Embed Size (px)
DESCRIPTION
Influenza Immunization Update 2007-2008. Sheila L. Palevsky, MD MPH Bureau of Immunization New York City Department of Health and Mental Hygiene October 17, 2007. Impact of Influenza. - PowerPoint PPT Presentation
Citation preview

Influenza Immunization Update2007-2008
Sheila L. Palevsky, MD MPHBureau of Immunization
New York City Department of Health and Mental Hygiene
October 17, 2007


Impact of Influenza
• It is estimated that 10-20% of all adults and up to 40% of children in the U.S. are infected with influenza each year
• ~226,000 hospitalizations annually– About half among those in persons >65 years of age– Rates of influenza hospitalization in children <5 years
similar to rates in adults >65 years• >36,000 deaths during each influenza season
– More than 90% are in adults >65 years

Influenza Virus
• Orthomyxoviridae family• 3 types: A, B, C• Only influenza A and B cause epidemic human
disease• Influenza A viruses categorized into subtypes
on the basis of two surface antigens:– hemagglutinin
– neuraminidase

Influenza Virus
A/Fujian/411/2002 (H3N2)
Neuraminidase
Hemagglutinin
Type of nuclearmaterial
Virustype
Geographicorigin
Strainnumber
Year of isolation
Virus subtype
CDC

Influenza Antigenic Changes
Shift• Major change,new subtype
• Exchange of gene segments
• Occurs only in A subtypes
• May cause periodic pandemics
Drift• Minor changes, same subtype
• Genetic point mutations
• Occurs in A and B subtypes
• May cause yearly epidemics t
Influenza viruses undergo genetic changes
⇛ Occurs frequently ⇛ Occurs infrequently

The Next Antigenic Shift
The question is not if, but when
…nor do we know what kind it will be

Immunity to Influenza Antigens
• Immunity to the surface antigens, especially the hemagglutinin, reduces the likelihood of infection
• Antibody against one influenza virus type or subtype confers limited or no protection against another type or subtype of influenza
• Antibody to one antigenic type or subtype might not protect against infection with a new antigenic variant of the same type or subtype

Influenza – Clinical Features
• Respiratory transmission of virus• Contagious prior to the onset of symptoms • Incubation period 1-5 days (average 2 days)• Abrupt onset of fever, myalgia, sore throat,
nonproductive cough, headache (vomiting and diarrhea may be seen in childhood illness)
• Severity of illness depends on prior experience with antigenically related variants
All that is called the “flu” is not influenza

Influenza - Complications
• Pneumonia– Primary influenza– Secondary bacterial
• Otitis media (children)• CNS complications including Reye Syndrome• Myocarditis / myositis / rhabdomyolysis• Exacerbations of underlying medical
condition(s)• Death 0.5 – 1 per 1,000 cases (for all ages)

Important to Remember
• Influenza is spread by coughing, sneezing – through droplet spread
• Individuals are contagious for 1-4 days before the onset of symptoms and for 5-10 days after the first symptoms• Children may shed virus for >10 days after onset of
symptoms
• About 50% of infected individuals do not have any symptoms but are still contagious

Differentiating Respiratory Illnesses• Difficult to distinguish influenza from other respiratory
illnesses on the basis of signs and symptoms– Young children less likely to have typical symptoms of cough
and fever– Older adults may not have typical symptoms
• The absence of symptoms of influenza-like illness (ILI) does not effectively rule out influenza
Use laboratory tests to confirm the diagnosis

Influenza Vaccine Efficacy• Dependent upon:
– Age and immunocompetence of the vaccine recipient– The degree of similarity between virus in the vaccine and
those in circulation– Outcomes being measured
• Medically attended acute respiratory illness (MAARI)• Laboratory confirmed influenza• Prevention of influenza-associated hospitalization or death • Seroconversion to circulating vaccine strains• Seroconversionto circlutaing virus strains

