Embed Size (px)
Citation preview

Influence of weight discrimination on weight lossgoals and self-selected weight loss interventionscob_28 153..160
S. Sharma1, S. Wharton1,2, M. Forhan3 and J. L. Kuk1
What is already known about this subject
• There is a discrepancy between clinical and patient goals for weight
loss.
• Evidence suggests that some bariatric patients highly value, and are
willing to endure hardships for weight loss.
• Obesity is commonly framed as an easily reversed and individual
problem, which in turn promotes weight discrimination.
What this study adds
• Patient beliefs about weight loss are in accordance with social
understandings of obesity but not with current treatment options.
• Patients may not be willing to endure hardships for weight loss.
• Weight discrimination may relate to how patients approach weight
loss.
1Department of Kinesiology and Health
Science, York University, Toronto, Ontario,
Canada; 2The Wharton Medical Clinic,
Hamilton and Burlington, Ontario, Canada;3School of Rehabilitation Science, McMaster
University, Hamilton, Ontario, Canada
Received 14 April 2011; revised 26
October 2011; accepted 7 November 2011
Address for correspondence: Dr JL Kuk,
School of Kinesiology and Health Science,
York University, 2002 Sherman Health Science
Centre, 4700 Keele Street, Toronto, Ontario
M3J 1P3, Canada. E-mail: [email protected]
SummaryBariatric patients report weight loss goals, which are three times higher thanweight loss recommended by clinicians. It is unclear which weight loss interven-tions patients feel are necessary to reach these goals or whether responses asso-ciate with perceptions of weight discrimination. One hundred fifteen patients(BMI = 40.0 � 6.9 kg m-2, age = 47.2 � 12.2 years, 85% female, 77% reportingweight discrimination) were surveyed from weight management clinics. Partici-pants reported ideal weight losses of 37.6 � 16.7 kg (33% of initial weight), andthe majority felt weight loss could be achieved through lifestyle changes such asimproved physical activity (80%) or diet (52%), with fewer reporting pharma-cotherapy (8%), surgery (12%) or genetic modification (7%) as necessary for goalattainment. Participants selecting lifestyle changes or pharmacotherapy for weightloss reported ideal weight loss goals that would generally be achievable throughsurgical means (32% and 33%, respectively), and participants selecting surgicalintervention reported ideal goals at the upper end of what is generally achievablewith this intervention (38%). All participants selecting surgery or genetic modi-fications reported experiencing weight discrimination. These results indicate adisparity between weight loss goals and selected interventions, and suggest thatweight discrimination is associated with the selection of potentially riskier weightloss interventions.
Keywords: Bariatric, motivation, stigma, weight management clinic.
Introduction
It is well documented that obesity is a risk factor forvarious comorbidities and that weight reduction is of vitalimportance for improving health risk (1,2). During the1980s, treatment focused on weight reduction to ‘normal’
values as defined by height-weight charts (2,3). In the1990s, a change to clinical guidelines occurred whereinsuccessful weight loss became defined by some as moremodest reductions of 5–10% of initial body weight (2,3) asa consequence of both the observed difficulty in main-taining larger reductions in weight (4) and the evident
clinical obesity doi: 10.1111/j.1758-8111.2011.00028.x
153© 2011 The AuthorsClinical Obesity © 2011 International Association for the Study of Obesity. clinical obesity 1, 153–160

improvements in metabolic and haemodynamic function-ing with smaller reductions (2,5). It is recognized that thereis often a discrepancy between patient and clinician goalsfor weight loss, and individuals with obesity often haveideal weight loss goals, which are three times higher thanclinical guidelines for weight loss (3,6–9). The methodspatients believe are necessary for achieving such weight lossremain unclear. It has further been documented that bari-atric surgery candidates are willing to risk dying to achievemoderate to high amounts of weight loss (10). Similarly,patients who have undergone surgery report a willingnessto endure hardships such as deafness, blindness and dys-lexia in lieu of returning to their formerly obese state (11).It remains to be seen whether similar results are foundamong patients seeking non-surgical weight loss.
