Embed Size (px)
Citation preview

IFC
TTlrdtsjtrt
SSoetlaTrw
RA
1d
njuries of the Flexor Tendons:ocus on the Superficial Digital Flexor Tendonhristopher B. O’Sullivan, BVSc, MS, Dip ACVS
Of the two flexor tendons in horses’ lower limbs, the superficial digital flexor tendon is morecommonly injured than the deep digital flexor tendon. Flexor tendon injuries are caused byeither overstrain of the tendon or direct trauma. Overstrain injuries have a typical swellingof the tendon that requires ultrasonographic evaluation to confirm the diagnosis. Treatmentof these injuries includes anti-inflammatory therapy initially followed by a rehabilitationprogram. New therapies are emerging for modulating healing of these injuries. Flexortendon lacerations are usually the result of direct penetrating trauma to the limb. Manage-ment of these injuries includes surgical management combined with appropriate coapta-tion. Involvement of a tendon sheath complicates management with the potential formationof septic tenosynovitis. The prognosis for returning successfully to athletic function in thecase of overstrain injuries is fair, but re-injury is common, and for tendon lacerations, it isguarded to poor.Clin Tech Equine Pract 6:189-197 © 2007 Elsevier Inc. All rights reserved.
KEYWORDS horse tendon, superficial digital flexor tendon, deep digital flexor tendon, bowedtendon, overstrain injury, tendon laceration
yjl
rjodh
cmcd
Flocfiioirbsi
he flexor tendons of horses’ lower limbs are importantweight-bearing structures at rest and during locomotion.
he anatomic arrangement of tendons and joints in the lowerimb provides an efficient transfer of muscular energy forapid locomotion. Of the two flexor tendons, the superficialigital flexor tendon (SDFT) is more commonly injured thanhe deep digital flexor tendon (DDFT). The SDFT provides apring-like store of energy in the galloping horse and is sub-ect to strains close to its mechanical limits, making it suscep-ible to overstrain injuries. Tendon damage may occur as aesult of either overstrain of the tendon or a traumatic pene-rating injury.
train-Induced Tendon Injuriestrain-induced tendon injuries are seen relatively commonlyver a variety of different equine sporting disciplines. Mostquine athletes place loads on the flexor tendons duringraining and competition that are close to the physiologicimit of the tendon. Thoroughbred racehorses appear to trainnd compete closer to this limit than other equine athletes.1
he incidence of flexor tendon injuries in Thoroughbredacehorses ranges from 8% to 43% in different populations,ith the injuries being more prevalent in horses older than 2
andwick Equine Centre, Randwick.ddress reprint requests to: Christopher B. O’Sullivan, Randwick Equine
Centre, PO Box 195, Randwick, NSW, 2031, Australia. E-mail:
[email protected]534-7516/07/$-see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1053/j.ctep.2007.08.005
ears of age.2-8 In racing Thoroughbreds, SDFT forelimb in-uries predominate, and a slight predilection for injury to theead or inside leg exists.3
Non-racehorse athletes also suffer from a variety of strain-elated tendon injuries. SDFT injuries are commonly seen inumpers, eventers, and polo ponies. Dressage horses, on thether hand, rarely injure their SDFT and are more likely toevelop a DDFT injury either in the metatarsal region of theind limb or in the palmar heel region of the forelimb.Since tendons are operating close to their load-bearing
apacity in sport horses, there is little leeway for factors thatay increase loading on the tendon. A variety of factors may
ontribute to an injury by increasing the peak loads on ten-ons during exercise, and some of these are discussed below.
oot Balance. Poor foot balance, particularly low heels andong toes, has traditionally been suggested to increase the riskf tendon injuries. This has not been supported by biome-hanical studies which suggest the possibility that this con-ormation is protective.9 Current research suggests that rais-ng a horse’s heel will decrease the load on the DDFT,ncreasing fetlock joint extension and subsequently the loadn SDFT and suspensory.10,11 Further studies looking at thenfluence of foot balance at high speed on tendon strains areequired. With this contradiction in mind, attempts shoulde made to obtain an ideal neutral foot balance. With anyudden changes in foot balance, even in cases where it ismproved, it is wise to allow a period of adaptation before
aximally loading the tendon.
189

Tsatppcmaaitm
FstraFci
Cmt
Wwp
tjpswmllhrlo
istltBcfioota
toar
tfltfla
DOctltbbbmitoimwi
ito
Ftti
190 C.B. O’Sullivan
rack Surfaces. Tracks that are very hard result in higherpeeds and increased peak impact loads.12 These fast tracksre therefore more likely to produce overstrain injuries ofendons. However, tracks where the surface is uneven, slip-ery, or shifty seem also to contribute to damaging loadingatterns on tendons. Numerous factors influence the me-hanical behavior of a track surface; the weather and trackaintenance have a major influence. Moisture content affects
ll tracks’ mechanical properties, and extreme temperaturesppear to affect some synthetic tracks’ mechanical character-stics dramatically. Experience over years with a particularrack type will allow identification of track conditions thatay predispose to tendon injuries.
atigue. Fatigue is influenced primarily by the horse’s workchedule, level of fitness, and intensity of competition. Fa-igue should be considered as a contributor to tendon inju-ies. With the onset of muscle fatigue, a horse’s stride char-cteristics change,13 altering the forces on the tendons.atigue in any sport results in an inevitable loss of form andoordination in each stride, which is likely to result in anncrease risk of injury.
ontralateral Limb Lameness. At high speed, lamenessay result in excessive loading of the tendons in the con-
ralateral limb.
eight. Horses who are overweight or carrying excesseight will produce greater forces on their tendons com-ared with lower weight individuals.
