Embed Size (px)
Citation preview

Induced Abortions in Minnesota January - December 2016
Report to the Legislature
July 2017
Induced Abortions in Minnesota January ndash December 2016 Report to the Legislature
July 2017
Minnesota Department of Health Center for Health Statistics PO Box 64882 St Paul MN 55164-0882 651-201-5945 800-657-3900 HEALTHHealthStatsstatemnus wwwhealthstatemnus
As requested by Minnesota Statute 3197 This report cost approximately $4000 to prepare including staff time printing and mailing expenses
Upon request this material will be made available in an alternative format such as large print Braille or audio recording Printed on recycled paper
Table of Contents
Introduction hellip iii
Technical Notes hellip vii
Tables Table 11 Abortions by Month and Provider for Facilities helliphelliphelliphelliphelliphellip 3 Table 12 Abortions by Month and Provider for Physicians helliphelliphelliphelliphellip 4 Table 2 Medical Specialty of Physician hellip 6 Table 3 Type of Admission hellip 6 Table 4 Age of Woman 7 Table 5 Marital Status of Woman 7 Table 6 CountryState Residence of Woman 8 Table 7 County of Residence for Women Residing in Minnesota 9 Table 8 Hispanic Origin of Woman 10 Table 9 Race of Woman hellip 10 Table 10 Education Level of Woman hellip 11 Table 11 Clinical Estimate of Fetal Gestational Age(grouped)helliphelliphellip 12 Table 11a Clinical Estimate of Fetal Gestational Age helliphelliphellip 13 Table 12 Prior Pregnancies hellip 14
15 16
17 18
19
Table 13 Contraceptive Use and Method Table 14 Abortion ProcedureTable 15 Method of Disposal of Fetal RemainsTable 16 Payment Type and Health Insurance CoverageTable 17 Reason for Abortion Table 17a Other Stated Reason for Abortion helliphelliphellip 20 Table 18 Intraoperative Complications hellip 21 Table 19 Postoperative Complications 22 Table 20 Induced Abortions by Gestational Age - Performed Out of State and Paid for with State Funds hellip 23 Table 21 Total and Resident Induced Abortions 1975-2015 helliphelliphelliphelliphellip 24 Table 22 Abortions per 100 Live Births by Selected Characteristics helliphellip 25 Table 23 Selected Statistics by Age Group helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 26 Table 24 Contraceptive Use by Age Group and Marital Status helliphelliphelliphellip 27 Table 25 Medical Risks Information Informed Consent helliphelliphellip helliphelliphellip 31 Table 26 Medical AssistancePrinted Materials Information
Informed Consent helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 32 Table 27 Patient Access to Printed Materials Informed Consent helliphelliphellip 33 Born Alive Infants Protection Act Report helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 37
Appendix Born Alive Infants Protection Acthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 41 Updates to 2015 Data helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Data Collection Instruments
47 Definitions hellip 53
Figure 1 Report of Induced Abortion hellip 57 Figure 2 Report of Complication(s) from Induced Abortion hellip 61
Figure 3 Report of Informed Consent for Induced Abortion helliphelliphelliphellip 63
Introduction
Introduction
This report is issued in compliance with Minnesota Statutes section 1454134 which requires a yearly public report of induced abortion statistics for the previous calendar year and statistics for prior years adjusted to reflect any additional information from late andor corrected report forms beginning with October 1 1998 data This is the eighteenth such report and covers the period from January 1 through December 31 2016 Additional Report of Informed Consent Related to Induced Abortion forms for 2015 were submitted after publication of the 2015 data in July of 2016 Applicable updated tables can be found in the appendix
History
The 1998 Minnesota Legislature amended Minnesotarsquos abortion reporting requirement to include all physicians licensed and practicing in Minnesota who perform abortions and all Minnesota facilities in which abortions are performed (Minnesota Statutes sections 1454131 shy1454136) A report must be completed and submitted to the Minnesota Department of Health (MDH) for each procedure performed This law also expanded the content of the reporting form The number of induced abortions performed out-of-state and paid for with state funds must be reported to MDH by the Minnesota Department of Human Services Furthermore any medical facility or any licensed practicing physician in Minnesota who encounters an illness or injury that is the result of an induced abortion must submit a report of that complication on a separate form developed for that purpose Both of these forms Report of Induced Abortion and Report of Complication(s) from Induced Abortion are included in the Appendix of this publication
The 2003 Minnesota Legislature enacted the Womanrsquos Right to Know Act This law [Minnesota Statutes sections 1454241 ndash 1454249] requires physicians to provide women with certain information at least 24 hours prior to an abortion and to collect and report to MDH the number of women who were provided this information Physicians were required to begin collecting this data on January 1 2004 and to submit their 2016 data to MDH by April 1 2017 Additional information about the Womanrsquos Right to Know Act can be found at httpwwwhealthstatemnuswrtkindexhtml
The 2006 Minnesota Legislature amended the Womanrsquos Right to Know Act (WRTK) regarding the circumstance of a patient seeking an abortion of an unborn child diagnosed with a fetal anomaly incompatible with life The patient must be informed of available perinatal hospice services and offered this care as an alternative to abortion If the patient accepts the care the information required under the WRTK need not be provided to her If she declines hospice services and elects abortion only information about medical risks gestational age and anesthesia must be given
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infant Protection Actrdquo a portion of which amended the abortion reporting requirements to add whether an abortion results in a born alive infant Information collected includes medical actions taken to preserve the life of the infant whether the infant survived and the status of a surviving infant The text of this act can be found in the Appendix of this publication [Minnesota Statutes sections 1454131 subdivision 1 and 145423 subdivisions 1 through 9]
Page iii
Technical Notes
Technical Notes
Data included in this report are submitted to the Minnesota Department of Health by facilities and physicians who perform abortions in Minnesota The Report of Induced Abortion (see Appendix Figure 1) may be submitted by a facilityclinic on behalf of physicians who practice therein or physicians may submit reports independently A number of data items on the report form are specifically required by Minnesota Statutes These items include medical specialty of the physician performing the abortion patient age date of the abortion clinical estimate of gestation number of previous spontaneous and induced abortions type of abortion procedure intra-operative complications (post-operative complications are collected using the Report of Complication(s) from Induced Abortion) method of disposal of fetal remains type of payment health coverage type and reason for the abortion The items type of admission patient residence date of last menses and contraceptive use and method were included to provide continuity with previous abortion report forms Marital status Hispanic origin race education and previous live births correspond to items on the Minnesota Medical Supplement to the Certificate of Live Birth and thus allow for statistical comparison with birth data and the calculation of pregnancy rates
Report forms submitted with incomplete data are required by law to be returned to the clinicfacility or independently reporting physician for correction Overall compliance and cooperation in completing the forms is excellent however some data remain unreported In some cases this is due to a facility being unable to locate the record in question and in other instances due to a patientrsquos refusal to provide the data Continuing efforts are being made to further improve reporting compliance completeness and timeliness
Due to the sensitivity of abortion data there are concerns about revealing an individualrsquos identity whether patient or provider from data presented in this publication Minnesota Statutes section 1454134 states ldquoThe commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included on the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which an individual having performed or having had an abortion may be identified using epidemiologic principlesrdquo
Data generally are suppressed when there are such small numbers of two or more variables that it would be difficult to protect the confidentiality of individuals For instance age groups tallied for only a single town in Minnesota would most likely have small counts in some of the age groups Likewise a table of age group by race for each county in Minnesota would have small counts in cells for those counties with small populations and few minority residents Suppression of those small counts are be necessary to protect the confidentiality of the individual
Page vii
Data by provider Tables 11 and 12 are presented for individual clinics that have been publicly identified as abortion providers but aggregated into a single group for independently reporting physicians Table 12 presents data on individual physicians with no small-number suppression as the law requires counts by physician by month Physicians are simply identified as Physician A Physician B etc to protect confidentiality Please note that the identifiers are arbitrarily assigned to those physicians who reported in a given calendar year Thus Physician X in a prior yearrsquos report may not be the same individual as Physician X in this report Data presented in frequency tables for the state as a whole have no small-number data suppressed Likewise Table 6 CountryState Residence of Woman contains sufficiently large groups to confound identification of an individual Table 7 County of Residence for Women Residing in Minnesota is the only table for which counts of zero to five are suppressed Some of the counties have a small population of females of childbearing age andor a small number of physicians who may be qualified to provide abortion services and thus though unlikely it could be possible for a provider or patient to be identified
Page viii
Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Induced Abortions in Minnesota January ndash December 2016 Report to the Legislature
July 2017
Minnesota Department of Health Center for Health Statistics PO Box 64882 St Paul MN 55164-0882 651-201-5945 800-657-3900 HEALTHHealthStatsstatemnus wwwhealthstatemnus
As requested by Minnesota Statute 3197 This report cost approximately $4000 to prepare including staff time printing and mailing expenses
Upon request this material will be made available in an alternative format such as large print Braille or audio recording Printed on recycled paper
Table of Contents
Introduction hellip iii
Technical Notes hellip vii
Tables Table 11 Abortions by Month and Provider for Facilities helliphelliphelliphelliphelliphellip 3 Table 12 Abortions by Month and Provider for Physicians helliphelliphelliphelliphellip 4 Table 2 Medical Specialty of Physician hellip 6 Table 3 Type of Admission hellip 6 Table 4 Age of Woman 7 Table 5 Marital Status of Woman 7 Table 6 CountryState Residence of Woman 8 Table 7 County of Residence for Women Residing in Minnesota 9 Table 8 Hispanic Origin of Woman 10 Table 9 Race of Woman hellip 10 Table 10 Education Level of Woman hellip 11 Table 11 Clinical Estimate of Fetal Gestational Age(grouped)helliphelliphellip 12 Table 11a Clinical Estimate of Fetal Gestational Age helliphelliphellip 13 Table 12 Prior Pregnancies hellip 14
15 16
17 18
19
Table 13 Contraceptive Use and Method Table 14 Abortion ProcedureTable 15 Method of Disposal of Fetal RemainsTable 16 Payment Type and Health Insurance CoverageTable 17 Reason for Abortion Table 17a Other Stated Reason for Abortion helliphelliphellip 20 Table 18 Intraoperative Complications hellip 21 Table 19 Postoperative Complications 22 Table 20 Induced Abortions by Gestational Age - Performed Out of State and Paid for with State Funds hellip 23 Table 21 Total and Resident Induced Abortions 1975-2015 helliphelliphelliphelliphellip 24 Table 22 Abortions per 100 Live Births by Selected Characteristics helliphellip 25 Table 23 Selected Statistics by Age Group helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 26 Table 24 Contraceptive Use by Age Group and Marital Status helliphelliphelliphellip 27 Table 25 Medical Risks Information Informed Consent helliphelliphellip helliphelliphellip 31 Table 26 Medical AssistancePrinted Materials Information
Informed Consent helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 32 Table 27 Patient Access to Printed Materials Informed Consent helliphelliphellip 33 Born Alive Infants Protection Act Report helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 37
Appendix Born Alive Infants Protection Acthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 41 Updates to 2015 Data helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Data Collection Instruments
47 Definitions hellip 53
Figure 1 Report of Induced Abortion hellip 57 Figure 2 Report of Complication(s) from Induced Abortion hellip 61
Figure 3 Report of Informed Consent for Induced Abortion helliphelliphelliphellip 63
Introduction
Introduction
This report is issued in compliance with Minnesota Statutes section 1454134 which requires a yearly public report of induced abortion statistics for the previous calendar year and statistics for prior years adjusted to reflect any additional information from late andor corrected report forms beginning with October 1 1998 data This is the eighteenth such report and covers the period from January 1 through December 31 2016 Additional Report of Informed Consent Related to Induced Abortion forms for 2015 were submitted after publication of the 2015 data in July of 2016 Applicable updated tables can be found in the appendix
History