Influenza Vaccine EfficacyHealthy Adults
• For healthy adults <65 years of age:– 70%-90% effective in preventing clinical illness in healthy
adults when vaccine matches circulating strains of virus– 50%-77% against laboratory-confirmed illness when vaccine
strains were antigenically dissimilar to circulating strains– Protection against healthy adults against influenza-related
hospitalization was 90%
You cannot get “the flu” from the flu shot

Influenza Vaccine EfficacyAdults With Chronic Disease
• For adults <65 years of age with chronic disease:– Vaccine generally less effective than in healthy adults– In adults 50-64 years of age, when circulating strain and
vaccine were not well matched (2003-2004), vaccine efficacy: • 60% for healthy adults vs. 48% among high-risk adults in
preventing laboratory confirmed illness • 90% for healthy adults vs. 36% among high-risk adults in
preventing hospitalization
You cannot get “the flu” from the flu shot

Influenza Vaccine EfficacyOlder Adults
• For adults >65 years, the goal is to prevent secondary complications and reduce the risk for influenza-related hospitalization and death– Among non-institutionalized persons >60 years, ~60% effective
in preventing clinical illness (lower efficacy in those >70 years)– 30%-70% effective in preventing hospitalization in non-
institutionalized seniors– In older nursing home residents:
• 20-40% effective in preventing MAARI• ~80% effective in preventing death
You cannot get “the flu” from the flu shot

Flu Vaccine
• Although the efficacy of flu vaccine in the elderly may be less than desired, it is the best protection against influenza and its complications
• The risk of hospitalization and death due to flu is high in the elderly (about 5% of deaths)
• Preventing spread of the flu is important !

Flu Vaccine in Children
• Influenza vaccine is effective in children >6 months of age• Children 6 months <9 years of age should receive 2 doses of
flu vaccine in the first season they receive vaccine – Among children <9 years of age who have never received
influenza vaccine before and who received only 1 dose of vaccine in their first year of vaccination, vaccine is less effective as compared with children who received 2 doses in their first year of being vaccinated.

Influenza Vaccine (TIV) Adverse Reactions
Local reactions* 15% - 20%
Fever, malaise* uncommon
Allergic reactions rare
Neurological reactions very rare
You cannot get “the flu” from the flu shot
*Local rxns and fever may be more common in young children

The Flu Shot (TIV)
• Contraindications - anaphylactic reaction to a previous dose or to egg protein, gelatin, or other vaccine component
• Precaution – moderate to severe illness– Vaccinate if minor illness: diarrhea, upper
respiratory tract illness (including otitis media) with or without fever or on current antimicrobial therapy
• Precaution – history of GBS within 6 weeks of receipt of a dose of flu vaccine

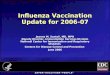
Month of Peak Influenza Activity United States, 1976-2006
13%
19%
45%
13%
3% 3%3%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Nov Dec Jan Feb Mar Apr May
CDCMMWR 2007:56(RR6)


2007-2008 Influenza Vaccine
• A/Solomon Islands/3/2006(H1N1) - like
• A/Wisconsin/67/2005 (H3N2) - like
• B/Malaysia/2506/2004 - like
Strains included in the vaccine change every year based on surveillance data
You need this year’s flu vaccine to protect against this year’s flu!!
Vaccine supply information will be available at www.cdc.gov/nip/flu

Flu Vaccine Availability and Timing of Vaccination
• Influenza vaccine is being received in offices now!
• Vaccine is usually most plentiful later in the calendar year – in November and December – prior to the peak of influenza activity
• Influenza peaks in late winter; vaccine should continue to be given well into the spring
• Keep vaccinating so long as supply is available
• If indicated, give pneumococcal (and any other indicated) vaccine(s) along with flu vaccine

