Embed Size (px)
Citation preview
Inter-Professional Care Coordination: Looking to the Future
Susan C. Reinhard, RN, PhD, FAAN
Senior Vice PresidentAARP Public Policy Institute
May 24, 2011
Purpose
• Provide context for panel discussions
• Highlight consumers’ view on why inter-professional care coordination is needed
• Review evidence on care coordination as background for why transitional care is the focus now
• Summarize public policy opportunities provided in ACA
Context: Chronic Conditions
Finally, the US and developed countries are talking about chronic conditions!
Why?
What can we/professionals do?
Inter-professional Care Coordination has become the promise for the future
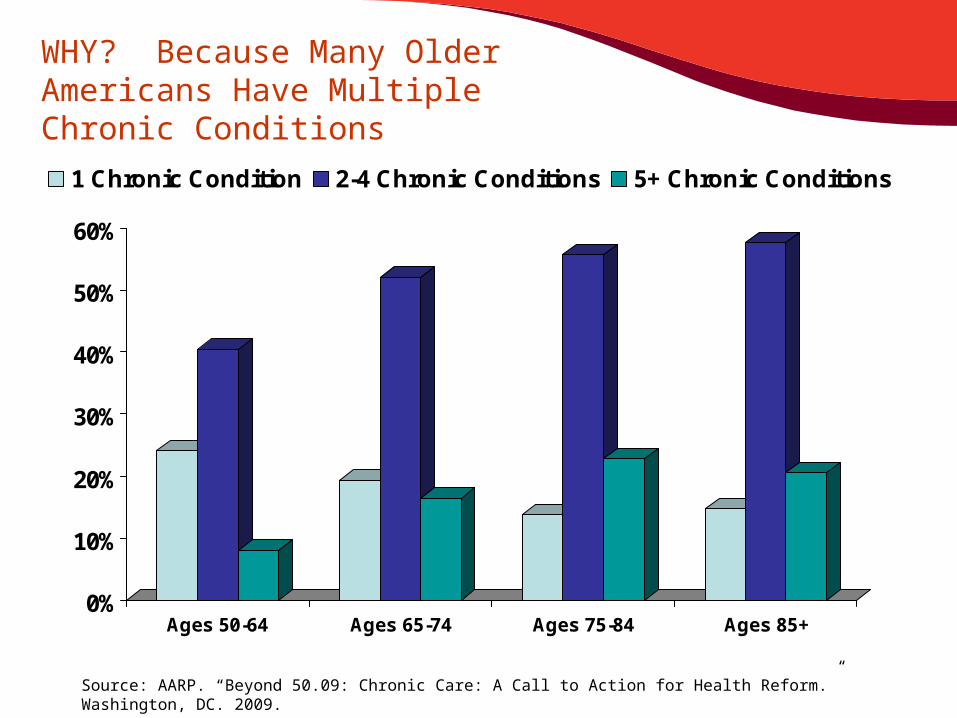
WHY? Because Many Older Americans Have Multiple Chronic Conditions
0%
10%
20%
30%
40%
50%
60%
Ages 50-64 Ages 65-74 Ages 75-84 Ages 85+
1 Chronic Condition 2-4 Chronic Conditions 5+ Chronic Conditions
Source: AARP. “Beyond 50.09: Chronic Care: A Call to Action for Health Reform.” Washington, DC. 2009.