The 1998 Minnesota Legislature amended Minnesotarsquos abortion reporting requirement to include all physicians licensed and practicing in Minnesota who perform abortions and all Minnesota facilities in which abortions are performed (Minnesota Statutes sections 1454131 shy1454136) A report must be completed and submitted to the Minnesota Department of Health (MDH) for each procedure performed This law also expanded the content of the reporting form The number of induced abortions performed out-of-state and paid for with state funds must be reported to MDH by the Minnesota Department of Human Services Furthermore any medical facility or any licensed practicing physician in Minnesota who encounters an illness or injury that is the result of an induced abortion must submit a report of that complication on a separate form developed for that purpose Both of these forms Report of Induced Abortion and Report of Complication(s) from Induced Abortion are included in the Appendix of this publication
The 2003 Minnesota Legislature enacted the Womanrsquos Right to Know Act This law [Minnesota Statutes sections 1454241 ndash 1454249] requires physicians to provide women with certain information at least 24 hours prior to an abortion and to collect and report to MDH the number of women who were provided this information Physicians were required to begin collecting this data on January 1 2004 and to submit their 2016 data to MDH by April 1 2017 Additional information about the Womanrsquos Right to Know Act can be found at httpwwwhealthstatemnuswrtkindexhtml
The 2006 Minnesota Legislature amended the Womanrsquos Right to Know Act (WRTK) regarding the circumstance of a patient seeking an abortion of an unborn child diagnosed with a fetal anomaly incompatible with life The patient must be informed of available perinatal hospice services and offered this care as an alternative to abortion If the patient accepts the care the information required under the WRTK need not be provided to her If she declines hospice services and elects abortion only information about medical risks gestational age and anesthesia must be given
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infant Protection Actrdquo a portion of which amended the abortion reporting requirements to add whether an abortion results in a born alive infant Information collected includes medical actions taken to preserve the life of the infant whether the infant survived and the status of a surviving infant The text of this act can be found in the Appendix of this publication [Minnesota Statutes sections 1454131 subdivision 1 and 145423 subdivisions 1 through 9]
Page iii
Technical Notes
Technical Notes
Data included in this report are submitted to the Minnesota Department of Health by facilities and physicians who perform abortions in Minnesota The Report of Induced Abortion (see Appendix Figure 1) may be submitted by a facilityclinic on behalf of physicians who practice therein or physicians may submit reports independently A number of data items on the report form are specifically required by Minnesota Statutes These items include medical specialty of the physician performing the abortion patient age date of the abortion clinical estimate of gestation number of previous spontaneous and induced abortions type of abortion procedure intra-operative complications (post-operative complications are collected using the Report of Complication(s) from Induced Abortion) method of disposal of fetal remains type of payment health coverage type and reason for the abortion The items type of admission patient residence date of last menses and contraceptive use and method were included to provide continuity with previous abortion report forms Marital status Hispanic origin race education and previous live births correspond to items on the Minnesota Medical Supplement to the Certificate of Live Birth and thus allow for statistical comparison with birth data and the calculation of pregnancy rates
Report forms submitted with incomplete data are required by law to be returned to the clinicfacility or independently reporting physician for correction Overall compliance and cooperation in completing the forms is excellent however some data remain unreported In some cases this is due to a facility being unable to locate the record in question and in other instances due to a patientrsquos refusal to provide the data Continuing efforts are being made to further improve reporting compliance completeness and timeliness
Due to the sensitivity of abortion data there are concerns about revealing an individualrsquos identity whether patient or provider from data presented in this publication Minnesota Statutes section 1454134 states ldquoThe commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included on the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which an individual having performed or having had an abortion may be identified using epidemiologic principlesrdquo
Data generally are suppressed when there are such small numbers of two or more variables that it would be difficult to protect the confidentiality of individuals For instance age groups tallied for only a single town in Minnesota would most likely have small counts in some of the age groups Likewise a table of age group by race for each county in Minnesota would have small counts in cells for those counties with small populations and few minority residents Suppression of those small counts are be necessary to protect the confidentiality of the individual
Page vii
Data by provider Tables 11 and 12 are presented for individual clinics that have been publicly identified as abortion providers but aggregated into a single group for independently reporting physicians Table 12 presents data on individual physicians with no small-number suppression as the law requires counts by physician by month Physicians are simply identified as Physician A Physician B etc to protect confidentiality Please note that the identifiers are arbitrarily assigned to those physicians who reported in a given calendar year Thus Physician X in a prior yearrsquos report may not be the same individual as Physician X in this report Data presented in frequency tables for the state as a whole have no small-number data suppressed Likewise Table 6 CountryState Residence of Woman contains sufficiently large groups to confound identification of an individual Table 7 County of Residence for Women Residing in Minnesota is the only table for which counts of zero to five are suppressed Some of the counties have a small population of females of childbearing age andor a small number of physicians who may be qualified to provide abortion services and thus though unlikely it could be possible for a provider or patient to be identified
Page viii
Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table of Contents
Introduction hellip iii
Technical Notes hellip vii
Tables Table 11 Abortions by Month and Provider for Facilities helliphelliphelliphelliphelliphellip 3 Table 12 Abortions by Month and Provider for Physicians helliphelliphelliphelliphellip 4 Table 2 Medical Specialty of Physician hellip 6 Table 3 Type of Admission hellip 6 Table 4 Age of Woman 7 Table 5 Marital Status of Woman 7 Table 6 CountryState Residence of Woman 8 Table 7 County of Residence for Women Residing in Minnesota 9 Table 8 Hispanic Origin of Woman 10 Table 9 Race of Woman hellip 10 Table 10 Education Level of Woman hellip 11 Table 11 Clinical Estimate of Fetal Gestational Age(grouped)helliphelliphellip 12 Table 11a Clinical Estimate of Fetal Gestational Age helliphelliphellip 13 Table 12 Prior Pregnancies hellip 14
15 16
17 18
19
Table 13 Contraceptive Use and Method Table 14 Abortion ProcedureTable 15 Method of Disposal of Fetal RemainsTable 16 Payment Type and Health Insurance CoverageTable 17 Reason for Abortion Table 17a Other Stated Reason for Abortion helliphelliphellip 20 Table 18 Intraoperative Complications hellip 21 Table 19 Postoperative Complications 22 Table 20 Induced Abortions by Gestational Age - Performed Out of State and Paid for with State Funds hellip 23 Table 21 Total and Resident Induced Abortions 1975-2015 helliphelliphelliphelliphellip 24 Table 22 Abortions per 100 Live Births by Selected Characteristics helliphellip 25 Table 23 Selected Statistics by Age Group helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 26 Table 24 Contraceptive Use by Age Group and Marital Status helliphelliphelliphellip 27 Table 25 Medical Risks Information Informed Consent helliphelliphellip helliphelliphellip 31 Table 26 Medical AssistancePrinted Materials Information
Informed Consent helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 32 Table 27 Patient Access to Printed Materials Informed Consent helliphelliphellip 33 Born Alive Infants Protection Act Report helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 37
Appendix Born Alive Infants Protection Acthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 41 Updates to 2015 Data helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
Data Collection Instruments
47 Definitions hellip 53
Figure 1 Report of Induced Abortion hellip 57 Figure 2 Report of Complication(s) from Induced Abortion hellip 61
Figure 3 Report of Informed Consent for Induced Abortion helliphelliphelliphellip 63
Introduction
Introduction
This report is issued in compliance with Minnesota Statutes section 1454134 which requires a yearly public report of induced abortion statistics for the previous calendar year and statistics for prior years adjusted to reflect any additional information from late andor corrected report forms beginning with October 1 1998 data This is the eighteenth such report and covers the period from January 1 through December 31 2016 Additional Report of Informed Consent Related to Induced Abortion forms for 2015 were submitted after publication of the 2015 data in July of 2016 Applicable updated tables can be found in the appendix
History
The 1998 Minnesota Legislature amended Minnesotarsquos abortion reporting requirement to include all physicians licensed and practicing in Minnesota who perform abortions and all Minnesota facilities in which abortions are performed (Minnesota Statutes sections 1454131 shy1454136) A report must be completed and submitted to the Minnesota Department of Health (MDH) for each procedure performed This law also expanded the content of the reporting form The number of induced abortions performed out-of-state and paid for with state funds must be reported to MDH by the Minnesota Department of Human Services Furthermore any medical facility or any licensed practicing physician in Minnesota who encounters an illness or injury that is the result of an induced abortion must submit a report of that complication on a separate form developed for that purpose Both of these forms Report of Induced Abortion and Report of Complication(s) from Induced Abortion are included in the Appendix of this publication
The 2003 Minnesota Legislature enacted the Womanrsquos Right to Know Act This law [Minnesota Statutes sections 1454241 ndash 1454249] requires physicians to provide women with certain information at least 24 hours prior to an abortion and to collect and report to MDH the number of women who were provided this information Physicians were required to begin collecting this data on January 1 2004 and to submit their 2016 data to MDH by April 1 2017 Additional information about the Womanrsquos Right to Know Act can be found at httpwwwhealthstatemnuswrtkindexhtml
The 2006 Minnesota Legislature amended the Womanrsquos Right to Know Act (WRTK) regarding the circumstance of a patient seeking an abortion of an unborn child diagnosed with a fetal anomaly incompatible with life The patient must be informed of available perinatal hospice services and offered this care as an alternative to abortion If the patient accepts the care the information required under the WRTK need not be provided to her If she declines hospice services and elects abortion only information about medical risks gestational age and anesthesia must be given
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infant Protection Actrdquo a portion of which amended the abortion reporting requirements to add whether an abortion results in a born alive infant Information collected includes medical actions taken to preserve the life of the infant whether the infant survived and the status of a surviving infant The text of this act can be found in the Appendix of this publication [Minnesota Statutes sections 1454131 subdivision 1 and 145423 subdivisions 1 through 9]
Page iii
Technical Notes
Technical Notes
Data included in this report are submitted to the Minnesota Department of Health by facilities and physicians who perform abortions in Minnesota The Report of Induced Abortion (see Appendix Figure 1) may be submitted by a facilityclinic on behalf of physicians who practice therein or physicians may submit reports independently A number of data items on the report form are specifically required by Minnesota Statutes These items include medical specialty of the physician performing the abortion patient age date of the abortion clinical estimate of gestation number of previous spontaneous and induced abortions type of abortion procedure intra-operative complications (post-operative complications are collected using the Report of Complication(s) from Induced Abortion) method of disposal of fetal remains type of payment health coverage type and reason for the abortion The items type of admission patient residence date of last menses and contraceptive use and method were included to provide continuity with previous abortion report forms Marital status Hispanic origin race education and previous live births correspond to items on the Minnesota Medical Supplement to the Certificate of Live Birth and thus allow for statistical comparison with birth data and the calculation of pregnancy rates
Report forms submitted with incomplete data are required by law to be returned to the clinicfacility or independently reporting physician for correction Overall compliance and cooperation in completing the forms is excellent however some data remain unreported In some cases this is due to a facility being unable to locate the record in question and in other instances due to a patientrsquos refusal to provide the data Continuing efforts are being made to further improve reporting compliance completeness and timeliness
Due to the sensitivity of abortion data there are concerns about revealing an individualrsquos identity whether patient or provider from data presented in this publication Minnesota Statutes section 1454134 states ldquoThe commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included on the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which an individual having performed or having had an abortion may be identified using epidemiologic principlesrdquo
