Embed Size (px)
Citation preview

INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
38 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
Prevalence, Distribution, Risk Factors and Antifungal Susceptibility
Profiles of Candida Isolates from Patients Attending Mombasa Hospital
Abdulrahman Subira, Jomo Kenyatta University of Agriculture & Technology, Kenya
Dr. Rahma Udu, Technical University of Mombasa, Kenya
Prof. Simon Karanja, Jomo Kenyatta University of Agriculture & Technology, Kenya
1. Introduction
Candida commonly occurs as commensal organisms on the mucosal surfaces of gastrointestinal, genitourinary tracts and skin
of humans but can cause mucocutaneous or invasive infections [(Pappas et al., 2004), (Kabir & Ahmad, 2013), (Mayer, Wilson,
& Hube, 2013)]. Candida are emerging as a potentially pathogenic fungus in patients with broncho-pulmonary diseases (Kali et
al., 2013).
2. Problem Statement
Most laboratories in Mombasa do not undertake Candida identification and antifungal susceptibility tests although the Vitek
(BioMérieux) system enables clinical laboratories to perform routine identification of Candida and antifungal susceptibility easier
and more accurately (Melhem et al., 2013). Various Candida species (Mainly mucocutaneous but also few cases of systemic
Candida infections) are isolated from clinical specimens in the Microbiology laboratory at Mombasa Hospital with few cases of
resistance to some antifungal agents identified (Mombasa hospital health management information system).
3. Research Objective
The study was guided by the following specific objectives:
i. To determine the prevalence and distribution of Candida species among patients attending Mombasa Hospital.
ii. To determine the antifungal susceptibility profiles of the Candida isolated from clinical specimens in Mombasa
Hospital.
iii. To determine the risk factors associated with isolation of Candida among patients attending Mombasa Hospital
Abstract
Candida causes mucocutaneous or invasive infections. Most laboratories in Mombasa do not undertake Candida species
identification and antifungal susceptibility routinely. Objectives: This study sought to determine the prevalence, distribution,
risk factors and antifungal susceptibilities of Candida isolated in Mombasa Hospital. Materials and Methods: In a cross-
sectional study, 384 patient samples selected by systematic random sampling were cultured. Identification and antifungal
susceptibilities for yeast isolates were done on Vitek 2 compact. Chi-square and logistic regression analysis were done using
SPSS version 20. Differences in parameter estimates were deemed statistically significant at P < 0.05. Results: The prevalence
of Candida was 8.6%. Candida albicans (7.8%) and Candida tropicalis (0.8%). Candida isolates were susceptible to
Flucytosine (100%), Micafungin and Caspofungin (96.97%), Voriconazole (93.94%) and Fluconazole (81.82%). 9.09%
isolates were resistant and intermediate to Fluconazole while 15.15% were resistant to Amphotericin B. Pregnant women (P =
0.000), diabetics (P = 0.008), chronically ill patients (P = 0.026) and catheterized patients (P = 0.023) were at most risk of
Candida infections. Conclusion: Candida is a common cause of infections among patients in Mombasa Hospital. Flucytosine
is an effective antifungal agent. Resistance to azoles and Amphotericin B should be considered when starting empirical
treatment.
Key words: Candida species, Prevalence, Antifungal sensitivity, Risk Factors
INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE (IJARKE Science & Technology Journal)
INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
39 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
4. Justification of the Study
The isolation of non albicans Candida from clinical samples, growing resistance trends to some common antifungal agents,
and the existence of some intrinsic and secondary resistance by some Candida and other yeasts to antifungal agents demonstrates
the need to provide clinicians with information regarding the local epidemiological patterns. Whereas traditionally laboratories
and clinicians have not put much emphasis on the identification of Candida and their antifungal susceptibility profiles, it is
becoming more useful now to provide such information to facilitate a more informed and evidence based treatment decision.
5. Literature Review
Risk factors for Candida infections include immune compromised states, diabetes mellitus, antibiotic use, indwelling devices,
intravenous drug use among others (Kojic, Darouiche, & Biofilms, 2004). Improved management of high-risk patients with novel
treatment methods has partly contributed to the increase in Candidiasis (Diaz & Fell, 2004),(Pappas et al., 2016). Significant
geographic variation is evident among cases of candidemia in different parts of the world hence local epidemiological data and
antifungal susceptibility profiles are of major significance (Falagas, Roussos, & Vardakas, 2010), (Colombo et al., 2006)].
Candida is the primary cause of fungal infections, particularly in immunosuppressed patients with Candida albicans being the
most common etiologic agent (Haddadi et al., 1970). A prevalence of 42.7% vaginal Candida infections was reported among
pregnant women in Thika District Hospital, Kenya with Candida albicans being the most commonly isolated species (Menza
Nelson, Wanyoike Wanjiru2, 2013). An increasing prevalence of vulvo vaginitis (Kumari et al., 2013) and pulmonary candidiasis
(Kali et al., 2013) due to non-albicans Candida species has been reported. Some Candida exhibit primary resistance due to
intrinsic resistance mechanisms and others develop secondary resistance to certain antifungal agents due to prior exposure of the
patient to the antifungal agents (Fothergill, 2012) hence empirical antifungal agents may not be efficient in treating high risk and
systemic candidiasis patients [(Aguilar et al., 2015), (Collins, Eschenauer, Salo, & Newton, 2007), (Falagas et al., 2010)].