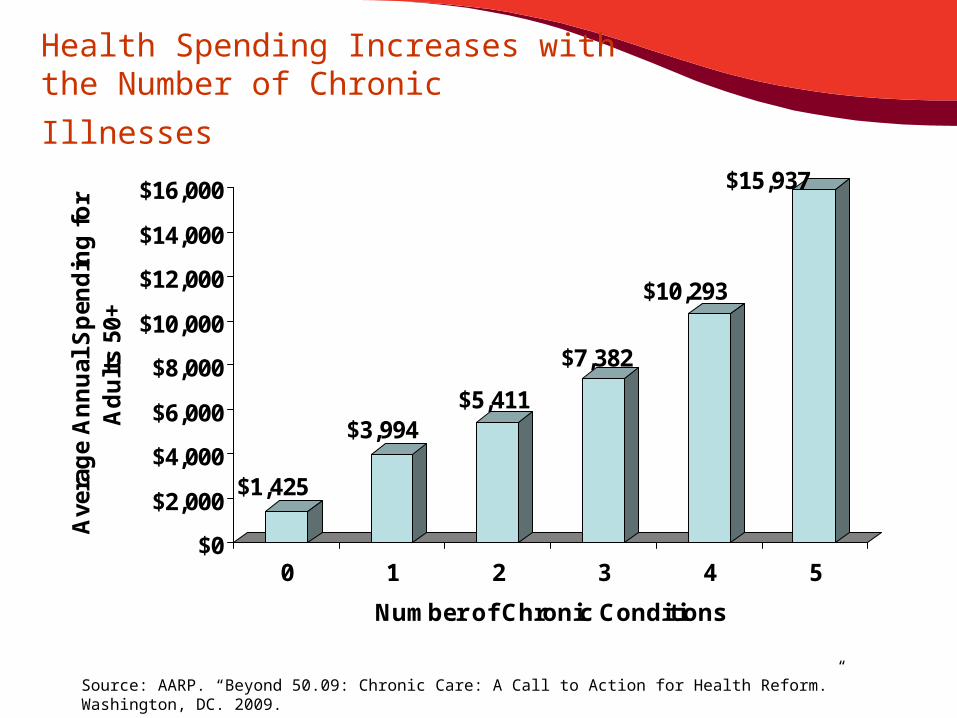
Health Spending Increases with the
Number of Chronic Illnesses
$1,425
$3,994$5,411
$7,382
$10,293
$15,937
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
$16,000
Ave
rag
e A
nn
ual
Sp
end
ing
fo
r A
du
lts
50+
0 1 2 3 4 5
Number of Chronic Conditions
Source: AARP. “Beyond 50.09: Chronic Care: A Call to Action for Health Reform.” Washington, DC. 2009.
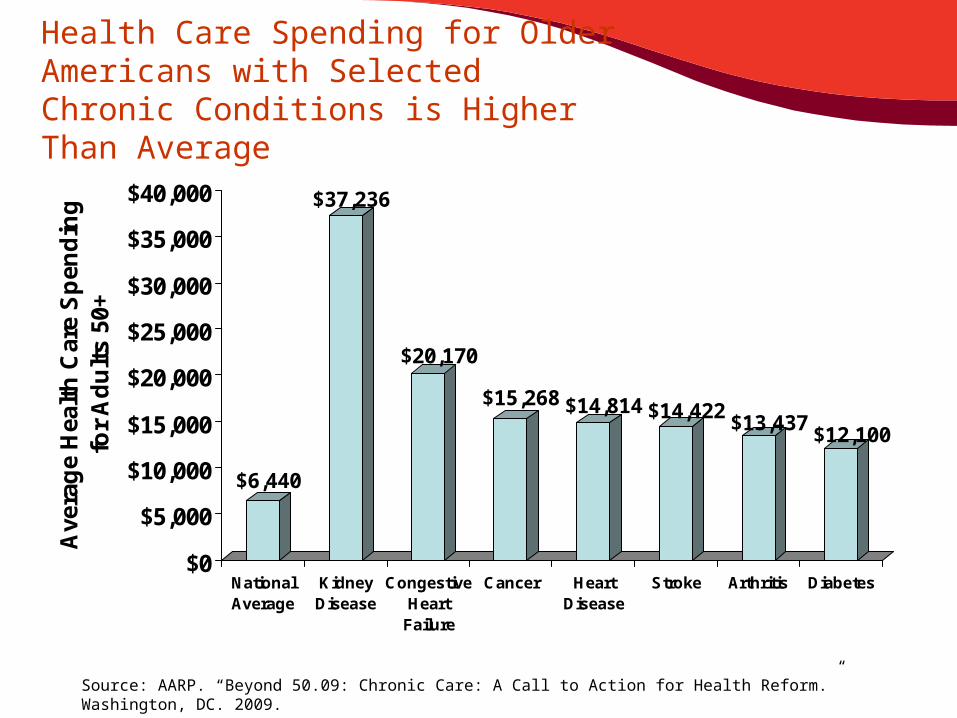
Health Care Spending for Older Americans with Selected Chronic Conditions is Higher Than Average
$6,440
$37,236
$20,170
$15,268 $14,814 $14,422$13,437
$12,100
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
$35,000
$40,000
Ave
rag
e H
ealt
h C
are
Sp
end
ing
fo
r A
du
lts
50+
NationalAverage
KidneyDisease
CongestiveHeart
Failure
Cancer HeartDisease
Stroke Arthritis Diabetes
Source: AARP. “Beyond 50.09: Chronic Care: A Call to Action for Health Reform.” Washington, DC. 2009.
