Embed Size (px)
Citation preview
International Nutrition QI Project 2007:
Debriefing Session
Friday June 15th, 2007
Confederation 3, Fairmont Royal York, Toronto
• Brief Overview of Survey Results • Review of Benchmarked Performance Reports • Small Group Discussion • Future Research • Summary and Closing Comments
Agenda
Purpose
• To describe and compare nutrition practices • To compare nutrition practices to the Canadian
Nutrition Support Clinical Practice Guidelines• To identify opportunities
for improvement • Illuminate research opportunities
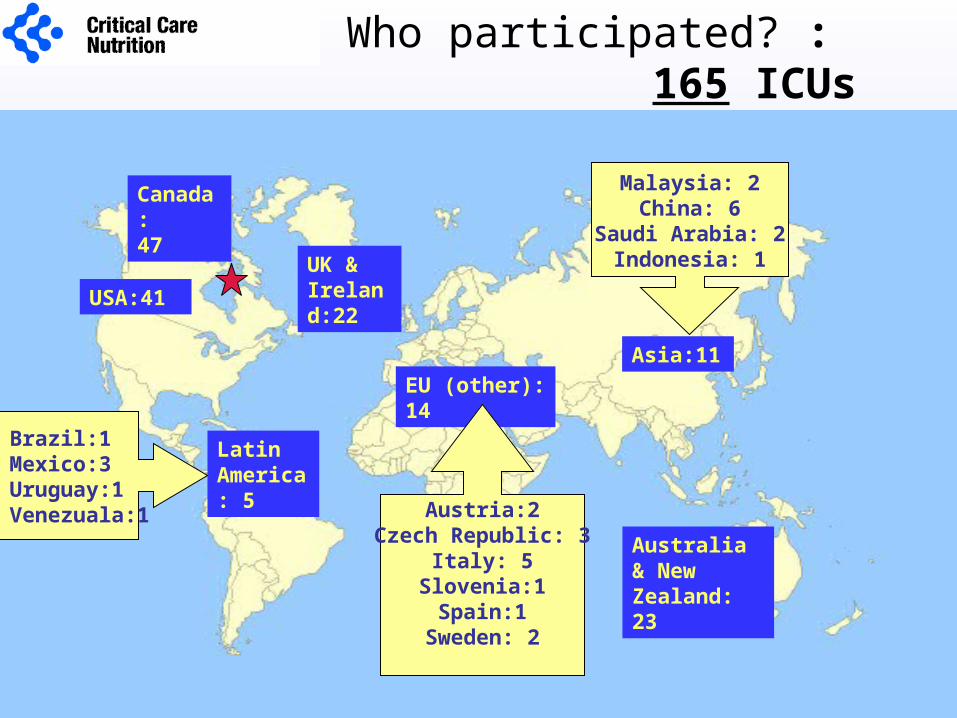
Canada:47
USA:41
Australia & New Zealand: 23
UK & Ireland:22
EU (other): 14
Latin America: 5
Asia:11
Brazil:1Mexico:3Uruguay:1Venezuala:1
Who participated? : 165 ICUs
Malaysia: 2China: 6
