendon repair rehabilitation shows that active finger flexion and place and hold with neutral wrist position, as well as tenodesis, can be used with lim-ited risk of repair rupture during the first 3 weeks after 4- or 6-strand surgi-cal repair. Isolated flexion of the FDP and FDS should be avoided through-out this initial 3-week postoperative period due to higher measured tendon forces. However, there are individual differences between patients and to reduce the risk of repair rupture, patients with transection of both the FDP and FDS tendons as well as older patients might benefit from rehabilitation using a less active regime e.g. place hold. Adjuvant treatment with PXL01 in HA might be beneficial for patients iden-tified with high risk of repair rupture and adhesion formation or patients unable to participate in early motion therapy due to multiple injuries or other medical conditions. Using a rabbit model, treatment with rabPXL01 in HA increased the levels of lubricin and reduced the levels of pro-inflammatory IL-1β, IL-6 and IL-8 which correspondingly reduces the gliding resistance and inhibits adhesion formation after flexor tendon repair.

51
Visions to improve tendon healing
Modifying the molecular mechanisms of tendon healing Modern treatment has improved the outcome after flexor tendon injury and repair. However, the incidence of reoperation has not clearly decreased since 2000.135 Further research on surgical techniques and rehabilitation protocols might not reduce the incidence of rupture of repair and it seems as this field of research is shifting towards modifying the molecular aspects of flexor tendon healing68 e.g. by gene transfers141 or autologous platelet rich plasma142 or serum143 containing growth factors and cytokines, or scaffolds loaded with mesenchymal stem cells and growth factors.144 Some of these treatments may hold significant promise, but they are still a long way from a complete therapy used in clinical practice.145
Identifying risk factors Besides manipulating the biological processes that occur during tendon heal-ing, patient and population based studies might further improve the outcome by investigating and identifying factors that contribute to postoperative com-plications.135-137 Population and patient based research could deepen the un-derstanding of the etiology of rupture of repair and impaired digit range of motion.135-137 This knowledge might make it possible to identify patients with high risks of rupture of repair and impaired digit range of motion. De-pending on individual risk factors, the initial injury and the repair, surgical technique and postoperative rehabilitation protocols can be modified to indi-vidualize and thereby improve the treatment of flexor tendon injuries.
52
Sammanfattning på svenska
Böjsenskador på fingernivå (handens zon I och II) är komplicerade då böj-senorna – den djupa böjsenan (FDP) och den ytliga böjsenan (FDS) – på denna nivå omsluts av en senskida. Senskidan och dess vätska är viktiga för senornas näringstillförsel. Utanpå senskidan finns starka fibrösa band (pul-leys) vars uppgift är att hålla senan mot fingerskelettet då fingret böjs och sträcks, utan dessa band skulle ett bågsträngsfenomen uppstå när fingret böjs. Senskidan och de fibrösa banden har ytterst viktiga anatomiska funkt-ioner och utgör en teknisk utmaning i samband med sutur av böjsenskador och rehabilitering efter en böjsensutur. Små förändringar i fingrarnas fina anatomi ger stora effekter på fingrarnas funktion. Böjsenorna utgörs av cell-fattig vävnad vilket medför att de läker långsamt. Böjsenorna är beroende av näring från senskidan och från små blodkärl från fingerartärerna. Det är där-för mycket viktigt att senan sys ihop på allra bästa sätt och att blodkärlens, senskidans och de fibrösa bandens anatomi bevaras. Lika viktigt är att det skadade fingret rehabiliteras på rätt sätt. För lätt rehabilitering ökar risken för att senan under läkningsprocessen ärrar fast i senskidan och därmed går det inte att böja och sträcka fingret, medan för omfattande rörelseövningar kan leda till att böjsensuturen släpper. Båda komplikationerna leder till ned-satt fingerrörlighet. Jag har i denna avhandling försökt utreda om patientrelaterade faktorer (t.ex. ålder, kön) och associerade skador (skada på båda böjsenorna eller nerv-skada tillsammans med skada på djupa böjsenan) påverkar risken för ruptur efter sutur av den djupa böjsenan i zon I och II (artikel I). Efter att ha identi-fierat patientrelaterade faktorer och associerade skador som ökar risken för ruptur efter sutur av den djupa böjsenan, har jag i artikel II utvärderat om dessa riskfaktorer påverkar fingerrörligheten på lång sikt (2 år). Jag fann att ökad ålder var starkt korrelerad till både ökad risk för ruptur efter sensutur samt nedsatt fingerrörlighet under det första året efter sutur av den djupa böjsenan. Två år efter senskadan kunde dock ingen skillnad i fingerrörlighet detekteras mellan de olika åldersgrupperna. Skada på den djupa böjsenan tillsammans med nervskada minskade risken för ruptur efter sensutur men påverkade inte fingerrörligheten. Detta resultat var något oväntat varför denna skadekombination kan vara intressant att studera ytterligare. Skada på fingrets båda böjsenor ökade risken för ruptur efter sensutur utan att påverka fingerrörligheten. Även detta var något förvånande eftersom en större skada