Recommendations for Influenza Vaccine: 2007-2008
• All persons, including school-aged children, who want to reduce the risk of becoming ill with influenza or of transmitting influenza to others
• All children 6-59 months of age• All persons >50 years • Children and teens (6 months -18 years) on long-term
aspirin therapy• Women who will be pregnant during influenza season• Children and adults with chronic pulmonary (asthma),
cardiovascular, renal, hepatic, hematological or metabolic disorders (diabetes mellitus)
• Children and adults with immunosuppression (medication, therapy, human immunodeficiency virus)
CDC
1

Recommendations for Influenza Vaccine: 2007-2008
• Children and adults who have any condition that compromise respiratory function or handling of secretions (cognitive dysfunction, spinal cord injuries, seizures, neuromuscular disorders)
• Residents of nursing homes or other chronic care facilities who are at least 6 months of age
• Health care personnel• Healthy contacts including children and caregivers of
children <5 years and adults >50 years, with emphasis on contacts of children <6 months of age
• Healthy household contacts (including children) and caregivers of persons with medical conditions that predispose to complications from influenza
CDC
2

Influenza Vaccine Recommendations Chronic Illness*
• Pulmonary disorders (includes emphysema and asthma)• Heart disease • Metabolic disease (e.g., diabetes)• Renal dysfunction• Hemoglobinopathies• Immunosupression
– HIV/AIDS– Medications and other treatments
• Conditions that compromise respiratory function or the the handling of secretions or increase the risk of aspiration
* >6 months of age

LAIV Indications
• Healthy* persons 2 - 49 years of age– Health care workers, except those who have direct
contact with severely immunocompromised patients who require protective isolation
– Contacts of those at high risk (including contacts of infants and young children)
– Persons who wish to reduce their own risk of influenza
Persons who do not have medical conditions that increase their risk for complications of influenza
*

Administration of LAIV
• Persons at increased risk for influenza complications* may administer LAIV
• Gloves and masks are not required
*e.g., pregnant women, persons with asthma and persons 50 years of age or older

Pregnancy and Influenza
• Risk of hospitalization due to complications of the flu is 4 times higher than in non-pregnant women
• Risk of complications comparable to non-pregnant women with high-risk medical conditions
• Vaccination (with TIV) is recommended if pregnant during influenza season
• Vaccination can occur during any trimester
• Vaccinate all contacts of pregnant women

HIV Infection and Influenza
• Persons with HIV at increased risk of complications of influenza
• TIV induces protective antibody titers in many HIV infected persons
• Transient increase in HIV replication reported
• TIV will benefit many HIV-infected persons
• Vaccinate all contacts of HIV-infected persons

Influenza Vaccines 2007-2008Vaccine Dose / Presentation Age Doses Route
INACTIVATED VACCINE (TIV)
Fluzone
(sanofi pasteur)
0.25 ml pre-filled syringe* 6-35 mos 1 or 2† IM
0.5 ml pre-filled syringe* >36 mos 1 or 2† IM
0.5 ml vial* >36 mos 1 or 2† IM
5.0 ml multi-dose vial* > 6 mos 1 or 2† IM
Fluvirin (Novartis) 5.0 ml multi-dose vial >4 yrs 1 or 2† IM
Fluarix (GSK) 0.5 ml pre-filled syringe >18 yrs 1 IM
FluLuval (GSK) 5.0 ml multi-dose vial >18 yrs 1 IM
Afluria (CSL Limited) 0.5 ml pre-filled syringe >18 yrs 1 IM
5.0 ml multi-dose vial >18 yrs 1 IM
LIVE, ATTENUATED (LAIV)
FluMist (LAIV) 0.1 ml spray in each nostril 2-49 yrs 1 or 2¶ Intra-nasal
*vaccines approved for children younger than 4 years† two doses administered at least one month apart for children 6 months <9 yrs who are receiving influenza vaccine for the first time; children <9 years who received only one dose in their first season of vaccination should receive 2 doses in the next year ¶ two doses administered at least one month apart for children 2 yrs <9 yrs who are receiving influenza vaccine for the first time; children 2 yrs <9 yrs who received only one dose in their first season of vaccination should receive 2 doses in the next year

Vaccination of Health Care Personnel
• All physicians, nurses, other health care personnel in all hospital and out-patient settings, including emergency rooms, and all home care attendants should receive vaccine annually
• But - - -• in the 2004 National Health Interview Survey, only
42% of health care workers reported receiving influenza vaccine in the previous 12 months; and
• in 2005, only 33% of health care workers in NYC reported they got a flu vaccine!
What about you ???

