Embed Size (px)
Citation preview

J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8
ª 2 0 1 8 P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E
A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
MINI-FOCUS ISSUE: HOSPTIALIZED HEART FAILURE AND CONGESTION
STATE-OF-THE-ART REVIEW
Integrative Assessment of Congestionin Heart Failure Throughout thePatient Journey
Nicolas Girerd, MD, PHD,a Marie-France Seronde, MD, PHD,b Stefano Coiro, MD,c Tahar Chouihed, MD,a,dPascal Bilbault, MD, PHD,e François Braun, MD,f David Kenizou, MD,g Bruno Maillier, MD,h
Pierre Nazeyrollas, MD, PHD,i Gérard Roul, MD, PHD,j Ludivine Fillieux, PHARMD,k William T. Abraham, MD,l
James Januzzi, JR, MD,m Laurent Sebbag, MD, PHD,n Faiez Zannad, MD, PHD,a Alexandre Mebazaa, MD, PHD,o
Patrick Rossignol, MD, PHD,a on behalf of INI-CRCT, Great Network, and the EF-HF Group
ABSTRACT
ISS
Fro
VabSe
Un
me
lat
Me
TrojPô
Ce
Ins
set
an
IN
Se
Ro
Ag
No
RE
an
Congestion is one of the main predictors of poor patient outcome in patients with heart failure. However, congestion
is difficult to assess, especially when symptoms are mild. Although numerous clinical scores, imaging tools, and
biological tests are available to assist physicians in ascertaining and quantifying congestion, not all are appropriate for
use in all stages of patient management. In recent years, multidisciplinary management in the community has become
increasingly important to prevent heart failure hospitalizations. Electronic alert systems and communication
platforms are emerging that could be used to facilitate patient home monitoring that identifies congestion from heart
failure decompensation at an earlier stage. This paper describes the role of congestion detection methods at key
stages of patient care: pre-admission, admission to the emergency department, in-hospital management, and lastly,
discharge and continued monitoring in the community. The multidisciplinary working group, which consisted of
cardiologists, emergency physicians, and a nephrologist with both clinical and research backgrounds, reviewed the
current literature regarding the various scores, tools, and tests to detect and quantify congestion. This paper
describes the role of each tool at key stages of patient care and discusses the advantages of telemedicine as a means
of providing true integrated patient care. (J Am Coll Cardiol HF 2018;6:273–85) © 2018 Published by Elsevier on
behalf of the American College of Cardiology Foundation.
N 2213-1779/$36.00 https://doi.org/10.1016/j.jchf.2017.09.023
m the aINSERM, Centre d’Investigations Cliniques 1433, Université de Lorraine, CHU de Nancy, Institut Lorrain du Coeur et des
isseaux, Nancy, France, Inserm 1116 and INI-CRCT (Cardiovascular and Renal Clinical Trialists) F-CRIN Network, Nancy, France;
rvice de cardiologie CHU de Besançon, EA 3920, Unité INSERM 942 CHU Lariboisière, Paris, France; cDivision of Cardiology,
iversity of Perugia, School of Medicine, Perugia, Italy; dEmergency Department, CHU de Nancy, France; eEmergency Depart-
nt, Hôpitaux Universitaires de Strasbourg, Strasbourg, France and EA 7293 Stress vasculaire, Fédération de Médecine Trans-
ionnelle de Strasbourg, Strasbourg, France; fStructures de Médecine d’Urgence, Centre Hospitalier Régional, Hôpital de Mercy,
tz, France; gService de cardiologie, Hôpital Emile Muller, Mulhouse, France; hService de cardiologie, Centre hospitalier de
yes, Anatole, France; iCentre de Recherche et d’Investigation Clinique, Service de Cardiologie, CHU de Reims, Reims, France;
le d’activité médico-chirurgicale cardiovasculaire Nouvel Hôpital Civil, Strasbourg, France and Unité d’insuffisance cardiaque,
ntre de compétence des cardiomyopathies; kNovartis Pharma SAS, Rueil-Malmaison, France; lDavis Heart and Lung Research
titute, Ohio State University, Columbus, Ohio; mDivision of Cardiology, Massachusetts General Hospital, Boston, Massachu-
ts; nHospices Civils de Lyon, Hôpital Louis Pradel, Pôle Médico-Chirurgical de Transplantation Cardiaque Adulte, Bron, France;
d the oDepartment of Anesthesiology, Critical Care and Burn Unit, St. Louis Hospital, University Paris, UMR-S942, INSERM and
I-CRCT (Cardiovascular and Renal Clinical Trialists) F-CRIN Network Nancy, GREAT Network, Paris, France. Drs. Girerd,
ronde, Coiro, Chouihed, Bilbaut, Braun, Kenizou, Mailleri, Nazeyrollas, and Rossignol received board fees from Novartis. Drs.
ssignol, Zannad, Mebazaa, Chouihed, and Girerd are supported by a public grant overseen by the French National Research
ency (ANR) as part of the second “Investissements d’Avenir” programme (ANR-15-RHU-0004). Dr. Fillieux is an employee of
vartis. Dr. Abraham is the co-principal investigator (PI) of the CHAMPION trial; a member of Steering Committees of the
DUCEhf and COMPASS-HF trials; is a PI of HOMEOSTASIS trial; and has received consulting fees from St. Jude Medical
d Medtronic. Dr. Januzzi has received grant support from Siemens, Singulex, and Prevencio; consulting income from Roche

ACRONYMS AND
ABBR EV I A T I ON S
AHF = acute heart failure
BNP = B-type natriuretic
peptide
EF = ejection fraction
HF = heart failure
LUS = lung ultrasound
LV = left ventricular
NP = natriuretic peptide
NT-proBNP = N-terminal
fragment pro- B-type
natriuretic peptide
PC = pulmonary congestion
Diagnostics
monitoring
Boston Sci
Quantum G
a compens
Company,
steering co
gnol is a c
Pharma, an
other auth
Teerlink, M
Manuscript
Girerd et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8
Assessing Congestion in Patients With HF A P R I L 2 0 1 8 : 2 7 3 – 8 5
274
P atients with heart failure (HF) oftendevelop congestion that may requireurgent hospitalization, especially if
pulmonary congestion (PC) is present. Devel-opment of congestion leading to HF decom-pensation is a powerful predictor of poorpatient outcome (1–5). Therefore, it may beimportant to better detect and monitorcongestion before it leads to decompensa-tion. However, congestion can be difficultto assess, especially when extrapulmonarysigns of congestion are mild, such as in thesetting of acute PC due to hypertension orin patients nearing discharge from a HFhospitalization.
Increased intracardiac filling pressures oftensilently precede the appearance of congestive symp-toms by days or weeks (1). Increasing filling pressuresare often subtle and difficult to detect, and can bemasked by other comorbidities (e.g., infections).Current European Society of Cardiology guidelinesrecommend treating signs and symptoms of conges-tion so that patients achieve near-optimal volumestatus (6,7). Unfortunately, 50% of patients admittedfor acute heart failure (AHF) are discharged with re-sidual congestion (2), possibly due to an absence of aclear congestion evaluation strategy. Such residualcongestion at discharge is associated with rehospi-talization and death within 6 months after discharge,independent of the underlying pathology (2). Impor-tantly, although current guidelines emphasize theimportance of aggressively treating congestion, theydo not stipulate which congestion targets should beaimed at discharge for AHF hospitalization or in anambulatory setting.