Current social representations of obesity commonlypresent weight as easily modifiable through lifestylechanges (12–14), thus framing excess weight as an indi-vidual problem and responsibility, while neglecting theinfluence of environmental and socio-cultural factors. As aresult, individuals with obesity are stigmatized as lazy, glut-tonous and unmotivated, and are prone to weight-baseddiscrimination (12–15). Further, individuals with over-weight or obesity may internalize these negative beliefsabout obesity and attribute their weight status to a char-acter flaw rather than external causes (16). Weight stigma-tization and discrimination may contribute to individuals’tendency to select high and unrealistic weight loss goalsand make large sacrifices in order to attain or maintain anormal weight, yet patient goals for clinical treatment havenot been explored in the context of the social discoursesurrounding obesity. Thus, the purpose of this study is totest the hypotheses that (i) the majority of patients believethat obesity is attributable to and can be ameliorated withlifestyle changes and (ii) patients who have experiencedweight discrimination desire greater weight loss.
Materials and methods
Participants
Participants were recruited from patients initiating weightmanagement treatment at the Wharton Medical Clinic(WMC) in Hamilton and Burlington, Ontario. The WMCis a referral-based specialist clinic, which utilizes an inter-disciplinary approach to bariatric care including a teamof medical doctors, medical technicians and exercise anddiet specialists. All patients are referred by family or spe-cialist physicians. The clinic operates within the OntarioHealth Insurance Plan and all services are provided at nocharge to the patient, including physician visits, nutritionalcounselling, exercise prescription and assessment, diagnos-tic testing, standard and indicated blood work and educa-tional group sessions.
Data collection and assessment
All new patients to the WMC were invited to participatein this study and were given consent forms and surveysduring their initial visit. Any completed surveys were col-lected after the initial visit. Written and informed consentfor participation in this research was obtained, andthe methods used were approved by the York UniversityEthics Review Board. Participants were given a paperquestionnaire at the beginning of their first visit thatincluded a Goals and Relative Weights Questionnaire (3),which asked them to report levels of weight losses theyconsidered to be ideal, realistic, and the minimal weightloss that they would be satisfied with. Participants alsoreported the time they anticipated it would take to achievethese magnitudes of weight losses (i.e. weeks to goalweight loss) and their perceived value of weight status(i.e. what they were willing to sacrifice to lose weightand under what situations they were willing to remaintheir current weight, as previously assessed by Randand Macgregor (11)). Attributions for weight gain werereported (i.e. over-eating, high-fat diet, junk food,not physically active, genetics, environment, lack ofwill-power, medical condition); and re-coded as lifestyle,medical conditions, environment and genetic categories.Participants reported what they felt was necessary toachieve weight loss; and these self-selected weight lossinterventions were classified into severity classes. Lifestylechanges (i.e. eat less, eat better, more physical activity,more will-power) were classified as intervention severityclass I; pharmacotherapy and meal replacement (i.e.weight loss drugs, weight loss supplements, meal replace-ment) were classified as class II; surgical intervention wasclassified as class III; and genetic modification (i.e. some-thing that is currently not possible) was classified as classIV. These variables were classified in this manner as theyare factors that have been found to contribute to obesity(17), or are clinically utilized weight loss interventions (1).Participants reported any experiences of weight discrimi-nation (‘Have you ever experienced weight discrimination,or had a negative experience because of your weight?’).Participants were instructed to specify the phase of life thealleged incident(s) occurred (i.e. childhood, adolescence,adulthood), the type (i.e. verbal, physical, physical barrier)and setting of experiences (i.e. home, work, medical facil-ity, public place, mode of transportation, school, other),as well as the relationship to (i.e. peer/friend, boyfriend/girlfriend, parent, child, spouse, sibling, other family,stranger, physician, nurse, other healthcare professional,boss/supervisor, teacher/professor, other), and the age ofthe perpetrator (child, adolescent, adult, N/A). Partici-pants chose up to three attributions and interventions forweight loss, and were given the opportunity to select asmany applicable responses for the weight discrimination
154 Weight discrimination and weight loss S. Sharma et al. clinical obesity
© 2011 The AuthorsClinical Obesity © 2011 International Association for the Study of Obesity. clinical obesity 1, 153–160

questions. Body mass index (BMI), age, sex and self-reported disappointed weight (i.e. the absolute weight theparticipant perceived they would be disappointed withafter treatment) were retrieved from patient electroniccharts. Disappointed weight loss was calculated by sub-tracting disappointed weight from the initial weight.