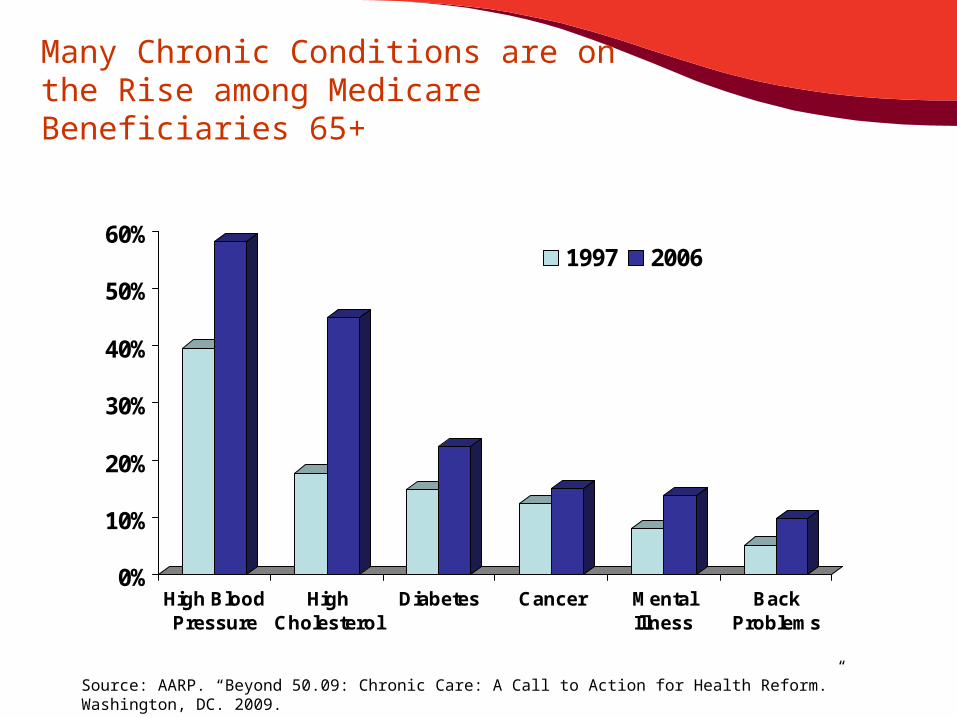
Many Chronic Conditions are on the Rise among Medicare Beneficiaries 65+
0%
10%
20%
30%
40%
50%
60%
High BloodPressure
HighCholesterol
Diabetes Cancer MentalIllness
BackProblems
1997 2006
Source: AARP. “Beyond 50.09: Chronic Care: A Call to Action for Health Reform.” Washington, DC. 2009.