53
teoretiskt sett ökar risken för att mycket ärrvävnad bildas och därmed leder till sammanväxningar mellan sena och senskida. Givet att man kan identifiera vilka patienter som har ökad risk för ruptur av en sensutur och dålig fingerrörlighet efter sutur av den djupa böjsenan (base-rat på resultaten i artikel I och II), var tanken att i artikel III undersöka hur stora krafter böjsenorna till pekfingret utsätts för under rehabiliteringsöv-ningarna. Med vetskap om de krafter en böjsensutur utsätts för skulle man kunna modifiera rehabiliteringsövningarna beroende på existerande riskfak-torer och beroende på hur stark sensutur man åstadkommit med den kirur-giska åtgärden. Dessa studier är ett steg närmare en individualisering av be-handlingen efter skada på den djupa böjsenan. Jag fann att rehabilitering enligt våra standardprotokoll (aktiva rörelseövningar och place and hold) med största sannolikhet kan användas efter sutur av böjsenskada i zon I och II utan att äventyra sensuturen. Isolerad aktivering av endast den djupa eller den ytliga böjsenan genererade mycket högre krafter än vid rörelseövningar-na enligt standardprotokollen (aktiva rörelseövningar och place and hold). Jag fann inget som stödjer teorin att en lätt böjd handled lättar på kraften över böjsenorna, snarare genererades större krafter vid lätt böjd handled. Således bör isolerad aktivering av den djupa och den ytliga böjsenan undvi-kas, och likaså bör man inte låta handleden vara lätt böjd i gips eller under rehabilitering efter böjsensutur. För att förbättra rörligheten efter böjsensutur har man provat olika tilläggs-behandlingar i samband med sensutur. PXL01 är en sådan tilläggsbehand-ling, en gel som administreras runt den suturerade böjsenan för att minska risken för sammanväxningar mellan sena och senskida. Tidigare studier har visat att behandling med PXL01 ökar fingerrörligheten efter sutur av den djupa böjsenan. I artikel IV studerade jag möjliga molekylära mekanismer bakom de positiva effekter man har sett efter tilläggsbehandling med PXL01. Som tecken på minskad inflammation fann jag minskade genuttryck för de pro-inflammatoriska mediatorerna interleukin 1β, 6, and 8, och som tecken på minskad friktion mellan sena och senskida fann jag ökat genuttryck för PRG4. PRG4 är en gen som kodar för lubricin, ett protein som minskar frikt-ionen mellan sena och senskida. Minskad friktion mellan sena och senskida tillsammans med reducerad inflammation kan teoretiskt minska risken för sammanväxningar mellan sena och senskida och därmed öka fingerrörlighet-en och förbättra resultatet efter böjsensutur. Sammanfattningsvis visar denna avhandling att resultatet efter böjsensutur i zon I och II sannolikt kan förbättras genom att planera behandlingen utifrån patientens individuella förutsättningar, typ av skada och beroende på hur stark sensutur som åstadkommits.

54
55
Acknowledgements
I would like to express my gratitude to everyone contributing to the work of this thesis. I would especially like to thank: Monica Wiig, my supervisor, for introducing me to science, for sharing your ideas with me, for giving me the opportunity to go to University of Calgary and learn about RNA extraction and RT-qPCR, and for encouraging me when I needed it. Thank you Monica and Johan for caring for my family when we moved back from San Francisco.
Kenneth Jonsson, my co-supervisor, for always giving me a short and hon-est answer to my questions. Your words of encouragement and your con-structive criticism helped me especially during my first year at the Depart-ment of Orthopaedics. Kenneth and Greta – I look forward to all the fun! Uppsala University, Professor Nils Hailer and Professor emeritus Olle Nils-son, for supporting me during the work of this thesis, and especially for giv-ing me the opportunity to go to San Francisco and study at UCSF – it was the best experience ever! Head of Department of Orthopaedics, Karin Bernhoff and former head of Department of Orthopaedics Katarina Lönn for encouragement and support and for giving me time to focus on research. Stephan Wilbrand, former head of Department of Hand Surgery, for trust-ing in me twice. Physiotherapist Majvor Davidsson, for your dedicated work during the flexor tendon study, Britt-Marie Andersson, for skillful technical assis-tance during the rabPXL01 study, and Anneli Johansson, for taking care of all practical problems. Björn Holm, Margit Mahlapuu, Carol Reno and David Hart, co-authors of the rabPXL01 study, for invaluable work throughout the study.
