-
1
Case Presentation
Intern 吳廷浩指導醫師: 梁啟源/林剛旭 醫師
-
2
General Data
病歷NO. Q121056104 姓名 :林X川 43y/o 床號 : 1121-1 入院日期 : 0940717
-
3
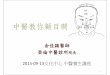
Right hand numbness in this morning
This 43 y/o male patient has no other
systemic disease. He smoke 1 PPD for
20 years but quit for 4 months. Since
yesterday, he felt dizziness. Last noon,
and right hand numbness developed
suddenly and recovered soon. Last night,
it happened again.
-
4
This morning, Right hand numbness developed
again. Right face tremor and then numbness,
deviated to right with dysarthria, dysphasia and
drooling developed transiently. At LMD,
hypertension was noted and anti-HTN drug was
taken. At our ER, brain CT showed no ICH or
mass lesion. Under the impression of stroke, he
was admitted.
-
5
Social Hx, Past Hx
Alcohol drinking: sometimesBetel nut chewing: 10#/QD for 7 years
Cigarette smoking(+): Quit now
Hypertension: NILDiabetes mellitus: NILOperative history: left
foot fracture s/p splint reduction Allergy: No known allergy
-
6
Physical ExaminationGeneral appearance:Vital sign: BT: 36.6C PR:
60/min RR: 16/min BP: 132/97mmHgNeurological
examination:Consciosness clear, GCS E4V5M6Speech:slurredCranial
nerve:Eye:pupil isocoric,EOM full,no nystagmus,no ptosis,VF
normalNo face numbness, open and close mouth normalFacial nerve: no
central palsyTongue protruding no deviationNeck: supple no Kernig
sign, no Brudzinski signMuscle status no atrophyMuscle tone no
rigidity, no spasticity, no tremorMuscle power 5/5DTR ++/++Babinski
sign -/-Sensory modalities: Numbness over right upper limbsPainful
sensation over left hip
-
7
LaboratoryLaboratory : 07/18 07:39 Blood TG 237 mg/dl
07/18 07:39 Blood TCH 220 mg/dl07/18 07:39 Blood U A 6.0 mg/dl
07/18 07:39 Blood HDL-C 46 mg/dl 07/18 07:39 Blood GLU-AC 87 mg/dl
07/17 10:30 Blood BUN 14 mg/dl 07/17 10:30 Blood CRE 1.0 mg/dl
07/17 10:30 Blood GOT/AST 19 IU/L 07/17 10:30 Blood GLU 123 mg/dl
07/17 10:30 Blood K 3.50 mmol/L 07/17 10:30 Blood Na 139.3 mmol/L
07/17 10:30 Blood APTT 28.0 sec 07/17 10:30 Blood Control 28.5
sec
-
8
07/17 10:30 Blood WBC 8.16 *10^3/ul 07/17 10:30 Blood RBC 5.26
*10^6/ul 07/17 10:30 Blood Hb 16.7 g/dl 07/17 10:30 Blood Ht 48.9 %
07/17 10:30 Blood MCV 93.0 fl 07/17 10:30 Blood MCH 31.7 pg 07/17
10:30 Blood MCHC 34.2 % 07/17 10:30 Blood PL 216 *10^3/ul 07/17
10:30 Blood RDW-CV 12.6 % 07/17 10:30 Blood MPV 10.1 fl 07/17 10:30
Blood PT 9.7 sec 07/17 10:30 Blood Control 10.0 sec 07/17 10:30
Blood INR 0.97 07/17 10:30 Blood N.seg. 60.1 % 07/17 10:30 Blood
Lym. 33.2 % 07/17 10:30 Blood Mono. 4.5 % 07/17 10:30 Blood Eosin.
1.7 % 07/17 10:30 Blood Baso. 0.5 %
-
9
-
10
The MRA study of the brain shows normal contour of the vessels
without significant stenosis and without vascular malformation.
-
11
Clinical Course
The patient was admitted due to right face tremor and then
numbness, deviated to right with dysarthria, dysphagia and drooling
developed transiently. The tentative diagnosis was CVA or focal
seizure. Brain CT didn`t show significant finding. However, his
right hemifacial spasm continued without improvement and
didn`tresponse to dilatin.
-
12
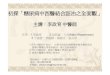
Brain MRI with contrast was arranged and showed no lesion over
brain or right facial nerve which was compatible with ENT`s
opinion. Tegretol and neurontin was prescribed and his symptoms
dramatically relieved. No other newly symptoms was complained
except slurred Speech (improved). Now, the patient was under stable
condition and would follow up at OPD.