Statistical analyses
Continuous variables are presented as means � standarddeviation and categorical variables are presented as preva-lences (%). Linear regression was used to determine theassociation between ideal weight loss and weight discrimi-nation adjusting for BMI. Analysis of variance was used toexamine differences in age and BMI between selected attri-butions and intervention severity class. Independent mea-sures t-test was used to determine differences in BMI andideal weight loss by weight discrimination for each inter-vention severity. The association between ideal weight lossand intervention severity was examined using general linearmodelling with adjustment for BMI. Because of a smallsample size, pharmacotherapy, surgery and genetic modifi-cation were collapsed into a ‘non-lifestyle’ category andlogistic regression was used to examine the likelihoodof selecting lifestyle interventions in comparison to non-lifestyle interventions after adjustment for BMI.
All analyses were conducted using SAS 9.2 (SAS Insti-tute, Cary, NC, USA).
Results
Sample characteristics
The baseline characteristics for 115 participants arepresented in Table 1. The majority of participants wereWhite females (85%) with a mean weight of 109.0 �
21.4 kg and a BMI of 40.0 � 6.9 kg m-2 (class III obesity).Participants reporting weight discrimination (n = 89, 77%)were younger, and had a higher weight than those reporting
no discrimination (P < 0.05). Participant goal weightsranged from 20% (disappointed weight loss) to 33% (idealweight loss). Ideal weight loss was associated with weightdiscrimination after adjustment for BMI (weight discrimi-nation: b = 6.4 � 2.06, P = 0.002; BMI: b = 2.0 � 0.13,P < 0.0001).
When asked for the reason for seeking weight loss, themajority of participants reported health (88%), with fewerreporting mobility (51%) or aesthetics (39%). However,only 29% agreed they would be satisfied with a 5% weightreduction if their health could be improved, and only 24%agreed to a 5% weight reduction if their health could benormalized. On average, participants believed they neededto lose 32 kg � 16.5 kg) to improve health (range = 0.45–90.9 kg).
Perceived value of weight
To assess the perceived value of weight status, participantswere asked what sacrifices they were willing to maketo have a normal weight, and under what situationsthey would be willing to remain at their current weight(Table 2). Participants reported being willing to exercise1–2 h d-1 (72%), or never eat their favourite foods (33%)to attain normal weight, but none reported a willingnessto have heart disease, be blind or paraplegic or go to jail.Some reported a willingness to remain at their currentweight if they could be disease free (34%), be a millionaire(19%) or live forever (12%).
Perceptions of weight discrimination
Seventy-seven percent of participants reported previousweight discrimination (Table 1). Experiences of weight dis-crimination are presented in Table 3. The most commonexperiences occurred during adulthood (59%), were verbalin nature (59%), and were committed by a stranger (31%)or peer/friend (31%) in a public place (44%). Ten percentreported a negative experience from a physician.
Table 1 Characteristics of 115 patientsinitiating treatment
Characteristic Participants reportingweight discrimination
Participants reporting noweight discrimination
n† 89 26Age (years) 44.6 � 11.3* 56.4 � 11.2Weight (kg) 111.9 � 22.0* 100.8 � 17.2Body mass index (kg m-2) 40.3 � 7.0 38.5 � 6.6Female (%) 85.4 84.6White (%) 97.0 90.5Black (%) 3.0 0South Asian (%) 0 4.8Southeast Asian (%) 0 4.8
*P < 0.005.†n = 87 for ethnicity variable.
