Embed Size (px)
DESCRIPTION
ppi
Citation preview

NosocomialNosocomial Urinary InfectionsUrinary InfectionsNosocomialNosocomial Urinary InfectionsUrinary Infections
Hani Hani JokhdarJokhdar, MD., MD.Consultant of Communicable Disease ControlConsultant of Communicable Disease ControlConsultant of Communicable Disease ControlConsultant of Communicable Disease Control

Case oneCase one
An An 60 60 y.oy.o. female admitted to the ICU. female admitted to the ICU2727//99//0606 k f CVA d tik f CVA d tion on 2727//99//0606; known case of CVA, dementia,; known case of CVA, dementia,
bedsore and hypothyroidism.bedsore and hypothyroidism.A i d th f ll iA i d th f ll iAcquired the following:Acquired the following:
44//1010//0606; UTI ; UTI Pseudomonas a. ESBL Pseudomonas a. ESBL t t d itht t d ith MMtreated with treated with MeropenemMeropenem1010//1010//0505; Extension of infection to ; Extension of infection to
dd b t ib t i ((P dP dsecondary secondary baceteremiabaceteremia ((Pseudomonas Pseudomonas a.) a.) treated with treated with MeropenemMeropenem and and GentamicinGentamicinGentamicinGentamicin

1818//1111//0606; Bedsore get heavily colonized ; Bedsore get heavily colonized ((E. coli E. coli andand Proteus M.Proteus M.))(( ))2626//1111//0606; UTI (; UTI (E. coliE. coli) treated with ) treated with GentamicinGentamicinGentamicinGentamicin2626//1010//0606; vaginal infection (; vaginal infection (E. coliE. coli))

Th t t l t f thTh t t l t f thThe total money spent for the The total money spent for the treatment of the previous HAtreatment of the previous HAtreatment of the previous HA treatment of the previous HA
UTI and its consequencesUTI and its consequenceswas > was > 5050,,000 000 SRSR

Case twoCase two
54 54 y.oy.o male, admitted on male, admitted on 1717//1212//06 06 yy ,, // //Acute MI; Known IHD & cirrhotic liverAcute MI; Known IHD & cirrhotic liverOccupied ICU bed until death on MarchOccupied ICU bed until death on MarchOccupied ICU bed until death on March Occupied ICU bed until death on March 2020thth. . A i d th f ll iA i d th f ll i UTIUTI ith thith thAcquired the following Acquired the following UTIsUTIs with the with the following organisms throughout following organisms throughout h it li tih it li tihospitalizationhospitalization
ESBL pseudomonas a. ESBL pseudomonas a. treated with treated with 3 3 antibiotic for antibiotic for 3 3 weeks. weeks.

EnterobacterEnterobacter alsoalso ESBLESBL that was treatedthat was treatedEnterobacterEnterobacter alsoalso ESBL ESBL that was treated that was treated with with GentamicinGentamicinThe patient has also colonized hisThe patient has also colonized hisThe patient has also colonized his The patient has also colonized his sputum with MDR sputum with MDR AcinetobacterAcinetobacter spp. spp. Which was demonstrated in urine twoWhich was demonstrated in urine twoWhich was demonstrated in urine two Which was demonstrated in urine two days prior to death.days prior to death.

IntroductionIntroduction
Th th i f ti i d i thTh th i f ti i d i thThey are the infections acquired in the They are the infections acquired in the hospital after admissionhospital after admission
NIPatient’s own flora
Other patient Environment
Medical equipmentNI
Staff member

The alertThe alert
With the best hospital care; medical statistics p ;demonstrates that at least 10% of total hospital admission end up with nosocomial infectionsp
Nearly 100,000 people die of NI in the USANearly 100,000 people die of NI in the USAeach year
Adding an extra 4 days of hospital stay costing an average of $2000 per patientg p p

It is increasing: why?It is increasing: why?
The widespread use of antimicrobial in thephospitals together with the easy access in pharmacies led to emergence of resistant strainsp g
Failure to follow appropriate infection controli h it l ttimeasures in hospital settings
Increase in the number of theimmunocompromised in hospitals

More people undergoing extensive invasiveMore people undergoing extensive, invasive surgical procedure
Increase demand for blood transfusion
Increasing renovation in the aged hospital b ildibuilding

Main Types of InfectionsMain Types of Infections
44%
17% UTISSI44%
18%
SSIBSIP
11%10%
18% PneumoOthers
11%

HA HA -- UTIUTI
It is the most common type (± 40%) of NIinvolving both LTC and acute hospital settings
Instrumentation is almost always associated ith llwith all cases
Being the most common it is the most gpreventable
Adults and children are equally affected

HistoryHistory
Frederick Foley in 1927First to control bleeding post-operativelyg p p yThen to drain the obstructed tractDrain incontinent patientM iMeasure urinary output
1950s and the close sterile drainage system1970 k th ti ill1970s knows the routine surveillance

EpidemiologyEpidemiology
Catheter useCatheter useIt is an instrumentation that is almost used in all
h i lhospitals
Endemics occurs throughout the hospitalg p
The daily IR is 2-16% for the first 10 days in theclose system drainageclose system drainage
Universal infection by 30 days in the close d isystem drainage