Overstrain may occur as either an isolated incident or dueo accumulation of repetitive strains. Isolated overstrain in-uries are seen when the tendon receives a single bout of extra-hysiologic load. This may be caused by excessive bouts of high-peed exercise or a single excess force on the tendon, such ashen jumping an excessive height. Alternatively, tendonsay be injured if they receive a knock while under heavy
oad, causing a sudden increase in strain locally within theoaded tendon. Occasionally peripheral tendon injuries willave an accompanying skin contusion; these are likely theesult of a direct damaging blow on the loaded tendon. Iso-ated overload injuries are an uncommon cause of tendonverstrain in normal tendons.Repetitive strain is the most common scenario contribut-
ng to tendon overstrain injuries. Since tendons accumulateubclinical micro-damage with age and progressive cycling,he tendon becomes weaker and less able to cope with a givenoad. This progresses to a point where the tendon is subjectedo a level of strain which it previously could have dealt with.ut due to its loss of elasticity and strength, the tendon be-omes overloaded, which results in disruption of the tendonbers and a clinical tendon injury. These injuries typicallyccur at or just below the mid metacarpal level in the “core”r central region of the SDFT. This area of the SDFT appearso be preferentially loaded and degenerates more with agend exercise than other areas within the tendon.14
While a core lesion of the mid or distal metacarpal SDFT ishe most common presentation, injuries are seen at all levelsf the tendon from insertion to musculotendinous junction,ffecting the core or tendons periphery. Distal tendon inju-
ies within the digital sheath are also relatively common. The gendon and ligament structures associated with the digitalexor sheath are anatomically complex. Injuries may involvehe SDFT and/or its related structures, such as the manicaexoria, DDFT, sesamoidean ligaments, or palmar/plantarnnular ligament.
iagnosisbservation of the flexor tendons profile combined with
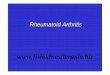
areful palpation are the first steps in clinical assessment of aendon injury (Fig. 1). The change in profile of the back of theimb associated with overstrain tendon injuries is the deriva-ion of the term “bowed tendon.” Palpation of the tendonetween thumb and forefinger with the limb both weight-earing and non-weight-bearing allows subtle thickening toe identified. When holding the limb up, work along theargins between the SDFT and DDFT. During weight-bear-
ng, ensure that the branches of the SDFT in the pastern andhe proximal tendon/musculotendinous junction at the levelf the carpus are carefully assessed for enlargement. The dig-tal and carpal sheaths should be assessed for effusion. When
oderately firm palpation of a thickened area of the tendonhile non-weight-bearing elicits an obvious pain response, it
s highly likely that there is an active tendonitis present.The lameness associated with SDFT tendon injuries is typ-
cally fairly mild, approximately 1 to 2 grades out of 5 at therot on firm ground.15 Lameness seems to improve rapidlyver the first week. Very mild tendonitis cases may not be
igure 1 Palpation of the SDFT, assessing both the thickness of theendon and its profile. There is a subtle change in the contour andhickness of the SDFT in the distal third of the metacarpus, indicat-ng the likelihood of a tendon injury and the need for ultrasono-
raphic assessment. (Color version of figure is available online.)
lnapi
ievtd
clpotbm
utabstuo
tdTw
lwg
TATcsiicmMtim
TPihio
REs
etupsi
mflmmigwimbp6ata
PTpsSnbhol
obtla
BPcautpTtstctttr
Injuries of the flexor tendons 191
ame at all. However, in rare cases, a significant severe lame-ess may accompany a moderate tendonitis. There does notppear to be a good correlation between the level of pain onalpation and lameness with the severity of the lesion, except
n the most severe of lesions.Clinically apparent swelling, heat, and pain on palpation
ndicate the need for careful ultrasonographic evaluation. Re-valuation of a tendon at 1 to 3 weeks after injury may pro-ide a more accurate indication of lesion severity and is par-icularly important when a lesion is suspected but not wellefined on the initial examination.4,5,16,17
A quality ultrasound examination is essential for identifi-ation and documentation of the position and severity of theesion. An ultrasound machine with a linear 7.5- to 10-Mzrobe with a stand-off is a suitable machine for the evaluationf the majority of flexor tendon injuries. Both the clinicalendon and the contralateral clinically normal tendon shoulde examined, because subclinical ultrasonographic changesay be noted in the normal tendon.Severity of the injury is determined based on the following
ltrasonographic measurements assessed systematically downhe limb: echogenicity of the lesion, cross-sectional area (CSA) offfected and contralateral tendon, percentage CSA occupiedy the lesion, and position and length of the lesion. A scoringystem using some of the above measurements has been usedo categorize the severity of SDFT injuries.18 This may beseful for prognostication and ultrasonographic monitoringf healing.19
Within the confines of tendon sheaths, ultrasound may failo demonstrate some lesions, including longitudinal tears ofigital flexor tendons or tears of the manica flexoria.20,21
enoscopy offers both diagnostic and therapeutic optionshen a tendon lesion is suspected within a tendon sheath.21
While a tendon injury is suspected, the horse’s activityevel should be limited to stall rest, with only limited handalking until injury to the tendon can be ruled out ultrasono-raphically or tenoscopically.