clinical obesity Weight discrimination and weight loss S. Sharma et al. 155
© 2011 The AuthorsClinical Obesity © 2011 International Association for the Study of Obesity. clinical obesity 1, 153–160

Attributions to weight gain and self-selected weightloss interventions
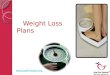
A lack of physical activity (61%), over-eating (58%) anda lack of will-power (50%) were the most commonlyreported attributions for weight gain as compared to envi-ronment (12%) or stress (6%; Table 4). Accordingly, themajority of participants felt changes to physical activity(80%), eating (54%) and will-power (52%) were requiredto meet goal weight loss, with fewer reporting pharmaco-therapy (8%) or surgery (12%) as a requirement for goalattainment (Table 4). Average patient age (F(3,5) = 1.36,h2 = 0.04, P = 0.26) or BMI (F(3,5) = 1.12, h2 = 0.03,P = 0.34) did not differ among attribution classes; and age(F(3,7) = 1.82, h2 = 0.05, P = 0.15) or BMI (F(3,7) = 1.76,h2 = 0.05, P = 0.16) did not differ among interventionseverity classes. However, a significant trend was observedbetween average patient BMI and intervention severityclass wherein those who chose more severe interventionstended to have a higher BMI (Ptrend � 0.05). For a givenintervention severity class, mean BMI did not differ amongthose reporting weight discrimination in comparison tothose reporting none (Fig. 1A). Participants selecting lif-estyle intervention for weight loss reported ideal weightloss goals of 32%, 33% with pharmacotherapy, 38% withsurgery and 42% via genetic modification. Ideal weightloss was significantly higher in those reporting previousweight discrimination and selecting lifestyle interventionsthan those reporting no weight discrimination (33% vs.28%, respectively, t(74) = 2.23, P = 0.03), with no differ-ences among those who selected pharmacotherapy (t(14) =-1.07, P = 0.30). This significant difference remained withadjustment for BMI (33% vs. 29%, F(1,21) = 27.92,h2 = 0.44, P = 0.001, Fig. 1B) All patients selecting surgery
Table 2 Participant-reported sacrifices to attain a normal weight andtheir willingness to remain at the same weight
Sacrifice to attain a normal weight n agreeing (%)
Exercise 1–2 h daily 83 (72.2)No favourite foods 38 (33.0)20 years less to live 5 (4.3)Only 5 more years to live 3 (2.6)Heart disease 1 (0.9)Paraplegia 0 (0.0)Blindness 0 (0.0)Jail 0 (0.0)
Willing to remain at the same weight if
Disease free 39 (33.9)Millionaire 22 (19.1)Live forever 14 (12.0)Famous 6 (5.2)
Tab
le3
Par
ticip
ant
exp
erie
nces
ofw
eig
htd
iscr
imin
atio
n
Rel
atio
nto
per
pet
rato
rn
(%)*
Whe
nit
hap
pen
edn
(%)*
Typ
eof
exp
erie
nce
n(%
)*A
ge
ofp
erp
etra
tor
n(%
)*S
ettin
gn
(%)*
Pee
r/fr
iend
36(3
1.3)
Ad
ulth
ood
68(5
9.1)
Verb
al68
(59.
1)A
dul
t67
(58.
3)P
ublic
pla
ce50
(43.
5)S
tran
ger
36(3
1.3)
Ad
oles
cenc
e38
(33.
0)P
hysi
cal
23(2
0.0)
Ad
oles
cent
40(3
4.8)
Hom
e40
(34.
8)P
aren
t24
(21.
9)C
hild
hood
33(2
9.0)
Phy
sica
lbar
rier
11(1
0.0)
Chi
ld32
(27.
8)S
choo
l31
(27.
0)S
iblin
g17
(15.
0)O
ther
2(1
.7)
Wor
k18
(15.
7)B
oyfr
iend
/girl
frie
nd13
(11.
3)M
edic
alfa
cilit
y7
(6.1
)P
hysi
cian
11(9
.6)
Mod
eof
tran
spor
tatio
n6
(5.2
)S
pou
se10
(9.0
)O
ther
3(2
.6)
Oth
erfa
mily
10(9
.0)
Chi
ld9
(7.8
)B
oss/
sup
ervi
sor
9(7
.8)
Teac
her/
pro
fess
or8
(7.0
)N
urse
1(0
.9)
*Pre
vale
nces
will
not
sum
to10
0%as
pat
ient
sse
lect
edas
man
yre
spon
ses
asap
plic
able
.
156 Weight discrimination and weight loss S. Sharma et al. clinical obesity
© 2011 The AuthorsClinical Obesity © 2011 International Association for the Study of Obesity. clinical obesity 1, 153–160

or genetic modification as a means to attain ideal weightloss reported experiencing weight discrimination. Theselection of lifestyle interventions vs. non-lifestyle interven-tions was not associated with weight discrimination with orwithout adjustment for BMI (P > 0.05).