Saudi Arabia: 2Indonesia: 1
Austria:2Czech Republic: 3
Italy: 5Slovenia:1
Spain:1Sweden: 2
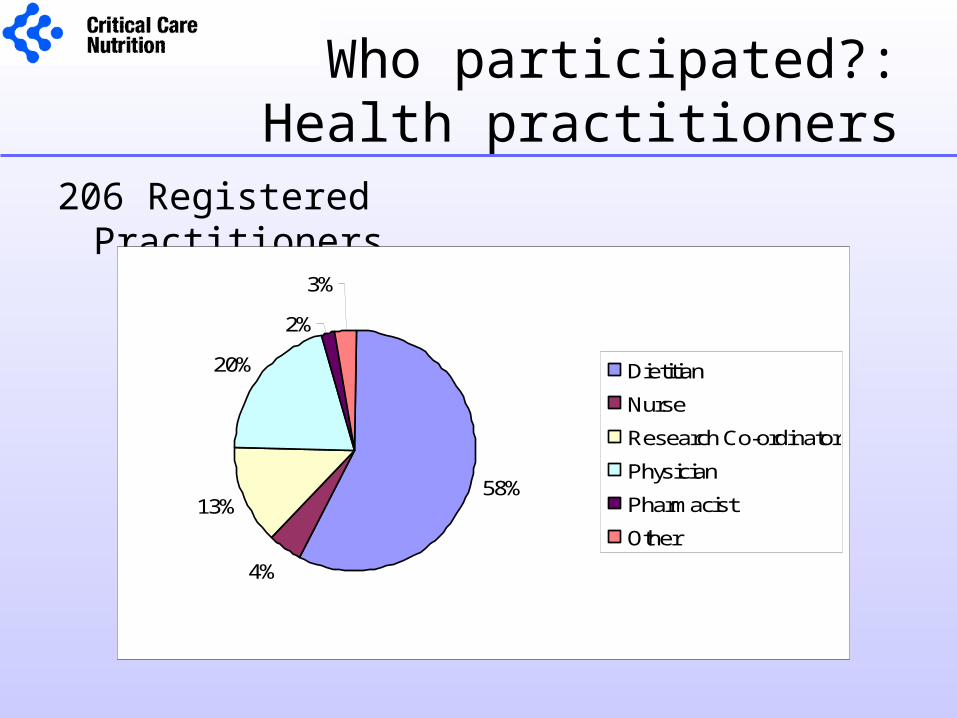
Who participated?:Health practitioners
206 Registered Practitioners
58%
4%
13%
20%
2%
3%
Dietitian
Nurse
Research Co-ordinator
Physician
Pharmacist
Other
Ethics Approval
• 206 Registered ICUs• 41 ICUs excluded as no data entered
Reason for attrition: ? Ethics approval• 120 ICUs (57.5%) required local ethics approval
– 97 expedited review – 1 expedited review plus informed consent required– 21 full review– 1 full review plus informed consent required
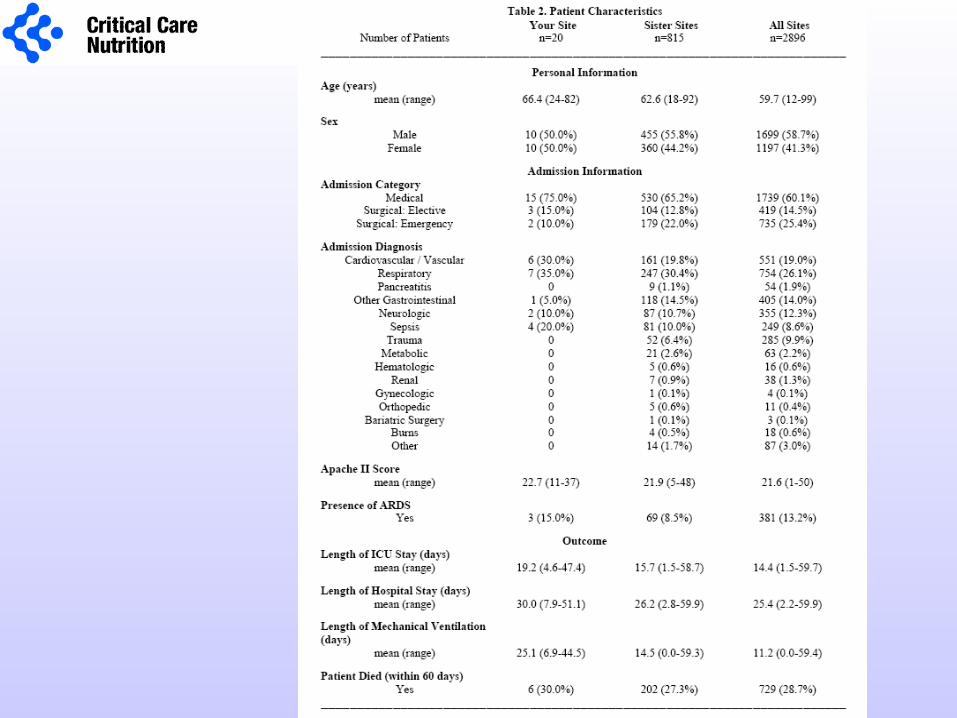
Who participated?Patients
• Number of patients per site– 19.3 (1-40)
• Total number of patients– 2896
• Days of observation per patient– 9.5 (1-12)