Detection of Candida and determination of their susceptibility to antifungal agents can help improve the clinical management
of systemic mycosis (Haddadi et al., 1970). Overuse of antifungals has promoted a shift to Candida with reduced susceptibility to
antifungal agents (Lortholary, Desnos-ollivier, Sitbon, & Fontanet, 2011). Fluconazole should probably not be considered as a
first-line treatment of Candida glabrata infections and empirical treatment with echinocandins may be withheld due to decreased
susceptibility of Candida parapsilosis to echinocandins, especially Caspofungin (Falagas et al., 2010). However, susceptibility
testing of Candida glabrata isolates resulted in lower overall treatment costs, based on de-escalation in therapy from an expensive
echinocandin to Fluconazole for patients with Candida glabrata fungemia (Collins et al., 2007). Echinocandin drugs are
recommended as the first line for invasive Candida infections (Alexander et al., 2013), (Haddadi et al., 1970). Flucytosine is
administered in combination with Amphotericin B in the treatment of life threatening Candida infections or in circumstances
where drug penetration may be problematic (Hope, Tabernero, Denning, & Anderson, 2004) since yeasts develop resistance to
Flucytosine monotherapy very quickly (Kanafani & Perfect, 2008). Though its prevalence remained low (1% – 2%) among
Candida (Kanafani & Perfect, 2008) there has been reports of increasing Echinocandin resistance from 4.9% to 12.3% between
2001 and 2010 (Alexander et al., 2013).
6. Research Design
This was a cross-sectional study that was done in Mombasa Hospital, a level 5 private referral hospital in Mombasa, Kenya.
384 patient specimens that met the sample acceptance criteria for culture and sensitivity testing submitted between January and
June 2016 were selected by systematic random sampling and analyzed. Samples from non-consenting patients were not included.
6.1 Sample Collection and Laboratory Analysis
Urine (66.9%), pus swabs (11.7%), catheter tips (6.5%), sputum (5.7%), High vaginal swabs (5.2%), wound swabs (2.1%) and
tracheal aspirates (1.8%) specimens were collected and analyzed. Urine and catheter tips specimens were inoculated on blood agar
(BA), Cystine Lactose Electrolyte Deficiency (CLED) and Sabouraud Dextrose Agar (SDA) media. High vaginal swabs, Sputum,
tracheal aspirates, pus and wound swabs were cultured onto BA, Chocolate agar and SDA media and incubated aerobically for 18
to 48 hours. Gram stain was done and slides examined microscopically for Candida. McFarland adjusted turbidity level 1.8 – 2.20
suspensions were prepared. Identification and antifungal susceptibility tests were done using the Vitek 2 compact (BioMérieux).
Amphotericin B, Caspofungin, Fluconazole, Flucytosine, Micafungin and Voriconazole were selected for study. Isolates were
determined as susceptible, intermediate or resistant according to the EUCAST resistance breakpoints for antifungal agents.
INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
40 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
6.2 Data Analysis
Demographic information, patient diagnosis, treatment, surgery, catheterization and culture and sensitivity data were collected
from consenting patients using standard forms. Data were analyzed using SPSS software version 20. Descriptive statistics was
used to describe the trends. Chi-square statistics and multivariate logistic regressions analysis were done test the relationship
between the risk factors and the isolation of Candida Spp.
6.3 Ethical Issues
Approval to conduct this study was given by the ethical review committee at Pwani University, Kilifi, Kenya. Participation in
the study was voluntarily. There were no health risks to the study subjects. Confidentiality to participants’ information was
maintained by means of codes and unauthorized access to the data was not allowed.
7. Research Findings
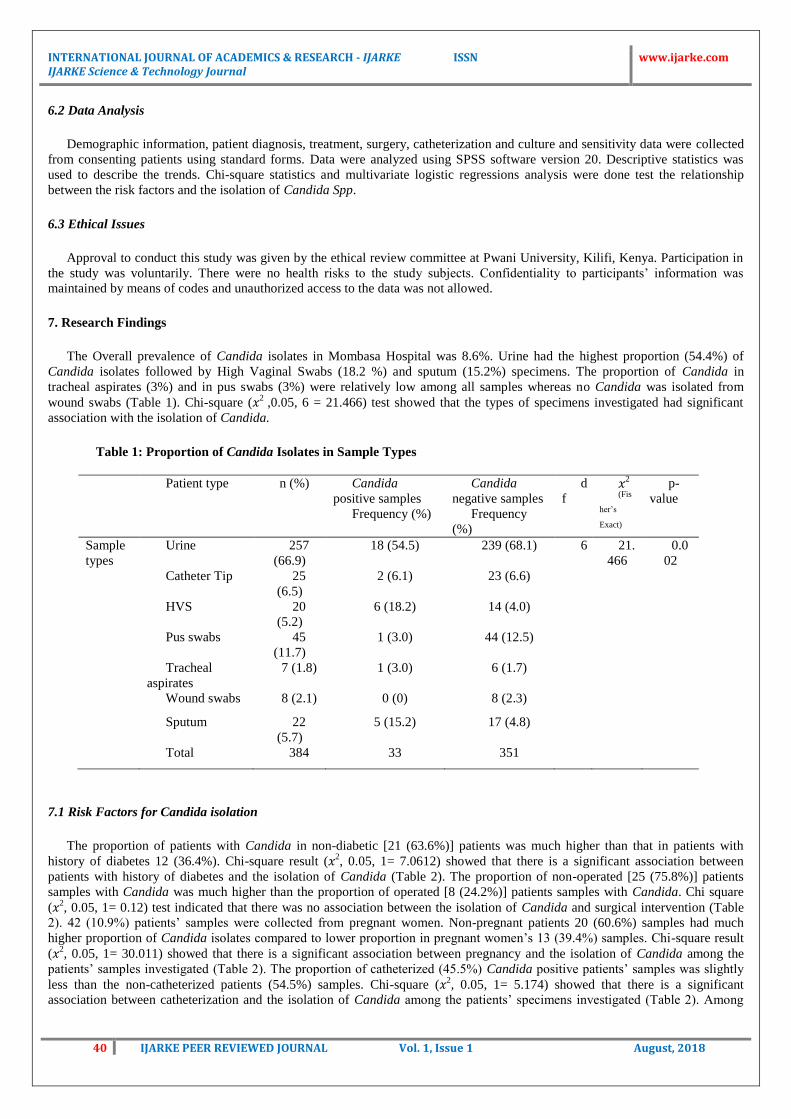
The Overall prevalence of Candida isolates in Mombasa Hospital was 8.6%. Urine had the highest proportion (54.4%) of
Candida isolates followed by High Vaginal Swabs (18.2 %) and sputum (15.2%) specimens. The proportion of Candida in
tracheal aspirates (3%) and in pus swabs (3%) were relatively low among all samples whereas no Candida was isolated from
wound swabs (Table 1). Chi-square (𝑥2 ,0.05, 6 = 21.466) test showed that the types of specimens investigated had significant
association with the isolation of Candida.