Discussion
This study highlights the intersection between clinical andsocial realms of obesity. There is a discrepancy betweenpatient and clinician goals for weight loss and the majorityof patients believe that large amounts of weight loss maybe attained through lifestyle changes alone. Participantsreporting weight discrimination report higher ideal weightloss goals than those reporting none after adjustment forBMI, and tend to select riskier weight loss interventions.These findings may be attributable to obesity discourses,which suggest excess weight is easily modifiable and con-tribute to weight stigma and bias.
Goal weight loss
Participants reported ideal weight loss of 33%, a goalconsistently reported among patients with obesity seekingweight loss (3,8,9,18). The association between idealweight loss and BMI indicates that heavier patients seek tolose more weight; a finding also corroborated by others
(6,7,9). In accordance with our hypothesis, weight dis-crimination status was associated with the amount ofweight patients ideally wanted to lose, with those report-ing weight discrimination wanting to lose 6.4 kg morethan an individual of the same BMI reporting no weightdiscrimination.
A 33% weight loss for the average patient with a BMI of40 kg m-2 (class III obesity) would reduce their BMI to26.8 kg m-2 (overweight). At the rate of 0.5–1.0 kg weightloss/week, this weight reduction would be achievable in thegoal time frames reported by participants (54.3 weeks forideal weight loss) if weight loss were to continue uninter-rupted. Although modifications in diet, exercise and behav-iour are typically effective in inducing a 7–10% weight lossin 16–24 weeks (i.e. 4–6 months) (19,20), such interven-tions are often unsuccessful after this time period becauseof poor adherence to the intervention and/or physiologicalresistance maintaining the initial weight loss (21). Pharma-cotherapy interventions induce a 10–15% weight loss after1 year (22), but are associated with treatment barriers suchas poor compliance (2,12). Surgical intervention is associ-ated with a 30–40% weight loss but is not readily available(23,24). Given the limitations of current weight loss inter-ventions, in addition to the common belief that lifestylechanges are sufficient for ideal weight loss attainment, thereported goal weight losses are likely unachievable for mostparticipants.
Table 4 Participant-reported attributions forweight gain and self-selected weight lossinterventions for weight loss
Attributions forweight gain (%)
n (%)* Self-selected weight lossintervention (%)
n (%)*
Lack of physical activity 70 (60.9) More physical activity 92 (80.0)Over-eat 67 (58.3) Eat better 75 (65.2)Lack of will-power 57 (50.0) Eat less 62 (53.9)Genetics 43 (37.4) More will-power 60 (52.2)Medical condition 40 (35.0) Weight loss supplements 15 (13.0)Junk food 36 (31.3) Surgery 14 (12.2)Fat diet 24 (20.9) Weight loss drugs 9 (7.8)Environment 14 (12.1) Genetic modification 8 (7.0)Stress 7 (6.1) Meal replacement 8 (7.0)Other 5 (4.3) Other 6 (5.2)
*Prevalences will not sum to 100% as participants selected up to three responses.
Figure 1 Mean body mass index (A) andpercent ideal weight loss goals (B) for agiven type of weight loss interventionstratified by weight discrimination. Panel B isadjusted for BMI. Black bars: reported priorexperience of weight discrimination; greybars: no reported experience of weightdiscrimination (frequency = 0 for severity IIIand IV). *Significantly different from thosereporting no weight discrimination for a givenseverity class; P < 0.05.
clinical obesity Weight discrimination and weight loss S. Sharma et al. 157
© 2011 The AuthorsClinical Obesity © 2011 International Association for the Study of Obesity. clinical obesity 1, 153–160

Perceived value of weight status
In contrast with studies suggesting bariatric surgery,patients are willing to accept an impairment such as dys-lexia or blindness (11), or risk dying to attain a goalweight (10), the majority of WMC participants wereunwilling to give up years of their life, their health ortheir mobility to have a normal weight. These findingsare not entirely surprising given that most participantsreported health as a motivation for weight loss. Thepresent study also presented participants with the hypo-thetical option of remaining their current weight inexchange for a positive outcome such as becoming a mil-lionaire or living forever, and less than 34% of the sampleaccepted these scenarios. This suggests that individualsseeking non-surgical weight loss are neither willing toendure an extremely negative outcome to be normalweight nor willing to accept an extremely positive expe-rience to remain at their weight. This is perhaps attribut-able to representations of weight loss as the productof self-control over diet and exercise, which imply thatweight loss should be relatively easy (15). However, it isimportant to note that although such hypothetical sce-narios provide insight into the perceived value of weightstatus, they may also bias participant responses by pre-senting extreme circumstances and are inherently limitedby their suppositional nature.