• Total number of patient days in ICU– 27192 days
• <3% missing data for ALL variables
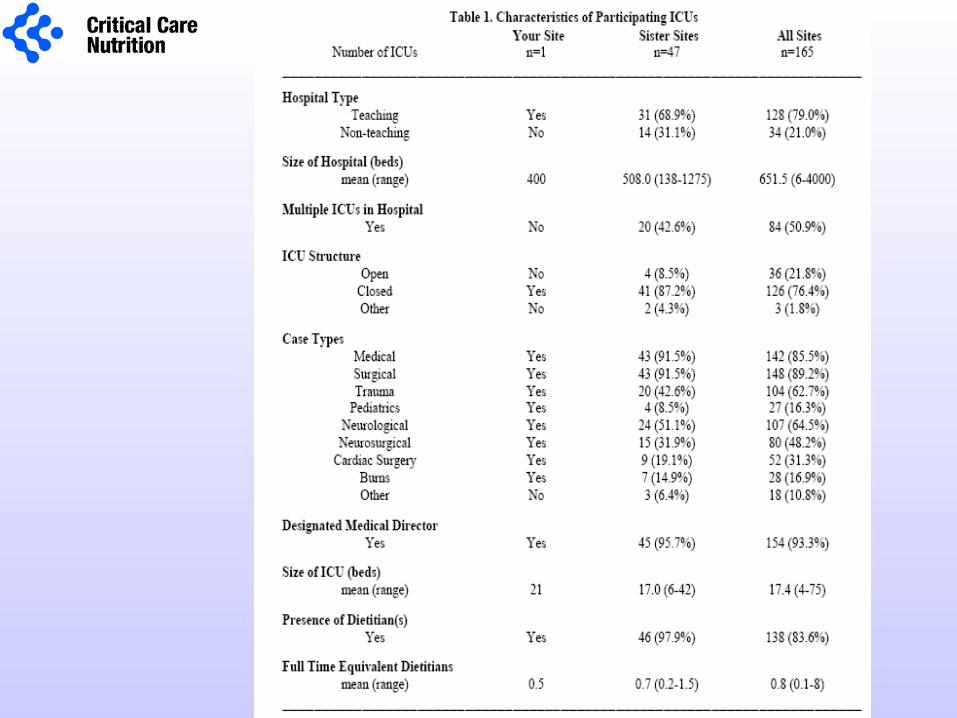
Preliminary Site Report
Purpose of review:
1. Communicate how to interpret your site report2. Review ‘preliminary’ results of the survey3. Receive feedback on format of site reports

Sister Sites
Sister Site Groupings Countries
Canada Canada
United States of America USA
United Kingdom and Republic of Ireland
England, Scotland, Ireland
Europe Austria, Czech Republic, Italy, Slovenia. Spain, Sweden
Australia and New Zealand Australia, New Zealand
Latin America Brazil, Mexico, Uruguay, Venezuela,
Asia Malaysia, China, Indonesia, Russia, Saudi Arabia
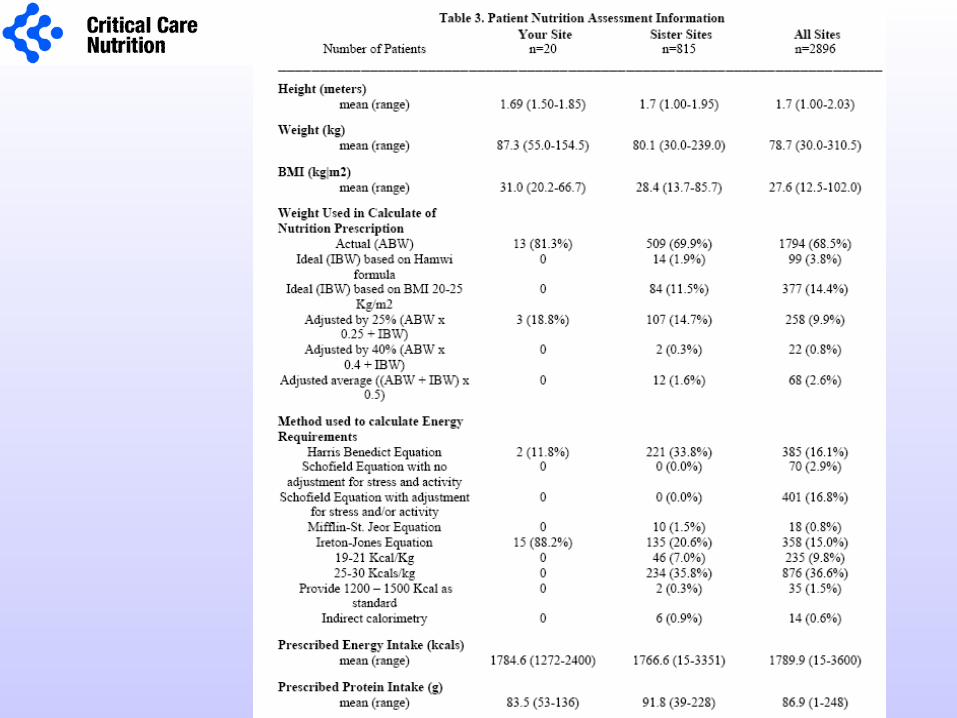
Overall Performance
Adequacy of Nutrition Support =