Table 1: Proportion of Candida Isolates in Sample Types
Patient type n (%) Candida
positive samples
Frequency (%)
Candida
negative samples
Frequency
(%)
d
f 𝑥2
(Fis
her’s
Exact)
p-
value
Sample
types
Urine 257
(66.9)
18 (54.5) 239 (68.1) 6 21.
466
0.0
02
Catheter Tip 25
(6.5)
2 (6.1) 23 (6.6)
HVS 20
(5.2)
6 (18.2) 14 (4.0)
Pus swabs 45
(11.7)
1 (3.0) 44 (12.5)
Tracheal
aspirates
7 (1.8) 1 (3.0) 6 (1.7)
Wound swabs 8 (2.1) 0 (0) 8 (2.3)
Sputum 22
(5.7)
5 (15.2) 17 (4.8)
Total 384 33 351
7.1 Risk Factors for Candida isolation
The proportion of patients with Candida in non-diabetic [21 (63.6%)] patients was much higher than that in patients with
history of diabetes 12 (36.4%). Chi-square result (𝑥2, 0.05, 1= 7.0612) showed that there is a significant association between
patients with history of diabetes and the isolation of Candida (Table 2). The proportion of non-operated [25 (75.8%)] patients
samples with Candida was much higher than the proportion of operated [8 (24.2%)] patients samples with Candida. Chi square
(𝑥2, 0.05, 1= 0.12) test indicated that there was no association between the isolation of Candida and surgical intervention (Table
2). 42 (10.9%) patients’ samples were collected from pregnant women. Non-pregnant patients 20 (60.6%) samples had much
higher proportion of Candida isolates compared to lower proportion in pregnant women’s 13 (39.4%) samples. Chi-square result
(𝑥2, 0.05, 1= 30.011) showed that there is a significant association between pregnancy and the isolation of Candida among the
patients’ samples investigated (Table 2). The proportion of catheterized (45.5%) Candida positive patients’ samples was slightly
less than the non-catheterized patients (54.5%) samples. Chi-square (𝑥2, 0.05, 1= 5.174) showed that there is a significant
association between catheterization and the isolation of Candida among the patients’ specimens investigated (Table 2). Among

INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
41 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
the patients with chronic illnesses, (18.2%) had Candida. Chi-squares statistics (𝑥2, 0.05, 1= 4.971) indicated a significant
association between chronic illness and isolation of Candida (Table 2).
Table 2: Prevalence of Isolation of Candida with regards to various Risk Factors
Patients’ characteristics n (%) Candida
positive
samples
Frequency (%)
Candida
negative
samples
Frequency (%)
𝑥2 df p-
value
OR
Diabetes Diabetic 73 (19) 12 (36.4) 61 (17.4) 7.0612 1 0.008 0.37
Non diabetic 311 (81) 21 (63.6) 290 (82.6)
Total 384 33 351
Surgery Done 103
(26.8)
8 (24.2) 95 (27.1) 0.123 1 0.726 1.16
Not done 281
(73.2)
25 (75.8) 256 (72.9)
Total 384 33 351
Pregnancy pregnant 42 (10.9) 13 (39.4) 29 (8.3) 30.011 1 0.000 0.14
Non Pregnant 342
(89.1)
20 (60.6) 322 (91.7)
Total 384 33 351
Catheterization Catheterized 109
(28.4)
15 (45.5) 94 (26.8) 5.174 1 0.023 0.44
Non
Catheterized
275
(71.6)
18 (54.5) 257 (73.2)
Total 384 33 351
Chronic
illnesses
Chronically ill 31 (8.1) 6 (18.2) 25 (7.1) 4.971 1 0.026 0.35
Not chronically
ill
353
(91.9)
27 (81.8) 326 (92.9)
Total 384 33 351
7.2 Distribution of Candida Species among Patients Attending Mombasa Hospital
Two types of Candida were isolated from all samples investigated. Candida albicans 30 (90.9%) was the predominant species
while 3(9.1%) Candida tropicalis were isolated.
7.3 Antifungal Susceptibility Profiles of the Candida Isolates
All [33 (100%)] Candida isolates were sensitive to Flucytosine. [32 (97%)] Candida were sensitive to Micafungin and
Caspofungin and 1 (3.0%) isolate showed resistance to the two drugs. 31 (93.9%) Candida isolates were sensitive to Voriconazole

INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
42 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
with two isolates showing resistance. 27 (81.8%) of the isolates were sensitive to Fluconazole while [3 (9.1%)] isolates showed
resistance and [3 (9.1%)] intermediate responses. 5 (15.2%) Candida isolates showed resistance to Amphotericin B. Chi square
(𝑥2, 0.05, 1 = 20.165) results indicated that there is an association between the antifungal drug used and susceptibility of the
Candida species isolated. (Table 3)
Table 3: Response of Candida to the Six Anti-fungal Drugs Investigated
Antifungal Susceptibility: Frequency (%) n = 198
Antifungal Sensitive Intermediate Resistant 𝑥2
(Fisher’s Exact)
p-value
Voriconazole 31 (93.9) 0 (0) 2 (6.1) 20.165 0.028
Fluconazole 27 (81.8) 3 (9.1) 3 (9.1)
Micafungin 32 (97) 0 (0) 1 (3.0)
Caspofungin 32 (97) 0 (0) 1 (3.0)
Amphotericin B 27 (81.8) 1 (3.0) 5 (15.2)
Flucytosine 33 (100) 0 (0) 0 (0)
Total 182 (91.9) 4 (2.0) 12 (6.1)
7.4 Analysis
Bivariate correlation analysis to determine the correlation between the dependent variable (isolation of Candida) and the risk
factors; diabetes, pregnancy, surgical interventions, catheterization and chronic illnesses showed a strong positive correlation
between pregnancy and the isolation of Candida. Hence, Pregnant women (p = 0.000) stand a relatively higher risk of isolation of
Candida followed by diabetics (p = 0.008), catheterization (p = 0.023) and those patients with chronic illnesses (p = 0.026). No
correlation was found between surgery and isolation of Candida in this study (Table 4).