Weight loss for health
Health has previously been documented as a primary moti-vator for weight loss among bariatric surgery patients(10,25–27). The majority of participants in the presentstudy also reported health as the major reason for seekingweight loss, yet very few were willing to accept a smallerweight loss for health benefits. This discrepancy may be afunction of social desirability in that participants reporthealth as a reason for weight loss to appease the healthcareteam, yet truly desire weight loss for the resulting improve-ment in aesthetics. This is supported by the finding thatonly a third of participants reported they would be willingto remain their current weight if they could be ‘diseasefree’. Alternatively, participants’ unwillingness to accepta smaller weight loss may be attributable to differencesin how people perceive health. For example, exercise isoften equated with fitness and health such that exerciseis thought to improve fitness and effectively result in goodhealth (which is identified by a particular body size andshape) (14). Given this conflation between physical appear-ance and health status, it is plausible that participantsdisagree with the notion of heath improvements withsmaller weight reductions because this concept disrupts thelogic of this exercise-fitness-health triplex and mobility andaesthetics may be included in what participants perceive to
be healthy. This is supported by the finding that the major-ity of participants (80%) felt exercise was necessary forweight loss.
Weight discrimination
Consistent with previous reports, 77% of the samplereported a previous negative experience of weight dis-crimination with experiences ranging among personal,employment, educational and medical domains of life(28). The majority of reported experiences in the presentstudy were verbal and personal in nature (i.e. committedby a peer/friend, partner, parent or other family member).This is of concern provided that verbal stigmatizingexperiences, which are perpetrated by peers/friends andparents, have been reported as the worst stigmatizingoccurrences experienced by victims (29). Such personalattacks may represent an attempt to encourage weightloss, or may alternatively indicate the societal acceptanceof weight discrimination, even within close relationships(29).
Weight gain attributions and self-selected weightloss interventions
The majority of participants attributed their weight statusto their lifestyle (i.e. inactivity, over-eating and lack ofwill-power) and correspondingly, felt changes to lifestylewould correct their weight problem, which may representan internalization of stereotypes of obesity (16). Although37% of participants identified genetics as a reason forweight gain, only 7% felt genetic modification was requiredto attain weight loss goals. These findings may be explainedby representations of obesity as easily modified with dietand exercise (13,14), which suggests that weight problemscan be overcome through such modifications. Participantsreported higher weight loss goals than is typically observedfor those weight loss interventions, thus indicating adisparity between participant goals for weight loss andlikely intervention outcome. Among those selecting lifestyleinterventions, participants reporting weight discriminationreported greater weight loss goals than those who reportedno weight discrimination independent of BMI; and allthe participants who felt surgery or genetic modificationwas necessary for weight loss success reported weight dis-crimination. Thus, participants reporting weight discrimi-nation desired greater weight reduction than those whoreported no weight discrimination and selected riskiersurgical interventions (30–32) that are also more effectiveweight loss interventions. Although causality cannot beinferred, it is plausible that individuals may both desiregreater weight loss and select bariatric surgery as an inter-vention as a consequence of negative weight-based dis-crimination and social pressures to be thin.
158 Weight discrimination and weight loss S. Sharma et al. clinical obesity
© 2011 The AuthorsClinical Obesity © 2011 International Association for the Study of Obesity. clinical obesity 1, 153–160

Limitations
This study has several limitations. Few participantsreported no previous experience of weight discrimination,and although this suggests that perceptions of weight dis-crimination are highly prevalent within this sample, thismay have limited our ability to make conclusions about itsassociations. Additionally, the use of a broad measure ofweight discrimination (i.e. any negative event) may havecontributed to the inclusion of non-discriminatory events.The ethnic and sex homogeneity within the sample, andthe lack of data on economic status is also a limitationgiven that sex, ethnicity and socioeconomic status mayinfluence how individuals perceive and cope with weightdiscrimination (33). Similarly, the patient base is mainlyWhite and female and the findings may be subject torecruitment bias as those who elected to participate inthis study may differ from those who did not. Because ofthe cross-sectional nature of this study, it is not possibleto determine whether weight discrimination mediatesthe selection of treatments among these participants.Additionally, although we were interested in assessingwhat participants felt that they needed to achieve theirweight loss goals, we did not assess their intentions. Wetherefore do not know whether participants will attemptweight loss interventions selected, or how many patientsare waiting for bariatric surgery.