reatmentnti-Inflammatory Therapyhe aim of early and rapid control of the inflammatory cas-ade is to minimize further damage to the tendon structureecondary to the inflammatory response. Non-steroidal anti-nflammatory drugs are indicated as the mainstay of anti-nflammatory therapy for tendon injuries; a 3- to 5-dayourse is typical. A single dose of short-acting corticosteroidsay offer a more potent initial anti-inflammatory effect.edical therapy is combined with physical anti-inflamma-
ory therapies, including cold therapy for 5 days (20 minutescing, 3 times daily) and pressure bandaging for approxi-
ately 3 to 4 weeks.
herapies Aimed at Modulating More Ideal Healingolysulfated glycosaminoglycans (PSGAGs) have also been
ndicated to be beneficial during the early phase of tendonealing.22,23 Other therapies aimed at production of the most
deal healing tissue include the use of growth factors (IGF-1)r stem cells.
ehabilitation Programsxercise and mobilization of the healing tendon can begin
oon after injury once the inflammation is subsiding. How- gver, if the horse is lame or the injury is severe enough thathere is loss of fetlock support, then this should be delayedntil it is judged that suitable healing has taken place torevent further damage. At this stage, the horse’s foot balancehould be corrected if required and carefully maintained dur-ng the rehabilitation period.
A graded exercise program is the mainstay of therapy andany have been suggested.19,24,25 The program should beexible and adjusted based on the severity of the injury andonitored by regular clinical and ultrasonographic assess-ent of the tendon. Typically, walking commences once the
nflammatory phase has subsided after the fist week, withradually increasing duration. Trotting is introduced after 12eeks and cantering after approximately 32 weeks. Race train-
ng is not usually resumed until approximately 48 weeks, withany horses requiring longer. Typically, the total time required
efore re-introduction to race training is 8 to 12 months; a worserognosis is documented for horses rested for less thanmonths.5,17,25 Controlled exercise rehabilitation programsppear to dramatically improve the numbers of horses re-urning to competition compared with pasture turnoutlone.19
rognosishe prognosis for SDFT injuries in the Thoroughbred is re-orted to range from 20% to 60% of horses returning touccessful racing and up to 80% sustaining a re-injury.5,26-29
tandardbred racehorses and sport horses have a better prog-osis for successful return to competition than Thorough-red racehorses. Ultimately, the severity of the damage willave a major influence on the outcome. A significant numberf horses with re-injuries occur in the opposite unaffectedimb.
Although not recommended due to safety concerns, racingr competition can continue with mildly damaged tendons,ut progressive damage to the tendon will occur, worseninghe long-term prognosis. Standardbred racehorses are moreikely to successfully compete and for a longer duration withn acute tendon injury than Thoroughbred racehorses.
andage Bowseritendinous inflammation “bandage bow” may sometimeslinically resemble a tendonitis. The inflammation is usuallyssociated with trauma to the limb caused by blunt force orneven excessive pressure applied by a bandage. Clinically,here is apparent tendon swelling, typically with less intenseain on palpation when compared with tendonitis cases.here is no damage to the tendon itself; however, the subcu-
aneous and peritendinous tissues become inflamed andwollen. Palpation of the tendon margins is difficult due tohe subcutaneous and peritendinous swelling. Ultrasoundonformation of the diagnosis is often required to rule outendonitis. Treatment consists of aggressive anti-inflamma-ory therapy and cessation of pace work until all inflamma-ion has resolved.30,31 Slow resolution of inflammation oresidual thickening should prompt a follow-up ultrasono-
raphic examination.