Calories received from EN & appropriate PN X 100
Calories prescribed
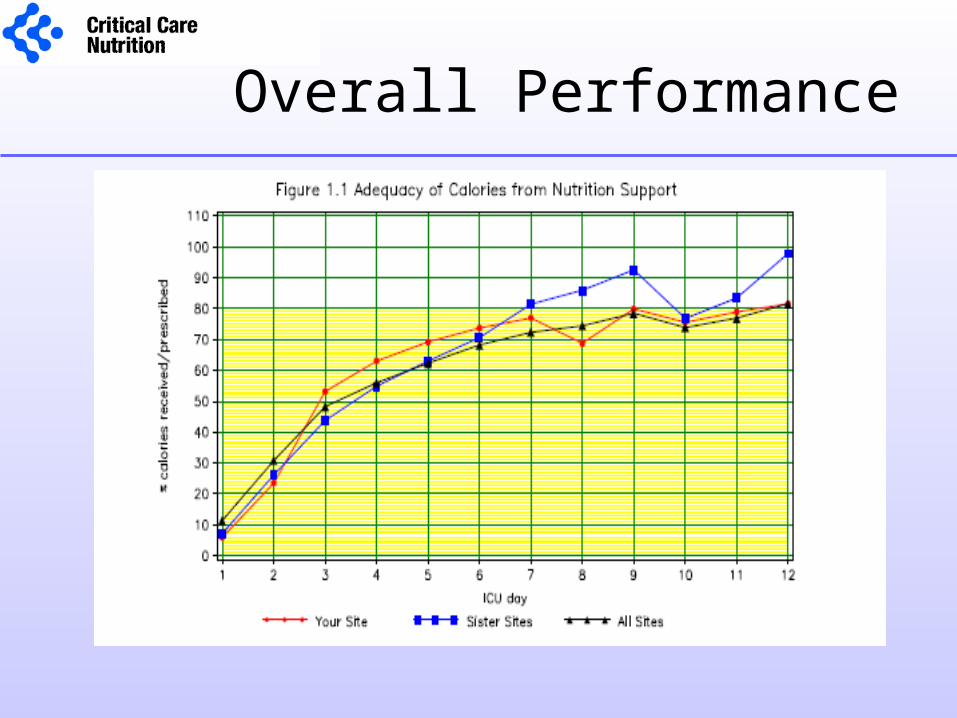
Overall Performance
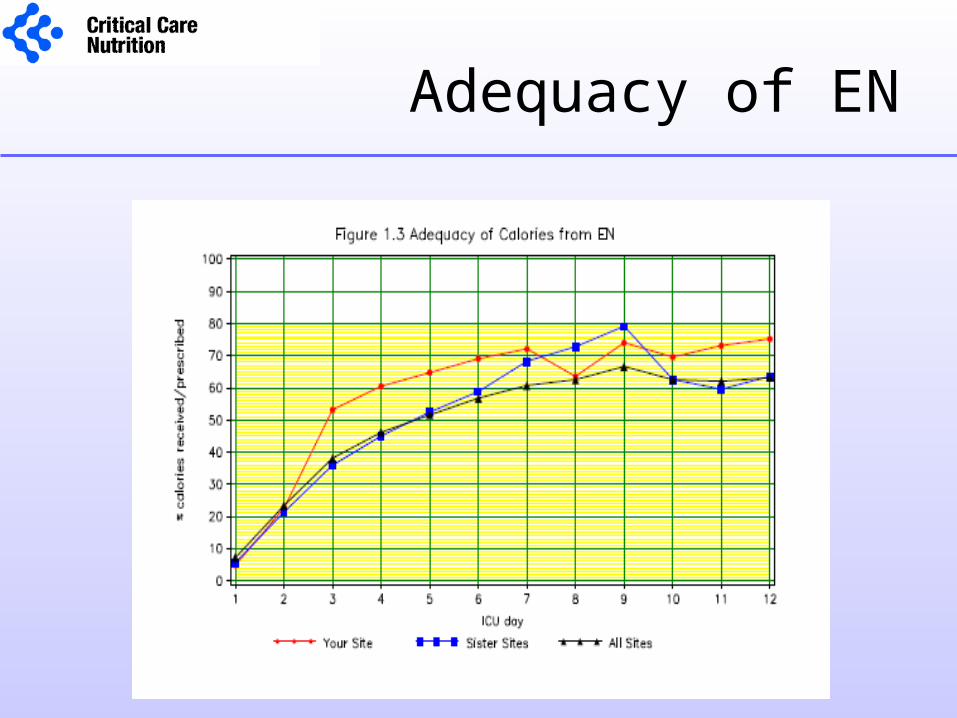
Adequacy of EN
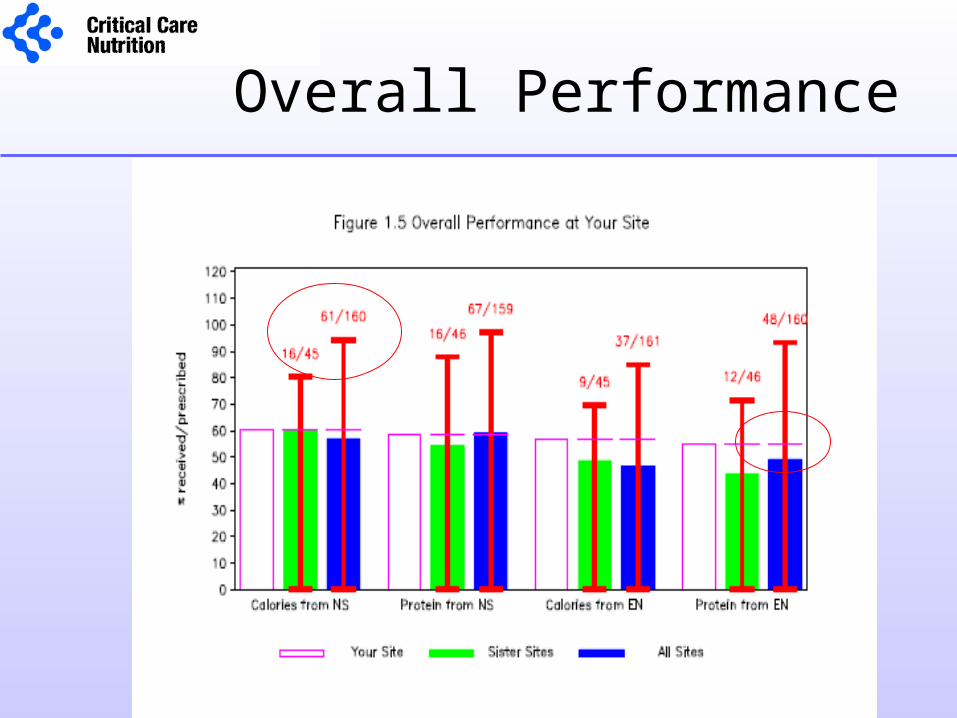
Overall Performance
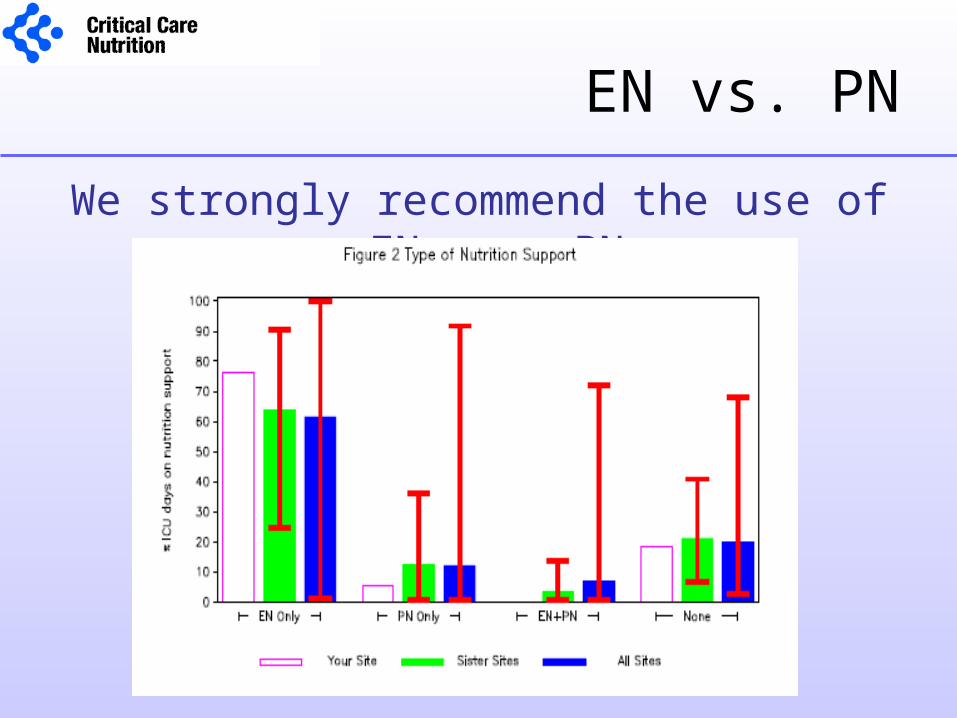
EN vs. PN
We strongly recommend the use of EN over PN
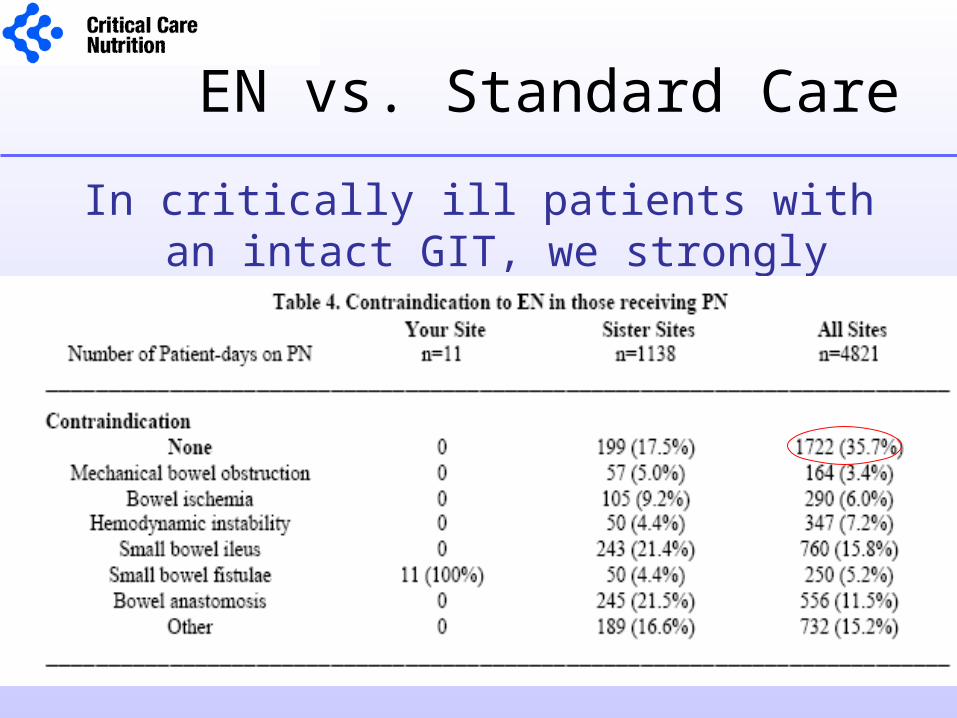
EN vs. Standard Care
In critically ill patients with an intact GIT, we strongly recommend that PN not be used routinely
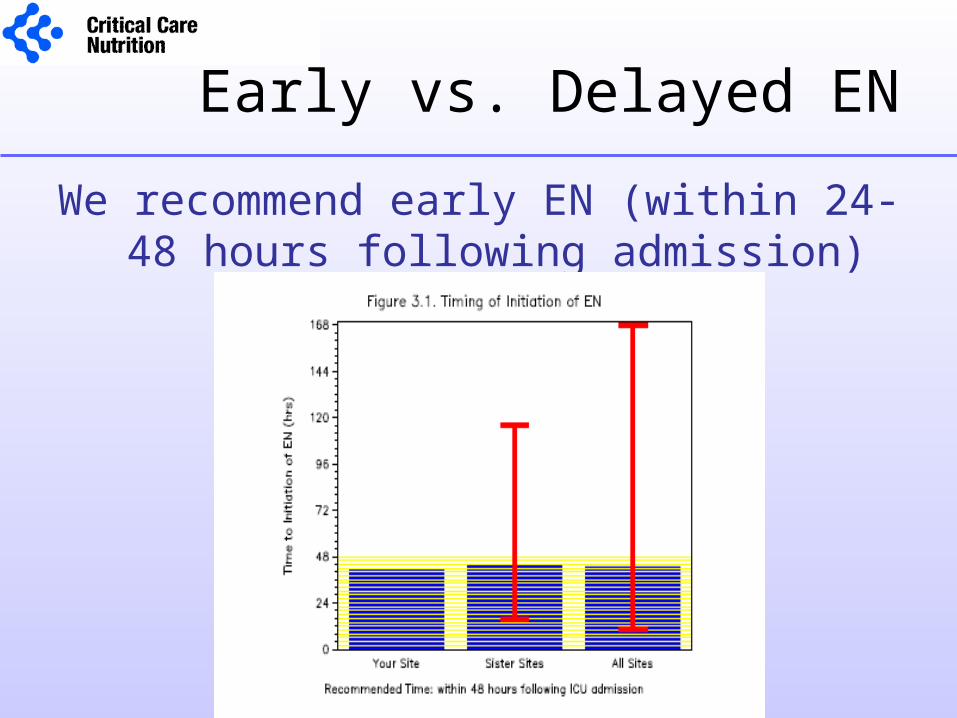
Early vs. Delayed EN
We recommend early EN (within 24-48 hours following admission)
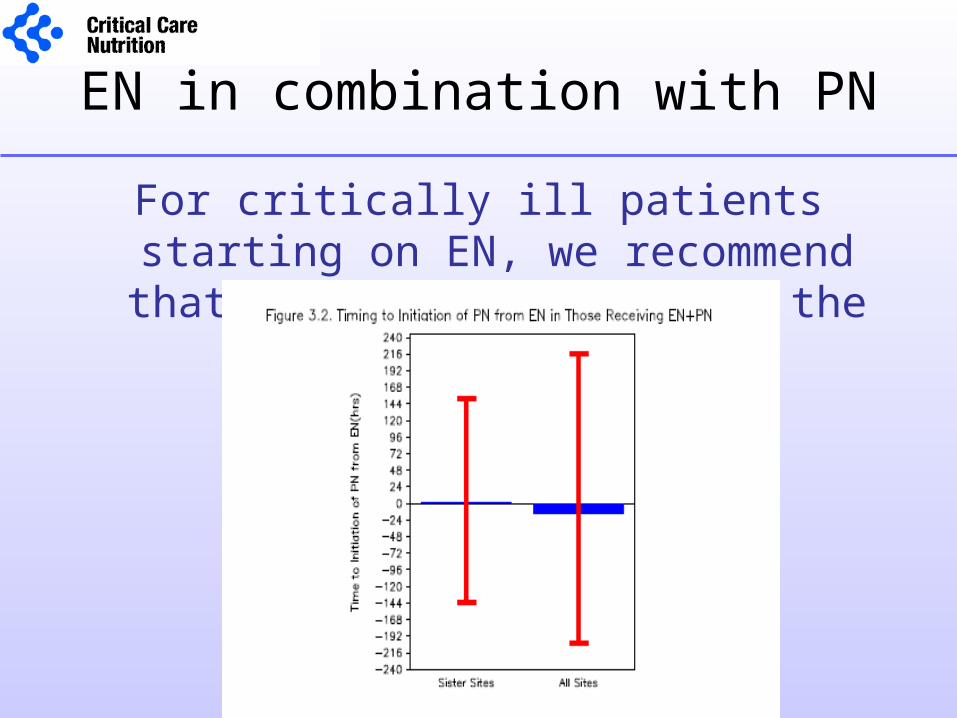
EN in combination with PN
For critically ill patients starting on EN, we recommend that PN not be started at the same time as EN