Data generally are suppressed when there are such small numbers of two or more variables that it would be difficult to protect the confidentiality of individuals For instance age groups tallied for only a single town in Minnesota would most likely have small counts in some of the age groups Likewise a table of age group by race for each county in Minnesota would have small counts in cells for those counties with small populations and few minority residents Suppression of those small counts are be necessary to protect the confidentiality of the individual
Page vii
Data by provider Tables 11 and 12 are presented for individual clinics that have been publicly identified as abortion providers but aggregated into a single group for independently reporting physicians Table 12 presents data on individual physicians with no small-number suppression as the law requires counts by physician by month Physicians are simply identified as Physician A Physician B etc to protect confidentiality Please note that the identifiers are arbitrarily assigned to those physicians who reported in a given calendar year Thus Physician X in a prior yearrsquos report may not be the same individual as Physician X in this report Data presented in frequency tables for the state as a whole have no small-number data suppressed Likewise Table 6 CountryState Residence of Woman contains sufficiently large groups to confound identification of an individual Table 7 County of Residence for Women Residing in Minnesota is the only table for which counts of zero to five are suppressed Some of the counties have a small population of females of childbearing age andor a small number of physicians who may be qualified to provide abortion services and thus though unlikely it could be possible for a provider or patient to be identified
Page viii
Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Introduction
Introduction
This report is issued in compliance with Minnesota Statutes section 1454134 which requires a yearly public report of induced abortion statistics for the previous calendar year and statistics for prior years adjusted to reflect any additional information from late andor corrected report forms beginning with October 1 1998 data This is the eighteenth such report and covers the period from January 1 through December 31 2016 Additional Report of Informed Consent Related to Induced Abortion forms for 2015 were submitted after publication of the 2015 data in July of 2016 Applicable updated tables can be found in the appendix
History
The 1998 Minnesota Legislature amended Minnesotarsquos abortion reporting requirement to include all physicians licensed and practicing in Minnesota who perform abortions and all Minnesota facilities in which abortions are performed (Minnesota Statutes sections 1454131 shy1454136) A report must be completed and submitted to the Minnesota Department of Health (MDH) for each procedure performed This law also expanded the content of the reporting form The number of induced abortions performed out-of-state and paid for with state funds must be reported to MDH by the Minnesota Department of Human Services Furthermore any medical facility or any licensed practicing physician in Minnesota who encounters an illness or injury that is the result of an induced abortion must submit a report of that complication on a separate form developed for that purpose Both of these forms Report of Induced Abortion and Report of Complication(s) from Induced Abortion are included in the Appendix of this publication
The 2003 Minnesota Legislature enacted the Womanrsquos Right to Know Act This law [Minnesota Statutes sections 1454241 ndash 1454249] requires physicians to provide women with certain information at least 24 hours prior to an abortion and to collect and report to MDH the number of women who were provided this information Physicians were required to begin collecting this data on January 1 2004 and to submit their 2016 data to MDH by April 1 2017 Additional information about the Womanrsquos Right to Know Act can be found at httpwwwhealthstatemnuswrtkindexhtml
The 2006 Minnesota Legislature amended the Womanrsquos Right to Know Act (WRTK) regarding the circumstance of a patient seeking an abortion of an unborn child diagnosed with a fetal anomaly incompatible with life The patient must be informed of available perinatal hospice services and offered this care as an alternative to abortion If the patient accepts the care the information required under the WRTK need not be provided to her If she declines hospice services and elects abortion only information about medical risks gestational age and anesthesia must be given
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infant Protection Actrdquo a portion of which amended the abortion reporting requirements to add whether an abortion results in a born alive infant Information collected includes medical actions taken to preserve the life of the infant whether the infant survived and the status of a surviving infant The text of this act can be found in the Appendix of this publication [Minnesota Statutes sections 1454131 subdivision 1 and 145423 subdivisions 1 through 9]
Page iii
Technical Notes
Technical Notes
Data included in this report are submitted to the Minnesota Department of Health by facilities and physicians who perform abortions in Minnesota The Report of Induced Abortion (see Appendix Figure 1) may be submitted by a facilityclinic on behalf of physicians who practice therein or physicians may submit reports independently A number of data items on the report form are specifically required by Minnesota Statutes These items include medical specialty of the physician performing the abortion patient age date of the abortion clinical estimate of gestation number of previous spontaneous and induced abortions type of abortion procedure intra-operative complications (post-operative complications are collected using the Report of Complication(s) from Induced Abortion) method of disposal of fetal remains type of payment health coverage type and reason for the abortion The items type of admission patient residence date of last menses and contraceptive use and method were included to provide continuity with previous abortion report forms Marital status Hispanic origin race education and previous live births correspond to items on the Minnesota Medical Supplement to the Certificate of Live Birth and thus allow for statistical comparison with birth data and the calculation of pregnancy rates
Report forms submitted with incomplete data are required by law to be returned to the clinicfacility or independently reporting physician for correction Overall compliance and cooperation in completing the forms is excellent however some data remain unreported In some cases this is due to a facility being unable to locate the record in question and in other instances due to a patientrsquos refusal to provide the data Continuing efforts are being made to further improve reporting compliance completeness and timeliness
Due to the sensitivity of abortion data there are concerns about revealing an individualrsquos identity whether patient or provider from data presented in this publication Minnesota Statutes section 1454134 states ldquoThe commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included on the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which an individual having performed or having had an abortion may be identified using epidemiologic principlesrdquo
Data generally are suppressed when there are such small numbers of two or more variables that it would be difficult to protect the confidentiality of individuals For instance age groups tallied for only a single town in Minnesota would most likely have small counts in some of the age groups Likewise a table of age group by race for each county in Minnesota would have small counts in cells for those counties with small populations and few minority residents Suppression of those small counts are be necessary to protect the confidentiality of the individual
Page vii
Data by provider Tables 11 and 12 are presented for individual clinics that have been publicly identified as abortion providers but aggregated into a single group for independently reporting physicians Table 12 presents data on individual physicians with no small-number suppression as the law requires counts by physician by month Physicians are simply identified as Physician A Physician B etc to protect confidentiality Please note that the identifiers are arbitrarily assigned to those physicians who reported in a given calendar year Thus Physician X in a prior yearrsquos report may not be the same individual as Physician X in this report Data presented in frequency tables for the state as a whole have no small-number data suppressed Likewise Table 6 CountryState Residence of Woman contains sufficiently large groups to confound identification of an individual Table 7 County of Residence for Women Residing in Minnesota is the only table for which counts of zero to five are suppressed Some of the counties have a small population of females of childbearing age andor a small number of physicians who may be qualified to provide abortion services and thus though unlikely it could be possible for a provider or patient to be identified
Page viii
Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Introduction
This report is issued in compliance with Minnesota Statutes section 1454134 which requires a yearly public report of induced abortion statistics for the previous calendar year and statistics for prior years adjusted to reflect any additional information from late andor corrected report forms beginning with October 1 1998 data This is the eighteenth such report and covers the period from January 1 through December 31 2016 Additional Report of Informed Consent Related to Induced Abortion forms for 2015 were submitted after publication of the 2015 data in July of 2016 Applicable updated tables can be found in the appendix
History
The 1998 Minnesota Legislature amended Minnesotarsquos abortion reporting requirement to include all physicians licensed and practicing in Minnesota who perform abortions and all Minnesota facilities in which abortions are performed (Minnesota Statutes sections 1454131 shy1454136) A report must be completed and submitted to the Minnesota Department of Health (MDH) for each procedure performed This law also expanded the content of the reporting form The number of induced abortions performed out-of-state and paid for with state funds must be reported to MDH by the Minnesota Department of Human Services Furthermore any medical facility or any licensed practicing physician in Minnesota who encounters an illness or injury that is the result of an induced abortion must submit a report of that complication on a separate form developed for that purpose Both of these forms Report of Induced Abortion and Report of Complication(s) from Induced Abortion are included in the Appendix of this publication
The 2003 Minnesota Legislature enacted the Womanrsquos Right to Know Act This law [Minnesota Statutes sections 1454241 ndash 1454249] requires physicians to provide women with certain information at least 24 hours prior to an abortion and to collect and report to MDH the number of women who were provided this information Physicians were required to begin collecting this data on January 1 2004 and to submit their 2016 data to MDH by April 1 2017 Additional information about the Womanrsquos Right to Know Act can be found at httpwwwhealthstatemnuswrtkindexhtml
The 2006 Minnesota Legislature amended the Womanrsquos Right to Know Act (WRTK) regarding the circumstance of a patient seeking an abortion of an unborn child diagnosed with a fetal anomaly incompatible with life The patient must be informed of available perinatal hospice services and offered this care as an alternative to abortion If the patient accepts the care the information required under the WRTK need not be provided to her If she declines hospice services and elects abortion only information about medical risks gestational age and anesthesia must be given
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infant Protection Actrdquo a portion of which amended the abortion reporting requirements to add whether an abortion results in a born alive infant Information collected includes medical actions taken to preserve the life of the infant whether the infant survived and the status of a surviving infant The text of this act can be found in the Appendix of this publication [Minnesota Statutes sections 1454131 subdivision 1 and 145423 subdivisions 1 through 9]
Page iii
Technical Notes
Technical Notes
Data included in this report are submitted to the Minnesota Department of Health by facilities and physicians who perform abortions in Minnesota The Report of Induced Abortion (see Appendix Figure 1) may be submitted by a facilityclinic on behalf of physicians who practice therein or physicians may submit reports independently A number of data items on the report form are specifically required by Minnesota Statutes These items include medical specialty of the physician performing the abortion patient age date of the abortion clinical estimate of gestation number of previous spontaneous and induced abortions type of abortion procedure intra-operative complications (post-operative complications are collected using the Report of Complication(s) from Induced Abortion) method of disposal of fetal remains type of payment health coverage type and reason for the abortion The items type of admission patient residence date of last menses and contraceptive use and method were included to provide continuity with previous abortion report forms Marital status Hispanic origin race education and previous live births correspond to items on the Minnesota Medical Supplement to the Certificate of Live Birth and thus allow for statistical comparison with birth data and the calculation of pregnancy rates
Report forms submitted with incomplete data are required by law to be returned to the clinicfacility or independently reporting physician for correction Overall compliance and cooperation in completing the forms is excellent however some data remain unreported In some cases this is due to a facility being unable to locate the record in question and in other instances due to a patientrsquos refusal to provide the data Continuing efforts are being made to further improve reporting compliance completeness and timeliness