Conclusion
In conclusion, WMC patients expect greater weightreduction than typically observed for the chosen interven-tion and are generally unwilling to life-altering sacrificesto attain a normal weight. Participants reporting weightdiscrimination desired greater weight loss via lifestylemodification after adjustment for BMI, and all partici-pants who felt surgery or genetic modification was nec-essary for weight loss success reported experiencingweight discrimination. Patients and the public at largemay need to be educated on realistic weight loss expec-tations for the various interventions in order to betterbalance the risk associated with each intervention againstthe risks associated with obesity, so that patients canmake an informed and rational decision regarding theirweight management.
Conflict of Interest Statement
S. Sharma held a 6-month internship at Wharton MedicalClinic and S. Wharton is the medical director at WhartonMedical Clinic. J.L. Kuk holds a research grant from theWharton Medical Clinic. M.A. Forhan has no conflicts todisclose.
Author contributions
This study was conceived by J.L. Kuk. S. Sharma and J.L.Kuk contributed to the collection, analysis and interpreta-tion of data. All authors contributed to the preparationof the manuscript and gave final approval of the publishedversion.
Acknowledgements
The authors of this paper would like to acknowledge thestaff and patients at WMC for participating in and accom-modating this study. This research was funded by an indus-try grant by the MITACS-Accelerate internship program inpartnership with the Wharton Medical Clinic.
References
1. Lau DC, Douketis JD, Morrison KM et al. 2006 Canadianclinical practice guidelines on the management and prevention ofobesity in adults and children (summary). CMAJ 2007; 176:S1–13.2. Expert Panel on the Identification, Evaluation, and Treatmentof Overweight and Obesity in Adults. Executive summary of theclinical guidelines on the identification, evaluation, and treatmentof overweight and obesity in adults. Arch Intern Med 1998; 158:1855–1867.3. Foster GD, Wadden TA, Vogt RA, Brewer G. What is a reason-able weight loss? Patients’ expectations and evaluations of obesitytreatment outcomes. J Consult Clin Psychol 1997; 65: 79–85.4. Wadden TA. Treatment of obesity by moderate and severecaloric restriction. Results of clinical research trials. Ann InternMed 1993; 119(7 Pt 2): 688–693.5. NHLBI. Obesity Guidelines. 2009. [WWW document]. URLhttp://www.nhlbi.nih.gov/guidelines/obesity/ (accessed October2009).6. Foster GD, Wadden TA, Phelan S, Sarwer DB, Sanderson RS.Obese patients’ perceptions of treatment outcomes and the factorsthat influence them. Arch Intern Med 2001; 161: 2133–2139.7. Dalle Grave R, Calugi S, Magri F et al. Weight loss expectationsin obese patients seeking treatment at medical centers. Obes Res2004; 12: 2005–2012.8. Dutton GR, Perri MG, Dancer-Brown M, Goble M,Van Vessem N. Weight loss goals of patients in a health mainte-nance organization. Eat Behav 2010; 11: 74–78.9. Fabricatore AN, Wadden TA, Womble LG et al. The role ofpatients’ expectations and goals in the behavioral and pharmaco-logical treatment of obesity. Int J Obes (Lond) 2007; 31: 1739–1745.10. Wee CC, Jones DB, Davis RB, Bourland AC, Hamel MB.Understanding patients’ value of weight loss and expectations forbariatric surgery. Obes Surg 2006; 16: 496–500.11. Rand CS, Macgregor AM. Successful weight loss followingobesity surgery and the perceived liability of morbid obesity. Int JObes 1991; 15: 577–579.12. Crawford R. Healthism and the medicalization of everydaylife. Int J Health Serv 1980; 10: 365–388.13. Rich E, Evans J. ‘Fat ethics’ – the obesity discourse and bodypolitics. Soc Theor Health 2005; 3: 341–358.14. Gard M. Managing uncertainty: obesity discourses andphysical education in a risk society. Stud Philos Educ 2001; 20:535–549.