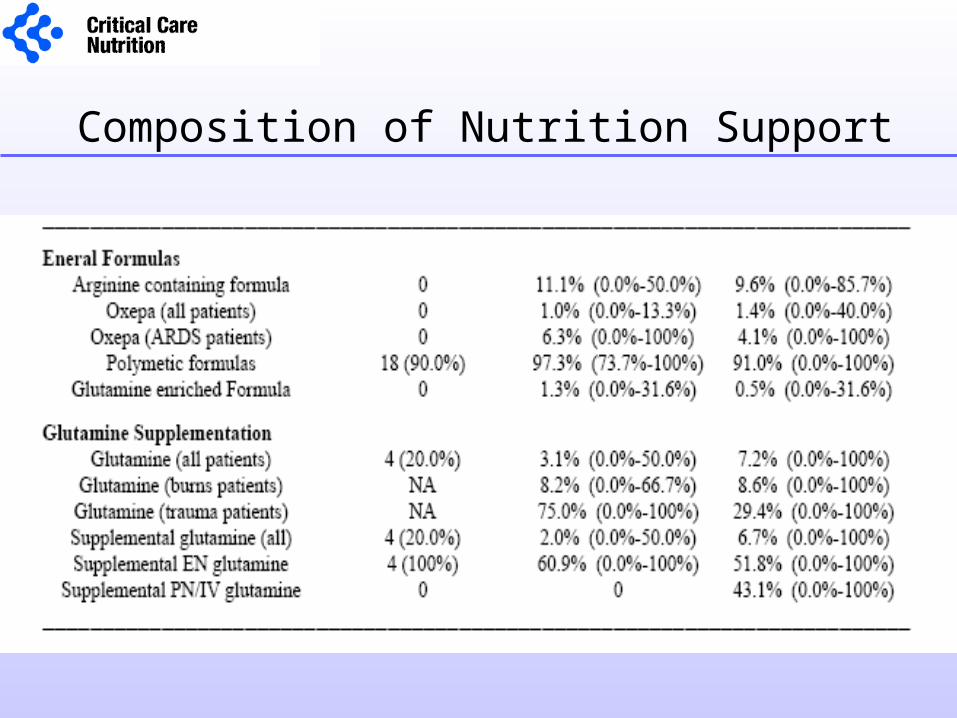
Composition of Nutrition Support
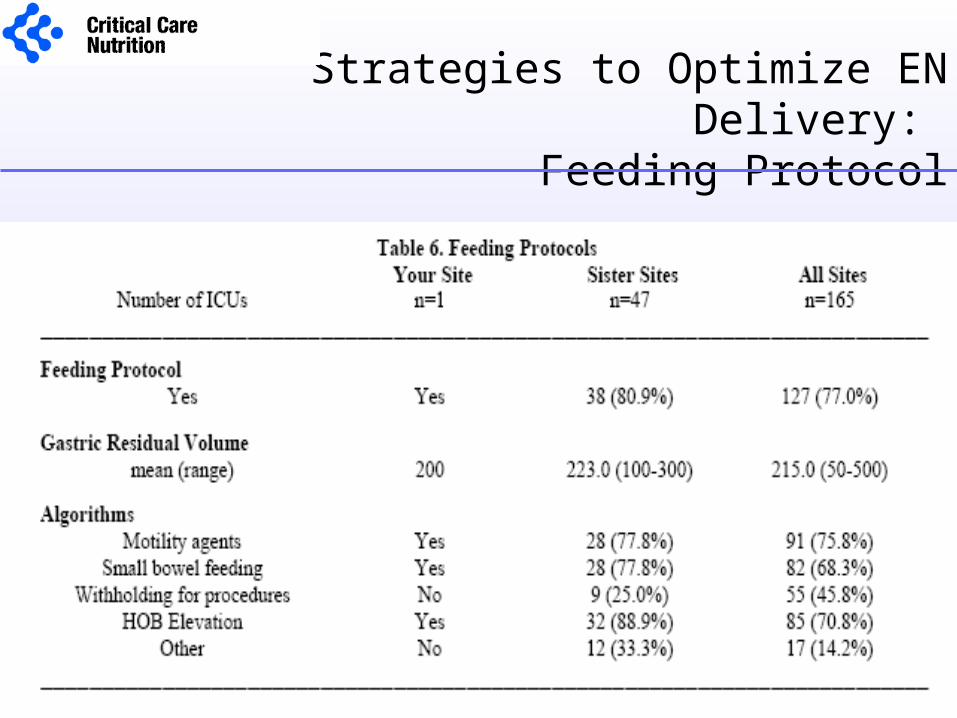
Strategies to Optimize EN Delivery: Feeding Protocol
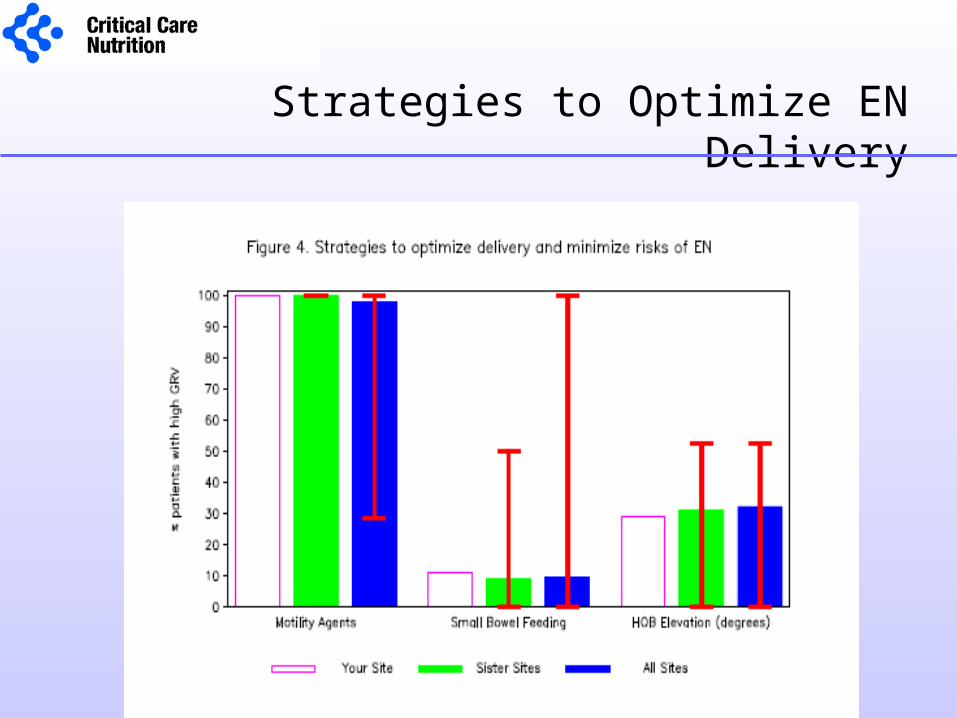
Strategies to Optimize EN Delivery
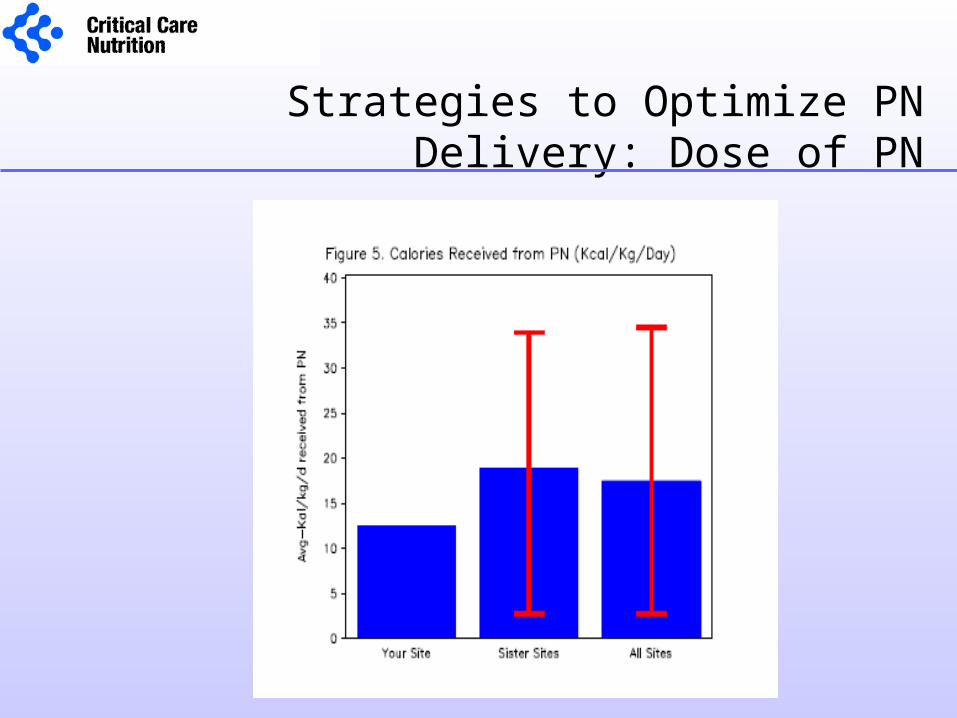
Strategies to Optimize PN Delivery: Dose of PN
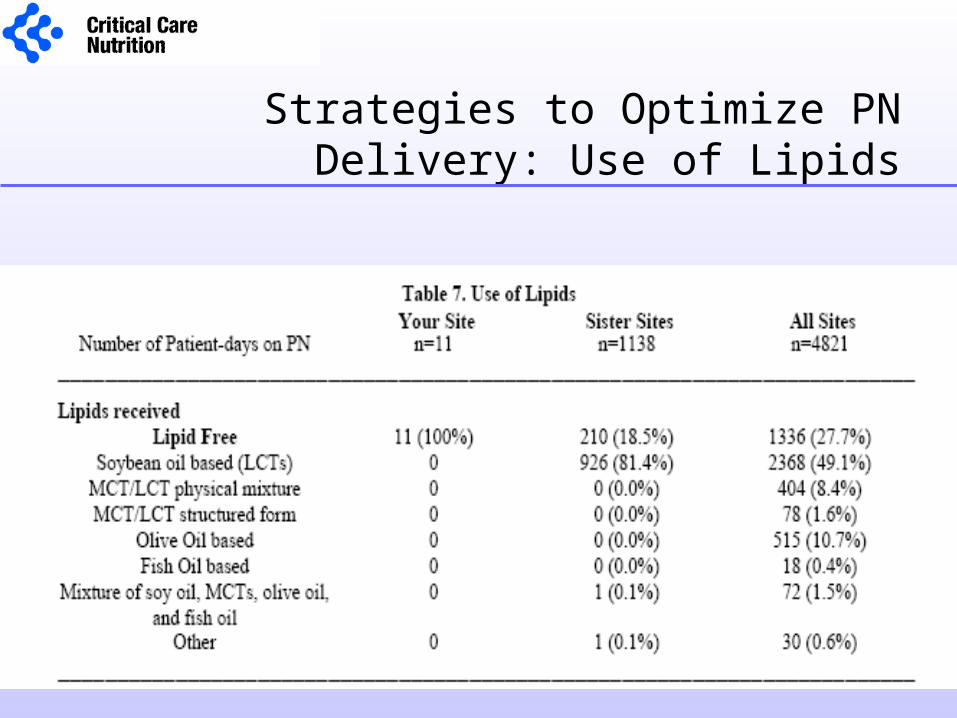
Strategies to Optimize PN Delivery: Use of Lipids
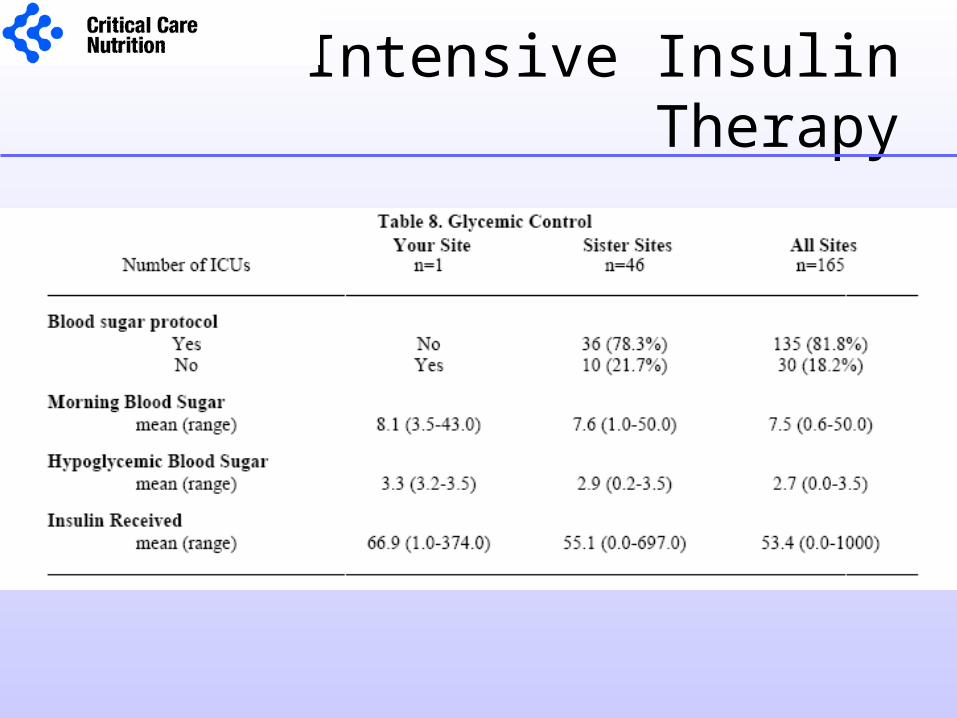
Intensive Insulin Therapy
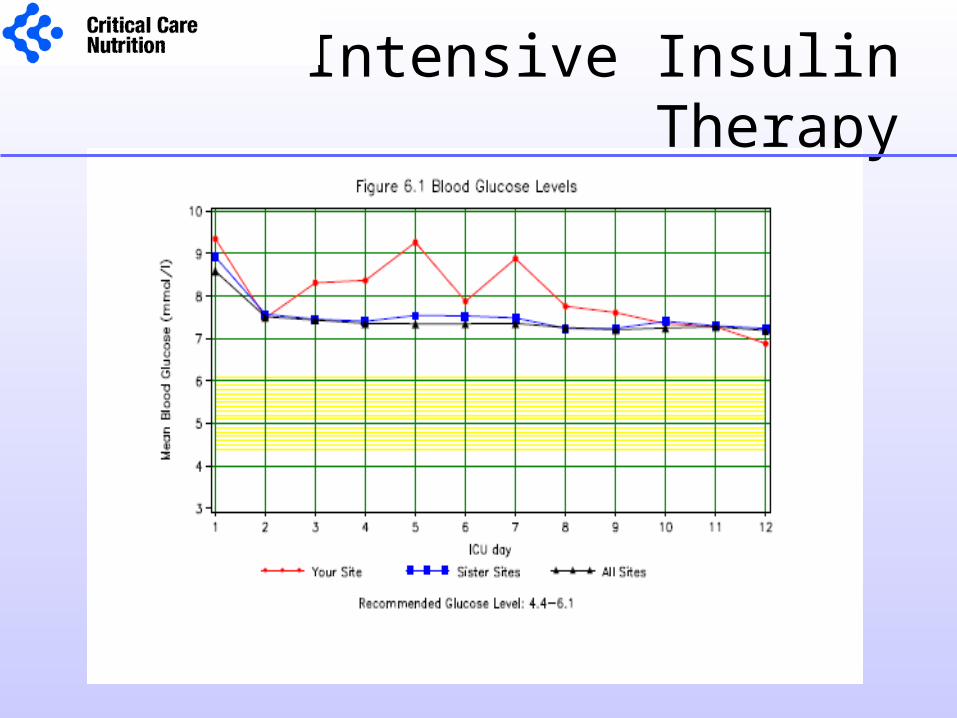
Intensive Insulin Therapy
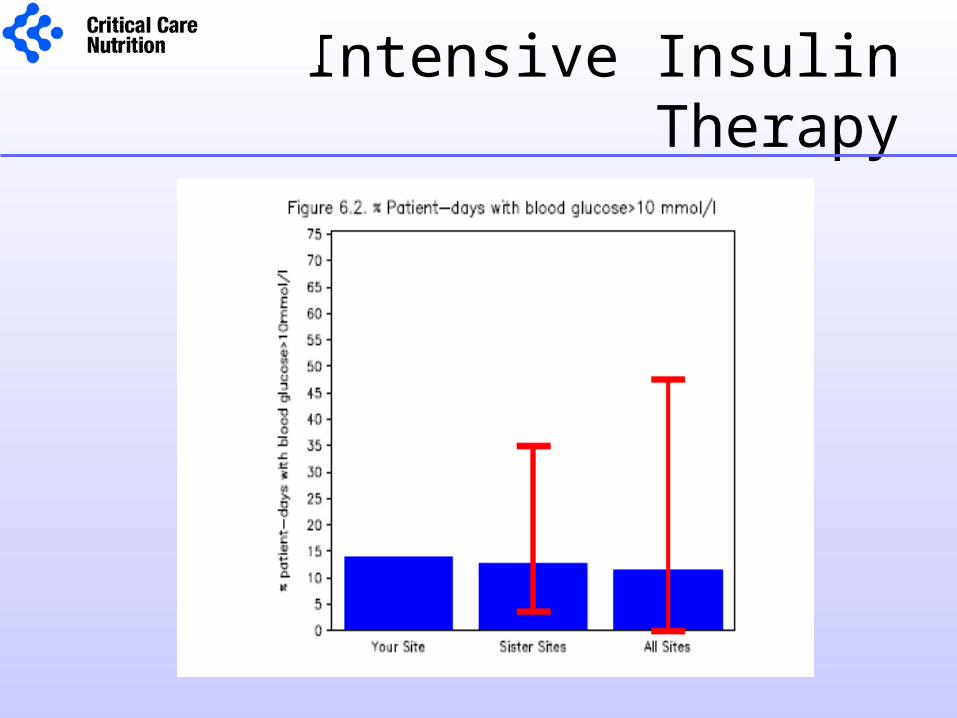
Intensive Insulin Therapy
Small Group Discussion
What are your thoughts on the data elements collected in the
survey, the method of data collection,
and how it is represented in the
site reports?