Table 4 Correlation of Risk Factors and Isolation of Candida
Risk factors associated with isolation of Candida
Correlations Diabetes Pregnant Operated On Catheterization Chronic illnesses
Pearson Correlation 0.136** 0.280** -0.018 0.116* 0.114*
Sig. (2-tailed) /p-value 0.008 0.000 0.727 0.023 0.026
N 384 384 384 384 384
* Correlation is significant at the 0.05 level(2-tailed).
** Correlation is significant at the 0.01 level (2-tailed).
The logistic regression model affirmed that at 5% level of significance, pregnancy (p = 0.000), chronic illness (p = 0.049),
diabetes (p = 0.024) and age (p = 0.024) were statistically significant. The probability of patient acquiring Candida infection and
hence isolation of Candida keeping other factors constant is given by the following equation;
4321
4321
028.0176.196.21.1621
028.0176.12.96x1.162
xxxxe
xxxei
Where 421 ,...;, xxx represents diabetes, pregnancy, chronic illness, age respectively.

INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
43 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
On the other hand, the logistic regression model showed that, surgery (p = 0.398) and catheterization (p = 0.27) were not
statistically significant risk factors associated with the isolation of Candida in Mombasa hospital (Table 5).
Table 5 Logistic Regression Analysis for the Risk Factors
Variables in the Equation B S.E. Wald df Sig.
(p - value)
Exp (B)
(Odds Ratio)
Step 1a
Diabetes 1.162 0.515 5.090 1 0.024 3.196
Pregnant 2.967 0.642 21.384 1 0.000 19.439
Operated On -0.467 0.553 0.715 1 0.398 0.627
Catheterisation 0.595 0.539 1.218 1 0.270 1.813
Chronic Illnesses 1.176 0.599 3.860 1 0.049 3.241
Constant -4.260 2.282 3.487 1 0.062 0.014
a. Variable(s) entered on step 1: Diabetes, Pregnant, Operated On, Catheterization, Chronic Illnesses.
7.5 Risk Estimates
The likelihood of a pregnant woman acquiring Candida is seven times that of non-pregnant women and catheterized patients
are twice as likely to acquire Candida infections as non-catheterized patients. Moreover, patients with chronic illness are three
times riskier of acquiring Candida infections compared to those without chronic illness. Finally, diabetic patients are almost three
times as likely as non-diabetic patients to acquire Candida Infections (Table 6).
Table 6 Risk Estimate for Various Risk Factors
8. Discussion
8.1 Prevalence of Candida
The prevalence of superficial (19.68%) and invasive (12.42%) Candida infections is relatively high in Africa and Middle East
region and a decreasing proportion of Candida albicans in more recent years (Omrani, Pecen, Hajek, Raghubir, & Zigmond,
2014) is seen.
Findings of the current study incriminated Candida 33 (8.6%) as the most prevalent pathogen in urogenital and broncho-
pulmonary infections. Geographic differences could be a contributing factor for the variation in prevalence of Candida (Li et al.,
2013). The prevalence of Candida was high in urine (54.5%) and High vaginal swabs (HVS) (18.2%) samples compared to other
sample types investigated in this study. These findings resonate with those of a North India study which reported that (30.6%) of
patients with complaints of vulvovaginitis grew Candida (Kumari et al., 2013). Candida was isolated from 13 (39.4%) pregnant
women’s samples in this study concurring with the Thika District Hospital study which reported a prevalence of 42.7% of
candidiasis in pregnant women (Menza Nelson, Wanyoike Wanjiru, 2013).
Pregnancy Catheterization chronic illness Diabetes
(pregnant / Non pregnant) (Catheterization / Non
Catheterization)
(chronic illness / no
chronic illness)
(Diabetic/Non diabetic)
Risk estimate value 95% Confidence
Interval
value 95% Confidence
Interval
value 95% Confidence
Interval
value 95% Confidence
Interval
Lower Upper Lower Upper Lower Upper Lower Upper
Odds Ratio 7.217 3.259 15.982 2.278 1.104 4.703 2.898 1.095 7.672 2.717 1.269 5.815
For Cohort
Candida positive
5.293 2.846 9.843 2.102 1.099 4.021 2.530 1.132 5.659 2.434 1.256 4.719
For Cohort
Candida negative
0.733 0.598 0.900 0.851 1.001 0.851 0.873 0.733 1.040 0.896 0.806 0.996
N of valid cases 384 384 384 384
INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
44 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
Further, the results are in congruence with previous studies that identified Candida as an emerging potential pathogen in
patients with broncho-pulmonary diseases (Kali et al., 2013) since it rated sputum (15.2%) samples as the third most prevalent
source of Candida.