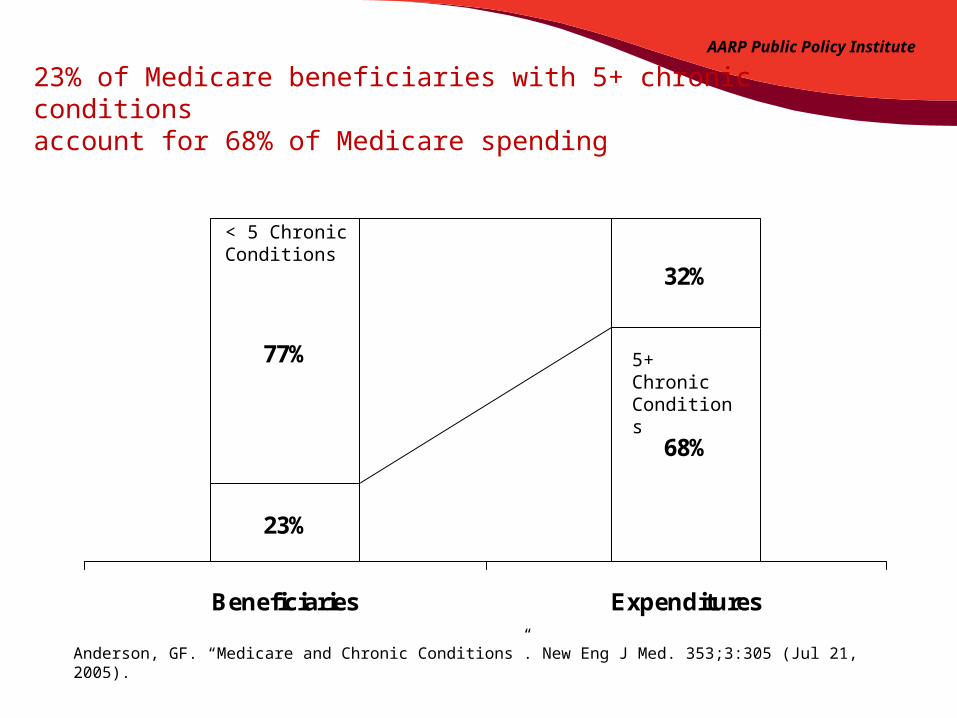
23%
68%
77%
32%
Beneficiaries Expenditures
23% of Medicare beneficiaries with 5+ chronic conditions account for 68% of Medicare spending
Anderson, GF. “Medicare and Chronic Conditions”. New Eng J Med. 353;3:305 (Jul 21, 2005).
5+ Chronic Conditions
< 5 Chronic Conditions
AARP Public Policy Institute
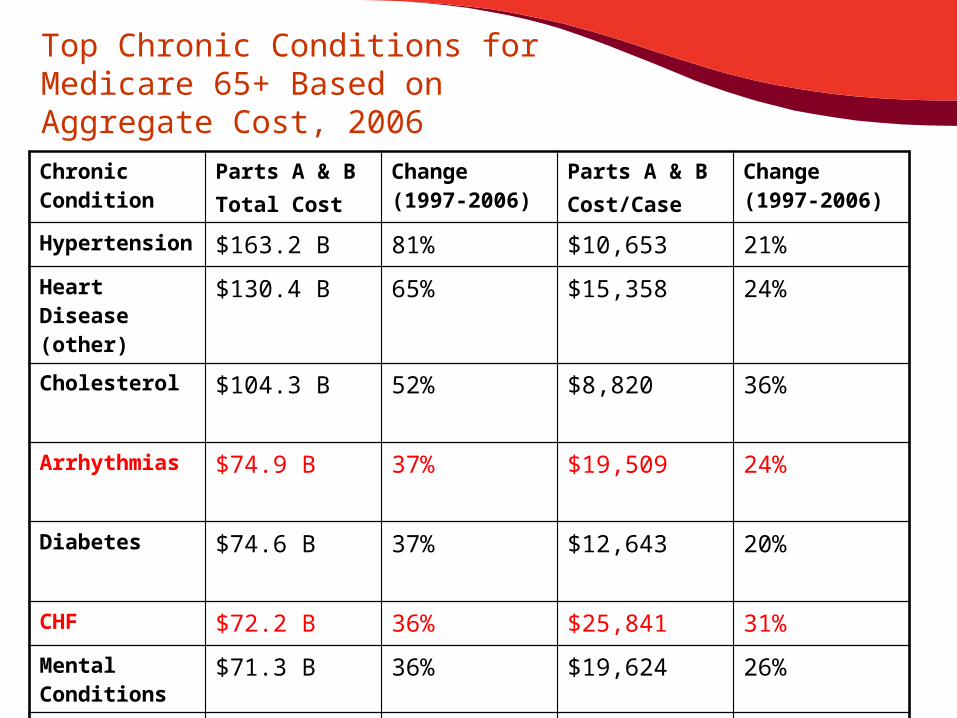
Top Chronic Conditions for Medicare 65+ Based on Aggregate Cost, 2006
Chronic Condition
Parts A & BTotal Cost
Change (1997-2006)
Parts A & B Cost/Case
Change (1997-2006)
Hypertension $163.2 B 81% $10,653 21%
Heart Disease (other)
$130.4 B 65% $15,358 24%
Cholesterol $104.3 B 52% $8,820 36%
Arrhythmias $74.9 B 37% $19,509 24%
Diabetes $74.6 B 37% $12,643 20%
CHF $72.2 B 36% $25,841 31%
Mental Conditions
$71.3 B 36% $19,624 26%
COPD $63.9 B 32% $18,511 27%
Delivery System Problems
• Health care systems (public and private) need improvement, especially chronic care delivery
• Barriers to improvements in care for people with chronic conditions include:– Fragmented care delivery, – Poor transitions across settings, and – Poorly aligned payment incentives that fail to
recognize the value of better integration of services
Delivery System Problems
• Medicare is not perfect and needs improvement
• Care is not well coordinated, particularly for those with chronic conditions
• Fee-For-Service payments encourage over utilization of services
AARP Public Policy Institute Research on Improving Care Coordination and Transitions
Beyond 50.09 Chronic Care: A Call to Action for Health Reform--Consumers’ Views• Data Analysis of Care Coordination for Chronic
Conditions• Focus Groups of patients and caregivers with
transitions• National Opinion Surveys
– Patients with chronic conditions and transitions– Caregivers of patients with chronic conditions and
transitions• Promising Models of Chronic Care Coordination
– Transitional Care Model - Mary Naylor– Care Transitions Intervention - Eric Coleman– Guided Care (medical home w/ transitional care) – Chad Boult
Patients Report Problems with TransitionsThe most frequently reported issues around transitions between hospitals (and other health care facilities) and home were:
– Loss of mobility and/or independence– Uncertain expectations for recovery and/or
prognosis– Pain– Anxiety– Not remembering their clinician’s
instructions– Feeling abandoned
Source: AARP. “Beyond 50.09: Chronic Care: A Call to Action for Health Reform.” Washington, DC. 2009.
Caregivers Report Problems with TransitionsThe most frequently reported issues around transitions between hospitals (and other health care facilities) and home were:
– Finding resources, such as medical equipment and services
– Arranging for assistance in and around the home, both paid and unpaid
– Communication with doctors and other health professionals
– Finances/affordability
Source: AARP. “Beyond 50.09: Chronic Care: A Call to Action for Health Reform.” Washington, DC. 2009.
Chronic Care Coordination
Based on these findings, AARP advanced bipartisan legislation in both houses (rare)
Medicare Transitional Care Act—components incorporated into ACA—one of AARP’s top 6 “asks”
Advocacy from N3C and others very successful!
Source: National Coalition on Care Coordination (N3C)
N3C Definition of Care Coordination
Policy Brief: Implementing Care Coordination in the Patient Protection and Affordable Care Act: “Care coordination” is a person-centered, assessment-based, interdisciplinary approach to integrating health care and social support services in a cost-effective manner in which an individual’s needs and preferences are assessed, a comprehensive care plan is developed, and services are managed and monitored by an evidence-based process which typically involves a designated lead care coordinator.”
Source: National Coalition on Care Coordination (N3C)
Evidence: Medicare Coordinated Care Efforts
Since 1999, Medicare has tested more than 30 chronic care programs involving more than 300,000 traditional Medicare beneficiaries.
– To name a few, these programs have included Medicare Health Support (also known as the Chronic Care Improvement Program),
– The Medicare Coordinated Care Demonstration, – Care Management for High-Cost Beneficiaries
and – The Physician Group Practice Demonstration
Source: Bott DM, Kapp MC, Johnson LB, Magno LM. “Disease management for chronically ill beneficiaries in traditional Medicare.” Health Affairs (2009);28(1):86-98.
Evidence: Medicare Coordinated Care Efforts• Final evaluations on 20 Medicare
Coordinated Care demonstrations found only three had improved quality without substantially increasing Medicare spending, net of program fees.
• Interim assessments of 15 other programs suggest that only four have been able to cover their fees and approximately breakeven.
Source: Bott DM, Kapp MC, Johnson LB, Magno LM. “Disease management for chronically ill beneficiaries in traditional Medicare.” Health Affairs (2009);28(1):86-98.
Medicare Coordinated Care Efforts
An exhaustive survey (Boult, 2009) of successful models of comprehensive health care delivery that have shown potential to improve the quality, efficiency and outcomes of care for chronically ill older persons found that 15 models, including, among others, transitional care, have improved at least one outcome.
