Embed Size (px)
Citation preview

7/17/2017
1
FSHP 2017 ANNUAL MEETING
Inpatient Management of Oncology Specialty DrugsInpatient Management of Oncology Specialty DrugsNew Agents, Opportunities, and ChallengesJennifer Swank, PharmD, BCOP
2017 ANNUAL MEETING
#FSHP2017DisclosureDisclosureDo not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with an organization whose philosophy could potentially bias my presentation
2017 ANNUAL MEETING
#FSHP2017Pharmacist ObjectivesPharmacist Objectives• Identify common toxicities of oral oncology therapies in
the internal medicine patient• Describe management of oral oncology therapy toxicity
balanced with internal medicine complications• Discuss the identification and treatment of immune
related adverse events in the internal medicine patient
2017 ANNUAL MEETING
#FSHP2017Technician ObjectivesTechnician Objectives• Recognize oncology therapies by brand/generic name• Identify storage and dispensing issues with these
medications• Apply proper disposal techniques for these medications
in daily practice
2017 ANNUAL MEETING
#FSHP2017Vascular Endothelial Growth Factor (VEGF)Vascular Endothelial Growth Factor (VEGF)• Glycoprotein that activates intracellular signaling by
binding to VEGF receptor• Key role in the maintenance of vascular homeostasis
• Mediation of the production of vasodilator nitric oxide• Decreased vascular resistance trough the generation of new
blood vessels• VEGF inhibition
• Prevention of angiogenesis • Promotion of apoptosis• Causes endothelial dysfunction and increased endogenous
sFlt1 and endothelin-1 production
References: Brinda BJ, et al. Curr Treat Options Cardio Med 2016; 18(33): 1-16. 2017 ANNUAL MEETING
#FSHP2017Inhibiting Tyrosine Kinase SignalingInhibiting Tyrosine Kinase Signaling
References: Chen, MH, etal. Circulation 2008; 118: 84-95.

7/17/2017
2
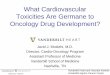
Agent Indication Incidence of all grade HTN Other Cardiotoxicity
Bevacizumab (Avastin®) Cervical, ovarian, colorectal, NSCLC, RCC, GBM 22-24% Thrombosis
Sunitinib (Sutent®) GIST, PNET, RCC 15-34% HF
Sorafenib (Sorafenib®) HCC, RCC, Thyroid 17-29% ACS, HF
Axitinib (Inlyta®) RCC 40% Thombosis
Pazopanib (Votrient®) RCC, Soft tissue sarcoma 36-46% ACS, HF
Levantinib (Lenvima®) RCC, Thyroid cancer 73% QTC changes, thrombosis, CHF
Ziv-afibercept (Zaltrap®) Colorectal cancer 41% Thrombosis
Regorafenib (Stivarga®) Colorectal cancer, GIST 28-48.5% ACS
Ramucirumab (Cyramza®) Colorectal cancer, Gastric, NSCLC 16% Thrombosis
Vandetanib (Caprelsa®) Medullary thyroid cancer 33% QTC changes
Cabozantinib (Cometriq®) Thyroid cancer 32-37% ThrombosisReferences: Brinda BJ, et al. Curr Treat Options Cardio Med 2016; 18(33): 1-16. Key: Non Small Cell Lung Cancer (NSCLC), Renal Cell Carcinoma (RCC), Gleoblastoma multeforme (GBM), Gastrointestinal Stromal tumor (GIST), Pancreatic neuroendocrine tumor (PNET), Acute lymphoblastic leukemia (ALL), Chronic myelogenous leukemia (CML), Myelodysplastic syndrome (MDS)
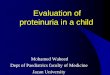
VEGF Induced HTN
Set BP goal & implement lifestyle interventions
Initiate ACEs, ARB, or dihydrophyridine CCB
-Reinforce medication & lifestyle adherence
- Titrate doses of initial medications to max - Add & titrate second agent- If BP not controlled consider adding medication of other class (thiazide, b-blocker)
At BP Goal
Consider therapy with long acting NO donors
At BP Goal
Consider dose reduction or cessation of VEGF therapy
Initiate ACE or ARB
At BP Goal
Yes
Continue current treatment & monioring
Diabetes, Proteinuria or CKDGeneral Population
No
No
No
Yes
Yes
2017 ANNUAL MEETING
#FSHP2017VEGF Toxicity Management VEGF Toxicity Management • Rash: severe dermatologic toxicity rare• Diarrhea: maintain appropriate hydration and treat