TTotfihcoda
AAcimeaoadptDmcrofa
ew
fiwstdsb
tetidctt
tatacsiistpb
WWoetea
NNbpaoapCpa
asab
atspt
Fps
192 C.B. O’Sullivan
endon Lacerationsendon lacerations occur most commonly as a consequencef paddock accidents, transport injuries, or during competi-ion caused by other horses or self-inflicted. The impactorces involved in tendon lacerations that occur during rac-ng or competition are particularly high. Relatively bluntorseshoes can cause disruption of whole tendons with ac-ompanying severe skin and soft tissue injuries. The severityf tissue damage is often not apparent for a couple of daysue to vascular damage and deep bruising. These injuries arelso usually heavily contaminated with sand and dirt.
ssessmentssessment of distal limb wounds that may involve tendonsommences with observation of the horse while weight-bear-ng on the affected limb and at the walk. Horses are typically
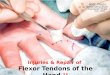
ild to moderately lame at the walk with acute tendon lac-rations. Evaluation of fetlock angle while weight-bearingnd at the walk provides information regarding compromisef its major support structures, the SDFT and the suspensorypparatus. Damage to either of these structures results inropping of the fetlock (hyperextension of the metacarpo-halangeal joint). With complete laceration of the SDFT,here is significant dropping of the fetlock (Fig. 2). TheDFT, on the other hand, offers limited fetlock support butaintains the foot in its position while weight-bearing. A
omplete loss of DDFT support results in the toe becomingaised off the ground while weight-bearing (hyperextensionf the distal interphalangeal joint). In the case where theetlock is dropped and the toe is elevated, then both SDFTnd DDFT have been lacerated.
A thorough knowledge of the anatomy of the distal limb isssential to identify structures that may be involved in a givenound. Thorough exploration of the wound with a gloved
igure 2 Complete laceration of the SDFT results in moderate drop-ing of the fetlock joint (metacarpophalangeal joint hyperexten-
rion).
nger is essential with the limb weight-bearing and non-eight-bearing, to assess both tendon damage and other
tructures involved. Palpation of both lacerated ends of aendon may not always be possible due to retraction of ten-on ends and the fact that the skin wound may not corre-pond with the tendon laceration when at rest or non-weight-earing.If it is suspected that there is significant compromise to a
endon, either a complete laceration or more than 50% lac-rated, an obviously dropped fetlock, or an elevated toe, thenhe horse’s limb should be immobilized for transport to min-mize any further damage. Ongoing loss of tendon supportue to vascular injury, progressive infection, or inadequateoaptation can occur. This may result in progressive damageo the remaining tendon tissue and subsequent tendon rup-ure up to 2 weeks post injury.
If the wound is over a synovial structure, most commonlyhe digital palmar/plantar sheath, then it should be appropri-tely assessed for any communication with the wound. Po-ential trauma to bones near the injury site should also bessessed radiographically. Sesamoid and splint bones are oc-asionally damaged with tendon lacerations. Bone phasecintigraphy may be of assistance after the first week if bonenvolvement is suspected but radiographic evidence is lack-ng. This is particularly useful in cases of septic osteitis of aesamoid bone. With some severe injuries, blood supply tohe distal limb may be compromised. Doppler ultrasonogra-hy or vascular phase scintigraphy 48 hours post injury maye useful to determine viability of the distal limb.
ound Management and Debridementound management will depend primarily on the location
f the tendon injury and most importantly whether the lac-ration involves the sheathed section of a tendon. The dura-ion of the injury and its level of contamination or the pres-nce of infection will determine initial management aimed atvoiding or resolving infection.
on-Sheathed Flexor Tendon Lacerationson-sheathed flexor tendon lacerations heal predominatelyy an intrinsic healing process. The epitenon and endotenonrovide the majority of progenitor cells for scar formationnd healing of the tendon defect. With this in mind, the aimf tendon laceration repair in this region should be to realignnd reduce the gap between the lacerated tendon ends andreserve their blood supply for the intrinsic healing process.areful anatomic reconstruction of the surrounding tissues,articularly the paratenon, will minimize adhesion formationnd preserve tendon gliding function.
Wounds that are relatively clean caused by sharp objectsnd of short duration (typically less than 6 hours old) areuitable for immediate primary repair. Whereas wounds thatre contaminated, caused by blunt objects, or infected areetter candidates for delayed primary closure.Tendons suitable for primary repair should be debrided of
ll contaminated or avascular tissue. The skin, subcutaneousissues, lacerated tendon, and paratenon all usually requireome debridement. Limited debridement is preferred if arimary closure is to be achieved. Assessing the vascularity ofhe tendon ends is difficult in acute wounds since tendons are
elatively avascular structures and active hemorrhage is not
pasi
wamthtvlcd
flotrlpatlsa
whtdnsBgi
bpitsdtsfp
SSetT
Injuries of the flexor tendons 193
articularly obvious during debridement. With that in mind,ll frayed and discolored tendon is likely avascular andhould be debrided along with nonviable or heavily contam-nated subcutaneous tissues.
