Embed Size (px)
Citation preview

Lecture 1:
Inequalities and inequities in health
and health care utilization
Concentration curve and
concentration index
1

Health inequality and inequity
• Rich-poor inequalities in health largely, if not entirely, derive from differences in constraints (e.g. incomes, time costs, health insurance, environment) rather than in preferences.
• Hence they are often considered to represent inequities.
• But in high-income countries the poor often use more health care and this may not represent inequity.
• Drawing conclusions about health equity involves consideration of the causes of health inequalities.

Equity of what?
• Health outcomes, e.g. infant mortality, child growth,
disability, incidence of illness, general health, life
expectancy.
• Health care utilisation, e.g. doctor visits, inpatient
stays, vaccinations, maternity care.
• Subsidies received through use of public health care.
• Payments for health care (both direct and indirect).

Equity in relation to what?
• Equity in health, health care and health payments could be examined in relation to gender, ethnicity, geographic location, education, income….
• This course focuses on equity by socioeconomic status, usually measured by income, wealth or consumption.
• Many of the techniques are applicable to equity in relation to other characteristics but they often require that individuals can be ranked by that characteristic.

The basic idea

The basic idea
• The poor typically lag behind the better off in terms of health outcomes and utilization of health services
• Policymakers would like to track progress – is the gap narrowing? – and see how their country compares to other countries
• Data are often presented in terms of economic or socioeconomic groups
• With several groups, it’s not easy to see how inequalities compare or have changed

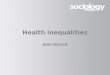
In which country are child deaths
distributed most unequally?
0
50
100
150
200
250
300
India Mali
U5M
R p
er
1000 liv
e b
irth
s
Poorest"quintile"
2nd poorest"quintile
Middle "quintile"
2nd richest"quintile"
Richest"quintile"
Rate ratios can be used: but don’t consider how skewed the distribution is in the
middle quintiles
Comparison made difficult by differences in average levels

In which country is child stunting distributed most
unequally? Which country has made the largest
progress in reducing inequalities?

Let’s get measuring!

How to measure health disparities?
• Measures of dispersion like the variance, coefficient of variation, or Theil’s entropy inform of total, not socioeconomic-related health inequality
• Relative risk ratios, e.g. mortality in top to bottom occupation class, do not take account of group sizes
• Rate ratios of top to bottom quintiles do not reflect the complete distribution
• Borrow rank-dependent measures—Lorenz curve and GiniIndex—and their bivariate extensions—concentration curve and index—from income distribution literature and apply to socioeconomic-related inequality in health variables

Illness concentration curve
Poorest 50% of population
75% of
disease
burden
Cu
mu
lati
ve %
of
illn
ess
Cumulative % population,
ranked in ascending order of income, wealth, etc.
Here inequality
disfavors the poor:
they bear a greater
share of illness
than their share in
the population
The further the CC
is from the line of
equality, the
greater the
inequality!

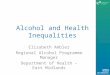
Comparing too many concentration
curves is bad for your eyes!
0%
20%
40%
60%
80%
100%
0% 20% 40% 60% 80% 100%
cumul % live births,
ranked by equiv consumption
cu
mu
l %
un
de
r-5
de
ath
s
Equality
Brazil
Cote d'Ivoire
Ghana
Nepal
Nicaragua
Pakistan
Cebu
S Africa
Vietnam
Brazil is most unequal,
but how do the rest
compare?

The concentration index
is a useful tie-breaker
Poorest 50% of population
75% of
disease
burden
Cu
mu
lati
ve p
rop
ort
ion
of
illn
ess
Concentration index (CI) = 2 x shaded area
CI lies in range (-1,1)
CI < 0 because variableis “concentrated” among the poor

The case where inequalities in illness
favor the poor
Poorest 50% of population
25% of
disease
burden
Cu
mu
lati
ve p
rop
ort
ion
of
illn
ess
Here inequality
favors the poor:
they bear a smaller
share of illness
than their share in
the population
Concentration index (=2 x shaded area, as before) is positive in this case because variable is “concentrated” among the better off

Beware!
A negative CI doesn’t necessarily imply poor
outcomes for the poor. It depends on whether
the health variable being analyzed is a “good”
outcome or a “bad” outcome.

0%
25%
50%
75%
100%
0% 25% 50% 75% 100%
cum. % population ranked by income
cum
. %
of
hea
lth
va
ria
ble
C = 2 x area between 450 line and concentration curve
= 2A=2(0.5 - B) = 1 - 2B
C>0 (<0) if health variable is disproportionately concentrated on rich (poor)
C=0 if distribution is proportionate(unless crossing diagonal)
C lies in range (-1,1)
C=1 if richest person has all of the health variableC=-1 of poorest person has all of the health variable
Concentration index defined
A
B( )h
L p

Some formulae for the concentration index
( )1
0
1 2 hC L p dp= − ∫
1
2 11
n
i i
i
C h rn nµ =
= − −∑
If the living standards variable is discrete:
where n is sample size, h the
health variable, μ its mean and
r the fractional rank by income
( )2
cov ,C h rµ
=
For computation, this is more convenient:

Properties of the concentration index
• depend on the measurement characteristics of the health variable of interest.
• Strictly, requires ratio scaled, non-negative variable
• Invariant to multiplication by scalar
• But not to any linear transformation
• So, not appropriate for interval scaled variable with arbitrary mean
• This can be problematic for measures of health that are often ordinal
• If variable is dichotomous, C lies in the interval (μ-1, 1-μ) (Wagstaff, 2005):
– So interval shrinks as mean rises.
– Normalise by dividing C by 1-μ