Benefits of Influenza Vaccination of Health Care Workers
• Reduction in nosocomial influenza and influenza-related deaths
• Reduction in staff illness and illness-related absenteeism
• Reduction of direct medical costs and indirect costs from work absenteeism
MMWR. 2006;55 (RR-2)

Reasons Health Care Workers Do Not Receive Influenza Vaccine
• Concern about vaccine adverse events• Perception of a low personal risk of
influenza virus infection• Insufficient time or inconvenience• Reliance on homeopathic medications• Avoidance of all medications• Fear of needles• Mistrust of government recommendations
MMWR. 2006;55 (RR-2)

Factors Facilitating Health Care Worker Influenza Vaccination
• Desire for self-protection• Previous receipt of influenza vaccine• Desire to protect patients• Perceived effectiveness of the vaccine• Legislative and regulatory mandates
– Effective January 2007, JCAHO requires facilities to offer flu vaccine on site to staff as part of employee health programs
MMWR. 2006;55 (RR-2)

Barriers to Vaccination
• Health care workers’ misconceptions about influenza as a disease
• Lack of understanding by health care workers that influenza can be deadly for patients and contacts
“flu is not a serious disease”

Barriers to Vaccination
• Perception of a low personal risk of contracting influenza
“I don’t get sick; I don’t need it”
“absenteeism vs. presenteeism”

Barriers to Vaccination
• Failure of health care workers to explain vaccine efficacy and safety
“the flu vaccine will make me sick” “I don’t think the vaccine really works”

Barriers to Vaccination
• Health care workers are poor role models
Did you have your flu vaccine last year?

Influenza in Healthcare Workers
• Healthcare workers – Implicated in introducing influenza into and
causing outbreaks among patients in health care settings
• ICU, neonatal intensive care units, nursing homes
– Often work while ill, exposing vulnerable patients and their coworkers to influenza
– May be able to spread influenza if infected, but not symptomatic
• Can shed virus before symptoms develop• About half of all influenza infections asymptomatic

Barriers to Vaccination
• Need for annual vaccination
“I had the flu shot before, I don’t need it again”

Barriers to Vaccination
• Need to address popular myths – taking of vitamins, never get sick, etc.
“home remedies and preventives are better”
“I don’t need foreign substances in my body”

Barriers to Vaccination
• Fear of needles
LAIV is a good alternative, if eligible

Barriers to Vaccination
• There are many excuses offered to avoid vaccine – don’t give in to them
“I don’t eat eggs”
“I am taking medications”
“now isn’t convenient -I’ll get it later”

Barriers to Vaccination
• Low reimbursement

Reimbursement
• Medicare covers flu vaccine and includes an administration fee
• All Medicaid managed care plans will cover influenza vaccine for at-risk adults 19-64 years
• Commercial insurance plans should provide coverage for at-risk patients
• Commercial insurance must cover children with an indication for flu vaccine
• Influenza vaccine is available through the Vaccines for Children program for eligible children and teens

Barriers to Vaccination
• Missed opportunities
Use every encounter as an opportunity to vaccinate

Cultural and Ethnic Issues
• Understand and address different cultural beliefs of health and sickness
• Address socio-political issues such as distrust of governmental recommendations and the memory of Tuskegee