symptomatically• Myocardial infarction: use with caution in patients with significant
cardiac history• Thrombosis: monitor for symptoms of clots and treat if identified• Heart Failure: monitor for symptoms of HF or EF reduction, if
symptoms obtain ECHO and discontinue therapy if EF <50% or 10% in baseline EF
• QTC prolongation: baseline EKG, maintain appropriate electrolyte levels, hold therapy if QTC >500msec
• Thyroid abnormalities: order labs if symptoms of hypothyroidism• Many drugs with CYP drug interaction be aware
2017 ANNUAL MEETING
#FSHP2017Bevacizumab (Avastin®)Bevacizumab (Avastin®)• Impaired wound healing
• Discontinue therapy at least 28 days prior to surgery and continue to hold for 28 days post surgery and until wound is healed
• Thromboembolism• Risk factors include h/o of thrombosis, diabetes, >65 years of age
• GI perforation• Higher incidence with tumors involving the bowel
• Hemorrhage• Avoid use in patients with recent hemorrhage or hemoptysis
• Proteinuria/nephrotic syndrome• Withhold treatment for ≥2g proteinuria/24 hours, discontinue if nephrotic
syndrome
2017 ANNUAL MEETING
#FSHP2017Toxicity Monitoring and ManagementToxicity Monitoring and Management• Thromboembolic events• Myocardial infarction• Left ventricular dysfunction• Heart failure (HF)• QT interval prolongation
•BTK: Bruton’s tyrosine kinase, CML: Chronic Myelogenous Leukemia, CLL: Chronic lymphocytic lymphoma , FNHL: Follicular Non-Hodgkin’s Lymphoma, GIST: Gastrointestinal Stromal Tumors, HES: Hypereosinophilic Syndrome MCL: Mantle cell lymphoma, MDS: Myelodysplastic Syndrome PDGFR: Platelet Derived Growth Factor Receptor, SLL: Small Lymphocytic Lymphoma
Drug Indication Toxicity Monitoring
Bosutinib (Bosulif®) CML N/V
Dasatinib (Sprycel®) CML, ALL Pleural effusion, pulmonary arterial HTN CXray
Ibrutinib (Imbruvica®) CLL, MCL, WaldenstromsMacroglobulinemia
lymphocytosis, Afib, bleeding
Idelaisib (Zydelig®) CLL, SLL, FNHL Lymphocytosis, hepatotoxicity Monitor for infections
Imatinib (Gleevac®) ALL, CML, GIST, HES, MDS N/V
Nilotinib (Tasigna®) CML QTC prolongation ECG baseline & electrolytes
Panobinostat (Farydak®) MM Diarrhea, EKG changes EKG baseline
Ponatinib (Iclusig®) MM MI/Stroke Prevention with ACE I & ASA
Ruxolitinib (Jakafi®) Myelofibrosis, PCV QTC prolongation, blood counts EKG baseline & labs
Venetoclax (Venclexta®) CLL Tumor lysis syndrome CMP uric acid and LDH
Vorinostat (Zolinza®) Cutaneous T cell lymphoma Reduced blood counts
2017 ANNUAL MEETING
#FSHP2017Mammalian Target of Rapamycin (mTOR) InhibitorsMammalian Target of Rapamycin (mTOR) Inhibitors• mTOR pathway plays a central role in the control of the
growth of cells• When activated it induces mRNA transcription and
translation of numerous proteins stimulating cell cycle progression, division, and inhibiting apoptosis
• mTOR inhibitors halt cell cycle at G1 phase and blocking downstream phosphorylation of ribosomal proteins; exhibits anti-angiogenesis activity by reducing levels of hypoxia inducible factors (HIF) and VEGF
References:.

7/17/2017
3
2017 ANNUAL MEETING
#FSHP2017Mammalian Target of Rapamycin (mTOR) InhibitorsMammalian Target of Rapamycin (mTOR) Inhibitors
References: Everolimus prescribing informaton 2017 ANNUAL MEETING
#FSHP2017mTOR Inhibitor ToxicitymTOR Inhibitor Toxicity• Drugs• Temsirolimus (Torisel®)• Everolimus (Afinitor ®)• Electrolyte abnormalities
• Hypokalemia, hypomagnesemia, hypophosphatemia
• Hyperglycemia• Hypercholesterolemia• Mucositis• Interstitial pneumonitis
• Monitor for respiratory symptoms and start inhaled corticosteroids• Treatment Prednisone 40mg daily and taper by 10mg every 2 weeks• Perminately discontinue mTOR therapy
References: Martins F, et al. Oral Oncology 2013;49:293-98. Annelieke EC, et al. Int J Cancer 2016; 138: 2312-21.