Medicare Coordinated Care Efforts
In particular, studies (JAMA, 2009) suggest that a number of elements are important for the success of chronic care coordination programs, including:
– Targeting high cost patients who are at high risk for hospitalization;
– Frequent in-person contact with a health professional (at least once per month);
– Teaching patients how to take their medications;– Strong care coordinator ties to primary care practitioners
(i.e., care coordinators co-located with physicians and each physician’s patients assigned to a single coordinator);
– Care coordinators with timely information about hospitalizations and discharges; and
– Financial incentives to encourage cooperation and collaboration by physicians and other clinicians.

Transitional Care Research
Focus on Transitional Care has become a strong focus of care coordination because:
• Evidence-based research has shown that Transitional Care Services can smooth transitions across care setting, improve care coordination, and reduce costs for high risk patients.
• Transitional Care Services can also be easily incorporated into larger health care delivery system and payment reforms.
Source: Brown, Randall. (Brown, 2009) “The Promise of Care Coordination: Models that Decrease Hospitalizations and Improve Outcomes for Medicare Beneficiaries with Chronic Illnesses.” A Report Commissioned by the National Coalition on Care Coordination, March 2009.
Transitional Care Research
Some key elements of effective Transitional Care Services:
– coordinating early face-to-face contact with patients and families while still in the hospital,
– improving discharge planning by using check lists and patient education tools,
– implementing early follow-up after discharge with in-person home visits,
– performing comprehensive assessment of the patient’s health status, clinical needs, home environment, and social support network,
– developing a care plan, – educating and assisting patients and caregivers about how to
navigate the health care system, find resources and obtain community and supportive services, such as meals-on-wheels and Aging and Disability Resource Centers, and
– following-up to monitor, provide oversight and care coordination, as needed, for up to 90 days.
Source: Brown, Randall. (Brown, 2009) “The Promise of Care Coordination: Models that Decrease Hospitalizations and Improve Outcomes for Medicare Beneficiaries with Chronic Illnesses.” A Report Commissioned by the National Coalition on Care Coordination, March 2009.
National Attention to Chronic Care• ACA has multiple policy tools to change the way people with
chronic conditions get better care, and many involve inter-professional care coordination
• CMS leadership offers fresh, strong, collaborative approach
– “Discovery of duals” by top leaders• 45% of Medicaid spending• 25% of Medicare spending
– Acknowledgement of family caregivers in Congress and CMS
– CMS officials working together to develop integrated RFPs that bring primary, acute, behavioral and LTC together
Payment Reforms that Support Care Transitions and Coordination• Hospital Readmission Reduce Incentives (§
3025)– Penalties for avoidable readmissions (the “stick”)
• Accountable Care Organizations (§ 3022)– Medicare Shared Savings Program– Provider bonuses for saving money and improving quality
• National Payment Bundling Pilot (§ 3023)– Bundled payment for episodes of care – Physicians, acute hospitals and post-acute care providers
Medicare Payment Reforms that Support Care Transitions and CoordinationAvoidable Readmission Penalty (§ 3025)
– Incentive to improve care transitions and reduce avoidable readmissions
– Reduced Medicare DRG payments by 1%, rising to 3%
– For certain avoidable readmissions exceeding a threshold (TBD)
– 3 Target conditions TBD starting in FY 2012, 7 in 2015
– Readmission window TBD (ie, 30 days post discharge)
– Hospital-specific readmission rates will be published on Medicare Hospital Compare website
– Expand to skilled nursing homes and HH Agencies

Medicare Innovations to Improve Care Transitions and Coordination
The “Carrots”• Medicare Community-Based Care Transitions
Program• Medicare Independence at Home Demonstration• CMS Center for Medicare & Medicaid Innovation• Patient-Centered Medical Home Demonstration• Medicaid Health Homes for Chronic Conditions• Community Health Teams for Medical Homes• Workforce Improvements that support Transitional
Care
See PPI Fact Sheet: Health Reform Initiatives to Improve Care Coordination and Transitional Care for Chronic Conditions
Innovations to Improve Care Transitions and Coordination
Community-Based Care Transitions Program (§ 3026)– Hospitals with high Medicare readmission rates,
applications accepted as of April 12, 2011– Partner with Community-based
organizations– Preference for medically underserved areas,
small communities, rural areas and AOA programs.