56
Lisa Lattanza for showing me your clinical world at UCSF and, together with David Rempel, for giving me the opportunity to complete the flexor tendon study. Laura Esserman and Michael Endicott, for generous hospitality and for sharing your network in San Francisco. My colleagues and friends at the Department(s) of Orthopaedics and Hand Surgery, for making our work so interesting and fun. Spjutharna – because we have so much fun! I hope we will share a lot of Kodak moments. My dearest Linda Unge, my superstar, Kristina Lundberg, my lifeline, and Miriam Talah, my moral compass, for everything. Britta Eklund och Göran Eklund, for your kindness and support, for al-ways welcoming me into your loving and safe home, and for showing me that hard work pays off. I cannot explain how much you mean to me! Per och Anna Edsfeld, Sara Åström och Markus Elving – for joyful din-ners, chaotic Christmases, lively discussions, and especially for Lea’s and Ellen’s wonderful cousins. I love to see our children play, laugh and debate. Per Edsfeldt, for being my partner in crime during the gangsta era, and to-day for giving me perspectives in life. Sara Åström, for being my advisor and for handing me simple solutions to difficult problems. My co-parents: Margareta Andersson, for supporting me and helping me through years of education, and Tomas Johansson – tack för att du alltid ställer upp för Martin och mig! My wonderful parents, Barbro Edsfeldt and Gunnar Edsfeldt, for your endless love and support, and for being the best parents and grandparents. Vad skulle vi göra utan er? Mamma, jag älskar dig! Pappa, jag älskar dig! Lea and Ellen, my sources of inspiration. I love you! Most important of all, Martin, the love of my life and my best friend. For believing in me, for your enthusiasm and for tutoring me through the statisti-cal difficulties and hard work writing this thesis. For sharing the most pre-cious gifts in life with me, our lovely daughters, Lea and Ellen. You make me happy ♥

57
58
References
1. Bunnell S. Surgery of the Hand. 1 st ed. Philadelphia: JB Lippincott; 1944.
2. Verdan CE. Primary repair of flexor tendons. J Bone Joint Surg Am. 1960;42-A:647-657.
3. Kleinert HE, Kutz JE, Ashbell TS, et al. Primary repair of lacerated flexor tendons in “no man’s land. J Bone Joint Surg. 1967;49A:577(abstract).
4. Kessler I, Nissim F. Primary repair without immobilization of flexor tendon division within the digital sheath. An experimental and clinical study. Acta Orthop Scand. 1969;40(5):587-601.
5. Kleinert HE, Kutz JE, Atasoy E, et al. Primary repair of flexor tendons. Orthop Clin North Am. 1973;4(4):865-876.
6. Duran RJ, Houser RG. Controlled passive motion following flexor tendon repair in zones 2 and 3. AAOS symposium on tendon surgery in the hand. Saint Louis: CV Mosby. 1975:105 - 114.
7. Strickland JW. Development of flexor tendon surgery: twenty-five years of progress. J Hand Surg Am. 2000;25(2):214-235.
8. Lin TW, Cardenas L, Soslowsky LJ. Biomechanics of tendon injury and repair. J Biomech. 2004;37(6):865-877.
9. James R, Kesturu G, Balian G, et al. Tendon: biology, biomechanics, repair, growth factors, and evolving treatment options. J Hand Surg Am. 2008;33(1):102-112.
10. Berglund M, Reno C, Hart DA, et al. Patterns of mRNA expression for matrix molecules and growth factors in flexor tendon injury: differences in the regulation between tendon and tendon sheath. J Hand Surg Am. 2006;31(8):1279-1287.
11. Juneja SC, Schwarz EM, O'Keefe RJ, et al. Cellular and molecular factors in flexor tendon repair and adhesions: a histological and gene expression analysis. Connect Tissue Res. 2013;54(3):218-226.
12. Doyle JR. Anatomy of the finger flexor tendon sheath and pulley system. J Hand Surg Am. 1988;13(4):473-484.
13. Doyle JR. Palmar and digital flexor tendon pulleys. Clin Orthop Relat Res. 2001(383):84-96.
14. Tang JB, Xie RG. Effect of A3 pulley and adjacent sheath integrity on tendon excursion and bowstringing. J Hand Surg Am. 2001;26(5):855-861.
15. Phillips C, Mass D. Mechanical analysis of the palmar aponeurosis pulley in human cadavers. J Hand Surg Am. 1996;21(2):240-244.
59
16. Hamman J, Ali A, Phillips C, et al. A biomechanical study of the flexor digitorum superficialis: effects of digital pulley excision and loss of the flexor digitorum profundus. J Hand Surg Am. 1997;22(2):328-335.
17. Xie RG, Zhang S, Tang JB, et al. Biomechanical studies of 3 different 6-strand flexor tendon repair techniques. J Hand Surg Am. 2002;27(4):621-627.
18. Barrie KA, Wolfe SW, Shean C, et al. A biomechanical comparison of multistrand flexor tendon repairs using an in situ testing model. J Hand Surg Am. 2000;25(3):499-506.
19. Viinikainen A, Goransson H, Huovinen K, et al. A comparative analysis of the biomechanical behaviour of five flexor tendon core sutures. J Hand Surg Br. 2004;29(6):536-543.
20. Vigler M, Palti R, Goldstein R, et al. Biomechanical study of cross-locked cruciate versus Strickland flexor tendon repair. J Hand Surg Am. 2008;33(10):1826-1833.
21. Miller B, Dodds SD, deMars A, et al. Flexor tendon repairs: the impact of fiberwire on grasping and locking core sutures. J Hand Surg Am. 2007;32(5):591-596.