Erreygers’ (2009) has normalized the
concentration index for bounded variables
• This satisfies the following axioms:
– Level independence: E(h*)=E(h), h*=k+h
– Cardinal consistency: E(h*)=E(h), h*=k+gH, k>0, g>0
– Mirror: E(h)=-E(s), s=bh-h
– Monotonicity
– Transfer
( ) ( )4h h
E h C hb a
µ=
−
Where bh and ah are the max and min
of the health variable (h), and μ is the mean

Total inequality in health and
socioeconomic-related health inequality
0%
20%
40%
60%
80%
100%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
cum % of pop, ranked by health or income
cu
m %
of
he
alt
h
diagonal Lorenz curve Conc curve
By definition, the
health Lorenz curve
must lie below the
concentration curve.
That is, total health
inequality is greater
than income-related
health inequality.

Total inequality in health is larger than
socioeconomic-related health inequalityGini index of total health inequality
Then
Thus, G = C + R, where R>=0 and measures the outward move from the health concentration curve to the health Lorenz curve, or the re-ranking in moving from the SES to the health distribution
“even if the social class gradient was magically eliminated, dispersion in health outcomes in the population would remain very much the same”
Smith J, 1999, Healthy bodies and thick wallets”, J Econ Perspectives
µ=
2cov( , )
hG h r
= ≥cov( , )
1cov( , )
hh rG
C h r
rh is rank in health distribution

Estimating the concentration index from
micro data
• Use “convenient covariance” formula C=2cov(h,r)/μ– Weights applied in computation of mean, covar and rank
• Equivalently, use “convenient regression”
– Where the fractional rank (r) is calculated as follows if there are weights (w)
– OLS estimate of β is the estimate of the concentration index
22 ir i i
hrσ α β ε
µ
= + +
1
0
0
, 02
ii
i j
j
wr w w
−
=
= + =∑

Sensitivity of the concentration index to
the living standards measure
• C reflects covariance between health and rank in
the living standards distribution
• C will differ across living standards measures if re-
ranking of individuals is correlated with health
(Wagstaff & Watanabe, 2003)
22 i
r i i
hrσ α γ ε
µ∆
= + ∆ +
1 2ˆC C γ− =
From OLS estimate of
where is the re-ranking and 1 2i i i
r r r∆ = − 2
rσ ∆ its variance,
the difference in concentration indices is

Evidence on sensitivity of concentration
index
Wagstaff & Watanabe (2003) – signif. difference b/w C estimated
from consumption and assets index in only 6/19 cases for
underweight and stunting
But Lindelow (2006) finds greater sensitivity in concentration
indices for health service utilization in Mozambique
Consumption Asset index
Difference
CIC – CIAI
t-value for
differenceCI t-value CI t-value
Hospital visits 0.166 8.72 0.231 12.94 -0.065 -3.35
Health center visits 0.066 3.85 -0.136 -8.49 0.202 9.99
Complete immunizations 0.059 8.35 0.194 34.69 -0.135 -19.1
Delivery control 0.063 11.86 0.154 35.01 -0.091 -15.27
Institutional delivery 0.089 11.31 0.266 43.26 -0.176 -20.06

Concentration indices for U5MR
25
-0.5
-0.4
-0.3
-0.2
-0.1
0.0
0.1
Vie
tnam
1982-9
3
Pakis
tan 1
981-9
0
Ghana 1
978-8
9
Cote
d’Ivoire 1
978-8
9
Nepal 1985-9
6
South
Afr
ica 1
985-8
9
Phillipin
es (
Cebu)
1981-9
1
Nic
ara
gua 1
983-8
8
Bra
zil (
NE &
SE)
1987-
92
C a
nd 9
5%
conf in
terv
al

Changes in CIs of stunting

Taking account of the level and the
distribution of healthIf there is concern for the level of health, and not only socioeconomic-
related inequality in its distribution, then may want a summary statistic to reflect mean health in addition to this inequality.
Might refer to such a measure as an index of ‘health achievement’.
An index of health achievement can be obtained by taking a weighted average of levels of health, rather than of health shares, as follows:
That is simply the product of the mean and one minus the extended CI.
So, for a desirable health variable, increases in the mean may be traded-off against increases in pro-rich inequality
For a non-desirable health variable, decreases in the mean can be traded-off against increases in its concentration on the poor.
( )( )
( )( )ν
ν ν µ ν−
== − = −∑
1
1
1( ) 1 1
n
i iiI h r C
n

Mean and inequality-weighted mean in
under-five mortality

Mean and inequality-weighted
mean of medically attended birthsDeliveries by a medically-trained person
0
10
20
30
40
50
60
70
80
90
100
Guate
mala
Haiti
Peru
Boliv
ia
Nicara
gua
Colo
mbia
Bra
zil
Dom
inican
Rep.
% b
abie
s deliv
ere
d b
y a
medically
-tra
ined p
ers
on
Mean
Achievement

Where to go from here?
• Analyses of equity in health requires data on
– Health
• Infant mortality, stunting/wasting, self-assessed health
• Chronic conditions -> reporting bias!
• Measured hypertension, grip strength, blood tests
– Socioeconomic status
• Need to be able to rank people from poor to reach
• Consumption, expenditure, wealth index