clinical obesity Weight discrimination and weight loss S. Sharma et al. 159
© 2011 The AuthorsClinical Obesity © 2011 International Association for the Study of Obesity. clinical obesity 1, 153–160

15. Puhl RM, Heuer CA. The stigma of obesity: a review andupdate. Obesity (Silver Spring) 2009; 17: 941–964.16. Puhl RM, Moss-Racusin CA, Schwartz MB. Internalization ofweight bias: implications for binge eating and emotional well-being. Obesity (Silver Spring) 2007; 15: 19–23.17. Sharma AM, Padwal R. Obesity is a sign – over-eating is asymptom: an aetiological framework for the assessment and man-agement of obesity. Obes Rev 2010; 11: 362–370.18. Dalle Grave R, Calugi S, Molinari E et al. Weight loss expec-tations in obese patients and treatment attrition: an observationalmulticenter study. Obes Res 2005; 13: 1961–1969.19. Fabricatore AN, Wadden TA. Obesity. Annu Rev Clin Psychol2006; 2: 357–377.20. Shaw K, Gennat H, O’Rourke P, Del Mar C. Exercise foroverweight or obesity. Cochrane Database Syst Rev 2006; (4):CD003817.21. Miller WC. How effective are traditional dietary and exerciseinterventions for weight loss? Med Sci Sports Exerc 1999; 31:1129–1134.22. Padwal R, Li SK, Lau DC. Long-term pharmacotherapy foroverweight and obesity: a systematic review and meta-analysis ofrandomized controlled trials. Int J Obes Relat Metab Disord 2003;27: 1437–1446.23. Christou NV, Efthimiou E. Bariatric surgery waiting times inCanada. Can J Surg 2009; 52: 229–234.24. Colquitt J, Clegg A, Loveman E, Royle P, Sidhu MK. Surgeryfor morbid obesity. Cochrane Database Syst Rev 2005; (4):CD003641.
25. Munoz DJ, Lal M, Chen EY et al. Why patients seek bariatricsurgery: a qualitative and quantitative analysis of patient motiva-tion. Obes Surg 2007; 17: 1487–1491.26. Karmali S, Kadikoy H, Brandt ML, Sherman V. What is mygoal? Expected weight loss and comorbidity outcomes amongbariatric surgery patients. Obes Surg 2011; 21: 595–603.27. Libeton M, Dixon JB, Laurie C, O’Brien PE. Patient motiva-tion for bariatric surgery: characteristics and impact on outcomes.Obes Surg 2004; 14: 392–398.28. Puhl R, Brownell KD. Bias, discrimination, and obesity. ObesRes 2001; 9: 788–805.29. Puhl RM, Moss-Racusin CA, Schwartz MB, Brownell KD.Weight stigmatization and bias reduction: perspectives of over-weight and obese adults. Health Educ Res 2008; 23: 347–358.30. Tolonen P, Victorzon M, Makela J. 11-Year experiencewith laparoscopic adjustable gastric banding for morbid obesity –what happened to the first 123 patients? Obes Surg 2008; 18:251–255.31. Lanthaler M, Aigner F, Kinzl J et al. Long-term results andcomplications following adjustable gastric banding. Obes Surg2010; 20: 1078–1085.32. Poirier P, Alpert MA, Fleisher LA et al. Cardiovascular evalu-ation and management of severely obese patients undergoingsurgery: a science advisory from the American Heart Association.Circulation 2009; 120: 86–95.33. Carr D, Jaffe KJ, Friedman MA. Perceived interpersonal mis-treatment among obese Americans: do race, class, and gendermatter? Obesity (Silver Spring) 2008; 16(Suppl. 2): S60–S68.
160 Weight discrimination and weight loss S. Sharma et al. clinical obesity
© 2011 The AuthorsClinical Obesity © 2011 International Association for the Study of Obesity. clinical obesity 1, 153–160