Due to the sensitivity of abortion data there are concerns about revealing an individualrsquos identity whether patient or provider from data presented in this publication Minnesota Statutes section 1454134 states ldquoThe commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included on the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which an individual having performed or having had an abortion may be identified using epidemiologic principlesrdquo
Data generally are suppressed when there are such small numbers of two or more variables that it would be difficult to protect the confidentiality of individuals For instance age groups tallied for only a single town in Minnesota would most likely have small counts in some of the age groups Likewise a table of age group by race for each county in Minnesota would have small counts in cells for those counties with small populations and few minority residents Suppression of those small counts are be necessary to protect the confidentiality of the individual
Page vii
Data by provider Tables 11 and 12 are presented for individual clinics that have been publicly identified as abortion providers but aggregated into a single group for independently reporting physicians Table 12 presents data on individual physicians with no small-number suppression as the law requires counts by physician by month Physicians are simply identified as Physician A Physician B etc to protect confidentiality Please note that the identifiers are arbitrarily assigned to those physicians who reported in a given calendar year Thus Physician X in a prior yearrsquos report may not be the same individual as Physician X in this report Data presented in frequency tables for the state as a whole have no small-number data suppressed Likewise Table 6 CountryState Residence of Woman contains sufficiently large groups to confound identification of an individual Table 7 County of Residence for Women Residing in Minnesota is the only table for which counts of zero to five are suppressed Some of the counties have a small population of females of childbearing age andor a small number of physicians who may be qualified to provide abortion services and thus though unlikely it could be possible for a provider or patient to be identified
Page viii
Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Technical Notes
Technical Notes
Data included in this report are submitted to the Minnesota Department of Health by facilities and physicians who perform abortions in Minnesota The Report of Induced Abortion (see Appendix Figure 1) may be submitted by a facilityclinic on behalf of physicians who practice therein or physicians may submit reports independently A number of data items on the report form are specifically required by Minnesota Statutes These items include medical specialty of the physician performing the abortion patient age date of the abortion clinical estimate of gestation number of previous spontaneous and induced abortions type of abortion procedure intra-operative complications (post-operative complications are collected using the Report of Complication(s) from Induced Abortion) method of disposal of fetal remains type of payment health coverage type and reason for the abortion The items type of admission patient residence date of last menses and contraceptive use and method were included to provide continuity with previous abortion report forms Marital status Hispanic origin race education and previous live births correspond to items on the Minnesota Medical Supplement to the Certificate of Live Birth and thus allow for statistical comparison with birth data and the calculation of pregnancy rates
Report forms submitted with incomplete data are required by law to be returned to the clinicfacility or independently reporting physician for correction Overall compliance and cooperation in completing the forms is excellent however some data remain unreported In some cases this is due to a facility being unable to locate the record in question and in other instances due to a patientrsquos refusal to provide the data Continuing efforts are being made to further improve reporting compliance completeness and timeliness
Due to the sensitivity of abortion data there are concerns about revealing an individualrsquos identity whether patient or provider from data presented in this publication Minnesota Statutes section 1454134 states ldquoThe commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included on the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which an individual having performed or having had an abortion may be identified using epidemiologic principlesrdquo
Data generally are suppressed when there are such small numbers of two or more variables that it would be difficult to protect the confidentiality of individuals For instance age groups tallied for only a single town in Minnesota would most likely have small counts in some of the age groups Likewise a table of age group by race for each county in Minnesota would have small counts in cells for those counties with small populations and few minority residents Suppression of those small counts are be necessary to protect the confidentiality of the individual
Page vii
Data by provider Tables 11 and 12 are presented for individual clinics that have been publicly identified as abortion providers but aggregated into a single group for independently reporting physicians Table 12 presents data on individual physicians with no small-number suppression as the law requires counts by physician by month Physicians are simply identified as Physician A Physician B etc to protect confidentiality Please note that the identifiers are arbitrarily assigned to those physicians who reported in a given calendar year Thus Physician X in a prior yearrsquos report may not be the same individual as Physician X in this report Data presented in frequency tables for the state as a whole have no small-number data suppressed Likewise Table 6 CountryState Residence of Woman contains sufficiently large groups to confound identification of an individual Table 7 County of Residence for Women Residing in Minnesota is the only table for which counts of zero to five are suppressed Some of the counties have a small population of females of childbearing age andor a small number of physicians who may be qualified to provide abortion services and thus though unlikely it could be possible for a provider or patient to be identified
Page viii
Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Technical Notes
Data included in this report are submitted to the Minnesota Department of Health by facilities and physicians who perform abortions in Minnesota The Report of Induced Abortion (see Appendix Figure 1) may be submitted by a facilityclinic on behalf of physicians who practice therein or physicians may submit reports independently A number of data items on the report form are specifically required by Minnesota Statutes These items include medical specialty of the physician performing the abortion patient age date of the abortion clinical estimate of gestation number of previous spontaneous and induced abortions type of abortion procedure intra-operative complications (post-operative complications are collected using the Report of Complication(s) from Induced Abortion) method of disposal of fetal remains type of payment health coverage type and reason for the abortion The items type of admission patient residence date of last menses and contraceptive use and method were included to provide continuity with previous abortion report forms Marital status Hispanic origin race education and previous live births correspond to items on the Minnesota Medical Supplement to the Certificate of Live Birth and thus allow for statistical comparison with birth data and the calculation of pregnancy rates
Report forms submitted with incomplete data are required by law to be returned to the clinicfacility or independently reporting physician for correction Overall compliance and cooperation in completing the forms is excellent however some data remain unreported In some cases this is due to a facility being unable to locate the record in question and in other instances due to a patientrsquos refusal to provide the data Continuing efforts are being made to further improve reporting compliance completeness and timeliness
Due to the sensitivity of abortion data there are concerns about revealing an individualrsquos identity whether patient or provider from data presented in this publication Minnesota Statutes section 1454134 states ldquoThe commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included on the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which an individual having performed or having had an abortion may be identified using epidemiologic principlesrdquo
Data generally are suppressed when there are such small numbers of two or more variables that it would be difficult to protect the confidentiality of individuals For instance age groups tallied for only a single town in Minnesota would most likely have small counts in some of the age groups Likewise a table of age group by race for each county in Minnesota would have small counts in cells for those counties with small populations and few minority residents Suppression of those small counts are be necessary to protect the confidentiality of the individual
Page vii
Data by provider Tables 11 and 12 are presented for individual clinics that have been publicly identified as abortion providers but aggregated into a single group for independently reporting physicians Table 12 presents data on individual physicians with no small-number suppression as the law requires counts by physician by month Physicians are simply identified as Physician A Physician B etc to protect confidentiality Please note that the identifiers are arbitrarily assigned to those physicians who reported in a given calendar year Thus Physician X in a prior yearrsquos report may not be the same individual as Physician X in this report Data presented in frequency tables for the state as a whole have no small-number data suppressed Likewise Table 6 CountryState Residence of Woman contains sufficiently large groups to confound identification of an individual Table 7 County of Residence for Women Residing in Minnesota is the only table for which counts of zero to five are suppressed Some of the counties have a small population of females of childbearing age andor a small number of physicians who may be qualified to provide abortion services and thus though unlikely it could be possible for a provider or patient to be identified
Page viii
Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Data by provider Tables 11 and 12 are presented for individual clinics that have been publicly identified as abortion providers but aggregated into a single group for independently reporting physicians Table 12 presents data on individual physicians with no small-number suppression as the law requires counts by physician by month Physicians are simply identified as Physician A Physician B etc to protect confidentiality Please note that the identifiers are arbitrarily assigned to those physicians who reported in a given calendar year Thus Physician X in a prior yearrsquos report may not be the same individual as Physician X in this report Data presented in frequency tables for the state as a whole have no small-number data suppressed Likewise Table 6 CountryState Residence of Woman contains sufficiently large groups to confound identification of an individual Table 7 County of Residence for Women Residing in Minnesota is the only table for which counts of zero to five are suppressed Some of the counties have a small population of females of childbearing age andor a small number of physicians who may be qualified to provide abortion services and thus though unlikely it could be possible for a provider or patient to be identified
Page viii
Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Tables
3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

3
Table 11 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016
Womens Health Center 35 23 36 36 30 20 27 28 33 37 27 30 362
Robbinsdale Clinic 89 81 107 80 67 64 76 56 78 65 75 91 929
Dr Mildred Hansen Clinic 65 58 83 56 38 36 46 40 45 33 47 63 610
Planned Parenthood of Minnesota 470 439 470 479 495 497 477 524 442 439 432 465 5629
Whole Womans Health LLC 211 200 248 222 182 192 191 213 198 150 168 190 2365
Independent Physicians1 4 8 6 9 5 4 3 3 5 5 3 3 58
Total Minnesota Occurrence 874 809 950 882 817 813 820 864 801 729 752 842 9953
1This represents 10 reporting physicians small clinics and hospitals Counts include only St Paul location No abortions were performed at the Rochester location in 2016
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
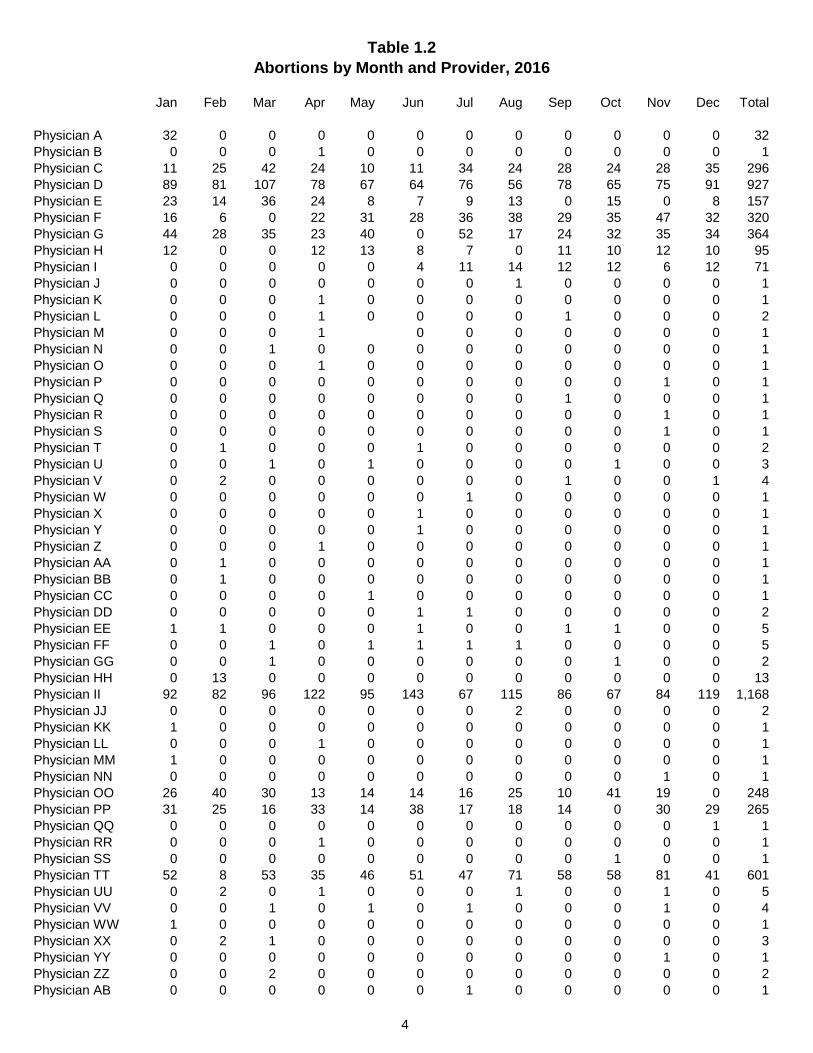
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician A 32 0 0 0 0 0 0 0 0 0 0 0 32 Physician B 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician C 11 25 42 24 10 11 34 24 28 24 28 35 296 Physician D 89 81 107 78 67 64 76 56 78 65 75 91 927 Physician E 23 14 36 24 8 7 9 13 0 15 0 8 157 Physician F 16 6 0 22 31 28 36 38 29 35 47 32 320 Physician G 44 28 35 23 40 0 52 17 24 32 35 34 364 Physician H 12 0 0 12 13 8 7 0 11 10 12 10 95 Physician I 0 0 0 0 0 4 11 14 12 12 6 12 71 Physician J 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician K 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician L 0 0 0 1 0 0 0 0 1 0 0 0 2 Physician M 0 0 0 1 0 0 0 0 0 0 0 1 Physician N 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician O 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician P 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician Q 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician R 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician S 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician T 0 1 0 0 0 1 0 0 0 0 0 0 2 Physician U 0 0 1 0 1 0 0 0 0 1 0 0 3 Physician V 0 2 0 0 0 0 0 0 1 0 0 1 4 Physician W 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician X 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Y 0 0 0 0 0 1 0 0 0 0 0 0 1 Physician Z 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AA 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BB 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician CC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician DD 0 0 0 0 0 1 1 0 0 0 0 0 2 Physician EE 1 1 0 0 0 1 0 0 1 1 0 0 5 Physician FF 0 0 1 0 1 1 1 1 0 0 0 0 5 Physician GG 0 0 1 0 0 0 0 0 0 1 0 0 2 Physician HH 0 13 0 0 0 0 0 0 0 0 0 0 13 Physician II 92 82 96 122 95 143 67 115 86 67 84 119 1168 Physician JJ 0 0 0 0 0 0 0 2 0 0 0 0 2 Physician KK 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician LL 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician MM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician NN 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician OO 26 40 30 13 14 14 16 25 10 41 19 0 248 Physician PP 31 25 16 33 14 38 17 18 14 0 30 29 265 Physician QQ 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician RR 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician SS 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician TT 52 8 53 35 46 51 47 71 58 58 81 41 601 Physician UU 0 2 0 1 0 0 0 1 0 0 1 0 5 Physician VV 0 0 1 0 1 0 1 0 0 0 1 0 4 Physician WW 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician XX 0 2 1 0 0 0 0 0 0 0 0 0 3 Physician YY 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician ZZ 0 0 2 0 0 0 0 0 0 0 0 0 2 Physician AB 0 0 0 0 0 0 1 0 0 0 0 0 1