22. Osei DA, Stepan JG, Calfee RP, et al. The effect of suture caliber and number of core suture strands on zone II flexor tendon repair: a study in human cadavers. J Hand Surg Am. 2014;39(2):262-268.
23. Lawrence TM, Davis TR. A biomechanical analysis of suture materials and their influence on a four-strand flexor tendon repair. J Hand Surg Am. 2005;30(4):836-841.
24. Taras JS, Raphael JS, Marczyk SC, et al. Evaluation of suture caliber in flexor tendon repair. J Hand Surg Am. 2001;26(6):1100-1104.
25. Tang JB. Clinical outcomes associated with flexor tendon repair. Hand Clin. 2005;21(2):199-210.
26. Su BW, Solomons M, Barrow A, et al. Device for zone-II flexor tendon repair. A multicenter, randomized, blinded, clinical trial. J Bone Joint Surg Am. 2005;87(5):923-935.
27. Rosberg HE, Carlsson KS, Hojgard S, et al. What determines the costs of repair and rehabilitation of flexor tendon injuries in zone II? A multiple regression analysis of data from southern Sweden. J Hand Surg Br. 2003;28(2):106-112.
28. Trumble TE, Vedder NB, Seiler JG, 3rd, et al. Zone-II flexor tendon repair: a randomized prospective trial of active place-and-hold therapy compared with passive motion therapy. J Bone Joint Surg Am. 2010;92(6):1381-1389.
29. Dy CJ, Daluiski A, Do HT, et al. The epidemiology of reoperation after flexor tendon repair. J Hand Surg Am. 2012;37(5):919-924.
30. Green's operative hand surgery. Vol 1:220-222. Fifth ed. 31. Lundborg G, Holm S, Myrhage R. The role of the synovial fluid and
tendon sheath for flexor tendon nutrition. An experimental tracer
60
study on diffusional pathways in dogs. Scand J Plast Reconstr Surg. 1980;14(1):99-107.
32. Harrison RK, Jones ME, Clayton E, et al. Mapping of vascular endothelium in the human flexor digitorum profundus tendon. J Hand Surg Am. 2003;28(5):806-813.
33. Pike JM, Gelberman RH. Zone II combined flexor digitorum superficialis and flexor digitorum profundus repair distal to the A2 pulley. J Hand Surg Am. 2010;35(9):1523-1527.
34. Kannus P. Structure of the tendon connective tissue. Scand J Med Sci Sports. 2000;10(6):312-320.
35. Moore MJ, De Beaux A. A quantitative ultrastructural study of rat tendon from birth to maturity. J Anat. 1987;153:163-169.
36. Ehrlich HP, Lambert PA, Saggers GC, et al. Dynamic changes appearing in collagen fibers during intrinsic tendon repair. Ann Plast Surg. 2005;54(2):201-206.
37. Jarvinen TA, Jarvinen TL, Kannus P, et al. Collagen fibres of the spontaneously ruptured human tendons display decreased thickness and crimp angle. J Orthop Res. 2004;22(6):1303-1309.
38. Gelberman RH, Vande Berg JS, Lundborg GN, et al. Flexor tendon healing and restoration of the gliding surface. An ultrastructural study in dogs. J Bone Joint Surg Am. 1983;65(1):70-80.
39. Lundborg G. Experimental flexor tendon healing without adhesion formation--a new concept of tendon nutrition and intrinsic healing mechanisms. A preliminary report. Hand. 1976;8(3):235-238.
40. Sharma P, Maffulli N. Tendon injury and tendinopathy: healing and repair. J Bone Joint Surg Am. 2005;87(1):187-202.
41. Amadio PC. Friction of the gliding surface. Implications for tendon surgery and rehabilitation. J Hand Ther. 2005;18(2):112-119.
42. Zhao C, Amadio PC, Zobitz ME, et al. Gliding resistance after repair of partially lacerated human flexor digitorum profundus tendon in vitro. Clin Biomech (Bristol, Avon). 2001;16(8):696-701.
43. Zhao C, Amadio PC, Tanaka T, et al. Effect of gap size on gliding resistance after flexor tendon repair. J Bone Joint Surg Am. 2004;86-A(11):2482-2488.
44. Strick MJ, Filan SL, Hile M, et al. Adhesion formation after flexor tendon repair: a histologic and biomechanical comparison of 2- and 4-strand repairs in a chicken model. J Hand Surg Am. 2004;29(1):15-21.
45. Wang XT, Liu PY, Tang JB. Tendon healing in vitro: genetic modification of tenocytes with exogenous PDGF gene and promotion of collagen gene expression. J Hand Surg Am. 2004;29(5):884-890.
46. Elliot D, Barbieri CH, Evans RB, et al. IFSSH Flexor Tendon Committee Report 2007. J Hand Surg Eur Vol. 2007;32(3):346-356.
47. Chen CH, Cao Y, Wu YF, et al. Tendon healing in vivo: gene expression and production of multiple growth factors in early tendon healing period. J Hand Surg Am. 2008;33(10):1834-1842.