– Targeting high risk fee-for-service Medicare beneficiaries (many likely to have LTC needs, duals)• Risk score• Cognitive impairment, depression, multiple
readmissions, other factors (TBD)
Innovations to Improve Care Transitions and Coordination
Community-Based Care Transitions Program (§ 3026) continued
– Services must include at least one of 5 interventions• Arranging post-discharge services• Providing self-management support (or
caregiver support)• Conducting medication management review
– Funding of $500 million over 5 years
– CMS will have authority to expand the program if it will reduce Medicare spending without reducing
quality
Innovations to Improve Care Transitions and Coordination
Independence at Home Demonstration (§ 3024)– Starting in 2012 (or sooner), funding of $5 million/5 years– House Calls to help Medicare beneficiaries remain at
home• Medical Practices (MDs and Nurse practitioners) must have
experience delivering home-based primary care, available 24 x 7
• Target Medicare Beneficiaries with Multiple Chronic Illnesses– 2 or more chronic conditions; 2 or more functional dependencies
(ADLs)– Hospitalized in past 12 months (non-elective)– Rehab therapy in past 12 months– Voluntary enrollment of up to 10,000 beneficiaries
– Bonus for savings exceeding 5%
Medicare Innovations to Improve Care Transitions and Coordination
CMS Center for Innovation
• Testing promising models for improving chronic care coordination
• Funding of $1 billion per year for 10 years• Budget neutrality requirement waived during
testing• Authority to expand any model
– Reduces cost but not quality– Increases quality but not cost

Medicare Innovations to Improve Care Transitions and Coordination
Patient-Centered Medical Home Demonstration
– Addressing needs of high-risk Medicare beneficiaries with chronic conditions
– Home health providers and interdisciplinary teams provide chronic care management to Medicare beneficiaries
– Geriatric assessments and comprehensive care plans to coordinate care
Medicaid Innovations to Improve Care Transitions and Coordination
Medicaid Health Homes for Chronic Conditions (§ 2703)– Also known as Medical Homes– State Medicaid Option
• Targets high-risk Medicaid beneficiaries– 2 chronic conditions or– 1 existing chronic condition plus risk of 1 or
more additional or– Serious mental illness
• Services– Enhanced integration and coordination of primary care,
acute care, behavioral care, and long term care– Care management, transitional care, community
support services
Medicaid Innovations to Improve Care Transitions and CoordinationMedicaid Health Homes for Chronic Conditions
(cont)
• Funding– Planning grants starting in 2011, rolling– CMS will base approval on Letter to State Medicaid
Directors, Nov 16, 2010, and subsequent regulations– Matching funds totaling up to $25 million ($500,000 each?)– Over 20 states have expressed interest in planning grants
• Conditions• During first 2 years, 90% federal matching funds for Health
Home services– States must track avoidable readmissions– Estimate savings from care coordination– Report lessons learned
Innovations to Improve All Care Transitions and Coordination
Community Health Teams (§ 3502)• Interdisciplinary teams contract with Medical
Homes– Collaborate with community support services– Teams must be designated by states or Indian
tribes– Chronic care coordination, discharge planning,
transitional care, medication therapy management
(§ 3503), mental health referrals, 24 x 7 availability
– HHS grants: ACA does not authorize funding but HHS has indicated funding will be available
• Teams must become self-sustaining in 3 years• Targets patients with chronic conditions regardless of
payer type (Medicare, Medicaid, private)
Duals
• CMS RFP on duals: $1 million per state to 15 states, including New York, to support design
• Inter-professional care coordination critical
• Person-centered models that integrate the full range of acute, behavioral health and long-trm supports and services
• Does not prescribe managed care per se---CMS open to innovative models
Selected Workforce Improvements
Key workforce improvement programs authorized under ACA include (funding is pending for several of these initiatives):
• establishment of a National Health Care Workforce Commission to review projected workforce needs (ACA § 5101);
• training grants in primary care to educate students in team-based approaches to care, including patient-centered medical homes (ACA § 5301);
Resources
• AARP Public Policy Institute– Health Reform Legislation – Key Facts
• www.AARP.Org• Center to Champion Nursing in America
– http://championnursing.org/
• White House / HHS Health Reform Information– www.HealthCare.Gov
• Medicare – www.Medicare.Gov– www.CMS.Gov
Inter-Professional Care Coordination• Thank you!• Questions?• Susan C. Reinhard, RN, PhD