4
Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 12 Abortions by Month and Provider 2016
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Physician AC 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician AD 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AE 0 9 0 0 9 0 0 0 10 0 0 0 28 Physician AF 26 35 4 19 26 22 15 18 22 9 0 9 205 Physician AG 14 25 20 15 15 13 1 8 13 0 0 0 124 Physician AH 41 59 111 99 59 71 55 14 35 46 33 33 656 Physician AI 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician AJ 0 0 3 0 0 0 0 0 0 0 0 1 4 Physician AK 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician AL 85 45 16 37 65 39 61 45 63 49 36 58 599 Physician AM 1 0 0 0 0 0 0 0 0 0 0 0 1 Physician AN 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician AO 0 0 1 0 0 0 0 1 0 0 0 0 2 Physician AP 1 0 0 0 0 0 0 0 0 0 0 1 2 Physician AQ 0 0 0 0 0 0 0 0 0 0 1 0 1 Physician AR 1 0 1 0 0 0 0 0 0 0 0 0 2 Physician AS 0 0 0 0 0 0 0 1 0 0 0 0 1 Physician AT 27 37 45 35 34 31 11 68 22 24 36 22 392 Physician AU 12 0 0 12 11 14 7 3 0 0 10 13 82 Physician AV 0 0 28 14 30 15 21 33 17 32 31 16 237 Physician AW 0 0 0 0 0 0 0 0 0 1 0 0 1 Physician AX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician AY 49 39 35 31 30 28 40 30 49 18 16 27 392 Physician AZ 40 8 20 17 12 12 11 8 4 9 19 28 188 Physician BC 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BD 29 28 32 26 27 24 30 25 18 25 39 22 325 Physician BE 1 0 0 0 0 0 0 1 0 0 0 0 2 Physician BF 10 18 19 17 21 18 24 40 36 22 15 36 276 Physician BG 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BH 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BI 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BJ 0 0 1 0 0 0 0 0 0 0 0 0 1 Physician BK 13 22 42 69 29 51 46 36 23 34 11 11 387 Physician BL 0 11 0 0 0 18 0 24 12 12 0 0 77 Physician BM 53 93 81 69 79 74 68 57 58 28 10 73 743 Physician BN 26 35 37 15 25 0 15 18 28 25 12 17 253 Physician BO 12 11 27 8 0 9 37 36 25 29 58 45 297 Physician BP 1 0 0 0 0 0 0 2 8 1 1 4 17 Physician BQ 0 0 0 0 0 0 0 0 1 0 0 0 1 Physician BR 0 0 0 0 0 0 1 0 0 0 0 0 1 Physician BS 0 0 1 1 0 0 0 0 0 1 0 0 3 Physician BT 0 0 0 0 0 0 0 0 0 0 0 11 11 Physician BU 0 1 0 0 0 0 0 0 0 0 0 0 1 Physician BV 0 0 1 0 0 0 0 0 1 0 0 0 2 Physician BW 0 0 0 0 0 0 0 0 0 0 0 1 1 Physician BX 0 0 0 1 0 0 0 0 0 0 0 0 1 Physician BY 0 0 0 0 1 0 0 0 0 0 0 0 1 Physician BZ 0 0 0 1 0 0 0 0 0 0 0 0 1
Total MN 874 809 950 882 817 813 820 864 801 729 752 842 9953
5
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
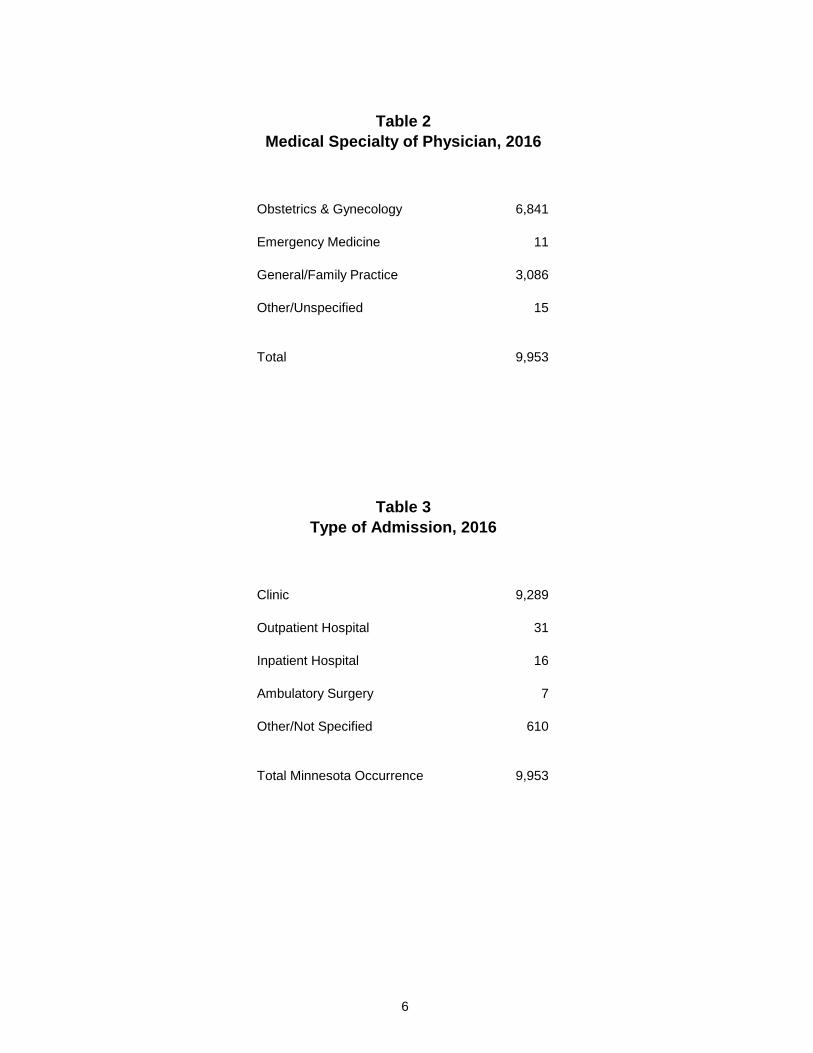
Table 2 Medical Specialty of Physician 2016
Obstetrics amp Gynecology 6841
Emergency Medicine 11
GeneralFamily Practice 3086
OtherUnspecified 15
Total 9953
Table 3 Type of Admission 2016
Clinic 9289
Outpatient Hospital 31
Inpatient Hospital 16
Ambulatory Surgery 7
OtherNot Specified 610
Total Minnesota Occurrence 9953
6
Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 4 Age of Woman 2016
Occurring in Minnesota Minnesota Residents
lt 15 Years 28 26
15 - 17 Years 263 238
18 - 19 Years 607 550
20 - 24 Years 2845 2562
25 - 29 Years 2800 2559
30 - 34 Years 1974 1814
35 - 39 Years 1090 1001
40 Years amp Over 346 303
Not Reported 0 0
Total 9953 9053
Table 5 Marital Status 2016
Occurring in Minnesota Minnesota Residents
Married 1386 1243
Not Married 7996 7280
Not Reported 571 530
Total 9953 9053
7
Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 6 CountryState of Residence 2016
Minnesota 9053
Other States Iowa 39 Michigan 17 North Dakota 67 South Dakota 76 Wisconsin 638 Other States 61
Canada 1
Other Foreign Countries 0
Not Reported 1
Total MN Occurrence 9953
8
Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 7 County of Residence for Women Residing in Minnesota 2016
State Total Aitkin Anoka Becker Beltrami Benton Big Stone Blue Earth Brown Carlton Carver Cass Chippewa Chisago Clay Clearwater Cook Cottonwood Crow Wing Dakota Dodge Douglas Faribault Fillmore Freeborn Goodhue Grant Hennepin Houston Hubbard Isanti Itasca Jackson Kanabec Kandiyohi Kittson Koochiching Lac Qui Parle Lake Lake of the Woods Le Sueur Lincoln Lyon McLeod Mahnomen
9053 11
553
36 68
101 17 36 91 21 9
45 10
7
71 719 18 19 12 20 29 42
3350
10 6
47 29 8
10 36
8
11
22
18 31
Marshall Martin 15 Meeker 9 Mille Lacs 36 Morrison 27 Mower 50 Murray Nicollet 45 Nobles 7 Norman Olmsted 217 Otter Tail 12 Pennington Pine 27 Pipestone Polk Pope Ramsey 1624 Red Lake Redwood 9 Renville 10 Rice 67 Rock Roseau Saint Louis 259 Scott 165 Sherburne 91 Sibley 14 Stearns 197 Steele 36 Stevens Swift Todd 9 Traverse Wabasha 20 Wadena Waseca 18 Washington 331 Watonwan 6 Wilkin Winona 46 Wright 122 Yellow Medicine 5 Unknown County 0
Counts of 0 to 5 are indicated by an asterisk
9
Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 8 Hispanic Origin of Woman 2016
Occurring in Minnesota
Minnesota Residents
Non-Hispanic
Hispanic
Not Reported
8887
700
366
8047
665
341
Total 9953 9053
Table 9 Race of Woman 2016
Occurring in Minnesota
Minnesota Residents
White
Black
American Indian
5063
2623
212
4339
2581
186
Asian 735 695
Other
Not Reported
1162
158
1102
150
Total 9953 9053
10
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
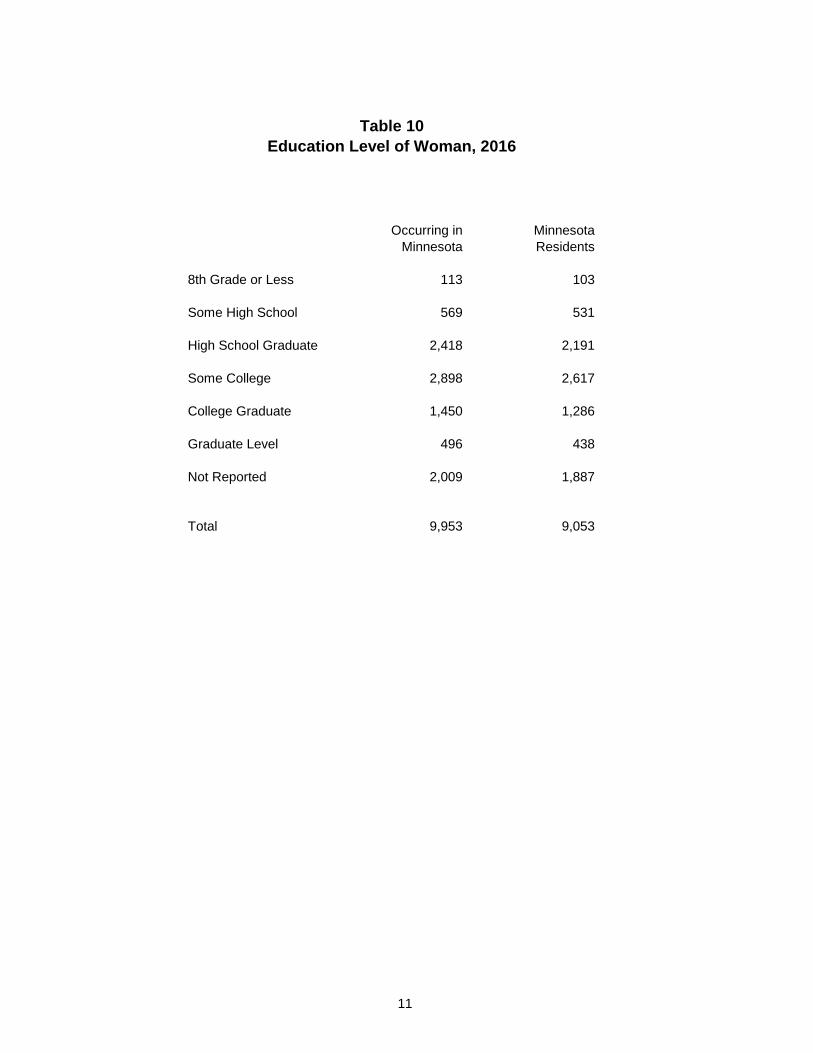
Table 10 Education Level of Woman 2016
Occurring in Minnesota Minnesota Residents
8th Grade or Less 113 103
Some High School 569 531
High School Graduate 2418 2191
Some College 2898 2617
College Graduate 1450 1286
Graduate Level 496 438
Not Reported 2009 1887
Total 9953 9053
11
Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 11 Clinical Estimate of Fetal Gestational Age 2016
Occurring in Minnesota Minnesota Residents
lt9 weeks 6703 6153
9 - 10 weeks 1418 1299
11 - 12 weeks 630 560
13 - 15 weeks 584 519
16 - 20 weeks 478 415
21 - 24 weeks 139 106
25 - 30 weeks 1 1
31 - 36 weeks 0 0
37 weeks amp over 0 0
Not Reported 0 0
Total 9953 9053
12
Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 11a Clinical Estimate of Fetal Gestational Age 2016
13
First Trimester Second Trimester Third Trimester Estimated Occurring in Minnesota Estimated Occurring in Minnesota Estimated Occurring in Minnesota
Week Minnesota Residents Week Minnesota Residents Week Minnesota Residents
lt3 4 3 14 202 180 28 0 0 3 6 5 15 169 154 29 0 0 4 175 159 16 133 120 30 0 0 5 1461 1349 17 94 85 31 0 0 6 2208 2011 18 87 76 32 0 0 7 1591 1455 19 80 64 33 0 0 8 1258 1171 20 84 70 34 0 0 9 868 799 21 77 61 35 0 0 10 550 500 22 39 30 36 0 0 11 359 327 23 22 15 37 0 0 12 271 233 24 1 0 38 0 0 13 213 185 25 0 0 39 0 0
26 1 1 40+ 0 0 27 0 0
Trimester Total 8964 8197 989 856 0 0
Total Induced Abortions Occurring in Minnesota 9953 Minnesota Residents 9053
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
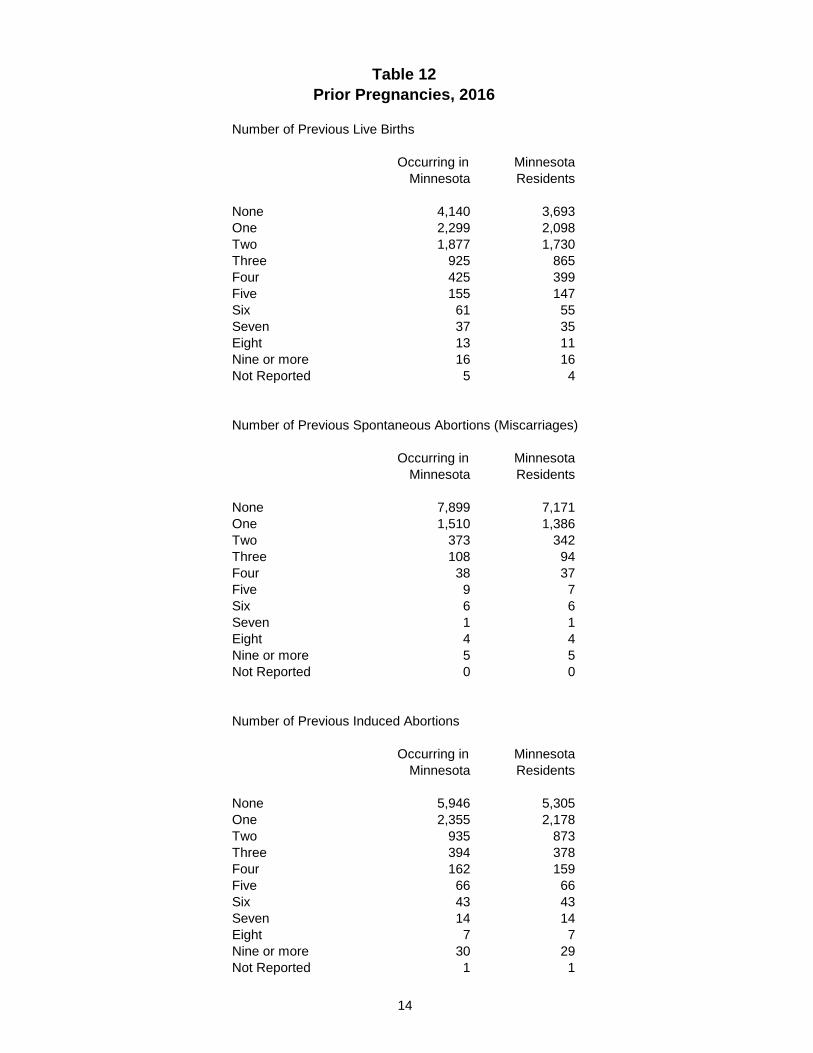
Table 12 Prior Pregnancies 2016
Number of Previous Live Births
Occurring in Minnesota Minnesota Residents
None 4140 3693 One 2299 2098 Two 1877 1730 Three 925 865 Four 425 399 Five 155 147 Six 61 55 Seven 37 35 Eight 13 11 Nine or more 16 16 Not Reported 5 4
Number of Previous Spontaneous Abortions (Miscarriages)
Occurring in Minnesota Minnesota Residents
None 7899 7171 One 1510 1386 Two 373 342 Three 108 94 Four 38 37 Five 9 7 Six 6 6 Seven 1 1 Eight 4 4 Nine or more 5 5 Not Reported 0 0
Number of Previous Induced Abortions
Occurring in Minnesota Minnesota Residents
None 5946 5305 One 2355 2178 Two 935 873 Three 394 378 Four 162 159 Five 66 66 Six 43 43 Seven 14 14 Eight 7 7 Nine or more 30 29 Not Reported 1 1
14
Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 13 Contraceptive Use and Method 2016
Occurring in Minnesota Minnesota Residents
Woman did not provide information 1863 1689
Woman did not know whether she used 202 184 contraception
Woman has never used contraceptives 653 611
Woman has used contraceptives but not 5606 5116 at the time of conception
Woman used contraceptives at the time 1629 1453 of conception
Method Used Condoms 523 464 Condoms amp Spermicide 9 9 Spermicide Alone 11 10 Sterilization - Male 11 11 Sterilization - Female 4 4 Injectable (Depo-Provera) 51 47 IUD 65 59 Mini Pills 84 66 Combination Pills 488 440 Diaphragm amp Spermicide 3 3 Diaphragm Alone 1 1 Cervical Cap 0 0 RhythmNatural Family Planning 15 11 Fertility Awareness 11 10 Withdrawal 53 50 Other 289 257 Method Not Reported 11 11
The accuracy of reporting Use of Contraceptives at the Time of Conception is dependent upon self-reporting by the woman Thus these data should not be interpreted as an indication of the effectiveness of any particular method of birth control
15
Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 14 Abortion Procedure 2016
Occurring in Minnesota Minnesota Residents
Suction Currettage 5571 5114
Medical (non-surgical) 3522 3198
Dilation amp Evacuation (DampE) 825 711
Intra-Uterine Instillation 4 4
Hysterectomyotomy 2 2
Sharp Curettage (DampC) 18 15
Induction of Labor (Pitocin etc) 10 8
Intact Dilation amp Extraction (DampX) 0 0
Other Dilation amp Extraction (DampX) 0 0
Other Method 1 1
Total 9953 9053
16
Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 15 Method of Disposal of Fetal Remains 2016
Occurring in Minnesota
Minnesota Residents
Cremation
Burial
4315
13
3894
12
Not Reported 5625 5147
Total 9953 9053
Method of Disposal of Fetal Remains is required to be reported only for those fetuses having reached the developmental stage outlined in Minnesota Statute 1451621 subd 2 Thus not all reports contained this information
17
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
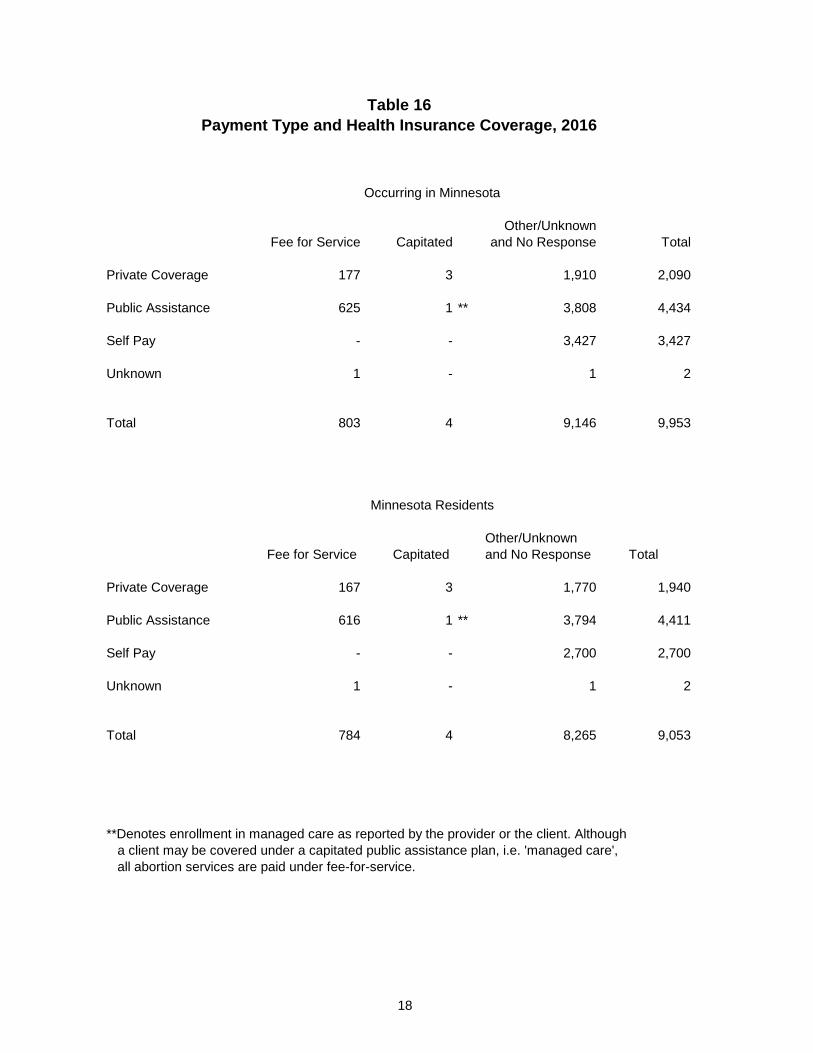
Table 16 Payment Type and Health Insurance Coverage 2016
Occurring in Minnesota
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 177 3 1910 2090
Public Assistance 625 1 3808 4434
Self Pay - - 3427 3427
Unknown 1 - 1 2
Total 803 4 9146 9953
Minnesota Residents
OtherUnknown Fee for Service Capitated and No Response Total
Private Coverage 167 3 1770 1940
Public Assistance 616 1 3794 4411
Self Pay - - 2700 2700
Unknown 1 - 1 2
Total 784 4 8265 9053
Denotes enrollment in managed care as reported by the provider or the client Although a client may be covered under a capitated public assistance plan ie managed care all abortion services are paid under fee-for-service
18
Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 17 Reason for Abortion 2016
Occurring in Minnesota Minnesota Residents
Pregnancy was a result of rape 77 64
Pregnancy was a result of incest 8 7
Economic reasons 2865 2572
Does not want children at this time 6933 6306
Emotional health is at stake 1014 910
Physical Health is at stake 666 610
Continued pregnancy will cause 36 32 impairment of major bodily function
Pregnancy resulted in fetal anomalies 174 136
Unknown or the woman refused 1596 1466 to answer
Other stated reason 364 335
Note No totals are given because a woman may have given more than one response
See Table 17a
19
Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 17a Other Stated Reason for Abortion 2016
Physical or mental health issues and concerns 63
Education career and employment issues 10
Not ready or prepared for a child or more children at this time or family already completed 84
Relationship issues including abuse separation divorce and extra-marital affairs 36
Other miscellaneous responses 66
Other Reason was indicated but not specified 116
Total 375
Note that these categories were changed from those of previous years beginning with the 2015 data year The categories previously used were no longer representative of the typical responses given
Total is greater than Other Stated Reason total on Table 17 because some women stated more than one other reason
20
Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 18 Intraoperative Complications 2016
Occurring in Minnesota Minnesota Residents
No Complications 9889 8994
Cervical laceration requiring suture 20 17 or repair
Heavy bleedinghemorrhage with 2 2 estimated blood loss in excess of 500cc
Uterine perforation 5 4
Other complication 35 34
Not Reported 2 2
Total 9953 9053
Complication occurring at the time of the abortion procedure
21
Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 19 Postoperative Complications 2016
reported on Report of Complication from Induced Abortion form
Cervical laceration requiring suture or repair 0
Heavy bleedinghemorrhage with estimated blood loss in excess of 500cc 0
Uterine perforation 3
Infection requiring inpatient treatment 4
Heavy bleedinganemia requiring transfusion 1
Failed termination of pregnancy (continued viable pregnancy) 18
Incomplete termination of pregnancy (retained products of conception requiring re-evacuation) 54
Other complication 7
Complication not specified 2
Total Reported Complications 89 1
183 Report of Complication(s) from Induced Abortion forms were received
Neither location where the abortion was performed nor residence of patient is collected on the Report of Complication(s) from Induced Abortion Therefore these numbers cannot be directly correlated with counts of induced abortions in an attempt to seek a ratio of complications per procedure
22
Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 20 Induced Abortions by Gestational Age
Performed Out of State and Paid for with State Funds1
reported by the Minnesota Department of Human Services 20152
lt9 weeks 0
9 - 10 weeks 0
11 - 12 weeks 0
13 - 15 weeks 0
16 - 20 weeks 0
21 - 24 weeks 0
25 - 30 weeks 0
31 - 36 weeks 0
37 weeks amp over 0
Unknown 124
Total Occurrence 124
Total state funds used to pay for out of state abortion procedures including incidental expenses $2282459
1All procedures occurred within the local trade area that is the geographic area surrounding the persons residence including portions of states other than Minnesota which is commonly used by other persons in the same area to obtain similar necessary goods and services
2Gestation weeks were not reported on claims data received by DHS for 2015
23
Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 21 Total and Resident Induced Abortions