At each stage of the journey of a patient with HF,specific evaluation tools are used to qualify andquantify congestion to support treatment decisions.However, not all of these tools are appropriate for useat each point of clinical care within this journey (i.e.,clinical settings where a patient may be managed).
, Critical Diagnostics, Sphingotec, Phillips, and Novartis; and par
boards for Novartis, Amgen, Janssen, and Boehringer Ingelheim
entific; a consultant for Boston Scientific, CVRx, LivaNova, J
enomics, Takeda, General Electric, Boehringer, Relypsa, ZS Ph
ated speaker with Pfizer and AstraZeneca. Dr. Mebaza has
Novartis, Orion, Roche, Servier, and Vifor Pharma; and has r
mmittee from Cardiorentis, The Medicine Company, Adrenom
onsultant for Bayer, Relypsa, AstraZeneca, Stealth Peptides
d CTMA; has received lecture fees from CVRx from Relypsa; an
ors have reported that they have no relationships relevant t
D, served as Guest Editor for this paper.
received January 30, 2017; revised manuscript received Septemb
The objective of this position paper is to outline the4 types of tools for evaluating and quantifyingcongestion, namely: 1) clinical tools and scores; 2)biological biomarkers; 3) imaging; and 4) pressure(hemodynamics) and impedance-based tools. Therole of each tool is described during key stages ofpatient care and according to the main points ofclinical care.
CLINICAL TOOLS FOR
EVALUATING CONGESTION
SIGNS AND SYMPTOMS OF CONGESTION. Physicalassessment can only detect a moderate to high levelof congestion. Although many clinical signs andsymptoms of congestion have been well characterizedand are recognized by published guidelines (8), nosingle element from clinical history or physical ex-amination can accurately detect the underlying he-modynamic changes that lead to congestion.Dyspnea, orthopnea, systemic edema, jugular venouspressure, and the third heart sound are all importantclinical findings to identify decompensated HF. Areview of clinical signs and symptoms is detailed inthe Online Appendix. However, relying on only 1single clinical finding to identify decompensated HFhas a low sensitivity and poor predictive value (9),whereas the reproducibility of the medical interview,especially to assess dyspnea, is poor (10).
CLINICAL CONGESTION SCORES. Clinical scores thatcombine several clinical indicators have been shown toassess the level of congestionmore accurately than anystandalone indicator (9). Yet, they are more often usedas prognostic rather than diagnostic tools. The Ste-venson classification, Lucas Score, and Rhode Scoreare detailed in the Online Appendix and are reported inTable 1. The EVEREST score, which was developed byAmbrosy et al. in 2013 (2) within the EVEREST (Efficacyof Vasopressin Antagonism in Heart Failure OutcomeStudy with Tolvaptan) trial (Table 1), captures changesin congestion within a hospitalization time frame and
ticipates in clinical endpoint committees/data safety
. Dr. Zannad is a compensated board member for
anssen, Bayer, Pfizer, Novartis, Resmed, Amgen,
arma, AstraZeneca, and Roche Diagnostics; and is
received speaker honoraria from The Medicines
eceived fees as member of advisory board and/or
ed, MyCartis, and Critical Diagnostics. Dr. Rossi-
, Fresenius, Vifor Fresenius Medical Care Renal
d is the cofounder of CardioRenal Diagnostics. All
o the contents of this paper to disclose. John R.
er 15, 2017, accepted September 26, 2017.

TABLE 1 Summary of Key Scores
Key Clinical and Mixed Clinical/Biomarker Scores
Lucas Score(Online Ref. 11)
Rohde Score(Online Ref. 12)
EVEREST Score(Online Ref. 7)
Gheorgiade Score(4)
Dyspnea 0 ¼ None1 ¼ Seldom2 ¼ Frequent3 ¼ Continuous
Orthopnea 1 ¼ Any respiratory distressassociated with lyingdown or perceived need touse >1 pillow to avoidrespiratory distress
Evaluated during thelast weekGraded from 0 to 4
0 ¼ Need no more than1 pillow
4 ¼ At least 1 night spentsleeping in a sittingposition
0 ¼ None1 ¼ Seldom2 ¼ Frequent3 ¼ Continuous
0¼ None1 ¼ Mild (1 pillow)2 ¼ Moderate (>1 pillow)3 ¼ Severe (sleeps sitting)
JVD* 1 ¼ $10 cm H2O Graded from 0 to 40 ¼ Jugulars not visible4 ¼ Crests visible at the
earlobe with thepatient at 30� to 45�
0 ¼ #61 ¼ 6–92 ¼ 10–153 ¼ $15
�1 ¼ <8 and no hepatojugular reflux1 ¼ 8–10 or hepatojugular reflux2 ¼ 11–153 ¼ >16
Rales 0 ¼ None1 ¼ <25%2 ¼ 25%�50%3 ¼ >50%4 ¼ Entire lung
0 ¼ None1 ¼ Bases2 ¼ Up to <50%3 ¼ >50%
Edema 1 ¼ Yes 0 ¼ None1–4 ¼ According to the
indentation at theankle
0 ¼ Absent/trace1 ¼ Slight2 ¼ Moderate3 ¼ Marked
0 ¼ None1 ¼ 1þ2 ¼ 2þ3 ¼ 3þ/4þ
Other bedsideparameters
1 ¼ Increase diuretics duringthe past week
1 ¼ $2 lbs increase since theprevious clinic visit
1 ¼ Third heart sound Fatigue:0 ¼ None1 ¼ Seldom2 ¼ Frequent3 ¼ Continuous
Hepatomegaly:�1 ¼ Absent in the setting of normal JVP0 ¼ Absent1 ¼ Liver edge2 ¼ Moderate pulsatile enlargement3 ¼ Massive tender enlargement
extending to midline
Dynamicparameters
Orthostatic testing:�1 ¼ Significant SBP decrease
or HR increase0 ¼ No change in SBP or
HR and no difficulty1 ¼ Mild difficulty/2 ¼ Moderate3 ¼ Severe/worst6-min walk test:�1 ¼ >400 m/0 ¼ 300–400 m1 ¼ 200–300 m/2 ¼ 100–200 m3 ¼ <100 mValsalva maneuver:�1 ¼ Normal response1 ¼ Absent overshoot pattern2 ¼ Square wave pattern
Nonclinicalparameters
BNP (pg/ml):0 ¼ <100/1 ¼ 100–2992 ¼ 300–500/3 ¼ >500NT-proBNP (pg/ml):0 ¼ <400/1 ¼ 400–1,5002 ¼ 1,500–3,000/3 ¼ >3,000
Setting 4–6 weeks after dischargefrom HF hospitalization
HF outpatient clinic Discharge from HF hospitalization
Interpretation 0 ¼ no congestion1–2 ¼ mild congestion3–5 ¼ major congestionThe score predicts 2-yr
survival:0 ¼ 13% mortality1–2 ¼ 33% mortality3–5 ¼ 59% mortality
$5 ¼ Increased right andleft atrial pressurecompared withpatients with no HFsigns (score ¼ 0)
$3 ¼ Increased theabsolute 6-monthmortality risk by 25%.