2017 ANNUAL MEETING
#FSHP2017
Immuno-Oncology: The Pharmacist Perspective
Immuno-Oncology: The Pharmacist Perspective
2017 ANNUAL MEETING
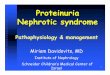
#FSHP2017T Cell Antitumor ResponseT Cell Antitumor Response
References: Andersen MH, et al. J Invest Dermatol 2006; 126(1):32-41; Pardoll DM. Nat Rev Cancer 2012; 12(4):252-64; Mellman I, et al. Nature 2011; 480(7378):480-9; Heemskerk B, et al. EMBO J 2013; 32(2):194-203; Boudreau JE, et al. Mol Ther 2011; 19(5):841-53
Tumor antigens released bytumor cells
Tumor antigens presented to T cells T cells are
activated and proliferate
T cells recognize tumor antigens
T cells kill tumor cells
1
4
23
5
2017 ANNUAL MEETING
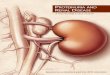
#FSHP2017Tumor Mechanism to Evade Immune SystemTumor Mechanism to Evade Immune System
References: Drake CG, et al. Adv Immunol 2006; 90:51-81; Vesely MD, et al. Annu Rev Immunol 2011; 29:235-71.
(e.g., T-reg)
(e.g., TGF-B)
(e.g., down-regulation of MHC I)
(e.g., disruption of T cell checkpoint pathways)
Inhibition of tumor antigen presentation
1
Secretion of immunosuppressive factors
2
Inhibition of attack by immune cells
3
Recruitment of immunosuppressive
cell types
4
APCTumor Cell
T-regActivated
T cell
2017 ANNUAL MEETING
#FSHP2017T-Cell Checkpoint RegulationT-Cell Checkpoint Regulation• T-cell responses are regulated
through a complex balance of inhibitory (“checkpoint”) and activating signals
• Tumors can dysregulate checkpoint and activating pathways, and consequentlythe immune response
• Targeting checkpoint and activating pathways is an evolving approach to cancer therapy, designed to promote an immune response
References: Mellman I, et al. Nature 2011; 480(7378):480-9; Pardoll DM. Nat Rev Cancer 2012; 12(4):252-64
PD-1
CTLA-4
Inhibitory receptors
Activating receptors
TIM-3
LAG-3
Antagonistic (blocking) antibodies
Agonistic antibodies
T-cell stimulation
CD28
OX40
CD137

7/17/2017
4
2017 ANNUAL MEETING
#FSHP2017Mechanism of Action of Checkpoint InhibitorsMechanism of Action of Checkpoint Inhibitors• Anti-PD-1 therapies are designed to bind to PD-1 on activated T
cells in tumor microenvironment, Anti-CTLA-4 agents are designed to act by binding to CTLA-4 on activated T cells in the lymph nodes.
References: Wolchok J, et al. J Clin Oncol 31, 2013 (suppl; abstr 9012^); Wolchok JD, et al. New Engl J Med 2013; 369(2):122-33
2017 ANNUAL MEETING
#FSHP2017Available AgentsAvailable Agents• Cytotoxic T-lymphocyte antigen 4 (CTLA-4) inhibitor
• Ipilimumab (Yervoy®)• Programmed cell death-1 (PD-1) inhibitors
• Nivolumab (Opdivo®)• Pembrolizumab (Keytruda®)
• Programmed cell death ligand-1 (PDL-1) inhibitors• Atezolizumab (Tecentriq®)• Avelumab (Bavencio®)• Durvalumab (Imfinzi®)
References:.