1975 1980 - 2016
Occurring in Minnesota
Minnesota Residents
Resident Percent
Resident Rate1
1975 10565 8924 845 103 1980 19028 16490 867 172 1981 18304 15821 864 163 1982 17758 15559 876 158 1983 16428 14514 883 147 1984 17314 15556 898 157 1985 17686 16002 905 161 1986 17383 15716 904 158 1987 17653 15746 892 157 1988 17975 16124 897 158 1989 17398 15506 891 151 1990 17156 15280 891 149 1991 16178 14441 893 139 1992 15546 13846 891 131 1993 14348 12955 903 121 1994 14027 12702 906 118 1995 14017 12715 907 121 1996 14193 12876 907 121 1997 14224 12997 914 124 1998 14422 13050 905 124 1999 14342 13037 909 124 2000 14477 13208 912 122 2001 14833 13448 907 123 2002 14239 12953 910 118 2003 14174 12995 917 119 2004 13788 12753 925 116 2005 13365 12306 921 113 2006 14065 12948 921 121 2007 13843 12770 922 121 2008 12948 11896 919 113 2009 12388 11391 920 109 2010 11505 10570 919 101 2011 11071 10150 917 97 2012 10701 9758 912 93 2013 9903 9030 912 86 2014 10123 9180 907 87 2015 9861 8898 902 84 2016 9953 9053 910 86 2
1Rate per 1000 female population ages 15 through 44 22016 population estimates not available at time of publication 2015 count was used
24
Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 22 Abortions per 100 Live Births by Selected Patient Characteristics
Minnesota Residents 1980 1990 2000 2010 2013-2016
1980 1990 2000 2010 2013 2014 2015 3 2016
Total Resident Abortions 243 225 196 155 142 131 127 130
Age Group lt15 2311 681 713 894 806 1304 727 1733
15-17 Years 802 1 692 402 373 318 332 345 475 18-19 Years 575 395 305 303 299 306 327 20-24 Years 269 356 318 280 246 244 241 249 25-29 Years 117 141 156 120 110 117 114 120 30-34 Years 108 112 105 87 75 73 74 77 35-39 Years 198 183 137 115 97 103 104 97
40 Years amp Over 419 359 282 201 182 196 164 157
Race of Patient White 225 209 145 118 88 87 87 88
African American na 2 na 2 603 401 298 287 291 311 American Indian na 2 na 2 263 206 128 175 152 150
Asian na 2 na 2 348 168 121 125 130 125 All Other 451 334 -shy -shy -shy -shy -shy -shyHispanic na na 184 129 109 124 124 137
Marital Status Married 35 42 40 34 26 27 28 26
Not Married 1593 484 569 389 308 315 308 326
Unknowns are not included in ratios 1Ratio is for age 15-19 Separate data for 15-17 and 18-19 is not available for 1980 2RaceEthnicity data was collected differently prior to 1999 thus ratios are not available for individual categories other than White 3Figures have been updated from those published in the 2015 table with finalized 2015 birth data
25
26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

26
Table 23 Selected Statistics by Age Group 2016
Minnesota Residents
Total Abortions
Total
9053
lt15 Years
26
15 - 17 Years
238
18 - 19 Years
550
20 - 24 Years
2562
25 - 29 Years
2559
30 - 34 Years
1814
35 - 39 Years
1001
40+ Years
303
Unkwn Age
0
Marital Status Married Not Married Unknown
1243 7280
530
0 25 1
1 224 13
6 509 35
99 2322
141
274 2139
146
439 1247
128
310 639 52
114 175 14
0 0 0
RaceEthnicity White
African American American Indian Asian Hispanic
4339
2581 186 695 665
8
9 1 1 4
112
59 7
17 29
253
152 10 29 58
1184
792 60
137 239
1178
811 56
158 146
881
492 32
203 100
557
207 15
103 72
166
59 5
47 17
0
0 0 0 0
Gestation Estimate First Trimester Second Trimester Third Trimester Unknown
8197
856 0 0
19 7 0 0
200 38 0 0
477 73 0 0
2341 221
0 0
2313 246
0 0
1662 152
0 0
906 95
0 0
279 24
0 0
0 0 0 0
Persons of Hispanic origin are included in the race counts above 1st Trimester 0-13 weeks 2nd Trimester 14-27 weeks 3rd Trimester 28-40+ weeks
27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

27
Table 24 Contraceptive Use by Age Group and Marital Status 2016
Minnesota Residents
All Induced Abortions Women with at Least One Prior Induced Abortion Never Past Use Was Never Past Use Was
Total Used Not Now Using Unknown Total Used Not Now Using Unknown
Total Abortions 9053 611 5116 1453 1873 3748 160 2231 620 737
Age Group lt15 Years 26 11 5 3 7 1 1 0 0 0 15-17 Years 238 51 104 31 52 16 2 10 2 2 18-19 Years 550 75 292 77 106 91 10 46 15 20
20-24 Years 2562 187 1448 398 529 800 36 474 140 150 25-29 Years 2559 129 1473 426 531 1214 43 735 190 246 30-34 Years 1814 95 1056 296 367 905 39 551 151 164 35-39 Years 1001 48 576 163 214 551 20 325 87 119 40+ Years 303 15 162 59 67 170 9 90 35 36 Unknown Age 0 0 0 0 0 0 0 0 0 0
Marital Status Married 1243 93 660 214 276 463 20 259 86 98 Not Married 7280 473 4212 1161 1434 3088 125 1885 502 576 Unknown 530 45 244 78 163 197 15 87 32 63
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
Informed Consent
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2016
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 9933 1465 11398
In Person 113 28 141
Total Contacts 10046 1493 11539
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 1
Medical Risks Information section was left blank 45
Total reports received 11585
31
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2016
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 31 9408 36 1361 10836
In Person 43 32 615 17 707
Total Contacts 74 9440 651 1378 11543
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 32
Total reports received 11585
32
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2016
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 276 25 17 318
Patient did not obtain printed copies 8955 747 882 10584
Total 9231 772 899 10902
Patient Access to Printed Materials section was left blank 683
Total reports received 11585
33
Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Born Alive Infants Protection Act
Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Born Alive Infants Protection Act Report
The 2015 Minnesota Legislature enacted the ldquoBorn Alive Infants Protection Actrdquo (section 145423) recognizing a born alive infant resulting from an induced abortion as a human person (section 145423 subdivision 1) and requiring that ldquoreasonable measures consistent with good medical practice shall be taken by the responsible medical personnel to preserve the life and health of the born alive infantrdquo (section 145423 subdivision 5) As part of this act the abortion reporting requirements were modified to include the following information
bull Whether the abortion resulted in a born alive infant as defined by section 145423 subdivision 4 bull What medical actions were taken to preserve the life of the infant bull Whether the infant survived bull The status if known of a surviving infant
Reporting was required beginning July 1 2015 The text of the amended sections can be found in the appendix
For the calendar year of January 1 2016 through December 31 2016 five abortion procedures resulting in a born-alive infant were reported
bull In one instance residual transient cardiac contractions were briefly present No measures were taken to prolong these transient contractions and the infant did not survive
bull In two instances the infants had been diagnosed with lethal fetal anomalies No efforts were made to preserve the lives of these infants and neither survived
bull In two instances comfort care measures were provided as planned and neither infant survived
37
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
Appendix
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
Minnesota Statutes 2014 section 1454131 subdivision 1 is amended to read
Subdivision 1 Forms (a) Within 90 days of July 1 1998 the commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached to the form A physician or facility performing an abortion shall obtain a form from the commissioner
(a) The form shall require the following information
(1) the number of abortions performed by the physician in the previous calendar year reported by month
(2) the method used for each abortion
(3) the approximate gestational age expressed in one of the following increments
(i) less than nine weeks
(ii) nine to ten weeks
(iii) 11 to 12 weeks
(iv) 13 to 15 weeks
(v) 16 to 20 weeks
(vi) 21 to 24 weeks
(vii) 25 to 30 weeks
(viii) 31 to 36 weeks or
(ix) 37 weeks to term
(4) the age of the woman at the time the abortion wasperformed
(5) the specific reason for the abortion including but not limited to the following
(i) the pregnancy was a result of rape
(ii) the pregnancy was a result of incest
(iii) economic reasons
(iv) the woman does not want children at this time
(v) the womans emotional health is at stake
(vi) the womans physical health is at stake
(vii) the woman will suffer substantial and irreversible impairment of a major bodily function if the pregnancy continues
41
(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

(viii) the pregnancy resulted in fetal anomalies or
(ix) unknown or the woman refused to answer
(6) the number of prior induced abortions
(7) the number of prior spontaneous abortions
(8) whether the abortion was paid for by
(i) private coverage
(ii) public assistance health coverage or
(iii) self-pay
(9) whether coverage was under
(i) a fee-for-service plan
(ii) a capitated private plan or
(iii) other
(10) complications if any for each abortion and for the aftermath of each abortion Space for a description of any complications shall be available on the form
(11) the medical specialty of the physician performing theabortion
(12) whether the abortion resulted in a born alive infant as defined in section 145423 subdivision 4 and
(i) any medical actions taken to preserve the life of the born aliveinfant
(ii) whether the born alive infant survived and
(iii) the status of the born alive infant should the infant survive ifknown
Sec 44 Minnesota Statutes 2014 section 145423 is amended to read
145423 ABORTION LIVE BIRTHS
Subdivision 1 Recognition medical care A born alive infant as a result of an abortion shall be fully recognized as a human person and accorded immediate protection under the law All reasonable measures consistent with good medical practice including the compilation of appropriate medical records shall be taken by the responsible medical personnel to preserve the life and health of the born alive infant
Subd 2 Physician required When an abortion is performed after the twentieth week of pregnancy a physician other than the physician performing the abortion shall be immediately accessible to take all reasonable measures consistent with good medical practice including the compilation of appropriate medical records to preserve the life and health of any
42
born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

born alive infant that is the result of the abortion
Subd 3 Death If a born alive infant described in subdivision 1 dies after birth the body shall be disposed of in accordance with the provisions of section 1451621
Subd 4 Definition of born alive infant
(a) In determining the meaning of any Minnesota statute or of any ruling regulation or interpretation of the various administrative bureaus and agencies of Minnesota the words person human being child and individual shall include every infant member of the species Homo sapiens who is born alive at any stage of development
(b) As used in this section the term born alive with respect to a member of the species Homo sapiens means the complete expulsion or extraction from his or her mother of that member at any stage of development who after such expulsion or extraction breathes or has a beating heart pulsation of the umbilical cord or definite movement of voluntary muscles regardless of whether the umbilical cord has been cut and regardless of whether the expulsion or extraction occurs as a result of a natural or induced labor cesarean section or induced abortion
(c) Nothing in this section shall be construed to affirm deny expand or contract any legal status or legal right applicable to any member of the species Homo sapiens at any point prior to being born alive as defined in this section
Subd 5 Civil and disciplinary actions
(a) Any person upon whom an abortion has been performed or the parent or guardian of the mother if the mother is a minor and the abortion results in the infant having been born alive may maintain an action for death of or injury to the born alive infant against the person who performed the abortion if the death or injury was a result of simple negligence gross negligence wantonness willfulness intentional conduct or another violation of the legal standard ofcare
(b) Any responsible medical personnel that does not take all reasonable measures consistent with good medical practice to preserve the life and health of the born alive infant as required by subdivision 1 may be subject to the suspension or revocation of that persons professional license by the professional board with authority over that person Any person who has performed an abortion and against whom judgment has been rendered pursuant to paragraph (a) shall be subject to an automatic suspension of the persons professional license for at least one year and said license shall be reinstated only after the persons professional board requires compliance with this section by all board licensees
(c) Nothing in this subdivision shall be construed to hold the mother of the born alive infant criminally or civilly liable for the actions of a physician nurse or other licensed health care provider in violation of this section to which the mother did not give her consent
Subd 6 Protection of privacy in court proceedings
In every civil action brought under this section the court shall rule whether the anonymity of any female upon whom an abortion has been performed or attempted shall be preserved from public disclosure if she does not give her consent to such disclosure The court upon motion or sua sponte shall make such a ruling and upon determining that her anonymity should be preserved shall issue orders to the parties witnesses and counsel and shall direct the sealing of the record and exclusion of individuals from courtrooms or hearing rooms to the extent necessary to safeguard her identity from public disclosure Each order must be accompanied by specific written findings explaining why the anonymity of the female should be preserved from public disclosure why the order is essential to that end how the order is narrowly tailored to serve that interest and why no reasonable less restrictive alternative exists This section may not be construed to conceal the identity of the plaintiff or of witnesses from the defendant
Subd 7 Status of born alive infant
43
Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Unless the abortion is performed to save the life of the woman or fetus or unless one or both of the parents of the born alive infant agree within 30 days of the birth to accept the parental rights and responsibilities for the child the child shall be an abandoned ward of the state and the parents shall have no parental rights or obligations as if the parental rights had been terminated pursuant to section 260C301 The child shall be provided for pursuant to chapter 256J