A score from 0–18 can beobtained.
Having a discharge score $1is associated with a 10%absolute increase in theprobability ofhospitalization at 6 months.
Having a discharge score $3 isassociated with a 10%absolute increase in theprobability of all-cause deathat 6 months.
No cutoffs are specified.This score emerged from an expert
consensus. It was not constructedfrom a clinical cohort.
*Jugular vein distention (JVD) is measured in seated patients.
BNP ¼ B-type natriuretic peptide; HF¼ heart failure; HR ¼ heart rate; JVP¼ jugular vein pressure; NT-proBNP¼ N-terminal factor pro-B-type natriuretic peptide; SBP ¼ systolic blood pressure.
J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8 Girerd et al.A P R I L 2 0 1 8 : 2 7 3 – 8 5 Assessing Congestion in Patients With HF
275

Girerd et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8
Assessing Congestion in Patients With HF A P R I L 2 0 1 8 : 2 7 3 – 8 5
276
is associated with a markedly increased risk of HFmortality in the 15% of patients with overt clinicalcongestion (2). The Gheorghiade score (4) has beenpromoted as an integrative congestion score, inte-grating bedside clinical parameters, dynamic parame-ters, and natriuretic peptides (NPs) (Table 1).
The respective role of these congestion scores inroutine clinical practice still remains to be determined.However, the EVEREST score is the most evidence-based in the current era of AHF management, and itappears to be the best candidate for routine use.
CIRCULATING BIOMARKERS FOR
EVALUATING CONGESTION
NPs, such as B-type natriuretic peptide (BNP),N-terminal fragment pro-B-type natriuretic peptide(NT-proBNP), and atrial NP, are the most studiedcirculating biomarkers in HF. The characteristics ofNPs are listed in Online Table 1.
Current clinical practice guidelines recommendBNPor NT-proBNP for assisting with the diagnosis of AHF(7,11). Biomarkers are also useful for determiningprognosis after hospitalization, aswell as in the chronicphase of HF. NT-proBNP is likely to become the stan-dard because of its better risk-stratifying properties inthe setting of AHF (12) and its straightforward inter-pretation in patients treated with sacubitril/valsartan.
PLASMA VOLUME, HEMOCONCENTRATION. Severalroutinely assessed biological parameters, such asserum protein, albumin, hemoglobin, and hematocrithave been proposed as surrogate markers of (de)congestion and have been found to be associated withcardiovascular endpoints (13).
Several formulas have also been developed toindirectly estimate plasma volume, using hemoglobinand/or hematocrit, which may therefore be valuablefor monitoring both acute and chronic (de)congestion(14). One simple formula to assess estimated plasmavolume variations is the Strauss formula:
% change in plasma volume ¼ 100
� hemoglobinðbeforeÞhemoglobinðafterÞ � 1� hematocritðafterÞ
1� hematocritðbeforeÞ � 100
An instantaneous version of this formula (Duarte’sformula [14]) enables calculating plasma volumewithout previous hemoglobin and hematocrit data:
ePVS ¼ 1� hematocrithemoglobinðg=dlÞ � 100
RENAL MARKERS. Evaluating renal function is partof routine care in AHF and has links with evaluatingand managing congestion. Worsening renal function
can alternately be a marker of congestion or it mayimply adequate decongestion; increased venouscongestion has been elegantly shown to be themost important hemodynamic factor driving wors-ening renal function in decompensated patients (5).However, other causes of renal dysfunction (dehy-dration following an intensive decongestion, neph-roangiosclerosis, and drug adverse effects) arefrequently observed in patients with HF. The bloodurea nitrogen to creatinine ratio is a useful variable tobetter identify patients with renal dysfunction due tocongestion (15).
LIVER FUNCTION MARKERS. Cholestatic liver injurydue to congestion is primarily observed when centralvenous pressure is particularly high. The resultingright atrial pressure transmitted directly to the he-patic veins impairs hepatocyte function (16). There-fore, bilirubin and gamma-glutamyl transpeptidasehave been suggested as possible biomarkers forcongestion in the appropriate clinical setting.
IMAGING TOOLS FOR
EVALUATING CONGESTION
Radiological findings reflect the anatomical andpathological alterations induced by PC. Traditionally,a chest x-ray is the first-line procedure. X-ray signs(including peri-bronchial cuffing, cardiomegaly, pul-monary venous congestion, or pleural effusion) arereasonably specific but poorly sensitive; negativechest x-ray findings have been reported in a sub-stantial percentage of patients with AHF (17).
Echocardiography is currently the gold standardnon invasive tool for detecting and monitoring HF. Itis most useful in the assessment of HF etiology and inclassifying HF according to the left ventricular (LV)ejection fraction (EF).
Comprehensive echocardiography may serve as abaseline for serial evaluations in patients whoseclinical status may change over time as disease pro-gresses or it may be used to follow therapeutic in-terventions (18). However, it involves a lengthyprocedure that is typically not performed at bedsideother than in intensive care units. Logistically, it isimpractical to repeatedly perform these examina-tions; thus, comprehensive echocardiography is notusually performed at discharge if already performedduring hospitalization. Furthermore, the algorithmused to determine elevated filling pressures can onlybe performed by an experienced cardiologist skilledin echocardiography. Despite these drawbacks,echocardiography remains the gold standard forevaluating blood volume and LV filling pressuresbefore discharge (18). It is superior to clinical scores

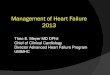
FIGURE 1 Quantification of Pulmonary Congestion and Systemic Congestion Using Echocardiography
Lung ultrasound and quantification of inferior vena cava (IVC) diameters through respiratory cycles. (A and B) Two techniques for quantifying pulmonary congestion
using lung ultrasound (LUS). With the 28 scanning-site LUS technique, a precise quantification of extravascular lung water can be achieved; 16 to 30 comets
(also called B-lines) detected in the entire lung are evocative of moderate pulmonary congestion and >30 comets are evocative of severe pulmonary congestion.
The 8-region LUS technique is a semiquantitative technique. A positive region is defined by the presence of $3 B-lines in a longitudinal plane between 2 ribs and $2
positive regions on each lung, which suggest significant pulmonary congestion. LUS lasts <5 min using both techniques. (C) Upper images: Normally aerated lung and
regular interstitium, the only image that can be visualized below the pleural line is the reflection of the chest wall from the probe to the parietal pleura (A lines), or a
few vertical artifacts can be detected (images with 1 and 2 lung comets). (C) Bottom images: Progressive extravascular lung water accumulation as shown by the
increasing number of lung comets. Lung comets are a simple echographic sign, originating from water thickened interlobular septa. Frequently, images evaluation is
much less reproducible and reliable than video loops, which are important to determine the number of lung comets when they are numerous. Evaluating still images
may be complicated by variations in comet position and strength, as well as a variety of image artifacts that typically occur with lung imaging. These mostly stem from
secondary reflections from the lung surface, and are not comets, resulting in a widely varying comet count. In addition, when comet tail artifacts are confluent, only
real-time loops permit an efficient counting. Even if real-time analysis is more difficult for inexperienced practitioners, we strongly advise using loops to quantify lung
comet count, especially in patients with a moderate to high degree of pulmonary congestion. (Right panels) Right atrial pressures can be assessed with IVC diameters
as shown in the upper and lower right panels.