2017 ANNUAL MEETING
#FSHP2017Toxicity of Checkpoint InhibitorsToxicity of Checkpoint Inhibitors• Therapies designed to enhance the patient’s immune
response against the tumor can result in novel spectrum of adverse events arising from the activation of the immune system
• Termed “immune related adverse events (IrAEs)• May be due to cytokine release by activated T cells• May be unfamiliar to clinicians• Can be serious and potentially fatal• Requires prompt recognition and treatment• Requires education of the patients and healthcare team
References:
Skin•Skin rash or pruritus
Hepatic•Abnormal LFTs (e.g., AST, ALT, total bilirubin)
Renal•Abnormal SCR
Gastrointestinal•Diarrhea•Stomach pain •Nausea/vomiting/pain
•Blood in stool •Constipation
Endocrine•Headache •Visual changes •Fever •Fatigue/weakness •Confusion
Pulmonary•SOB on excertion•Hypoxia•Cough
Neurologic•Sensory or motor neuropathy
•Muscle weakness •Fatigue •Difficulty waking up
2017 ANNUAL MEETING
#FSHP2017Role of PharmacistRole of Pharmacist• Understanding irAEs:
• Diarrhea is common with CTLA-4 inhibitors but less common with PD-1/PDL-1 therapies
• Rash is common, but severe dermatitis is not• Endocrinopathies, hepatitis, and nephritis are uncommon• Infusion reactions are very rare• Pneumonitis and neurologic toxicities are very rare
• Early recognition of irAEs• Familiarity with side effects of newer therapies• Awareness of timing/onset of irAEs to ensure quick diagnosis
and prompt initiation of treatment• irAEs are dose-dependent, schedule-related, and
cumulative• irAEs are correlated with response
Referenc es: Weber JS, et al. J Clin Oncol 2012; 30(21):2691-7; Tarhini A. Scientifica (Cairo) 2013; 2013:857519
2017 ANNUAL MEETING
#FSHP2017Kinetics of irAEsKinetics of irAEs
References: Weber JS, et al. J Clin Oncol 2012; 30(21):2691-7.
Rash, pruritisLiver toxicityDiarrhea, colitisHypophysitis
Toxi
cit
y g
rad
e
0 2 4 6 8 10 12 14
Weeks

7/17/2017
5
2017 ANNUAL MEETING
#FSHP2017Early Diagnosis and ManagementEarly Diagnosis and Management
Immune-related adverse
reactions
Result from increased or
excessive immune activity
Patient education for early recognition
Systemic high-dose corticosteroids*
may be required for severe events
Unless an alternate etiology
has been identified,
consider all signs and symptoms
Can be severe or life-threatening;
may involve various organs
Early diagnosis and appropriate management is
essential to minimise
life-threatening complications
2017 ANNUAL MEETING
#FSHP2017Guidelines for irAE TreatmentGuidelines for irAE Treatment
FOLLOW-UPResolved or improved to
grade 1
• Continue immunotherapy if grade 1 or 2 toxicity once steroids tapered to ≤ 10mg/day Prednisone equivalent
Ongoing symptoms
• If symptoms persist, treat as per organ-specific irAE algorithm
• If no improvement or in severity, permanently discontinue immunotherapy
Assess symptoms and
grade appropriately via CTAE 4 guidelines
Gra
de
3 &
gra
de
4
Gra
de
2
Treatment
• Follow organ-specific irAE guidelines
irAE MANAGEMENT
Gra
de
1
Don’t forget:GI prophylaxis for long-term steroid useConsider PCP prophylaxis for long-term high-dose steroid use
2017 ANNUAL MEETING
#FSHP2017Cutaneous Toxicity ManagementCutaneous Toxicity Management• Symptoms: erythematous and/or maculopapular rash,
dry skin, pruritus, vitiligo, blisters, ulceration, bullae, necrotic or hemhorrhagic lesions
References: Weber JS, et al. J Clin Oncol 2012; 30(21):2691-7., Eigentler TK, et al. Cancer Treatment Reviews 2016; 45:7-18.
Mild (Grade 1)<10% BSA
Moderate (Grade 2)10-30% BSA
Severe (Grade 3 /4)>30% BSA, blisters, ulceration, bullae, necrotic or hemhorragic
lesions, TEN
Treat symptomatically: topical moisturizers, topical/oral antihistamines, antipruritic agents
Consider hospitalization, dermatology consult and biopsyConcern for secondary infection start empiric antibioticsMethylprednisolone IV 1-2 mg/kg/dayConcern for TEN, DRES, or SJS need burn unit careIf symptoms improve then 4-6 week steroid taperDiscontinue immunotherapy
Treat symptomatically as above Topical steroids (hydrocortisone/triamcinolone)Persistent symptoms 1-2 weeks then start Prednisone 0.5 mg/kg/day 2-3 week steroid taper if responds to <grade 1Persists or worsens treat as Grade 3 /4
2017 ANNUAL MEETING
#FSHP2017Gastrointestinal Toxicity ManagementGastrointestinal Toxicity Management• Symptoms: changes in bowel habits, abdominal pain,
blood or mucus in stool, nausea • Rule out other causes (ie. Infection)
References: Weber JS, et al. J Clin Oncol 2012; 30(21):2691-7., Eigentler TK, et al. Cancer Treatment Reviews 2016; 45:7-18.