What are the most effective strategies
for changing behaviour around nutrition practices
in the ICU?
Small Group Discussion
• 20 mins• Nominate ‘recorder’ and ‘spokesperson’• Give freely of your experience• Keep confidences and assume others will• Feel free to ask us questions• Summarize key points
Moving Forward:QI in the ICU
• Changing nutrition practice is complex
• Need to identify barriers and enablers to changing practice
• Need to understand factors associated with guideline implementation and adherence
Understanding Guideline Implementation
• Secondary Analysis of Canadian Nutrition Survey 2004 dataset
• Multiple case study 4 case ICU sites 28 Semi-structured
key informant interviews
Identified Barriers
Guidelines• Information overload • Weak evidence• Impractical / ComplexInstitution• Community Hospital setting• Open ICU• Slow administrative process• Resource constraints
Practitioner• Lack of awareness• Limited critical care experience • Resistance to change• Nursing workloadPatient• Poor clinical condition• Surgical
Enablers
• Agreement of the attending physician & ICU team• Part of routine practice• Dietitian / Opinion leader• Access / Visibility• Easy to follow and perform• Provision of education• Open discussion
Successful Implementation Strategies
• Informal one-on-one discussions– Academic detailing, ward rounds
• Bed-side reminders– Check-list, algorithms,
• Feedback and audit– Site reports
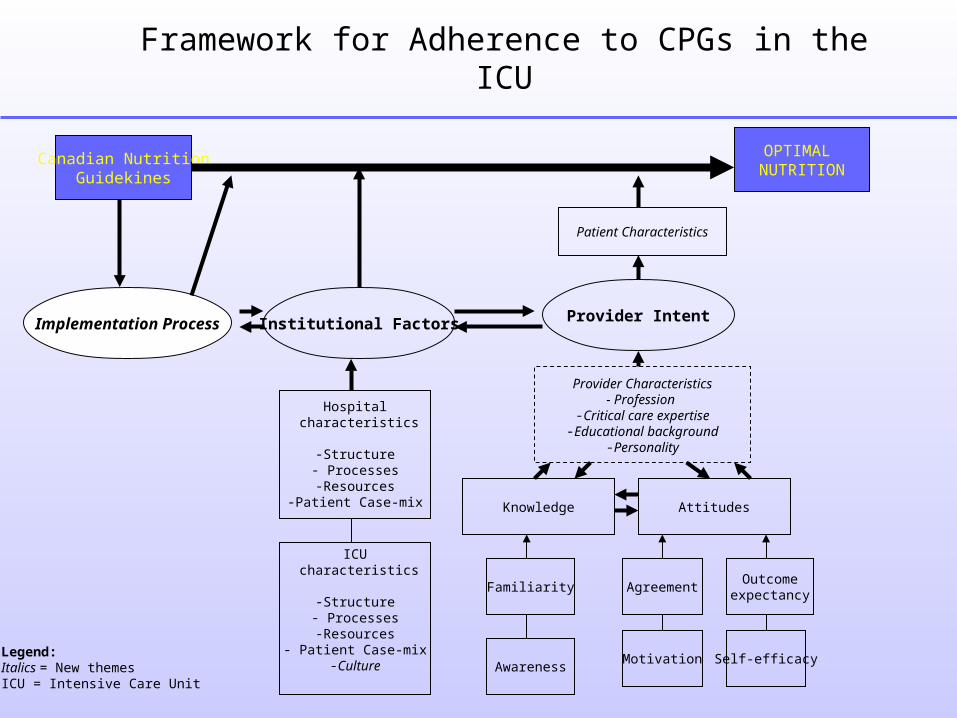
Canadian NutritionGuidekines
OPTIMAL NUTRITION
Implementation Process Institutional Factors Provider Intent
Hospital characteristics
-Structure- Processes-Resources
-Patient Case-mix Knowledge Attitudes
Familiarity
AwarenessMotivation Self-efficacy
Outcomeexpectancy
Agreement
ICU characteristics
-Structure- Processes-Resources
- Patient Case-mix-Culture
Legend:Italics = New themesICU = Intensive Care Unit
Provider Characteristics- Profession
-Critical care expertise-Educational background
-Personality
Patient Characteristics
Framework for Adherence to CPGs in the ICU
Future Research
• Survey of Attitudes towards the Canadian Nutrition Support Clinical Practice Guidelines
• Tailored approach to guideline implementaton– Development of screening questionnaire and
educational toolkit– ? Future Cluster Randomized Controlled Trial

International QI Project 2008 !!

Thank you