-
13
Chapter 355. Trigeminal Neuralgia, Bell's Palsy, and Other
Cranial Nerve Disorders…Harrison’s IM 16E
….. be due to an irritative lesion of the facial nerve (e.g., an
acoustic neuroma, an aberrant artery that compresses the nerve, or
a basilar artery aneurysm). However, in the most common form of
hemifacial spasm, the cause and pathology are unknown …
-
14
Hemifacial spasm can be treated successfully with carbamazepine
or, if this drug fails, with baclofen. Refractory cases due to
vascular compression usually respond to surgical decompression of
the facial nerve …
-
15
Problem
Is any other choice for hemifacial spasm?Botulinum!
-
16
Structure of PICO
Patient/Problem: Hemifacial spasmIntervention:
botulinumComparison, if any: placeboOutcome: Benefit/Long term
follow
-
17
Process of Searching Evidence
-
18
-
19
-
20
-
21
Treatment of hemifacial spasm with botulinum toxin
Department of Neurology, University of California, San
Francisco.
The effectiveness of botulinum toxin injections in 11 patients
with hemifacial spasm was investigated in a prospective
placebo-controlled blinded study.
Muscle Nerve. 1992 Sep;15(9):1045-9
-
22
The patients were treated with four sets of injections to
various facial muscles, selected by clinical evaluation. Three
injections were with graded doses of toxin and one was with
placebo.The order of injections was random and unknown to the
patients. Results were scored both subjectively by patient
assessment of symptoms and objectively by blinded review of
videotapes made one month after each injection.
-
23
Subjective improvement occurred after 79% of injections with
botulinum toxinOnly 1 patient improved after placebo. Objective
improvement was seen after 84% of injections with botulinum
toxin.
The most frequent side effect was facial weakness, seen after
97% of injections of botulinum toxin. Facial bruising (20%),
diplopia (13%), ptosis (7%), and various other mild side effects
were seen less frequently
Botulinum toxin appears to be an effective and safe method of
therapy for hemifacial spasm !!
-
24
Randomized controlBlindedPlacebo-control trialSmall
populationSingle center
-
25
-
26
-
27
-
28
Botulinum Toxin A Treatment for Primary Hemifacial Spasm : A
10-Year Multicenter Study
Background: Botulinum toxin A (BTX) is the currently preferred
symptomatic treatment for primary hemifacial spasm (HFS), but its
long-term efficacy and safety are not known.
Objective: To assess the long-term effectiveness and safety of
BTX in the treatment of primary HFS.
Design: Retrospective review of medical records of the 1st and
10th years of treatment.
Setting: Outpatient clinics of 4 Italian university centers in
the Italian Movement Disorders Study Group.
Participants: A series of 65 patients with primary HFS who had
received BTX injections regularly for at least 10 years.
-
29
-
30
Results: 95% response rate and an overall mean duration of
improvement of 12.6 weeks during year 1.
The effectiveness of BTX remained unchanged in the 1st and 10th
years. Patients needed statistically similar BTX doses in the 1st
and 10th years. The rate of local adverse effects (including upper
lid ptosis, facial weakness, and diplopia) diminished significantly
in the 10th year of treatment.
Conclusion: Treatment with BTX effectively induces sustained
relief from symptoms of HFS in the long term, with only minimal and
transient adverse reactions!!!
-
31
RetrospectiveMulticenterStandard methodLong-term follow up(1~10
years)Population
-
32
Conclusion
Botulinum toxin appears to be an effective and safe method of
therapy for hemifacial spasm !!
Treatment with BTX effectively induces sustained relief from
symptoms of HFS in the long term
-
33Thanks!!
-
34
Comment by Dr.李宜恭
報告History宜用time sequence可讓聽眾就有印象。
Laboratory Data可稍微整理一下,如果是強調Normal就直接寫出來。善於利用EBM
Case PresentationGeneral DataRight hand numbness in this morning
Social Hx, Past HxPhysical ExaminationLaboratoryClinical
CourseChapter 355. Trigeminal Neuralgia, Bell's Palsy, and Other
Cranial Nerve Disorders…Harrison’s IM 16EProblemStructure of
PICOProcess of Searching EvidenceTreatment of hemifacial spasm with
botulinum toxinBotulinum Toxin A Treatment for Primary Hemifacial
Spasm : A 10-Year Multicenter Study�ConclusionComment by Dr.李宜恭