J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8 Girerd et al.A P R I L 2 0 1 8 : 2 7 3 – 8 5 Assessing Congestion in Patients With HF
277
alone for predicting readmission over short- tomedium-term follow-up (19).
In the emergency department or during clinicalpoints of care, simple echocardiography may be per-formed relatively easily with portable, pocket-sizedultrasound devices. These devices are capable ofmeasuring important variables such as inferior vena
cava diameter, ejection fraction, and the right atrialvolume index.
Lung ultrasound (LUS) is highly useful incomprehensive congestion evaluation at the bedside.LUS produces comet-like images, and the number of“comets” viewed is proportional to the severity ofcongestion (Figure 1). LUS effectively measures the

Girerd et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8
Assessing Congestion in Patients With HF A P R I L 2 0 1 8 : 2 7 3 – 8 5
278
amount of intrapulmonary fluid, indicating PC,which is associated with the level of pulmonaryarterial pressure (20). LUS provides useful informa-tion for the prognostic stratification of patientsadmitted to the emergency department with dyspneaand/or chest pain syndrome (21). In patients hospi-talized for AHF, residual PC as assessed by LUS is astrong predictor of post-discharge outcome (3).Minimum training is required; reproducible resultshave been obtained after 30 min to 1 h of training(22). This technique can rapidly detect changes incongestion over a few hours using freelyavailable and easy to use hand-held ultrasounddevices (23).
PRESSURE AND IMPEDANCE-BASED TOOLS
In some difficult clinical settings, right heart cathe-terization (details described in the Online Appendix)remains the gold standard assessment to evaluateboth right ventricular and LV filling pressures andhemodynamic congestion.
Importantly, and in contrast to the ESCAPE (Eval-uation study of congestive heart failure and pulmo-nary artery catheterization effectiveness) results, theCHAMPION (CardioMEMS Heart Sensor Allows Moni-toring of Pressure to Improve Outcomes in NYHAClass III Heart Failure Patients) trial demonstratedthat tailoring HF management to achieve protocol-defined pulmonary artery pressures according to along-term implanted wireless pulmonary artery he-modynamic monitoring system was associated withfewer HF hospitalizations in patients with chronic HF(1). In CHAMPION, a significant reduction in HF hos-pitalizations was observed in patients with HFreduced EF and patients with HF preserved EF,making pressure-guided HF therapy an option for HFpatients, regardless of LVEF (24). The use of thesewireless devices may change the management of AHFand chronic HF, especially the management ofcongestion in the near future.
Bioimpedance vector analysis is a promisingnoninvasive technique (Online Appendix). Of note,the IMPEDANCE-HF (Outpatient Lung Impedance-Guided Preventive Therapy in Patients With ChronicHeart Failure) trial recently demonstrated that lungbioimpedance-guided management could reducehospitalization rates (25).
APPLYING THE RIGHT TOOL FOR EACH
STAGE OF PATIENT MANAGEMENT
Based on the preceding literature review, the authorsrecommend the following parameters for evaluatingcongestion at each step of patient management until
appropriate discharge (Central Illustration, OnlineTable 2).
PRE-HOSPITAL AND EMERGENCY DEPARTMENT.
Before hospital arrival, the objective is to accuratelyidentify AHF and direct the patient to the appropriateservice. The tools are mainly related to clinicalassessment (including patient history, clinical evalu-ation of breathlessness, and physical examination toassess signs of HF) and may include LUS, BNP, or NT-proBNP measurement. Preliminary data regarding theuse of pre-hospital LUS are promising (26). In theemergency department, most validated tools forassessing congestion are routinely available. Inparticular, our group recommends that LUS should besystematically performed, because it is easy to use,and results are rapid. We also recommend confirmingthe diagnosis with either BNP or NT-proBNP dosing asrecommended by the current clinical guidelines,although the results can take several hours to pro-duce. Because patients with AHF benefit from earlyinitiation of therapeutic interventions (27), conges-tion should be treated as early as possible based onthe LUS results. Therapy can be adjusted lateraccording to the BNP or NT-proBNP results. A chestx-ray should also be systematically performed in theemergency department.
HOSPITALIZATION COURSE THROUGH DISCHARGE. Theobjective of care in the hospitalized setting is tomonitor changes in congestion level and overallcondition following treatment in patients admittedfor congestive symptoms. Because of the risk ofrehospitalization observed in these patients, which isattributable to residual congestion at discharge, werecommend using a repeated multiparameter testingstrategy to achieve the best possible decongestion.This would involve clinical examinations (EVERESTscore), quantitative dyspnea evaluation (Likert,visual analogic score), biological biomarkers (BNP/NT-proBNP concentrations, plasma volume estima-tion based on hematologic data, and liver and kidneybiomarkers in appropriate patients), and ultrasounds(both echocardiography and LUS).
Although clinical evaluation is typically per-formed repeatedly within routine care, only refinedclinical scoring such as the EVEREST score canidentify rapid congestion changes, except in patientsin whom the baseline congestion level is mild.However, this clinical score is time-consuming andrequires clinical expertise; it is rarely performedwith routine care.
NPs could be used to guide decongestion therapy.However, the half-life of NT-proBNP renders it un-suitable to assess rapid congestion changes, and the

CENTRAL ILLUSTRATION Congestion Assessment in HF Patient Journey
Girerd, N. et al. J Am Coll Cardiol HF. 2018;6(4):273–85.
BNP ¼ B-type natriuretic peptide; HF ¼ heart failure; IVC ¼ inferior vena cava; NP ¼ natriuretic peptide.
J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8 Girerd et al.A P R I L 2 0 1 8 : 2 7 3 – 8 5 Assessing Congestion in Patients With HF
279

TABLE 2 Selected Set of Decongestion Targets at Discharge From Hospitalization for Worsening Heart Failure
Congestion Parameter Target at Discharge Reference
Clinical tools
EVEREST score #2 Ambrosy et al. (2).
NYHA functional class #2 Salah et al. The ELAN-HF study. Heart 2014;100:115–25
Biomarkers
NT-proBNP >30% drop during hospitalizationDischarge value <1,500 pg/ml
McQuade et al. (28).Salah et al. The ELAN-HF study. Heart 2014;100:115–25and Kociol et al. The DOSE-AHF trial. Circ Heart Fail 2013;6:240–5
BNP Discharge value <250 pg/ml McQuade et al. (28)
Hemoglobin >10 g/l increase during hospitalization Van der Meer et al. The PROTECT trial. J Am Coll Cardiol 2013;61:1973–81
Imaging tools
IVC imaging Maximum diameter <2.1 cmIVC collapsibility index >50%
Goonewardena et al. J Am Coll Cardiol Img 2008;1:595–601
Lung ultrasound <30 us-B lines Coiro et al. (3) and Gargani. Cardiovasc Ultrasound 2015;13:40
IVC ¼ inferior vena cava; NYHA ¼ New York Heart Association; us ¼ ultrasound.