8.2 Candida species distribution
The most frequently isolated Candida was Candida albicans (San Miguel et al., 2005), (Celebi, Hacimustafaoglu, Ozdemir,
& Ozkaya, 2008). In congruence with previous studies, which identified Candida albicans as the most common etiologic agent of
fungal infections (Haddadi et al., 1970), (Menza Nelson, Wanyoike Wanjiru2, 2013), (Mutua, Revathi, & Machoki, 2010), the
proportion of Candida albicans (90.9%) was significantly higher than Candida tropicalis (1.9%) in this study. No other Candida
was isolated. The findings of Candida albicans as the most predominant Candida in all sample types corresponds with a study in
India which identified Candida albicans as the most predominant in pulmonary Candidiasis (Kali et al., 2013). Contrary to a study
which reported an increasing prevalence of vulvo vaginitis due to non-albicans Candida species (Kumari et al., 2013), this study
reported a very low proportion of non albicans Candida amongst vaginal samples. This could be attributed to geographical
variation (Falagas et al., 2010), (Li et al., 2013), Candida tropicalis has been identified as the most prevalent of the non-Candida
albicans group (Kothavade, Kura, Valand, & Panthaki, 2016), (Ann et al., 2007). Furthermore, this study concurs with a study in
Brazil which reported Candidaalbicans83(92.3%) as the most predominantly isolated Candida from pregnant women (Dias,
Souza, Melhem, Szeszs, & Filho, 2011).
8.3 Antifungal susceptibility profiles
Although the and antifungal resistance of Candida differ among geographies necessitating localized surveys of the prevalence
and drug resistance of Candida in order to ensure effective antifungal therapy against invasive Candida (Li et al., 2013), routine
typing and antifungal susceptibility testing of Candida isolates prior to therapy has not been given appropriate attention to
determine the occurrence of resistant genotypes and consequently, there is no data about prevalent Candida and their antifungal
susceptibility patterns in some regions (Mukasa et al., 2015). Also culture procedures are considered to be expensive, time
consuming thus leading to a delay in the treatment and there is a risk of loss of patients on follow-up (Dias, Souza, Melhem,
Szeszs, & Filho, 2011b).
Majority of the Candida responded well to the antifungal drugs investigated in this study. However, the finding of some
resistant Candida isolates here is supported by studies that reported trends of increasing resistance to antifungal agents amongst
some Candida infections [(Cisterna, Ezpeleta, & Tellería, 2005),(Ingham et al., 2012)].
In the current study, 3 (9.1%) Candida showed resistance and 3 (9.1%) intermediate responses to Fluconazole. 2(6.1%)
Candida showed resistance to Voriconazole. Fluconazole resistance has been reported albeit at higher prevalence (13.6 % )
(Aguilar et al., 2015) compared to the current findings.
Azole resistance has been reported as a cause of recurrent vulvovaginal candidiasis and has been associated with the use and
occasional overuse of Fluconazole (White, Marr, & Bowden, 1998) and in surgical intensive care patients treated with
Fluconazole. Amphotericin B recorded the highest 5 (15.2%) Candida isolates resistance in the current study. Several strains of
Fluconazole and Amphotericin B-resistant Candida albicans have been found elsewhere in HIV infected patients who have
received prolonged courses of antifungal prophylaxis with azoles (White et al., 1998).All 33 (100%) Candida were sensitive to
Flucytosine hence it was affirmed that Flucytosine is a potent antifungal agent. This confirms that although there is primary
resistance to Flucytosine, its prevalence remains very low in certain yeasts (1%–2% among Candida isolates). However,
secondary resistance to Flucytosine is common in patients receiving Flucytosine monotherapy (Lopez-ribot et al., 1998), (Hope et
al., 2004). Caspofungin is the most effective agent against all Candida species (Haddadi et al., 1970) hence the minimal resistance
to Micafungin (3.03%) and Caspofungin (3.03%) in this study. However, although echinocandin drugs are recommended as the
first line for invasive candidiasis, reports of echinocandin resistance in patients with infections due to resistance in Candida
glabrata has increased (Alexander et al., 2013).
8.4 Risk factors associated with isolation of Candida
8.4.1 Pregnancy
Patients who presented with candiduria were younger, more commonly female and pregnant (Achkar & Fries, 2010). This
study reported a (39.4%) prevalence of Candida in pregnant women correlating with a prevalence of 36% vulvovaginal
candidiasis among pregnant women in Nigerian cities (Olowe, Makanjuola, Olowe, & Adekanle, 2014) and 45.4% prevalence of
Candida in HVS samples in Mbarara, Uganda (Mukasa et al., 2015). Chi-square test confirmed that indeed pregnancy was a
significant risk factor associated with isolation of Candida. This could be attributed mainly to the fact that pregnant women have
relatively reduced immunity [(Nnaemeka, 2010), (Mukasa et al., 2015)]that predisposes them to developing candidiasis of the
genitourinary tract. Although Candida albicans often colonises the vagina (Apalata, B, Aw, Wh, & Moodley, 2014) and Candida
INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
45 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
also live commensally in the genitor-urinary tract [(S et al., 2016)]. Candida infections mainly occur as opportunistic infections
due to altered conditions of the host [(Okungbowa, Isikhuemhen, & Dede, 2003),(Apalata et al., 2014)].The change in pH of
vaginal secretions from an alkaline pH to an acid pH during pregnancy facilitates thriving of Candida organisms [(Apalata et al.,
2014), (Kamath, Pais, & Nayak, 2013), (Nnaemeka, 2010)]. Higher estrogen levels (Soong & Einarson, 2009) and higher
glycogen content in vaginal secretions during pregnancy increase a woman’s risk of developing vulvo vaginal candidiasis
(Kamath et al., 2013). Pregnancy is one among several risk factors associated with Vulvovaginal Candidiasis (Apalata et al.,
2014).
8.4.2 Diabetes
The current study in Mombasa hospital established that the prevalence of isolation of Candida in diabetic patients is 3.1%. The
chi-square and logistic regression results revealed that diabetes was a significant risk factor associated with isolation of Candida.
These findings concurred with those of other studies in recognizing diabetes as a significant risk factor associated with isolation of
Candida in various patient sub populations. Diabetes mellitus is one of the common predisposing factors for vaginal Candidiasis
[(Leon, Jacober, Sobel, & Foxman, 2002)]. In a study in Pakistan involving Candida esophagitis, it was revealed that diabetes
mellitus was one of the major risk factors for candidiasis (Yakoob et al., 2003). This is because the elevated glucose levels
characteristic of diabetes provide the carbon needed for Candida overgrowth and infection (S et al., 2016).