Delayed repairs can usually be performed any time theound has reached a suitable clean contaminated status. Ide-
lly the tendon is repaired within a week of injury. In theeantime, the wound may be wet to dry bandaged once or
wice daily using sterile technique and bandages while theorse is treated with broad spectrum antibiotics. The advan-ages of a delayed repair include accurate assessment of theascularity of damaged tendon and skin. Retraction of theacerated tendon ends and skin edges is a disadvantage thatan make primary closure and gap minimization difficult inelayed repairs.Tenorraphy should be considered for all non-sheathed
exor tendon lacerations which involve a significant amountf the tendon approximately 50% or greater. However, anyendon laceration that could be better aligned with a tenor-aphy apposing its lacerated ends would benefit. The three-oop pulley and the compound locking loop are the two mostopular suture patterns.31 The three-loop pulley is easier topply, results in less suture material in the wound, and seemso align the tendon ends with less crimping than the lockingoop. The preferred suture material is a monofilament ab-orbable suture (Maxon-polyglyconate or PDS-polydiox-none) which maintains adequate strength over the initial 4
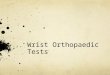
Figure 3 A partial SDFT laceration, with approximatelyafter injury showing a moderately contaminated wound.placed on antibiotics. (B) The wound on day 5 ready forwas performed and the paratenon has been closed overof the remaining subcutaneous tissues and skin. A smal
drainage. (Color version of figure is available online.)eeks of healing. The distal limb typically requires beingeld in mild flexion while the tendon is being sutured; it willhen be cast in a similar position. If the tendon ends areebrided or there is loss of a portion of the tendon, then it isot unusual to have a gap at the tenorraphy site with theutures providing alignment and preventing further gapping.ioabsorbable matrices and autologous extensor tendonrafts are currently being investigated, which may be usefuln these situations where a gap is left.32
When a tenorraphy is performed, it is advantageous foroth blood supply and gliding function to close thearatenon over the repaired tendon. It can be difficult to
dentify and close in acute cases; it is often more easily iden-ified and utilized in delayed repairs. The subcutaneous tis-ues and skin are then closed, and typically a small longitu-inal stab incision needs to be placed through the skin distalo the repair to assist drainage (Fig. 3). The stab is usuallyufficient without the need for a drain. A cast is the most idealorm of coaptation for tendon lacerations after primary re-air.
heathed Flexor Tendon Lacerationsheathed flexor tendon lacerations heal by a predominatelyxtrinsic process where the progenitor cells for scar forma-ion are derived from the tendon sheath’s synovial lining.his creates complications with the formation of restrictive
the tendon affected. (A) Day of presentation 24 hoursound was wet to dry bandaged for 4 days and the horseed primary closure. (C) A three-loop pulley tenorraphyorraphy site. (D) This was followed by primary closurencision has been placed distal to the closure to provide
50% ofThe w
a delaythe tenl stab i

at
soimdr
tisIetss
abvctd
wosbcTamri
CMtlttLbmsdwhcf
CAmtutbp
maiol
tdbfltoSiit
drra
STlWaetewp
flt
Ft
194 C.B. O’Sullivan
dhesions between structures within the sheath occurring inhe majority of cases.
Most severe lacerations within sheaths heal as one largecar resulting in tendons adhered to the sheath wall, eachther, and in some cases complete ablation of the sheathtself. This can result in significant ongoing lameness and in
any cases complete loss of the gliding function of the ten-ons within the sheath. Cases with severe discomfort mayequire a fetlock arthrodesis to become paddock sound.
The major complicating factor with sheathed lacerations ishe development of septic tenosynovitis. If the sheath is likelynfected, bacterial culture and sensitivity samples should beubmitted to determine appropriate antimicrobial therapy.deally these cases are dealt with by debridement under gen-ral anesthesia as soon after injury as possible with the aid ofenoscopy. This allows removal of foreign material from theheath, debridement of the injured structures within theheath, and copious lavage to reduce the bacterial load.
Septic tenosynovitis is managed with antibiotics, lavage,nd drainage. Appropriate antibiotic parenteral therapy maye augmented by intravenous limb perfusion and intrasyno-ial delivery. Adequate lavage and drainage is required andan be provided by a variety of methods, including tenosyno-omy, combined with daily lavage or indwelling lavage andrainage systems.This creates major problems regarding management of the
ound and sheath combined with coaptation. The majorityf unsuccessful cases seem to be due to the development ofupport limb laminitis. Case management is on an individualasis determined by the severity of the injury, the need foroaptation, level of comfort, and the presence of infection.ypically splints such as the Kimzey splint are useful initially,nd casts only become indicated once the risk of infection isinimal. Currently, tenorraphy within tendon sheaths is not
ecommended with failure of the technique to achieve heal-ng even under ideal conditions.33
oaptationany forms of coaptation are available for management of
endon lacerations. The appropriate choice depends on theevel of support and mobility required and the need to accesshe wound. Tendon lacerations affecting greater than 50% ofhe tendon warrant coaptation in the form of cast or splint.acerations that are smaller with an accompanying woundenefit from the immobility to assist healing of the skin andinimizing the size of the scar. Complete tendon lacerations
hould be cast for a minimum of 6 to 8 weeks and providedecreasing coaptation after this period up to 12 weeks. At 6eeks, the breaking strength of the tendon approximates theorse’s body weight.34 At this stage, they are likely suitable toome out of a cast and be managed with a less supportiveorm of coaptation, such as a modified fetlock support shoe.