Cont…Cont…EpidemEpidem
Magnitude of the problemMagnitude of the problemg pg pIncidence and costIncidence and cost
1515 –– 2020 % of total hospital admission have FC% of total hospital admission have FC15 15 20 20 % of total hospital admission have FC% of total hospital admission have FCNearly Nearly 900900,,000 000 nosocomial UTI in the USnosocomial UTI in the USIt cost $It cost $600600 million if LOS increased bymillion if LOS increased by 11 daydayIt cost $It cost $600 600 million if LOS increased by million if LOS increased by 1 1 daydayIn reality LOS increased by average of In reality LOS increased by average of 33..8 8 days days costing $costing $33 billionbillioncosting $costing $3 3 billionbillion

Cont…Cont…EpidemEpidem
MortalityMortalityRelated to Related to bacteremiabacteremia which accounts for which accounts for 00..3 3 –– 33..99% of total % of total UTIsUTIsOut of which fatality exceed Out of which fatality exceed 3030% (% (4500 4500 death/year)death/year)
MorbidityMorbiditySpread of infection through out urinary tract Spread of infection through out urinary tract causing; causing; absessesabsesses, , epididymitisepididymitis, , orchitisorchitis…etc.…etc.O h li i lik d lO h li i lik d lOther complications like stones and polyps Other complications like stones and polyps

Consequences of antibiotic useConsequences of antibiotic useqqEmergence of resistant strainsEmergence of resistant strains
Epidemics of HA UTIEpidemics of HA UTIEpidemics of HA UTIEpidemics of HA UTIUrinary drainage bag act as a reservoir for Urinary drainage bag act as a reservoir for the organisms to colonize and to transfer thethe organisms to colonize and to transfer thethe organisms to colonize and to transfer the the organisms to colonize and to transfer the resistant plasmid resistant plasmid With poor hand hygiene crossWith poor hand hygiene cross--infection lead infection lead p ygp ygto hospital wide organismsto hospital wide organisms

Etiologic AgentsEtiologic Agents
Fecal FloraFecal Flora
15%25%
7%
16%11%
8%
E.Coli Enterococcus P.aeruginosa C.albican K.Pneumoniae Others

PathogenesisPathogenesis
Role of catheterTransurethral catheter break the normal defense mechanismTh i b ll l iThe retention balloon prevents complete emptyingOpen channel to the bladder
i b dForeign body

Bacterial factorsBacterial factorsPiliPiliHemolysinHemolysin
UreaseUreaseUreaseUrease
Pathways of infectionPathways of infectionIntraluminal (exogenous organism)Intraluminal (exogenous organism)Intraluminal (exogenous organism)Intraluminal (exogenous organism)Extraluminal (endogenous organism)Extraluminal (endogenous organism)

Host factorsHost factorsDuration of useDuration of useFemale genderFemale genderAbsence of systemic antibioticsAbsence of systemic antibioticsyyDMDMRenal insufficiency Renal insufficiency yyAdvanced ageAdvanced ageSevere underlying illnessesSevere underlying illnessesSevere underlying illnessesSevere underlying illnesses

DiagnosisDiagnosis
CDC definition
Exclude infections that acquired prior to admission
Asymptomatic bacteriuia should have > 100,000 cfu/cchave 100,000 cfu/cc
Culturing the catheter tip is of NO VALUEg p
Uses of symptoms; only fever

Specimen collectionSpecimen collection
It is preferable to obtain specimen from It is preferable to obtain specimen from new catheter rather than old catheternew catheter rather than old catheterUrine obtained through inserting needle Urine obtained through inserting needle into catheter or through diaphragminto catheter or through diaphragminto catheter or through diaphragm into catheter or through diaphragm For suprapubic and straight catheter; For suprapubic and straight catheter; specimen obtained directly from bladderspecimen obtained directly from bladderspecimen obtained directly from bladderspecimen obtained directly from bladder

PreventionPrevention
Close sterile drainage system
Infection control and surveillance programsInfection control and surveillance programsGuidelines
Alternative to FC
Adjunct to closed drainage
Alternative to FC
Secondary prevention

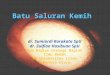
Surveillance dataSurveillance data
BenchmarkingBenchmarking
13 66 1416
9.19.43
13.66
11.0311.6
6 96 98.45
7 2 8101214
00 F
-day
s
6.96.26.97.2
3.43.43.83.64
0246
Per 1
00
0MarchFebruaryJanuaryDecemberNovember
Hospital 1 Hospital 2 Hospital 3p p p

RecommendationRecommendation
Put your evidencePut your evidence--based IC guidelinesbased IC guidelinesHCW behavioral modificationHCW behavioral modificationDo your surveillance properlyDo your surveillance properlyo you u a p op yo you u a p op yBenchmark yourself overtimeBenchmark yourself overtimePI projectsPI projectsPI projectsPI projectsNNIS NNIS
Fully computerized patient recordsFully computerized patient recordsDataData--miningmining--derived epidemiologyderived epidemiology