Subd 8 Severability
If any one or more provision section subdivision sentence clause phrase or word of this section or the application of it to any person or circumstance is found to be unconstitutional it is declared to be severable and the balance of this section shall remain effective notwithstanding such unconstitutionality The legislature intends that it would have passed this section and each provision section subdivision sentence clause phrase or word regardless of the fact that any one provision section subdivision sentence clause phrase or word is declared unconstitutional
Subd 9 Short title
This act may be cited as the Born Alive Infants Protection Act
44
Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Updates to 2015 Data
Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Minnesota Statutes sections 1454134 and 1454246 require that each yearly report provide the statistics for any previous calendar year for which additional information from late or corrected reports was received adjusted to reflect these new numbers Following the publication of the report for calendar year 2015 in July of 2016 additional Report of Informed Consent Related to Induced Abortion forms were received Tables 25 26 and 27 on which these data are tabulated are included in this section of the Appendix and reflect the updated counts Tables for which the data did not change have not been republished here
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
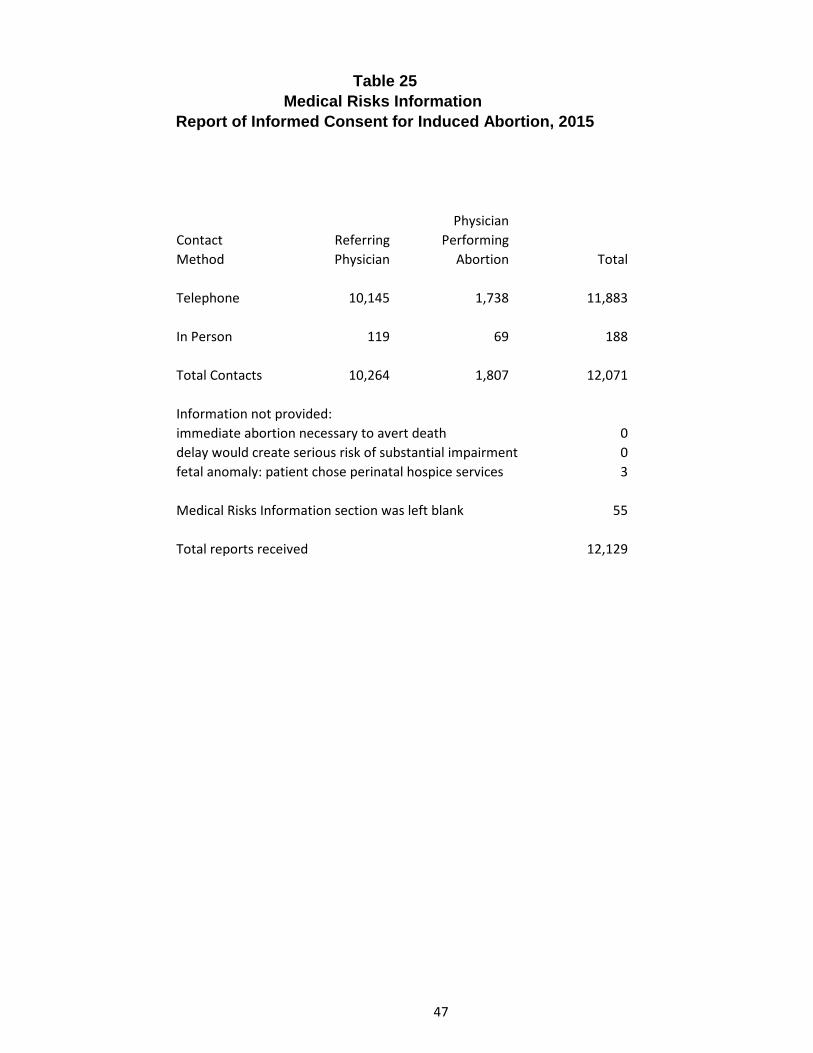
Table 25 Medical Risks Information
Report of Informed Consent for Induced Abortion 2015
Physician Contact Referring Performing Method Physician Abortion Total
Telephone 10145 1738 11883
In Person 119 69 188
Total Contacts 10264 1807 12071
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 0 fetal anomaly patient chose perinatal hospice services 3
Medical Risks Information section was left blank 55
Total reports received 12129
47
Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 26 Medical Assistance and Printed Materials Information Report of Informed Consent for Induced Abortion 2015
Agent of Agent of Physician Physician
Contact Referring Referring Performing Performing Method Physician Physician Abortion Abortion Total
Telephone 69 9102 851 1704 11726
In Person 32 54 191 16 293
Total Contacts 101 9156 1042 1720 12019
Information not provided immediate abortion necessary to avert death 0 delay would create serious risk of substantial impairment 1 fetal anomaly incompatible with life 10
Medical Assistance amp Printed Materials Information section was left blank 99
Total reports received 12129
48
Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Table 27 Patient Access to Printed Materials
Report of Informed Consent for Induced Abortion 2015
Did Not Obtained Obtain Do Not Abortion Abortion Know Total
Patient obtained printed copies 139 4 94 237
Patient did not obtain printed copies 8665 107 2036 10808
Total 8804 111 2130 11045
Patient Access to Printed Materials section was left blank 1084
Total reports received 12129
49
Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Definitions
Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Definitions
Induced Abortion The purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following a fetal death
Fetal Death Death prior to the complete expulsion or extraction of a product of conception from its mother irrespective of the duration of pregnancy The death is indicated by the fact that after such expulsion or extraction the fetus does not breathe or show any other evidence of life such as beating of the heart pulsation of the umbilical cord or definite movement of voluntary muscles
Fetal Remains MN Statutes 1451621 subd 2 The remains of a dead offspring of a human being that has reached a stage of development so that there are cartilaginous structures fetal or skeletal parts after an abortion or miscarriage whether or not the remains have been obtained by induced spontaneous or accidental means
Method of Abortion Suction Curettage Mechanical dilation of the cervix with removal of the uterine contents by low pressure suction created by an electric suction pump Medical Administration of medication to induce abortion This does not include administration of morning-after pills or post-coidal IUD insertion Dilation amp Evacuation Dilation of the cervix by insertion of laminaria several hours before removal of uterine contents by suction andor sharp curettage Intra-Uterine Instillation Induction of labor by injection of a sterile saline or prostaglandin (a naturally occurring hormone) solution into the amniotic sac Laminaria are often inserted in
the cervix several hours before the injection to aid dilation Hysterectomyotomy Removal of the fetus by means of a surgical incision made in the uterine wall In the case of a hysterectomy the entire uterus is removed Sharp Curettage Mechanical dilation of the cervix with removal of uterine contents by scraping the uterine wall with a surgical curette Induction of Labor Induction of labor by means of Pitocin andor related medications which causes uterine contractions and expulsion of uterine contents Dilation amp Extraction Dilation of the cervix and removal of fetal tissues
53
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
Data Collection Instruments
Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Center for Health Statistics REPORT OF INDUCED ABORTION Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
1-800-657-3900
3 Medical Specialty of the Physician Performing the Induced Abortion
Obstetrics amp Gynecology GeneralFamily Practice Emergency Medicine Other (Specify) _______________________
2 Physician Reporting Code
1 Facility Reporting Code
4 Type of Admission Clinic Outpatient hospital Inpatient hospital Ambulatory surgery Other (Specify) _______________
5 Patient Age at Last Birthday 6 Married Yes No
7 Date of Pregnancy Termination _____________________ Month Day Year
8 Patient Residence City_______________________________________ County ____________________________
State _____________ Zip Code
12 Date Last Normal Menses Began 13 Clinical Estimate of Gestation Month Day Year (LMP Weeks)
10 Race American Indian Asian Black White Other
(Specify) ___________________
9 Of Hispanic Origin Specify No or Yes If yes specify
Cuban Mexican Puerto Rican etc
No Yes
(Specify)___________
11 Education (Specify only highest grade completed)
ElementarySecondary (0-12)
College (1-4 or 5+)
14 Previous Pregnancies (Complete each section)
L i v e B i r t h s O t h e r T e r m i n a t i o n s
14a Now Living
Number
None
14b Now Dead
Number
None
14c Spontaneous
Number
None
14d Induced (Do not include this abortion)
Number
None
15 Contraceptive Use at Time of Conception A Use Status (Check only one)
Unknown - patient did not know if they used a method (Do not fill out Part B)
Never used any contraceptive method (Do not fill out Part B)
Has used contraception but not at the estimated time of conception (Do not fill out Part B)
Method used at time of conception (Fill out PART B METHOD USED)
Patient did not provide information
B Method Used Condoms Combination Pills Condoms amp Spermicide Diaphragm amp Spermicide Spermicide alone Diaphragm alone Sterilization (M) Cervical cap Sterilization (F) RhythmNatural Fam Planning Injectable (Depo-Provera) Fertility Awareness IUD Withdrawal Mini Pills Other (Specify)___________________________
57
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
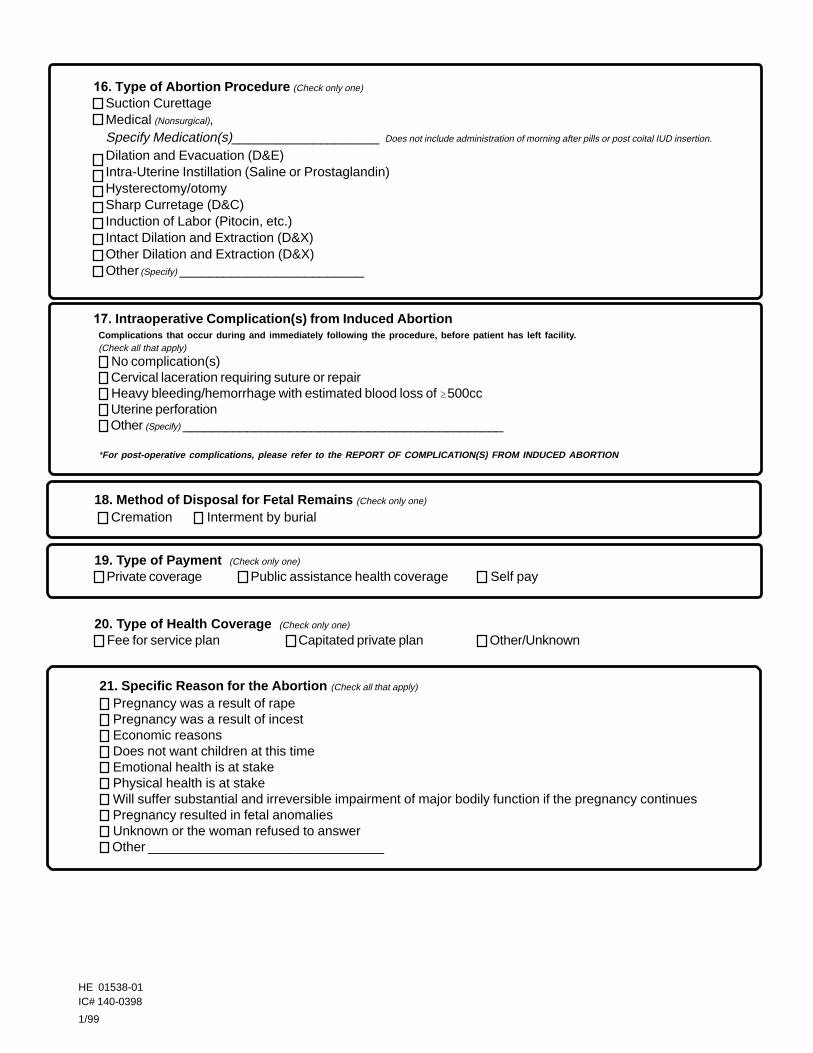
Complications that occur during and immediately following the procedure before patient has left facility (Check all that apply)
No complication(s) Cervical laceration requiring suture or repair Heavy bleedinghemorrhage with estimated blood loss of 500cc Uterine perforation Other (Specify) _____________________________________________
For post-operative complications please refer to the REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
16 Type of Abortion Procedure (Check only one)
Suction CurettageMedical (Nonsurgical)Specify Medication(s)____________________Does not include administration of morning after pills or post coital IUD insertion
Dilation and Evacuation (DampE)Intra-Uterine Instillation (Saline or Prostaglandin)HysterectomyotomySharp Curretage (DampC)Induction of Labor (Pitocin etc)Intact Dilation and Extraction (DampX)Other Dilation and Extraction (DampX)Other (Specify) _________________________
17 Intraoperative Complication(s) from Induced Abortion
18 Method of Disposal for Fetal Remains (Check only one)
Cremation Interment by burial
19 Type of Payment (Check only one)
Private coverage Public assistance health coverage Self pay
20 Type of Health Coverage (Check only one)
Fee for service plan Capitated private plan OtherUnknown
21 Specific Reason for the Abortion (Check all that apply)
Pregnancy was a result of rapePregnancy was a result of incestEconomic reasonsDoes not want children at this timeEmotional health is at stakePhysical health is at stakeWill suffer substantial and irreversible impairment of major bodily function if the pregnancy continuesPregnancy resulted in fetal anomaliesUnknown or the woman refused to answerOther ________________________________
HE 01538-01 IC 140-0398
199
58
Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Center for Health Statistics Minnesota Department of Health
85 East 7th Place Box 64882 Saint Paul MN 55164-0882
(800)657-3900
REPORT OF INDUCED ABORTION
Mandated reporters All physicians or facilities that perform induced abortions by medical or surgical methods
Induced abortion defined For purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
Importance of induced abortion reporting Reports of induced abortion are not legal records and are not maintained permanently in the files of the State office of vital statistics However the data they provide are very important from both a demographic and a public health viewpoint Data from reports of induced abortion provide unique information on the characteristics of women having induced abortions Uniform annual data of such quality are nowhere else available Medical and health information is provided to evaluate risks associated with induced abortion at various lengths of gestation and by the type of abortion procedure used Information on the characteristics of the women is used to evaluate the impact that induced abortion has on the birth rate teenage pregnancy and out-of-wedlock births Because these abortion data provide information necessary to promote and monitor health it is important that the reports be completed carefully
Physician and patient confidentiality According to MN Statutes sect1454134 the commissioner shall issue a public report providing statistics for the previous calendar year compiled from the data submitted under sections 1454131 to 1454133 Each report shall provide the statistics for all previous calendar years adjusted to reflect any additional information from late or corrected reports The commissioner shall ensure that none of the information included in the public reports can reasonably lead to identification of an individual having performed or having had an abortion All data included on the forms under sections 1454131 to 1454133 must be included in the public report except that the commissioner shall maintain as confidential data which alone or in combination may constitute information from which using epidemiologic principles an individual having performed or having had an abortion may be identified Service cannot be contingent upon a patient=s answering or refusing to answer questions on this form
MINNESOTA STATE LAW ARTICLE 10 HEALTH DATA REPORTING sect1454131 [RECORDING AND REPORTING ABORTION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this sectionthe commissioner shall prepare a reporting form for use by physicians or facilities performing abortions A copy of this section shall be attached tothe form A physician or facility performing an abortion shall obtain a form from the commissioner (b) The form shall require the followinginformation (1) the number of abortions performed by the physician in the previous calendar year reported by month (2) the method used for eachabortion (3) the approximate gestational age expressed in one of the following increments (i) less than nine weeks (ii) nine to ten weeks (iii) 11 to12 weeks (iv) 13 to 15 weeks (v) 16 to 20 weeks (vi) 21 to 24 weeks (vii) 25 to 30 weeks (viii) 31 to 36 weeks or (ix) 37 weeks to term (4) theage of the woman at the time the abortion was performed (5) the specific reason for the abortion including but not limited to the following (i) thepregnancy was a result of rape (ii) the pregnancy was a result of incest (iii) economic reasons (iv) the woman does not want children at this time(v) the womans emotional health is at stake (vi) the womans physical health is at stake (vii) the woman will suffer substantial and irreversibleimpairment of a major bodily function if the pregnancy continues (viii) the pregnancy resulted in fetal anomalies or (ix) unknown or the womanrefused to answer (6) the number of prior induced abortions (7) the number of prior spontaneous abortions (8) whether the abortion was paid forby (i) private coverage (ii) public assistance health coverage or (iii) self-pay (9) whether coverage was under (i) a fee-for-service plan (ii) acapitated private plan or (iii) other (10) complications if any for each abortion and for the aftermath of each abortion Space for a description of anycomplications shall be available on the form and (11) the medical specialty of the physician performing the abortion Subd 2 SUBMISSION] Aphysician performing an abortion or a facility at which an abortion is performed shall complete and submit the form to the commissioner no later thanApril 1 for abortions performed in the previous calendar year The annual report to the commissioner shall include the methods used to dispose offetal tissue and remains Subd 3 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or requiredsubmission of other reports or forms regarding abortions
59
REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

REPORTING PROCEDURE
COMPLETION AND SUBMISSION OF REPORTS
1 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Induced Abortion MDH recommends that these policies designate either the physician or the facility as having the overall responsibility and authority to see that the report is completed and filed on time This may help prevent duplicate reporting and failure to report If facilities take the responsibility to report on behalf of their physicians MDH suggests the following reporting procedure