61
48. Kim HM, Nelson G, Thomopoulos S, et al. Technical and biological modifications for enhanced flexor tendon repair. J Hand Surg Am. 2010;35(6):1031-1037; quiz 1038.
49. Klein MB, Yalamanchi N, Pham H, et al. Flexor tendon healing in vitro: effects of TGF-beta on tendon cell collagen production. J Hand Surg Am. 2002;27(4):615-620.
50. Bennett NT, Schultz GS. Growth factors and wound healing: biochemical properties of growth factors and their receptors. Am J Surg. 1993;165(6):728-737.
51. Chang J, Thunder R, Most D, et al. Studies in flexor tendon wound healing: neutralizing antibody to TGF-beta1 increases postoperative range of motion. Plast Reconstr Surg. 2000;105(1):148-155.
52. Mustoe TA, Pierce GF, Thomason A, et al. Accelerated healing of incisional wounds in rats induced by transforming growth factor-beta. Science. 1987;237(4820):1333-1336.
53. Border WA, Noble NA. Transforming growth factor beta in tissue fibrosis. N Engl J Med. 1994;331(19):1286-1292.
54. Bates SJ, Morrow E, Zhang AY, et al. Mannose-6-phosphate, an inhibitor of transforming growth factor-beta, improves range of motion after flexor tendon repair. J Bone Joint Surg Am. 2006;88(11):2465-2472.
55. Zhao C, Zobitz ME, Sun YL, et al. Surface treatment with 5-fluorouracil after flexor tendon repair in a canine in vivo model. J Bone Joint Surg Am. 2009;91(11):2673-2682.
56. Jay GD, Britt DE, Cha CJ. Lubricin is a product of megakaryocyte stimulating factor gene expression by human synovial fibroblasts. J Rheumatol. 2000;27(3):594-600.
57. Schumacher BL, Block JA, Schmid TM, et al. A novel proteoglycan synthesized and secreted by chondrocytes of the superficial zone of articular cartilage. Arch Biochem Biophys. 1994;311(1):144-152.
58. Schumacher BL, Schmidt TA, Voegtline MS, et al. Proteoglycan 4 (PRG4) synthesis and immunolocalization in bovine meniscus. J Orthop Res. 2005;23(3):562-568.
59. Rees SG, Davies JR, Tudor D, et al. Immunolocalisation and expression of proteoglycan 4 (cartilage superficial zone proteoglycan) in tendon. Matrix Biol. 2002;21(7):593-602.
60. Hayashi M, Zhao C, Thoreson AR, et al. The effect of lubricin on the gliding resistance of mouse intrasynovial tendon. PLoS One. 2013;8(12):e83836.
61. Taguchi M, Sun YL, Zhao C, et al. Lubricin surface modification improves tendon gliding after tendon repair in a canine model in vitro. J Orthop Res. 2009;27(2):257-263.
62. Swann DA, Slayter HS, Silver FH. The molecular structure of lubricating glycoprotein-I, the boundary lubricant for articular cartilage. J Biol Chem. 1981;256(11):5921-5925.
62
63. Rhee DK, Marcelino J, Baker M, et al. The secreted glycoprotein lubricin protects cartilage surfaces and inhibits synovial cell overgrowth. J Clin Invest. 2005;115(3):622-631.
64. Zhao C, Sun YL, Jay GD, et al. Surface modification counteracts adverse effects associated with immobilization after flexor tendon repair. J Orthop Res. 2012;30(12):1940-1944.
65. Zhao C, Hashimoto T, Kirk RL, et al. Resurfacing with chemically modified hyaluronic acid and lubricin for flexor tendon reconstruction. J Orthop Res. 2013;31(6):969-975.
66. Zhao C, Sun YL, Kirk RL, et al. Effects of a lubricin-containing compound on the results of flexor tendon repair in a canine model in vivo. J Bone Joint Surg Am. 2010;92(6):1453-1461.
67. Szpaderska AM, DiPietro LA. Inflammation in surgical wound healing: friend or foe? Surgery. 2005;137(5):571-573.
68. Manning CN, Havlioglu N, Knutsen E, et al. The early inflammatory response after flexor tendon healing: a gene expression and histological analysis. J Orthop Res. 2014;32(5):645-652.
69. Dinarello CA. Immunological and inflammatory functions of the interleukin-1 family. Annu Rev Immunol. 2009;27:519-550.
70. Yang G, Im HJ, Wang JH. Repetitive mechanical stretching modulates IL-1beta induced COX-2, MMP-1 expression, and PGE2 production in human patellar tendon fibroblasts. Gene. 2005;363:166-172.
71. Thampatty BP, Li H, Im HJ, et al. EP4 receptor regulates collagen type-I, MMP-1, and MMP-3 gene expression in human tendon fibroblasts in response to IL-1 beta treatment. Gene. 2007;386(1-2):154-161.
72. Cilli F, Khan M, Fu F, et al. Prostaglandin E2 affects proliferation and collagen synthesis by human patellar tendon fibroblasts. Clin J Sport Med. 2004;14(4):232-236.