8.4.3 Surgical interventions
Colonization with Candida in surgical patients is common and occurs before development into invasive candidiasis (Liew et
al., 2015). An increasing number of serious Candida infections on surgical patients that may be related to improvements in
surgical technique and perioperative care (Marsh, Tally, Kellum, & Callow, 1982). 8(2.1%) patients who had undergone surgery
at the Mombasa hospital had Candida. Surgery was not a statistically significant factor associated with isolation of Candida.
These findings were lower compared to a previous study where Candida were observed in 33% of the colonized patients
confirming the vulnerability of the critically ill surgical patients to fungal infections (Rasilainen, Juhani, & Kalevi, 2015). The
observed difference could be due to the kind of patients selected. The higher prevalence may be due to the focus on critically ill
surgical patients in the former study while the current study has included non-critically ill surgical patients including those
undergoing simple surgeries like caesarean section and appendectomy.
8.4.4 Catheterization
Prolonged duration of catheterization is a common risk factor for fungal infections (Mohammad, 2012) since fungal infections
constitutes a significant proportion of all catheter associated urinary tract infection.
Both Chi-square results (P = 0.023 at 5% level of significance) and logistic regression analysis (P = 0.0026) showed that
catheterization is a significant risk factor associated with isolation of Candida at Mombasa hospital. Moreover, urinary
catheterization, among other factors has also been associated with isolation of Candida and a common predisposing factors for
invasive Candidiasis (Aguilar et al., 2015).
8.4.5 Chronic Illnesses (HIV, Cancer and Renal Transplant)
The advent of the human immunodeficiency virus (HIV) epidemic and the increased use of immunosuppressive drugs for
serious medical conditions dramatically increased the number of persons who are severely immunocompromised (Enrique &
Puebla, 2012) and in whom Candida are the most common cause of fungal infection (Enrique & Puebla, 2012). Such patients
require prolonged prophylactic antifungal treatments due to the risk of developing fungal infections including candidiasis. The
current study indicated that 31(8.1%) patients had chronic illnesses including HIV, cancer and kidney diseases. Chi-square results
revealed a correlation between chronic illnesses and isolation of Candida (P = 0.026 at 5 % level of significance) and concurred
with the logistic regression analysis (P = 0.033). Candiduria occurs typically in elderly, hospitalized, or immunocompromised
patients and in neonates (Achkar & Fries, 2010) hence the findings of high prevalence of Candida in urine (4.7%) specimens in
this study. A higher proportion of samples were collected from elderly (51%) and hospitalized (65.1%) patients. The risk of
isolation of Candida in patients suffering from chronic illnesses in this study concurs with findings of earlier studies where
Candida esophagitis was associated with chronic diseases (Yakoob et al., 2003). Candida infections in the gut occur mostly in
immunocompromised patients, in patients who are on steroid therapy, in those with diabetes mellitus and HIV infection [(Report
& Gupta, 2012),(Omrani et al., 2014)].
9. Conclusions and Recommendations

INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
46 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
Candida 33(8.6%) is a major cause of genitourinary and broncho-pulmonary infections in Mombasa hospital. Candida
albicans 30 (90.9%) and Candida tropicalis 3 (1.9%) were isolated. No resistance to Flucytosine was observed but minimal
resistance in Micafungin (3%) and Caspofungin (3%) was observed. Amphotericin B, Voriconazole and Fluconazole showed
some considerable resistance hence resistance to azoles and Amphotericin B should be envisaged when considering an empirical
or de-escalation treatment strategy. This study affirmed that pregnancy, chronic illness and diabetes were statistically significant
risk factors and provided a model equation for the estimation of the probability of a patient acquiring Candida infections in
Mombasa hospital to aid in prevention approaches.
References
1. Achkar, J. M., & Fries, B. C. (2010). Candida Infections of the Genitourinary Tract, 23(2), 253–273.
https://doi.org/10.1128/CMR.00076-09
2. Aguilar, G., Delgado, C., Corrales, I., Izquierdo, A., Gracia, E., Moreno, T., … Belda, F. J. (2015). Epidemiology of
invasive candidiasis in a surgical intensive care unit : an observational study. BMC Research Notes, 4–9.
https://doi.org/10.1186/s13104-015-1458-4
3. Alexander, B. D., Johnson, M. D., Pfeiffer, C. D., Jiménez-Ortigosa, C., Catania, J., Booker, R., … Pfaller, M. a. (2013).
Increasing echinocandin resistance in candida glabrata: Clinical failure correlates with presence of FKS mutations and
elevated minimum inhibitory concentrations. Clinical Infectious Diseases, 56(12), 1724–1732.
https://doi.org/10.1093/cid/cit136
4. Ann, Y. I., Chai, L., Wang, Y. U. E., Khoo, A. I. L., Chan, F. Y. E. E., & Chow, C. (2007). Predominance of Candida
tropicalis bloodstream infections in a Singapore teaching hospital, (August), 435–439.
https://doi.org/10.1080/13693780701385868
5. Apalata, T., B, L. M., Aw, S., Wh, C., & Moodley, P. (2014). Factors Associated with Symptomatic Vulvovaginal
Candidiasis : A Study among Women Attending a Primary Healthcare Clinic in Kwazulu ‑ Natal , South Africa, 4(3).
https://doi.org/10.4103/2141-9248.133470
6. Celebi, S., Hacimustafaoglu, M., Ozdemir, O., & Ozkaya, G. (2008). Nosocomial candidaemia in children: Results of a
9-year study. Mycoses, 51(3), 248–257. https://doi.org/10.1111/j.1439-0507.2007.01464.x
7. Cisterna, R., Ezpeleta, G., & Tellería, O. (2005). Epidemiology of Bloodstream Candida spp . Infections Observed
During a Surveillance Study Conducted in Spain. Epidemiology Insights.