Girerd et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8
Assessing Congestion in Patients With HF A P R I L 2 0 1 8 : 2 7 3 – 8 5
280
cost of both BNP and NT-proBNP measurementsmakes daily quantification uneconomical and notrecommended. However, a lack of reduction of atleast 30% in the pre-discharge value for either pep-tide or a discharge BNP <250 pg/ml reveals the lack ofsignificant decongestion and of a high risk for repeathospitalization and/or death (28). The Strauss for-mula, based on hemoglobin and hematocrit levels, isa useful, inexpensive, and simple method to assessdaily hemoconcentrations. Nonetheless, it is scarcelyused despite these practical advantages (29).
Echocardiography can be repeatedly performedduring a hospitalization for AHF. However, additionalechographic examinations would be impractical toperform. In contrast, LUS and inferior vena cava echocan be performed at the bedside with a hand-helddevice in several minutes. This simple heart andlung ultrasound captures rapid changes in congestionand provides valuable information to guide choicesfor decongestion therapy (23,30), and may representthe extension of clinical examination in patients withAHF.
Other multimodal evaluations could be envisioned,including clinical evaluations, with special focus onthe determination of dry weight and BNP and/orNT-proBNP quantification at discharge. Measuringin-hospital changes in estimated plasma volume andcomprehensive but simple cardiac and lung echo-graphic data could become the tools of choice duringhospitalization and could be included in this multi-modal evaluation at discharge. LUS- and simplifiedechocardiography�based in-hospital management ofAHF patients has been recently shown to decrease therisk of death or rehospitalization in a proof-of-concept study (30). However, this strategy, asacknowledged previously by our group, has yet to bevalidated in a randomized clinical trial.
Typically, multimodal congestion assessmentcould be most useful upon admission, during decon-gestion therapy, and upon discharge. Ideally, optimaldecongestion should be achieved before patients aredischarged, especially in wet and warm patients withovert signs of clinical congestion at admission, and inwhom congestion is the key driver of hospitalization.A selected set of decongestion targets to achievebefore discharge are proposed in Table 2.POST-DISCHARGE AND LONG-TERM MANAGEMENT.
Patients with AHF remain at high risk of death andrehospitalization in the months after discharge; asmany as 35% of patients are readmitted for AHFwithin a month after the index AHF hospitalizationdischarge (31). With each rehospitalization, the risk ofmortality rises. Accordingly, once discharged, amultidisciplinary disease management team focusedon HF, which includes a cardiologist, a generalpractitioner, and a HF nurse, should follow the pa-tient to reduce the risk of rehospitalization (7).Because of the frequency of early rehospitalizations,the first post-discharge visit with general practi-tioners is advisable within 7 days after the initialdischarge and with the hospital cardiology teamwithin 2 weeks (7). During this phase, simplifiedclinical, biological and imaging resources should beused. Patient-reported clinical status and BNP and/orNT-proBNP or plasma volume, because of their scal-able nature, would be particularly useful in thissetting (Central Illustration, Online Table 2). Inagreement with others (32), we also strongly recom-mend going beyond the clinical evaluation becausesubclinical congestion is frequent. Using biologicalbiomarkers, implantable hemodynamic monitoring,and/or lung bioimpedance monitoring in selectedpatients could easily identify patients with subclinicalresidual congestion who might benefit greatly from

J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8 Girerd et al.A P R I L 2 0 1 8 : 2 7 3 – 8 5 Assessing Congestion in Patients With HF
281
intensive treatment optimization. Importantly,identifying congestion could trigger an increase indosages of life-saving therapy (angiotensin-convertingenzyme inhibitors, beta-blockers, mineralocorticoidreceptor antagonists), diuretics, and/or nitrates.Higher diuretic doses needed to alleviate congestionmight activate the renin-angiotensin-aldosterone sys-tem, which could contribute to the progression of HF.However, analyses adjusted for congestion variablesusually result in a neutral association between diureticdose and outcome (33), which suggests that a higherdegree of congestion, rather than the diuretic dose it-self, is harmful to HF patients.
The GUIDE-IT (Guiding Evidence Based TherapyUsing Biomarker Intensified Treatment) trial, whichalso prioritized an increase of titration of neurohor-monal antagonists over diuretics (i.e., it was notprimarily focused on congestion relief) in patientswith high levels of NPs, provided neutral results (34).The results of GUIDE-IT did not end the discussionregarding NT-proBNP-guided care, because the trialdemonstrated no significant difference in HF thera-pies in the NT-proBNP-guided arm, whereas those inthe usual care arm were seen far more frequentlythan usual (10 visits in 15 months). In total, bothstudy arms had comparable reductions in NT-proBNPduring follow-up, which explained the lack ofdifferences in outcome. Future studies that focus onstricter adherence to NT-proBNP–mandated drugtherapy adjustment, together with a more rationalusual care approach are needed. Importantly, in thesuccessful CHAMPION trial, hemodynamic conges-tion in the intervention group was treated withdiuretics and/or nitrates (i.e., primarily focused oncongestion relief), which eventually alleviatedcongestion and was translated into a lower risk ofreadmission, whereas diuretics and nitrates treat-ment were less frequently changed in the controlgroup. In addition, treatment changes were unrelatedto pulmonary pressure in the control group, whichelicited a poor discrimination of clinical examinationalone (32,35).
INTEGRATING THESE TOOLS INTO
HEART FAILURE NETWORKS:
THE ROLE OF TELEMEDICINE
Although the validated clinical, radiological, andbiological tools discussed in the first section ofthis review might improve patient care both duringpre-hospital admission and in the hospital setting,implementing these tools into community-baseddisease management programs could also providetremendous improvement in patient outcome.
Clinical signs and symptoms that can be easilymonitored in the community setting include heartrate, blood pressure, weight, dyspnea, and edema.Biomarkers such as BNP and/or NT-proBNP and plasmavolume status could also be obtained. Once collected,these data could then be incorporated into eitherexisting or new electronic disease management plat-forms. The value of home-based fingerstick testing forBNP and/or NT-proBNP has been suggested, althoughmore prospective studies are needed.
Telemedicine is likely to be the most useful andscalable solution to implement network manage-ment. However, several randomized trials have re-ported neutral association of remote monitoring withoutcome, including the BEAT-HF (Better Effective-ness After Transition-Heart Failure) trial (36).Importantly, a Cochrane meta-analysis recently pro-vided a comprehensive overview of the currentliterature and reported that “telehealth leads tosimilar health outcomes as face-to-face or telephonedelivery of care” (37). Nonetheless, randomized evi-dence is still insufficient to formally recommend thesystematic use of telemedicine in this setting.
Telemedicine may be a solution to reduce the gapbetween the increase of the older adult populationliving with complex, multimorbid conditions and thedecreasing amount of available health services. Thus,in the future, patient-centered telemedicine couldprobably play a key role in HF patient care, particu-larly by avoiding (re)hospitalizations. Biomarkers(and possibly volume biomarkers) could be of greatinterest in this field, especially if point-of-care ser-vices are developed and used at home by the patientsthemselves (38). Likewise, pulmonary pressure dataderived from wireless devices could be incorporatedinto these telemedicine modalities. A computer-based algorithm that incorporates the patient-reported signs and symptoms and point-of-carebiomarker evaluation could greatly improve patientcare through a telemedicine loop, which wouldtrigger alarms and lead to optimization of treatment.This could be managed by trained nurses and physi-cians possibly via a call platform that is manned for24 h/7 days by emergency callout services.