astswell-applied cast offers the most ideal form of overall im-obilization for repaired or healing flexor tendon lacera-
ions. For forelimbs, generally a distal limb cast is sufficientnless the injury is extremely high in the proximal third ofhe tendon, in which case a full-limb cast would be moreeneficial from both a mechanical and wound position stand-
oint. Hindlimb flexor tendon lacerations are, in theory, best panaged with a full limb cast to immobilize the reciprocalpparatus, since the action of flexing the tarsus results inncreased strains on the SDFT. However, tendon lacerationsccurring in the distal two-thirds of the metatarsus in hind-imbs can be managed adequately with only a distal limb cast.
When placing casts in cases with a loss of fetlock support,he limb is ideally placed such that weight-bearing occursown the boney column (with the dorsal cortices of theones in the lower limb aligned and the fetlock in a degree ofexion) (Fig. 4). The limb is then not relying on the damagedendon ligament structures down the palmar/plantar surfacef the limb for support, reducing the strain on the healingDFT. If a limb with loss of fetlock support is placed in a castn a normal weight-bearing position, the fetlock will subsidento the cast and a large pressure sore will develop rapidly onhe palmar distal aspect of the fetlock (Fig. 5).
Slightly more fetlock flexion is required for a hindlimbistal limb cast to minimize the pull of the reciprocal appa-atus on the SDFT. In this position, the contralateral limb willequire an elevated shoe to attempt to even limb lengths;lternatively, the horse can be placed in a sand stall.
plintshe most commonly applied commercial splint is the fore-
imb model Kimzey leg saver splint (Kimzey Metal Products,oodland, CA).35 It is designed as an emergency device to be
pplied to limbs with loss of palmar/plantar support. It isxcellent for initial management of tendon lacerations, par-icularly for transport to a referral facility. The ability to gainasy access to the limb makes it useful for managing horsesith tendon sheath injuries and wounds destined for delayedrimary closure and requiring regular wound access.The forelimb model splint can be modified to best fit either
orelimbs or hindlimbs by bending the upright section at theevel of the distal interphalangeal joint or the fetlock joint forhe desired fit (http://www.kimzeymetalproducts.com). Placing
igure 4 When casting a complete SDFT laceration. The dorsal cor-ices of the bones in the lower limb are aligned, and the fetlock is
laced in a degree of flexion.
tobswhbstal
iett
blamwr
Fwia
Fsb
FKo
F
Injuries of the flexor tendons 195
he horse in a sand stall or alternately welding a flat base platen the splint will provide a more stable platform for weight-earing (Figs. 6 and 7). Maintaining a horse in a Kimzeyplint becomes progressively difficult beyond the first weekith the development of pressure sores, particularly of theeels, palmar fetlock, and dorsal proximal cannon. Carefulandaging and the use of orthopedic felt at these predisposedites can extend its useful duration. Managing a horse longerhan 3 weeks comfortably in the splint is extremely difficult,nd the subsequent splint rubs can then make casting theimb extremely difficult.
Other forms of more basic splints have been described,ncluding dorsal and plantar splints, but they are useful formergency transport only and are of limited use for long-erm management.35,36 Board splints and other modifica-ions, such as the Hitchcock splint, have been described for
igure 5 If a complete SDFT laceration has the limb cast in a normaleight-bearing position, the fetlock will drop in the cast and result
n pressure and rapid development of pressure necrosis of the skint this site on the palmar distal aspect of the fetlock joint.
igure 6 Two different forelimb model Kimzey splints. (Right) Thetandard; (Left) a modified splint with a baseplate welded onto the
ottom of the splint. (Color version of figure is available online.) soth emergency and long-term management for loss of fet-ock support due to traumatic disruption of the suspensorypparatus.37 These devices can also be utilized in manage-ent of tendon lacerations. However, horses are rarely fullyeight-bearing in these types of splints and run an increased
isk of support limb laminitis.
igure 7 A horse comfortably standing with a forelimb modelimzey splint in a sand stall. (Color version of figure is availablenline.)
igure 8 A version of the Roberts fetlock support shoe. (Color ver-
ion of figure is available online.)