73. Mihara M, Hashizume M, Yoshida H, et al. IL-6/IL-6 receptor system and its role in physiological and pathological conditions. Clin Sci (Lond). 2012;122(4):143-159.
74. Legerlotz K, Jones ER, Screen HR, et al. Increased expression of IL-6 family members in tendon pathology. Rheumatology (Oxford). 2012;51(7):1161-1165.
75. Lin TW, Cardenas L, Glaser DL, et al. Tendon healing in interleukin-4 and interleukin-6 knockout mice. J Biomech. 2006;39(1):61-69.
76. Baggiolini M, Clark-Lewis I. Interleukin-8, a chemotactic and inflammatory cytokine. FEBS Lett. 1992;307(1):97-101.
77. John T, Lodka D, Kohl B, et al. Effect of pro-inflammatory and immunoregulatory cytokines on human tenocytes. J Orthop Res. 2010;28(8):1071-1077.
78. Szabo RM, Younger E. Effects of indomethacin on adhesion formation after repair of zone II tendon lacerations in the rabbit. J Hand Surg Am. 1990;15(3):480-483.
63
79. Riley GP, Cox M, Harrall RL, et al. Inhibition of tendon cell proliferation and matrix glycosaminoglycan synthesis by non-steroidal anti-inflammatory drugs in vitro. J Hand Surg Br. 2001;26(3):224-228.
80. Tan V, Nourbakhsh A, Capo J, et al. Effects of nonsteroidal anti-inflammatory drugs on flexor tendon adhesion. J Hand Surg Am. 2010;35(6):941-947.
81. Radi ZA, Khan NK. Effects of cyclooxygenase inhibition on bone, tendon, and ligament healing. Inflamm Res. 2005;54(9):358-366.
82. Bokhari AR, Murrell GA. The role of nitric oxide in tendon healing. J Shoulder Elbow Surg. 2012;21(2):238-244.
83. Murrell GA, Tang G, Appleyard RC, et al. Addition of nitric oxide through nitric oxide-paracetamol enhances healing rat achilles tendon. Clin Orthop Relat Res. 2008;466(7):1618-1624.
84. Paoloni JA, Appleyard RC, Nelson J, et al. Topical nitric oxide application in the treatment of chronic extensor tendinosis at the elbow: a randomized, double-blinded, placebo-controlled clinical trial. Am J Sports Med. 2003;31(6):915-920.
85. Paoloni JA, Appleyard RC, Nelson J, et al. Topical glyceryl trinitrate treatment of chronic noninsertional achilles tendinopathy. A randomized, double-blind, placebo-controlled trial. J Bone Joint Surg Am. 2004;86-A(5):916-922.
86. Desmouliere A, Chaponnier C, Gabbiani G. Tissue repair, contraction, and the myofibroblast. Wound Repair Regen. 2005;13(1):7-12.
87. Hinz B, Celetta G, Tomasek JJ, et al. Alpha-smooth muscle actin expression upregulates fibroblast contractile activity. Mol Biol Cell. 2001;12(9):2730-2741.
88. Wang J, Jiao H, Stewart TL, et al. Improvement in postburn hypertrophic scar after treatment with IFN-alpha2b is associated with decreased fibrocytes. J Interferon Cytokine Res. 2007;27(11):921-930.
89. Winters SC, Gelberman RH, Woo SL, et al. The effects of multiple-strand suture methods on the strength and excursion of repaired intrasynovial flexor tendons: a biomechanical study in dogs. J Hand Surg Am. 1998;23(1):97-104.
90. Nelson GN, Potter R, Ntouvali E, et al. Intrasynovial flexor tendon repair: a biomechanical study of variations in suture application in human cadavera. J Orthop Res. 2012;30(10):1652-1659.
91. Wu YF, Tang JB. Recent developments in flexor tendon repair techniques and factors influencing strength of the tendon repair. J Hand Surg Eur Vol. 2014;39(1):6-19.
92. Savage R. The search for the ideal tendon repair in zone 2: strand number, anchor points and suture thickness. J Hand Surg Eur Vol. 2014;39(1):20-29.
93. Lee SK, Goldstein RY, Zingman A, et al. The effects of core suture purchase on the biomechanical characteristics of a multistrand
64
locking flexor tendon repair: a cadaveric study. J Hand Surg Am. 2010;35(7):1165-1171.
94. Tang JB, Zhang Y, Cao Y, et al. Core suture purchase affects strength of tendon repairs. J Hand Surg Am. 2005;30(6):1262-1266.
95. Hotokezaka S, Manske PR. Differences between locking loops and grasping loops: effects on 2-strand core suture. J Hand Surg Am. 1997;22(6):995-1003.
96. Pennington DG. The locking loop tendon suture. Plast Reconstr Surg. 1979;63(5):648-652.
97. Wada A, Kubota H, Hatanaka H, et al. The mechanical properties of locking and grasping suture loop configurations in four-strand core suture techniques. J Hand Surg Br. 2000;25(6):548-551.