Mild (Grade 1)Diarrhea <4 stools/dayColitis asymptomatic
Moderate (Grade 2)Diarrhea 4-6 stools/day
Colitis: abd pain, blood in stool
Severe (Grade 3 /4)Diarrhea ≥ 7 stools/day, need for IVF, interfering with ADL
Colitis: severe abd pain, ileus, or peritoneal signs
Treat symptomatically: Imodium 4mg at onset of loose stool & 2mg after each loose stool (max 16mg/day)Lomotil #2 tabs po every 6 hours as needed
Hospitalization, strict NPO, CT Abd/pelvis, consider GI Endoscopy consult or GI surgery consult if peritoneal signsMethylprednisolone IV 2 mg/kg/dayIf symptoms improve then 4-6 week steroid taperIf symptoms persist >3 days or relapse with steroid taperInfliximab 5mg/kg IV x 1 dose (may repeat in 1 week if symptoms persist)• Discontinue immunotherapy
Treat symptomatically as abovePersistent symptoms >3 days then start Prednisone or IV Methylprednisolone 0.5-1mg/kg/day 2-4 week steroid taper if responds to <grade 1Persists or worsens treat as Grade 3
2017 ANNUAL MEETING
#FSHP2017Pulmonary Toxicity ManagementPulmonary Toxicity Management• Symptoms: new/worsening cough, dyspnea, or chest pain• Rule out other causes (ie. Infection, COPD exacerbation, PE)• High resolution CT scan of chest or CT angiogram
Activities of daily living (ADL) References: Weber JS, et al. J Clin Oncol 2012; 30(21):2691-7., Eigentler TK, et al. Cancer Treatment Reviews 2016; 45:7-18.
Mild (Grade 1)Asymptomatic radiographic
changes only
Moderate (Grade 2)Cough, shortness of breath but
does not interfere with ADL
Severe (Grade 3 /4)Severe shortness of breath
limiting ADL, hypoxia, oxygen needed
Delay treatment and monitor symptoms every 2-3 daysRe-image at least every 3 weeks
Hospitalization, infectious disease and pulmonary consultsInitiate empiric antibiotic therapyMethylprednisolone IV 2-4 mg/kg/dayIf symptoms improve then 4-6 week steroid taperIf symptoms persist >48 hours or relapse with steroid taperInfliximab 5mg/kg IV x 1 dose (may repeat in 1 week if symptoms persist)• Discontinue immunotherapy
Hold treatment and consider hospitalizationPrednisone po or Methylprednisolone 1mg/kg/dayInitiate empiric antibiotic therapyInfectious disease and pulmonary consults 4 week steroid taper if responds No improvement re-image and treat as Grade 3 /4
2017 ANNUAL MEETING
#FSHP2017Neurologic Toxicity ManagementNeurologic Toxicity Management• Symptoms: neuropathies, myopathy, severe refractory
constipation, aseptic meningitis, Guillain-Barre syndrome, motor neuropathy, myasthenia gravis
Activities of daily living (ADL) References: Weber JS, et al. J Clin Oncol 2012; 30(21):2691-7., Eigentler TK, et al. Cancer Treatment Reviews 2016; 45:7-18.
Mild (Grade 1)Asymptomatic or neuropathy
Moderate (Grade 2)Moderate symptoms limiting ADL
Severe (Grade 3 /4)Limiting self-care ADL or life-
threatening
Monitor and continue therapyIf worsens treat as grade 2 or grade 3 /4
Hospitalization, neurology or neuro-oncology consultsMRI brain/spine, LP with cytology, infectious work-upMethylprednisolone IV 4 mg/kg/dayIf symptoms improve then 6 week steroid taperIf symptoms persist or atypical presentation IVIG 400mg/kg/day x 5 days, if responds to therapy then 6 week steroid taper; no improvement consider plasmapheresis• Discontinue immunotherapy
Hold treatment and consider hospitalizationPrednisone po or Methylprednisolone 1mg/kg/dayConsider neurology consultImproves < grade 1 2-4 week steroid taper and may restart therapyNo improvement or persistent symptoms treat as Grade 3 /4

7/17/2017
6
2017 ANNUAL MEETING
#FSHP2017Endocrine Toxicity ManagementEndocrine Toxicity ManagementAE management
• Taper HD steroid over a minimum of 4 weeks
• Continue HRT as needed• Monitor endocrine labs as appropriate• Repeat MRI as clinically indicated
• Rule out other etiologies• Repeat endocrine labs in 1-3 weeks• Initiate frequent patient follow-up
• Initiate short course (7 days) of HD corticosteroids to reverse inflammation, dexamethasone 4 mg every 6 hours or equivalent
• Initiate HRT to manage endocrinopathy• Consult endocrinologist
Long-term follow-up
Improvement
Determine causeand severity
No
Abnormalworkup?