8. Collins, C. D., Eschenauer, G. a., Salo, S. L., & Newton, D. W. (2007). To test or not to test: A cost minimization
analysis of susceptibility testing for patients with documented Candida glabrata fungemias. Journal of Clinical
Microbiology, 45(6), 1884–1888. https://doi.org/10.1128/JCM.00192-07
9. Colombo, A. L., Nucci, M., Park, B. J., Nouér, S. a., Arthington-Skaggs, B., Da Matta, D. a., … Morgan, J. (2006).
Epidemiology of candidemia in Brazil: A nationwide sentinel surveillance of candidemia in eleven medical centers.
Journal of Clinical Microbiology, 44(8), 2816–2823. https://doi.org/10.1128/JCM.00773-06
10. Dias, L. B., Souza, M. De, Melhem, C., Szeszs, M. W., & Filho, J. M. (2011a). No Title, 1300–1307.
11. Dias, L. B., Souza, M. De, Melhem, C., Szeszs, M. W., & Filho, J. M. (2011b). No Title, 1300–1307.
12. Diaz, M. R., & Fell, J. W. (2004). High-Throughput Detection of Pathogenic Yeasts of the Genus Trichosporon, 42(8),
3696–3706. https://doi.org/10.1128/JCM.42.8.3696
13. Enrique, L., & Puebla, J. (2012). Fungal Infections in Immunosuppressed Patients.
14. Falagas, M. E., Roussos, N., & Vardakas, K. Z. (2010). Relative frequency of albicans and the various non-albicans
Candida spp among candidemia isolates from inpatients in various parts of the world: A systematic review. International
Journal of Infectious Diseases, 14(11), e954–e966. https://doi.org/10.1016/j.ijid.2010.04.006
15. Fothergill, A. W. (2012). Interactions of Yeasts, Moulds, and Antifungal Agents. Interactions of Yeast, Moulds, and
Antifungal Agents: How to Detect Resistance, 65–75. https://doi.org/10.1007/978-1-59745-134-5
16. Haddadi, P., Zareifar, S., Badiee, P., Alborzi, A., Mokhtari, M., Zomorodian, K., … Jafarian, H. (1970). Yeast
Colonization and Drug Susceptibility Pattern in the Pediatric Patients With Neutropenia. Jundishapur Journal of
Microbiology, 7(8), 1–6. https://doi.org/10.5812/jjm.11858
17. Hope, W. W., Tabernero, L., Denning, D. W., & Anderson, M. J. (2004). Molecular Mechanisms of Primary Resistance
to Flucytosine in Candida albicans Molecular Mechanisms of Primary Resistance to Flucytosine in Candida albicans,
48(11), 4377–4386. https://doi.org/10.1128/AAC.48.11.4377
18. Ingham, C. J., Boonstra, S., Levels, S., Lange, M. De, Meis, J. F., & Peter, M. (2012). Rapid Susceptibility Testing and
Microcolony Analysis of Candida spp . Cultured and Imaged on Porous Aluminum Oxide, 7(3), 1–8.
https://doi.org/10.1371/journal.pone.0033818
19. Kabir, M. A., & Ahmad, Z. (2013). Candida infections and their prevention. ISRN Preventive Medicine, 2013(Vvc),
763628. https://doi.org/10.5402/2013/763628
20. Kali, A., Charles, M. P., Joseph, N. M., Umadevi, S., Kumar, S., & Easow, J. M. (2013). Prevalence of Candida co-
infection in patients with pulmonary tuberculosis. Australasian Medical Journal, 6(8), 387–391.
https://doi.org/10.4066/AMJ.2013.1709
INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
47 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
21. Kamath, P., Pais, M., & Nayak, M. G. (2013). Original Research Article Risk of vaginal candidiasis among pregnant
women, 2(9), 141–146.
22. Kanafani, Z. A., & Perfect, J. R. (2008). Resistance to Antifungal Agents : Mechanisms and Clinical Impact, 46.
https://doi.org/10.1086/524071
23. Kojic, E. M., Darouiche, R. O., & Biofilms, C. (2004). Candida Infections of Medical Devices, 17(2), 255–267.
https://doi.org/10.1128/CMR.17.2.255
24. Kothavade, R. J., Kura, M. M., Valand, A. G., & Panthaki, M. H. (2016). Candida tropicalis : its prevalence ,
pathogenicity and increasing resistance to fluconazole, (2010), 873–880. https://doi.org/10.1099/jmm.0.013227-0
25. Kumari, V., Banerjee, T., Kumar, P., Pandey, S., Tilak, R., & Pradesh, U. (2013). Emergence of non-albicans Candida
among candidal vulvovaginitis cases and study of their potential virulence factors , from a tertiary care center , North,
144–147.
26. Leon, E. M. De, Jacober, S. J., Sobel, J. D., & Foxman, B. (2002). women with type 1 and type 2 diabetes, 6, 1–6.
27. Li, F., Wu, L., Cao, B., Zhang, Y., Li, X., & Liu, Y. (2013). Surveillance of the prevalence, antibiotic susceptibility, and
genotypic characterization of invasive candidiasis in a teaching hospital in China between 2006 to 2011. BMC Infectious
Diseases, 13(1), 353. https://doi.org/10.1186/1471-2334-13-353
28. Liew, Y. X., Teo, J., Too, I. A., Ngan, C. C., Tan, A. L., Chlebicki, M. P., … Lee, W. (2015). Candida Surveillance in
Surgical Intensive Care Unit ( SICU ) in a Tertiary Institution. BMC Infectious Diseases, 1–8.
https://doi.org/10.1186/s12879-015-0997-6
29. Lopez-ribot, J. L., Atee, R. K. M. C., Lee, L. N., Kirkpatrick, W. R., White, T. C., Sanglard, D., & Patterson, T. F.
(1998). Distinct Patterns of Gene Expression Associated with Development of Fluconazole Resistance in Serial Candida
albicans Isolates from Human Immunodeficiency Virus-Infected Patients with Oropharyngeal Candidiasis, 42(11), 2932–
2937.