The economical viability of this approach remainsto be evaluated. Focusing on high-risk populationswould be key to achieve the highest possible treat-ment effect from this strategy. However, most ofthe cost of HF care is currently focused of the cost ofhospitalizations; hence, a dedicated strategy toavoid HF hospitalization could consequently behighly cost-effective. Our group recently quantifiedthe cost-effectiveness of a classical HF managementprogram in a real-world, population-based setting

Girerd et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8
Assessing Congestion in Patients With HF A P R I L 2 0 1 8 : 2 7 3 – 8 5
282
and accordingly found that such a program coulddecrease health costs through a greater decrease inHF hospitalization despite the extra cost related tothe program itself (39). The expected cost-efficiencyof a telemedicine loop, which decreases humancosts, is likely to be similar.
GAPS IN EVIDENCE AND UNMET NEEDS
Congestion is strongly associated with HF prognosis,especially during and following AHF hospitalization.Detection, dynamic monitoring, and management ofcongestion could help improve HF management at allstages of the journey of the patient.
Congestion quantification using a standardizedquantitative approach (e.g., the EVEREST clinicalscore and B-lines count) could represent a valuablemanagement tool upon admission and during an AHFhospitalization. In our view, LUS is a strong candidateto test these congestion-guided treatments becauseof its strong association with outcome (3,23,30). Onemajor aspect that will undoubtedly promote LUSexpansion is the need for early treatment (as early as1 h) after admission to the emergency department asemphasized in the current European Society of Car-diology guidelines for the management of AHF (6,27).The strong association of early treatment usingintravenous loop diuretics with lower in-hospitalmortality supports this recommendation (27). LUScould represent the key practice-changing tool thatwould enable physicians to provide the right treat-ment (i.e., vasodilators and/or diuretics) to the rightpatients (i.e., patients with AHF) as quickly aspossible. In addition, the swift AHF diagnosis that canbe achieved by LUS could allow patients to be triagedto the most appropriate facilities (cardiology ward orintensive care unit with cardiovascular focus) almostimmediately after the first medical contact. Duringthe hospital stay, daily LUS could also guide diureticand/or vasodilator therapy and optimize the timing ofdischarge (30). The impact of LUS-guided AHF man-agement at every step of the AHF hospitalization willultimately need to be tested in specific randomizedclinical trials.
At post-discharge and in ambulatory HF patients,aside from the randomized evidence from theCHAMPION trial (1), there is little evidence that HFmanagement guided by standardized congestionassessment strategies is associated with better prog-nosis. Thus, pulmonary artery pressure–guided HFmanagement should be considered in selected pa-tients, similar to those studied in the CHAMPIONtrial. NPs provide information relative to HF severityas well as congestion, and BNP- and/or NT-
proBNP–guided HF care (which in large part isdependent on treatment and prevention of conges-tion) seems to be appear promising (40). However,the GUIDE-IT trial, which was expected to providedefinitive evidence of the impact of NP-guided ther-apy on clinical outcome in high-risk patients with HF,was terminated for futility and retrieved neutralresults for all considered outcomes (34). Importantly,titration of neurohormonal antagonists over diureticswas prioritized in GUIDE-IT; thus, this study did notprimarily target decongestion in patients with highNP levels. In addition, although there were moreadjustments to therapy in the biomarker-guidedgroup, neither doses of HF therapy nor the achievedNT-proBNP concentrations were significantlydifferent between the treatment groups. Althoughthis would likely decrease our confidence on theefficiency of management mainly or solely based onrepeated NP measurements, it did not, however,solve the question regarding the use of NPmeasurements within a multimodality strategy orthe impact of a strategy based primarily on decon-gestion (as in the CHAMPION trial) guided withNT-proBNP.
There is strong evidence to support the risk-stratifying properties of residual congestion atdischarge for AHF hospitalizations. However,congestion assessed at the beginning (21) or during(19) hospitalization for AHF is also strongly associatedwith outcome. To strengthen the case of congestionas a therapeutic target, it would be useful to assesswhether residual congestion is more, less, or equallyprognostic than initial congestion. Such an analysiswould support that residual congestion is not simplya marker for the severity of illness.
A ROADMAP FOR THE CLINICAL
VALIDATION OF CONGESTION VARIABLES
AS ACTIONABLE BIOMARKERS
FOR HF MANAGEMENT
As already emphasized, established tools such asbiomarker measurement and echocardiography,which are currently used to guide treatment de-cisions, did not require evidence of improvement inoutcomes for their use to be approved (41). Concur-rently, none of the congestion variables were suffi-ciently validated to be considered as a Class I, Level ofEvidence: A, actionable biomarker to guide conges-tion treatment. However, NPs do have a class Irecommendation for HF identification, mostly fortheir ability to detect left-sided congestion. AlthoughNPs provide the strongest evidence of congestionvariables, there is uncertainty regarding the best

FIGURE 2 Current and Future Framework for Congestion Detection
BP ¼ blood pressure; HF ¼ heart failure.
J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8 Girerd et al.A P R I L 2 0 1 8 : 2 7 3 – 8 5 Assessing Congestion in Patients With HF
283
strategy to use in NP-guided therapy in clinicalpractice. Overall, much of the literature on conges-tion consists of observational data.
One limitation of some of the congestion trials wasthe absence of a strictly defined therapeutic strategythat was applied according to biomarker results. Incontrast with most trials in this field, the CHAMPIONtrial used a strict therapeutic algorithmic strategyaccording to congestion assessments (1), which mightbe one of the factors that led to the success of thistrial. Interinvestigator management practice vari-ability could be a major source of “noise” within trialsthat could be reduced by implementing protocol-specified management strategies for treatingcongestion.
Importantly, 2 recently published trials thatinvestigated the effect of vasodilator treatment, theTRUE-AHF (Efficacy and Safety of Ularitide for theTreatment of Acute Decompensated Heart Failure)(42) and RELAX-AHF 2 (Efficacy, Safety and Tolera-bility of Serelaxin When Added to Standard Therapyin AHF) (43) trials, provided neutral results. Theseresults greatly hampered the concept of reachingbetter mid-term outcome by a better and/or smartertreatment of congestion during the early hospitali-zation period. Notwithstanding the latter, it shouldbe acknowledged that in both trials, interventions
lasted for 48 h, and treatment was not tailored to thecongestion phenotype (including hemodynamiccongestion) of patients admitted with AHF. In addi-tion, the CHAMPION trial, which monitored andsubsequently acted on congestion during a longerperiod of time, was successful. From our point ofview, it is likely that future successful AHF trialswould not use decongestion therapies equally,regardless of the congestion profile, but wouldinstead constitute genuine congestion-guided treat-ment trials that use specifically defined individual-ized therapeutic algorithms triggered byindividualized biomarker or clinical assessment tar-gets according to the clinical context. This hypothesisis appealing, although extensive work is needed to fillin the gaps in evidence with regard to optimaldecongestion therapy, especially in the aftermath ofthe results of TRUE-AHF and RELAX-AHF2. From ourstandpoint, there is a need for a trial that tests apersonalized algorithm, in contrast to the strategyused in TRUE-AHF and RELAX-AHF 2, which werebased on LUS and echographic biomarkers ofcongestion during the hospital stay in patients withAHF. In these trials, as in the CHAMPION trial, amanagement algorithm personalized to the clinicalsetting would guide investigator intervention,thus decreasing interinvestigator variability, and

Girerd et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8
Assessing Congestion in Patients With HF A P R I L 2 0 1 8 : 2 7 3 – 8 5
284
ultimately ensuring that the information leads toappropriate interventions. These individualizednovel strategies have the potential to answer manylingering questions related to congestion-basedtreatment of acute and post-acute worsening HF.