SMFtschbhoidwowpEbmtmm
PTgts1r5
lalaoflfnp
AIag
R
1
1
1
1
1
tape. (C
196 C.B. O’Sullivan
upport Shoes andodified Shoe Splint Combinations
etlock support shoes, such as the Roberts shoe, are an op-ion for providing fetlock support for SDFT injuries that canuitably bear some weight but are at risk of damage if notoapted (Fig. 8). They are typically used once the level ofealing is adequate to take strains consistent with the horse’sody weight. The author uses a combination of an extendedeel shoe combined with a palmar splint attached to the shoe,ffering fetlock support in cases which don’t need completemmobilization but require more support than a heavy ban-age alone. It is a modification of the fetlock support shoeith some additional support provided up the palmar surfacef the limb (Fig. 9). This form of shoe splint combinationorks well for both SDFT injuries offering some fetlock sup-ort and for DDFT injuries offering the extended heel shoe.xtended heel shoes alone offer limited support to the SDFTut offer excellent support for the DDFT. The heel extensionust be very generous to have maximal effect, ideally as far as
he palmar/plantar fetlock. This shoe splint set up is able to beaintained for a prolonged period of time if required withinimal complications.
rognosishe prognosis for survival with flexor tendon lacerations isood with 1 retrospective review of 50 cases of digital flexorendon lacerations having 78% survival at 1 year, with similarurvival rates for partial lacerations or complete lacerations ofor both tendons.38 The same study found the prognosis for
eturn to athletic endeavor to be fair; a retrospective review of0 cases reported a return to function of 54%.38
Although not supported by studies, the prognosis for ath-etic return is assumed to be more favorable for partial lacer-tions of tendons compared with full lacerations, and hind-imbs carry a better prognosis than forelimbs. Involvement oftendon sheath with a tendon laceration impacts negativelyn the prognosis due to the potential for sepsis of the digitalexor tendon sheath affecting both survival and return to
unction. Early treatment is advised with an improved prog-osis when tenoscopic lavage, debridement, and repair are
Figure 9 A modified shoe splint combination used to prgauze placed under fetlock. (C) With the palmar splintbandaged to the limb it compresses the gauze roll and slimb and the rolled gauze is all taped up with adhesive
erformed within 36 hours of injury.39
cknowledgmentsthank Kip Carter for graphics and art work on Figures 2, 4,nd 5; and thanks to Charlie Hayward for photography andraphics on Figures 1, 3, 5-9.
eferences1. Smith RKW: Pathophysiology of tendon injury, in Dyson SJ, Ross MW
(eds): Diagnosis and Management of Lameness in the Horse. St. Louis,MO, 2003, pp 616-628
2. Wilson JH, Robinson RA, Jensen RC, et al: Equine soft tissue injuriesassociated with racing: descriptive statistics from American racetracks,in Dubai International Equine Symposium Proceedings: “The equineathlete: tendon, ligament and soft tissue injuries” 1:1-21, 1996
3. Rooney JR, Genovese A: Survey and analysis of bowed tendon in Thor-oughbred racehorses. J Equine Vet Sc 1:49-53, 1981
4. Genovese RL, Rantanen NW, Simpson BS, et al: Clinical experiencewith quantitative analysis of superficial digital flexor tendon injuries inThoroughbred and Standardbred racehorses. Vet Clin North AmEquine Pract 6:129-147, 1990
5. Genovese RL: Prognosis of superficial flexor tendon and suspensoryligament injuries, in Proceedings of the 39th Annual AAEP Convention,1993, pp 9-10
6. Goodship AE: The pathophysiology of flexor tendon injury in thehorse. Equine Vet Educ 5:23-29, 1993
7. Dowling BA, Dart AJ, Hodgson DR, et al: Superficial digital flexortendonitis. Equine Vet J 32:369-378, 2000
8. Gibson KT, Burbridge HM, Pfeiffer DU: Superficial digital flexor tendonitisin Thoroughbred racehorses: outcome following non-surgical treatmentand superior check desmotomy. Aust Vet J 75:631-635, 1997
9. Riemersma DJ, van den Bogert AJ, Jansen MO, et al: Influence of shoe-ing on ground reaction forces and tendon strains in the forelimb ofponies. Equine Vet J 28:126-132, 1996
0. Crevier-Denoix N, Roosen C, Kardillat C, et al: Effects of heel and toeelevation upon the digital joint angles in the standing horse. Equine VetJ 33:74, 2001 (suppl)
1. Eliashar E, McGuigan MP, Wilson AM: Relationship of foot conforma-tion and force applied to the navicular bone of sound horses at the trot.Equine Vet J 36:431, 2004
2. Williams RB, Harkins LS, Hammond CJ, et al: Racehorse injuries, clin-ical problems and fatalities recorded on British racecourses form flatracing and National Hunt racing during 1996, 1997 and 1998. EquineVet J 33:478-486, 2001
3. Leach DH, Spinings EJ: Gait fatigue in the racing Thoroughbred. JEquine Med Surg 3:436-443,1979
4. Patterson-Kane JC, Wilson AM, Firth EC, et al: Exercise-related alter-ations in crimp morphology in the central regions of superficial digitalflexor tendons from young thoroughbreds: a controlled study. Equine
etlock support. (A) The extended heal shoe. (B) Rolledd to the shoe distally with wire or ziplocks. When it iss the fetlock joint. (D) Finally the splint along with theolor version of figure is available online.)