Getting Ready for Flu Season• Order sufficient vaccine • Vaccinate all office staff • Develop protocols within the health care setting
– Have patient information available (posters, flyers)
– Flag charts of high-risk patients– Use standing orders – Have special designated vaccination hours– Make every encounter an opportunity to vaccinate– Use signed declination forms if is vaccine refused
• Offer vaccine once available: continue vaccinating into the spring

Influenza Vaccine: Strategies to Increase Coverage
• Expand use of standing orders • For employees:
– Vaccination sessions• Institute vaccination days • Use traveling teams – take the vaccine to the employee• Use incentives• Monitor and report influenza vaccination levels in the facility
– Education• Education, education, education, education, education
Get documentation if vaccine was given at another location


Pneumococcal Disease
• Pneumococcal pneumonia is a common complication of influenza
• Rates of severe pneumococcal infection and death are highest in the elderly

Incidence of Invasive Pneumococcal Disease in Adults >18 yrs, US 1999-2000
Category Incidence rate (cases/100,000 persons)
Healthy 8.8
Diabetes 51.4
Chronic heart disease 93.7
Chronic lung disease 62.9
Solid cancer 300.4
HIV/AIDS 422.9
Hematological cancer 503.1
Alcohol abuse 100.4
Adapted from Kyaw, et al., JID. 2005;192:377-386.

Age-Specific Incidence, by Race, of Invasive Pneumococcal Disease in Adults (>18 yrs) with No Reported Underlying Illness
United States, 1999-2000
Kyaw, et al., JID. 2005;192:377-382.

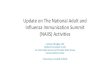
Johnstone, J. et al. Arch Intern Med 2007;167:1938-1943.
Rates of Death or Intensive Care Unit (ICU) Admission, by Pneumococcal Vaccination Status and Age

PPV23 Recommendations
• All adults >65 years of age
• Persons >2 years with– certain chronic illness– functional or anatomic asplenia– immunocompromised (disease, chemotherapy,
radiation therapy, high-dose steroids)– HIV infection– cerebrospinal fluid leaks and cochlear implants – environments or settings with increased risk

PPV 23 Vaccination: Chronic Illness*
• Diabetes or other metabolic disease• Chronic heart disease• Chronic respiratory disorders • Chronic liver disease including alcoholism• Kidney failure, ESRD, hemodialysis• Hemoglobinopathies• Immunosupression
– HIV/AIDS– cancer– medications and other treatments
* >2 years of age

PPV23 Revaccination
• Routine revaccination of immuno-competent persons is not recommended
• Revaccination recommended for persons age >2 years at highest risk of serious pneumococcal infection
• Single revaccination dose >5 years after first dose

PPV23 Candidates for Revaccination
• Persons >2 years of age with:– the highest risk of complications from IPD – persons whose antibodies decline rapidly
• functional or anatomic asplenia
• immunosuppression
• chronic renal failure
• nephrotic syndrome
• transplant recipients
• Persons vaccinated at <65 years of age

PPV23 Revaccination
• Revaccination once, 5 years after 1st dose for those aged >65 years:– if received vaccine >5 years ago, and – were aged <65 years at the time of
vaccination

PPV23 Vaccination and Revaccination
• If previous vaccination is uncertain – no available record or date of vaccine
VACCINATE
do not miss the opportunity

There are no contraindications to simultaneous administration
of any vaccines
Give influenza and pneumococcal vaccines at the same visit if both are indicated

VPD Surveillance
Report suspected cases of vaccine preventable diseases
to
212-676-2284/88 after hours: 212-POISONS

Vaccine Adverse Events
Reportsuspected
vaccine adverse events (VAERS)
800-822 7967or
www.vaers.org
or call 212-676-2284


A vaccine not given is
100% not effective

Sheila L. Palevsky, MD MPHProvider LiaisonChief, Professional Education UnitNew York City Department of Health and Mental Hygiene2 Lafayette Street – 19th floor - CN21New York, NY 10007Phone: 212-676-2264Fax: 212-442-8091Email: [email protected]