98. Wu YF, Tang JB. How much does a Pennington lock add to strength of a tendon repair? J Hand Surg Eur Vol. 2011;36(6):476-484.
99. Tanaka T, Amadio PC, Zhao C, et al. Gliding characteristics and gap formation for locking and grasping tendon repairs: a biomechanical study in a human cadaver model. J Hand Surg Am. 2004;29(1):6-14.
100. Moriya T, Larson MC, Zhao C, et al. The effect of core suture flexor tendon repair techniques on gliding resistance during static cycle motion and load to failure: a human cadaver study. J Hand Surg Eur Vol. 2012;37(4):316-322.
101. Moriya T, Zhao C, Yamashita T, et al. Effect of core suture technique and type on the gliding resistance during cyclic motion following flexor tendon repair: a cadaveric study. J Orthop Res. 2010;28(11):1475-1481.
102. Zhao C, Amadio PC, Momose T, et al. The effect of suture technique on adhesion formation after flexor tendon repair for partial lacerations in a canine model. J Trauma. 2001;51(5):917-921.
103. Zhao C, Amadio PC, Zobitz ME, et al. Gliding characteristics of tendon repair in canine flexor digitorum profundus tendons. J Orthop Res. 2001;19(4):580-586.
104. Pruitt DL, Aoki M, Manske PR. Effect of suture knot location on tensile strength after flexor tendon repair. J Hand Surg Am. 1996;21(6):969-973.
105. Momose T, Amadio PC, Zhao C, et al. The effect of knot location, suture material, and suture size on the gliding resistance of flexor tendons. J Biomed Mater Res. 2000;53(6):806-811.
106. Aoki M, Manske PR, Pruitt DL, et al. Work of flexion after flexor tendon repair according to the placement of sutures. Clin Orthop Relat Res. 1995(320):205-210.
107. Silva JM, Zhao C, An KN, et al. Gliding resistance and strength of composite sutures in human flexor digitorum profundus tendon repair: an in vitro biomechanical study. J Hand Surg Am. 2009;34(1):87-92.
108. Alavanja G, Dailey E, Mass DP. Repair of zone II flexor digitorum profundus lacerations using varying suture sizes: a comparative biomechanical study. J Hand Surg Am. 2005;30(3):448-454.
65
109. Wade PJ, Wetherell RG, Amis AA. Flexor tendon repair: significant gain in strength from the Halsted peripheral suture technique. J Hand Surg Br. 1989;14(2):232-235.
110. Diao E, Hariharan JS, Soejima O, et al. Effect of peripheral suture depth on strength of tendon repairs. J Hand Surg Am. 1996;21(2):234-239.
111. Moriya T, Zhao C, An KN, et al. The effect of epitendinous suture technique on gliding resistance during cyclic motion after flexor tendon repair: a cadaveric study. J Hand Surg Am. 2010;35(4):552-558.
112. Strickland JW, Glogovac SV. Digital function following flexor tendon repair in Zone II: A comparison of immobilization and controlled passive motion techniques. J Hand Surg Am. 1980;5(6):537-543.
113. Wada A, Kubota H, Miyanishi K, et al. Comparison of postoperative early active mobilization and immobilization in vivo utilising a four-strand flexor tendon repair. J Hand Surg Br. 2001;26(4):301-306.
114. Silfverskiold KL, May EJ. Flexor tendon repair in zone II with a new suture technique and an early mobilization program combining passive and active flexion. J Hand Surg Am. 1994;19(1):53-60.
115. Strickland JW. Flexor Tendon Injuries: I. Foundations of Treatment. J Am Acad Orthop Surg. 1995;3(1):44-54.
116. Small JO, Brennen MD, Colville J. Early active mobilisation following flexor tendon repair in zone 2. J Hand Surg Br. 1989;14(4):383-391.
117. Elliot D, Moiemen NS, Flemming AF, et al. The rupture rate of acute flexor tendon repairs mobilized by the controlled active motion regimen. J Hand Surg Br. 1994;19(5):607-612.
118. Starr HM, Snoddy M, Hammond KE, et al. Flexor tendon repair rehabilitation protocols: a systematic review. J Hand Surg Am. 2013;38(9):1712-1717 e1714.
119. Kleinert HE, Verdan C. Report of the Committee on Tendon Injuries (International Federation of Societies for Surgery of the Hand). J Hand Surg Am. 1983;8(5 Pt 2):794-798.
120. Adolfsson L, Soderberg G, Larsson M, et al. The effects of a shortened postoperative mobilization programme after flexor tendon repair in zone 2. J Hand Surg Br. 1996;21(1):67-71.
121. Schuind F, Garcia-Elias M, Cooney WP, 3rd, et al. Flexor tendon forces: in vivo measurements. J Hand Surg Am. 1992;17(2):291-298.
122. Powell ES, Trail IA. Forces transmitted along human flexor tendons during passive and active movements of the fingers. J Hand Surg Br. 2004;29(4):386-389.
123. Dennerlein JT, Diao E, Mote CD, Jr., et al. In vivo finger flexor tendon force while tapping on a keyswitch. J Orthop Res. 1999;17(2):178-184.