ovide fattacheupport
Vet J 30:61-64, 1998

1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
Injuries of the flexor tendons 197
5. Kester WO: Definition and classification of lameness, in Guide for Veteri-nary Service and Judging of Equestrian Events (ed 4). Lexington, KY,AAEP, 1991, p 19
6. Marr CM, McMillan I, Boyd JS, et al: Ultrasonographic and histopatho-logical findings in equine superficial digital flexor tendon injury.Equine Vet J 25:23-29, 1993
7. Genovese RL, Reef VB, Longo KL, et al: Superficial digital flexor ten-donitis-long term sonographic and clinical study of racehorses, inDubai International Equine Symposium Proceedings: “The equine ath-lete: tendon, ligament and soft tissue injuries,” 1996, pp 187-205
8. Rantanen NW, Jorgensen JS, Genovese RL: Ultrasonographic examinationof the equine limb, in Dyson SJ, Ross MW (eds): Diagnosis and Manage-ment of Lameness in the Horse. St. Louis, MO, 2003, pp 166-188
9. Gillis CL: Rehabilitation of tendon and ligament injuries, in The Pro-ceedings of the 43rd Annual AAEP Convention 43:306-309, 1997
0. Wright IM, McMahon PJ: Tendosynovitis associated with longitudinaltears of the digital flexor tendons in horses: a report of 20 cases. EquineVet J 31:12-18, 1999
1. Smith MR, Wright IM: Non-infected tensosynovitis of the digital flexortendon sheath: a retrospective analysis of 76 cases. Equine Vet J 38:134-141, 2006
2. McIlwraith CW, Nixon AJ, Wright IM, et al: Tenoscopy, in Diagnosticand Surgical Arthroscopy in the Horse. Philadelphia, PA, Mosby, 2005,pp 365-408
3. Dow SM, Wilson AM, Goodship AE: Treatment of acute superficialdigital flexor tendon injury in horses with polysulphated glycosamino-glycan, Vet Rec 139:413-416, 1996
4. Genovese RL, Rantanen NW: The superficial digital flexor tendon, inRantanen NW, McKinnon AO (eds): Equine Diagnostic Ultrasonogra-phy. Baltimore, MD, Williams and Wilkins, 1998, pp 289-398
5. Gillis C: Tendon and ligament rehabilitation, in Dubai InternationalEquine Symposium Proceedings: “The equine athlete: tendon, ligamentand soft tissue injuries,” 1996, pp 417-421
6. Silver IA, Brown PN, Goodship AE, et al: A clinical and experimentalstudy of tendon injury, healing and treatment in the horse. Equine Vet
J Suppl 1:1-43,19837. Bramlage LR: Superior check ligament desmotomy as treatment forsuperficial digital flexor tendonitis: initial report, in The Proceedings ofthe 32nd Annual AAEP Convention, 1986, p 365
8. Sawdon H, Yovich JV, Booth T: Superficial digital flexor tendonitis inracehorses. Long term follow up of conservatively managed cases. AustEquine Vet 14:21-25, 1996
9. Genovese R, Longo K, Berthold B, et al: Quantitative sonographic as-sessment of superficial digital flexor injuries in Thoroughbred race-horses, in Proceedings of the 43rd Annual AAEP Convention, 1997, pp285-290
0. Reef VB: Musculoskeletal ultrasonography, in Reef VB (ed): EquineDiagnostic Ultrasound. Philadelphia, PA, WB Saunders, 1998, pp 39-186
1. Romero JM, Dyson SJ: The diffusely filled limb, in Robinson NE (ed):Current Therapy in Equine Medicine 4. Philadelphia, PA, WB Saun-ders, 1997, pp 23-27
2. Davis CS, Smith RKW: Diagnosis and management of tendon and lig-ament disorders, in Auer JA, Stick JA (eds): Equine Surgery (ed 3). St.Louis, MO, Saunders Elsevier, 2006, pp 1086-1111
3. Jann HW, Blaik MA, Emerson R, et al: Healing characteristics of deepdigital flexor tenorraphy within the digital sheath of horses. Vet Surg32:421-430, 2003
4. Bertone A: Tendon lacerations. Vet Clin North Am Equine Pract 11:239-314, 1995
5. Hardy J: Emergency procedures and first aid, in Hinchcliff KW, KanepsAJ, Geor RJ (eds): Equine Sports Medicine and Surgery. Philadelphia,PA, Saunders, 2004, pp 1179-1192
6. Bramlage LR: Emergency first aid treatment and transportation ofequine fracture patients, in Auer JA, Stick JA (eds): Equine Surgery(ed 2). Philadelphia, PA, WB Saunders, 1999 pp 635-638
7. Wheat JD, Pascoe JR: A technique for management of traumatic ruptureof the equine suspensory apparatus. J Am Vet Med Assoc 176:205-210,1980
8. Taylor S, Pascoe J, Meagher D, et al: Digital flexor lacerations in horses50 cases (1975-1990). J Am Vet Med Assoc 206:342, 1995
9. Fraser BS, Bladon BM: Tenoscopic surgery for treatment of laceration of
the digital flexor tendon sheath. Equine Vet J 36:528-531, 2004