From our standpoint, a need for a trial at the initialstage of AHF management still remains, when diag-nostic uncertainty is often still present. The use ofLUS has been successfully explored for triage in pre-hospital pilot studies (44), but its use within thefirst minutes of acute dyspnea management is not yetcommonplace, at least in Europe. We advocate for arandomized trial to investigate the impact of earlyLUS on clinical outcome in patients with acute dys-pnea. Improving the certainty in early diagnosis ofcongestion due to AHF would enable rapid imple-mentation of treatments for AHF worldwide, andpotentially translate into improved outcomes that aredirely needed in this group of patients.
CONCLUSIONS
Evaluating congestion in HF is as complex as it iscrucial, and its timely and effective treatment canimprove outcome (35). Because of the importance ofcongestion in HF, we and others (32), recommendthat assessments extend beyond basic clinical evalu-ations. The currently available various tools need tobe applied in a coherent and effective manner withineach stage of the patient management cycle.
We recommend the use of the EVEREST clinicalscore in most nonemergency situations. NPs (alreadywidely used), together with estimated plasma volumevariables (almost never used), can be useful torepeatedly assess congestion throughout the patientmanagement cycle. LUS is easy to use, provides rapid
results, and may be a practice-changing tool in thepre- and in-hospital management of patients withAHF.
Telemedicine, although currently underdeveloped,could represent the cornerstone for out-of-hospitalmonitoring of patients with HF by mostly using acombination of self-reported clinical congestion var-iables and point-of-care biological data.
The CHAMPION trial convincingly showed thattreating hemodynamic congestion, mostly by opti-mizing diuretics and nitrates, results in better patientoutcomes (1,35). In patients who do not have wirelesspulmonary artery hemodynamic monitoring (as usedin the CHAMPION trial), it appears suboptimal toguide treatment based only on clinical consider-ations. These patients could benefit from a multipa-rameter approach to detect signs of congestion,including clinical evaluation, biological biomarkers,and ultrasound, to improve outcome and reduce re-hospitalizations. The framework in which thesetools could operate in detecting congestion is shownin Figure 2.
ACKNOWLEDGMENTS Medical writing support wasprovided by Amy Whereat for Matrix Consultants andfunded by an unrestricted grant from Novartis Phar-maceuticals (Bâle, Switzerland). The authors alsothank Wendy Gattis Stough and Erwan Bozec for theediting of the paper.
ADDRESS FOR CORRESPONDENCE: Prof. PatrickRossignol, Centre d’Investigations Cliniques-INSERM CHU de Nancy, Institut lorrain du Cœuret des Vaisseaux Louis Mathieu, 4 rue duMorvan, 54500 Vandoeuvre Lès Nancy, France.E-mail: [email protected].
RE F E RENCE S
1. Abraham WT, Adamson PB, Bourge RC, et al.Wireless pulmonary artery haemodynamic moni-toring in chronic heart failure: a randomisedcontrolled trial. Lancet 2011;377:658–66.
2. Ambrosy AP, Pang PS, Khan S, et al. Clinicalcourse and predictive value of congestion duringhospitalization in patients admitted for worseningsigns and symptoms of heart failure with reducedejection fraction: findings from the EVEREST trial.Eur Heart J 2013;34:835–43.
3. Coiro S, Rossignol P, Ambrosio G, et al. Prog-nostic value of residual pulmonary congestion atdischarge assessed by lung ultrasound imaging inheart failure. Eur J Heart Fail 2015;17:1172–81.
4. Gheorghiade M, Follath F, Ponikowski P, et al.Assessing and grading congestion in acute heartfailure: a scientific statement from the acute heartfailure committee of the Heart Failure Association
of the European Society of Cardiology andendorsed by the European Society of IntensiveCare Medicine. Eur J Heart Fail 2010;12:423–33.
5. Mullens W, Abrahams Z, Francis GS, et al.Importance of venous congestion for worsening ofrenal function in advanced decompensated heartfailure. J Am Coll Cardiol 2009;53:589–96.
6. Mebazaa A, Yilmaz MB, Levy P, et al. Recom-mendations on pre-hospital & early hospitalmanagement of acute heart failure: a consensuspaper from the Heart Failure Association of theEuropean Society of Cardiology, the EuropeanSociety of Emergency Medicine and the Society ofAcademic Emergency Medicine. Eur J Heart Fail2015;17:544–58.
7. Ponikowski P, Voors AA, Anker SD, et al. 2016ESC Guidelines for the diagnosis and treatment ofacute and chronic heart failure: The Task Force for
the diagnosis and treatment of acute and chronicheart failure of the European Society of Cardiology(ESC). Developed with the special contribution ofthe Heart Failure Association (HFA) of the ESC. EurJ Heart Fail 2016;18:891–975.
8. McMurray JJ, Adamopoulos S, Anker SD, et al.ESC Guidelines for the diagnosis and treatment ofacute and chronic heart failure 2012: The TaskForce for the Diagnosis and Treatment of Acuteand Chronic Heart Failure 2012 of the EuropeanSociety of Cardiology. Developed in collaborationwith the Heart Failure Association (HFA) of theESC. Eur Heart J 2012;33:1787–847.
9. Stevenson LW, Perloff JK. The limited reliabilityof physical signs for estimating hemodynamics inchronic heart failure. JAMA 1989;261:884–8.
10. Raphael C, Briscoe C, Davies J, et al. Limita-tions of the New York Heart Association functional

J A C C : H E A R T F A I L U R E V O L . 6 , N O . 4 , 2 0 1 8 Girerd et al.A P R I L 2 0 1 8 : 2 7 3 – 8 5 Assessing Congestion in Patients With HF
285
classification system and self-reported walkingdistances in chronic heart failure. Heart 2007;93:476–82.
11. Yancy CW, Jessup M, Bozkurt B, et al. 2013ACCF/AHA guideline for the management of heartfailure: a report of the American College of Car-diology Foundation/American Heart AssociationTask Force on practice guidelines. J Am Coll Car-diol 2013;62:e147–239.
12. Lassus J, Gayat E, Mueller C, et al. Incrementalvalue of biomarkers to clinical variables for mor-tality prediction in acutely decompensated heartfailure: the Multinational Observational Cohort onAcute Heart Failure (MOCA) study. Int J Cardiol2013;168:2186–94.
13. Mentz RJ, Kjeldsen K, Rossi GP, et al. Decon-gestion in acute heart failure. Eur J Heart Fail2014;16:471–82.
14. Duarte K, Monnez JM, Albuisson E, Pitt B,Zannad F, Rossignol P. Prognostic value of esti-mated plasma volume in heart failure. J Am CollCardiol HF 2015;3:886–93.