lowast Notify physicians that the facility will be reporting on their behalf lowast Call the Minnesota Center for Health Statistics for assignment of facility reporting codes
and physician reporting codes (See instructions 2-3) Assign physician reporting codes to physicians and maintain a list of these assignments lowast Develop efficient procedures for prompt preparation and filing of the reports Collect and record the information required by the report lowast Prepare a correct and legible report for each abortion performed lowast Submit the reports to the Minnesota Center for Health Statistics within the time specified by the law lowast Cooperate with the Minnesota Center for Health Statistics concerning queries on report entries lowast Call on the Minnesota Center for Health Statistics for advice and assistance when necessary
If a facility decides not to report on behalf of their physicians or for physicians who perform induced abortions outside a hospital clinic or other institution the physician performing the abortion is responsible for obtaining a physician reporting code from MDH (See instruction 3) collecting all of the necessary data completing the report and filing it with the Minnesota Center for Health Statistics within the time period specified by law (See instruction 7)
2 Facility reporting codes All facilities reporting on behalf of physicians must be assigned a reporting code from MDH This code is in addition to individual physician reporting codes (See instruction 3) Facilities must submit a name and address to receive a facility code For facilities that have been reporting to MDH prior to October 1 1998 already have a facility reporting code and may continue to use the same code for future reporting
3 Physician reporting codes All physicians must be assigned a reporting code in order to submit a Report of Induced Abortion Reports submitted without a physician reporting code will be considered incomplete To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 1) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address
4 One report per induced termination of pregnancy Complete one report for each termination of pregnancy procedure performed
5 Criterion for a complete report All items on the report should have a response even if the response is ldquo0 Nonerdquo ldquoUnknownrdquo or ldquoRefuse to Answerrdquo
6 ldquoReason for abortionrdquo question MDH recommends that Item 21 on the report be reviewed with each patient All responses can be reviewed with the patient before completing the question If this question is transcribed to another piece of paper or read to the patient the question must be copied or read exactly as it is worded on the Report of Induced Abortion If the patient does not complete the question because she refuses to answer then the facility or physician must check the appropriate response which is ldquoRefuse to answerrdquo
7 Method of disposal for fetal remains Reporters should be informed that this question applies to disposal of fetal remains as defined under MN Statutes sect1451621 subd2
8 Submission dates Reports should be completed and submitted to the Center for Health Statistics as soon as possible following each procedure MDH encourages facilities and physicians to submit reports on a monthly basis but the final date for submitting reports is April 1 of the following year (eg all reports for procedures done in 1998 are due by April 1 1999) (MN Statutes 1998 sect145411)
60
Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

Center for Health Statistics Minnesota Department of Health
85 East 7th Place PO Box 64882 St Paul MN 55164-0882
(800)657-3900
REPORT OF COMPLICATION(S) FROM INDUCED ABORTION
A Facility where patient was attended for complication_________________________________________________ Name City
B Physician who treated patientrsquos complication (See instruction 1)
Name _______________________ ________________________ or Physician code ____ ____ ____ ____ Last First
C Medical specialty of physician who treated patientrsquos complication______________________________________
D Date complication was diagnosed ____________
E Exact date or patient recall of the date the induced abortion was performed
___ ___ Day ___ ___ Month ___ ___Year (Please indicate numeric day month and year If only month andor year is known please indicate in the spaces provided)
F Clinical or patientrsquos estimate of gestation at time of induced abortion _____ (weeks)
G Has patient acknowledged being seen previously by another provider for the same complication ____Yes ____No
1 Cervical laceration requiring suture or repair
2 Heavy bleedinghemorrhage with estimated blood loss of gt=500 cc
3 Uterine Perforation
4 Infection requiring inpatient treatment
5 Heavy bleedinganemia requiring transfusion
6 Failed termination of pregnancy (Continued viable pregnancy)
7 Incomplete termination of pregnancy (Retained products of conception requiring re-evacuation)
8 Other (May include psychological complications future reproductive complications or other illnesses or injuries that in the physicianrsquos medical judgment occurred as a result of an induced abortion Please specify diagnosis)
61
INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706

INSTRUCTIONS
MANDATED REPORTERS Any physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit the Report of Complication(s) from Induced Abortion
DEFINITION OF INDUCED ABORTION For the purpose of these reports induced abortion means the purposeful interruption of an intrauterine pregnancy with the intention other than to produce a live-born infant and which does not result in a live birth This definition excludes management of prolonged retention of products of conception following fetal death
PROCEDURE FOR COMPLETION AND SUBMISSION OF FORMS
1 Completion of items All forms should have completed information for items A-G Physicians may choose to use their name or a physician reporting code when submitting the Report of Complication(s) from Induced Abortion To obtain a code physicians or facilities reporting on behalf of physicians (See instruction 3) must call MDH to be assigned one code per physician MDH will require that a valid mailing address be provided for the purposes of keying the reporting code but no other identifying information will be asked or accepted Addresses provided may be a business address or an address established by the physician or facility such as a PO Box If facilities are reporting on behalf of their physicians the facility address may be used for the physician address Please note physicians who perform abortions should use the same physician reporting code when submitting the Report of Complication(s) from Induced Abortion and the Report of Induced Abortion
2 Reporting complications not indicated on the current list The category ldquoOtherrdquo should be used for any diagnosed complications that are not part of the current list The current complications list includes those complications that are supported both in the medical literature and by clinical opinion as being directly associated with induced abortion Because there are clinical opinions and data that suggest that there may be more complications associated with induced abortion the ldquoOtherrdquo category is provided to capture those types of complications If ldquoOtherrdquo is used be sure to clearly state the diagnosed complication in the space provided
3 Reporting by physician or facility The Minnesota Department of Health (MDH) Center for Health Statistics encourages physicians and facilities to develop internal policies for the completion and submission of the Report of Complication(s) from Induced Abortion These policies should designate either the individual physician or the facility as having the overall responsibility and authority to see that the reports are completed This may help prevent duplicate reporting or a failure to report When a complication from an induced abortion is encountered outside a hospital clinic or other institution the physician who encounters the complication is responsible for obtaining all of the necessary data completing the form and filing it with the Center for Health Statistics
4 Submission dates The Report of Complication(s) from Induced Abortion must be submitted by a physician or facility to the Center for Health Statistics as soon as practicable after the encounter with the abortion related illness or injury (MN Statutes 1998 sect 1453132)
MINNESOTA STATE LAW sect1454132 [RECORDING AND REPORTING ABORTION COMPLICATION DATA] Subdivision 1 [FORMS] (a) Within 90 days of the effective date of this section the commissioner shall prepare an abortion complication reporting form for all physicians licensed and practicing in the state A copy of this section shall be attached to the form (b) The board of medical practice shall ensure that the abortion complication reporting form is distributed (1) to all physicians licensed to practice in the state within 120 days after the effective date of this section and by December 1 of each subsequent year and (2) to a physician who is newly licensed to practice in the state at the same time as official notification to the physician that the physician is so licensed Subd 2 [REQUIRED REPORTING] A physician licensed and practicing in the state who knowingly encounters an illness or injury that in the physicians medical judgment is related to an induced abortion or the facility where the illness or injury is encountered shall complete and submit an abortion complication reporting form to the commissioner Subd 3 [SUBMISSION] A physician or facility required to submit an abortion complication reporting form to the commissioner shall do so as soon as practicable after the encounter with the abortion related illness or injury Subd 4 [ADDITIONAL REPORTING] Nothing in this section shall be construed to preclude the voluntary or required submission of other reports or forms regarding abortion complications
HE 01539-01 IC 140-0595
62199
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706
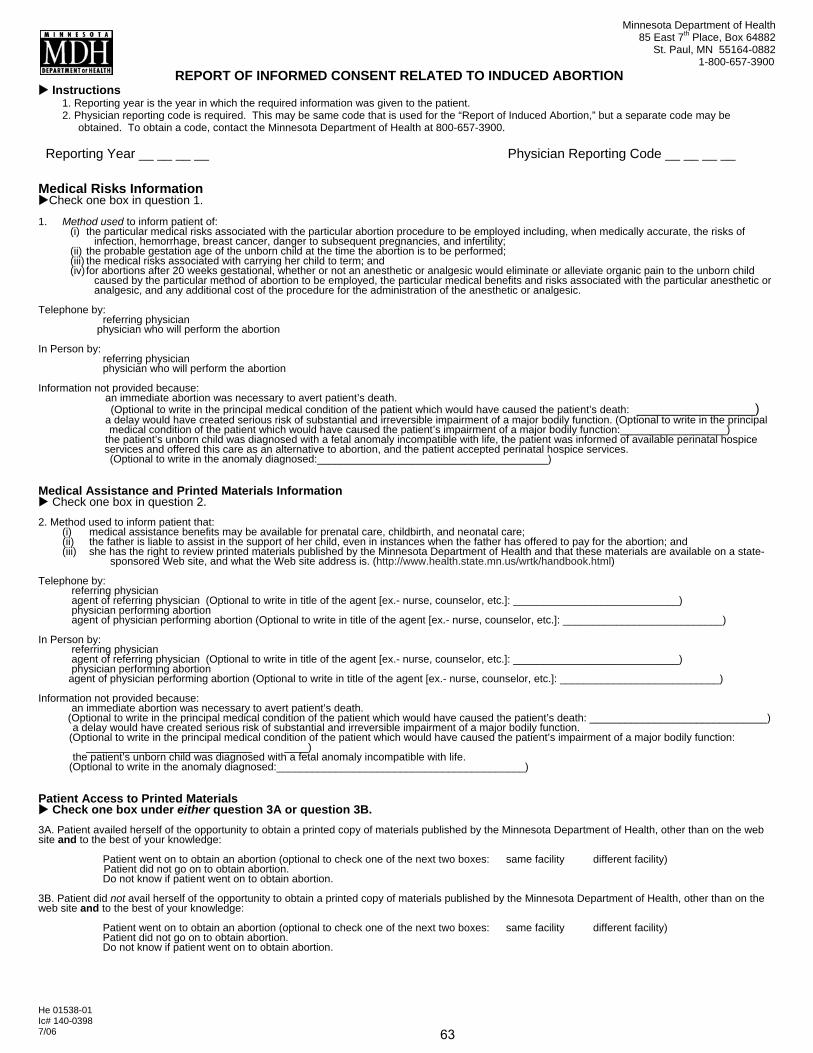
Minnesota Department of Health 85 East 7th Place Box 64882
St Paul MN 55164-0882 1-800-657-3900
REPORT OF INFORMED CONSENT RELATED TO INDUCED ABORTION X Instructions
1 Reporting year is the year in which the required information was given to the patient 2 Physician reporting code is required This may be same code that is used for the ldquoReport of Induced Abortionrdquo but a separate code may be
obtained To obtain a code contact the Minnesota Department of Health at 800-657-3900
Reporting Year __ __ __ __ Physician Reporting Code __ __ __ __
Medical Risks Information XCheck one box in question 1
1 Method used to inform patient of(i) the particular medical risks associated with the particular abortion procedure to be employed including when medically accurate the risks of
infection hemorrhage breast cancer danger to subsequent pregnancies and infertility(ii) the probable gestation age of the unborn child at the time the abortion is to be performed(iii) the medical risks associated with carrying her child to term and(iv) for abortions after 20 weeks gestational whether or not an anesthetic or analgesic would eliminate or alleviate organic pain to the unborn child
caused by the particular method of abortion to be employed the particular medical benefits and risks associated with the particular anesthetic or analgesic and any additional cost of the procedure for the administration of the anesthetic or analgesic
Telephone by referring physician physician who will perform the abortion
In Person by referring physician physician who will perform the abortion
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function (Optional to write in the principal
medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function__________________) the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life the patient was informed of available perinatal hospice services and offered this care as an alternative to abortion and the patient accepted perinatal hospice services
(Optional to write in the anomaly diagnosed_______________________________________)
Medical Assistance and Printed Materials Information X Check one box in question 2 2 Method used to inform patient that
(i) medical assistance benefits may be available for prenatal care childbirth and neonatal care (ii) the father is liable to assist in the support of her child even in instances when the father has offered to pay for the abortion and (iii) she has the right to review printed materials published by the Minnesota Department of Health and that these materials are available on a state-
sponsored Web site and what the Web site address is (httpwwwhealthstatemnuswrtkhandbookhtml)
Telephone by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
In Person by referring physician agent of referring physician (Optional to write in title of the agent [ex- nurse counselor etc] ____________________________) physician performing abortion agent of physician performing abortion (Optional to write in title of the agent [ex- nurse counselor etc] ___________________________)
Information not provided because an immediate abortion was necessary to avert patientrsquos death
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos death ______________________________) a delay would have created serious risk of substantial and irreversible impairment of a major bodily function
(Optional to write in the principal medical condition of the patient which would have caused the patientrsquos impairment of a major bodily function ____________________________ ____)
the patientrsquos unborn child was diagnosed with a fetal anomaly incompatible with life (Optional to write in the anomaly diagnosed__________________________________________)
Patient Access to Printed Materials X Check one box under either question 3A or question 3B 3A Patient availed herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion
Do not know if patient went on to obtain abortion
3B Patient did not avail herself of the opportunity to obtain a printed copy of materials published by the Minnesota Department of Health other than on the web site and to the best of your knowledge
Patient went on to obtain an abortion (optional to check one of the next two boxes same facility different facility) Patient did not go on to obtain abortion Do not know if patient went on to obtain abortion
He 01538-01 Ic 140-0398
63706