Yes
Signs and symptomspresent
Suspectadrenal
crisis?
No
Yes
Performance workup
1. Imaging for evidence of disease progression
2. Check endocrine labs (i.e., TSH, free T4, ACTH)
3. MRI head with pituitary cuts plus visual field testing, if appropriate
4. Obtain endocrine consult and medical monitor consult
Treat adrenal crisis
Rule out sepsis
Signs and symptoms suggestive of underlying
endocrinopathy
Hypophysitis, headache, visual field defects, fatigue, weakness, asthenia, failure to thrive, anorexia, nausea
and vomiting, lethargy, impotence, amenorrhea,
fever, coma, new-onset atrial fibrillation,
hypotension, hypoglycemia,
hyponatremia, eosinophilia
2017 ANNUAL MEETING
#FSHP2017Hepatic Toxicity ManagementHepatic Toxicity Management• Symptoms: yellowing of skin or whites of eyes, severe nausea/
vomiting, pain in right side of abdomen, drowsiness, dark urine, bleeding or bruising more than normal, feeling less hungry
• Evaluate other causes: medications, infection, progression of disease
Activities of daily living (ADL) References: Weber JS, et al. J Clin Oncol 2012; 30(21):2691-7., Eigentler TK, et al. Cancer Treatment Reviews 2016; 45:7-18.
Mild (Grade 1)AST/ALT <3 x ULN &/or Tbili <1.5 x ULN or <2 x baseline
Moderate (Grade 2)AST/ALT 3 to ≤5 x ULN &/or Tbili >1.5 to ≤3 x ULN or ≥2 x baseline
Severe (Grade 3 /4)AST/ALT >5 x ULN &/or Tbili >3
x ULN r >3 x baseline
Monitor liver function 1 to 2 times weeklyContinue therapyIf worsens treat as grade 2 or grade 3 /4
Hospitalization, CT abd/pelvis, autoimmune workup, daily liver function monitoring, hepatology and gastrointestinal endoscopy consults, consider liver biopsyMethylprednisolone IV 2-4 mg/kg/dayIf symptoms improve then prednisone 2mg/kg and 6 week steroid taperNo response in 3-5 days then mycophenolate mofetil 1gm po BID; no response in additional 3-5 days consider IVIG 400mg/kg IV daily x 5 days
Hold immunotherapy and monitor liver function every 3 daysConsider CT abd/pelvisNo improvement in 3 days consider hospitalization Prednisone 0.5mg/kg/day; twice weekly LFTReturn to grade 1 or baseline taper steroids over 4 weeksWorsen or no response treat as grade 3/ 4
2017 ANNUAL MEETING
#FSHP2017Renal Toxicity ManagementRenal Toxicity Management• Evaluate for other causes: recent IV contrast, medications,
fluid status, etc
Activities of daily living (ADL) References: Weber JS, et al. J Clin Oncol 2012; 30(21):2691-7., Eigentler TK, et al. Cancer Treatment Reviews 2016; 45:7-18.
Mild (Grade 1)SCr increase >0.3mg/dL; SCr
1.5-2 x above baseline
Moderate (Grade 2)SCr level 2-3 x above baseline
Severe (Grade 3 /4)SCr >3 x baseline or >4 mg/dL
OR dialysis indicated
Monitor SCr weekly and continue therapyIf worsens treat as grade 2 or grade 3 /4
Hospitalization, renal panel daily, nephrology consult, consider renal biopsyMethylprednisolone IV 1-2 mg/kg/dayIf symptoms improve then 6 week steroid taperIf elevations persist >5 days Infliximab 5mg/kg x 1 dose (may repeat in 1 week if elevations persist)
Hold treatment, monitor SCr every 3 days, nephrology consult, and consider renal biopsyPrednisone po 1mg/kg/dayImproves < grade 1 4 week steroid taper and may restart therapy once <10mg/day prednisone equivalentNo improvement in >7 days treat as Grade 3 /4
FSHP 2017 ANNUAL MEETING
Inpatient Management of Oncology Specialty DrugsInpatient Management of Oncology Specialty DrugsNew Agents, Opportunities, and ChallengesJennifer Swank, PharmD, BCOP