15. Brisco MA, Coca SG, Chen J, et al. Blood ureanitrogen/creatinine ratio identifies a high-risk butpotentially reversible form of renal dysfunction inpatients with decompensated heart failure. CircHeart Fail 2013;6:233–9.
16. Shinagawa H, Inomata T, Koitabashi T, et al.Prognostic significance of increased serum bili-rubin levels coincident with cardiac decompen-sation in chronic heart failure. Circ J 2008;72:364–9.
17. Collins SP, Lindsell CJ, Storrow AB, et al.Prevalence of negative chest radiography resultsin the emergency department patient withdecompensated heart failure. Ann Emerg Med2006;47:13–8.
18. Kirkpatrick JN, Vannan MA, Narula J, Lang RM.Echocardiography in heart failure: applications,utility, and new horizons. J Am Coll Cardiol 2007;50:381–96.
19. Thavendiranathan P, Yingchoncharoen T,Grant A, et al. Prediction of 30-day heart failure-specific readmission risk by echocardiographicparameters. Am J Cardiol 2014;113:335–41.
20. Gargani L. Lung ultrasound: a new tool for thecardiologist. Cardiovasc Ultrasound 2011;9:6.
21. Frassi F, Gargani L, Tesorio P, Raciti M,Mottola G, Picano E. Prognostic value of extra-vascular lung water assessed with ultrasound lungcomets by chest sonography in patients withdyspnea and/or chest pain. J Cardiac Fail 2007;13:830–5.
22. Noble VE, Lamhaut L, Capp R, et al. Evaluationof a thoracic ultrasound training module for thedetection of pneumothorax and pulmonary edemaby prehospital physician care providers. BMC MedEduc 2009;9:3.
23. Ohman J, Harjola VP, Karjalainen P, Lassus J.Assessment of early treatment response byrapid cardiothoracic ultrasound in acute heartfailure: cardiac filling pressures, pulmonarycongestion and mortality. Eur Heart J AcuteCardiovasc Care 2017 May 1 [E-pub ahead ofprint].
24. Adamson PB, Abraham WT, Bourge RC, et al.Wireless pulmonary artery pressure monitoringguides management to reduce decompensation inheart failure with preserved ejection fraction. CircHeart Fail 2014;7:935–44.
25. Shochat MK, Shotan A, Blondheim DS, et al.Non-invasive lung IMPEDANCE-guided preemp-tive treatment in chronic heart failure patients: arandomized controlled trial (IMPEDANCE-HFTrial). J Cardiac Fail 2016;22:713–22.
26. Prosen G, Klemen P, Strnad M, Grmec S.Combination of lung ultrasound (a comet-tail sign)and N-terminal pro-brain natriuretic peptide indifferentiating acute heart failure from chronicobstructive pulmonary disease and asthma ascause of acute dyspnea in prehospital emergencysetting. Crit Care 2011;15:R114.
27. Matsue Y, Damman K, Voors AA, et al. Time-to-furosemide treatment and mortality in patientshospitalized with acute heart failure. J Am CollCardiol 2017;69:3042–51.
28. McQuade CN, Mizus M, Wald JW, Goldberg L,Jessup M, Umscheid CA. Brain-type natriureticpeptide and amino-terminal pro-brain-type natri-uretic peptide discharge thresholds for acutedecompensated heart failure: a systematic review.Ann Intern Med 2017;166:180–90.
29. Vaduganathan M, Greene SJ, Fonarow GC,Voors AA, Butler J, Gheorghiade M. Hemo-concentration-guided diuresis in heart failure. AmJ Med 2014;127:1154–9.
30. Öhman J, Harjola VP, Karjalainen P, Lassus J.Focused echocardiography and lung ultrasoundprotocol for guiding treatment in acute heartfailure. ESC Heart Fail 2018;5:120–8.
31. Dharmarajan K, Hsieh AF, Lin Z, et al. Di-agnoses and timing of 30-day readmissions afterhospitalization for heart failure, acute myocardialinfarction, or pneumonia. JAMA 2013;309:355–63.
32. Klein L. Treating hemodynamic congestion isthe key to prevent heart failure hospitalizations.J Am Coll Cardiol HF 2016;4:345–7.
33. Pellicori P, Cleland JG, Zhang J, et al. Cardiacdysfunction, congestion and loop diuretics: theirrelationship to prognosis in heart failure. Car-diovasc Drugs Ther 2016;30:599–609.
34. Felker GM, Anstrom KJ, Adams KF, et al. Ef-fect of natriuretic peptide-guided therapy onhospitalization or cardiovascular mortality in high-risk patients with heart failure and reduced
ejection fraction: a randomized clinical trial. JAMA2017;318:713–20.
35. Costanzo MR, Stevenson LW, Adamson PB,et al. Interventions linked to decreased heartfailure hospitalizations during ambulatory pulmo-nary artery pressure monitoring. J Am Coll CardiolHF 2016;4:333–44.
36. Ong MK, Romano PS, Edgington S, et al.Effectiveness of remote patient monitoring afterdischarge of hospitalized patients with heart fail-ure: the Better Effectiveness After Transition –
Heart Failure (BEAT-HF) Randomized Clinical Trial.JAMA Intern Med 2016;176:310–8.
37. Flodgren G, Rachas A, Farmer AJ, Inzitari M,Shepperd S. Interactive telemedicine: effectson professional practice and health care outcomes.Cochrane Database Syst Rev 2015:CD002098.
38. Maisel A, Barnard D, Jaski B, et al. Primaryresults of the HABIT Trial (Heart Failure Assess-ment with BNP in the home). J Am Coll Cardiol2013;61:1726–35.
39. Agrinier N, Altieri C, Alla F, et al. Effectivenessof a multidimensional home nurse led heart failuredisease management program–a French nation-wide time-series comparison. Int J Cardiol 2013;168:3652–8.
40. Troughton RW, Frampton CM, Brunner-LaRocca HP, et al. Effect of B-type natriureticpeptide-guided treatment of chronic heart fail-ure on total mortality and hospitalization: anindividual patient meta-analysis. Eur Heart J2014;35:1559–67.
41. Abraham WT, Stough WG, Pina IL, et al. Trialsof implantable monitoring devices in heart failure:which design is optimal? Nat Rev Cardiol 2014;11:576–85.
42. Packer M, O’Connor C, McMurray JJV, et al.Effect of ularitide on cardiovascular mortality inacute heart failure. N Engl J Med 2017;376:1956–64.
43. Teerlink JR, Voors AA, Ponikowski P, et al.Serelaxin in addition to standard therapy inacute heart failure: rationale and design of theRELAX-AHF-2 study. Eur J Heart Fail 2017;19:800–9.
44. Neesse A, Jerrentrup A, Hoffmann S, et al.Prehospital chest emergency sonography trial inGermany: a prospective study. Eur J Emerg Med2012;19:161–6.
KEY WORDS biomarkers, congestion, heartfailure, lung ultrasound, natriuretic peptides,plasma volume
APPENDIX For supplemental material andtables, please see the online version of thispaper.