30. Lortholary, O., Desnos-ollivier, M., Sitbon, K., & Fontanet, A. (2011). Recent Exposure to Caspofungin or Fluconazole
Influences the Epidemiology of Candidemia : a Prospective Multicenter Study Involving 2 , 441 Patients ᰔ, 55(2), 532–
538. https://doi.org/10.1128/AAC.01128-10
31. Marsh, P. K., Tally, F. P., Kellum, J., & Callow, A. (1982). Candida Infections in Surgical Patients Risk Factors for
Candida Infection, (January 1977), 42–47.
32. Mayer, F. L., Wilson, D., & Hube, B. (2013). Candida albicans pathogenicity mechanisms. Virulence, 4(2), 119–128.
https://doi.org/10.4161/viru.22913
33. Melhem, M. S. C., Bertoletti, a., Lucca, H. R. L., Silva, R. B. O., Meneghin, F. a., & Szeszs, M. W. (2013). Use of the
VITEK 2 system to identify and test the antifungal susceptibility of clinically relevant yeast species. Brazilian Journal of
Microbiology, 44(4), 1257–1266. https://doi.org/10.1590/S1517-83822014005000018
34. Menza Nelson, Wanyoike Wanjiru2, M. W. M. (2013). Prevalence of Vaginal Candidiasis and Determination of the
Occurrence of Candida Species in Pregnant Women Attending the Antenatal Clinic of Thika. Open Journal of Medical
Microbiology, 2013(December), 264–272. http://dx.doi.org/10.4236/ojmm.2013.34040
35. Mohammad, E. J. (2012). Catheter Associated Fungal Urinary Tract Infection, 11(3), 326–329.
36. Mukasa, K. J., Herbert, I., Daniel, A., Livingstone, K., Joel, B., & Frederick, B. (2015). HHS Public Access, 5(4), 322–
331. https://doi.org/10.9734/BMRJ/2015/13804.Antifungal
37. Mutua, F., Revathi, G., & Machoki, J. M. (2010). SPECIES DISTRIBUTION AND ANTIFUNGAL SENSITIVITY
PATTERNS OF VAGINAL YEASTS SPECIES DISTRIBUTION AND ANTIFUNGAL SENSITIVITY PATTERNS
OF VAGINAL YEASTS, 87(4), 156–162.
38. Nnaemeka, O. (2010). Prevalence of Vaginal Candidiasis among Pregnant Women in Nnewi Town of Anambra State ,
Nigeria ( Pp . 539-548 ), 4(17), 539–548.
39. Okungbowa, F. I., Isikhuemhen, O. S., & Dede, A. P. O. (2003). The distribution frequency of Candida species in the
genitourinary tract among symptomatic individuals in Nigerian cities, 60–63.
40. Olowe, O. A., Makanjuola, O. B., Olowe, R., & Adekanle, D. A. (2014). Original paper Prevalence of vulvovaginal
candidiasis , trichomoniasis and bacterial vaginosis among pregnant women receiving antenatal care in southwestern
nigeria, 4, 193–197. https://doi.org/10.1556/EUJMI-D-14-00027
41. Omrani, A. S., Pecen, L., Hajek, P., Raghubir, N., & Zigmond, J. (2014). Prevalence of invasive and superficial candida
infections in africa and middle east ; a systematic review and meta-analysis, 48(5), 2019.
42. Pappas, P. G., Kauffman, C. A., Andes, D. R., Clancy, C. J., Marr, K. A., Ostrosky-zeichner, L., … Sobel, J. D. (2016).
Clinical Practice Guideline for the Management of Candidiasis : 2016 Update by the Infectious Diseases Society of
America, 62, 1–50. https://doi.org/10.1093/cid/civ933
43. Pappas, P. G., Rex, J. H., Sobel, J. D., Filler, S. G., Dismukes, W. E., Walsh, T. J., & Edwards, J. E. (2004). Guidelines
for treatment of candidiasis. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of
America, 38(2), 161–189. https://doi.org/10.1097/01.idc.0000130888.27859.52
44. Rasilainen, S. K., Juhani, M. P., & Kalevi, L. A. (2015). Microbial colonization of open abdomen in critically ill surgical
patients. World Journal of Emergency Surgery, 1–8. https://doi.org/10.1186/s13017-015-0018-5
45. Report, C., & Gupta, N. (2012). A Rare Cause of Gastric Perforation- Candida Infection : A Case Report and Review of
the Literature, 6(9), 1564–1565. https://doi.org/10.7860/JCDR/2012/4632.2563

INTERNATIONAL JOURNAL OF ACADEMICS & RESEARCH - IJARKE ISSN IJARKE Science & Technology Journal
www.ijarke.com
48 IJARKE PEER REVIEWED JOURNAL Vol. 1, Issue 1 August, 2018
46. S, I. L., Sa, S., Adam, M., Than, L., Thian, L., & Doblin, S. (2016). Yeast Infection and Diabetes Mellitus among
Pregnant Mother in Malaysia, 23(6), 27–34.
47. San Miguel, L. G., Cobo, J., Otheo, E., Sánchez-Sousa, A., Abraira, V., & Moreno, S. (2005). Secular trends of
candidemia in a large tertiary-care hospital from 1988 to 2000: emergence of Candida parapsilosis. Infection Control and
Hospital Epidemiology : The Official Journal of the Society of Hospital Epidemiologists of America, 26(6), 548–552.
https://doi.org/10.1086/502582
48. Soong, D., & Einarson, A. (2009). Motherisk Update Vaginal yeast infections during pregnancy, 55, 255–256.
https://doi.org/10.1002/14651858.CD000225.9.
49. White, T. C., Marr, K. a, & Bowden, R. a. (1998). Clinical, cellular, and molecular factors that contribute to antifungal
drug resistance. Clinical Microbiology Reviews, 11(2), 382–402.
50. Yakoob, J., Jafri, W., Abid, S., Jafri, N., Islam, M., Hamid, S., Jafri, N. (2003). Candida esophagitis : Risk factors in non-
HIV population in Pakistan, 9(10), 2328–2331.