66
124. Kursa K, Lattanza L, Diao E, et al. In vivo flexor tendon forces increase with finger and wrist flexion during active finger flexion and extension. J Orthop Res. 2006;24(4):763-769.
125. Boyer MI, Gelberman RH, Burns ME, et al. Intrasynovial flexor tendon repair. An experimental study comparing low and high levels of in vivo force during rehabilitation in canines. J Bone Joint Surg Am. 2001;83-A(6):891-899.
126. Hatanaka H, Zhang J, Manske PR. An in vivo study of locking and grasping techniques using a passive mobilization protocol in experimental animals. J Hand Surg Am. 2000;25(2):260-269.
127. Aoki M, Kubota H, Pruitt DL, et al. Biomechanical and histologic characteristics of canine flexor tendon repair using early postoperative mobilization. J Hand Surg Am. 1997;22(1):107-114.
128. Gelberman RH, Boyer MI, Brodt MD, et al. The effect of gap formation at the repair site on the strength and excursion of intrasynovial flexor tendons. An experimental study on the early stages of tendon-healing in dogs. J Bone Joint Surg Am. 1999;81(7):975-982.
129. Nilsson E, Bjorn C, Sjostrand V, et al. A novel polypeptide derived from human lactoferrin in sodium hyaluronate prevents postsurgical adhesion formation in the rat. Ann Surg. 2009;250(6):1021-1028.
130. Wiig M, Olmarker K, Hakansson J, et al. A lactoferrin-derived peptide (PXL01) for the reduction of adhesion formation in flexor tendon surgery: an experimental study in rabbits. J Hand Surg Eur Vol. 2011;36(8):656-662.
131. Hakansson J, Mahlapuu M, Ekstrom L, et al. Effect of lactoferrin peptide (PXL01) on rabbit digit mobility after flexor tendon repair. J Hand Surg Am. 2012;37(12):2519-2525.
132. Wiig ME, Dahlin LB, Friden J, et al. PXL01 in Sodium Hyaluronate for Improvement of Hand Recovery after Flexor Tendon Repair Surgery: Randomized Controlled Trial. PLoS One. 2014;9(10):e110735.
133. Jaibaji M. Advances in the biology of zone II flexor tendon healing and adhesion formation. Ann Plast Surg. 2000;45(1):83-92.
134. Wu YF, Tang JB. Effects of tension across the tendon repair site on tendon gap and ultimate strength. J Hand Surg Am. 2012;37(5):906-912.
135. Dy CJ, Hernandez-Soria A, Ma Y, et al. Complications after flexor tendon repair: a systematic review and meta-analysis. J Hand Surg Am. 2012;37(3):543-551 e541.
136. Moriya K, Yoshizu T, Maki Y, et al. Clinical outcomes of early active mobilization following flexor tendon repair using the six-strand technique: short- and long-term evaluations. J Hand Surg Eur Vol. 2015;40(3):250-258.
137. Rigo IZ, Rokkum M. Predictors of outcome after primary flexor tendon repair in zone 1, 2 and 3. J Hand Surg Eur Vol. 2016;41(8):793-801.
67
138. Reno C, Marchuk L, Sciore P, et al. Rapid isolation of total RNAfrom small samples of hypocellular, dense connective tissues.Biotechniques. 1997;22(6):1082-1086.
139. Baktir A, Turk CY, Kabak S, et al. Flexor tendon repair in zone 2followed by early active mobilization. J Hand Surg Br.1996;21(5):624-628.
140. Sapienza A, Yoon HK, Karia R, et al. Flexor tendon excursion andload during passive and active simulated motion: a cadaver study. JHand Surg Eur Vol. 2013;38(9):964-971.
141. Hildebrand KA, Frank CB, Hart DA. Gene intervention in ligamentand tendon: current status, challenges, future directions. Gene Ther.2004;11(4):368-378.
142. de Vos RJ, Weir A, van Schie HT, et al. Platelet-rich plasmainjection for chronic Achilles tendinopathy: a randomized controlledtrial. Jama. 2010;303(2):144-149.
143. Majewski M, Ochsner PE, Liu F, et al. Accelerated healing of the ratAchilles tendon in response to autologous conditioned serum. Am JSports Med. 2009;37(11):2117-2125.
144. Manning CN, Schwartz AG, Liu W, et al. Controlled delivery ofmesenchymal stem cells and growth factors using a nanofiberscaffold for tendon repair. Acta Biomater. 2013;9(6):6905-6914.
145. Muller SA, Todorov A, Heisterbach PE, et al. Tendon healing: anoverview of physiology, biology, and pathology of tendon healingand systematic review of state of the art in tendon bioengineering.Knee Surg Sports Traumatol Arthrosc. 2013.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1307
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-316559
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2017























![Flexor Tendon Injuries[1]](https://img.pdfslide.us/doc/110x75/546eeaf2b4af9f8c068b465a/flexor-tendon-injuries1-558457890f347.jpg)

